If you have ever stared at a freshly reconstituted vial and a U-100 insulin syringe wondering how many little tick marks equals my dose, this page is the answer. A peptide dosage chart collapses three separate questions — how much bacteriostatic water to add, what the documented research dose is, and how many syringe units that dose works out to — into a single row you can read at a glance. That is the problem this hub solves: it turns the intimidating arithmetic of reconstitution into a lookup table, then teaches you the one formula underneath it so you are never dependent on the table alone. Whether you searched for peptide dosages, a peptide reconstitution chart, or simply “how many units” a compound works out to, everything is derived here from two documented inputs and shown as arithmetic you can check.
One honest sentence about the evidence before we go further: the numbers below are the documented research starting points published on the individual protocol pages in our peptide dosage catalog — they are reference figures for research handling, not medical prescriptions, and the human clinical evidence behind most of these compounds ranges from robust (the GLP-1 agonists) to preliminary or preclinical (most of the recovery and longevity peptides). Read every number here as “this is the dose used in the documented research protocol,” never as “this is the dose you should take.”
Who is this chart for? It is built for the person who already has a vial and a syringe in front of them and needs to translate a documented protocol figure into a physical mark on a plunger — not for someone deciding whether to use a compound at all. That decision belongs to a qualified professional and to the full evidence discussion on each protocol page. What a chart is genuinely good at is the mechanical translation step: it removes the mental arithmetic between “the protocol says 200 mcg” and “draw to the 12-unit line.” That is the narrow, honest job of the tables below, and everything on this page is organised around doing that one step transparently.

At a Glance: What This Chart Gives You
| Item | What it means on this page |
|---|---|
| Scope | 20 of the most-used peptides across 6 categories — Blends, Recovery, Growth Hormone, Metabolic/GLP-1, Longevity, Sexual/Hormonal |
| Vial size | The milligrams (mg) of lyophilized peptide in the vial, as documented on the protocol page |
| BAC water | The volume of bacteriostatic water (mL) added in the documented protocol to reconstitute the vial |
| Concentration | Computed: vial mg ÷ BAC mL = mg/mL (the strength of your solution) |
| Documented starting dose | The per-injection research starting amount from the protocol page (never a prescription) |
| Units on U-100 | Computed: the tick mark on a standard 1 mL / 100-unit insulin syringe that equals that dose |
| Framing | Research-use-only (RUO). Documented starting points, not personal recommendations. For any other vial size or dose, use the interactive dosage calculator. |
Every concentration and unit figure in the category tables below was computed from the two inputs the protocol pages give — vial strength and BAC volume — using the formula in the next section. Nothing is estimated; the arithmetic is shown so you can verify it yourself. Where a figure required rounding — most concentrations that are not whole numbers, such as 1.67, 3.33 or 26.67 mg/mL — we round to two decimal places for the concentration and to the nearest half-unit for the syringe mark, which mirrors what a U-100 barrel can actually be read to. The underlying division is always exact; the rounding lives only in how the number is displayed, and each category table is followed by a worked check so you can trace the full-precision math yourself.
The One Formula Behind Every Row
You do not need to memorize twenty rows. You need one three-step formula, and then the whole chart becomes readable — including vial sizes and doses that are not printed here. Here it is in plain English before the symbols:
- Find the concentration. Divide the peptide in the vial by the water you added. That tells you how strong every milliliter of your solution is.
- Find the volume to draw. Divide your target dose by that concentration. That tells you how many milliliters of solution contain your dose.
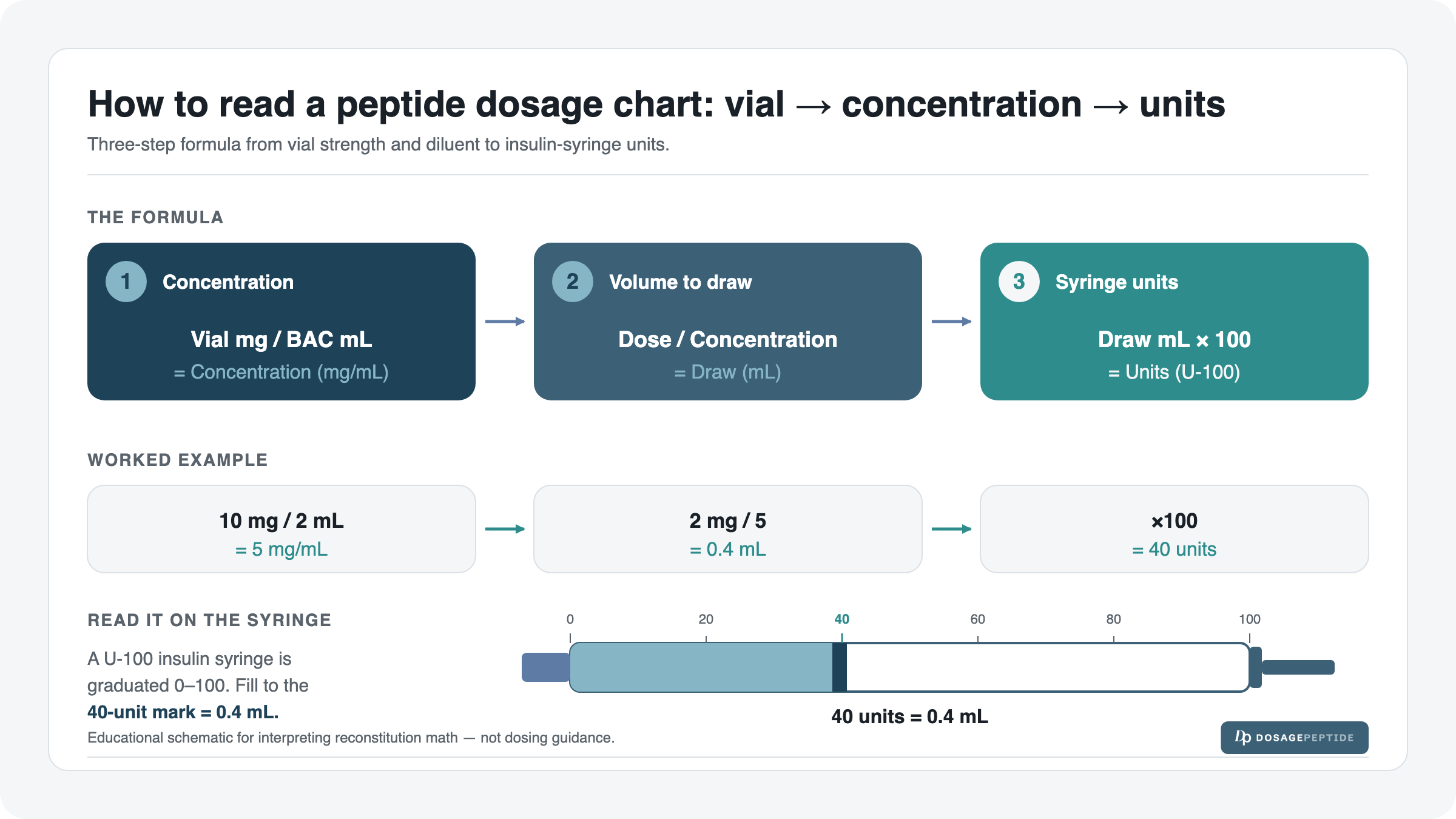
- Convert to syringe units. Multiply the milliliters by 100. On a U-100 insulin syringe, 100 units = 1 mL, so 1 unit = 0.01 mL — multiplying by 100 lands you directly on the tick mark to draw to.
| Step | Formula | Gives you |
|---|---|---|
| 1. Concentration | vial mg ÷ BAC mL | mg per mL (mg/mL) |
| 2. Draw volume | dose ÷ concentration | millilitres to draw (mL) |
| 3. Syringe units | draw mL × 100 | units on a U-100 syringe |
A note on units before the doses: keep the dose and the concentration in the same mass unit before you divide. If a dose is written in micrograms and the concentration is in mg/mL, convert the dose to milligrams first (divide mcg by 1,000). Every worked example below does this conversion explicitly so the division is apples-to-apples.
One Fully Worked Example (Retatrutide, 10 mg vial)
Let us walk a single row from raw vial to a mark on the plunger so the pattern is unmistakable. Take a 10 mg Retatrutide vial reconstituted with 2 mL of bacteriostatic water, aiming for the documented 2 mg starting dose.
- Concentration: 10 mg ÷ 2 mL = 5 mg/mL. Every millilitre of this solution holds 5 mg of peptide.
- Draw volume: 2 mg ÷ 5 mg/mL = 0.4 mL. Four-tenths of a millilitre contains the 2 mg dose.
- Syringe units: 0.4 mL × 100 = 40 units. On a U-100 syringe you draw the plunger to the 40-unit line.
That is the entire skill. Concentration, then volume, then units. If you can do it once, you can read any row in the chart — and if your vial or dose differs from the tables, the same three steps still apply. When the arithmetic gets awkward (odd vial sizes, half-doses, titration steps), send it to the dosage calculator rather than rounding in your head. If the reconstitution step itself is new to you, the peptide reconstitution guide walks through adding the water without foaming or degrading the peptide, and the companion article on how much bacteriostatic water to use explains why the same vial can be reconstituted to different concentrations on purpose.
How to Read Any Row of the Chart Start to Finish
Once the formula is in hand, reading a chart row is a matter of matching what you see on the shelf to what the table lists. Work through it in this order every time and you will never mis-read a row:
- Match the vial size. Look at the milligram figure printed on your vial and find the row with the same “Vial” value. If your vial is a different strength, the row’s units do not apply — jump to the calculator.
- Match the BAC water volume. The units column is computed for the exact “BAC water” figure shown. If you added a different volume, your concentration is different, so your units are different.
- Confirm the concentration. Divide the two matched numbers yourself as a sanity check. If your division does not match the “Concentration” column, you have mismatched a vial or a volume somewhere.
- Locate the documented dose. This is the per-injection research starting figure. It is the number the row’s units are calculated from — not a target you should scale up on your own.
- Draw to the units mark. The final column is the tick on a U-100 syringe. Pull the plunger to that line, having first cleared air bubbles so the meniscus sits cleanly on the mark.
If any of steps 1–3 fail to match, the row is not yours — that is the single most common way people end up drawing the wrong amount. The chart is a set of pre-solved equations for specific inputs, and a pre-solved answer is only correct for the inputs it was solved for.
Why mcg vs mg — and Reading a U-100 Syringe
Two units of mass appear across this chart and confusing them is the single most common dosing error. A milligram (mg) is one-thousandth of a gram. A microgram (mcg or µg) is one-thousandth of a milligram. So 1 mg = 1,000 mcg. A recovery peptide dosed at “200 mcg” and a GLP-1 dosed at “2 mg” differ by a factor of ten in that example, and by far more in others — writing 200 mg where 200 mcg was meant is a thousand-fold error. In the tables below we keep each peptide in whichever unit its protocol page uses, but the computed columns normalise everything so the syringe units are directly comparable.
| Unit | Equal to | Typical peptides dosed this way |
|---|---|---|
| 1 gram (g) | 1,000 mg | Not used for peptide doses — vial-total scale only |
| 1 milligram (mg) | 1,000 mcg | GLP-1 agonists, longevity compounds (Epithalon, NAD+) |
| 1 microgram (mcg / µg) | 0.001 mg | Recovery peptides, most GH-axis secretagogues |
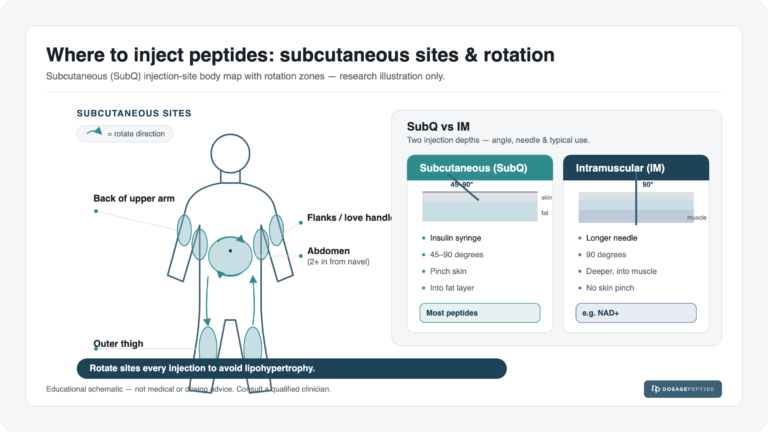
The U-100 insulin syringe is the reference instrument for almost every peptide here. “U-100” means the syringe is calibrated so that 100 units of fluid equals exactly 1 mL. That gives you the two conversions you will use constantly:
- 100 units = 1 mL
- 50 units = 0.5 mL
- 10 units = 0.1 mL
- 1 unit = 0.01 mL
Because the syringe measures volume, not mass, the same peptide dose can land on a different unit mark depending on how concentrated your solution is — which is exactly why the chart’s “units” column is only valid for the specific vial/BAC pairing in that row. For a deeper walkthrough of reading the barrel and why unit marks are not the same as milligrams, see the insulin syringe units guide.
The Master Peptide Dosage Chart
Below is the complete chart, split into the six catalog categories. For every row: Concentration = vial mg ÷ BAC mL, and Units on U-100 = (documented dose ÷ concentration) × 100. All figures are computed directly from the two documented inputs. Remember: these are documented research starting points tied to the exact vial size and reconstitution volume shown — not prescriptions, and not valid for a different vial or a different amount of water.
The categories are ordered the way the catalog is organised, and each has its own dosing personality worth skimming for before you dive into a row. Blends carry the highest total milligrams but small draws. Recovery peptides live in the microgram range at gentle concentrations. The growth-hormone group has the widest spread of any category on the page. The metabolic/GLP-1 compounds are the best-evidenced and are dosed in milligrams with formal titration behind them. Longevity spans the numeric extremes, from micrograms to a 500 mg NAD+ vial. And the sexual/hormonal pair is a clean matched-concentration illustration of dose-versus-units. Reading the short paragraph above each table first tells you what to expect before the numbers do.
Blends
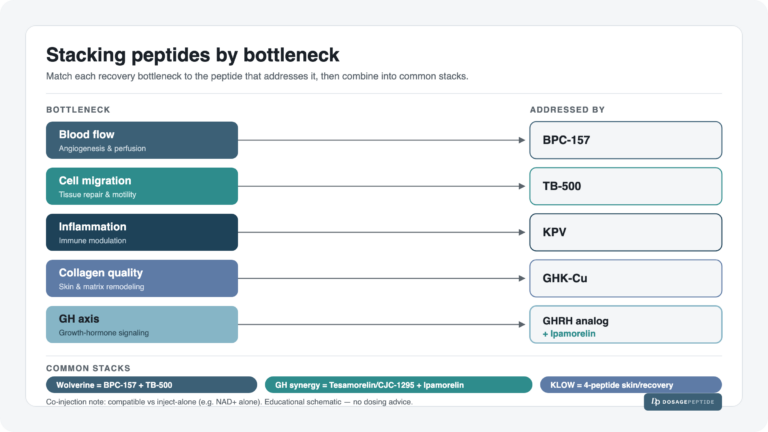
Blends pre-combine two or more peptides in a single vial, so a modest draw delivers several compounds at once. Note how the high total-milligram blends (KLOW, GLOW) reach their large mcg doses on a very small unit mark, because the solution is so concentrated.
| Peptide | Vial | BAC water | Concentration | Documented starting dose | Units on U-100 |
|---|---|---|---|---|---|
| KLOW (blend) | 80 mg | 3 mL | 26.67 mg/mL | 2,667 mcg | 10 units |
| GLOW (blend) | 70 mg | 3 mL | 23.33 mg/mL | 2,330 mcg | 10 units |
| BPC-157 + TB-500 (blend) | 10 mg | 3 mL | 3.33 mg/mL | 600 mcg | 18 units |
| Ipamorelin + Tesamorelin (blend) | 10 mg | 3 mL | 3.33 mg/mL | 330 mcg | 10 units |
Worked check on KLOW: 80 mg ÷ 3 mL = 26.67 mg/mL; 2,667 mcg = 2.667 mg; 2.667 ÷ 26.67 = 0.10 mL; × 100 = 10 units. The KLOW dosage protocol guide covers the full blend rationale and cycle.
Recovery
The recovery peptides are dosed in micrograms and, at 5 mg/3 mL, sit at a gentle 1.67 mg/mL concentration — so their doses spread across a comfortable range of unit marks. TB-500’s larger 500 mcg dose lands at 30 units precisely because the solution is dilute.
| Peptide | Vial | BAC water | Concentration | Documented starting dose | Units on U-100 |
|---|---|---|---|---|---|
| BPC-157 | 5 mg | 3 mL | 1.67 mg/mL | 200 mcg | 12 units |
| TB-500 | 5 mg | 3 mL | 1.67 mg/mL | 500 mcg | 30 units |
| GHK-Cu | 50 mg | 3 mL | 16.67 mg/mL | 1 mg (1,000 mcg) | 6 units |
Worked check on BPC-157: 5 mg ÷ 3 mL = 1.67 mg/mL; 200 mcg = 0.2 mg; 0.2 ÷ 1.67 = 0.12 mL; × 100 = 12 units. GHK-Cu’s 50 mg vial makes a strong 16.67 mg/mL solution, so its 1 mg dose is only 6 units — a good example of why concentration, not dose alone, sets the mark.
Growth Hormone (GHRH analogs & secretagogues)
This category shows the widest spread of unit marks on the whole chart. Tesamorelin’s 2 mg dose from a 3.33 mg/mL vial reaches all the way to 60 units, while Ipamorelin and Sermorelin at 100 mcg barely move the plunger to 6 units — same category, tenfold-plus difference in draw.
| Peptide | Vial | BAC water | Concentration | Documented starting dose | Units on U-100 |
|---|---|---|---|---|---|
| Tesamorelin | 10 mg | 3 mL | 3.33 mg/mL | 2 mg (2,000 mcg) | 60 units |
| Ipamorelin | 5 mg | 3 mL | 1.67 mg/mL | 100 mcg | 6 units |
| CJC-1295 DAC | 2 mg | 2 mL | 1.00 mg/mL | 300 mcg | 30 units |
| Sermorelin | 5 mg | 3 mL | 1.67 mg/mL | 100 mcg | 6 units |
Worked check on Tesamorelin: 10 mg ÷ 3 mL = 3.33 mg/mL; 2 mg ÷ 3.33 = 0.60 mL; × 100 = 60 units — three-fifths of the entire syringe. CJC-1295 DAC is a clean case: 2 mg ÷ 2 mL = exactly 1 mg/mL, so 300 mcg = 0.3 mL = 30 units with no rounding at all.
Metabolic / GLP-1
The GLP-1 and GLP-1/GIP/glucagon agonists are the best-studied compounds on this chart in human trials, and their doses are given in milligrams. Watch the concentration effect: Tirzepatide’s 2.5 mg from a 2.5 mg/mL solution needs a full 1 mL (100 units), whereas Semaglutide’s much smaller 0.25 mg from the same-strength solution is just 10 units. (5-Amino-1MQ is an orally-studied metabolic compound grouped here for the catalog; its documented figure is shown for completeness.)
| Peptide | Vial | BAC water | Concentration | Documented starting dose | Units on U-100 |
|---|---|---|---|---|---|
| Semaglutide | 5 mg | 2 mL | 2.50 mg/mL | 0.25 mg (250 mcg) | 10 units |
| Tirzepatide | 5 mg | 2 mL | 2.50 mg/mL | 2.5 mg (2,500 mcg) | 100 units |
| Retatrutide | 10 mg | 2 mL | 5.00 mg/mL | 2 mg (2,000 mcg) | 40 units |
| 5-Amino-1MQ | 10 mg | 3 mL | 3.33 mg/mL | 150 mcg | 4.5 units |
Worked check on Semaglutide: 5 mg ÷ 2 mL = 2.5 mg/mL; 0.25 mg ÷ 2.5 = 0.10 mL; × 100 = 10 units. Tirzepatide’s 2.5 mg from that identical 2.5 mg/mL solution fills the whole barrel at 100 units — a vivid reminder that the unit mark tracks the dose, not the peptide. Both GLP-1s are titrated upward slowly; the Semaglutide titration protocol and Tirzepatide titration protocol lay out the documented step-up schedules that this single “starting dose” row cannot show.
Longevity
The longevity group spans the extremes of the chart. Epithalon’s 5 mg dose and NAD+’s 50 mg dose are enormous relative to a recovery peptide, but NAD+’s highly concentrated 100 mg/mL vial keeps even 50 mg to a moderate 50-unit draw.
| Peptide | Vial | BAC water | Concentration | Documented starting dose | Units on U-100 |
|---|---|---|---|---|---|
| MOTS-C | 10 mg | 3 mL | 3.33 mg/mL | 200 mcg | 6 units |
| Epithalon | 10 mg | 2 mL | 5.00 mg/mL | 5 mg (5,000 mcg) | 100 units |
| NAD+ | 500 mg | 5 mL | 100.00 mg/mL | 50 mg (50,000 mcg) | 50 units |
Worked check on NAD+: 500 mg ÷ 5 mL = 100 mg/mL; 50 mg ÷ 100 = 0.5 mL; × 100 = 50 units. Epithalon’s 5 mg from a 5 mg/mL solution is exactly 1 mL, i.e. the full 100-unit barrel — another clean, no-rounding row.
Sexual / Hormonal
These two share an identical 10 mg vial reconstituted with 2 mL, so both sit at 5.00 mg/mL — a clean setup for seeing how dose alone moves the unit mark within one fixed concentration.
| Peptide | Vial | BAC water | Concentration | Documented starting dose | Units on U-100 |
|---|---|---|---|---|---|
| PT-141 | 10 mg | 2 mL | 5.00 mg/mL | 1 mg (1,000 mcg) | 20 units |
| Melanotan II | 10 mg | 2 mL | 5.00 mg/mL | 250 mcg | 5 units |
Worked check on PT-141: 10 mg ÷ 2 mL = 5 mg/mL; 1 mg ÷ 5 = 0.2 mL; × 100 = 20 units. Melanotan II shares the identical vial and concentration but its smaller 250 mcg dose is only 5 units — the same two-inputs, different-dose lesson one more time.
Why the Same Dose Can Be a Different Unit Mark
The single most important idea in this whole page is that the unit mark you draw to is a product of both your dose and your concentration — never the dose alone. Concentration is set by how you reconstituted the vial: more water makes a weaker, more dilute solution (a bigger draw for the same dose); less water makes a stronger, more concentrated solution (a smaller draw). Two examples from the chart make it concrete:
| Comparison | Dose | Concentration | Units on U-100 | Takeaway |
|---|---|---|---|---|
| Ipamorelin vs Melanotan II | 100 mcg vs 250 mcg | 1.67 vs 5.00 mg/mL | 6 vs 5 units | A larger dose (250 mcg) can be a smaller unit mark when its solution is more concentrated |
| Semaglutide vs Tirzepatide | 0.25 mg vs 2.5 mg | 2.50 vs 2.50 mg/mL | 10 vs 100 units | Identical concentration; the 10× dose difference is the entire 10× unit difference |
The practical consequence: a unit count copied from a friend, a forum, or even this chart is only valid if their vial size AND their bacteriostatic-water volume match yours exactly. Change either input and the unit mark changes. This is precisely why we show concentration in every row and why, for any vial or dose that differs from the documented pairing, the right move is the interactive calculator — it recomputes concentration and units for your specific inputs instead of leaving you to reverse-engineer a chart built for a different vial.
How Vial Strength and BAC Volume Interact
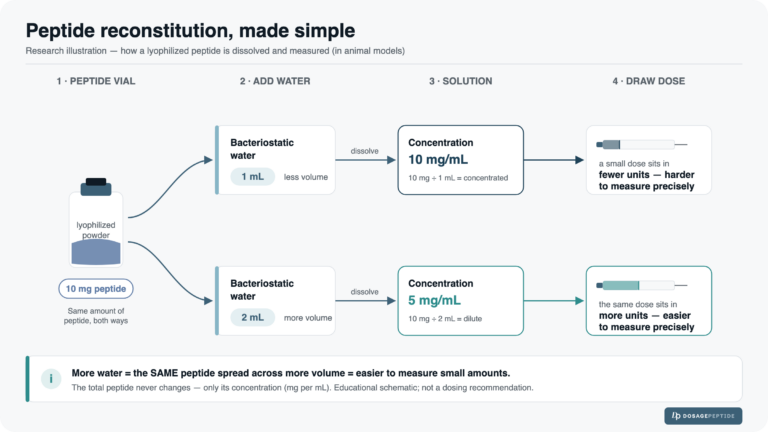
Reconstitution gives you two levers, and it helps to see how each one moves the result. Holding the peptide amount fixed and varying only the water shows the concentration lever in isolation. Here is a 5 mg vial reconstituted three different ways, dosed at a constant 250 mcg:
| Vial | BAC water | Concentration | Dose | Draw volume | Units on U-100 |
|---|---|---|---|---|---|
| 5 mg | 1 mL | 5.00 mg/mL | 250 mcg | 0.05 mL | 5 units |
| 5 mg | 2 mL | 2.50 mg/mL | 250 mcg | 0.10 mL | 10 units |
| 5 mg | 3 mL | 1.67 mg/mL | 250 mcg | 0.15 mL | 15 units |
Same peptide, same dose — but 5, 10, or 15 units depending only on the water. More water is not “more” or “less” peptide; it is the same peptide spread across a larger, easier-to-measure volume. Many people deliberately add more water to a potent, small-dose peptide so the draw lands on a readable unit mark instead of an unmeasurable sliver near zero. This is a technique choice, not a dose change, and it is one of the main reasons the bacteriostatic water article exists. Once the water is chosen, the reconstitution guide covers adding it correctly, and the syringe units guide covers drawing to the resulting mark.
There is a practical floor to this, too. A U-100 syringe is realistically readable to about half a unit, so a draw computed at, say, 4.5 units (the 5-Amino-1MQ row) sits near the low end of comfortable precision. When the documented dose lands below roughly 3–5 units at a given concentration, adding a little more water to spread that same dose across more units is the usual remedy — again, a measurement decision, not a dose decision. The calculator will show you the exact units for any water volume so you can pick a pairing that reads cleanly.
The opposite edge matters as well. A dose that computes to more than 100 units cannot be drawn in a single U-100 syringe at that concentration — you would either split it across two draws or reconstitute at a higher concentration (less water) so the same dose fits under the 100-unit mark. Nothing on this chart crosses that ceiling at its documented pairing, but it is exactly the kind of constraint that appears the moment you deviate from the listed vial or water volume, and it is another reason the interactive tool is the safer path for off-chart inputs than mental arithmetic. Choosing a water volume is, in practice, choosing where on the barrel your dose will sit — and the sweet spot is a mark far enough from zero to read precisely and far enough from 100 to draw in one pull.
Common Mistakes When Reading a Peptide Dosage Chart
Most dosing errors are not exotic — they come from a small handful of predictable slips. Knowing them in advance is the cheapest possible safeguard.
| Mistake | What goes wrong | The fix |
|---|---|---|
| Borrowing a unit count from a mismatched vial | The units column is only valid for one vial/water pairing; a different vial makes the same “10 units” a different dose entirely | Confirm both vial mg and BAC mL match the row before trusting its units; otherwise recompute |
| Confusing mcg with mg | A 1,000-fold error — reading “200 mg” where “200 mcg” was meant | Convert the dose to the same unit as the concentration before dividing; 1 mg = 1,000 mcg |
| Reading units as milligrams | Syringe units measure volume, not mass; “40 units” is never “40 mg” | Treat the units column strictly as a plunger position for one specific solution |
| Assuming more water means less peptide | Water changes the volume a dose occupies, not the milligrams delivered | Remember the mg in the vial is fixed; water only sets how many units that mg spreads across |
| Treating a starting dose as a target | Several compounds (the GLP-1s) are titrated; the row shows only step one | Read the linked titration protocols for the documented multi-week schedule |
| Rounding awkward draws in your head | Odd vial sizes and half-units invite arithmetic slips | Use the calculator for anything off-chart instead of estimating |
Notice that four of the six mistakes trace back to one root cause: the units column is a computed answer for one exact pairing of vial and water, and it silently becomes wrong the moment either input changes. Internalise that and most chart-reading errors disappear.
Using the Chart Safely: Documented Research Starting Points
Everything above is presented as reference information for handling research compounds, and it is worth being explicit about the limits of that framing before you rely on any single number.
- These are documented starting points, not prescriptions. Each dose is the figure published on that peptide’s protocol page as the documented research starting amount. It is not a personal recommendation, not titrated to any individual, and not a substitute for a clinician’s judgment.
- The chart is valid only for the exact vial/BAC pairing shown. A different vial size or a different water volume changes the concentration and therefore the units. For anything off-chart, use the dosage calculator.
- Evidence quality varies enormously. The GLP-1 agonists (Semaglutide, Tirzepatide, Retatrutide) have substantial registered human-trial data behind their dosing frameworks. Most recovery, growth-hormone-axis, and longevity peptides on this chart rest on preclinical or early-stage evidence, and several have no approved human indication at all. Read efficacy claims for those compounds as preliminary.
- The full per-peptide context lives on the protocol pages. A one-row summary cannot convey titration schedules, cycling, timing, or contraindications. Follow the internal links to the individual guides in the catalog for the complete documented protocol before treating any row as actionable.
To make the evidence gradient explicit rather than leaving it as a caveat, here is how the categories on this chart sort by the strength of their human data. This is a framing aid, not a ranking of usefulness — a compound with limited human data can still have a clearly documented research protocol.
| Evidence tier | Categories / examples | How to read their figures |
|---|---|---|
| Substantial registered human-trial data | GLP-1 / dual & triple agonists (Semaglutide, Tirzepatide, Retatrutide) | Dosing frameworks are backed by formal trials; still titrated, still not a prescription here |
| Mixed / emerging human evidence | Some GH-axis secretagogues and metabolic compounds | Treat efficacy as provisional; documented figures are research starting points |
| Largely preclinical or early-stage | Most recovery, longevity and blend peptides (BPC-157, TB-500, Epithalon, KLOW, GLOW) | Read efficacy claims as preliminary; several have no approved human indication |
Bottom line: a chart tells you what a documented research dose converts to on your syringe. It does not tell you whether that compound, dose, or route is appropriate for a given person — that is a decision for a qualified professional, not a lookup table.
Quick Reference: All 20 Peptides, One Table
For readers who just want the whole thing in one scrollable grid, here is every row from the category tables consolidated and sorted by category. All figures computed as above.
| Category | Peptide | Vial | BAC | Concentration | Dose | Units (U-100) |
|---|---|---|---|---|---|---|
| Blends | KLOW | 80 mg | 3 mL | 26.67 mg/mL | 2,667 mcg | 10 |
| Blends | GLOW | 70 mg | 3 mL | 23.33 mg/mL | 2,330 mcg | 10 |
| Blends | BPC-157 + TB-500 | 10 mg | 3 mL | 3.33 mg/mL | 600 mcg | 18 |
| Blends | Ipamorelin + Tesamorelin | 10 mg | 3 mL | 3.33 mg/mL | 330 mcg | 10 |
| Recovery | BPC-157 | 5 mg | 3 mL | 1.67 mg/mL | 200 mcg | 12 |
| Recovery | TB-500 | 5 mg | 3 mL | 1.67 mg/mL | 500 mcg | 30 |
| Recovery/Skin | GHK-Cu | 50 mg | 3 mL | 16.67 mg/mL | 1 mg | 6 |
| Growth Hormone | Tesamorelin | 10 mg | 3 mL | 3.33 mg/mL | 2 mg | 60 |
| Growth Hormone | Ipamorelin | 5 mg | 3 mL | 1.67 mg/mL | 100 mcg | 6 |
| Growth Hormone | CJC-1295 DAC | 2 mg | 2 mL | 1.00 mg/mL | 300 mcg | 30 |
| Growth Hormone | Sermorelin | 5 mg | 3 mL | 1.67 mg/mL | 100 mcg | 6 |
| Metabolic/GLP-1 | Semaglutide | 5 mg | 2 mL | 2.50 mg/mL | 0.25 mg | 10 |
| Metabolic/GLP-1 | Tirzepatide | 5 mg | 2 mL | 2.50 mg/mL | 2.5 mg | 100 |
| Metabolic/GLP-1 | Retatrutide | 10 mg | 2 mL | 5.00 mg/mL | 2 mg | 40 |
| Metabolic | 5-Amino-1MQ | 10 mg | 3 mL | 3.33 mg/mL | 150 mcg | 4.5 |
| Longevity | MOTS-C | 10 mg | 3 mL | 3.33 mg/mL | 200 mcg | 6 |
| Longevity | Epithalon | 10 mg | 2 mL | 5.00 mg/mL | 5 mg | 100 |
| Longevity | NAD+ | 500 mg | 5 mL | 100.00 mg/mL | 50 mg | 50 |
| Sexual/Hormonal | PT-141 | 10 mg | 2 mL | 5.00 mg/mL | 1 mg | 20 |
| Sexual/Hormonal | Melanotan II | 10 mg | 2 mL | 5.00 mg/mL | 250 mcg | 5 |
A few patterns jump out once every peptide sits in one grid. The unit marks range from 4.5 (5-Amino-1MQ) all the way to 100 (Tirzepatide, Epithalon), a more than twenty-fold spread, yet every one of those numbers came from the identical three-step formula applied to two documented inputs. Concentrations run from a dilute 1.00 mg/mL (CJC-1295 DAC) to a dense 100 mg/mL (NAD+), and it is that concentration column — not the raw dose — that most often explains why two similar-looking doses land on very different marks. If you take one habit from this whole grid, let it be reading concentration and units together rather than either alone.
Every peptide in this grid has its own full documented protocol — timing, cycling, safety and the complete evidence picture — in the peptide dosage catalog. This chart is the index; the catalog is the library.
Frequently Asked Questions
Reading the Chart & Doing the Math
How do I calculate peptide dosage in units? Three steps. First, concentration = vial mg ÷ BAC mL. Second, draw volume = your dose ÷ concentration. Third, units = draw mL × 100. For a 10 mg vial in 2 mL dosed at 2 mg: 10÷2 = 5 mg/mL, 2÷5 = 0.4 mL, 0.4×100 = 40 units. For any vial or dose not on this chart, the dosage calculator does all three steps for you.
How many units of peptide is my dose? It depends on both the dose and the concentration, so there is no single answer without knowing your vial size and water volume. That is why every row of this chart lists concentration and units for one specific pairing. Copy a unit count only if your vial and BAC volume match the row exactly; otherwise recompute.
What is a U-100 syringe and why does it matter? A U-100 insulin syringe is calibrated so 100 units = 1 mL, meaning 1 unit = 0.01 mL. Almost every peptide dose here is measured on one. Because it measures volume rather than mass, the same peptide dose lands on different unit marks at different concentrations — see the syringe units guide.
What is the difference between mcg and mg on this chart? 1 mg = 1,000 mcg. Recovery and some growth-hormone peptides are dosed in micrograms (e.g. 100–500 mcg); GLP-1 and longevity compounds are often dosed in milligrams (e.g. 0.25–50 mg). Mixing them up is a thousand-fold error, so we keep each peptide in its protocol’s native unit and normalise only the computed columns.
Why does the same dose show a different unit mark for different peptides? Because the syringe measures volume. A dose in a concentrated solution occupies fewer millilitres (fewer units) than the same dose in a dilute solution. Ipamorelin’s 100 mcg at 1.67 mg/mL is 6 units; a 250 mcg Melanotan II dose at 5 mg/mL is only 5 units despite being a larger dose.
Reconstitution & Concentration
How does the amount of bacteriostatic water change my dose? It does not change the dose — it changes the volume that dose occupies. More water = weaker solution = larger draw (more units) for the same dose; less water = stronger solution = smaller draw. See the worked 5 mg-vial comparison above, and the full bacteriostatic water article.
Can I add more water to make a peptide easier to measure? Yes — this is a common technique for potent, small-dose peptides whose accurate draw would otherwise be an unmeasurable sliver near the zero mark. Adding water spreads the same dose across more units. It changes the unit math, not the milligrams delivered. The reconstitution guide explains how to add water without foaming or degrading the peptide.
Why is bacteriostatic water used instead of plain sterile water? Bacteriostatic water contains a small amount of benzyl alcohol as a preservative, which inhibits bacterial growth and allows a reconstituted multi-dose vial to be used over time rather than discarded after one draw. This is the standard reconstitution diluent referenced throughout the chart.
Are these concentrations exact? The concentrations are exact arithmetic from the documented vial-and-water pairing (vial mg ÷ BAC mL). The doses are the documented research starting points from each protocol page. What varies in the real world is your measurement precision — hence the emphasis on landing doses on readable unit marks.
My vial size is different from the chart — now what? The three-step formula still applies; just plug in your own numbers. Or skip the arithmetic entirely and enter your vial size, water volume and target dose into the interactive calculator, which returns concentration and units for your exact inputs.
Safety, Evidence & Scope
Are these doses prescriptions or recommendations? No. Every number is a documented research starting point — the figure used in the documented research protocol on that peptide’s page. This site is research-use-only. Nothing here is a prescription, a personal recommendation, or medical advice, and none of it substitutes for a qualified clinician.
How strong is the evidence behind these peptides? It varies widely. The GLP-1 and dual/triple-agonist compounds (Semaglutide, Tirzepatide, Retatrutide) have substantial registered human-trial data. Most recovery, growth-hormone-axis, and longevity peptides on this chart rest on preclinical or early human evidence, and several have no approved human indication. Treat efficacy claims for those as preliminary.
Is this chart a substitute for reading the individual protocol pages? No. A single row cannot capture titration, cycling, injection timing, contraindications or the evidence base. Use this chart as an index, then read the full documented protocol for each compound in the catalog before treating any figure as actionable.
Which peptides here are titrated rather than dosed at a flat amount? The GLP-1/metabolic compounds are the clearest examples — the “starting dose” row is just the first step of a documented step-up schedule. See the Semaglutide and Tirzepatide titration protocols for the full multi-week frameworks a chart cannot show.
Where do I go for exact numbers for my specific situation? The dosage calculator for concentration and unit math on any vial/dose, and the full catalog for the complete documented protocol behind every peptide in this chart. This page deliberately stops at documented starting points and the formula to read them.
References
- United States Pharmacopeia (USP), Bacteriostatic Water for Injection monograph — benzyl alcohol preservative.
- Manufacturer and diabetes-education references on the U-100 insulin syringe standard (100 units = 1 mL).
- Dosage Peptide protocol pages — the per-peptide documented research protocols (internal reference).
Research-use-only. This peptide dosage chart is provided strictly for educational and research reference. Every dose listed is a documented research starting point tied to a specific vial size and reconstitution volume — not a prescription, personal recommendation, or medical advice, and not a substitute for consultation with a qualified healthcare professional. The compounds referenced are not FDA-approved for the uses discussed unless otherwise stated, and the human evidence behind most of them is preliminary. Do not use this information to diagnose, treat, or self-administer.