Retatrutide is the most talked-about molecule in the incretin field because it does something neither semaglutide nor tirzepatide does: it engages three metabolic receptors at once. In its Phase 2 obesity trial it produced the largest average body-weight reductions yet reported for a once-weekly agent — but every gram of that effect was built on a slow, deliberate dose-escalation schedule. Get the titration right and tolerability is manageable; skip the ramp and the gastrointestinal side effects become the whole story.
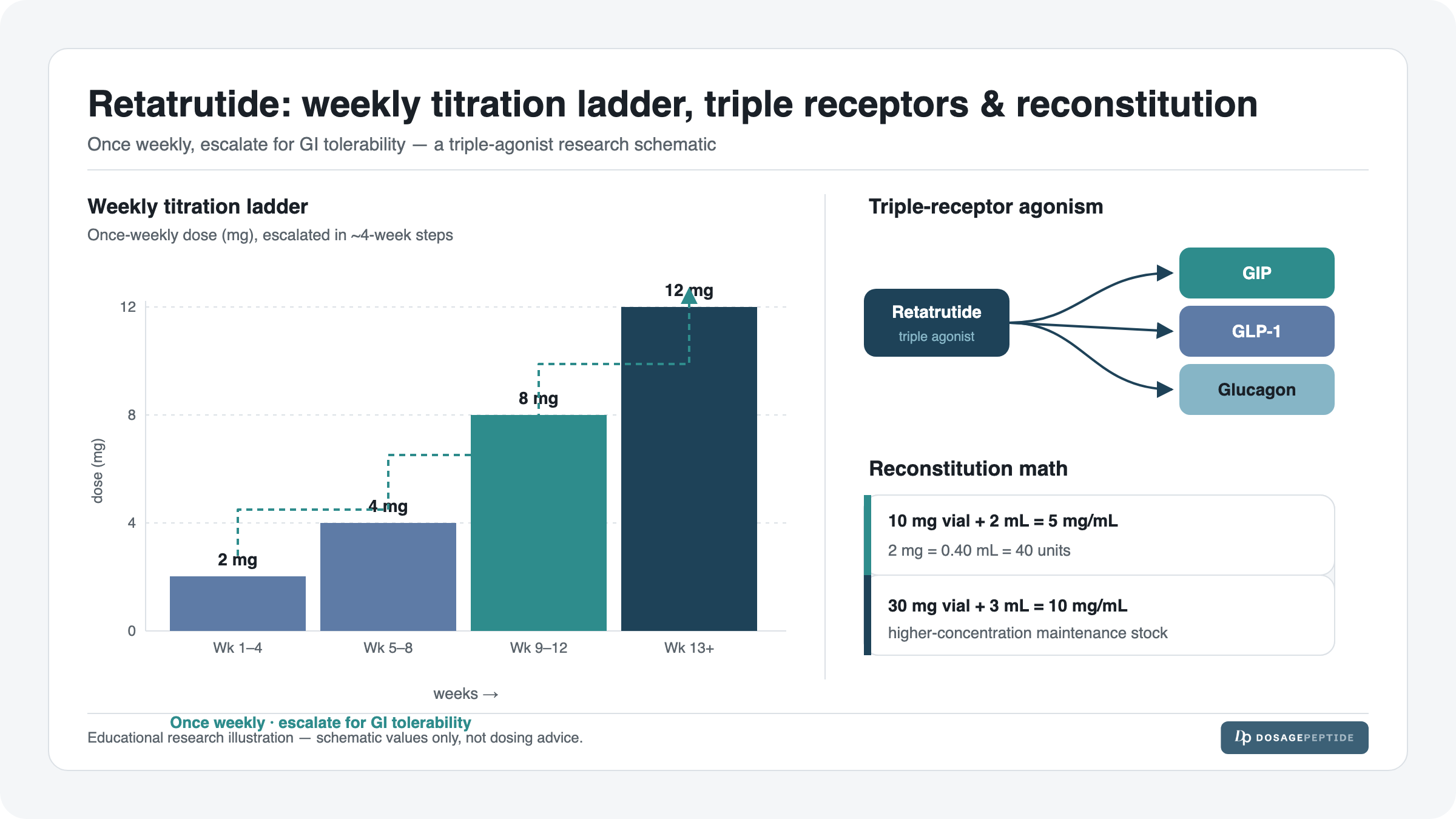
The mechanism is the reason the ladder exists. Retatrutide is a single-molecule triple agonist hitting the GIP, GLP-1, and glucagon receptors. The GLP-1 and GIP arms slow gastric emptying and blunt appetite (that is where nausea comes from), while the glucagon arm nudges energy expenditure and hepatic fat handling. Because each of those pathways ramps up its own physiological load, the documented protocol starts low and climbs in roughly four-week steps so the gut can adapt before the next increment lands.
Read this as reference information, not a prescription. Retatrutide is an investigational drug that is not approved by the FDA or EMA for any use; its Phase 3 TRIUMPH program is still running. Everything below documents the once-weekly research/trial protocol under a strict research-use-only framing, with the reconstitution arithmetic shown so the numbers are auditable. It is not medical advice, and the material is not intended for human consumption.

Retatrutide at a Glance
| Attribute | Detail (documented research protocol) |
|---|---|
| Use (studied) | Chronic weight management and type 2 diabetes (Phase 2 completed; Phase 3 TRIUMPH ongoing) |
| Class / mechanism | Single-molecule triple agonist: GIP + GLP-1 + glucagon receptors (“GGG”) |
| Typical vial strengths | 5, 6, 10, 12, 20, 24, and 30 mg lyophilized |
| Reconstitution (example) | 10 mg vial + 2 mL bacteriostatic water = 5 mg/mL |
| Documented starting dose | 2 mg once weekly (across sizes) |
| Per-dose (2 mg from 5 mg/mL) | 0.40 mL = 40 units on a U-100 syringe |
| Schedule | Once weekly — the same day each week, not daily |
| Titration | Stepwise, roughly every 4 weeks (e.g. 2 → 4 → 8 → 12 mg maintenance targets) |
| Onset / timeline | Appetite suppression within the first weeks; weight change accumulates over months in trials |
| Common side effects | Nausea, diarrhea, vomiting, constipation, decreased appetite (dose-dependent, mostly early) |
| Best studied alongside | Standalone in trials; compared against semaglutide/tirzepatide in the research literature |
| Regulatory status | Investigational — NOT FDA/EMA approved. Prescription-class molecule; research-use-only here |
What Retatrutide Is: Composition & Mechanism
Retatrutide (development code LY3437943, informally “GGG” for its three targets) is not a blend — it is one engineered peptide agonist that binds three different receptors. That single-molecule design is what separates it from stacking three drugs: the pharmacokinetics are unified, and the once-weekly half-life comes from a fatty-acid modification similar to the one used on semaglutide and tirzepatide.
Understanding the three arms clarifies both the benefits and why the titration ladder is non-negotiable:
| Receptor arm | What it drives | Relevance to dosing |
|---|---|---|
| GLP-1 agonism | Appetite suppression, slowed gastric emptying, glucose-dependent insulin release | Primary source of early nausea; the reason for a low start |
| GIP agonism | Additional insulinotropic effect; may modulate nausea and adipose handling | Amplifies satiety; contributes to the strong appetite effect |
| Glucagon agonism | Increased energy expenditure and hepatic fat mobilization | Adds metabolic “burn” but requires careful up-titration to stay tolerable |
The glucagon arm is the novel piece. Glucagon is usually thought of as a glucose-raising hormone, but in the context of simultaneous GLP-1/GIP agonism the net effect studied in trials was increased energy expenditure alongside strong glycemic control — a combination that appears to explain the outsized weight effect observed in the research. For a side-by-side of how this compares to the dual and single agonists, see our breakdown of Retatrutide vs Semaglutide vs Tirzepatide.
One practical consequence of the triple mechanism: because three pathways are being engaged simultaneously, the total physiological load at any given milligram is higher than a single- or dual-agonist at the same number. That is precisely why the documented starting dose is a conservative 2 mg once weekly and why the escalation is unhurried — the ladder is calibrated to the combined receptor load, not to any one arm.
It also helps to understand why the three arms were combined in the first place. Single GLP-1 agonism (the semaglutide model) drives appetite suppression and glucose control but plateaus in how much weight it can shift. Adding GIP (the tirzepatide model) deepens the effect and, somewhat counterintuitively, appears to improve gastrointestinal tolerability relative to GLP-1 alone. The glucagon arm is the third lever: rather than only reducing energy intake through appetite, glucagon agonism raises energy expenditure and pushes the liver to mobilize stored fat. In principle, that means Retatrutide attacks the energy-balance equation from both sides at once — less in, more out — which is the pharmacological rationale for why its trial weight reductions exceeded what the single and dual agonists had achieved.
The trade-off is that glucagon agonism is the arm most likely to nudge metabolic parameters in directions that need watching (heart rate and glycemic dynamics among them), which is another reason the documented protocol climbs slowly and why the class monitoring guidance below is not optional context. The elegance of the single-molecule design is that all three effects rise and fall together on one predictable once-weekly curve, instead of three separate drugs each with its own half-life and interaction profile.
How to Dose Retatrutide (The Documented Research Protocol)
The single most important framing: Retatrutide is dosed once weekly, not daily. The documented starting dose across vial sizes is 2 mg per week, held for the initial adaptation period before the first escalation. The table below presents the trial-documented escalation as reference information under research-use-only framing — it is the schedule studied, not a personal recommendation.
| Titration step | Once-weekly dose | Typical duration | Purpose |
|---|---|---|---|
| Step 1 (start) | 2 mg | ~4 weeks | Introduce the molecule; let the gut adapt |
| Step 2 | 4 mg | ~4 weeks | First escalation once 2 mg is tolerated |
| Step 3 | 8 mg | ~4 weeks | Approaching mid-range maintenance |
| Step 4 (maintenance target) | 12 mg | Ongoing | Common maintenance target in the Phase 2 trial |
In the Phase 2 study the highest arm continued upward toward higher maintenance targets, but the core principle held throughout: escalate only after the current step is tolerated, in roughly four-week increments. The reason is entirely about gastrointestinal tolerability — nausea, diarrhea, and vomiting were clearly dose-dependent and concentrated in the weeks right after each step-up. A slower ramp trades a few extra weeks for a far smoother experience. If side effects are the concern, our dedicated write-up on Retatrutide side effects and safety research goes deeper.
Note that the milligram numbers on this ladder are doses, not vial sizes. A single 30 mg vial, for instance, is a supply that covers many weekly doses — it is not a 30 mg injection. Confusing the two is the most common and most dangerous misreading of any GLP-1-class protocol, so the reconstitution section below shows exactly how each vial size maps to each step of the ladder in millilitres and syringe units.
The search-popular phrase “retatrutide 30 mg” is worth flagging directly here for the same reason. People searching it are usually asking one of two very different questions — “is 30 mg a dose I take?” (no; it is a vial size) or “how do I use a 30 mg vial?” (reconstitute to 10 mg/mL and draw the ladder doses from it, as shown below). Keeping the dose-versus-vial distinction crisp is the single most important literacy point for reading any of these protocols, and it is the difference between a 20-unit starting draw and a dangerous overdose. When in doubt, anchor on the once-weekly dose in milligrams from the titration table, then let the reconstitution math translate that dose into a draw volume for whatever vial you happen to be holding.
Reconstitution & Draw (With the Real Math)
Every vial ships as a lyophilized (freeze-dried) powder and must be reconstituted with bacteriostatic water before drawing. The governing equations are simple, and every dose below is auditable from them:
Concentration: vial mg ÷ BAC water mL = mg/mL
Draw volume: dose mg ÷ concentration (mg/mL) = mL
Syringe units: mL × 100 = units on a U-100 insulin syringe
Worked example 1 — the 10 mg vial (the reference build)
- Concentration: 10 mg ÷ 2 mL = 5 mg/mL
- Starting 2 mg dose: 2 mg ÷ 5 mg/mL = 0.40 mL
- On the syringe: 0.40 mL × 100 = 40 units
So a 2 mg starting dose from a 10 mg / 2 mL build is a clean 40-unit draw. As you titrate on the same concentration: 4 mg = 0.80 mL = 80 units, 8 mg = 1.60 mL = 160 units (this exceeds a single 100-unit barrel, so it is drawn as two fills), and 12 mg = 2.40 mL = 240 units (drawn across multiple fills).
Worked example 2 — the 30 mg vial
- Concentration: 30 mg ÷ 3 mL = 10 mg/mL
- Starting 2 mg dose: 2 mg ÷ 10 mg/mL = 0.20 mL = 20 units
- At 4 mg: 0.40 mL = 40 units | at 8 mg: 0.80 mL = 80 units | at 12 mg: 1.20 mL = 120 units
Notice the higher-strength 30 mg build keeps every draw small — the 20 mg, 24 mg and 30 mg vials all reconstitute to the same tidy 10 mg/mL, which is why they are convenient for higher maintenance doses. The full concentration map for all seven sizes:
| Vial | BAC water | Concentration | 2 mg dose | 4 mg dose | 8 mg dose | 12 mg dose |
|---|---|---|---|---|---|---|
| 5 mg | 2 mL | 2.5 mg/mL | 0.80 mL / 80 u | 1.60 mL / 160 u | 3.20 mL / 320 u | 4.80 mL / 480 u* |
| 6 mg | 1.2 mL | 5 mg/mL | 0.40 mL / 40 u | 0.80 mL / 80 u | 1.60 mL / 160 u | 2.40 mL / 240 u |
| 10 mg | 2 mL | 5 mg/mL | 0.40 mL / 40 u | 0.80 mL / 80 u | 1.60 mL / 160 u | 2.40 mL / 240 u |
| 12 mg | 1.2 mL | 10 mg/mL | 0.20 mL / 20 u | 0.40 mL / 40 u | 0.80 mL / 80 u | 1.20 mL / 120 u |
| 20 mg | 2 mL | 10 mg/mL | 0.20 mL / 20 u | 0.40 mL / 40 u | 0.80 mL / 80 u | 1.20 mL / 120 u |
| 24 mg | 2.4 mL | 10 mg/mL | 0.20 mL / 20 u | 0.40 mL / 40 u | 0.80 mL / 80 u | 1.20 mL / 120 u |
| 30 mg | 3 mL | 10 mg/mL | 0.20 mL / 20 u | 0.40 mL / 40 u | 0.80 mL / 80 u | 1.20 mL / 120 u |
*Any draw larger than 100 units (1.00 mL) exceeds a single U-100 barrel and must be split across multiple fills — which is why the low-concentration 5 mg build becomes impractical at higher doses.
The 5 mg vial deliberately reconstitutes to the lowest 2.5 mg/mL concentration, which makes the small starting doses easy to measure but pushes larger doses well past a single barrel. To avoid re-deriving these by hand, run your exact vial and dose through our peptide dosage calculator, and if you are new to reading a barrel, our insulin syringe units guide maps mL to units directly.
A note on why the concentration choice matters beyond convenience: a higher-concentration build (10 mg/mL) keeps every draw comfortably inside one barrel across the whole ladder, but leaves less margin for a small measurement slip, since each unit carries more drug. A lower-concentration build (2.5 mg/mL) spreads the dose across more units, so a one- or two-unit error is proportionally smaller — at the cost of multi-fill draws later. Neither is “correct” in the abstract; the documented builds above simply pick a sensible concentration for each vial size, and the calculator lets you model any alternative before you commit to a BAC volume.
Reconstitution and draw, step by step
The arithmetic above is only half the picture; the physical technique is what keeps a build sterile and accurate. The documented approach follows the same sequence used for any lyophilized GLP-1-class peptide:
- Let both components reach handling temperature and wipe the vial stopper and the bacteriostatic-water vial with fresh alcohol before every puncture.
- Draw the exact BAC volume for your chosen build (for the 10 mg reference build, 2 mL) into a reconstitution syringe.
- Add the water slowly down the inside wall of the peptide vial — aim the stream at the glass, not directly onto the powder cake. This limits foaming and shear stress on the peptide.
- Swirl, never shake. Gently roll the vial until the powder fully dissolves into a clear solution. Vigorous shaking can denature the peptide and introduce air.
- Let it settle, then draw your dose with a U-100 insulin syringe to the unit count from the table (40 units for a 2 mg dose at 5 mg/mL). Expel air bubbles back into the vial and re-read the meniscus before withdrawing the needle.
- Inject subcutaneously into a rotated site (abdomen or thigh are common), and return the vial straight to the fridge.
Two accuracy habits matter most: always read the syringe at eye level so the plunger tip lines up cleanly with the unit mark, and never “top up” a partial draw from memory — if you lose count, expel and start the draw again. Because a single vial covers several weekly doses, a repeated one- or two-unit error compounds across the whole vial’s life.
Weekly Schedule (Example Week)
Because Retatrutide is once-weekly, the “schedule” is really about anchoring a single injection to a fixed day and letting the other six days stay empty. The grid below shows a representative maintenance week at a 2 mg dose from a 10 mg / 5 mg/mL vial (40 units):
| Day | Action | Notes |
|---|---|---|
| Monday | Inject: 2 mg (40 units) | Chosen dosing day; rotate SC injection sites (abdomen/thigh) |
| Tuesday | None | Watch for post-dose GI symptoms; hydrate |
| Wednesday | None | Symptoms typically easing by now |
| Thursday | None | — |
| Friday | None | — |
| Saturday | None | — |
| Sunday | None | Prep next dose; assess whether an escalation week is due |
Because the molecule is long-acting, the exact day is flexible as long as it is consistent — the documented protocol keeps a roughly seven-day interval. If a dose is missed, the general trial guidance is to take it as soon as it is remembered if several days remain before the next scheduled dose, then resume the regular day; do not double up. This once-weekly cadence is one of the practical advantages of the long half-life: a single anchored injection covers the entire week, and there is no daily-dosing burden to maintain.
Dosing Phases, Titration & Cycling
Unlike recovery or cosmetic peptides that follow an on/off “cycle,” GLP-1-class agents like Retatrutide are studied as continuous therapy — the titration is the protocol, and there is no built-in off phase in the trials. The phases are best thought of as escalation stages:
- Induction (Step 1, ~weeks 1–4): 2 mg weekly. The goal is tolerability, not effect. Expect the strongest early appetite change and the highest chance of nausea.
- Escalation (Steps 2–3, ~weeks 5–12): step to 4 mg, then 8 mg, roughly every four weeks, only advancing when the current step is comfortable.
- Maintenance (Step 4+, ~week 13 onward): hold at the tolerated target (e.g. 12 mg in the common trial arm). The documented protocol keeps the dose at the highest well-tolerated level rather than cycling off.
The cardinal rule of titration: the timeline is a floor, not a ceiling. If GI symptoms are still significant at the end of a four-week block, the documented approach is to hold the current dose longer rather than escalate on schedule. Slowing the ladder is always the safer lever. There is no evidence that reaching a higher dose faster produces a better outcome; the trials escalated deliberately, and the tolerability data is the reason.
The pharmacology behind the four-week step is worth spelling out. A long-acting once-weekly agonist does not reach its steady-state blood level after a single injection — it accumulates over several doses until intake and clearance balance. That means the true tolerability of a given step is not fully visible on the day of the first injection at that dose; it emerges over the following weeks as the level plateaus. A four-week hold is roughly the window needed for a step to reach steady state and for the gut to adapt to it, which is why escalating before the block is complete effectively means judging a dose you have not yet fully experienced. This is the mechanistic reason the ladder is deliberately patient rather than arbitrarily cautious.
A second point that trips people up: the induction dose is explicitly sub-therapeutic by design. The 2 mg starting step is not expected to deliver a maintenance-level effect — its only job is to introduce the molecule gently. Interpreting the modest early effect as “the drug isn’t working” and reacting by jumping steps is exactly the mistake the ladder is built to prevent. Effect deepens as the dose climbs; the early weeks are about earning tolerance, not about results.
Timeline: What to Expect
The table frames what was observed in the research, not a promise of individual results — response varied substantially across trial participants, and nothing here should be read as a guaranteed outcome.
| Week / phase | What’s happening | What is observed in research |
|---|---|---|
| Weeks 1–4 (2 mg) | Molecule introduced; receptors engaging | Noticeable appetite suppression; early GI side effects most common here |
| Weeks 5–8 (4 mg) | First escalation; effect deepening | Continued appetite reduction; GI symptoms flare briefly after step-up, then settle |
| Weeks 9–12 (8 mg) | Approaching maintenance range | Weight change accumulating steadily in trial cohorts |
| Weeks 13–24 (12 mg maintenance) | Held at tolerated target | Largest cumulative weight reductions reported for a once-weekly agent to date |
| Beyond ~6 months | Continued maintenance | Phase 2 showed weight reduction was still trending downward at 48 weeks (had not fully plateaued) |
One honest caveat from the data: because the Phase 2 curve had not clearly plateaued by the end of the study, the full ceiling of the effect is genuinely not yet known — that is one of the questions the Phase 3 TRIUMPH program is designed to answer. Read the timeline above as a description of aggregate trial behaviour, not as a schedule of results any individual should expect.
Stacking & Combinations
In the clinical trials Retatrutide was studied as a standalone agent, not stacked with other incretins — so there is no trial-validated combination to document. Combining it with another GLP-1 or GIP agonist (semaglutide, tirzepatide) would compound the same receptor load and the same GI and hypoglycemia risks with no efficacy evidence to support it; the documented protocol is monotherapy. The only meaningful “comparison” context is against the other agents in the class, covered in our Retatrutide vs Semaglutide vs Tirzepatide analysis, and the two entry points for the protocol itself are the 5 mg vial protocol for a gentle start and the 30 mg vial protocol for higher maintenance targets.
It is worth being blunt about why the “more is better” instinct is especially wrong for this molecule. Layering a second incretin agonist on top of Retatrutide does not add a new mechanism — it doubles down on receptors the triple agonist already saturates, so the predictable result is additive gastrointestinal load and, if either agent has glucose-lowering partners on board, additive hypoglycemia risk. There is no trial that studied such a combination, which means anyone attempting it would be operating with zero efficacy evidence and stacked-up known risks. The documented protocol is monotherapy for exactly this reason, and the honest comparison to make is not “Retatrutide plus X” but “Retatrutide versus X,” which is what the comparison article covers.
When Progress Stalls
A plateau is the most common reason people are tempted to break protocol. Work down this troubleshooting ladder before considering any dose change — and always inside the research-use-only, escalate-slowly framing:
- Confirm you are actually at a maintenance dose. Many apparent “stalls” are simply someone still early in the ladder expecting a maintenance-level effect. Effect deepens as the dose climbs.
- Verify the reconstitution math. A concentration error (wrong BAC volume) silently under- or over-doses every injection. Re-derive mg/mL and re-check your unit count against the table above.
- Hold, do not jump. If tolerated, the documented approach is to stay at the current step for the full interval before the next scheduled escalation — not to leapfrog steps.
- Respect the four-week cadence. Escalating faster than the documented ~4-week rhythm buys GI misery, not faster results.
- Check storage integrity. Degraded peptide from improper storage reduces potency; see storage rules below.
It also helps to reframe what a “plateau” even is. In the Phase 2 obesity data the weight curve was still trending downward at 48 weeks, so a genuine plateau at a tolerated maintenance dose may simply reflect the body settling toward a new set point rather than the protocol failing. A short flattening in a personal timeline is not automatically a signal to intervene — it is often the expected shape of the response. The lever that reliably backfires is impatience: compressing the ladder to chase a number trades the one tolerability tool the protocol has for a burst of avoidable GI symptoms.
The wrong move is to react to a stall by spiking the dose. The documented ladder is stepwise for a reason, and the safest response to a plateau is patience at the current step, not a jump. Any real decision to change dose on an investigational drug belongs with a licensed clinician, not a troubleshooting checklist.
Side Effects & Mitigation
Retatrutide’s side-effect profile is overwhelmingly gastrointestinal and dose-dependent, concentrated in the days after a dose and after each escalation. The mitigations below reflect the general approach to GLP-1-class tolerability documented in the research:
| Issue | Why it happens | Mitigation |
|---|---|---|
| Nausea | GLP-1/GIP slowing of gastric emptying | Smaller, lower-fat meals; eat to comfort not fullness; the slow titration is the primary defense |
| Diarrhea / vomiting | GI motility changes, strongest after step-ups | Hydrate and replace electrolytes; hold the dose (don’t escalate) until it settles |
| Constipation | Slowed transit | Fiber, fluids, movement |
| Decreased appetite (excessive) | The intended effect, overshooting | Ensure adequate protein/nutrient intake; a too-fast climb often drives this |
| Injection-site reaction | Subcutaneous administration | Rotate sites; proper aseptic technique |
| Increased heart rate | Class effect of incretin agonists | Reference-level monitoring; a clinician’s domain |
| Hypoglycemia (with other agents) | Additive glucose-lowering | Major risk only when combined with insulin/sulfonylureas — a clinician-managed scenario |
The through-line: nearly every one of these is mitigated first by titrating slowly. The four-week ladder is not bureaucratic caution — it is the single most effective tolerability tool in the protocol.
Safety & Contraindications
Regulatory reality first: Retatrutide is investigational and not approved by the FDA or EMA for any indication. There is no approved label, no pharmacy product, and the Phase 3 TRIUMPH program is still enrolling and reporting. Everything here is documented trial/research information under a research-use-only framing — it is not a prescription, not a recommendation, and not intended for human consumption.
Because Retatrutide is a GLP-1-class agonist, the well-established class safety warnings apply as reference context:
- Thyroid C-cell tumors / MTC (boxed-warning class effect): GLP-1 receptor agonists carry a boxed warning for thyroid C-cell tumors based on rodent data. A personal or family history of medullary thyroid carcinoma (MTC) or Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) is treated as a contraindication for the class.
- Pancreatitis: acute pancreatitis is a recognized class risk; severe, persistent abdominal pain is a stop-and-seek-care signal.
- Gallbladder disease: rapid weight change and the incretin effect are associated with gallbladder events in the class.
- Hypoglycemia: low risk alone, but meaningfully elevated when combined with insulin or sulfonylureas.
Beyond the absolute contraindications, several situations call for heightened caution in the class framing and are firmly a clinician’s domain: a history of pancreatitis or symptomatic gallstones, significant gastrointestinal motility disorders (such as gastroparesis, which slowed gastric emptying can worsen), diabetic retinopathy that is not stabilized, severe renal impairment where dehydration from GI side effects raises risk, and any concurrent use of insulin or a sulfonylurea, where the additive glucose-lowering can produce hypoglycemia. None of these is a footnote — each is a reason a real prescribing decision would require individual medical assessment rather than a generic protocol.
There are also two “stop and seek care” signals worth stating plainly as reference context, because they are the class’s more serious events: severe, persistent abdominal pain (which may radiate to the back and can signal pancreatitis) and symptoms of gallbladder disease such as right-upper-quadrant pain, fever, or jaundice. In the class labeling these are treated as prompts to halt and obtain evaluation, not symptoms to push through.
Who must avoid it entirely in the class framing: anyone pregnant or breastfeeding, anyone with the personal/family MTC or MEN 2 history above, and anyone with prior serious hypersensitivity to a GLP-1 agonist. Any real-world decision about an investigational drug belongs to a licensed clinician, full stop.
Storage & Handling
- Before reconstitution: the lyophilized vial is stable refrigerated; keep it cold and protected from light. Many suppliers note short-term room-temperature stability for shipping, but the fridge is the default.
- After reconstitution: store the mixed vial refrigerated at roughly 2–8°C and use it within the working window (commonly cited as up to ~4 weeks for reconstituted GLP-1-class peptides). Because a single vial spans several once-weekly doses, cold storage integrity directly affects the potency of your last dose.
- Handling: add bacteriostatic water slowly down the vial wall, do not shake (swirl gently), and never freeze a reconstituted solution.
- Light and transport: keep vials out of direct light and, when transporting, use a small insulated cold pack rather than leaving a reconstituted vial at ambient temperature for extended periods.
- Inspect before every draw: a properly reconstituted solution is clear and colorless. Cloudiness, visible particulates, or discoloration are signals to discard rather than inject.
The reason storage discipline matters more here than for a single-use peptide is arithmetic: because one vial spans several once-weekly doses over potentially a month, the solution has to hold potency across that entire window. A vial that was allowed to warm repeatedly, or that is nearing the end of its working window, may deliver a weaker last dose than its first — which can masquerade as a plateau. Full temperature and shelf-life detail is in our peptide reconstitution guide, which pairs with the calculator for building each vial correctly.
What the Evidence Actually Shows
Being transparent about the evidence tier matters here more than for almost any other peptide, because the hype has outrun the approval timeline. Here is the honest state of the data:
- Obesity (Phase 2, randomized controlled trial): the landmark New England Journal of Medicine Phase 2 trial in obesity established both the once-weekly dosing and the escalation approach, and reported the largest average weight reductions seen for a once-weekly agent — with the caveat that the reduction had not fully plateaued at 48 weeks.
- Type 2 diabetes (Phase 2, randomized controlled trial): a separate randomized Phase 2 trial published in The Lancet documented strong glycemic control in type 2 diabetes.
- Phase 3 (ongoing): the TRIUMPH program is the pivotal Phase 3 effort. Until it reports and a regulator reviews it, there is no approval and no confirmed long-term safety verdict — that is the central evidence gap.
- Class safety (regulatory labeling): the boxed warning and monitoring guidance are extrapolated from the broader FDA/EMA GLP-1 class labeling, not yet from a Retatrutide-specific approved label (there isn’t one).
It is worth being precise about what a Phase 2 trial can and cannot establish. A well-run randomized Phase 2 study is strong evidence of an efficacy signal and a first read on short-to-medium-term safety in a selected population — it is why the weight-reduction numbers are credible rather than anecdotal. What Phase 2 is not powered to do is detect rarer adverse events, confirm long-term safety, or establish outcomes over years of use. Those are precisely the questions the larger, longer Phase 3 TRIUMPH program is designed to answer, which is why an approval decision waits on it. Reading the current data honestly means holding two facts at once: the signal is real, and the verdict is not yet in.
The same discipline applies to the safety picture. Because there is no Retatrutide-specific approved label, every safety statement on this page is class-level extrapolation from the established GLP-1 receptor-agonist labeling — the boxed thyroid C-cell warning, the pancreatitis and gallbladder monitoring guidance, the hypoglycemia interaction with insulin and sulfonylureas. That extrapolation is reasonable and standard, but it is an extrapolation, not a Retatrutide-specific regulatory finding. Where the molecule’s triple mechanism might differ from single or dual agonists on safety is one of the open questions, not a settled one.
In short: the efficacy signal is genuinely strong and comes from real randomized trials, but Retatrutide remains investigational. The correct posture is enthusiasm about the science paired with sobriety about the still-open Phase 3 and safety questions. Nothing in the published data licenses treating this molecule as a finished, approved medicine.
Frequently Asked Questions
Choosing & Understanding Retatrutide
What is the typical Retatrutide dosage? The documented research protocol starts at 2 mg once weekly and escalates stepwise roughly every four weeks toward maintenance targets such as 4, 8, and 12 mg. It is a titrated dose, not a single fixed number.
How does Retatrutide differ from semaglutide and tirzepatide? Semaglutide is a single (GLP-1) agonist and tirzepatide is a dual (GIP + GLP-1) agonist, while Retatrutide is a triple agonist adding the glucagon receptor. That third arm is thought to drive its unusually large weight effect. See our full comparison.
Why does Retatrutide need titration at all? Because the GLP-1/GIP arms slow gastric emptying, jumping straight to a high dose provokes strong nausea, diarrhea, and vomiting. The slow ladder lets the gut adapt, which is why side effects are dose-dependent and mostly early.
Is the 30 mg vial a starting dose? No. The 30 mg figure is a vial strength, not a starting weekly dose. Even from a 30 mg vial the documented start is still 2 mg weekly (0.20 mL / 20 units at 10 mg/mL) — the large vial simply covers many doses.
Using It & the Titration
How do I reconstitute a 10 mg Retatrutide vial? Add 2 mL of bacteriostatic water for 5 mg/mL. A 2 mg dose is then 2 ÷ 5 = 0.40 mL = 40 units on a U-100 syringe. Run your own vial through the calculator to confirm.
What does a 30 mg vial reconstitute to? 30 mg + 3 mL = 10 mg/mL. At that concentration a 2 mg dose is 0.20 mL (20 units), 4 mg is 40 units, 8 mg is 80 units, and 12 mg is 120 units.
Is Retatrutide dosed daily or weekly? Once weekly. It is long-acting; the documented protocol uses a single weekly injection on a consistent day, not daily dosing.
How fast should the dose be escalated? The trial-documented cadence is roughly every four weeks, and only if the current step is well tolerated. If GI symptoms are still significant, the documented approach is to hold the current dose longer rather than escalate on schedule.
How many units is a Retatrutide dose? It depends entirely on the concentration. At 5 mg/mL (10 mg + 2 mL), 2 mg = 40 units. At 10 mg/mL (30 mg + 3 mL), 2 mg = 20 units. Multiply your draw volume in mL by 100 — our syringe units guide walks through it.
Which vial size gives the lowest, most measurable starting dose? The 5 mg vial + 2 mL gives 2.5 mg/mL, so a 2 mg start is a large, easy-to-measure 0.80 mL (80 units) — convenient early on, though larger doses later exceed one barrel. The 5 mg vial protocol covers this build.
Practical & Safety
Is Retatrutide FDA approved? No. Retatrutide is investigational; it is not approved by the FDA or EMA for any use, and its Phase 3 TRIUMPH program is still ongoing. This page is research-use-only reference information.
What are the main side effects? Predominantly gastrointestinal — nausea, diarrhea, vomiting, constipation, and decreased appetite — all dose-dependent and most common after a dose or an escalation. See Retatrutide side effects and safety research.
Who should not use Retatrutide? Under the GLP-1 class framing, it is contraindicated for anyone with a personal or family history of medullary thyroid carcinoma (MTC) or MEN 2, anyone pregnant or breastfeeding, and anyone with prior serious GLP-1 hypersensitivity. The class also carries pancreatitis and gallbladder warnings.
Can Retatrutide be stacked with another GLP-1? The trials studied it as a standalone. Combining it with another incretin agonist compounds GI and hypoglycemia risk with no supporting evidence, so the documented protocol is monotherapy.
How long can a reconstituted vial be kept? Store it refrigerated at ~2–8°C and use it within the working window commonly cited for reconstituted GLP-1-class peptides (up to ~4 weeks). Never freeze a reconstituted solution. Details in the reconstitution guide.
References
- Jastreboff AM, et al. Triple-Hormone-Receptor Agonist Retatrutide for Obesity — A Phase 2 Trial. N Engl J Med, 2023. doi:10.1056/NEJMoa2301972.
- Rosenstock J, et al. Retatrutide, a GIP, GLP-1 and glucagon receptor agonist, for people with type 2 diabetes: a randomised, double-blind, placebo and active-controlled, parallel-group, phase 2 trial. The Lancet, 2023.
- ClinicalTrials.gov — TRIUMPH-1: A Master Protocol to Investigate the Efficacy and Safety of Retatrutide (LY3437943) Once Weekly in Participants Without Type 2 Diabetes Who Have Obesity or Overweight (NCT05929066).
- FDA Prescribing Information, WEGOVY (semaglutide) — Boxed Warning: Risk of Thyroid C-Cell Tumors (medullary thyroid carcinoma); GLP-1 receptor-agonist class labeling. DailyMed.
Disclaimer: This article is provided for research and educational purposes only. Retatrutide is an investigational compound that is not approved by the FDA or EMA and is not a medicine. Nothing here is medical advice, a prescription, or a personal recommendation, and none of this material is intended for human consumption or for diagnosing, treating, or preventing any condition. All dosing figures describe the documented research/trial protocol under a strict research-use-only framing. Always consult a licensed clinician before making any health decision.