GLOW is a three-peptide combination vial built around one dominant skin-and-recovery molecule, GHK-Cu, supported by two repair peptides, BPC-157 and TB-500. In the research literature these compounds are associated with collagen signaling, angiogenesis, and tissue remodeling — which is why blends of this type are studied for skin quality, wound and soft-tissue recovery, and the “glow” that gives the vial its name. A single 70 mg vial is designed to be reconstituted once and drawn in small, repeatable microdoses.
The appeal of a blend is simplicity: instead of reconstituting and injecting three separate vials, a researcher works from one vial with a fixed internal ratio. The trade-off is that you cannot tune each component independently — the ratio of GHK-Cu to BPC-157 to TB-500 is locked at 50:10:10. This guide walks through the exact documented protocol for a 70 mg GLOW vial: how to reconstitute it, how much each microdose actually delivers per component, how often the research schedule administers it, and how a full on/off cycle is structured.
One honest sentence on evidence, up front: there is no registered human clinical trial of the GLOW blend itself. The mechanistic and preclinical evidence sits with the individual peptides — chiefly GHK-Cu, which has the deepest literature — while the specific three-peptide combination is used in research settings without combination-level trial data. Everything below is framed as the documented research protocol, for research use only, never as a prescription or a personal recommendation.

At a Glance
This table summarizes the documented GLOW research protocol for a standard 70 mg vial reconstituted with 3 mL of bacteriostatic water. Every number is derived and shown in the reconstitution section below.
| Attribute | Documented protocol (research use only) |
|---|---|
| Use (research context) | Skin quality / appearance, soft-tissue and wound recovery, connective-tissue remodeling |
| Typical vial | 70 mg blend — GHK-Cu 50 mg + BPC-157 10 mg + TB-500 10 mg |
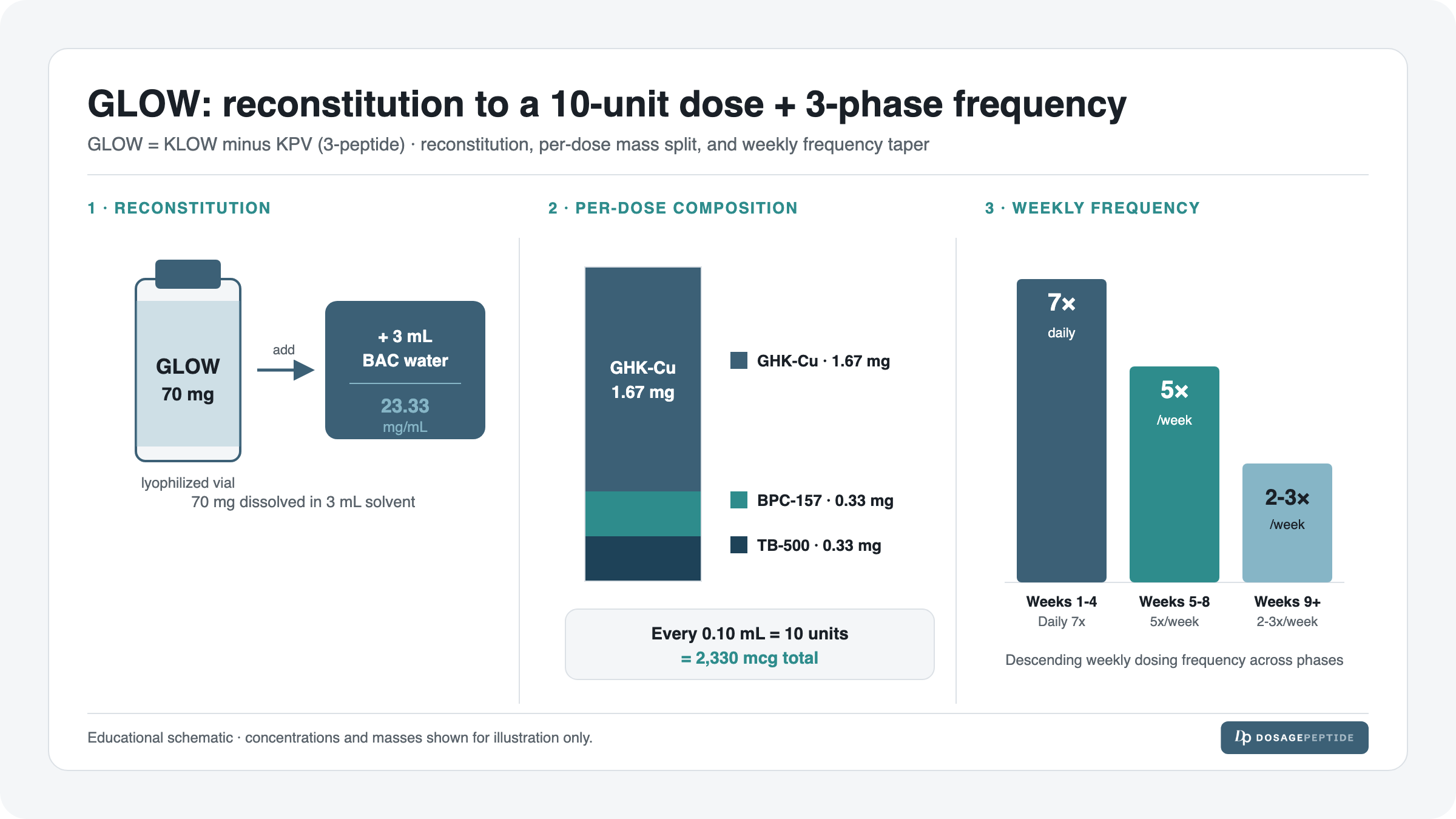
| Reconstitution | 70 mg + 3 mL bacteriostatic water → 23.33 mg/mL |
| Per-dose (documented) | ~2.33 mg total blend = 0.10 mL = 10 units on a U-100 syringe |
| Per-dose component split | GHK-Cu ~1.67 mg · BPC-157 ~0.33 mg · TB-500 ~0.33 mg |
| Schedule | 3-phase: daily (wks 1–4) → 5×/week (wks 5–8) → 2–3×/week maintenance |
| Onset / timeline (research-observed) | Subjective skin/recovery changes reported over weeks, not days; connective-tissue effects are cumulative |
| Common side effects | Injection-site redness/itch, transient flushing, histamine-type reactions (blend contains no antihistamine component) |
| Best stacked with | Discussed below — generally kept minimal; KPV-containing blends (KLOW) chosen for reactive skin |
| Regulatory status | Not an FDA-approved drug; research chemical; not for human use |
What GLOW Is / Composition
GLOW is a fixed-ratio blend of three research peptides in a single 70 mg vial. The name is functional shorthand: it is essentially the well-known KLOW stack minus KPV. Where KLOW is a four-peptide blend (GHK-Cu, BPC-157, TB-500, and KPV), GLOW drops KPV to leave a cleaner three-peptide skin-and-recovery base. If you are weighing the two, see the dedicated comparison of KLOW vs GLOW vs Wolverine peptide blends and the primer on what the KLOW peptide blend is. Both blends also appear in the wider peptide dosage catalog alongside single-peptide protocols.
The three components and their documented roles:
| Component | Amount in vial | Share of blend | Role in the blend (research context) |
|---|---|---|---|
| GHK-Cu (copper tripeptide-1) | 50 mg | 71.4% | Anchor compound. Copper-binding tripeptide associated in the literature with collagen/elastin signaling, skin remodeling and antioxidant activity. |
| BPC-157 (body protection compound) | 10 mg | 14.3% | Support peptide studied for angiogenesis and soft-tissue/gut repair signaling. |
| TB-500 (thymosin β4 fragment) | 10 mg | 14.3% | Support peptide associated with cell migration, actin regulation and tissue recovery. |
| Total | 70 mg | 100% | Fixed 50:10:10 ratio — cannot be tuned per component |
Anchor-compound logic. GHK-Cu is 71% of the blend by mass, so GLOW is best understood as a GHK-Cu protocol with two repair peptides layered in. When you set your dose by the total-blend number, you are really pinning down the GHK-Cu delivery; the BPC-157 and TB-500 amounts follow along at roughly one-fifth of the GHK-Cu mass each. That is the right mental model for reasoning about supply and frequency.
GLOW vs KLOW: which and when
The single practical difference between the two blends is KPV. KPV is a tripeptide fragment associated with anti-inflammatory and mast-cell/histamine-calming activity. That gives a simple heuristic:
- GLOW (3 peptides) — the leaner base, chosen when skin is calm and the goal is straightforward skin-quality and recovery support.
- KLOW (4 peptides) — adds KPV, often preferred when skin is reactive, inflamed or histamine-prone, because KPV is the calming component. Full dosing lives in the KLOW dosage protocol guide.
Neither is “stronger”; they target slightly different research questions. GLOW is the answer when you want the GHK-Cu-led base without the added KPV variable.
How to Dose GLOW (Research Protocol)
The documented GLOW research protocol works from a single per-dose figure of ~2.33 mg total blend (2330 mcg), drawn as 0.10 mL / 10 units on a U-100 insulin syringe. Because the ratio is fixed, that one draw always delivers the same three-way split. The table below is the documented dosing reference; frequency (how many of these doses per week) is set by the phase you are in, covered in the schedule and titration sections.
| Parameter | Documented value | How it is derived |
|---|---|---|
| Concentration after mixing | 23.33 mg/mL | 70 mg ÷ 3 mL |
| Per-dose total blend | 2.33 mg (2330 mcg) | Documented starting dose |
| Draw volume | 0.10 mL | 2.33 mg ÷ 23.33 mg/mL |
| Syringe units (U-100) | 10 units | 0.10 mL × 100 |
| GHK-Cu per dose | ~1.67 mg | 2.33 mg × (50/70) |
| BPC-157 per dose | ~0.33 mg | 2.33 mg × (10/70) |
| TB-500 per dose | ~0.33 mg | 2.33 mg × (10/70) |
Administration in the documented research protocol is subcutaneous, using a small-gauge U-100 insulin syringe. The 10-unit draw is deliberately small and easy to read on the barrel, which is one reason the 3 mL reconstitution volume is chosen.
Reconstitution & Draw — With the Real Math
This is the load-bearing section. Get the reconstitution right and every subsequent number falls out automatically. GLOW ships as a lyophilized (freeze-dried) 70 mg powder that must be dissolved in bacteriostatic water before any dose can be drawn.
Step 1 — Concentration
Reconstitute the 70 mg vial with 3 mL of bacteriostatic water. Concentration is simply total mass divided by total volume:
70 mg ÷ 3 mL = 23.33 mg/mL
Every 1 mL now contains 23.33 mg of blended peptide. (For a refresher on choosing the diluent and why bacteriostatic — not sterile — water is used for multi-draw vials, see the bacteriostatic water reconstitution guide and the full peptide reconstitution guide.)
Step 2 — Draw volume for the documented dose
The documented per-dose is 2.33 mg of total blend. Draw volume is dose divided by concentration:
2.33 mg ÷ 23.33 mg/mL = 0.0999 mL ≈ 0.10 mL
Step 3 — Convert to syringe units
A U-100 insulin syringe is calibrated so that 1 mL = 100 units. Multiply the draw volume by 100:
0.10 mL × 100 = 10 units
So the documented GLOW dose is a 10-unit mark on a standard U-100 barrel. If your syringe units-to-mL conversion ever feels shaky, the insulin syringe units for peptides guide walks through the U-100 scale in detail. You can also plug your own vial size and target dose into the dosage calculator to confirm the draw.
Step 4 — The per-component breakdown at 0.10 mL
Because the 50:10:10 ratio is fixed, that same 0.10 mL draw always delivers this split:
| Component | Fraction of blend | Math | Delivered per 0.10 mL dose |
|---|---|---|---|
| GHK-Cu | 50/70 | 2.33 mg × 0.714 | ~1.67 mg |
| BPC-157 | 10/70 | 2.33 mg × 0.143 | ~0.33 mg |
| TB-500 | 10/70 | 2.33 mg × 0.143 | ~0.33 mg |
| Total blend | 2.33 mg | ||
This is why the blend is often described as “GHK-Cu-led”: a single documented dose delivers about 1.67 mg of GHK-Cu alongside roughly a third of a milligram each of BPC-157 and TB-500.
Supply math
A 70 mg vial reconstituted in 3 mL holds 3.00 mL of solution. Each dose draws 0.10 mL, so:
3.00 mL ÷ 0.10 mL = 30 doses per vial
How long 30 doses lasts depends entirely on frequency — which is the whole point of the phase schedule:
| Phase | Frequency | Doses/week | Vial duration (30 doses) |
|---|---|---|---|
| Loading (wks 1–4) | Daily | 7 | ~4.3 weeks |
| Step-down (wks 5–8) | 5×/week | 5 | ~6 weeks |
| Maintenance | 2–3×/week | 2–3 | ~10–15 weeks |
Practically, roughly one vial per month covers the daily loading phase, and the same vial stretches much further once you drop to maintenance frequency.
Weekly Schedule — Example Week
Below is an example of a single week in each of the three phases, so you can see how the same 10-unit dose maps onto a Monday-to-Sunday grid. “—” means no injection that day.
| Phase | Mon | Tue | Wed | Thu | Fri | Sat | Sun |
|---|---|---|---|---|---|---|---|
| Loading (wks 1–4, daily) | 10u | 10u | 10u | 10u | 10u | 10u | 10u |
| Step-down (wks 5–8, 5×/wk) | 10u | 10u | 10u | 10u | 10u | — | — |
| Maintenance (2–3×/wk) | 10u | — | 10u | — | 10u | — | — |
Each “10u” is the identical 0.10 mL / 2.33 mg draw described above. Nothing about the dose size changes across phases in the documented protocol — only the frequency changes. This keeps reconstitution math constant and makes the schedule easy to follow.
Dosing Phases, Titration & Cycling
The documented GLOW research schedule is a three-phase frequency taper rather than a dose-size titration. The rationale mirrors how GHK-Cu-led protocols are typically framed: front-load exposure to establish tissue effects, then step frequency down to a maintenance rhythm that sustains them.
| Phase | Weeks | Frequency | Per-dose | Purpose (research framing) |
|---|---|---|---|---|
| Phase 1 — Loading | Weeks 1–4 | Daily (7×/week) | 10 units / 2.33 mg | Establish consistent exposure across the loading window |
| Phase 2 — Step-down | Weeks 5–8 | 5×/week | 10 units / 2.33 mg | Reduce frequency while maintaining momentum |
| Phase 3 — Maintenance | Week 9+ | 2–3×/week | 10 units / 2.33 mg | Sustain with the lowest practical frequency |
Cycling: on and off
The documented cycling framework runs a continuous 8–12 week “on” block (loading through into maintenance) followed by a 4–8 week “off” period. A representative full cycle:
- On (8–12 weeks): 4 weeks daily → 4 weeks at 5×/week → remaining weeks at 2–3×/week maintenance.
- Off (4–8 weeks): no administration, allowing a washout before any subsequent cycle.
The off-block is part of the documented research schedule; it is not a dosing recommendation. Because GLOW is a blend led by GHK-Cu, cycle length is usually reasoned from the GHK-Cu component rather than the smaller BPC-157/TB-500 fractions.
Timeline: What to Expect
Connective-tissue and skin effects in the underlying peptide literature are cumulative — reported over weeks, not overnight. The table below frames a research-observed timeline; it is descriptive of what the literature and protocol structure suggest, not a promise of results.
| Week / Phase | What is happening (mechanistic framing) | What is observed in research/anecdote |
|---|---|---|
| Week 1 (loading start) | Consistent daily exposure begins; local peptide signaling initiated | Little visible change; injection-site reactions if any appear here |
| Weeks 2–4 (loading) | Cumulative GHK-Cu exposure; collagen/remodeling signaling in the literature is time-dependent | Earliest subjective skin-texture or recovery reports in some accounts |
| Weeks 5–8 (step-down) | Frequency reduced; established signaling maintained | Skin-quality and soft-tissue recovery reports more consistent in this window |
| Weeks 9–12 (maintenance) | Low-frequency upkeep of accumulated effect | Effects, where reported, tend to plateau and hold at maintenance frequency |
| Off block | Washout; no administration | Basis for evaluating whether effects persist between cycles |
Because there is no combination-level trial, this timeline is a synthesis of the individual-peptide literature and the protocol’s own structure — treat it as a framework for observation, not a guarantee. Individual results are not established and should not be assumed.
Stacking / Combinations
GLOW is already a three-peptide stack, so the default posture is to keep additions minimal and change one variable at a time. Documented considerations:
- Switch to KLOW instead of stacking KPV separately. If reactive or histamine-prone skin is the concern, the cleaner move is to run the four-peptide KLOW blend (which includes KPV) rather than co-administering a loose KPV vial. See the KLOW protocol guide and the blend comparison.
- Avoid duplicating components. GLOW already contains BPC-157 and TB-500; adding standalone BPC-157 or TB-500 on top double-counts those peptides and muddies attribution of any effect.
- Keep the blend as the anchor. If additional peptides are studied alongside GLOW, run GLOW at its documented schedule first and introduce anything else only after establishing a stable baseline.
When Progress Stalls
If the documented protocol is running and observed changes flatten, the research-troubleshooting ladder is to check variables in order before touching the dose:
- Verify reconstitution. Re-confirm 70 mg + 3 mL = 23.33 mg/mL and that draws are truly 10 units. An under-filled or mis-drawn syringe is the most common cause of “nothing is happening.” Recheck on the dosage calculator.
- Confirm storage integrity. Degraded peptide delivers less active compound; see storage below and the peptide storage guide.
- Confirm frequency adherence. Missed doses during the loading phase are the usual reason a stall shows up in weeks 3–5.
- Complete the phase before judging. Effects in the underlying literature are cumulative; evaluating at week 2 of a loading phase is premature.
- Consider the blend choice. If reactive skin is limiting tolerability, the KPV-containing KLOW blend may be the better-matched research option — not a higher GLOW dose.
Note that the documented GLOW protocol holds the per-dose size constant; the lever it exposes is frequency and cycle structure, not dose escalation.
Side Effects & Mitigation
GLOW’s side-effect profile is driven mainly by its components’ known reactions in research settings. Because GLOW (unlike KLOW) contains no KPV, it has no built-in histamine-calming component — a relevant point for reactive skin.
| Issue | Why it happens | Mitigation (research context) |
|---|---|---|
| Injection-site redness / itch | Local reaction to peptide or diluent; GHK-Cu is copper-bound | Rotate injection sites; confirm sterile technique; smaller-gauge needle |
| Transient flushing | Vasoactive/histamine-type response after a dose | Often settles over the loading phase; note timing and severity |
| Histamine-type reactions | No KPV in GLOW to buffer mast-cell/histamine activity | Consider the KPV-containing KLOW blend for reactive skin instead of pushing GLOW |
| Taste/metallic sensation | Copper content of GHK-Cu | Generally benign; note if persistent |
| Under-dosing / “no effect” | Draw error or degraded peptide, not a true stall | Recheck the 10-unit draw and storage; verify on the calculator |
Safety & Contraindications
GLOW and its component peptides are not FDA-approved drugs. They are sold and handled as research chemicals for laboratory use only and are not intended for human consumption. None of GHK-Cu, BPC-157, or TB-500 has an approved human indication, and the GLOW combination specifically has no clinical trial establishing safety or efficacy in humans.
Because the blend is copper-containing (GHK-Cu) and lacks the KPV calming component, particular caution in the research literature attaches to histamine-reactive or highly sensitive skin. There is no established safety data for the combination in any population, so the honest position is that contraindication data does not exist at the combination level. Anyone considering peptides for a health purpose should consult a licensed clinician; this guide does not substitute for medical advice and is not a recommendation to use GLOW.
Storage & Handling
- Before reconstitution: store the lyophilized 70 mg vial cold and dark; the freeze-dried powder is the most stable form.
- After reconstitution: refrigerate the mixed vial and use bacteriostatic (not sterile) water so the multi-dose vial resists microbial growth across ~30 draws.
- Handling: reconstitute gently — add the water down the vial wall rather than jetting it onto the powder — and avoid shaking, which can shear peptide.
- Integrity: discard if the solution becomes cloudy, discolored beyond the expected faint blue of copper-bound GHK-Cu, or shows particulates.
For diluent choice, temperatures, and post-mix shelf-life specifics, follow the peptide storage guide and the full peptide reconstitution guide. Degraded peptide is a frequent hidden cause of an apparent “stall,” so storage is a safety and an efficacy variable.
What the Evidence Actually Shows
Here is the honest evidence status, component by component:
- GHK-Cu has the deepest literature of the three. Reviews describe regenerative and protective actions, roles in skin regeneration, and modulation of multiple cellular pathways — but this is largely mechanistic and preclinical work, not large human efficacy trials.
- BPC-157 is supported by animal and in-vitro studies and reviews of its pharmacology; robust human clinical trial evidence remains limited.
- TB-500 (thymosin β4) is studied for cell migration and tissue repair mechanisms, again predominantly in preclinical settings.
- The GLOW blend itself has no registered clinical trial. There is no combination-level human data — a genuine evidence gap that this guide does not paper over.
In short: the ingredients have plausible mechanistic support (strongest for GHK-Cu); the specific three-peptide product does not have trial-level proof. Any expectation of results should be calibrated accordingly.
Frequently Asked Questions
Choosing GLOW
What is the GLOW peptide dosage? The documented research dose is ~2.33 mg of total blend per administration, which for a 70 mg vial reconstituted in 3 mL equals 0.10 mL, or 10 units on a U-100 syringe. That single draw delivers ~1.67 mg GHK-Cu, ~0.33 mg BPC-157 and ~0.33 mg TB-500.
GLOW vs KLOW — what’s the dosage and difference? Both use the same per-draw approach, but KLOW is a four-peptide blend that adds KPV, while GLOW is the three-peptide base without it. The heuristic: GLOW for calm skin, KLOW for reactive or histamine-prone skin. See the KLOW vs GLOW vs Wolverine comparison and the KLOW dosage guide.
Why is GLOW described as “GHK-Cu-led”? GHK-Cu is 50 of the 70 mg (71%) of the blend, so each dose is dominated by GHK-Cu with BPC-157 and TB-500 as minority support peptides.
Is GLOW stronger than KLOW? No — neither is “stronger.” They differ by the presence of KPV, which changes the profile (calming component present vs absent), not raw potency.
Using GLOW
How do I reconstitute GLOW? Add 3 mL of bacteriostatic water to the 70 mg vial: 70 ÷ 3 = 23.33 mg/mL. A 2.33 mg dose is 2.33 ÷ 23.33 = 0.10 mL = 10 units. Confirm on the dosage calculator.
How often is GLOW dosed — what’s the frequency? The documented schedule is three phases: daily in weeks 1–4, then 5×/week in weeks 5–8, then 2–3×/week for maintenance. The dose size stays 10 units throughout; only frequency changes.
How to dose GLOW on a weekly grid? During loading you inject every day; in step-down you take weekends off (Mon–Fri); in maintenance you inject about every other active day (e.g., Mon/Wed/Fri). See the weekly schedule table above.
How many doses are in one vial? 3.00 mL ÷ 0.10 mL = 30 doses. That’s about 4.3 weeks of daily loading, or 10–15 weeks at maintenance frequency.
What is the GLOW cycle length? The documented cycle is 8–12 weeks “on” (loading through maintenance) followed by 4–8 weeks “off” before any repeat cycle.
How many units of GLOW is one dose? Ten units on a U-100 insulin syringe, equal to 0.10 mL. If unit conversions are unclear, the insulin syringe units guide explains the U-100 scale.
Practical & safety
Is GLOW FDA-approved or a prescription? No. GLOW and its component peptides are not FDA-approved, are handled as research chemicals for laboratory use only, and are not for human consumption. This guide is research information, not medical advice.
Are there side effects? Reported reactions include injection-site redness/itch, transient flushing and histamine-type reactions. Because GLOW has no KPV, it lacks a built-in histamine-calming component — a reason reactive skin sometimes points to KLOW instead.
Is there human trial evidence for the GLOW blend? No — there is no registered clinical trial of the GLOW combination. The mechanistic evidence sits with the individual peptides, strongest for GHK-Cu. Treat combination-level claims cautiously.
How should GLOW be stored? Keep the lyophilized vial cold and dark before mixing; refrigerate after reconstitution and use bacteriostatic water for the multi-draw vial. Discard if cloudy or discolored beyond the faint blue of copper-bound GHK-Cu.
Where can I see the full product protocol? The vial-specific page is the GLOW 70 mg vial dosage protocol, and reconstitution mechanics are covered in the reconstitution guide.
References
- Pickart L, Margolina A. Regenerative and Protective Actions of the GHK-Cu Peptide. Int J Mol Sci, 2018. PMC6073405.
- GHK Peptide as a Natural Modulator of Multiple Cellular Pathways in Skin Regeneration, 2015. PMC4508379.
- Jozwiak M, et al. BPC-157 literature and patent review. Pharmaceuticals, 2025. PMC11859134.
- ClinicalTrials.gov — no registered GLOW-blend clinical trial (evidence-gap note).
Disclaimer: This article is provided for research and educational purposes only. GLOW and its component peptides are research chemicals that are not FDA-approved, are not medical advice, and are not intended for human consumption or for the diagnosis, treatment, cure, or prevention of any disease. All dosing figures describe a documented research protocol, not a prescription or personal recommendation. Consult a licensed clinician before making any health decision.