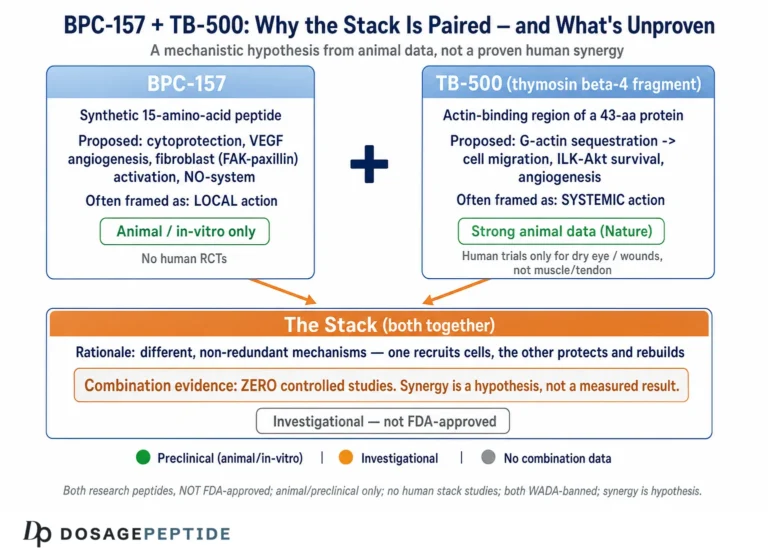
The BPC-157 + TB-500 blend is a two-peptide combination studied for soft-tissue repair, tendon and ligament recovery, and gut-lining integrity. It pairs BPC-157 (a synthetic 15-amino-acid fragment modeled on a protein found in gastric juice) with TB-500 (a synthetic fragment of the naturally occurring protein thymosin beta-4). Together they are the pairing most often called the “Wolverine stack” in recovery circles, and they are sold as a single 1:1 vial so the two are drawn and injected together.
The logic behind the pairing is that healing is rarely blocked by a single bottleneck. BPC-157 is studied for its effect on angiogenesis (the growth of new blood vessels that carry oxygen and nutrients into damaged tissue) and on the nitric-oxide pathway that governs local blood flow. TB-500, the active region of thymosin beta-4, is studied for its role in cell migration and actin regulation (actin is the internal scaffolding a cell uses to crawl into a wound and rebuild it). One compound is studied for improving the supply line; the other for helping repair cells move and reorganize. Stacking them targets two different rate-limiting steps at once.
Here is the honest evidence status up front, because it shapes everything that follows: the human data on this combination is essentially non-existent. The supportive research is overwhelmingly preclinical — rat and cell-culture studies of the individual peptides, not randomized human trials of the blend. There is no registered clinical trial of BPC-157 combined with TB-500. Everything below is framed as the documented research protocol used on our own product pages for research and reference purposes only. It is not a prescription, not medical advice, and not a promise of any outcome.

At a Glance
The table below is the fast reference. Every number in it is expanded, with the arithmetic shown, further down the page.
| Attribute | Details |
|---|---|
| Use (research context) | Soft-tissue, tendon, ligament and gut-lining repair; connective-tissue recovery |
| Typical vial | 10 mg blend vial or 20 mg blend vial (BPC-157 + TB-500, 1:1) |
| Reconstitution | 3 mL bacteriostatic water per vial (both sizes) |
| Per-dose (documented) | 10 mg vial: 600 mcg = 0.18 mL = 18 units | 20 mg vial: 250 mcg = ~0.0375 mL = ~4 units |
| Schedule | Once daily in the activation phase; tapering to 3-5x/week in maintenance |
| Onset / timeline | Research-framed: early biological activity within days; connective-tissue phases play out over 4-8 weeks |
| Common side effects (reported) | Injection-site redness/irritation, transient lightheadedness/flushing, mild fatigue, occasional nausea |
| Best stacked with | Studied alongside recovery-support compounds; the blend itself already combines the two main “bottleneck” peptides |
| Regulatory status | Research-use-only. Neither peptide is FDA-approved. Not for human consumption. |
What It Is / Composition
The product is a fixed-ratio blend of two research peptides combined in one vial at a 1:1 mass ratio. It is offered in two total masses: a 10 mg vial (5 mg BPC-157 + 5 mg TB-500) and a 20 mg vial (10 mg BPC-157 + 10 mg TB-500). Because the two peptides are pre-mixed, they cannot be dosed independently — every draw contains both in equal mass. That is by design: the protocol treats them as a single recovery unit rather than two separate injection schedules. For a plain-language breakdown of why the two are combined, see our overview of the BPC-157 + TB-500 recovery blend explained, and browse related protocols in the full dosage catalog.
| Component | Amount (10 mg vial / 20 mg vial) | Role in the blend (research context) |
|---|---|---|
| BPC-157 | 5 mg / 10 mg | Studied for angiogenesis (new blood-vessel growth) and nitric-oxide signaling — the “blood flow / supply line” arm. Also studied for gastrointestinal and tendon-to-bone healing. |
| TB-500 (thymosin beta-4 fragment) | 5 mg / 10 mg | Studied for cell migration and actin regulation — the “rebuild crew mobility” arm. Helps repair cells move into and reorganize damaged tissue in animal models. |
BPC-157 (body-protection compound 157) is a stable synthetic peptide derived from a sequence in human gastric juice. The bulk of its supportive literature comes from rodent injury models — Achilles tendon detachment, muscle and ligament transection, and gut lesions — where it has been associated with faster functional recovery. TB-500 is a synthetic version of the most biologically active fragment of thymosin beta-4, a protein present in nearly every cell type, that is studied for wound healing and tissue regeneration through its effect on the actin cytoskeleton. Neither is a hormone; neither builds muscle directly. Their studied value is in the repair environment.
How to Dose (the Research Protocol)
The dosing below reflects the documented starting protocol on our own product pages. It is expressed as total blend mass per dose (both peptides combined, since they share the vial). Read this as the research protocol we document, not as a recommendation for any person to inject anything.
| Vial | Documented research dose (total blend) | Frequency | Route |
|---|---|---|---|
| 10 mg blend vial | 600 mcg (0.6 mg) per dose | Once daily in activation; taper to 3-5x/week in maintenance | Subcutaneous |
| 20 mg blend vial | 250 mcg (0.25 mg) per dose | Once daily in activation; taper to 3-5x/week in maintenance | Subcutaneous |
The two vials carry different documented per-dose amounts (600 mcg vs 250 mcg). This is a deliberate feature of how each protocol page is built, not an inconsistency — the 20 mg vial’s more concentrated fill is documented at a smaller per-dose so a single vial stretches across a longer research window. Always follow the documented dose for the specific vial being referenced, and for anything user-specific, run the numbers through the dosage calculator rather than improvising.
Anchor logic: why the two are stacked
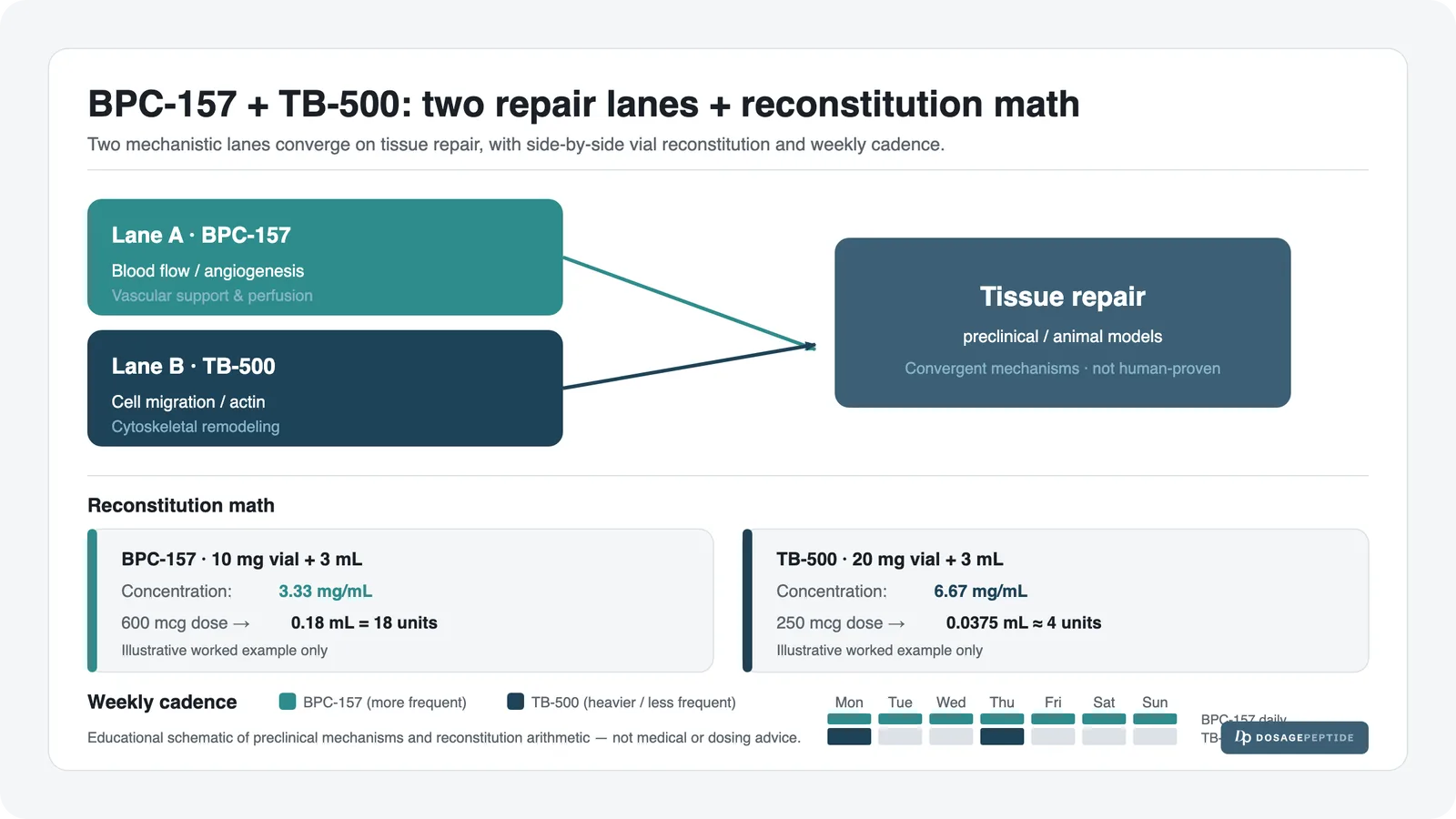
Think of tissue repair as a construction project with two independent bottlenecks. The first bottleneck is supply: damaged tissue needs fresh blood vessels to deliver oxygen, nutrients and repair signals. BPC-157 is the compound studied against that bottleneck — its association with angiogenesis and nitric-oxide signaling is the most-replicated finding in its literature. The second bottleneck is the crew: even with a good supply line, repair cells (fibroblasts, and others) have to physically migrate into the wound and rebuild the matrix. That migration depends on actin dynamics, which is exactly where TB-500 / thymosin beta-4 is studied.
Because these are two different rate-limiting steps, addressing only one leaves the other in place. In the individual-peptide research world, BPC-157 was often run more frequently (its shorter action favored daily or twice-daily dosing) while TB-500 was run heavier and less frequently (loading a few times per week). The blend collapses that split-dose logic into one vial: instead of managing two schedules, the fixed 1:1 mixture is injected on a single daily-to-several-times-weekly cadence. That trades a little dosing finesse for a lot of practical simplicity — which is why the blend exists.
Reconstitution & Draw (with the Real Math)
Reconstitution means adding sterile bacteriostatic water to the dried peptide so it becomes an injectable liquid. The three quantities that matter are the concentration (how much peptide is in each mL of liquid), the draw volume (how many mL equal one dose), and the syringe units (that draw volume read on a U-100 insulin syringe, where 1 mL = 100 units). Both vials are documented with 3 mL of bacteriostatic water. For the full walkthrough, see the peptide reconstitution guide and our insulin-syringe units guide. Here is the arithmetic worked all the way through.
10 mg vial
- Concentration: 10 mg ÷ 3 mL = 3.333 mg/mL (equivalently 3,333 mcg/mL)
- Dose in mg: 600 mcg = 0.6 mg
- Draw volume: 0.6 mg ÷ 3.333 mg/mL = 0.18 mL
- Syringe units: 0.18 mL × 100 = 18 units on a U-100 syringe
So on the 10 mg vial, one documented dose is a draw to the 18-unit mark. That 0.18 mL contains 300 mcg of BPC-157 and 300 mcg of TB-500 (half and half, because the blend is 1:1).
20 mg vial
- Concentration: 20 mg ÷ 3 mL = 6.667 mg/mL (equivalently 6,667 mcg/mL)
- Dose in mg: 250 mcg = 0.25 mg
- Draw volume: 0.25 mg ÷ 6.667 mg/mL = 0.0375 mL
- Syringe units: 0.0375 mL × 100 = 3.75 units ≈ 4 units on a U-100 syringe
On the 20 mg vial, one documented dose is a very small draw — about the 4-unit mark. That 0.0375 mL contains 125 mcg of BPC-157 and 125 mcg of TB-500. Because 4 units is such a tiny, hard-to-measure volume, this is exactly the situation where a U-100 (rather than a larger-barrel) syringe matters. If the marks are ambiguous, confirm before injecting rather than eyeballing.
Supply math (doses per vial)
- 10 mg vial: 10 mg ÷ 0.6 mg per dose ≈ 16 doses per vial.
- 20 mg vial: 20 mg ÷ 0.25 mg per dose = 80 doses per vial.
These figures show why the two vials are documented at different per-dose amounts: the 20 mg vial is set up to last far longer per vial. To convert either of these into a per-user schedule and cost, use the dosage calculator. This is a research reference, not a prescription — do not scale doses on independent math.
Weekly Schedule (Example Grid)
The grid below shows one example activation-phase week for the 10 mg vial at the documented 600 mcg (18-unit) dose. It is an illustration of the cadence the research protocol uses, not an instruction for anyone to dose themselves.
| Day | Dose (10 mg vial) | Timing | Draw |
|---|---|---|---|
| Monday | 600 mcg | Consistent daily slot (e.g. morning or evening) | 18 units |
| Tuesday | 600 mcg | Same slot | 18 units |
| Wednesday | 600 mcg | Same slot | 18 units |
| Thursday | 600 mcg | Same slot | 18 units |
| Friday | 600 mcg | Same slot | 18 units |
| Saturday | 600 mcg | Same slot | 18 units |
| Sunday | 600 mcg | Same slot | 18 units |
In maintenance, that grid thins out — the same 600 mcg dose is documented at roughly 3-5 days per week instead of 7 (see the cycling section). The one thing the research cadence prizes is consistency of timing rather than clock-precision: a fixed daily slot matters more than whether that slot is 8 a.m. or 8 p.m.
Dosing Phases & Cycling
The documented protocol runs in three overlapping ideas: an activation (loading) phase, a maintenance phase, and an on/off cycle. Again — this describes the research schedule, not a treatment plan for a person.
- Activation (roughly weeks 1-4): once-daily dosing at the documented per-vial amount. The goal in the research framing is to establish continuous exposure across the early, most active repair window.
- Taper / maintenance (roughly weeks 5-8+): the same per-dose amount is documented at a reduced frequency — commonly 3-5 times per week rather than daily — as the tissue moves from acute repair into remodeling.
- Cycle length: a typical documented cycle is 6-10 weeks on, followed by a break. The break allows a reassessment before deciding whether to run another block. There is no human trial defining an “optimal” cycle length for the blend; the 6-10 week figure is a practitioner-derived research convention, not a clinical endpoint.
Because the two peptides share a vial, one cannot be tapered while the other is held — the whole blend moves together through the phases. That is another reason the fixed-ratio product simplifies the classic BPC-157-frequent / TB-500-heavier split into a single ramp-up-then-taper curve.
Timeline: What to Expect
The table below maps the connective-tissue repair biology to what research (again, mostly animal research) has observed at each phase. These are research-framed observations, not personal-result promises. Individual biology, the nature of any injury, and countless other factors make timelines unpredictable, and none of this is a claim that any person will experience anything.
| Week / Phase | What’s happening (biology) | What is observed in research |
|---|---|---|
| Days 1-7 (early) | Inflammatory phase; local blood-flow and signaling changes begin | In animal models, early markers of angiogenesis and reduced lesion size appear within days of dosing |
| Weeks 2-3 | Proliferative phase; fibroblasts migrate in and lay down new matrix | Rodent tendon and muscle studies show accelerated functional recovery and improved tissue organization in this window |
| Weeks 4-6 | Matrix maturation; new tissue gains structure | Preclinical work associates the peptides with improved tendon-to-bone and myotendinous-junction healing at this stage |
| Weeks 6-10 (remodeling / maintenance) | Collagen remodels toward its final, stronger arrangement | Research framing shifts from acute repair to consolidation; maintenance dosing is documented here |
Stacking / Combinations
The blend is itself a stack — the entire point is that it already combines the two peptides addressing the two main repair bottlenecks (supply via BPC-157, cell mobility via TB-500). In research contexts it is sometimes discussed alongside broader recovery-support compounds, but the blend does not require anything added to it to serve its documented purpose.
The bottleneck logic is worth restating because it explains when stacking helps at all: adding a second compound only matters if it clears a different rate-limiting step than the ones already covered. Piling on another angiogenesis-type agent when BPC-157 is already present is redundant; the useful additions in a research protocol are ones that address a step the current blend does not touch. If a recovery process is stalling, the question is always “which bottleneck is still closed?” rather than “what else can be added?”
When Progress Stalls
If the documented protocol appears to plateau in a research setting, the troubleshooting ladder below walks from the most likely mundane cause to the least. It is a diagnostic sequence, not dosing advice.
| Bottleneck / symptom | Likely cause | Adjustment (research framing) |
|---|---|---|
| No change and dosing feels “off” | Reconstitution or draw error — wrong concentration or wrong units | Re-derive the math (mg/mL, mL, units) and confirm the syringe reading; re-check with the calculator |
| Inconsistent response | Irregular timing / missed days | Hold a fixed daily slot in the activation phase; consistency is prioritized over dose size |
| Peptide seems inactive | Degradation — heat, light, or an expired beyond-use window | Verify cold-chain storage and beyond-use date (see storage section); a degraded vial cannot be “fixed” by more volume |
| Plateau after weeks | Remodeling phase reached; acute repair signaling has done its work | The documented protocol tapers to maintenance rather than escalating dose |
Side Effects & Mitigation
The blend has no completed human safety trial, so the side-effect picture is drawn from user reports and the individual-peptide literature. The table lists what has been reported and the mitigation logic behind each.
| Issue | Why | Mitigation |
|---|---|---|
| Injection-site redness, itch or irritation | Local reaction to subcutaneous injection or to the injection technique | Rotate sites; use clean technique; allow the solution to reach room temperature before injecting |
| Transient lightheadedness or flushing | Possibly linked to BPC-157’s effect on the nitric-oxide / blood-flow pathway | Reports are usually brief and self-limiting; dosing the smaller documented amounts and staying seated after injecting are common precautions |
| Mild fatigue or “off” feeling | Non-specific; commonly reported early in a cycle | Typically settles; consistent timing and hydration are the usual mitigations noted |
| Occasional nausea | Non-specific tolerability | Generally mild and transient; persistence is a reason to stop and reassess |
| Long-term unknowns | No long-horizon human safety data exist for either peptide or the blend | Honesty is the mitigation: the absence of long-term data is itself a limitation to weigh |
Safety & Contraindications
- Neither BPC-157 nor TB-500 is FDA-approved for human use. Both are sold and studied as research chemicals. The blend is not for human consumption.
- There is no registered clinical trial of the BPC-157 + TB-500 combination, so no combination safety profile exists in humans.
- A history of cancer or active malignancy is frequently flagged in the literature as a reason for caution, because pathways involved in angiogenesis and cell migration are also relevant to tumor biology. This is a caution, not a settled finding — but it is a reason to involve a clinician.
- Pregnancy, breastfeeding, and minors: excluded — there is no safety data in these groups.
- Anyone on other medications, or with a chronic condition, should consult a licensed clinician before considering any research peptide.
- Sterile technique, sterile supplies, and correct reconstitution matter — see the dosage calculator for the math and our storage guide for handling.
Storage & Handling
Correct storage is what keeps a reconstituted peptide biologically intact; a degraded vial will not perform no matter how carefully it is dosed. Full detail is in our guide to storing peptides before and after reconstitution, and the essentials are:
- Before reconstitution: the lyophilized (freeze-dried) vial is the most stable form. Store cool and dark; many labs keep unreconstituted vials refrigerated or frozen.
- After reconstitution: refrigerate at 2-8°C (36-46°F). Do not leave the reconstituted vial at room temperature between doses.
- Protect from light and from heat; both accelerate peptide breakdown.
- Beyond-use window: a reconstituted vial is generally treated as usable for a limited number of weeks refrigerated — track the reconstitution date and discard past the beyond-use window rather than pushing an old vial.
- Freeze rules: do not repeatedly freeze and thaw a reconstituted solution; freeze-thaw cycling damages peptides. If long-term storage of a reconstituted vial is needed, a single freeze is preferable to cycling.
What the Evidence Actually Shows
This is the section to read slowly, because it is where the honesty lives. The evidence base for this blend is preclinical and indirect. Almost all of it comes from studies of the two peptides individually, in animals, not from trials of the combination in people.
For BPC-157, the most-cited work is a series of rat studies. Krivic and colleagues reported that the stable gastric pentadecapeptide BPC 157 improved healing after Achilles tendon detachment in rats (PMID 16583442), and a related study reported modulation of early functional recovery at the Achilles tendon-to-bone junction (PMID 18594781). Separate preclinical work examined BPC 157 as a therapy for disabled myotendinous junctions in rats (PMC8615275). A 2025 review by Jozwiak and colleagues surveys the peptide’s multifunctionality and possible medical applications (PMC11859134), and is a useful map of what has — and has not — been established. Every one of these is a preclinical or review paper; none is a human efficacy trial.
For TB-500 / thymosin beta-4, the supportive rationale is the well-documented role of thymosin beta-4 in actin regulation, cell migration and wound healing — again, largely from cell and animal models rather than human recovery trials.
And for the combination itself: ClinicalTrials.gov lists no registered BPC-157 + TB-500 combination trial. That is the evidence gap in one sentence. The pairing is biologically reasoned and widely used in research settings, but it has not been tested as a combination in a controlled human study. Treat every efficacy statement here as “studies suggest” or “in animal models,” never as established human benefit.
FAQ
Choosing
What is the “Wolverine stack”? It is the informal name for the BPC-157 + TB-500 combination, referencing the comic-book character’s rapid healing. In our catalog it is the fixed 1:1 blend vial. The name is marketing shorthand, not a medical descriptor.
Should the 10 mg or the 20 mg vial be referenced? The two are documented differently: the 10 mg vial at 600 mcg per dose (about 16 doses), the 20 mg vial at 250 mcg per dose (about 80 doses). The 20 mg vial is set up to last far longer per vial at a smaller documented per-dose. Which one applies depends on the protocol page being followed — always match the dose to the vial. Run the specifics through the dosage calculator.
Why are BPC-157 and TB-500 combined in the first place? Because they address two different bottlenecks in tissue repair: BPC-157 is studied for blood flow and angiogenesis (the supply line), TB-500 for cell migration and actin dynamics (the repair crew’s mobility). Clearing one bottleneck does nothing for the other, which is the rationale for stacking. Our recovery blend explainer covers this in depth.
Is this the same as buying BPC-157 and TB-500 separately? Chemically the peptides are the same, but the blend fixes them at a 1:1 ratio in one vial and one injection schedule. Buying them separately allows the classic split (BPC-157 more frequent, TB-500 heavier and less often); the blend trades that flexibility for a single simple cadence.
Which vial suits a shorter research window? The 10 mg vial, at ~16 documented doses, maps to a shorter block; the 20 mg vial, at ~80 documented doses, is built for a longer one. See the 10 mg protocol page and the 20 mg protocol page for the exact documented schedules.
Using It
What is the BPC-157 + TB-500 dosing schedule? The documented research protocol is once-daily dosing in the activation phase (roughly weeks 1-4), then the same per-dose amount at a reduced 3-5x/week frequency in maintenance. This is a research schedule, not a prescription.
How much of the 10 mg blend vial is one dose? 600 mcg. At 10 mg in 3 mL (3.333 mg/mL), that is 0.18 mL, which reads as 18 units on a U-100 syringe. The 0.18 mL contains 300 mcg of BPC-157 and 300 mcg of TB-500.
How much of the 20 mg blend vial is one dose? 250 mcg. At 20 mg in 3 mL (6.667 mg/mL), that is about 0.0375 mL, which reads as roughly 4 units on a U-100 syringe (125 mcg of each peptide). Because 4 units is such a small draw, use a U-100 syringe and confirm the mark before injecting.
How long should a BPC-157 + TB-500 cycle be? The documented convention is a 6-10 week block followed by a break, then reassessment. There is no human trial defining an optimal cycle length — the figure is a practitioner-derived research convention.
How long does BPC-157 + TB-500 take to work? No timeline can be promised for any person. In animal research, early angiogenic and lesion-reduction markers appear within days, with connective-tissue phases playing out over roughly 4-8 weeks. Treat that as research-framed biology, not a personal result.
Can the two peptides be co-injected — are they pH-compatible? In the blend they are already pre-mixed in one vial, so co-injection is the intended use and no separate mixing is needed. When the peptides are run separately, they are generally reported as compatible for combined subcutaneous use, but the blend removes that question entirely.
Practical & Safety
What are the reported side effects? Injection-site redness or irritation, transient lightheadedness or flushing, mild fatigue, and occasional nausea. These come from user reports and the individual-peptide literature, not a controlled human trial. Persistent effects are a reason to stop and reassess.
Is BPC-157 + TB-500 FDA-approved? No. Neither peptide is FDA-approved, and there is no registered trial of the combination. Everything here is research-use-only and not for human consumption.
How is the reconstituted blend stored? Refrigerate at 2-8°C, protect from light and heat, track the beyond-use window, and avoid freeze-thaw cycling. Full detail is in our storage guide.
Who should avoid it entirely? Anyone pregnant, breastfeeding, or under 18; anyone with a history of or active malignancy (given the angiogenesis and cell-migration pathways involved); and anyone who has not discussed research peptides with a licensed clinician. This is a research compound, not a treatment.
References
- Krivic A, et al. Achilles detachment in rat and stable gastric pentadecapeptide BPC 157. J Orthop Res, 2006. PMID 16583442.
- Krivic A, et al. Modulation of early functional recovery of Achilles tendon-to-bone by BPC 157. PMID 18594781.
- Jozwiak M, et al. Multifunctionality and Possible Medical Application of the BPC 157 Peptide. Pharmaceuticals, 2025. PMC11859134.
- Stable Gastric Pentadecapeptide BPC 157 as a Therapy for the Disable Myotendinous Junctions in Rats. PMC8615275.
- ClinicalTrials.gov registry search for BPC-157 + TB-500 combination — 0 registered studies (accessed 2026-07-06), documenting the evidence gap.
Disclaimer: This article is for research and educational purposes only. It is not medical advice, and nothing in it is a prescription or a personal recommendation. The dosing figures describe a documented research protocol, not a treatment. The products discussed are research-use-only, are not FDA-approved, and are not for human consumption. Peptide research carries real and partly unknown risks; consult a licensed clinician before making any health decision.