5-Amino-1MQ is a small-molecule NNMT inhibitor studied for its effect on fat-cell (adipocyte) metabolism and cellular NAD+ levels — the reason it shows up in “metabolic” and body-recomposition research rather than in appetite-suppression work. It is not a peptide, and it is not a GLP-1 drug; it works upstream, on an enzyme called nicotinamide N-methyltransferase (NNMT) that fat cells over-express when they become metabolically sluggish. Blocking that enzyme, in the preclinical literature, appears to free up NAD+ and push adipocytes back toward burning energy instead of storing it.
The practical questions researchers ask are always the same: how much per day, and by what route? Because 5-Amino-1MQ is a small molecule (not a large peptide), it can be studied orally as well as reconstituted for subcutaneous injection — and that route question is one of the most common points of confusion. This guide lays out the documented research protocol for both the 10 mg and 50 mg vials, shows the reconstitution arithmetic step by step, and gives a scannable weekly schedule, cycling framework, and realistic timeline.
One honest caveat up front, because it shapes everything below: the evidence base for 5-Amino-1MQ is almost entirely preclinical — mouse and cell-culture studies. There is no completed human efficacy trial. Everything here is framed as the documented research protocol used on this site’s 5-Amino-1MQ protocol pages, for research use only. None of it is a prescription, a treatment recommendation, or medical advice.

5-Amino-1MQ At a Glance
| Attribute | Detail |
|---|---|
| Use (research context) | NNMT inhibition, NAD+ preservation, adipocyte metabolism / body-composition research |
| Typical vial | 10 mg or 50 mg lyophilised powder |
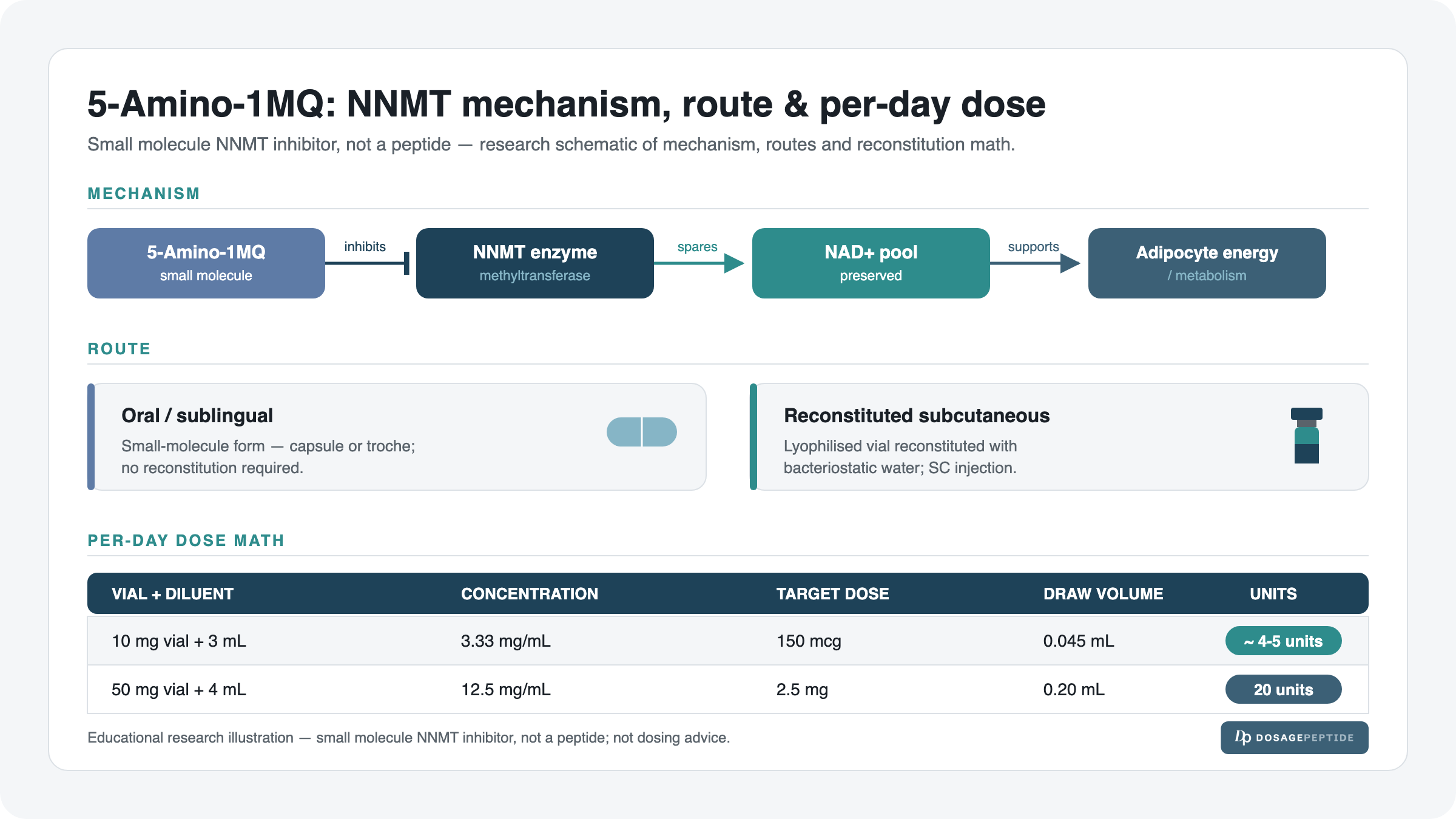
| Reconstitution | 10 mg vial in 3 mL bacteriostatic water (3.33 mg/mL); 50 mg vial in 4 mL (12.5 mg/mL) |
| Per-dose (documented) | 150 mcg from the 10 mg vial; 2.5 mg from the 50 mg vial |
| Schedule | Once daily in research; often morning; cycled (see cycling section) |
| Route | Small molecule — studied orally in the literature; also reconstituted for subcutaneous (SC) use in practitioner protocols |
| Onset / timeline | Gradual; metabolic changes reported over weeks in animal models, not instant |
| Common considerations | Injection-site reactions (SC route), GI upset (oral route); long-term human safety unknown |
| Best studied alongside | Caloric/exercise context in animal models; combined with NAD+ precursors in some research framing |
| Regulatory status | Not FDA-approved; investigational; research-use-only, not for human consumption |
What 5-Amino-1MQ Is (Composition & Mechanism)
5-Amino-1MQ (5-amino-1-methylquinolinium) is a small-molecule inhibitor of NNMT — nicotinamide N-methyltransferase. It is deliberately membrane-permeable, which is what lets it get inside cells and act on an intracellular enzyme. Chemically it is not a peptide at all, so the “peptide dosing” mental model only partly applies: the reconstitution math is identical, but the route options are broader (a small molecule can survive and be studied by mouth in a way most peptides cannot).
Because it is a single compound rather than a blend, there is no multi-component composition table to break down — but the mechanism is worth mapping out, because it explains why the research doses are so small and why the effect is gradual rather than acute.
| Step | What happens (biology) | Why it matters |
|---|---|---|
| 1. NNMT is over-expressed | In sluggish/enlarged fat cells, the NNMT enzyme is up-regulated and consumes methyl groups and NAD+ precursors | This is the “brake” on adipocyte energy metabolism |
| 2. 5-Amino-1MQ inhibits NNMT | The molecule blocks NNMT’s activity inside the cell | Takes the brake off — the target of the whole protocol |
| 3. NAD+ is spared | With NNMT inhibited, less nicotinamide is methylated away; cellular NAD+ is preserved | NAD+ is the currency of mitochondrial energy metabolism |
| 4. Adipocyte metabolism shifts | In mouse models, fat cells trend toward energy expenditure rather than storage | The mechanistic basis for its “metabolic” research interest |
The key contrast to draw for readers coming from the weight-management space: this is not a GLP-1. It does not suppress appetite or slow gastric emptying. It is an intracellular metabolic-enzyme modulator, which is why its research read-outs are things like NAD+ levels and adipocyte gene expression, not “how full you feel.” That mechanistic distinction is the single most important thing to understand before looking at any dose number.
To unpack why the mechanism matters for dosing: NNMT sits at a metabolic crossroads. It uses a methyl group donated by S-adenosylmethionine (SAM) to methylate nicotinamide — a vitamin B3 form that would otherwise be recycled back into NAD+. When a cell over-expresses NNMT, it does two costly things at once: it burns through methyl-donor capacity, and it diverts nicotinamide away from NAD+ regeneration into an inert metabolite (1-methylnicotinamide) that gets excreted. In enlarged, over-fed adipocytes, that combination effectively nudges the cell toward a low-energy, storage-favouring state. The research rationale for a selective NNMT inhibitor is to interrupt exactly that diversion, so the cell keeps more of its NAD+ pool and can run its mitochondrial machinery again.
Two practical consequences fall out of this mechanism, and both explain the shape of the protocol below. First, the effect is enzymatic and cumulative — you are shifting a metabolic set-point over days and weeks, not triggering an acute hormonal event, which is why steady daily exposure matters more than any single large dose. Second, the doses are small because the target is a high-affinity intracellular enzyme, not a receptor that needs saturating with milligrams of drug. That is why a 150 mcg figure — a fraction of what many injectable peptides use — is the documented starting point for the 10 mg vial. Neither point is a claim that it works in humans; both simply describe why the research protocol looks the way it does.
How to Dose 5-Amino-1MQ (The Documented Research Protocol)
Every number in this section is the documented research protocol from this site’s own protocol pages — the 10 mg vial protocol and the 50 mg vial protocol. These are research figures, framed for research use only; they are not a prescription and not a personal dosing recommendation. For any per-user calculation, use the dosage calculator rather than adjusting numbers by hand.
| Vial size | Documented research dose | Frequency | Route (research) |
|---|---|---|---|
| 10 mg vial | 150 mcg per dose | Once daily | Oral/sublingual in the literature; SC in practitioner protocols |
| 50 mg vial | 2.5 mg per dose | Once daily | Oral/sublingual in the literature; SC in practitioner protocols |
Note that these two documented starting doses are worlds apart in size — 150 mcg versus 2.5 mg is a roughly 17-fold difference. That is intentional: the two vial sizes reflect two different documented protocols and two different concentration setups, and it is a reminder never to eyeball a dose across vial sizes. Draw and dose against the concentration of the specific vial in front of you, which is exactly what the reconstitution math below forces you to do.
A word on why “once daily” is the anchoring frequency rather than something more elaborate. Because the target is an enzyme and the intended effect is a gradual shift in cellular NAD+ handling, the research framing does not treat 5-Amino-1MQ as a pulse-and-recover compound the way a growth-hormone secretagogue is treated. There is no receptor to desensitise on a fast clock, and no acute spike to time around a meal. The documented pattern is simply a steady daily presence of the inhibitor, held long enough for the downstream metabolic change to accumulate. That is why the schedule section below is deliberately boring — steadiness is the point.
It is also worth being explicit about what “documented” means here, because it is the load-bearing word for a YMYL page. These figures are not extrapolated from a human trial (there isn’t one) and they are not scaled from the mouse papers. They are the per-dose amounts published on this site’s own protocol pages for each vial size, which is the reference this guide is built to explain and make arithmetically checkable. That is a deliberately narrow claim: the number is what the protocol says, the math shows exactly how it converts to a syringe draw, and everything about whether the compound does anything in a human is left to the honest evidence section rather than smuggled into the dose. Keeping those two things separate — the documented figure versus the efficacy claim — is the whole point of the structure.
The route question: oral vs subcutaneous
This is the most-searched practical question about 5-Amino-1MQ, so let’s answer it directly and honestly. Because 5-Amino-1MQ is a small molecule — not a fragile peptide chain — it can be studied by mouth. Much of the research framing treats it as an orally administered compound, and in practitioner circles it circulates in oral/sublingual forms (capsules, or the reconstituted solution taken sublingually). That is genuinely different from most peptides, which are destroyed in the gut and therefore have to be injected.
At the same time, the vialed lyophilised powder can be reconstituted with bacteriostatic water and used subcutaneously (SC), which is why people search “5-amino-1mq dosage subcutaneous.” Both routes appear in research and practitioner protocols. The honest position is this: there is no head-to-head human bioavailability trial telling you which route is superior for this specific molecule, so the “best route” is not a settled question. The dose figures above are the documented per-dose amounts; how they translate across routes is an open research question, not a solved one. Whichever route a protocol specifies, the reconstitution math below is what governs the injectable draw.
It helps to understand why the route question is even open for this compound when it is closed for most peptides. A peptide is a chain of amino acids held together by peptide bonds, and those bonds are precisely what digestive enzymes (pepsin, trypsin) are built to cut, with the acidic stomach environment finishing the job — so an oral peptide is largely destroyed before it can be absorbed, which is why injection is the default. 5-Amino-1MQ has no peptide bonds to cleave. It is a single small aromatic molecule designed to be membrane-permeable, so in principle it can survive the gut and cross into cells. That is the entire basis for the “you can take it orally” framing you will see repeated online.
The catch — and this is where honesty matters on a YMYL page — is that “can survive the gut in principle” is not the same as “has a proven, quantified oral bioavailability in humans.” No such human number exists for this molecule. So the practical takeaway is not “oral is better” or “SC is better.” It is: pick one route, follow the documented per-dose figure for the vial you have, and keep the route constant so that whatever you observe is not confounded by a mid-stream route change. If a protocol specifies SC, the reconstitution math below is exactly what you need; if it specifies oral/sublingual, the same per-dose amount is the reference point, delivered by that route instead of a syringe.
Reconstitution & Draw (With the Real Math)
Here is the arithmetic, shown step by step for both vials. If you want the underlying logic explained from scratch, see the peptide reconstitution guide, the guide to how much bacteriostatic water to use, and the insulin syringe units guide. To skip the hand math entirely, the dosage calculator does all of this for you.
The single principle that makes every calculation below work is this: concentration is drug divided by water. Once you know the concentration in mg/mL, a dose in mg becomes a volume in mL by simple division, and that volume becomes insulin-syringe units by multiplying by 100 (because a U-100 syringe is marked so that 1 mL = 100 units). Every step is that same chain — mg into the vial, mL of water, then divide and multiply. The reason to show it long-hand rather than just stating the answer is that on the 10 mg vial the draw is tiny, and a reader who understands the chain can catch an error the moment a number looks wrong.
10 mg vial → 3 mL → 150 mcg dose
- Concentration: 10 mg ÷ 3 mL = 3.33 mg/mL (that is 3,333 mcg per mL).
- Draw volume for a 150 mcg dose: 0.150 mg ÷ 3.33 mg/mL = 0.045 mL.
- Units on a U-100 syringe: 0.045 mL × 100 = 4.5 units (round to the ~4–5 unit mark on the barrel).
Because 4.5 units is a very small draw, precision matters. A U-100 insulin syringe with half-unit or fine gradations makes this dose far easier to measure accurately than a standard 1 mL syringe. If you find the 4–5 unit mark uncomfortably small to read, the honest options are (a) use a finer-gradation syringe, or (b) follow a protocol built around the 50 mg vial, whose larger draw is more forgiving — not to freehand a bigger volume from the 10 mg vial, which would silently overdose relative to the documented figure.
50 mg vial → 4 mL → 2.5 mg dose
- Concentration: 50 mg ÷ 4 mL = 12.5 mg/mL.
- Draw volume for a 2.5 mg dose: 2.5 mg ÷ 12.5 mg/mL = 0.20 mL.
- Units on a U-100 syringe: 0.20 mL × 100 = 20 units.
The 50 mg setup is far easier to draw accurately (20 units is a clean, mid-barrel mark) because the higher concentration and larger per-dose amount land on a bigger, more forgiving volume. This is the practical reason a reader who is nervous about small-volume accuracy might prefer the 50 mg protocol — the trade-off being that each vial carries fewer total doses, as the supply math shows next.
Supply math (doses per vial)
| Vial | Total drug | Per dose | Doses per vial |
|---|---|---|---|
| 10 mg | 10 mg (10,000 mcg) | 150 mcg | 10,000 ÷ 150 ≈ 66 doses |
| 50 mg | 50 mg | 2.5 mg | 50 ÷ 2.5 = 20 doses |
At once-daily dosing, the 10 mg vial covers roughly nine weeks of research use, while the 50 mg vial (at its larger 2.5 mg documented dose) covers about twenty days. That gap is worth planning around: the beyond-use window of a reconstituted solution (covered in the storage section) can be shorter than the drug supply lasts, especially for the 10 mg vial, so re-order and reconstitution-volume decisions should be made against the shorter of the two limits — the stability window or the drug supply — not just the drug supply alone.
Example Weekly Schedule
The documented framing is once daily. Here is one example research week for the 10 mg vial at 150 mcg (≈4–5 units), dosed in the morning. This is an illustrative research schedule, not a prescription.
| Day | Mon | Tue | Wed | Thu | Fri | Sat | Sun |
|---|---|---|---|---|---|---|---|
| Dose | 150 mcg | 150 mcg | 150 mcg | 150 mcg | 150 mcg | 150 mcg | 150 mcg |
| Timing | AM | AM | AM | AM | AM | AM | AM |
| Route | Consistent route per protocol (oral/sublingual or SC) — do not switch mid-week | ||||||
Some research framings use a 5-days-on / 2-off pattern to build in a weekly break; others run continuous daily for a fixed block. Both appear below in the cycling section. The one constant is consistency of timing and route — for a mechanism that works by gradually shifting cellular metabolism, day-to-day steadiness matters more than any single dose. If a day is missed, the research-sensible response is simply to resume the next scheduled dose, not to “double up,” because there is no acute deficit to make good and doubling only departs from the documented figure.
Dosing Phases & Cycling
5-Amino-1MQ is a metabolic-enzyme modulator, so the documented research pattern treats it as a run-in, steady-state, then off compound rather than something you pulse and stop. Framed as a research schedule (not a prescription):
- Activation (Weeks 1–2): Begin at the documented once-daily dose and hold it steady. This is the run-in period where NNMT inhibition is being established; do not expect visible read-outs yet. The useful observation in this window is simple tolerability — whether the chosen route is comfortable and consistent.
- Steady state (Weeks 3–8): Continue the same daily dose. In animal models, this is the window over which metabolic and adipocyte changes accumulate. The temptation to escalate the dose because “nothing is happening yet” is exactly the mistake the timeline section is designed to head off — the mechanism is cumulative, not dose-chased.
- Off / washout (after the block): A typical research framing runs a defined block (commonly 8–12 weeks) followed by an off period before any subsequent block, rather than indefinite continuous use — because long-term human data simply do not exist.
On/off cycling here is driven by caution, not by tolerance data: because there is no long-term human safety record, building in scheduled off periods is the conservative research default. There is no established evidence that continuous use is either necessary or safe over long horizons. Put plainly, the off period is not there because the compound “stops working” — it is there because no one can point to human data showing that running it indefinitely is safe, and a scheduled break is the honest way to respect that gap.
Timeline: What to Expect
Set expectations honestly. 5-Amino-1MQ is not an acute-effect compound — there is no same-day “kick.” Everything below is research-framed and drawn largely from animal-model observations; these are not personal-result promises.
| Week / Phase | What’s happening (biology) | What is observed in research |
|---|---|---|
| Week 1–2 (activation) | NNMT inhibition establishing; NAD+ being spared at the cellular level | No visible metabolic read-out expected this early; tolerability is the main observation |
| Week 3–4 | Adipocyte energy metabolism trending toward expenditure in models | Early metabolic shifts reported in animal studies, not instant body changes |
| Week 5–8 (steady state) | Sustained NNMT inhibition; cumulative metabolic effect in preclinical work | Body-composition changes reported in mouse models over comparable windows |
| Week 8–12 (block end) | Effect assessed; washout considered | In animal models this is where the clearest preclinical differences appear; no human efficacy data exist |
For a fuller, expectations-level walk-through, see the 5-Amino-1MQ results timeline. The single most important framing: efficacy figures for this molecule come from cell and animal studies, so any timeline is a research expectation, not a guaranteed outcome. A mouse metabolises on a faster clock than a human, and a controlled diet in a cage is not a free-living human diet — so even the week-numbers above should be read as the shape of a gradual response, not a promise that a human would see anything on the same calendar.
Stacking & Combinations
Because its mechanism is NAD+ preservation, the logical research pairing is with the NAD+ pathway: in some research framings, an NNMT inhibitor like 5-Amino-1MQ is discussed alongside NAD+ precursors, on the reasoning that inhibiting the enzyme that drains NAD+ and supplying more NAD+ substrate address the same bottleneck from two directions. The bottleneck is cellular NAD+ availability; 5-Amino-1MQ removes a drain on it, while a precursor tops up the supply. On paper the two are complementary rather than redundant — one stops a leak, the other adds water to the tank.
The other consistent context in the preclinical literature is a metabolic environment — the mouse studies pair the compound with diet/energy-balance conditions rather than testing it in isolation. In other words, the preclinical signal appears against a backdrop of controlled energy intake and activity, not as a standalone effect that overrides diet. That is an important framing for anyone tempted to treat it as a shortcut: even in the animal work that generates the interest, the compound is one input alongside energy balance, not a replacement for it.
The bottleneck logic is worth stating cleanly, because it is what separates a coherent research pairing from wishful stacking. A useful combination targets a different rate-limiting step in the same pathway; a redundant one just hits the same step twice. On that test, an NNMT inhibitor plus an NAD+ precursor is at least internally coherent — one addresses the drain, the other the supply — while pairing 5-Amino-1MQ with an unrelated appetite-acting compound is not “synergy,” it is simply two separate interventions being run at once. The honest boundary is that even the coherent pairing is a mechanistic hypothesis with no human validation, so the most defensible research posture is to study the single compound at its documented dose first, and treat any combination as a further, clearly-labelled research question rather than a default.
Browse the wider dosage catalog to see how single compounds and blends are documented across the site, and treat any “stack” as an area of open research rather than a settled recipe.
When Progress Stalls
A short troubleshooting ladder, framed for research review rather than dose-chasing. The default response to a stall is almost never “take more” — it is to check the controllable variables first.
| Bottleneck | Likely cause | Adjustment (research-framed) |
|---|---|---|
| No observable change by week 4 | Too-early expectation; this is a gradual mechanism | Hold the documented dose; the preclinical timeline runs to weeks 8–12, not days |
| Inconsistent dosing | Missed days / variable timing undermine steady NNMT inhibition | Fix timing and route consistency before considering any dose question |
| Uncertain draw accuracy (10 mg vial) | 4–5 units is a very small volume to measure | Use a fine-gradation U-100 syringe; re-verify the math via the calculator |
| Route confusion | Switching between oral and SC mid-block | Pick one route per protocol and hold it; document it |
| Solution looks off / stored too long | Beyond-use window passed or freeze–thaw degradation | Discard and reconstitute fresh per the storage section; do not push a questionable vial |
Side Effects & Mitigation
Because there is no completed human safety trial, the honest statement is that the human side-effect profile is not well characterised. The items below are route-related and general-caution considerations, not a validated adverse-event list.
| Issue | Why | Mitigation |
|---|---|---|
| Injection-site redness / irritation (SC route) | Local reaction to subcutaneous injection | Rotate sites; sterile technique; correct reconstitution per the reconstitution guide |
| GI upset (oral/sublingual route) | Small molecules taken by mouth can cause mild GI effects | Consistent timing; note tolerability; researchers adjust route framing accordingly |
| Unknown long-term effects | No long-term human data exist for this compound | Use scheduled off periods; do not run indefinitely; keep doses to the documented figures |
| Dosing error (small draws) | 4–5 unit draws amplify measurement error | Fine-gradation syringe; verify with the calculator; never eyeball across vial sizes |
The most important line in that table is the third one. For most compounds the headline safety question is “what are the side effects?” For 5-Amino-1MQ the honest headline is “we do not yet know,” and the correct response to not-knowing is conservatism — documented doses, scheduled breaks, and a licensed clinician in the loop — rather than assuming the absence of reported effects means the absence of risk.
Safety & Contraindications
- Not FDA-approved. 5-Amino-1MQ is an investigational compound with no approved human indication. It is research-use-only and not for human consumption.
- No completed human efficacy or safety trial. The evidence is preclinical (mouse and cell studies). Human dosing, long-term safety, and drug interactions are not established.
- Not a substitute for evaluated metabolic care. It is not a GLP-1, not a weight-loss drug, and should not be treated as one.
- Anyone pregnant, breastfeeding, or with a diagnosed metabolic, hepatic, or endocrine condition falls entirely outside any studied context and should not be a subject of self-directed use.
- Unknown drug interactions. Because it modulates a methylation and NAD+ pathway, interactions with other metabolically active compounds cannot be ruled out and have not been characterised in humans.
- Consult a licensed clinician before any use. This guide documents a research protocol; it does not endorse human use.
The reason the “who should avoid” list is framed so broadly is not boilerplate caution. When a compound has no completed human trial, there is by definition no safety data in any subgroup — no pregnancy data, no hepatic-impairment data, no interaction data with common metabolic or endocrine medications. In that situation the responsible default is not “assume it is fine unless proven harmful”; it is the reverse. Anyone outside a healthy, monitored research context — and especially anyone in one of the sensitive groups above — sits entirely beyond the edge of what has been studied, which is exactly why a clinician’s judgement, not a web page, is the right place for that decision to be made.
Storage & Handling
- Before reconstitution: store the lyophilised vial per supplier guidance — cool, dry, dark. Many research powders are kept refrigerated or frozen until use.
- After reconstitution: store the solution at 2–8 °C (refrigerated) and protect it from light.
- Beyond-use window: reconstituted solution has a limited stable life (commonly a few weeks refrigerated); the exact window depends on the product and diluent. Discard past the beyond-use window rather than pushing it.
- Freeze rules: do not repeatedly freeze–thaw a reconstituted solution; freeze–thaw cycling degrades many research compounds. If long storage is needed, follow product-specific freezing guidance rather than improvising.
Use bacteriostatic (not plain sterile) water for a multi-dose vial so the preservative supports the multi-draw window, and reconstitute gently down the vial wall rather than blasting the powder. For a fuller walk-through of pre- and post-mixing storage, see the guide on how to store peptides before and after reconstitution. This is also where the supply-versus-stability point from the reconstitution section bites: if a reconstituted 10 mg vial holds ~66 doses but the solution is only reliably stable for a few weeks, plan the reconstitution volume so you are not left discarding drug you paid for.
What the Evidence Actually Shows
Here is the transparent version. The interest in 5-Amino-1MQ rests on a small number of preclinical studies, and it is important to name what kind of evidence each is.
The foundational obesity finding comes from Kraus and colleagues (Nature, 2014), who showed that knocking down NNMT protected mice against diet-induced obesity — establishing NNMT as a metabolic target in the first place. That is a genetic-knockdown study in mice, not a drug trial: it tells you the target is real and metabolically meaningful in an animal model, but it does not test a drug, a dose, or a route. It is the “why NNMT is interesting at all” paper.
Neelakantan and colleagues (Biochem Pharmacol, 2017) then took the pharmacological step, reporting that selective, membrane-permeable small-molecule NNMT inhibitors reversed high-fat-diet-induced obesity in mice — this is the study most directly relevant to the 5-Amino-1MQ class, because it moves from “the target matters” to “a drug against the target does something in a live animal.” And again, it is a mouse study. It supplies the mechanistic and directional rationale for the whole compound class, but it is not a human trial and does not establish a human dose.
Both are legitimate, mechanistically coherent, and encouraging as far as they go. But they are animal and cell work. There is, per ClinicalTrials.gov, no completed human efficacy trial for 5-Amino-1MQ. That is the evidence gap, stated plainly: the mechanism is well-motivated and the preclinical signal is consistent, but no human study has confirmed that any of it translates to people, at any dose, by any route. Being honest about that gap is not a weakness of this guide — it is the accurate picture, and it is why every dosing figure here is framed as a research protocol rather than a recommendation. A reader is best served by holding two things at once: the mechanism is genuinely interesting, and the human evidence does not yet exist.
How to read preclinical evidence without over-reading it
Preclinical does not mean worthless — it means early. A knockdown study and a small-molecule mouse study are exactly the steps that should precede a human trial, and they are the reason a compound gets taken seriously enough to be studied further. So the two papers above are doing real scientific work. The mistake is to treat them as if they were the last step rather than the first. Three specific gaps separate this preclinical evidence from a human recommendation, and it is worth naming each so the framing throughout this guide is not mistaken for false modesty.
The first gap is species. Mouse metabolism, mouse fat biology, and mouse dosing all differ from the human versions, and metabolic findings in rodents have a long history of not carrying over cleanly to people. The second is dose and route translation: even where an effect is real in a mouse, the human-equivalent dose is not a simple body-weight scaling, and — as the route section above stressed — there is no human bioavailability figure to anchor an oral-versus-injected comparison. The third is duration and safety: short controlled studies in animals say almost nothing about what months or years of exposure would do in a human, which is precisely why the cycling section defaults to scheduled off periods rather than open-ended use. None of this makes the mechanism uninteresting. It makes the correct posture one of documented, conservative, research-framed use — not confident self-treatment.
Frequently Asked Questions
Choosing it
Is 5-Amino-1MQ a peptide? No. It is a small-molecule NNMT inhibitor. That matters because, unlike most peptides, a small molecule can be studied orally as well as by injection — it has no peptide bonds for digestive enzymes to cleave.
Is 5-Amino-1MQ like a GLP-1 (e.g., semaglutide)? No. It does not suppress appetite or slow gastric emptying. It works intracellularly by inhibiting NNMT to preserve NAD+ and shift adipocyte metabolism — a completely different mechanism, with different research read-outs.
Should I choose the 10 mg or 50 mg vial? They correspond to two different documented protocols and per-dose amounts (150 mcg vs 2.5 mg). The 50 mg vial’s larger, cleaner draw is easier to measure; the 10 mg vial gives more doses per vial. Choose based on the protocol you are following, and never carry a dose over from one vial size to the other.
Does it have completed human trials behind it? No. The evidence is preclinical — mouse and cell studies. There is no completed human efficacy trial, which is why all dosing here is research-use-only.
Using it
How much 5-Amino-1MQ per day? The documented research protocol is once daily: 150 mcg from the 10 mg vial, or 2.5 mg from the 50 mg vial. Use only these documented figures; run per-user math through the dosage calculator.
How do I take 5-Amino-1MQ — oral or subcutaneous? Both appear in research and practitioner protocols. Because it is a small molecule, it is studied orally/sublingually in the literature; the vialed powder can also be reconstituted for subcutaneous use. There is no human head-to-head bioavailability trial declaring one route superior, so pick the route your protocol specifies and hold it consistently.
What is the subcutaneous dose specifically? The documented per-dose amounts (150 mcg from the 10 mg vial; 2.5 mg from the 50 mg vial) are what you draw and inject SC after reconstitution — 4–5 units and 20 units respectively on a U-100 syringe (see the math above).
How do I reconstitute the 10 mg vial? 10 mg in 3 mL bacteriostatic water = 3.33 mg/mL. A 150 mcg dose = 0.045 mL = about 4–5 units on a U-100 syringe. Full walk-through in the reconstitution guide.
What time of day should I dose it? Research framings commonly use morning, once daily. The most important factor is consistency of timing and route day to day, since the mechanism works cumulatively rather than as an acute event to time around a meal.
How long until 5-Amino-1MQ works? It is gradual, not instant. Preclinical timelines run over weeks — meaningful model-level changes appear across roughly weeks 4–12, not in the first days. See the results timeline.
Practical & safety
How many doses are in a vial? The 10 mg vial gives about 66 doses at 150 mcg; the 50 mg vial gives 20 doses at 2.5 mg. Match your re-order timing to the beyond-use window, not just the drug supply.
How should I cycle it? A common research framing is a defined block (often 8–12 weeks) followed by an off period, rather than indefinite continuous use — a conservative default given the absence of long-term human data.
What syringe do I need? A U-100 insulin syringe. For the 10 mg vial’s small 4–5 unit draw, use fine gradations for accuracy — details in the insulin syringe units guide.
How do I store it after mixing? Refrigerate at 2–8 °C, protect from light, and observe the beyond-use window. Avoid repeated freeze–thaw cycles.
Is it safe? Its human safety profile is not established — there is no completed human trial. It is not FDA-approved, is research-use-only, and is not for human consumption. Consult a licensed clinician before any use.
References
- Neelakantan H, et al. Selective and membrane-permeable small molecule inhibitors of nicotinamide N-methyltransferase reverse high fat diet-induced obesity in mice. Biochem Pharmacol, 2017. PMID 29155147.
- Kraus D, et al. Nicotinamide N-methyltransferase knockdown protects against diet-induced obesity. Nature, 2014. PMID 24717514.
- ClinicalTrials.gov — no completed 5-Amino-1MQ human efficacy trial (evidence-gap note).
Disclaimer: This article is for research and educational purposes only. It is not medical advice. 5-Amino-1MQ is an investigational, research-use-only compound; it is not FDA-approved and not for human consumption. All dosing figures describe a documented research protocol, not a prescription or a personal recommendation. No statement here is a guarantee of any outcome. Consult a licensed clinician before making any health-related decision.
