KLOW is an 80 mg four-peptide research blend studied as a single-vial convenience stack for skin quality, connective-tissue recovery, and inflammation modulation. It combines a copper-binding skin-remodeling peptide with three tissue-repair and anti-inflammatory peptides — bundling four compounds that researchers otherwise reconstitute and inject separately. In practice the vial contains GHK-Cu, BPC-157, TB-500, and KPV.
The problem KLOW is designed to address is fragmentation. Each of its four components targets a different bottleneck in the repair-and-remodel cascade: GHK-Cu drives extracellular-matrix remodeling and copper delivery, BPC-157 supports angiogenesis (new blood-vessel formation) and blood flow, TB-500 (a thymosin beta-4 fragment) promotes cell migration and actin regulation, and KPV is an anti-inflammatory tripeptide. Combining them into one blend means one reconstitution, one draw, and one injection instead of four — which is the entire practical appeal.
Honesty about evidence up front: there is no registered human clinical trial of the KLOW blend itself. The evidence base is largely preclinical (animal and cell) research on the individual components, supplemented by practitioner-derived protocols. Everything below documents the research protocol as published on our own protocol pages — it is research-use-only information, not a prescription or a personal recommendation.
This guide is organized so you can either read it end to end or jump to the number you need: the at-a-glance table first, then composition, the exact dosing protocol, the reconstitution math worked step by step, a weekly grid, the phased cycle, a research-framed timeline, stacking logic, troubleshooting, side effects, safety, storage, an honest read of the evidence, and a 15-question FAQ. Every figure traces back to our published KLOW protocol page and every dosing statement is research-use-only.

KLOW At a Glance
| Attribute | Detail (research protocol) |
|---|---|
| Use | Skin quality/remodeling + connective-tissue recovery + inflammation modulation (research) |
| Typical vial | 80 mg total (GHK-Cu 50 mg, BPC-157 10 mg, TB-500 10 mg, KPV 10 mg) |
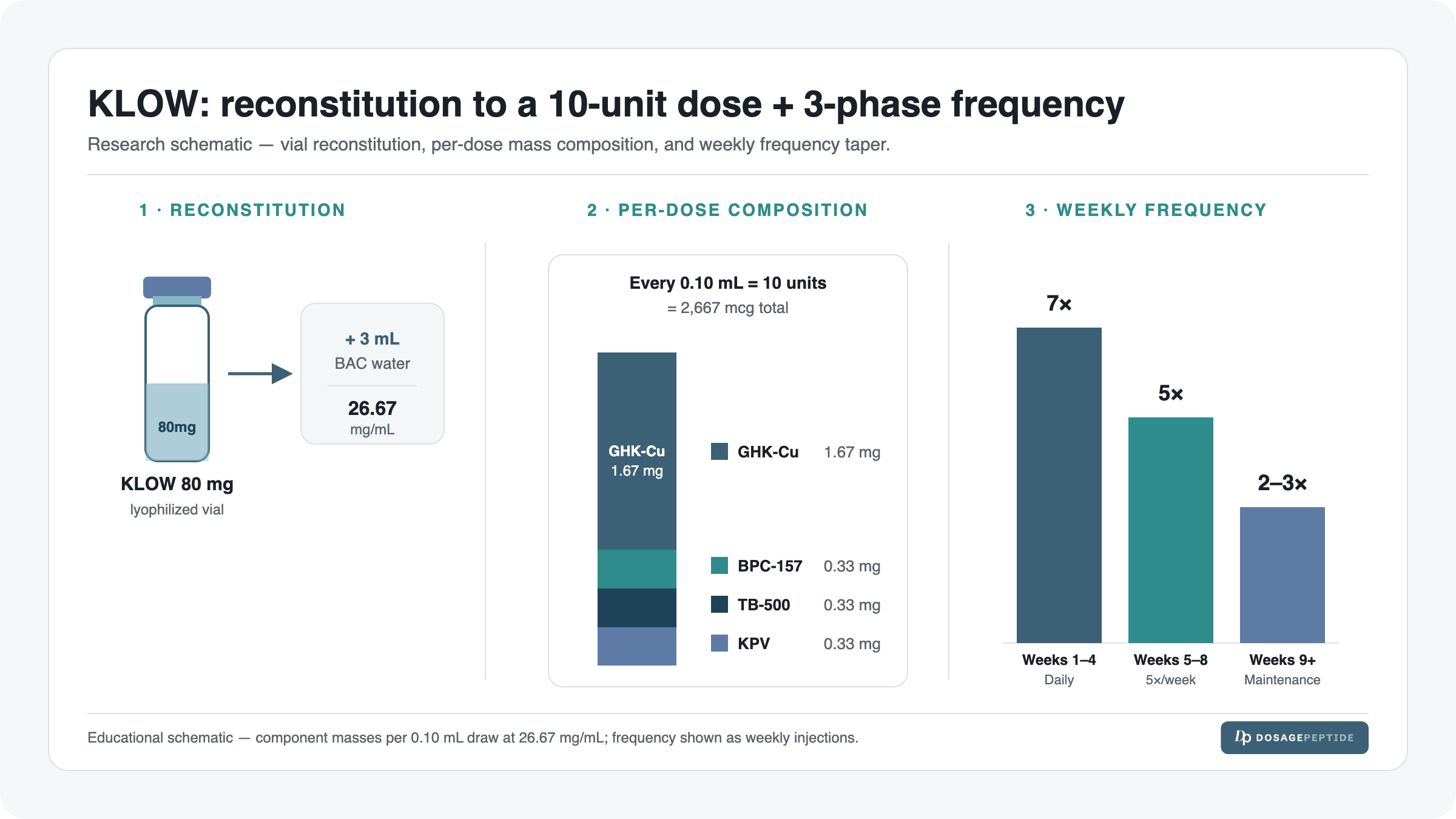
| Reconstitution | 3 mL bacteriostatic water → 26.67 mg/mL total blend |
| Per-dose | 2,667 mcg (~2.67 mg) total blend = 0.10 mL = 10 units on a U-100 syringe |
| Schedule | 3-phase: daily (wks 1–4) → 5×/week (wks 5–8) → 2–3×/week maintenance |
| Onset/timeline | Gradual; skin/recovery observations reported in component research over weeks, not days |
| Common side effects | Injection-site redness/itch, transient flushing, temporary taste/smell change (research reports) |
| Best stacked with | Usually run alone (it is already a 4-peptide stack); GH-axis or metabolic peptides added separately in research |
| Regulatory status | Not FDA-approved; research-use-only; not for human consumption |
What KLOW Is: Composition
KLOW is a fixed-ratio blend. A single 80 mg vial contains four distinct compounds, weighted heavily toward GHK-Cu as the anchor. For a deeper primer on the blend’s identity and rationale, see our explainer on what the KLOW peptide blend is, and for the outcomes literature see KLOW benefits: what research shows. You can also find it alongside every other protocol on our peptide dosage catalog.
| Component | Amount | Role in the blend |
|---|---|---|
| GHK-Cu (copper tripeptide-1) | 50 mg | The anchor. A copper-binding tripeptide studied for extracellular-matrix remodeling, collagen/elastin signaling, and antioxidant gene modulation in skin. Makes up ~62.5% of the vial by mass. |
| BPC-157 | 10 mg | A stable gastric pentadecapeptide studied for angiogenesis (new blood-vessel growth) and blood flow to healing tissue. The vascular/recovery lane. |
| TB-500 (thymosin beta-4 fragment) | 10 mg | Studied for cell migration and actin regulation — helping repair cells reach and organize at an injury site. The migration/remodeling lane. |
| KPV (Lys-Pro-Val) | 10 mg | An anti-inflammatory tripeptide derived from the C-terminus of α-MSH, studied for dampening inflammatory signaling. The calm-the-fire lane. |
The design logic is that skin and connective-tissue outcomes are rarely limited by one pathway. GHK-Cu can signal remodeling, but if inflammation is high (KPV’s target), blood flow is poor (BPC-157’s target), or repair cells cannot migrate (TB-500’s target), the remodeling signal has nothing to act on. KLOW bundles the four levers most often pulled together in research.
Why these four peptides, in this ratio
The 5:1:1:1 mass ratio (GHK-Cu 50 mg to 10 mg each of the other three) is not arbitrary. Read the four compounds as a small pipeline for tissue quality:
- GHK-Cu is the instruction set. In preclinical work it up- and down-regulates a large number of genes tied to matrix production, remodeling, and antioxidant defense, and it ferries copper — a cofactor for lysyl oxidase and superoxide dismutase — into tissue. It is the compound whose “dose” the blend is actually built around, which is why it takes the lion’s share of the vial.
- BPC-157 is the supply line. A remodeling signal is useless without perfusion. BPC-157 is studied for promoting angiogenesis and improving blood flow to healing tissue, effectively keeping the construction site fed with oxygen and nutrients.
- TB-500 is the logistics. As a thymosin beta-4 fragment it is studied for actin regulation and cell migration — helping fibroblasts and other repair cells physically reach and organize at the site that GHK-Cu is signaling to rebuild.
- KPV is the referee. Excess inflammation degrades the very matrix the other three are trying to build. KPV, the C-terminal tripeptide of α-MSH, is studied for damping pro-inflammatory signaling so remodeling can proceed on a calmer background.
None of these four is dosed to its own standalone research “sweet spot” inside KLOW — they are dosed to complement GHK-Cu at a single convenient injection volume. That is the fundamental compromise of any fixed blend, and understanding it is what separates informed research use from cargo-culting a protocol.
How to Dose KLOW (The Research Protocol)
The documented research protocol for the 80 mg KLOW vial uses a single fixed per-dose amount, then varies frequency across a cycle rather than changing the dose size. This is deliberate — see the anchor-compound logic below. All numbers here come directly from our KLOW 80 mg vial dosage protocol page and are documented for research purposes only.
| Compound | Research dose (per injection) | Frequency (by phase) | Route |
|---|---|---|---|
| KLOW total blend | 2,667 mcg (~2.67 mg) = 0.10 mL = 10 units | Daily → 5×/wk → 2–3×/wk (see phases) | Subcutaneous |
| — GHK-Cu portion | 1,667 mcg (~1.67 mg) | Same as blend (fixed ratio) | Subcutaneous |
| — BPC-157 portion | 333 mcg (~0.33 mg) | Same as blend (fixed ratio) | Subcutaneous |
| — TB-500 portion | 333 mcg (~0.33 mg) | Same as blend (fixed ratio) | Subcutaneous |
| — KPV portion | 333 mcg (~0.33 mg) | Same as blend (fixed ratio) | Subcutaneous |
Because KLOW is a fixed-ratio blend, you cannot dose one component without dosing all four in proportion. Every 0.10 mL draw delivers exactly the per-component amounts above. The four sub-amounts sum back to the total: 1,667 + 333 + 333 + 333 = 2,666 mcg, rounding to ~2,667 mcg. This is the single most important thing to understand about blend dosing: you dose the blend, and the components come along for the ride at their built-in ratio.
Anchor-compound logic: why the blend is set by GHK-Cu
KLOW’s fixed 0.10 mL dose is calibrated around GHK-Cu as the anchor compound. GHK-Cu is 62.5% of the vial by mass because skin-remodeling research typically uses it at the highest relative amount, and because — unlike the recovery peptides — its benefit in research tracks with consistency of exposure more than with any single large dose. So the protocol sets the dose to land GHK-Cu in a sensible daily range (~1.67 mg), and the three recovery/anti-inflammatory peptides ride along at their lower 0.33 mg each.
Put differently: if you tried to “anchor” the dose on BPC-157 or TB-500 instead (which are usually run at higher standalone amounts), you would have to inject a much larger volume and would flood GHK-Cu far past its useful range. Anchoring on GHK-Cu keeps all four components in reasonable research territory at one convenient 10-unit draw. That is the trade-off a skincare-anchored blend makes versus a recovery-anchored one: KLOW optimizes for the skin-remodeling compound and lets recovery peptides sit at supportive levels.
Skincare anchor vs recovery anchor — why it matters for who KLOW suits. A recovery-anchored blend (think a BPC-157/TB-500 “Wolverine” stack) sets its dose so the tendon-and-ligament peptides land in their studied range, and any skin peptide rides along as a bonus. KLOW inverts that. Its GHK-Cu anchor makes it a skin-and-connective-tissue-quality tool first, with the recovery peptides as supporting cast. So if the research goal is overwhelmingly acute tendon or ligament repair, a recovery-anchored blend may map better; if the goal is skin quality, collagen-adjacent remodeling, and general connective-tissue upkeep with a recovery tailwind, KLOW’s anchoring is the point. This is the single most useful decision heuristic in the whole guide: match the blend’s anchor to your primary research target.
Because the ratio is fixed, the only lever left in the KLOW protocol is frequency. You do not titrate the dose up and down the way you might with a standalone peptide; you titrate how often you inject the same 10 units. That is why the entire schedule below is expressed as a frequency curve — daily, then five times weekly, then two-to-three times weekly — rather than as a dose curve.
Reconstitution & Draw (With the Real Math)
Reconstitution is where most dosing errors happen, so we show every step. The KLOW protocol uses 3 mL of bacteriostatic water for the 80 mg vial. If you want the full walkthrough of the technique, read our peptide reconstitution guide and the primer on how much bacteriostatic water to use; to sanity-check any dose for your own vial use the dosage calculator.
Step 1 — Concentration (mg/mL)
Divide total peptide mass by the volume of bacteriostatic water added:
80 mg ÷ 3 mL = 26.67 mg/mL
That 26.67 mg/mL is the concentration of the total blend. Every millilitre you draw contains all four peptides at their fixed ratio.
Step 2 — Draw volume for the documented dose (mL)
Divide the target dose by the concentration. The documented starting dose is 2,667 mcg, which is 2.667 mg:
2.667 mg ÷ 26.67 mg/mL = 0.10 mL
Step 3 — Convert to insulin-syringe units
A U-100 insulin syringe reads 100 units per mL, so multiply the millilitres by 100:
0.10 mL × 100 = 10 units
So the documented KLOW dose is 0.10 mL = 10 units on a U-100 syringe. If you are unsure how the unit marks map to millilitres on your syringe, our insulin syringe units guide and the calculator walk it through; drawing to the 10-unit line is the whole task.
Step 4 — Vial supply math (doses per vial)
Total reconstituted volume divided by the per-dose volume tells you how many doses one vial holds:
3 mL ÷ 0.10 mL = 30 doses per vial
At the daily activation frequency, one 80 mg vial covers 30 days — roughly the four-week activation phase. That supply figure matters for planning a full cycle: an 8–12 week protocol that steps down in frequency will typically consume less than you would expect, because the maintenance phase uses far fewer doses per week.
Per-component check at 0.10 mL: each dose is 1/30th of the vial (0.10 mL of 3 mL). So GHK-Cu = 50 mg ÷ 30 = 1.67 mg; BPC-157 = 10 mg ÷ 30 = 0.33 mg; TB-500 = 10 mg ÷ 30 = 0.33 mg; KPV = 10 mg ÷ 30 = 0.33 mg. That is exactly the per-component breakdown in the dosing table — the math is internally consistent.
A note on the mixing itself (not just the math)
The arithmetic assumes a clean reconstitution. Two practical points that the numbers alone don’t capture:
- Add water slowly, down the vial wall. Do not squirt the bacteriostatic water directly onto the lyophilized powder. Aim the stream at the glass so it runs down gently — peptides are fragile, and shearing them with a hard jet or vigorous shaking can degrade them. Swirl, don’t shake; let it dissolve.
- Reconstituted volume is effectively the water you added. The dry peptide contributes negligible volume, so 3 mL of BAC water gives ~3 mL of solution and the 26.67 mg/mL figure holds. This is why “doses per vial” cleanly equals 3 mL ÷ 0.10 mL = 30.
If your vial size or water volume ever differs from this protocol, do not eyeball it — run the exact figures through the dosage calculator, which does the concentration → volume → units conversion for any inputs.
Weekly Schedule (Example Week)
The grid below shows one example week in each of the three phases. Every dose is the same 0.10 mL / 10 units; only the frequency changes across phases. Consistency of timing matters more than the exact hour — pick a slot and keep it.
| Phase | Mon | Tue | Wed | Thu | Fri | Sat | Sun |
|---|---|---|---|---|---|---|---|
| Activation (wks 1–4, daily) | 10u | 10u | 10u | 10u | 10u | 10u | 10u |
| Consolidation (wks 5–8, 5×/wk) | 10u | 10u | 10u | 10u | 10u | — | — |
| Maintenance (2–3×/wk) | 10u | — | 10u | — | 10u | — | — |
In research, KLOW is typically injected subcutaneously, rotating sites (abdomen, flank, thigh) to avoid repeated trauma at one spot. There is no strict food-timing requirement for KLOW the way there is for GH-axis peptides, so the practical rule is simply: same dose, same site-rotation habit, don’t skip.
Reading the grid across phases. The three rows are not three different weeks you run back to back — they are snapshots of what a representative week looks like in each phase. In weeks 1–4 every cell is filled (seven 10-unit doses). In weeks 5–8 two cells drop out (five doses). In maintenance only two or three cells remain. Notice what does not change down any column: the dose is always 10 units. The visual takeaway is that KLOW’s protocol is a fading frequency pattern laid over a flat dose line.
Site rotation, concretely. A simple rotation that prevents any one spot from being hit twice in a week is: left abdomen → right abdomen → left flank → right flank → left thigh → right thigh, then repeat. Pinch a fold of subcutaneous tissue, insert at the studied subcutaneous angle, and keep at least an inch of separation from a recent site. Repeated same-site injection is the most common self-inflicted cause of the injection-site irritation covered in the side-effects section below.
Dosing Phases & Cycling
The KLOW research protocol is built as three descending-frequency phases plus an on/off cycle. This is a research schedule, not a prescription. The logic is to front-load exposure while the tissue is remodeling, then taper to a maintenance rhythm that sustains the effect at a fraction of the vial cost.
- Phase 1 — Activation (weeks 1–4): daily, 10 units. Seven doses a week. This is the highest-consistency window, driving GHK-Cu exposure while BPC-157, TB-500, and KPV support blood flow, migration, and inflammation control. One vial ≈ 30 doses covers this phase.
- Phase 2 — Consolidation (weeks 5–8): 5×/week, 10 units. Two rest days a week. The remodeling signal is maintained but exposure eases, which also stretches vial supply.
- Phase 3 — Maintenance: 2–3×/week, 10 units. Enough to sustain the GHK-Cu-driven remodeling signal without daily injections. Many research protocols hold here for the remainder of a cycle.
On/off cycling: the documented pattern is 8–12 weeks on, then 4–8 weeks off. The off-window gives receptor and pathway signaling a reset and prevents open-ended, indefinite use. A common structure is 4 weeks activation + 4 weeks consolidation + 2–4 weeks maintenance ≈ a 10–12 week on-cycle, followed by a 4–8 week break before repeating. None of this is individualized medical advice — it is the documented research cadence.
Why the descending-frequency shape, not a flat schedule? The reasoning mirrors how tissue remodeling is thought to work. Early on, the tissue is being actively re-signaled and needs the most consistent exposure, so activation is daily. Once the remodeling program is running, the research rationale is that the signal can be sustained with less frequent reminders — hence the step down to five, then two-to-three times weekly. It is the same logic as a loading phase followed by a maintenance phase in many research protocols: front-load to establish, then hold with less.
Why bother with an off-cycle at all? Two reasons in the documented cadence. First, there is simply no component data supporting indefinite, continuous, year-round use — the honest position is that nobody has studied that, so the protocol builds in a stop. Second, a break is a natural checkpoint: it lets a researcher assess where things stand off-compound before deciding whether to re-run. The off-window is a feature of the protocol, not a gap in it.
Planning a full cycle against your vials. Do the supply arithmetic before you start so you are not caught short mid-activation. A 10–12 week on-cycle at the descending frequencies works out to roughly: activation ≈ 28 daily doses, consolidation ≈ 20 doses (5×/wk × 4 wks), and 2–4 maintenance weeks ≈ 6–12 doses — call it ~54–60 doses for the whole cycle, or about two 30-dose vials. Because each vial’s beyond-use window is finite, plan to open the second vial only when you reach it rather than reconstituting both up front.
Timeline: What to Expect
KLOW is a gradual, cumulative compound in research — not an instant one. The table frames what is happening biologically against what has been observed in research (on the individual components), deliberately avoiding any personal-result promise.
| Week / Phase | What’s happening (biology) | What is observed in research |
|---|---|---|
| Weeks 1–2 (early activation) | Copper delivery and initial signaling begin; BPC-157/TB-500 support perfusion and cell recruitment | Little visible change; injection-site tolerance established in reports |
| Weeks 3–4 (late activation) | Extracellular-matrix remodeling signaling ramps; inflammatory tone modulated by KPV | Preclinical GHK-Cu work reports collagen/matrix gene changes over this window |
| Weeks 5–8 (consolidation) | Sustained remodeling with reduced dosing frequency | Skin-quality and connective-tissue observations in component research accrue gradually, not abruptly |
| Weeks 9–12 (maintenance) | Signal held at 2–3×/week; pathway activity plateaus | Research treats this as a hold phase; effects are cumulative rather than escalating |
| Off-cycle (4–8 wks) | Signaling returns to baseline; pathway reset | No component data supports indefinite continuous use; the break is protocol-driven |
Every entry above reflects component-level preclinical research, not a KLOW-blend human trial. Observations are reported in study populations (usually animal or cell models), not guaranteed for any individual.
Setting honest expectations. The single most common source of disappointment with a compound like KLOW is expecting a fast, dramatic, visible change. The research picture is the opposite: slow, cumulative, and subtle, with the biology plausibly running weeks ahead of anything observable. The corollary is that the temptation to “increase the dose because nothing is happening yet” is exactly backwards — the protocol is built on consistency, and week 2 is not where you judge it. If a full documented cycle passes with no observed change in research conditions, that is information; escalating a fixed-ratio blend is not the documented response.
Stacking / Combinations
KLOW is unusual because it is already a four-peptide stack, so the most common “combination” question is really “do I need to add anything?” In research the answer is usually no for the skin-and-recovery use case — the blend covers four bottlenecks at once. The bottleneck logic that makes it self-contained:
- Inflammation bottleneck → KPV.
- Blood-flow bottleneck → BPC-157 (angiogenesis).
- Cell-migration bottleneck → TB-500.
- Remodeling-signal bottleneck → GHK-Cu (the anchor).
Where researchers do add compounds, they are usually pursuing a different axis entirely — for example a GH-axis or metabolic peptide for goals KLOW does not target. Those are run as separate protocols with their own reconstitution and schedule, not mixed into the KLOW draw. If you are deciding between KLOW and the other popular multi-peptide skin/recovery blends, our comparison of KLOW vs GLOW vs Wolverine blends lays out which bottlenecks each one prioritizes.
Don’t co-mingle blends in one syringe. Even when a second protocol is being run alongside KLOW in research, it is kept as a physically separate draw: its own reconstitution, its own concentration, its own units, its own site. Mixing two different peptide solutions in a single barrel muddies every calculation in this guide — you can no longer say what 10 units contains — and can raise compatibility questions that the fixed KLOW blend was specifically formulated to avoid. The whole appeal of KLOW is one clean draw; adding a second axis means a second clean draw, not a cocktail.
The honest default: run it alone. For the skin-and-connective-tissue-quality use case KLOW was built for, the research default is monotherapy — the blend already addresses inflammation, perfusion, migration, and remodeling. Reaching for additions usually signals that the actual goal has drifted to something KLOW does not target (fat loss, GH-axis effects, cognition), in which case the right move is a purpose-built protocol for that goal, not a heavier KLOW.
When Progress Stalls
A short troubleshooting ladder for the research protocol. The first move is almost never “increase the dose” — for an anchor like GHK-Cu, consistency beats magnitude. Because KLOW is a fixed-ratio blend, dose escalation is not even a clean lever: raising the volume raises all four peptides together and pushes GHK-Cu past its studied range without necessarily helping the others. So the ladder below adjusts frequency, technique, and adherence first, and only ever revisits the schedule — never invents a bigger dose. Work down it in order; most stalls resolve at the top of the ladder.
| Bottleneck | Likely cause | Adjustment (research protocol) |
|---|---|---|
| No change after 3–4 weeks | Missed doses / inconsistent activation phase | Tighten adherence to daily dosing before anything else — GHK-Cu benefit tracks consistency |
| Effect plateaus in maintenance | Frequency dropped too far, too soon | Step back up from 2×/wk to 3×/wk (dose size stays 10 units) |
| Injection-site irritation limiting adherence | Repeated same-site injection | Rotate sites (abdomen/flank/thigh); confirm proper reconstitution and BAC water |
| Uncertain the dose is right | Draw/units confusion | Re-verify with the calculator: 0.10 mL = 10 units at 26.67 mg/mL |
| Continuous use with fading response | No off-cycle taken | Take the documented 4–8 week off-window before re-running |
Side Effects & Mitigation
Reported effects come from the individual components’ research and practitioner reports; there is no adverse-event dataset for the KLOW blend specifically. Framed for research, not as a safety guarantee. Most reported issues are local and self-limiting; the mitigation column below is deliberately conservative, and the recurring theme is that technique and consistency solve more problems than dose changes. Anything that is severe, worsening, or systemic is a reason to stop and seek a clinician rather than to adjust the protocol.
| Issue | Why | Mitigation |
|---|---|---|
| Injection-site redness, itch, or welt | Local subcutaneous reaction; repeated same-site trauma | Rotate sites; ensure sterile technique and correct bacteriostatic water |
| Transient flushing / warmth | Vasoactive signaling (GHK-Cu copper delivery, BPC-157 perfusion) | Usually self-limiting; keep the fixed 10-unit dose rather than escalating |
| Temporary taste or smell changes | Reported anecdotally with copper-peptide exposure | Typically transient; note copper is the plausible driver (GHK-Cu is the anchor) |
| Fatigue or headache early in a cycle | Non-specific; reported in some peptide protocols | Maintain hydration; hold dose steady; reassess adherence |
| Lightheadedness at injection | Vasovagal response to injecting, not the peptide per se | Inject seated; standard needle-technique precautions |
Safety & Contraindications
Because there is no blend-level human safety dataset, the cautions below are extrapolated from the individual components’ known biology and the standard cautions applied across the peptide-research literature. They are framed conservatively for research use, not as a clinical clearance. When in doubt, the correct action is always to stop and consult a licensed clinician.
- Regulatory status: KLOW and its components are not FDA-approved for human use. The blend is sold and studied as research-use-only material; it is not for human consumption.
- No blend-level human data: there is no registered clinical trial of the KLOW blend, so its combined safety profile is not established in humans.
- Copper load: GHK-Cu delivers copper; anyone with copper-metabolism disorders (e.g., Wilson’s disease) is exactly the population that should avoid copper-peptide exposure in any research context.
- Cancer history / active malignancy: compounds that promote angiogenesis and cell migration (BPC-157, TB-500) are generally treated as contraindicated where uncontrolled cell growth is a concern — a standard caution across the recovery-peptide literature.
- Pregnancy / breastfeeding: no safety data; avoid.
- Immunosuppression or autoimmune conditions: KPV modulates inflammatory signaling; effects in these populations are unstudied.
- Drug interactions are unmapped. No formal interaction studies exist for the KLOW blend. Anyone already taking prescription medication should treat that as another reason to involve a clinician rather than assume compatibility.
- Sourcing and sterility. Research-grade material varies in purity; contamination or mis-labeled content is a real-world risk that no dosing table can protect against. This is a safety consideration independent of the protocol itself.
- Consult a licensed clinician before considering any peptide protocol. Nothing here substitutes for individualized medical advice.
Storage & Handling
Correct storage protects both potency and the beyond-use window. For the full walkthrough, see our guide on how to store peptides before and after reconstitution.
- Before reconstitution: store the lyophilized (freeze-dried) vial cold and dark. Long-term storage is typically in a freezer; short-term in the refrigerator.
- After reconstitution: refrigerate at 2–8 °C and protect from light — GHK-Cu’s copper complex is light-sensitive. Keep the vial upright.
- Beyond-use window: reconstituted peptide blends are generally used within a few weeks; discard if the solution becomes cloudy, discolored, or shows particulates.
- Freezing: do not freeze the reconstituted solution — freeze/thaw cycling can degrade the peptides. Freeze only the dry vial if long-term storage is needed.
- Bacteriostatic water (not sterile or plain water) is the correct diluent because its benzyl-alcohol preservative supports the multi-dose beyond-use window.
What the Evidence Actually Shows
Being precise here is what keeps this guide honest and useful. The evidence for KLOW is indirect: it rests on preclinical research into the individual components, not on the blend.
GHK-Cu has the strongest mechanistic literature of the four. Pickart and Margolina’s 2018 review in Int J Mol Sci catalogs its regenerative and protective actions — matrix remodeling, antioxidant and anti-inflammatory gene modulation, and wound-repair signaling — but this is a review of largely preclinical and cell-based work (PMC6073405). A 2015 paper on GHK as a natural modulator of skin-regeneration pathways similarly maps multiple cellular pathways, again in models rather than large human trials (PMC4508379).
BPC-157‘s evidence is dominated by rodent studies; a 2025 literature-and-patent review in Pharmaceuticals summarizes its multifunctional, mostly-preclinical profile (PMC11859134). TB-500 and KPV likewise rest on animal and cell research for migration/repair and anti-inflammatory activity respectively — mechanistically plausible, but not validated in humans as part of this blend.
Critically: there is no registered clinical trial of the KLOW blend on ClinicalTrials.gov. No human randomized controlled trial has tested these four peptides together at this ratio. So while the component science is real, any claim about the blend’s combined human efficacy is an extrapolation. That evidence gap is not a footnote — it is the honest headline. Treat KLOW as an investigational research protocol, not a validated therapy.
What “the evidence is preclinical” actually means for a reader
Preclinical means the findings come from cell cultures and animal models, not from controlled human trials. That distinction carries three practical caveats worth stating plainly:
- Dose translation is not one-to-one. A dose that produces an effect in a mouse does not scale linearly to a human by body weight, and the research doses in this protocol are practitioner-derived conventions, not figures validated against human outcomes.
- Mechanism is not the same as outcome. “GHK-Cu modulates matrix genes in a model” is a mechanistic finding. It suggests a plausible pathway; it does not prove a visible, durable human result. This guide deliberately reports mechanisms as mechanisms.
- The blend is untested as a blend. Even if each component’s individual literature were airtight, combining four peptides can produce interactions — additive, competitive, or neutral — that no one has measured for this specific formulation.
That is why every efficacy statement here is hedged with “studied for,” “in research,” or “preclinical.” It is not lawyerly throat-clearing; it is an accurate description of where the science stands. A guide that promised results would be less honest and, for a YMYL topic, less trustworthy.
Where the component evidence is strongest and weakest
GHK-Cu is the best-characterized of the four, with a substantial mechanistic and topical-skincare literature behind it — which makes it a reasonable anchor to build a blend around. BPC-157 has a large but overwhelmingly rodent-based body of work. TB-500 and KPV are the thinnest, resting on smaller sets of animal and cell studies for migration/repair and anti-inflammatory activity respectively. So even within KLOW, the evidence is uneven: strongest for the anchor, progressively more speculative for the supporting peptides. An honest reader weights their expectations accordingly.
Frequently Asked Questions
Choosing KLOW
What is the KLOW peptide dosage? The documented research protocol uses a fixed 2,667 mcg (~2.67 mg) total-blend dose = 0.10 mL = 10 units on a U-100 syringe, from an 80 mg vial reconstituted with 3 mL of bacteriostatic water (26.67 mg/mL). Frequency changes across the cycle, not the dose size.
Is there a KLOW peptide dosage and frequency chart? Yes — see the three-phase weekly schedule grid above: daily 10 units in weeks 1–4, 5×/week in weeks 5–8, then 2–3×/week for maintenance. Every entry is the same 10-unit dose.
What is actually in a KLOW vial? One 80 mg vial contains GHK-Cu 50 mg, BPC-157 10 mg, TB-500 10 mg, and KPV 10 mg — a copper-remodeling anchor plus three recovery/anti-inflammatory peptides.
How is KLOW different from GLOW or the Wolverine stack? Different bottleneck priorities and ratios. Our KLOW vs GLOW vs Wolverine comparison breaks down which pathways each blend emphasizes; KLOW’s distinguishing feature is its heavy GHK-Cu anchor plus KPV for inflammation, which tilts it toward skin remodeling rather than pure tendon/ligament recovery.
Using it
How do I reconstitute KLOW? Add 3 mL of bacteriostatic water to the 80 mg vial for a 26.67 mg/mL solution. Full technique is in the reconstitution guide. The documented dose then draws to 0.10 mL / 10 units.
How do I dose KLOW — what’s the draw? 2.667 mg ÷ 26.67 mg/mL = 0.10 mL, and 0.10 mL × 100 = 10 units. Draw to the 10-unit line on a U-100 insulin syringe. Verify with the dosage calculator if unsure.
How often should I use KLOW? In the documented protocol, daily during the 4-week activation phase, then 5×/week for weeks 5–8, then 2–3×/week for maintenance. Frequency steps down; the 10-unit dose stays constant.
What is the KLOW cycle length? The documented cycle is 8–12 weeks on, then 4–8 weeks off. The off-window is part of the protocol — continuous indefinite use is not supported by the component research.
Why does daily consistency matter more than dose size for KLOW? Because GHK-Cu, the anchor, shows benefit in research that tracks with steady, repeated exposure rather than with any single large dose. Larger doses do not “make up for” missed days; the protocol therefore front-loads frequency and holds the dose fixed.
What does each component work out to per dose? At 0.10 mL (1/30th of the vial): GHK-Cu ~1.67 mg, BPC-157 ~0.33 mg, TB-500 ~0.33 mg, KPV ~0.33 mg — summing to the ~2.67 mg total.
Practical & safety
How many doses are in one KLOW vial? 3 mL ÷ 0.10 mL = 30 doses. At daily activation that is ~30 days; the later step-down phases stretch a vial much further.
How should I store KLOW after reconstitution? Refrigerate at 2–8 °C, protect from light (the copper complex is light-sensitive), keep upright, and do not freeze the reconstituted solution. Discard if cloudy or discolored.
How long until KLOW is expected to show changes in research? It is gradual and cumulative — component studies report matrix/skin changes over weeks, not days. Research suggests a slow build across the activation and consolidation phases rather than an overnight effect. Observations are research-framed, not personal-result guarantees.
Is KLOW FDA-approved or safe for humans? No. KLOW is not FDA-approved, has no registered human trial as a blend, and is research-use-only material — not for human consumption. Anyone with copper-metabolism disorders, active malignancy, or during pregnancy/breastfeeding should avoid it, and everyone should consult a licensed clinician first. The absence of blend-level human data is not a technicality to route around — it is the central fact about KLOW’s status.
Can KLOW be injected at any time of day? There is no strict food or time-of-day requirement like GH-axis peptides have. In the documented protocol a consistent daily slot is chosen, sites are rotated, and the schedule is kept — consistency is the goal.
References
- Pickart L, Margolina A. Regenerative and Protective Actions of the GHK-Cu Peptide. Int J Mol Sci, 2018. PMC6073405.
- GHK Peptide as a Natural Modulator of Multiple Cellular Pathways in Skin Regeneration, 2015. PMC4508379.
- Jozwiak M, et al. BPC-157 literature and patent review. Pharmaceuticals, 2025. PMC11859134.
- ClinicalTrials.gov — search for the KLOW blend (GHK-Cu + BPC-157 + TB-500 + KPV) returns no registered clinical trial (evidence-gap note; searched July 2026).
Disclaimer: This article is provided for research and informational purposes only. It is not medical advice and does not establish a doctor–patient relationship. KLOW and its component peptides are research-use-only materials, are not FDA-approved, and are not intended for human consumption. All dosing described here documents a research protocol, not a prescription or personal recommendation. Consult a licensed clinician before considering any peptide compound.