The question in the title carries a quiet assumption worth surfacing before we examine a single data point: it presumes that clinical trials have something affirmative to say about AOD-9604 as a fat-burner — that the “fat-burning potential” is a real, measurable quantity waiting to be reported. The honest answer is more sobering. AOD-9604 has, in fact, been through a serious human clinical program — roughly six trials enrolling on the order of 900 participants — and that program did not end in a triumph. It ended in 2007 when the pivotal, largest, best-controlled study failed to separate the peptide from placebo on weight loss.3 So when clinical trials are invoked as evidence for AOD-9604’s fat-burning power, they are being invoked for a conclusion those trials did not reach.
This matters because AOD-9604 is marketed today, across a sprawling ecosystem of clinics and research-chemical vendors, almost exclusively as a “fat-loss peptide.” The molecule was genuinely engineered for that purpose — its very name abbreviates “Anti-Obesity Drug 9604” — and its proposed mechanism is a coherent, testable story about how a fragment of growth hormone might mobilize stored fat.1 The mechanistic elegance is real. What is missing is the human efficacy that would convert an elegant hypothesis into an established therapy. That gap between plausible mechanism and demonstrated clinical benefit is the central subject of this article.
The goal here is not to dismiss AOD-9604 as worthless, nor to inflate it. It is to give researchers and educated readers an honest map: what the compound is, how it is supposed to work, what the animal data actually showed, what the human trials actually found, how it stacks up against agents that have genuinely moved the needle on body weight, what its safety record looks like, and where it sits with regulators. Throughout, one distinction is kept in sharp focus — the difference between “this could reduce fat” (a mechanistic conjecture, reasonably supported in rodents) and “this does reduce fat in people” (a clinical claim that AOD-9604’s own pivotal trial failed to substantiate). AOD-9604 is not approved by any major regulator for weight loss or any other indication, and nothing below should be read as suggesting it treats, cures, or prevents obesity or any disease.
What AOD-9604 Is and Where It Came From
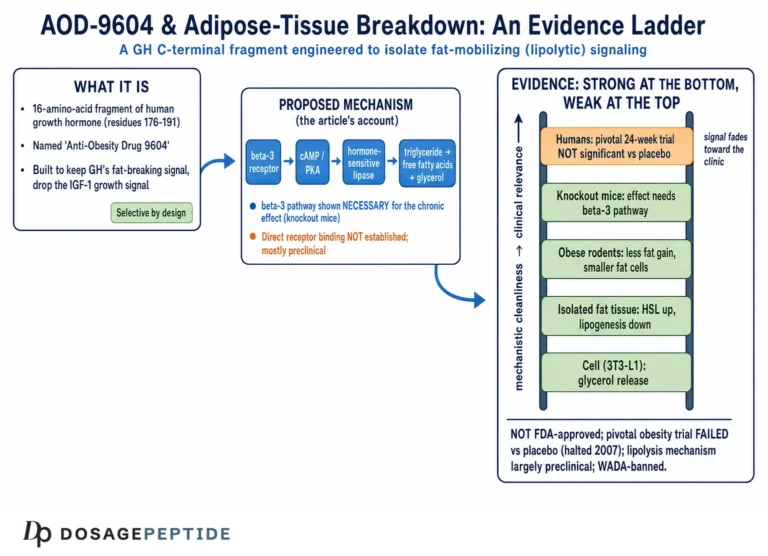
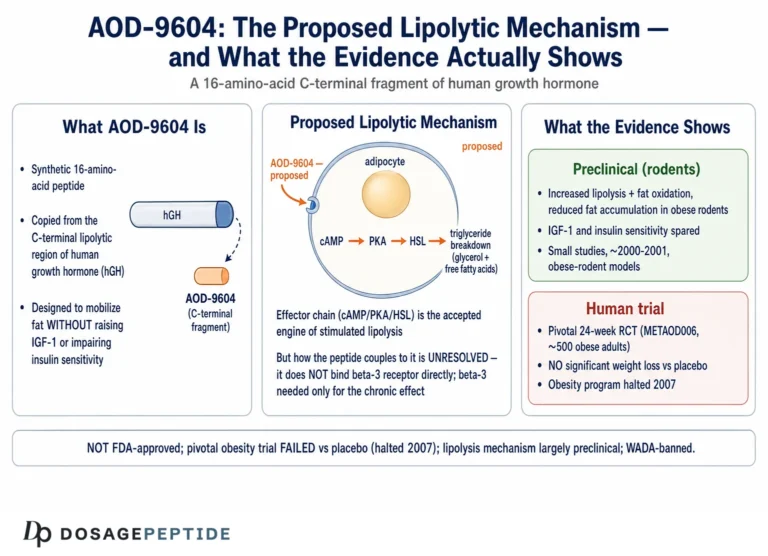
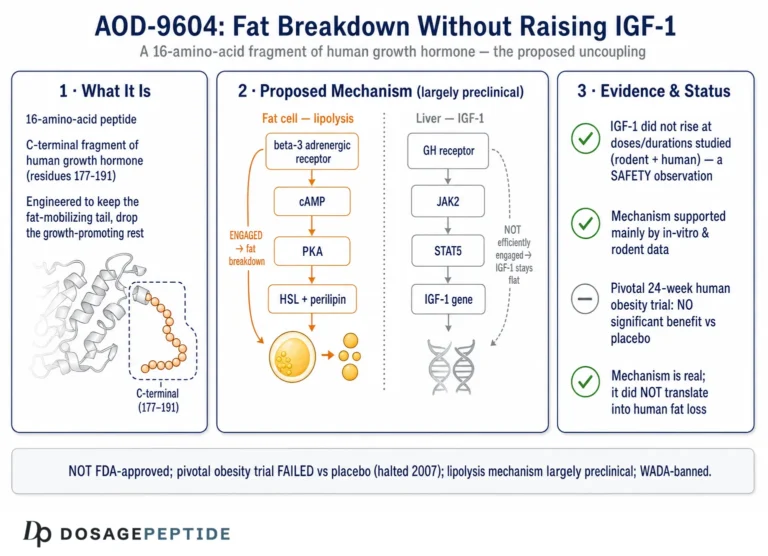
AOD-9604 is a synthetic 16-amino-acid peptide — a hexadecapeptide. Its sequence corresponds to the C-terminal region of human growth hormone (hGH), residues 176–191, with one deliberate modification: a tyrosine residue is added at the N-terminus, a change made to stabilize the fragment and improve its handling.1 The full sequence is H-Tyr-Leu-Arg-Ile-Val-Gln-Cys-Arg-Ser-Val-Glu-Gly-Ser-Cys-Gly-Phe-OH, and its two cysteine residues form a disulfide bridge that recreates the small loop present in the parent hormone’s lipolytic domain. In effect, AOD-9604 is a chemical attempt to isolate one narrow slice of growth-hormone biology and reproduce it in a small, drug-like molecule.
The compound originated in work at Monash University in Melbourne, Australia, and was developed commercially by Metabolic Pharmaceuticals Limited. The scientific rationale was genuinely clever. Full-length growth hormone does many things at once: it drives longitudinal bone growth in children, raises circulating insulin-like growth factor-1 (IGF-1), alters glucose handling and insulin sensitivity, and, as a distinct action, promotes the breakdown of stored fat. Decades of endocrine research had localized much of the fat-mobilizing (lipolytic) activity to the C-terminal portion of the hGH molecule. The hope was that a short peptide reproducing only that region could deliver the fat-burning signal while shedding the other growth-hormone effects — particularly the rise in IGF-1 and the deterioration in glucose tolerance associated with chronic GH exposure, both of which limit GH’s usefulness as a weight-loss agent.12
Early metabolic studies reported that AOD-9604 reproduced the lipolytic and fat-oxidizing actions of hGH in fat tissue and in obese rodents without raising IGF-1 or impairing glucose tolerance.1 That selective profile — fat effects without the endocrine baggage — became the compound’s defining pitch and remains the reason it is discussed today as a “clean” fat-loss research peptide. It is a genuinely attractive premise. The trouble, as we will see, is that attractiveness on paper repeatedly failed to translate into robust weight loss in the people who received it.
Historically, the obesity program was the entire story for the better part of a decade. Metabolic Pharmaceuticals ran a series of human trials through the early-to-mid 2000s, moving from safety and pharmacokinetic work into Phase 2 efficacy studies. When the pivotal 24-week trial underperformed, development as an anti-obesity drug was halted in 2007.3 The molecule then reappeared in two very different guises: as a self-affirmed “generally recognized as safe” (GRAS) ingredient marketed for metabolic-health supplements,5 and as an experimental intra-articular agent for osteoarthritis in animal models.10 Neither of those second acts restored its status as a proven weight-loss drug.
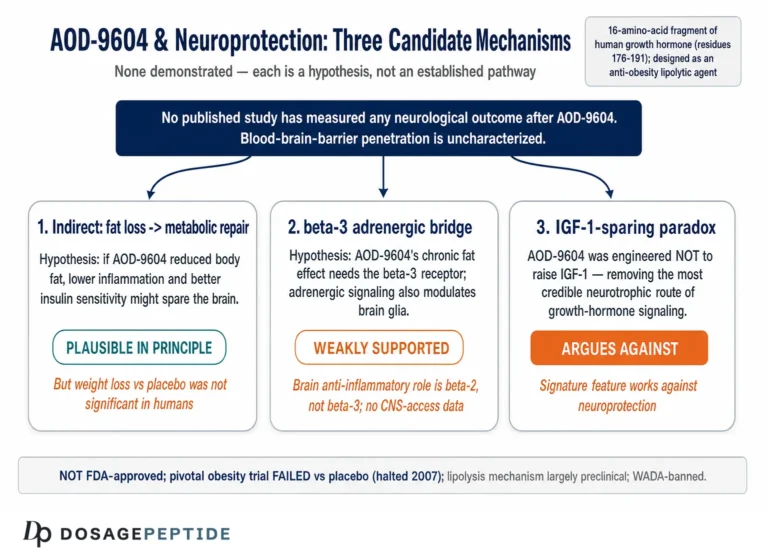
A useful mental model is to keep three things distinct that popular writing tends to blur. First, the parent hormone: full-length hGH, a 191-residue protein with broad endocrine effects. Second, the lipolytic domain: the C-terminal region thought to carry much of the fat-mobilizing signal. Third, the engineered fragment: AOD-9604 itself, a stabilized 16-residue reproduction of that domain. Each step narrows the biology — and each step also narrows the evidence. The parent hormone’s effects on human fat are well established; the fragment’s are not. When marketing collapses these three levels into “it’s basically the fat-burning part of growth hormone,” it borrows the parent’s credibility for a fragment that has to earn its own. Readers exploring adjacent research directions for the compound can see how this narrowing plays out in the peptide’s other proposed applications, such as the work on AOD-9604 and obesity-related cognitive decline and on AOD-9604 in diabetic wound repair, each of which faces the same evidence-maturity questions.
The Proposed Fat-Burning Mechanism
The mechanistic case for AOD-9604 as a fat-burner is the strongest part of the story, so it deserves a careful, honest telling — strong relative to the clinical data, but still incomplete at the molecular level.
The proposed mechanism centers on the adipocyte, the fat-storing cell. AOD-9604 is thought to reproduce the lipolytic signaling of growth hormone’s C-terminal domain, promoting the breakdown of stored triglycerides into free fatty acids (lipolysis) while simultaneously dampening the conversion of substrate into new fat (lipogenesis).1 The claimed net effect is a shift in fuel usage: more fat oxidized, less fat stored. In rodent models this translated into reduced body-fat accumulation and increased fat oxidation, and, importantly, it occurred without the IGF-1 elevation that accompanies full growth-hormone administration.1 That IGF-1-sparing feature is the mechanistic heart of the compound’s “clean” reputation.
The most frequently repeated specific claim is that AOD-9604 works by binding the beta-3 adrenergic receptor (β3-AR) on fat cells, activating adenylate cyclase, raising cyclic AMP, and switching on hormone-sensitive lipase. This deserves careful handling, because the popular shorthand overstates what the primary data actually establish. The strongest evidence for β3-AR involvement comes from a 2001 study in which chronic treatment with hGH and with AOD-9604 failed to reduce body weight or increase lipolysis in β3-AR knockout mice, whereas both worked in wild-type controls.2 That is a clean genetic result: it implicates the β3-adrenergic pathway in the compound’s chronic metabolic effect. But the same body of work found that acute increases in energy expenditure and fat oxidation still occurred in the knockout animals, which means at least part of the acute response is β3-independent.2 In other words, the receptor appears necessary for the sustained effect but is not the whole molecular story, and the precise way the peptide engages the pathway — whether by direct receptor binding or some upstream action — remains unresolved. Much of the confident “binds β3” language circulating online traces to commercial rather than primary sources.
There is a second, subtler point that matters for anyone weighing the fat-burning claim. Lipolysis — the release of free fatty acids from fat cells — is not the same as fat loss. Mobilizing a fatty acid into the bloodstream only reduces body fat if that fatty acid is subsequently oxidized (burned) rather than re-esterified and stored again. A compound can measurably raise circulating free fatty acids or acutely bump fat oxidation without producing meaningful, durable reductions in body-fat mass, especially if it does nothing to appetite or total energy intake. This distinction — acute biochemical signal versus chronic change in body composition — is precisely where AOD-9604’s story runs into trouble when it reaches human trials. The mechanism predicts fat mobilization; the pivotal clinical endpoint asks for pounds lost; and the two did not line up.
The honest mechanistic summary is therefore nuanced. AOD-9604 has a coherent, partly validated story for how it might act on fat tissue, anchored to at least one solid knockout study.2 It is not vaporware. But “coherent mechanism supported in rodents” is a much weaker claim than “proven fat-burner in humans,” and the marketing routinely elides the distance between the two.
The Preclinical Evidence: Rodents and Fat Cells
Before the human trials, AOD-9604’s case rested on animal and in-vitro work, and it is worth being specific about what that work did and did not show, because it is frequently cited as though it settled the fat-loss question.
The foundational metabolic studies examined lipolysis, lipogenesis, and fat oxidation in adipose tissue, isolated fat cells, and obese-rodent models.1 These reported that AOD-9604 reproduced key lipolytic actions of hGH — increasing fat breakdown and fat oxidation while reducing fat accumulation — and did so without elevating IGF-1 or degrading glucose tolerance. In the chronic obese-mouse experiments, treated animals accumulated less body fat than controls.12 The acute experiments showed a single dose could raise energy expenditure and fat oxidation and lower glucose oxidation, shifting the animal toward burning fat as fuel.2
Taken together, this is a respectable preclinical package for a lipolytic agent, and it justified moving the compound into humans. It is worth pausing on why that justification was reasonable at the time: a compound that increases fat oxidation, reduces fat accumulation, and does so without the IGF-1 rise or glucose deterioration that dog full growth hormone is, on paper, close to an ideal metabolic candidate. The rodent data did not merely show “an effect”; they showed the right kind of effect, selectively targeting fat while sparing the endocrine axes clinicians most worry about. That is precisely what made the eventual human failure so instructive rather than merely disappointing — it is a textbook example of a mechanistically attractive, preclinically validated candidate that simply did not carry its promise into people. But three caveats keep it in proportion. First, rodent obesity models are notoriously unfaithful predictors of human weight-loss efficacy; the pharmacology graveyard is full of compounds that stripped fat from mice and did nothing for people. Second, the effects were measured largely as biochemical and body-composition changes in animals whose energy intake and expenditure could be tightly controlled — conditions nothing like free-living humans. Third, and most importantly, preclinical fat-mobilization data are hypothesis-generating, not confirmatory: their entire purpose is to justify the human trials that follow, and it is those human trials, not the mouse data, that determine whether the fat-burning claim survives contact with reality. In AOD-9604’s case, the mouse data pointed one way and the pivotal human trial pointed another. When that happens, the human data win.
What the Human Clinical Trials Actually Found
This is the section the title’s question ultimately turns on, because “clinical trials” means human trials, and AOD-9604 has a real, if disappointing, human record.
Across its development, AOD-9604 was studied in roughly six human clinical trials enrolling more than 900 participants in total — a figure reported in the peer-reviewed pooled analysis of the program rather than in a single stand-alone efficacy paper.3 Early-phase work established safety, tolerability, and pharmacokinetics, and a dedicated human safety study characterized the peptide’s behavior at the doses tested.4 The efficacy question was addressed principally in two Phase 2 studies, and the contrast between them is the whole story.
The first, an approximately 12-week Phase 2 study designated METAOD005, tested oral AOD-9604 across several dose arms against placebo in obese adults. Its results were encouraging enough to generate optimistic press. In that shorter study, treated groups lost more weight than placebo — reported figures are on the order of 2.6 kg in a best-performing dose arm versus roughly 0.8 kg for placebo, a difference of nearly 1.8 kg — and, notably, the lower doses (around 1 mg) performed as well as or better than higher ones.3 On the strength of this signal, the compound advanced to a larger, longer, pivotal trial.
That pivotal study — the roughly 24-week METAOD006 trial, a randomized, double-blind, placebo-controlled, multicenter design enrolling on the order of 500 subjects — is the single most important piece of evidence about AOD-9604 and fat loss, and it is the one the marketing tends to omit. At its primary and key secondary endpoints, the weight-loss difference between AOD-9604 and placebo was too small to reach statistical significance.3 The promising signal from the 12-week study evaporated. Development of AOD-9604 as an obesity drug was terminated in 2007.
Why did the signal disappear? The most cited explanation is instructive and worth stating carefully rather than as an excuse. The pivotal trial incorporated an intensive diet-and-exercise regimen applied to all arms, including placebo. The lifestyle intervention was itself effective, so the placebo group lost meaningful weight on its own — a “floor effect” that shrank the room for any drug to demonstrate additional benefit. In plain terms: against a background of real diet and exercise, adding AOD-9604 produced no detectable extra fat loss. Some defenders read this charitably, arguing the trial design masked a genuine effect. A skeptic reads it more simply: a fat-loss drug that cannot beat placebo when both groups diet and exercise has not demonstrated that it does anything useful in the real world, where diet and exercise are exactly the co-interventions any responsible program would include. Either way, the endpoint that mattered was not met, and no subsequent trial reversed that verdict.
The clearest way to hold these results together is a table.
| Aspect | What the human obesity program showed |
|---|---|
| Human trials | ~6 studies, >900 participants total3 |
| Early signal (METAOD005, ~12 wk) | ~2.6 kg loss vs ~0.8 kg placebo; low (~1 mg) doses best3 |
| Pivotal trial (METAOD006, ~24 wk) | Randomized, double-blind, placebo-controlled, multicenter; ~500 subjects3 |
| Pivotal primary endpoint | Difference from placebo did NOT reach statistical significance3 |
| With intensive diet + exercise | No detectable added benefit over lifestyle alone (“floor effect”)3 |
| Outcome | Obesity drug development halted in 20073 |
| Endocrine profile | No reported rise in IGF-1; no impairment of glucose tolerance1 |
| Safety | Generally well tolerated at doses tested; no serious drug-attributed events reported4 |
Two honest conclusions follow. First, AOD-9604’s best-evidenced, purpose-built effect — fat loss in obesity — was not robustly demonstrated in humans. The trials are most accurately summarized as showing acceptable short-term safety with disappointing efficacy. Second, the frequent framing that “clinical trials support AOD-9604 for fat burning” is, at best, a selective reading that leans on a promising 12-week study while ignoring the larger, longer study designed specifically to confirm it — the study that failed. A researcher citing “the clinical trials” owes an honest account of both.
Dosing in a Research Context
Because AOD-9604 is not an approved medicine, there is no established therapeutic dose, and the figures that circulate come from the historical trial protocols and from research-chemical convention rather than from any regulatory label. This section is descriptive and strictly educational, not a usage recommendation.
The human efficacy trials used oral AOD-9604, with dose arms spanning roughly 0.25 mg to 30 mg once daily across the two studies.3 A striking and under-appreciated feature of the trial data is that the lower doses (around 1 mg) tended to perform at least as well as the higher ones — an inverted or flat dose-response that is unusual for a drug thought to act through a straightforward receptor-mediated pathway, and that in itself raises questions about how reliably the compound was doing what it was supposed to do. Oral peptide delivery is also notoriously inefficient, since the gut degrades peptides; the fact that development used an oral formulation complicates any attempt to reason from trial doses to the subcutaneous injection favored in contemporary research settings.
In non-clinical and research-chemical contexts today, AOD-9604 is typically encountered as a lyophilized powder reconstituted for subcutaneous use, and the microgram-per-injection figures quoted by vendors (commonly a few hundred micrograms) bear no validated relationship to the oral milligram doses used in the actual efficacy trials. This is a crucial honesty point: no one has run a properly powered human trial establishing that any subcutaneous dose of AOD-9604 produces meaningful fat loss. The dosing conventions in circulation are extrapolations layered on top of a compound whose oral trials failed, not evidence-based regimens. Researchers documenting handling parameters can consult general educational resources such as the site’s peptide reconstitution guide and dosage calculator for the arithmetic of concentration and volume, while recognizing that correct arithmetic does not manufacture clinical efficacy.
How AOD-9604 Compares With Agents That Actually Reduce Fat
The most illuminating way to calibrate AOD-9604’s fat-burning potential is to place it beside compounds that have unambiguously demonstrated fat loss in rigorous human trials. The contrast is stark, and it is the fastest way to see why AOD-9604’s clinical case is considered weak.
Over the past few years, the incretin-based drugs have redefined what “effective” means in obesity pharmacology. Once-weekly semaglutide, in the 68-week STEP 1 trial, produced a mean body-weight reduction of roughly 15% versus about 2.4% for placebo — a difference that is not merely statistically significant but clinically transformative.6 Tirzepatide, a dual GIP/GLP-1 receptor agonist, went further: in the 72-week SURMOUNT-1 trial, the highest dose delivered mean weight reductions of roughly 20–21%.7 The investigational triple agonist retatrutide, in a Phase 2 trial, reported mean reductions on the order of 24% at 48 weeks at the top dose.8 These are the benchmarks a serious fat-loss compound is now measured against, and readers can explore them further in dedicated discussions of how effective tirzepatide is according to recent clinical studies and of the emerging retatrutide triple-receptor agonist.
| Agent | Mechanism | Best human weight-loss result | Regulatory status (obesity) |
|---|---|---|---|
| Semaglutide (GLP-1 RA) | Appetite/satiety via GLP-1 receptor | ~15% mean loss vs ~2.4% placebo, 68 wk (STEP 1)6 | FDA-approved |
| Tirzepatide (GIP/GLP-1 RA) | Dual incretin appetite/energy effects | ~20–21% mean loss, 72 wk (SURMOUNT-1)7 | FDA-approved |
| Retatrutide (GGG triple agonist) | GIP/GLP-1/glucagon receptors | ~24% mean loss, 48 wk, Phase 28 | Investigational |
| AOD-9604 | Lipolytic hGH fragment; IGF-1-sparing | ~1.8 kg vs placebo at 12 wk; NOT significant at 24 wk3 | Not approved; development halted 2007 |
The pattern needs no embellishment. The approved and investigational incretin agents produce double-digit percentage weight loss in large, placebo-controlled trials with statistically robust separation from placebo. AOD-9604’s best human result was a sub-2-kilogram advantage in a short study that vanished in the longer, definitive one. These are not compounds in the same evidentiary universe. It would be a serious distortion to present AOD-9604 as a member of the effective-fat-loss category simply because it was designed to burn fat; design intent is not outcome.
Two caveats keep even this comparison honest, in fairness to all sides. The incretin drugs are not magic and their limits are real: weight tends to return after discontinuation — in the STEP 4 trial, participants switched to placebo regained a substantial fraction of lost weight over the following year9 — and they carry gastrointestinal side effects and cost and access barriers that AOD-9604’s mild profile does not. But “fewer side effects” is only a virtue in a drug that also works; a well-tolerated compound that does not produce meaningful fat loss is not a gentler alternative to effective therapy, it is simply an ineffective one. The right conclusion is not that AOD-9604 is a kinder weight-loss drug, but that it never became a weight-loss drug at all.
Safety and Tolerability
If AOD-9604’s efficacy record is its weakness, its short-term safety record is the relatively reassuring counterpart — a point that must be stated with care, because “well tolerated in obesity trials” is a narrower claim than it is often made to sound.
In the human obesity program, AOD-9604 was generally reported to be well tolerated over the studied durations, with no serious adverse events attributed to the compound and a profile that did not raise the endocrine concerns associated with full-length growth hormone.4 Specifically, it was reported not to elevate IGF-1 and not to impair glucose tolerance or insulin sensitivity in the studied settings — precisely the effects it was engineered to avoid.1 A dedicated human safety-and-tolerability evaluation supported an acceptable short-term profile at the doses tested,4 and later characterization framed the ingredient as having a favorable safety and metabolism profile in the sponsor’s assessment.5
Several caveats temper this picture and should travel with any statement about the compound’s safety:
- Safety is not efficacy. The single most important interpretive point is that a clean tolerability profile says nothing about whether the compound works. Absence of demonstrated harm and absence of demonstrated benefit coexist here, and marketing frequently smuggles the former in as though it implied the latter.
- Duration. Trials ran on the order of weeks to a few months. The long-term safety of repeated AOD-9604 administration — the pattern most relevant to anyone using it for ongoing body-composition goals — has not been characterized.
- Route and formulation. The pivotal human work used oral dosing. Contemporary research and non-clinical use typically involves reconstituted subcutaneous material, and safety data do not transfer automatically across routes and formulations.
- Product quality. Much material sold outside regulated channels is “research chemical” of variable purity. Impurities, endotoxin, and mislabeling are real hazards that have nothing to do with the molecule’s intrinsic safety and everything to do with sourcing — a concern the FDA explicitly raised in its 2024 compounding review.11
- Sport prohibition. AOD-9604 is prohibited in sport by the World Anti-Doping Agency; for athletes this is a safety-adjacent regulatory hazard independent of pharmacology.12
The reasonable reading is that AOD-9604 did not throw up major short-term safety signals in the limited, generally healthy-to-obese populations studied, and that its IGF-1-sparing design avoids some GH-related concerns. That is a genuine point in its favor as a research tool. It is not, and cannot be stretched into, evidence that the compound produces the fat loss for which it is sold.
Research Models and Methodology
Understanding how AOD-9604 was actually studied clarifies both what its data can support and what it cannot, and it explains why the fat-burning claim looks stronger in a slide deck than in a trial report.
In vitro and ex vivo fat-tissue work. The foundational studies measured lipolysis, lipogenesis, and fat oxidation in adipose tissue and isolated fat cells — free-fatty-acid release, oxidation rates, and the expression of enzymes involved in fat handling.1 These assays are well suited to characterizing a lipolytic agent, but they measure biochemical signals in isolated tissue, not weight change in a person. A robust free-fatty-acid response in a dish is a necessary starting point, not a demonstration of clinical fat loss.
Rodent models. The most methodologically informative animal work is the β3-AR knockout study, a clean genetic design that isolated the receptor’s contribution by comparing knockout and wild-type mice under identical treatment.2 Obese-rodent models assessed body-weight and fat-oxidation responses. These are legitimate, well-executed studies — but they are metabolic models in animals whose diet and activity are controlled, and their predictive value for free-living human weight loss is limited, as the eventual human trial results underscored.
Human trials. The clinical methodology was appropriate for an obesity drug: randomized, double-blind, placebo-controlled, multicenter designs with weight and body-composition endpoints, plus dedicated safety and pharmacokinetic studies.34 This is exactly the right architecture, which is what makes the null result meaningful rather than dismissible. When a well-designed, adequately powered, placebo-controlled pivotal trial fails to show significance, that is not a fluke to be explained away — it is the highest-quality evidence in the entire dossier, and it points against efficacy.
The methodological bottom line is that AOD-9604’s evidence architecture was built correctly to answer a fat-loss question, and it answered it: the answer, in the definitive human trial, was negative. Any confident present-day claim that the compound “burns fat” in humans is not supported by that architecture; it rests instead on the earlier, smaller, non-definitive signal and on rodent extrapolation. Researchers can situate AOD-9604 among related metabolic and growth-hormone-adjacent compounds through the site’s central dosage index, which catalogs these agents for educational reference rather than as endorsement of any efficacy claim.
Beyond Fat: The Compound’s Other Research Directions
Part of an honest appraisal is acknowledging that AOD-9604 has generated interest beyond obesity, because these adjacent findings are sometimes borrowed — illegitimately — to prop up the fat-loss narrative, and it helps to see them clearly for what they are.
The peptide’s best-documented regenerative signal comes not from fat but from cartilage. In a collagenase-induced knee osteoarthritis model in rabbits, weekly intra-articular injections of AOD-9604 (0.25 mg), alone or combined with hyaluronic acid, improved gross and histopathological cartilage scores relative to saline controls, with the combination outperforming either agent alone.10 This is a genuine, peer-reviewed preclinical finding. But it concerns joint cartilage under direct local injection — a different tissue, delivery route, and biological question from systemic fat loss — and it cannot be transferred to support a fat-burning claim. It is evidence that the molecule is biologically active in a specific local context, nothing more.
Other exploratory directions — proposed roles in metabolic-related cognitive health and in wound repair — occupy a similar status: mechanistically interesting, preclinically preliminary, and clinically unproven. The site’s discussions of AOD-9604 and muscle wasting and of its other proposed applications repeatedly reach the same conclusion this article reaches for fat loss: the human evidence is thin or absent, and the compound’s reputation runs well ahead of its data. Recognizing this consistent pattern is itself useful. AOD-9604 is a compound rich in plausible mechanisms and poor in confirmatory human outcomes, and the fat-loss indication — the one it was actually built and trialed for — is the clearest example of that gap, not an exception to it.
Regulatory Status
AOD-9604’s regulatory picture is layered and frequently misrepresented, so precision matters — especially because regulatory footnotes are often paraphrased as endorsements they are not.
No therapeutic approval, anywhere. AOD-9604 is not approved as a drug for obesity, weight loss, or any other condition by the U.S. Food and Drug Administration, the European Medicines Agency, or any comparable major regulator. Its pharmaceutical development for obesity was abandoned in 2007 after the pivotal trial failed to demonstrate a significant benefit over placebo.3 There is, correspondingly, no approved indication of any kind.
Supplement and food-ingredient framing. After the drug program ended, the compound was repositioned by its sponsor as a metabolic-health ingredient, supported by a self-affirmed “generally recognized as safe” (GRAS) characterization and safety/metabolism publications.5 This point is routinely abused in marketing, so it bears blunt statement: a GRAS self-affirmation addresses ingredient safety at supplement-level exposure; it is emphatically not a finding of efficacy and not drug approval. It can be declared by a sponsor without an affirmative FDA sign-off. A GRAS characterization for AOD-9604 tells you nothing whatsoever about whether the peptide produces fat loss. Conflating “recognized as safe as a food ingredient” with “shown to work as a fat-burner” is one of the most common errors in the literature around this compound.
U.S. compounding review. In 2024, AOD-9604 was among peptide substances considered by the FDA’s Pharmacy Compounding Advisory Committee for potential inclusion on the Section 503A bulk drug substances list. At the December 4, 2024 meeting, the committee voted against placing both the AOD-9604 free base and AOD-9604 acetate on the list, citing concerns including inadequate physicochemical characterization, potential immunogenicity and impurities, and a lack of clinical effectiveness data.11 This is a recent, explicit regulatory signal that AOD-9604 does not have a sanctioned place even within the compounding framework — and that the effectiveness gap this article describes is precisely what regulators flagged.
Anti-doping prohibition. The World Anti-Doping Agency has stated that AOD-9604 is prohibited in sport, falling under the categories covering growth hormone fragments, growth factors, and related substances.12 Athletes subject to WADA-compliant testing should assume that use constitutes an anti-doping rule violation, regardless of the compound’s clinical status.
The regulatory synthesis is straightforward: AOD-9604 occupies an ambiguous middle ground — not an approved drug, variously handled as a supplement ingredient, rejected for the U.S. compounding bulks list, and banned in sport — with no regulatory recognition of any therapeutic fat-loss use. Any legitimate exploration of the compound belongs in formal, authorized research, not in off-label or informal use marketed on the strength of a mechanism the pivotal trial failed to validate.
Reading the Evidence Honestly: A Tiered Summary
One reason confusion persists around AOD-9604 is that claims of very different evidentiary weight get repeated in the same breath, as though “it increases lipolysis in fat cells” and “it burns fat in people” sat on equal footing. They do not. It helps to sort the specific claims made about the compound by the strength of the evidence actually behind each one, because that sorting is what separates a careful reader from a marketing audience.
| Claim about AOD-9604 | Best supporting evidence | Honest evidence level |
|---|---|---|
| Stimulates lipolysis / fat oxidation in fat tissue | In-vitro and rodent metabolic studies1 | Moderate (preclinical, biochemical) |
| Chronic metabolic effect depends on β3-AR | β3-AR knockout-mouse study2 | Moderate (single clean animal study) |
| Does not raise IGF-1 or impair glucose tolerance | Metabolic and human safety studies14 | Reasonable (consistent across studies) |
| Short-term safety / good tolerability in adults | Human obesity trials; safety study4 | Reasonable (short-term, healthy-to-obese only) |
| Produces meaningful weight/fat loss in humans | Failed pivotal 24-wk RCT3 | Negative (definitive trial did not show it) |
| Effective long-term fat-loss therapy | None | Unproven / not demonstrated |
The gradient in that table is the entire point. As you move from “does something to fat cells in a dish” toward “reliably reduces a person’s body fat over time,” the evidence does not merely weaken — at the crucial final step it becomes actively negative, because the one trial built to test that step failed it.3 A responsible summary of AOD-9604 lives at the top of the table, where the preclinical and safety claims are defensible, and refuses to smuggle those defensible claims down to the bottom row where the fat-loss promise sits unsupported. When a vendor page cites the lipolysis mechanism and the “six clinical trials, 900 participants” safety record and then concludes “therefore, effective fat loss,” it is performing exactly the illegitimate slide the table is designed to expose: borrowing the credibility of the well-supported rows to underwrite the row that has none.
Limitations and the Honest Bottom Line
Pulling the threads together, the limitations that bear on the fat-burning question are substantial and mutually reinforcing.
The definitive human trial was negative. This is the load-bearing fact. AOD-9604’s pivotal, longest, best-controlled human study did not show statistically significant weight loss versus placebo, and development was halted as a result.3 Every optimistic account of the compound must be read against this, not around it.
The positive signal was early and fragile. The encouraging ~1.8 kg advantage came from a shorter study and did not survive replication in the longer one.3 Early-phase signals that vanish in pivotal trials are the rule, not the exception, in drug development; that is exactly why pivotal trials exist.
Mechanism is not outcome. The lipolytic, β3-linked mechanism is coherent and partly validated in rodents,12 but a mechanism that mobilizes fat in a mouse does not guarantee durable fat loss in a person, and in this case it did not deliver one.
Modern benchmarks are far higher. Against incretin agents producing 15–24% weight loss,678 a compound whose best human result was a non-durable sub-2-kilogram difference is not a competitive fat-loss agent by any current standard.
Sourcing and route uncertainty. The material sold today is subcutaneous research-chemical product of variable purity, dosed by convention rather than evidence, and unlike the oral formulation that was actually trialed — so even the failed trials do not directly characterize what people are currently using.
The honest bottom line is this. AOD-9604 is a real, purpose-built lipolytic peptide with a coherent mechanism, a reassuring short-term safety profile, and a genuine but ultimately disappointing human clinical record. Clinical trials do not indicate that it is an effective fat-burner in people; they indicate the opposite — that at its one properly powered, placebo-controlled test, it failed to separate from placebo. The compound remains a legitimate research tool for probing adipose biology and a candidate for further study under proper oversight. It is not a proven fat-loss therapy, it is not approved for weight loss anywhere, and responsible communication about it means resisting the pull of an appealing mechanism and stating plainly that the human efficacy evidence is, on the fat-burning question, negative rather than merely thin.
Frequently Asked Questions
Do clinical trials show that AOD-9604 burns fat in humans?
No, not convincingly. AOD-9604 went through roughly six human trials involving more than 900 participants, and an early ~12-week study (METAOD005) suggested about 1.8 kg more weight loss than placebo. But the pivotal, longer ~24-week study (METAOD006), a randomized double-blind placebo-controlled multicenter trial in about 500 subjects, did not reach statistical significance at its primary endpoint, and development was halted in 2007.3 The definitive human trial was negative, so the clinical trials do not support AOD-9604 as an effective human fat-burner.
How is AOD-9604 supposed to work?
It is a 16-amino-acid fragment of the C-terminal (residues 176–191) region of human growth hormone, engineered to reproduce the hormone’s fat-mobilizing signal while avoiding its other effects. It is thought to promote lipolysis (fat breakdown) and reduce lipogenesis (fat storage), with a chronic effect that depends on the β3-adrenergic receptor, as shown in a knockout-mouse study.12 Importantly, it was designed not to raise IGF-1 or impair glucose tolerance — a “cleaner” profile than full growth hormone, but one that has not translated into proven human fat loss.
Why did the pivotal AOD-9604 trial fail?
The 24-week pivotal trial applied an intensive diet-and-exercise regimen to all groups, including placebo. The lifestyle intervention worked well on its own, so the placebo group lost meaningful weight — a “floor effect” that left little room for the drug to show added benefit. Against that background, AOD-9604 produced no statistically significant extra weight loss.3 Whether one reads this as a masked effect or as a genuine lack of real-world benefit, the endpoint was not met and the program was discontinued.
How does AOD-9604 compare to semaglutide or tirzepatide?
There is no meaningful comparison in terms of demonstrated efficacy. Semaglutide produced roughly 15% mean weight loss in the STEP 1 trial and tirzepatide roughly 20–21% in SURMOUNT-1, both in large placebo-controlled studies.67 AOD-9604’s best human result was a non-durable sub-2-kilogram advantage that disappeared in its definitive trial.3 The incretin drugs are FDA-approved for weight management; AOD-9604 is not approved for anything.
Is AOD-9604 approved or legal?
It is not approved as a drug for weight loss or any condition by the FDA, EMA, or other major regulators. It has been handled as a supplement/food-type ingredient via a self-affirmed GRAS characterization (a safety framing, not efficacy or drug approval), was voted against for the FDA’s 503A compounding bulks list in December 2024, and is prohibited in sport by WADA.51112
Is AOD-9604 safe?
In the human obesity trials it was generally well tolerated over weeks-to-months, with no serious adverse events attributed to it and no reported rise in IGF-1 or impairment of glucose tolerance.14 However, that record covers short-term use in generally healthy-to-obese adults with an oral formulation. Long-term safety, the subcutaneous route used today, and the purity of research-chemical material are all uncharacterized or uncertain. A clean short-term safety profile does not imply efficacy.
What was the strongest evidence AOD-9604 does anything at all?
The best-supported mechanistic finding is that its chronic metabolic effects depend on the β3-adrenergic receptor, shown by a knockout-mouse study.2 Its clearest regenerative signal is in cartilage rather than fat: intra-articular injection improved cartilage scores in a rabbit osteoarthritis model.10 Neither result establishes clinically meaningful human fat loss.
Does the dose people use today match the trials?
No. The efficacy trials used oral dosing at roughly 0.25–30 mg daily, and low doses performed as well as high ones.3 The subcutaneous microgram doses common in research-chemical use today have no validated relationship to those trial doses, and no properly powered human trial has established that any subcutaneous regimen produces meaningful fat loss.
Could AOD-9604 still become an approved fat-loss drug?
It cannot be entirely ruled out, but it would require new, adequately powered human trials showing significant, durable weight loss — something its original program failed to achieve — and it would have to compete in an era where incretin drugs already deliver 15–24% weight loss.678 Realistically, a compound that could not beat placebo in its own pivotal trial faces a very steep path back.
References
- Ng FM, Sun J, Sharma L, et al. Metabolic studies of a synthetic lipolytic domain (AOD9604) of human growth hormone. Horm Res. 2000;53(6):274-278. PMID 11146367. https://pubmed.ncbi.nlm.nih.gov/11146367/
- Heffernan M, Summers RJ, Thorburn A, et al. The effects of human GH and its lipolytic fragment (AOD9604) on lipid metabolism following chronic treatment in obese mice and beta(3)-AR knock-out mice. Endocrinology. 2001;142(12):5182-5189. PMID 11713213. https://pubmed.ncbi.nlm.nih.gov/11713213/
- Stier H, Vos E, Kenley D. Safety and Tolerability of the Hexadecapeptide AOD9604 in Humans. J Endocrinol Metab. 2013;3(1-2):7-15 — the peer-reviewed pooled account of the AOD9604 human obesity program (six randomized, double-blind, placebo-controlled trials, >900 participants total), spanning the ~12-week METAOD005 and the pivotal ~24-week METAOD006 efficacy studies; the anti-obesity program was discontinued in 2007. https://www.jofem.org/index.php/jofem/article/view/157/194
- Stier H, Vos E, Kenley D. Safety and Tolerability of the Hexadecapeptide AOD9604 in Humans. Journal of Endocrinology and Metabolism. 2013;3(1-2):7-15. https://www.jofem.org/index.php/jofem/article/view/157
- Moré MI, Kenley D. Safety and Metabolism of AOD9604, a Novel Nutraceutical Ingredient for Improved Metabolic Health. Journal of Endocrinology and Metabolism. 2014;4(3):64-77. https://jofem.org/index.php/jofem/article/view/213/278
- Wilding JPH, Batterham RL, Calanna S, et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity (STEP 1). N Engl J Med. 2021;384(11):989-1002. PMID 33567185. https://pubmed.ncbi.nlm.nih.gov/33567185/
- Jastreboff AM, Aronne LJ, Ahmad NN, et al. Tirzepatide Once Weekly for the Treatment of Obesity (SURMOUNT-1). N Engl J Med. 2022;387(3):205-216. PMID 35658024. https://pubmed.ncbi.nlm.nih.gov/35658024/
- Jastreboff AM, Kaplan LM, Frías JP, et al. Triple-Hormone-Receptor Agonist Retatrutide for Obesity — A Phase 2 Trial. N Engl J Med. 2023;389(6):514-526. PMID 37366315. https://pubmed.ncbi.nlm.nih.gov/37366315/
- Rubino D, Abrahamsson N, Davies M, et al. Effect of Continued Weekly Subcutaneous Semaglutide vs Placebo on Weight Loss Maintenance in Adults With Overweight or Obesity (STEP 4). JAMA. 2021;325(14):1414-1425. PMID 33755728. https://pubmed.ncbi.nlm.nih.gov/33755728/
- Kwon DR, Park GY. Effect of Intra-articular Injection of AOD9604 with or without Hyaluronic Acid in Rabbit Osteoarthritis Model. Ann Clin Lab Sci. 2015;45(4):426-433. PMID 26275694. https://pubmed.ncbi.nlm.nih.gov/26275694/
- U.S. Food and Drug Administration. Pharmacy Compounding Advisory Committee (PCAC) Briefing Document, December 4, 2024 meeting (AOD-9604 review for Section 503A bulk drug substances list). https://www.fda.gov/media/183584/download
- World Anti-Doping Agency. WADA statement on substance AOD-9604. https://www.wada-ama.org/en/news/wada-statement-substance-aod-9604
Educational and research-use disclaimer: This article is provided solely for scientific and educational purposes. AOD-9604 is not approved by the FDA, EMA, or any comparable regulator for weight loss, obesity, or the treatment, cure, or prevention of any disease, and its pivotal human trial failed to demonstrate statistically significant fat loss versus placebo. Nothing here is medical advice or a recommendation for human use. AOD-9604 is prohibited in sport by WADA. Any legitimate investigation of this compound should occur within properly authorized preclinical or clinical research under appropriate oversight. Readers should consult qualified professionals and applicable regulations before making any decisions.