Ipamorelin is one of the most talked-about growth-hormone (GH) peptides in the research community, and for a simple reason: it is engineered to be clean. Where older GH-releasing peptides tend to drag cortisol, prolactin and hunger signaling along with the GH pulse they trigger, Ipamorelin is a highly selective molecule that, in the published literature, releases growth hormone with strikingly little of that off-target noise. For anyone studying how to raise GH output in a controlled, pulsatile way, it has become a reference compound.
This guide is the complete, research-framed protocol: exactly how the 5 mg and 10 mg vials are reconstituted, the arithmetic that turns a documented 100 mcg dose into a mark on an insulin syringe, when the dose is administered (and why timing matters so much for a GH peptide), how the weekly schedule is typically laid out, how cycling is framed, and what the research-observed timeline looks like. Everything below describes a documented research protocol, not a prescription or a personal recommendation.
One honest sentence up front, because it governs everything that follows: Ipamorelin is not an FDA-approved drug, its human clinical record is limited, and much of what is presented as an “expected” outcome comes from preclinical work and early characterization studies rather than large, long-term human trials. Treat the numbers here as the documented research starting points they are, and read the safety section before the rest.

Ipamorelin at a Glance
| Attribute | Detail |
|---|---|
| Compound class | Pentapeptide; selective growth-hormone secretagogue (GHRP) |
| Mechanism | Selective ghrelin / GHSR-1a receptor agonist at the pituitary |
| Signature feature | Clean, pulsatile GH release with minimal cortisol or prolactin |
| Common vial sizes | 5 mg and 10 mg lyophilized powder |
| Documented reconstitution | 3 mL bacteriostatic water per vial (both sizes) |
| Concentration (5 mg vial) | 1.67 mg/mL |
| Concentration (10 mg vial) | 3.33 mg/mL |
| Documented starting dose | 100 mcg per dose |
| 100 mcg on a U-100 syringe | 6 units (5 mg vial) or 3 units (10 mg vial) |
| Typical frequency | 1–3× per day, empty stomach (fasted AM and/or pre-bed) |
| Route | Subcutaneous injection |
| Often paired with | A GHRH analog (CJC-1295 or Tesamorelin) for synergy |
| Regulatory status | Not FDA-approved; no approved human indication; research-use-only |
What Ipamorelin Is and How It Works
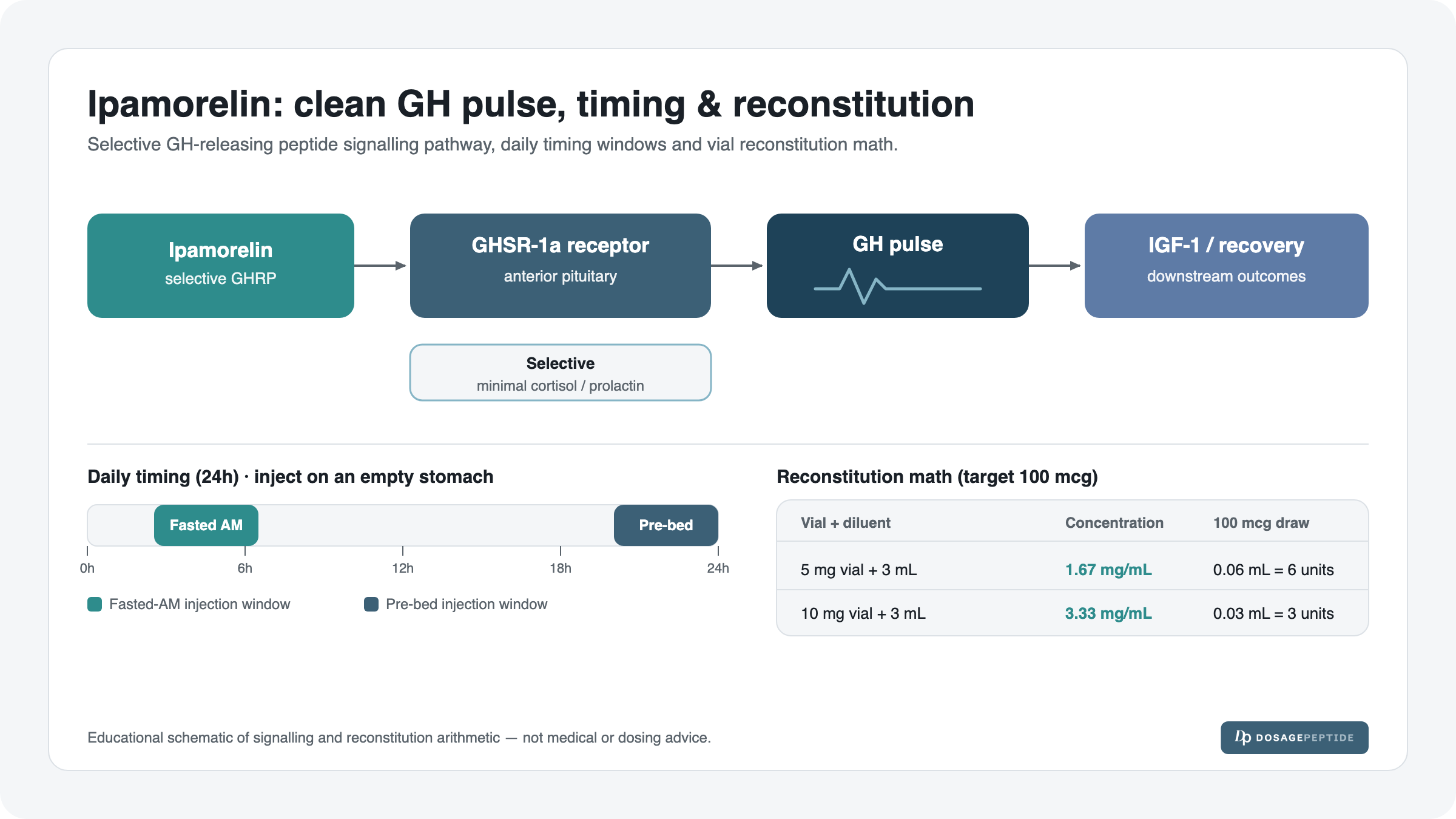
Ipamorelin is a pentapeptide — a chain of five amino acids — that belongs to the family of growth-hormone-releasing peptides (GHRPs). In plain English, it is a molecule that tells the pituitary gland to release a burst of growth hormone. It does this by acting as a selective agonist at the GHSR-1a receptor, the same receptor that the hunger hormone ghrelin normally activates.
The word that matters most is selective. Earlier secretagogues such as GHRP-6 and GHRP-2 do trigger GH release, but they also switch on other pathways: they can raise cortisol (a stress hormone), raise prolactin, and drive a strong hunger response. In the foundational characterization work by Raun and colleagues, Ipamorelin was described as the first GHRP to release growth hormone with a potency and specificity comparable to GHRP-6 but without the accompanying cortisol and prolactin rise. That “clean pulse” is the reason it remains a reference compound in GH-peptide research.
The downstream logic follows the body’s own GH axis. A GH pulse from the pituitary travels to the liver and peripheral tissues, where it drives the production of IGF-1 (insulin-like growth factor 1), the mediator responsible for most of GH’s anabolic and recovery-related effects. Because Ipamorelin works with the pituitary’s pulsatile machinery rather than replacing GH directly, the pulse it produces is shaped like a natural pulse — it rises and then clears, rather than sitting at a flat, elevated level.
Mechanistic reviews of ghrelin/GHSR-1a signaling frame Ipamorelin as a receptor agonist that harnesses the body’s own release machinery. This is a mechanism-level description of a research compound, not a statement of proven clinical benefit in humans.
Why “clean” matters for a dosing protocol
The selectivity is not just a talking point — it shapes how the compound is dosed. Because Ipamorelin does not meaningfully spike cortisol or prolactin at documented research doses, the protocol tends to emphasize pulse timing (getting the GH burst to land at a useful moment, such as during early sleep) rather than aggressive dose escalation. The goal in the research framing is a well-placed, physiological pulse, not the largest possible dose.
Reconstitution: The Arithmetic Behind Every Dose
Ipamorelin ships as a lyophilized (freeze-dried) powder. Before anything can be measured, the powder is dissolved in bacteriostatic water — sterile water with a small amount of benzyl alcohol that lets a multi-dose vial stay usable over its shelf life. The documented protocol for both vial sizes uses 3 mL of bacteriostatic water. For the underlying technique — how to add the diluent slowly down the vial wall, why you never shake it, and how to store the solution afterward — see the full peptide reconstitution guide and the companion note on how much bacteriostatic water to use.
The entire conversion rests on three small equations. Learn them once and every peptide dose becomes arithmetic instead of guesswork:
- Step 1 — Concentration: vial mg ÷ BAC water mL = mg/mL
- Step 2 — Draw volume: dose (mg) ÷ concentration (mg/mL) = mL to draw
- Step 3 — Syringe units: mL to draw × 100 = units on a U-100 insulin syringe
That last step works because a U-100 insulin syringe is standardized so that 100 units = 1 mL, which means 1 unit = 0.01 mL. If reading those tick marks is unfamiliar, the insulin syringe units guide walks through it visually.
The 5 mg vial (+ 3 mL bacteriostatic water)
Worked out step by step at the documented 100 mcg dose (remember 100 mcg = 0.1 mg):
- Concentration: 5 mg ÷ 3 mL = 1.67 mg/mL
- Draw volume: 0.1 mg ÷ 1.67 mg/mL = 0.06 mL
- Units: 0.06 mL × 100 = 6 units
The 10 mg vial (+ 3 mL bacteriostatic water)
Same diluent volume, double the powder, so the solution is twice as concentrated and the same dose occupies half the volume:
- Concentration: 10 mg ÷ 3 mL = 3.33 mg/mL
- Draw volume: 0.1 mg ÷ 3.33 mg/mL = 0.03 mL
- Units: 0.03 mL × 100 = 3 units
This is the single most important thing to internalize: the same 100 mcg dose is 6 units from a 5 mg vial but only 3 units from a 10 mg vial. The dose in micrograms is identical; the number of units on the syringe is not, because the vials are reconstituted to different concentrations. Confusing the two is the most common way to under- or over-draw.
| Vial | BAC water | Concentration | Documented dose | Draw volume | Units (U-100) |
|---|---|---|---|---|---|
| 5 mg | 3 mL | 1.67 mg/mL | 100 mcg | 0.06 mL | 6 units |
| 10 mg | 3 mL | 3.33 mg/mL | 100 mcg | 0.03 mL | 3 units |
The two documented vial protocols each have their own dedicated page — the Ipamorelin 5 mg vial dosage protocol and the Ipamorelin 10 mg vial dosage protocol. If you are working with a different vial strength or a different diluent volume than the documented 3 mL, do not try to eyeball it — run the numbers through the interactive dosage calculator, which does all three steps for any combination and shows the exact unit mark.
Composition and Physical Properties
| Property | 5 mg vial | 10 mg vial |
|---|---|---|
| Active peptide | Ipamorelin (pentapeptide) | Ipamorelin (pentapeptide) |
| Form as supplied | Lyophilized powder | Lyophilized powder |
| Total peptide per vial | 5 mg (5,000 mcg) | 10 mg (10,000 mcg) |
| Documented diluent | 3 mL bacteriostatic water | 3 mL bacteriostatic water |
| Resulting concentration | 1.67 mg/mL | 3.33 mg/mL |
| Doses per vial at 100 mcg | ~50 doses | ~100 doses |
| Storage (reconstituted) | Refrigerated, protected from light; discard per shelf-life guidance | |
At the documented 100 mcg per dose, a 5 mg vial holds roughly fifty doses and a 10 mg vial roughly one hundred. That doses-per-vial math is worth knowing before you plan a cycle, because reconstituted peptide has a finite shelf life once mixed — a vial that outlasts its stability window is wasted regardless of how much powder remains.
Documented Dosing: How Much, How Often
The documented research starting point is 100 mcg per dose. Frequency in the research framing runs from once to three times per day, and this is where the compound’s pharmacology does the talking: Ipamorelin produces a relatively short GH pulse, so a single daily dose places one pulse while two or three daily doses place multiple pulses across the day. The trade-off is more injections and faster vial turnover against more frequent pulses.
| Frequency | Dose each | Daily total | Research framing |
|---|---|---|---|
| 1× / day | 100 mcg | 100 mcg | Simplest schedule; the single pulse is usually placed pre-bed |
| 2× / day | 100 mcg | 200 mcg | Fasted AM + pre-bed; two pulses across the day |
| 3× / day | 100 mcg | 300 mcg | AM + midday + pre-bed; each dose still on an empty stomach |
Two rules hold across all three rows. First, the per-dose amount stays at the documented 100 mcg — the way the protocol scales is by adding pulses, not by inflating a single injection. Second, every dose is taken on an empty stomach, which the next section explains in detail. The “right” frequency is not something this guide can prescribe; it is a documented range, and the research literature has not established an optimal daily frequency for any human goal.
Timing: Why Empty Stomach and Pre-Bed Matter
Timing is not a nice-to-have with Ipamorelin — it is arguably the single biggest lever in the protocol, and it comes down to one piece of physiology: a rise in blood glucose and insulin blunts GH secretion. Eating, and especially eating carbohydrates, raises insulin, and elevated insulin suppresses the very GH pulse the protocol is trying to create. Inject right after a meal and much of the pulse can be wasted.
That is why the documented practice is to dose on an empty stomach — a common rule of thumb in the research framing is a fasted window before and after the injection, with no food or caloric drinks in that window. Two timing anchors dominate:
- Pre-bed: The body’s largest natural GH pulse occurs during early deep sleep. A pre-bed dose is timed to reinforce that natural nocturnal pulse, which is why the pre-bed slot is the one most consistently kept even in a once-daily schedule. It is taken a short while after the last meal, once the stomach is empty.
- Fasted AM: First thing in the morning, before eating, insulin is naturally low — a clean window for a second pulse in a twice-daily schedule.
| Slot | When | Why it is used | Food rule |
|---|---|---|---|
| Fasted AM | On waking, before breakfast | Low morning insulin; clean pulse window | No food before/after the fasted window |
| Midday (3×/day only) | Between meals, fasted | Adds a third daytime pulse | Away from meals on both sides |
| Pre-bed | After the stomach has emptied post-dinner | Reinforces the natural nocturnal GH pulse | No late carbohydrate snack near the dose |
The practical takeaway: it is not just how much Ipamorelin is administered but when — and specifically how far from food and insulin — that shapes the size of the GH pulse in the research framing.
A Weekly Schedule Grid
Two dosing patterns dominate the research framing: a continuous 7-day pattern (dose every day) and a 5-on / 2-off pattern (dose Monday through Friday, rest the weekend). The 5-on/2-off idea borrows from GH-therapy practice, where periodic breaks are used with the aim of limiting receptor down-regulation; whether it offers any advantage for Ipamorelin specifically has not been established in human trials, so it is presented as a documented option, not a proven-superior method.
The grid below lays out a twice-daily (fasted AM + pre-bed) example so the two patterns are easy to compare across the week:
| Slot | Mon | Tue | Wed | Thu | Fri | Sat | Sun |
|---|---|---|---|---|---|---|---|
| Continuous — AM (fasted) | 100 mcg | 100 mcg | 100 mcg | 100 mcg | 100 mcg | 100 mcg | 100 mcg |
| Continuous — Pre-bed | 100 mcg | 100 mcg | 100 mcg | 100 mcg | 100 mcg | 100 mcg | 100 mcg |
| 5-on/2-off — AM (fasted) | 100 mcg | 100 mcg | 100 mcg | 100 mcg | 100 mcg | — | — |
| 5-on/2-off — Pre-bed | 100 mcg | 100 mcg | 100 mcg | 100 mcg | 100 mcg | — | — |
On the continuous twice-daily pattern, a full week is 14 doses × 100 mcg = 1,400 mcg (1.4 mg). On 5-on/2-off it is 10 doses = 1,000 mcg (1.0 mg). Cross-referenced against the doses-per-vial table above, that tells you how long a vial lasts and when to reconstitute a fresh one before your current solution ages out.
Cycling: Length and Structure
Ipamorelin is generally discussed as a cycled compound rather than something run indefinitely. In the research framing, a cycle runs for a defined block of weeks followed by a break, with the rationale that the GH axis responds better to a stimulus that is not permanently present. The published human evidence does not define an optimal cycle length for Ipamorelin, so the ranges below are documented conventions, not established facts.
| Cycle element | Documented framing |
|---|---|
| Typical cycle length | A defined multi-week block (commonly discussed in the range of roughly 8–12 weeks) |
| Break between cycles | An off period before repeating, to limit receptor down-regulation |
| Within-week pattern | Continuous daily, or 5-on / 2-off |
| Dose across the cycle | Held at the documented 100 mcg per dose; scaled by frequency, not by inflating the dose |
The consistent theme is restraint: hold the per-dose amount steady, use frequency and cycle structure as the adjustable variables, and build in breaks. None of this substitutes for guidance from a qualified professional, and none of it is a recommendation to run any particular cycle.
Why Ipamorelin Is Often Paired With a GHRH Analog
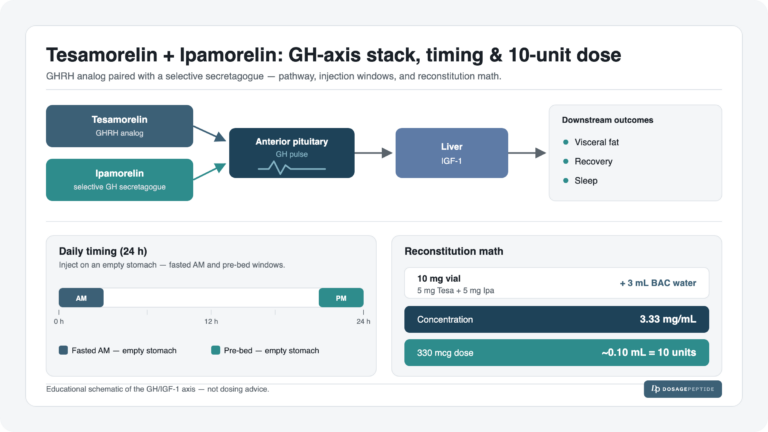
Ipamorelin rarely appears alone in the stacking literature. The most common companion is a GHRH analog — either CJC-1295 or Tesamorelin. The reason is a genuine physiological synergy, and it is worth understanding because it is the single most-repeated pairing in GH-peptide research.
The pituitary responds to two different signals. A GHRH analog (like CJC-1295 or Tesamorelin) tells the pituitary to make and get ready to release more GH — it primes the tank. A secretagogue like Ipamorelin acts on the GHSR-1a receptor to trigger the release and, at the same time, suppresses somatostatin, the brake that normally limits GH output. Combine the two and you have one compound filling the tank and easing off the brake while the other opens the valve. In research models this produces a larger, cleaner GH pulse than either compound alone.
| Role | Compound | What it does |
|---|---|---|
| GHRH analog | CJC-1295 or Tesamorelin | Primes and increases GH available for release |
| Secretagogue (GHRP) | Ipamorelin | Triggers the pulse; eases the somatostatin brake |
The best-known documented version of this pairing on our catalog is the Tesamorelin + Ipamorelin dosage protocol, where the two are run together as a blend. If you plan to study the pairing, start with that protocol page for the documented blend numbers rather than improvising a combination.
Research-Observed Timeline
Because Ipamorelin works through the body’s own GH axis, effects reported in the research and practitioner literature tend to unfold in phases rather than appearing all at once. The timeline below is research-framed and approximate — individual response varies widely, and none of these are guaranteed outcomes. Sleep-related observations tend to be reported earliest; body-composition changes, where reported, are the slowest.
| Window | Commonly reported in research framing |
|---|---|
| Week 1–2 | Sleep quality is the earliest commonly reported change, consistent with pre-bed pulse timing reinforcing the nocturnal GH pulse |
| Week 2–4 | Reports of improved recovery between training sessions and general well-being |
| Week 4–8 | Recovery effects reported as more consistent; IGF-1-mediated processes have more time to accumulate |
| Week 8–12 | Where reported, body-composition changes are the slowest and most variable; they depend heavily on training, nutrition and sleep |
Read this table as a map of what has been reported, not a promise of what will happen. The strongest, most consistent human data for Ipamorelin remain limited, and much of the timeline reasoning is extrapolated from GH physiology rather than large Ipamorelin-specific trials.
Safety, Side Effects and Contraindications
Ipamorelin’s clean receptor profile does not make it consequence-free. The following are documented considerations from the research and safety literature, framed for research handling — not medical advice and not an exhaustive list.
| Consideration | What the research framing notes |
|---|---|
| Water retention | Mild fluid retention is a known class effect of raising GH; can present as puffiness, especially early in a cycle |
| Injection-site reactions | Local redness, itching or minor irritation; site rotation is the standard mitigation |
| Headache / lightheadedness | Reported occasionally, particularly around dose changes |
| IGF-1 considerations | Sustained elevation of GH/IGF-1 is a meaningful long-term consideration; IGF-1 signaling interacts with tissue growth, which is why indefinite use is not the documented framing |
| Insulin sensitivity | GH can influence glucose handling; relevant context for anyone studying metabolic parameters |
| Regulatory status | Not FDA-approved; no approved human indication; sold and studied as research-use-only |
Two points deserve emphasis. First, the IGF-1 and long-term-elevation considerations are the main reason the research framing favors cycling with breaks over continuous indefinite use — chronically elevated growth signaling is not a trivial thing. Second, because Ipamorelin has no approved human indication (its status on ClinicalTrials.gov reflects a compound without an approved use), there is no established, regulator-vetted dosing for any medical condition; everything in this guide is documented research protocol, full stop.
Injection technique and storage are part of safety too. Handle the vial aseptically, rotate injection sites, and follow proper storage after reconstitution so the solution does not degrade — the reconstitution and storage practices linked earlier cover this in detail.
Frequently Asked Questions
Dosing and Reconstitution
How much Ipamorelin per day is the documented protocol? The documented starting dose is 100 mcg per dose, administered 1–3 times daily on an empty stomach. That puts the documented daily total at 100–300 mcg depending on frequency. The per-dose amount stays at 100 mcg; the protocol scales by adding pulses, not by enlarging a single injection.
What does a 100 mcg Ipamorelin dose look like on a syringe? It depends on the vial. From a 5 mg vial reconstituted with 3 mL (1.67 mg/mL), 100 mcg is 0.06 mL = 6 units on a U-100 syringe. From a 10 mg vial with 3 mL (3.33 mg/mL), the same 100 mcg is 0.03 mL = 3 units. Same dose, different unit mark, because the concentrations differ.
How do I reconstitute an Ipamorelin vial? The documented protocol uses 3 mL of bacteriostatic water for both the 5 mg and 10 mg vials. That yields 1.67 mg/mL and 3.33 mg/mL respectively. For the actual handling technique, see the reconstitution guide, and for any non-standard vial or diluent volume use the dosage calculator.
Why is the 10 mg vial only 3 units when the 5 mg vial is 6? Both use 3 mL of water, so the 10 mg vial is twice as concentrated. A dose of a given size therefore occupies half the volume — and half the units on the syringe. The micrograms delivered are identical; only the volume changes.
Can I use more or less than 3 mL of bacteriostatic water? The documented protocol uses 3 mL for both vials, and this guide only presents documented numbers. Changing the diluent volume changes the concentration and therefore the units for every dose — if the volume differs, recompute with the calculator rather than estimating.
Timing and Cycling
Why does Ipamorelin have to be taken on an empty stomach? Because elevated blood glucose and insulin blunt GH secretion. Food — especially carbohydrates — raises insulin, which suppresses the GH pulse Ipamorelin is meant to trigger. Dosing in a fasted window keeps insulin low so the pulse is not wasted.
Why is Ipamorelin taken before bed? The body’s largest natural GH pulse happens during early deep sleep. A pre-bed dose, taken once the stomach has emptied, is timed to reinforce that nocturnal pulse. It is the slot most consistently kept even in a once-daily schedule.
How often should Ipamorelin be dosed? The documented range is 1–3 times per day. Once daily is usually the pre-bed slot; twice daily adds a fasted-AM dose; three times daily adds a midday dose. Each dose stays at 100 mcg and each is taken away from food. The literature has not established an optimal frequency for any human goal.
How long is an Ipamorelin cycle? The research framing discusses defined multi-week blocks — commonly in the range of roughly 8–12 weeks — followed by an off period before repeating, with the aim of limiting receptor down-regulation. There is no clinically established optimal cycle length; these are documented conventions.
Is 5-on/2-off better than dosing every day? Neither pattern has been proven superior for Ipamorelin in human trials. The 5-on/2-off idea borrows from GH-therapy practice and is presented as a documented option, not a proven-better method. Both patterns are shown in the weekly grid above.
Pairing, Safety and Status
Why is Ipamorelin combined with CJC-1295 or Tesamorelin? Because they hit the GH axis from two angles. A GHRH analog primes the pituitary to make and ready more GH; Ipamorelin triggers the release and eases the somatostatin brake. Together they produce a larger, cleaner pulse than either alone. The documented example is the Tesamorelin + Ipamorelin protocol.
What makes Ipamorelin different from older GHRPs like GHRP-6? Selectivity. In the foundational literature, Ipamorelin releases GH with potency comparable to GHRP-6 but with minimal cortisol and prolactin release, and without the strong hunger response. That “clean pulse” is its defining characteristic.
What are the main side effects to be aware of? The documented considerations include mild water retention (a class effect of raising GH), injection-site reactions, occasional headache or lightheadedness, and — most importantly for long-term thinking — IGF-1 and sustained-GH-elevation considerations, which are why cycling with breaks is favored over indefinite use.
Is Ipamorelin FDA-approved? No. Ipamorelin is not FDA-approved and has no approved human indication; it is sold and studied as a research-use-only compound. Nothing in this guide is a prescription or a claim of proven clinical benefit. For the two documented Ipamorelin vials specifically, the 5 mg protocol and 10 mg protocol pages carry the full documented details.
References
- Raun K, et al. Ipamorelin, the first selective growth hormone secretagogue. European Journal of Endocrinology, 1998.
- Reviews on ghrelin / GHSR-1a receptor signaling and growth-hormone secretagogues (mechanism context).
- ClinicalTrials.gov — Ipamorelin has no approved human indication (regulatory status / context).
Research-use-only. This article is for informational and research purposes only. It is not medical advice, not a prescription, and not a personal recommendation to use any compound. Every dosing figure described here is a documented research protocol, not an instruction for human administration. Ipamorelin is not FDA-approved and has no approved human indication. Consult a qualified healthcare professional before making any health-related decision.