Few molecules have reshaped modern medicine as quickly as glucagon-like peptide-1 (GLP-1). What began as an obscure gut hormone studied in physiology labs has become the biological engine behind the most talked-about diabetes and weight-loss medications of the decade. Understanding GLP-1 means understanding how your body coordinates blood sugar, appetite, and digestion after every meal — and why pharmaceutical scientists spent thirty years learning to imitate it.
This guide is a deep educational dive into the science: what native GLP-1 actually is, how it works at the cellular level, why the hormone had to be re-engineered into stable drugs, and how the full modern class — from single-target agonists to dual and triple hormone mimics, injectable and oral — compares. It is written for peptide and health enthusiasts who want the real biology, not marketing copy. Nothing here is medical advice; it is research and education, and every therapeutic agent’s regulatory status is stated as accurately as current evidence allows.
What Is GLP-1 (Glucagon-Like Peptide-1)?
GLP-1 is an incretin hormone — a signaling peptide secreted by the gut in response to eating that amplifies the body’s insulin response and coordinates the metabolic handling of a meal. It is produced primarily by enteroendocrine L-cells lining the distal small intestine and colon, with the highest density in the ileum, and it is released within minutes of nutrients arriving in the gut.[1]
The name is a clue to its origins. GLP-1 is cleaved from a larger precursor protein called proglucagon, the same parent molecule that gives rise to glucagon in the pancreas. Depending on which tissue processes proglucagon and which enzymes act on it, the body produces either glucagon (in pancreatic alpha-cells) or GLP-1 and its sibling GLP-2 (in intestinal L-cells and in some neurons of the brainstem). This shared ancestry is why the peptide is called “glucagon-like” — it is structurally related to glucagon, even though its metabolic effects are largely opposite.
Despite that family resemblance, the functional distinction is critical. Glucagon raises blood glucose by telling the liver to release stored sugar. GLP-1 does the reverse: it lowers glucose through a coordinated set of actions that make it central to both glucose homeostasis and appetite regulation. That single biological fact — a naturally occurring hormone that safely lowers blood sugar and reduces hunger — is what made GLP-1 such an attractive drug target.
Where GLP-1 Comes From and When It Is Released
L-cells are open-type enteroendocrine cells, meaning they have a surface that faces directly into the gut lumen and can “taste” the contents of a meal. When carbohydrates, fats, and to a lesser extent proteins reach them, these cells secrete GLP-1 into the bloodstream. Carbohydrate and lipid ingestion are the most potent stimuli for secretion; protein is a weaker trigger.[1] Circulating GLP-1 rises within about 10 to 15 minutes of eating and reflects both the size and the composition of the meal.
A small amount of GLP-1 is also produced outside the gut — by certain neurons in the nucleus of the solitary tract in the brainstem, and in trace amounts by the pancreas — which helps explain why the hormone influences appetite and the central nervous system so directly, not just through the bloodstream.
It is worth pausing on the two active forms of the peptide. When proglucagon is processed in L-cells, the result is initially GLP-1(1-37), which is then trimmed to the biologically active forms GLP-1(7-37) and GLP-1(7-36)amide. The amidated form, GLP-1(7-36)amide, is the predominant circulating species in humans. Both are potent at the receptor, and both are equally vulnerable to the enzyme that cuts them down almost as soon as they appear. This detail matters because the exact position of that enzymatic cut — between the eighth and ninth amino acids — is precisely the vulnerability that drug designers had to engineer around, as described later in this guide.
GLP-1 Versus GIP: The Two Incretins
GLP-1 is one of two major incretin hormones. The other is glucose-dependent insulinotropic polypeptide (GIP), secreted by K-cells in the upper small intestine (the duodenum and jejunum). Together, GLP-1 and GIP account for the majority of the incretin effect — the phenomenon that lets your body extract more insulin from an oral meal than from the same amount of glucose delivered intravenously.
The two hormones are not interchangeable. GIP primarily stimulates insulin secretion and supports pancreatic beta-cell health, but has little effect on appetite or glucagon. GLP-1 stimulates insulin, suppresses glucagon, slows gastric emptying, and powerfully reduces appetite. Crucially, in people with type 2 diabetes the insulin-stimulating action of GIP is substantially blunted, whereas GLP-1 — especially at higher, pharmacological doses — still works.[1] That difference is exactly why the first generation of incretin drugs targeted GLP-1 rather than GIP, and why combining the two came only later.
What Is the Incretin Effect and Why Does It Matter?
The incretin effect is one of the most elegant discoveries in endocrine physiology. When researchers gave people glucose by mouth and then, on a separate occasion, infused glucose intravenously to reach the exact same blood-sugar levels, they found that the oral route triggered dramatically more insulin. The body somehow “knew” the glucose had come through the gut. The messengers responsible for that extra insulin are the incretin hormones.[1]
In healthy people, the incretin effect can account for roughly 50 to 70 percent of the total insulin response to an oral glucose load. This is the body’s way of anticipating a nutrient surge and pre-loading the pancreas to respond before blood sugar climbs too high. It is a feed-forward system: the gut senses food and warns the pancreas in advance.
In type 2 diabetes, the incretin effect is diminished. This impairment is driven mainly by the loss of GIP’s insulinotropic action, while responsiveness to GLP-1 is comparatively preserved.[1] Restoring or amplifying GLP-1 signaling therefore became a rational strategy for treating the disease — not by forcing insulin out regardless of blood sugar, but by rebuilding the body’s natural, glucose-sensing amplifier.
A Brief History: From a Clamp Experiment to a Drug Class
The intellectual foundation of the entire GLP-1 field was laid decades before any drug existed. In the 1960s, researchers first noticed that oral glucose produced more insulin than intravenous glucose, and coined the term “incretin” for the unknown gut factor responsible. In the mid-1980s, careful glucose-clamp experiments — matching blood-sugar profiles between oral and intravenous glucose so the only difference was the route — quantified the incretin effect precisely and confirmed that gut hormones, not glucose alone, were driving the extra insulin.[1]
The identification of GLP-1 itself came from cloning the proglucagon gene and realizing it encoded more than just glucagon. When scientists synthesized the GLP-1 fragment and infused it into people, they saw exactly what the incretin theory predicted: insulin rose, glucagon fell, and blood sugar dropped. But those early human infusion studies also revealed the frustrating catch — the effect vanished the moment the infusion stopped, because the peptide was degraded within minutes. That observation, more than any other, defined the engineering problem that the next twenty years of pharmaceutical chemistry would spend solving. Every drug in the modern class is, in one way or another, an answer to a single question first posed in those infusion studies: how do you make a two-minute hormone last?
How Does GLP-1 Work in the Body?
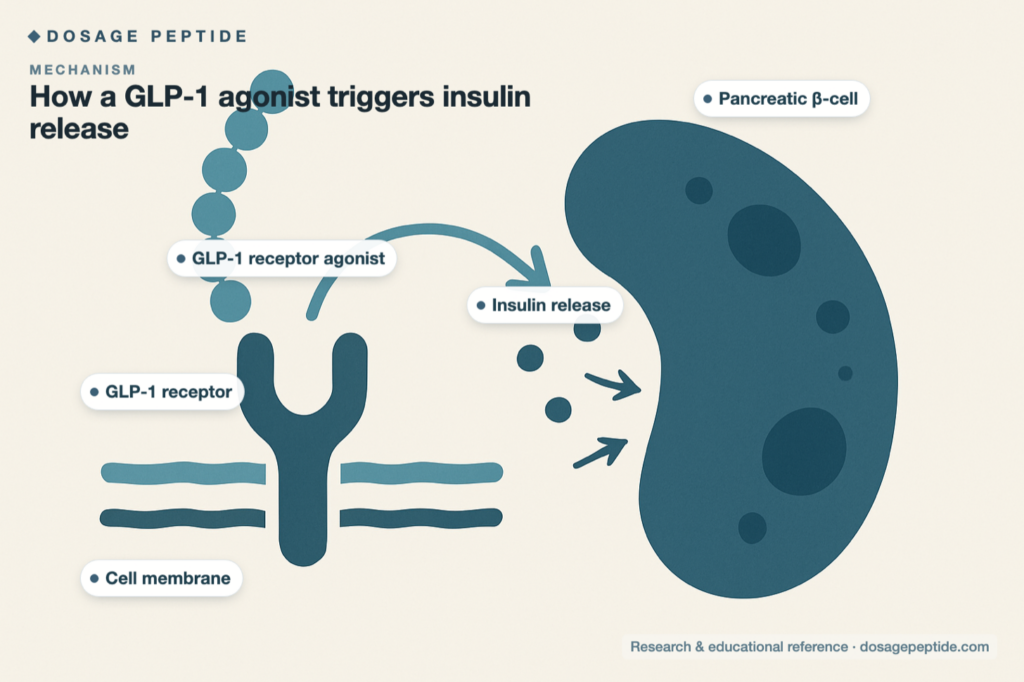
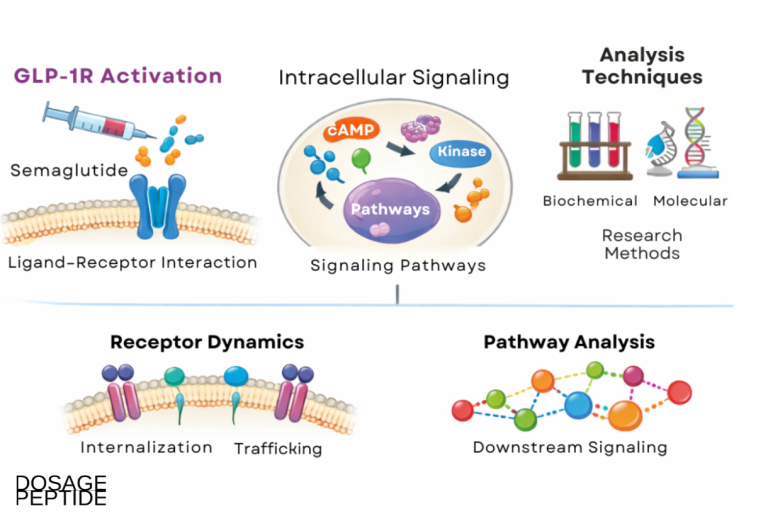
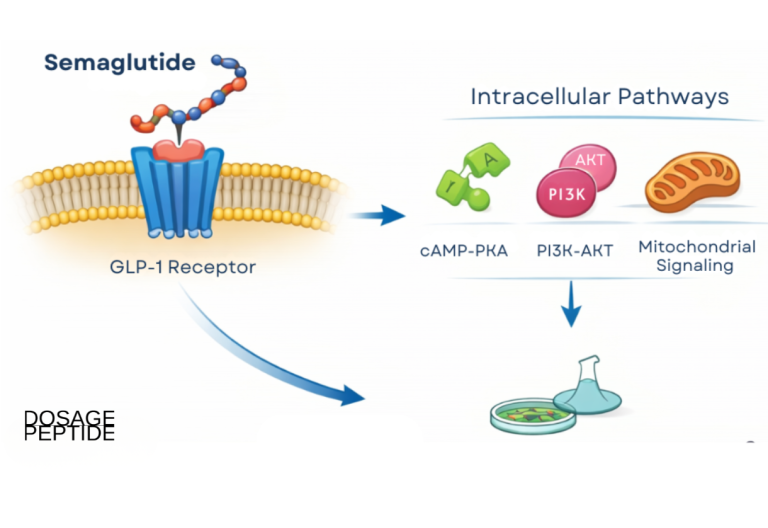
GLP-1 exerts its effects by binding to the GLP-1 receptor (GLP-1R), a class B G-protein-coupled receptor. When GLP-1 docks onto this receptor, it activates the enzyme adenylate cyclase, raising intracellular cyclic AMP and setting off a signaling cascade that changes how the target cell behaves. What makes GLP-1 so versatile is that GLP-1 receptors are not confined to one organ — they are expressed on pancreatic islet cells, in multiple regions of the brain, and in the heart, kidney, gastrointestinal tract, and blood vessels.[2]
This wide receptor distribution is why GLP-1 — and the drugs that mimic it — produces effects far beyond blood sugar. Below are the four core actions of the hormone, followed by its systemic reach.
Glucose-Dependent Insulin Secretion
The signature action of GLP-1 is to stimulate pancreatic beta-cells to release insulin — but only when blood glucose is elevated. This glucose dependence is a built-in safety feature. When blood sugar is normal or low, GLP-1’s push on insulin secretion largely switches off, which is why the hormone (and its drug mimics used alone) carries a low intrinsic risk of hypoglycemia compared with older insulin-secreting drugs like sulfonylureas.
Glucagon Suppression
Simultaneously, GLP-1 suppresses the release of glucagon from pancreatic alpha-cells. Because glucagon drives the liver to pump glucose into the blood, damping it prevents unnecessary hepatic glucose output. This suppression is also glucose-dependent, so the body can still mount a glucagon response if blood sugar drops dangerously low — another protective design feature.
Delayed Gastric Emptying
GLP-1 slows the rate at which the stomach empties its contents into the small intestine.[3] This flattens the post-meal glucose spike because nutrients are delivered to the gut more gradually. It also contributes to fullness — food lingers in the stomach longer, so you feel satisfied for more time after eating. This gastric effect is strongest with short-acting agents and tends to attenuate somewhat with long-acting, continuously dosed drugs.
Appetite Suppression and Satiety
Perhaps the most consequential action for modern weight management is GLP-1’s effect on the brain. Through GLP-1 receptors in appetite-regulating centers of the hypothalamus and brainstem, the hormone reduces hunger and enhances the feeling of fullness.[2] This central action — combined with the peripheral slowing of the gut — is what drives the substantial, sustained reductions in food intake seen with GLP-1-based medicines. Long-acting agonists reach the brain through both direct and indirect routes: some cross into brain regions with a permeable blood-brain barrier, and others signal via the vagus nerve, which relays gut-to-brain information about fullness.
Beyond the Four Core Actions: Cardiometabolic Signaling
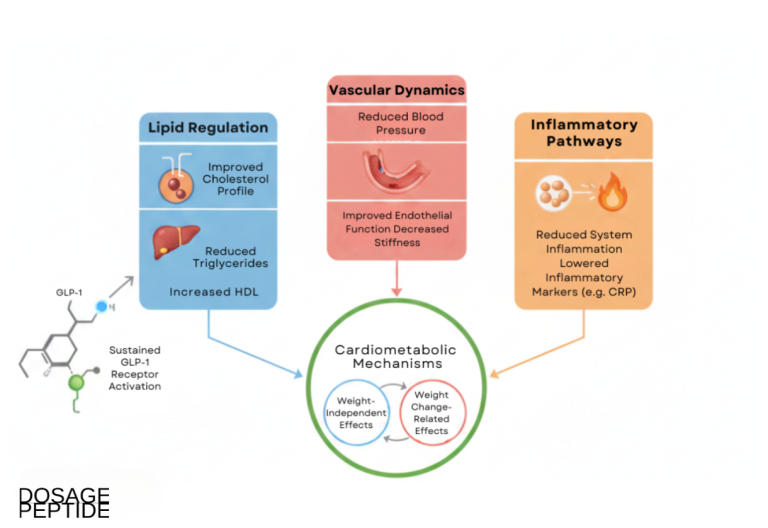
Because GLP-1 receptors sit on cells in the heart, blood vessels, and kidneys, the hormone influences the cardiovascular system in ways that go beyond glucose and weight. GLP-1 signaling is associated with modest reductions in blood pressure, improvements in the lipid profile, reduced vascular inflammation, and favorable effects on endothelial function — the health of the inner lining of blood vessels. Some of these benefits appear to be a direct consequence of receptor activation in cardiovascular tissue, while others follow indirectly from weight loss and improved insulin sensitivity. Untangling the direct from the indirect is an active research question, but the net clinical effect — demonstrated in large outcome trials discussed later — is a measurable reduction in cardiovascular events for several agents in the class.
| Action of GLP-1 | Where it happens | Metabolic result |
|---|---|---|
| Stimulates insulin (glucose-dependent) | Pancreatic beta-cells | Lowers blood glucose safely |
| Suppresses glucagon | Pancreatic alpha-cells | Reduces hepatic glucose output |
| Slows gastric emptying | Stomach and gut | Blunts post-meal glucose spikes; prolongs fullness |
| Reduces appetite | Hypothalamus and brainstem | Lowers food intake; supports weight loss |
| Cardiometabolic signaling | Heart, blood vessels, kidney | Blood pressure, lipid, and inflammatory improvements |
Why Native GLP-1 Barely Lasts Two Minutes
Here lies the central problem that shaped an entire drug class. Native, endogenous GLP-1 is destroyed almost immediately after it is secreted. The enzyme responsible is dipeptidyl peptidase-4 (DPP-4), which clips two amino acids off the N-terminus of the GLP-1 molecule and instantly inactivates it. Because DPP-4 is abundant in the blood and on the surface of endothelial cells, the biological half-life of active GLP-1 is only about one to two minutes.[2]
That fleeting half-life is fine for a natural meal signal, but it makes native GLP-1 useless as a medicine. You cannot inject a hormone that disappears in minutes and expect steady, all-day metabolic control. Solving this degradation problem — either by protecting the peptide from DPP-4 or by blocking DPP-4 itself — is the story of how the modern class was born.
Why Were GLP-1 Receptor Agonists Engineered?
Once researchers understood that GLP-1 could lower blood sugar without causing hypoglycemia, the therapeutic appeal was obvious. The challenge was purely pharmacological: how do you keep GLP-1 signaling active for hours or days when the natural hormone vanishes in minutes? Two distinct strategies emerged.
Strategy One: Block the Enzyme (DPP-4 Inhibitors)
The first approach was indirect — instead of replacing GLP-1, block the enzyme that destroys it. DPP-4 inhibitors (the “gliptins” such as sitagliptin and linagliptin) are oral drugs that prolong the life of a person’s own naturally secreted GLP-1 and GIP. Because they only raise incretin levels into the physiological range, they lower blood sugar modestly, are weight-neutral, and cause few gastrointestinal side effects. They are convenient oral agents but far less powerful than the drugs that came next.
Strategy Two: Build a DPP-4-Resistant Mimic (GLP-1 Receptor Agonists)
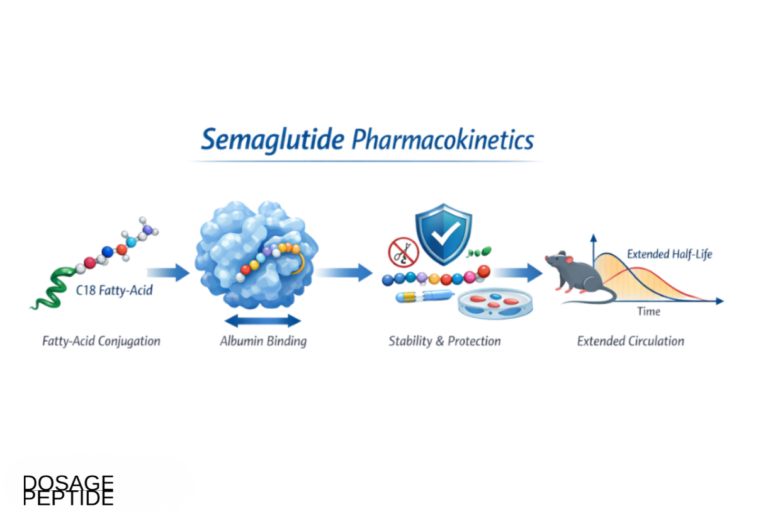
The more transformative approach was to engineer a molecule that activates the GLP-1 receptor but resists DPP-4 degradation. These are the GLP-1 receptor agonists (GLP-1 RAs), also called incretin mimetics or GLP-1 analogs. By modifying the peptide’s structure — changing key amino acids, or attaching a fatty-acid chain that binds to albumin and shields the molecule — scientists extended the half-life from minutes to hours or even a full week. Because these drugs reach receptor exposures far above what a meal would ever produce, they deliver much larger effects on appetite and body weight than the body’s own GLP-1 ever could.
The very first GLP-1 RA drew on an unexpected source. Exenatide, approved in 2005, is a synthetic version of exendin-4, a peptide found in the saliva of the Gila monster, a venomous lizard. Exendin-4 happens to be naturally resistant to DPP-4 and activates the human GLP-1 receptor, making it the perfect starting scaffold. From that proof of concept, the field advanced rapidly toward the long-acting, high-potency agents used today.
The Chemistry of Making a Two-Minute Hormone Last a Week
How exactly do you extend a peptide’s half-life from two minutes to seven days? Drug designers have used a handful of complementary tricks, and understanding them clarifies why the agents behave so differently:
- Amino-acid substitution. The simplest fix is to change the amino acid at the site where DPP-4 cuts. Liraglutide and semaglutide, for instance, carry a substitution that blocks the enzyme’s access, so the molecule survives far longer in circulation.
- Fatty-acid acylation. Attaching a fatty-acid chain to the peptide lets it bind reversibly to albumin, the most abundant protein in blood. Albumin acts as a slow-release reservoir: the drug stays tucked away, protected from enzymes and from kidney filtration, and is released gradually. This is the technology behind liraglutide (roughly once-daily) and, with a longer linker and stronger albumin binding, semaglutide (once-weekly).
- Large-protein fusion. Dulaglutide fuses two GLP-1 analog peptides to a fragment of an antibody. The resulting molecule is large enough to escape rapid kidney clearance, giving it a once-weekly profile.
- Non-peptide small molecules. The most radical departure abandons the peptide entirely. Orforglipron is a small organic molecule that activates the GLP-1 receptor but is chemically nothing like GLP-1, so digestive enzymes do not recognize or destroy it — which is precisely why it can be swallowed as a simple daily pill.
These design choices also explain a key clinical distinction between short-acting and long-acting agents. Short-acting agonists like exenatide (twice-daily) and lixisenatide produce sharp, intermittent peaks in drug level; their dominant effect is slowing gastric emptying, which controls the after-meal glucose spike but causes more pronounced, peak-related nausea. Long-acting agonists like semaglutide and dulaglutide maintain steady drug levels around the clock; they act more on fasting glucose, appetite, and body weight, and because the stomach adapts to continuous exposure, their gastric-slowing effect tends to wane over time while their appetite effect persists. This is why the most powerful weight-loss agents are all long-acting.
What Is the Full Modern Class of GLP-1 Medications?
The GLP-1 landscape has grown from a single lizard-derived injectable into a diverse class spanning three levels of hormonal targeting and two routes of administration. Understanding the class means understanding two axes: how many receptors a drug hits (single, dual, or triple agonism) and how it is taken (injectable peptide versus oral peptide versus oral small molecule).
Single-Target GLP-1 Receptor Agonists
These drugs activate only the GLP-1 receptor. They were the foundation of the class and remain widely used.
- Semaglutide (Ozempic and Rybelsus for type 2 diabetes; Wegovy for obesity) is the most prominent single-target agonist. It is available as a once-weekly injection and, in a special formulation, as a daily oral tablet. It produces the strongest weight loss of any pure GLP-1 RA. For a detailed dosing walkthrough, see the semaglutide 5mg vial dosage protocol.
- Liraglutide (Victoza for diabetes; Saxenda for weight management) was the first once-daily long-acting GLP-1 RA, using a fatty-acid tail to bind albumin and extend its half-life to about 13 hours.
- Dulaglutide (Trulicity) is a once-weekly injection built on an antibody-fragment backbone; it can be used down to an eGFR of 15 mL/min and has demonstrated cardiovascular benefit.
- Exenatide (Byetta twice-daily; Bydureon once-weekly) was the original GLP-1 RA, derived from the Gila monster peptide exendin-4.
- Lixisenatide (Adlyxin) is a short-acting once-daily agent whose main effect is delaying gastric emptying for post-meal glucose control.
Dual Agonists (GIP + GLP-1)
The next leap combined two incretins in a single molecule. Tirzepatide (Mounjaro for diabetes; Zepbound for obesity) activates both the GIP receptor and the GLP-1 receptor. By recruiting GIP alongside GLP-1, it produces greater weight loss and glucose lowering than single-target agonists in head-to-head and cross-trial comparisons. It is given as a once-weekly injection. You can read a focused explainer on how tirzepatide works, and a dosing walkthrough in the tirzepatide 5mg vial dosage protocol.
Triple Agonists (GIP + GLP-1 + Glucagon)
Retatrutide is a first-in-class single molecule that activates three receptors at once: GIP, GLP-1, and glucagon.[4] The addition of glucagon-receptor agonism is counterintuitive — glucagon raises blood sugar — but at controlled levels it increases energy expenditure and promotes fat breakdown, which appears to amplify weight loss when balanced against the glucose-lowering incretin arms. In its pivotal Phase 3 obesity program, retatrutide delivered some of the largest weight reductions yet reported for a pharmacological agent, and additional Phase 3 trials in obesity, type 2 diabetes, sleep apnea, and other conditions are reading out through 2026.[5] Retatrutide remains investigational and is not FDA-approved.
Oral Small-Molecule GLP-1 Agonists
The newest frontier moves away from peptides entirely. Orforglipron is a once-daily, non-peptide small-molecule GLP-1 receptor agonist — meaning it can survive the digestive tract and be taken as a simple pill without the strict fasting and water restrictions that oral semaglutide requires. In 2026 the FDA approved orforglipron under the brand name Foundayo for chronic weight management in adults with obesity or overweight with weight-related conditions, making it the first small-molecule oral GLP-1 pill cleared for weight loss that can be taken any time of day without food or water restrictions.[6] In head-to-head type 2 diabetes trials, orforglipron delivered superior A1C control and weight loss compared with oral semaglutide.[7] A type 2 diabetes indication is under regulatory review. For dosing detail, see the orforglipron 6mg dosage protocol.
How Does the GLP-1 Class Compare? (Comparison Table)
The table below summarizes the major agents by mechanism, route, typical efficacy, and regulatory status. Efficacy figures are drawn from pivotal trials and are approximate; individual results vary widely and depend on dose, duration, and adherence.
| Agent | Target(s) | Route & frequency | Typical weight effect | Status |
|---|---|---|---|---|
| Exenatide | GLP-1 | SC, twice daily or weekly | Modest | Approved (T2D) |
| Lixisenatide | GLP-1 | SC, once daily | Modest | Approved (T2D) |
| Liraglutide | GLP-1 | SC, once daily | ~5–8% | Approved (T2D & obesity) |
| Dulaglutide | GLP-1 | SC, once weekly | Modest | Approved (T2D) |
| Semaglutide (injectable) | GLP-1 | SC, once weekly | ~15% | Approved (T2D & obesity) |
| Semaglutide (oral) | GLP-1 | Oral, once daily | Moderate–high | Approved |
| Tirzepatide | GIP + GLP-1 | SC, once weekly | ~20%+ | Approved (T2D & obesity) |
| Orforglipron (Foundayo) | GLP-1 (small molecule) | Oral, once daily | High | Approved (obesity, 2026); T2D under review |
| Retatrutide | GIP + GLP-1 + glucagon | SC, once weekly | Very high (investigational) | Investigational (Phase 3) |
How Do GLP-1 Drugs Compare to Other Metabolic Therapies?
GLP-1 receptor agonists do not exist in a vacuum. They sit alongside several other classes of glucose-lowering and weight-management therapies, each with a distinct mechanism. Understanding where GLP-1 fits clarifies both its strengths and the situations where other tools remain relevant.
| Therapy | Mechanism | Route | Weight effect | Notes |
|---|---|---|---|---|
| GLP-1 receptor agonists | Mimic GLP-1: raise insulin, lower glucagon, slow gastric emptying, increase satiety | Injection (daily/weekly) or oral | Substantial (up to ~15%+) | Cardiovascular and kidney benefits; GI side effects |
| Dual/triple agonists | Add GIP and/or glucagon receptor activity | Weekly injection (oral emerging) | Greatest of the class | Tirzepatide approved; retatrutide investigational |
| DPP-4 inhibitors | Block DPP-4 to prolong the body’s own GLP-1 and GIP | Oral daily | Neutral | Mild, weight-neutral, few GI effects; modest potency |
| SGLT2 inhibitors | Block glucose reabsorption in the kidney (sugar excreted in urine) | Oral daily | Modest loss | Strong heart-failure and kidney benefits; UTI/DKA risk |
| Metformin | Reduce liver glucose output, improve insulin sensitivity | Oral daily | Neutral to modest | Inexpensive first-line for type 2 diabetes |
| Bariatric surgery | Anatomical change plus large shifts in gut hormones (including GLP-1) | Surgical | Largest and most durable | Most effective but invasive, with surgical risk |
A revealing detail: bariatric surgery works in part through GLP-1. Rerouting the gut dramatically increases the body’s own GLP-1 secretion after meals, which helps explain why surgery so powerfully reduces appetite and improves diabetes. In a sense, GLP-1 medications pursue pharmacologically what surgery achieves anatomically — a much larger GLP-1 signal. DPP-4 inhibitors and GLP-1 RAs represent two ends of the same idea: the former gently raises the body’s natural incretin levels, while the latter floods the receptor with a stable, long-acting mimic for a far larger effect. These classes are also frequently combined with metformin or SGLT2 inhibitors, since their mechanisms are complementary rather than redundant.
What Does the Evidence Show for GLP-1 Medications?
The GLP-1 class is one of the most extensively studied in modern endocrinology, backed by large randomized controlled trials with tens of thousands of participants. The evidence spans three domains: glucose control, weight loss, and cardiovascular and organ protection.
Glucose Control in Type 2 Diabetes
GLP-1 RAs were first developed for type 2 diabetes, and they reliably lower HbA1c — a marker of average blood sugar over roughly three months — while promoting weight loss rather than the weight gain seen with insulin and sulfonylureas. Once-weekly agents such as semaglutide and dulaglutide generally lower HbA1c more effectively than older twice-daily formulations, and they do so with low intrinsic hypoglycemia risk because their insulin-stimulating effect is glucose-dependent.
This combination of properties is what shifted the GLP-1 class from a niche add-on to a preferred option in modern diabetes guidelines. For decades, the trade-off in diabetes care was blunt: the drugs that lowered blood sugar most aggressively also caused weight gain and hypoglycemia. GLP-1 RAs broke that trade-off by lowering glucose, reducing weight, and carrying low hypoglycemia risk at the same time — and then, in outcome trials, by reducing cardiovascular events on top of it all. For a person with type 2 diabetes who also has obesity and cardiovascular risk — a very common combination — a single medication now addresses several problems at once. The newer dual and triple agonists extend this further, generally producing larger HbA1c reductions than single-target agents at comparable tolerability.
Weight Loss
The weight-loss evidence transformed obesity medicine. In the pivotal STEP 1 trial, once-weekly semaglutide 2.4 mg plus lifestyle intervention produced a mean body-weight reduction of 14.9% over 68 weeks, versus 2.4% with placebo, and 86% of participants achieved at least 5% weight loss.[8] The dual agonist tirzepatide pushed the ceiling higher: in SURMOUNT-1, the 10 mg and 15 mg doses produced average weight reductions of 19.5% and 20.9%, respectively, over 72 weeks.[9] The investigational triple agonist retatrutide has reported even larger reductions in Phase 3 obesity trials.[4] These magnitudes approach territory previously achievable only with bariatric surgery. What makes these figures credible is that they come from large, randomized, placebo-controlled trials with hundreds to thousands of participants each, followed for well over a year, and replicated across multiple studies within the same drug’s development program rather than resting on a single result.
Cardiovascular and Organ Protection
Beyond sugar and weight, several GLP-1 RAs have demonstrated cardiovascular benefit in dedicated outcome trials. In the landmark SELECT trial, once-weekly semaglutide reduced the risk of major adverse cardiovascular events — cardiovascular death, non-fatal heart attack, or non-fatal stroke — by 20% in more than 17,000 people with overweight or obesity and established cardiovascular disease but without diabetes (hazard ratio 0.80; 95% CI 0.72–0.90; p<0.001).[10] This was a pivotal finding because it showed benefit independent of diabetes. Earlier trials such as LEADER (liraglutide) and prior semaglutide outcome studies established the pattern of cardiovascular risk reduction across the class. Additional signals point to benefits in kidney function, fatty liver disease, and blood pressure, largely mediated by weight loss and improved insulin sensitivity.
What Are the Side Effects and Safety Considerations?
No drug is without risk, and GLP-1 medications are no exception. The good news is that the safety profile is well characterized after years of large-scale use, and the great majority of adverse effects are gastrointestinal, dose-dependent, and manageable with careful titration.
Gastrointestinal Effects: The Dominant Story
The most common side effects are nausea, vomiting, diarrhea, and constipation, driven largely by the slowing of gastric emptying and central actions on the brain. Nausea in particular can affect a substantial fraction of users, especially early in treatment.[8] These symptoms are usually mild to moderate, transient, and diminish as the body adapts. The universal clinical principle is “start low, go slow”: beginning at a low dose and escalating gradually over weeks dramatically reduces the intensity of GI symptoms. Reconstituting and dosing accurately matters here — the peptide reconstitution guide and the dosage calculator exist to support precise, gradual titration in a research context.
Appetite Suppression as a Double-Edged Effect
Decreased appetite is the intended mechanism for weight loss, but it must be monitored. If food intake drops too far, users can develop inadequate protein and micronutrient intake, and rapid weight loss can include loss of lean muscle mass alongside fat. Adequate protein and resistance exercise are commonly recommended to preserve muscle during treatment.
Rare but Serious Considerations
- Pancreatitis: Isolated case reports and early animal data raised concern, but large meta-analyses of randomized trials have not found a statistically significant increase in pancreatitis incidence. The association remains unproven; clinicians monitor for symptoms but the event is rare.
- Medullary thyroid carcinoma (MTC): Rodent studies showed a thyroid C-cell tumor signal that has not been confirmed in humans. Nonetheless, GLP-1 RAs carry a labeled contraindication in people with a personal or family history of MTC or multiple endocrine neoplasia type 2 (MEN 2).
- Gallbladder disease: Rapid weight loss of any cause raises the risk of gallstones, and this has been observed with GLP-1 therapy.
- Hypoglycemia: Low on its own because insulin release is glucose-dependent, but the risk rises when GLP-1 RAs are combined with insulin or sulfonylureas, so those companion doses often need to be reduced.
Who Should Not Use GLP-1 Receptor Agonists
GLP-1 RAs are not approved for type 1 diabetes, where the problem is absolute insulin deficiency rather than the insulin resistance and incretin dysfunction of type 2 diabetes. They are contraindicated in people with a history of MTC or MEN 2, should be used cautiously in severe gastrointestinal disease such as gastroparesis, and are generally avoided in pregnancy. People with chronic kidney disease may need to select an agent with established safety at low eGFR. These are prescription medicines that require individualized medical supervision.
Injectable Versus Oral: Which Route Is Right?
For most of the class’s history, GLP-1 drugs had to be injected because peptides are digested and destroyed in the stomach. That constraint is now loosening, and the route of administration has become a meaningful point of differentiation.
Injectable Peptides
The majority of GLP-1 RAs — semaglutide (injectable), tirzepatide, dulaglutide, liraglutide, exenatide, and investigational retatrutide — are subcutaneous injections. Weekly agents offer excellent convenience: a single small injection with a fine needle, often via a pre-filled pen, once every seven days. Injectable peptides also tend to achieve the highest and most consistent drug exposures, which is part of why the most powerful agents in the class are injectables.
Oral Peptides
Oral semaglutide (Rybelsus) was a landmark: it packages the same peptide with an absorption enhancer so a fraction survives the stomach. The trade-off is strict administration rules — it must be taken on an empty stomach with a small sip of water and a waiting period before eating — and only a small percentage of the dose is actually absorbed, so tablet strengths are high.
Oral Small Molecules
Orforglipron (Foundayo) represents the cleanest solution to the oral problem. Because it is a non-peptide small molecule rather than a fragile peptide, it is not destroyed by digestion and does not require fasting or water restrictions; it can be taken any time of day.[6] Small-molecule oral agonists are easier and cheaper to manufacture at scale than peptides, which could improve access as the class expands. This route may prove especially important for reaching the large global population that prefers pills over injections.
What Happens With Muscle, Maintenance, and Stopping Treatment?
Three practical realities of GLP-1 therapy get less attention than the headline weight-loss numbers but matter enormously for anyone thinking seriously about the class: what happens to muscle, what happens over the long term, and what happens when treatment stops.
Fat Loss Versus Lean Mass Loss
Any substantial, rapid weight loss — whether from dieting, surgery, or medication — includes some loss of lean body mass alongside fat. This is not unique to GLP-1 drugs, but the sheer magnitude of weight loss they produce makes the issue salient. In the SURMOUNT-1 tirzepatide trial, participants lost proportionally far more fat than lean tissue, with a roughly three-fold greater reduction in fat mass than in lean mass.[9] Still, preserving muscle during treatment is a genuine concern, particularly for older adults in whom muscle loss can affect strength and function. The practical countermeasures are consistent across the literature: adequate protein intake and regular resistance exercise, which together shift the composition of weight loss toward fat and help maintain metabolically active muscle.
A Chronic Condition, Not a Course of Treatment
Obesity and type 2 diabetes are chronic, relapsing conditions, and GLP-1 medications treat them the way blood-pressure drugs treat hypertension — by managing the underlying physiology for as long as the drug is taken. The appetite-regulating effects persist while drug levels are maintained; they do not permanently reset the body’s set point. This reframes the question from “how long until I’m done?” to “what is the long-term plan?” Extension trials show that weight loss is sustained as long as treatment continues, and that plateaus eventually occur as the body reaches a new equilibrium.
What Happens When You Stop
The evidence on discontinuation is sobering and important. When GLP-1 therapy is stopped, appetite tends to return and a substantial portion of lost weight is commonly regained over the following year, along with a partial reversal of the associated cardiometabolic improvements. This is not a failure of the drug or the patient — it is the expected behavior of a treatment for a chronic condition being withdrawn. It underscores why lifestyle foundations laid during treatment matter so much, and why decisions about tapering, maintenance dosing, or long-term continuation should be made deliberately with a clinician rather than abruptly.
What Is the Broader Research Landscape for GLP-1?
GLP-1 biology has become one of the most active areas in metabolic medicine, and the pipeline extends well beyond diabetes and weight loss. Because GLP-1 receptors are distributed across so many organs, researchers are probing effects in domains that would have seemed unrelated a decade ago.
- Metabolic liver disease: GLP-1 and multi-agonist molecules are being studied for metabolic dysfunction-associated steatotic liver disease (MASLD, formerly NAFLD) and its inflammatory form MASH, where weight loss and improved insulin sensitivity may reverse liver fat and fibrosis.
- Cardiovascular and kidney outcomes: Building on SELECT, dedicated trials continue to test whether these agents prevent heart failure, kidney decline, and death across diverse populations.
- Sleep apnea and osteoarthritis: Weight loss from potent agents has produced meaningful improvements in obstructive sleep apnea and in knee osteoarthritis pain, expanding the potential indications.
- Neuroprotection and addiction: Epidemiological and preclinical signals suggest possible benefit in neurodegenerative disease and in reducing addictive behaviors, reflecting GLP-1 receptor activity in the brain’s reward circuitry. This research is early and not yet a basis for clinical use.
The trajectory is toward more targeted and more powerful molecules: dual and triple agonists that fine-tune the balance of incretin and glucagon signaling, oral small molecules that broaden access, and combination approaches that pair GLP-1 activity with other hormonal pathways such as amylin. For readers building a working vocabulary of these mechanisms, the peptide glossary defines the incretin, receptor, and pharmacokinetic terms used throughout this class.
How Should Enthusiasts Think About GLP-1 Responsibly?
For peptide and health enthusiasts, GLP-1 is a fascinating case study in translating physiology into therapy — but enthusiasm should be grounded in a few sober principles.
First, the biology is real and the drugs are genuinely powerful, but they are not magic. Every pivotal trial paired the medication with diet and lifestyle intervention, and the benefits of GLP-1 therapy are best sustained alongside nutrition, resistance training, sleep, and behavioral change — not as a substitute for them. Weight regain is common when treatment stops, which underscores that these agents treat a chronic condition rather than curing it.
Second, regulatory status and product quality matter enormously. Semaglutide, tirzepatide, liraglutide, dulaglutide, exenatide, and now oral orforglipron are FDA-approved medicines with defined manufacturing standards and indications; retatrutide remains investigational. The surge in demand has produced a parallel market of unregulated and compounded products of variable purity and accuracy. Any use of these compounds should occur under qualified medical supervision with pharmaceutical-grade material.
Third, individual response varies. Weight loss and glucose response differ widely from person to person based on dose, adherence, genetics, and lifestyle. The trial averages cited here are population figures, not personal guarantees. Some people are strong responders who lose well above the average; others plateau early or tolerate the medication poorly. A careful, gradual, monitored approach — understanding the biology, clarifying goals, checking contraindications, titrating slowly, and reassessing over 6 to 12 months — is the framework that respects both the promise and the limits of this remarkable hormone.
Finally, it is worth keeping the big picture in view. GLP-1 began as a curiosity in a physiology lab — a hormone that lasted two minutes and seemed to do a little of everything. Within a generation it has become a therapeutic platform reshaping how medicine approaches diabetes, obesity, and increasingly cardiovascular and metabolic disease as a whole. For the informed enthusiast, the lesson is not that any single drug is a solution, but that understanding the underlying biology — the incretin effect, receptor signaling, DPP-4 degradation, and the engineering that overcame it — is the surest foundation for evaluating each new agent as the class continues to evolve. The tools on this site, from the dosage calculator to the glossary, exist to support exactly that kind of careful, evidence-first understanding.
Frequently Asked Questions
What is GLP-1 in simple terms?
GLP-1 (glucagon-like peptide-1) is a hormone your gut releases after you eat. It tells your pancreas to release insulin when blood sugar is high, tells the liver to stop dumping sugar, slows your stomach, and signals your brain that you are full. In short, it is your body’s natural “meal messenger” for balancing blood sugar and appetite.
How do GLP-1 medications cause weight loss?
GLP-1 receptor agonists reduce appetite through the brain’s satiety centers and slow how fast the stomach empties, so you feel full sooner and stay full longer. Together these effects lower total calorie intake. Improved insulin sensitivity and suppressed glucagon also help. In trials, semaglutide averaged about 15% weight loss and tirzepatide over 20%.
What is the difference between GLP-1 and GIP?
Both are incretin hormones that boost insulin release after eating. GLP-1 comes from L-cells in the lower gut and also suppresses glucagon and appetite. GIP comes from K-cells in the upper gut and mainly stimulates insulin and supports beta-cells. In type 2 diabetes, GIP’s insulin effect is blunted while GLP-1 still works, which is why GLP-1 became the first drug target.
Why does native GLP-1 have to be turned into a drug?
Natural GLP-1 is destroyed within one to two minutes by an enzyme called DPP-4, so it cannot work as a medicine on its own. Scientists engineered GLP-1 receptor agonists that resist DPP-4 — by altering the peptide or attaching a fatty-acid chain — extending the half-life from minutes to hours or a full week, and delivering far larger effects than the body’s own hormone.
What is the difference between single, dual, and triple agonists?
Single agonists like semaglutide hit only the GLP-1 receptor. Dual agonists like tirzepatide add GIP-receptor activity for greater effect. Triple agonists like investigational retatrutide add glucagon-receptor activity on top, which boosts energy expenditure and appears to produce even larger weight loss. More targets generally mean stronger metabolic effects.
Is orforglipron (Foundayo) FDA-approved?
Yes. Orforglipron, an oral non-peptide GLP-1 receptor agonist, was FDA-approved in 2026 under the brand name Foundayo for chronic weight management in adults with obesity or overweight with weight-related conditions. It can be taken any time of day without food or water restrictions. A separate type 2 diabetes indication is under regulatory review.
Do GLP-1 medications cause pancreatitis?
The link is unproven. Some case reports and animal studies raised concern, but large meta-analyses of randomized trials have not found a significant increase in pancreatitis risk. Clinicians monitor for symptoms because the event, while rare, is serious, but current evidence does not establish a causal relationship.
Can lifestyle changes replace GLP-1 medications?
For many people, diet, exercise, and behavior change alone produce meaningful improvement, and lifestyle remains the foundation of metabolic health. For those who cannot reach their goals that way, GLP-1 therapy is an additional tool that works best combined with lifestyle changes — not as a replacement for them. Benefits often fade if the medication is stopped without maintaining those habits.
References
- Nauck MA, Meier JJ. The evolving story of incretins (GIP and GLP-1) in metabolic and cardiovascular disease: a pathophysiological update. Diabetes, Obesity and Metabolism. 2021. https://dom-pubs.onlinelibrary.wiley.com/doi/full/10.1111/dom.14496
- Müller TD, et al. GLP-1 physiology in obesity and development of incretin-based drugs for chronic weight management. Nature Metabolism. 2024. https://www.nature.com/articles/s42255-024-01113-9
- Physiology and Pharmacology of Effects of GLP-1-based Therapies on Gastric, Biliary and Intestinal Motility. Endocrinology. 2025. https://academic.oup.com/endo/article/166/1/bqae155/7906037
- Eli Lilly and Company. Lilly’s triple agonist, retatrutide, delivered powerful weight loss in pivotal Phase 3 obesity trial. 2026. https://investor.lilly.com/news-releases/news-release-details/lillys-triple-agonist-retatrutide-delivered-powerful-weight-loss
- Eli Lilly and Company. Lilly’s triple agonist, retatrutide, delivered weight loss of up to an average of 71.2 lbs in first successful Phase 3 trial. 2026. https://investor.lilly.com/news-releases/news-release-details/lillys-triple-agonist-retatrutide-delivered-weight-loss-average
- Eli Lilly and Company. FDA approves Lilly’s Foundayo (orforglipron), the only GLP-1 pill for weight loss that can be taken any time of day without food or water restrictions. 2026. https://investor.lilly.com/news-releases/news-release-details/fda-approves-lillys-foundayotm-orforglipron-only-glp-1-pill
- Eli Lilly and Company. Lilly’s oral GLP-1 Foundayo (orforglipron) delivered superior A1C control and weight loss in three pivotal type 2 diabetes trials. 2026. https://www.prnewswire.com/news-releases/lillys-oral-glp-1-foundayo-orforglipron-delivered-superior-a1c-control-and-weight-loss-in-three-pivotal-type-2-diabetes-trials-302793407.html
- Wilding JPH, et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity (STEP 1). New England Journal of Medicine. 2021. https://www.nejm.org/doi/full/10.1056/NEJMoa2032183
- Jastreboff AM, et al. Tirzepatide Once Weekly for the Treatment of Obesity (SURMOUNT-1). New England Journal of Medicine. 2022. https://www.nejm.org/doi/full/10.1056/NEJMoa2206038
- Lincoff AM, et al. Semaglutide and Cardiovascular Outcomes in Obesity without Diabetes (SELECT). New England Journal of Medicine. 2023. https://www.nejm.org/doi/full/10.1056/NEJMoa2307563