Research-use-only notice. This article is a research and landscape comparison for educational purposes. It is not medical advice, and it does not tell anyone which compound to take, whether to use any of them, or at what dose. Retatrutide is investigational and not approved by any regulator. Nothing here is a recommendation to obtain or use any peptide or drug.
It is tempting to rank these three by a single number — whoever produces the biggest weight-loss percentage wins. But that misses the most important difference: two of these are FDA-approved medicines with years of human data, and the third is still an investigational compound that no regulator has approved. Comparing them fairly means comparing not just how much the research shows, but how much research there is. Here is the honest three-way readout — mechanism, evidence stage, and what the trials actually found.
All three sit in the same broad family. If you want a foundation before going further, start with our explainer on what a GLP-1 is, and keep our peptide glossary open for terms like agonist, GIP, glucagon, and half-life. This piece is the hub that ties the landscape together; it deliberately sends the actual numbers you would need for anything hands-on to the relevant protocol pages.

The three contenders at a glance (and why “which is best” is the wrong question)
Takeaway: “Best” is unanswerable in the abstract, because these three are not at the same stage of proof. Semaglutide and tirzepatide are approved obesity medicines studied in tens of thousands of people. Retatrutide is an investigational triple agonist with promising mid-stage data and phase 3 trials still reading out. Ranking a fully evidenced drug against one that has not finished its pivotal program is comparing apples to a very interesting, unripe orange.
So instead of “which wins,” the useful questions are: How does each one work? How far along is the research? And what did the trials actually measure? Those are the axes this comparison runs on. A headline percentage is only meaningful once you know the trial it came from, the dose, the duration, and the population — which is why the same number can mean very different things across studies.
How each one works — mechanism side by side
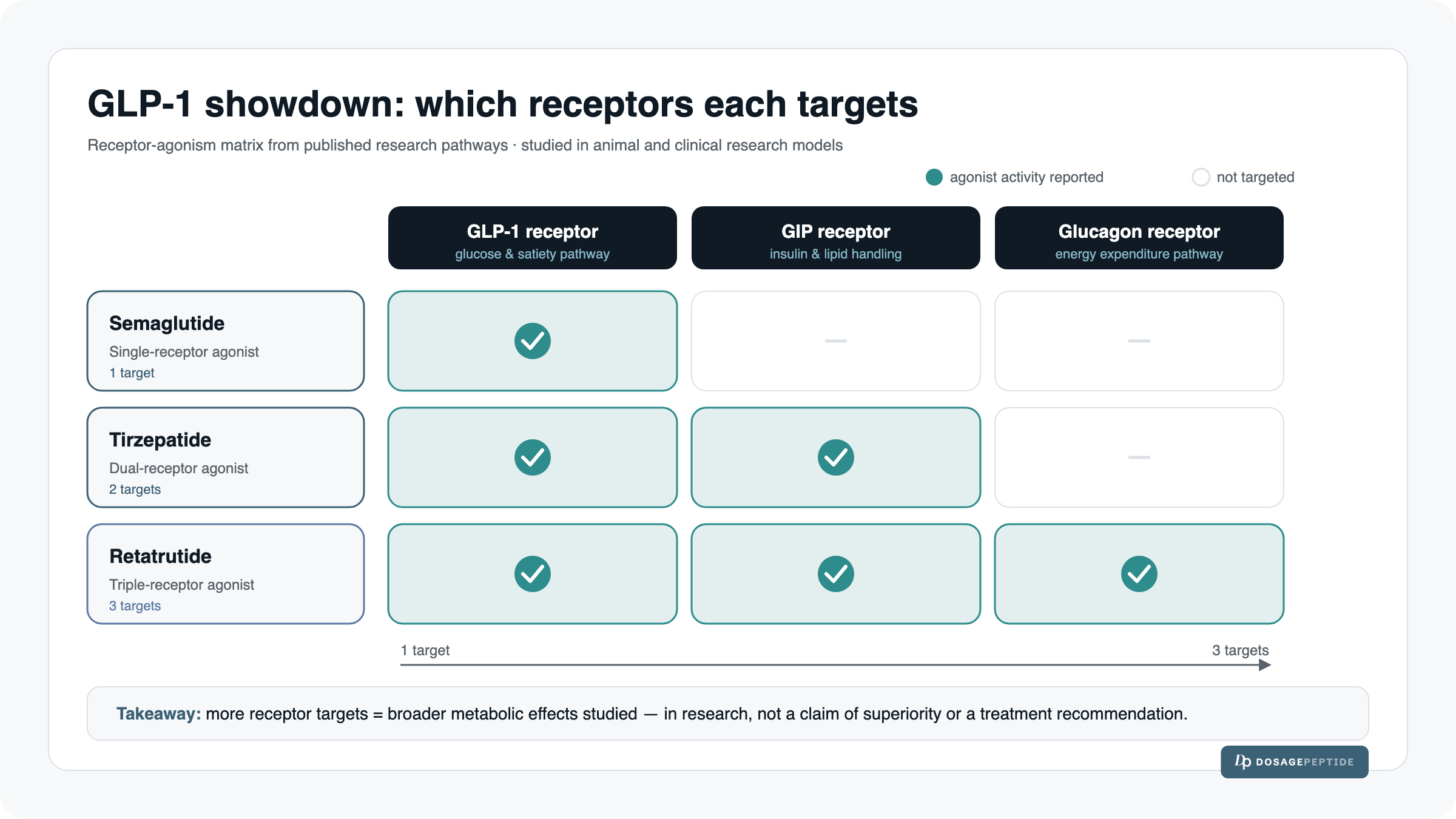
Takeaway: The three differ by how many gut-hormone receptors they engage. Semaglutide hits one, tirzepatide two, and retatrutide three. More receptor targets is the design theory behind the escalating trial numbers — but a mechanism on paper is a hypothesis about biology, not a guaranteed real-world outcome.
Semaglutide — single GLP-1 receptor agonist
Semaglutide is a single-agonist: it mimics glucagon-like peptide-1 (GLP-1), a hormone the gut releases after eating. By activating the GLP-1 receptor, it is understood to slow gastric emptying, increase satiety signaling, and improve glucose-dependent insulin release. It is the most established of the three in this category and, marketed as Wegovy, is FDA-approved for chronic weight management.
Tirzepatide — dual GIP + GLP-1 agonist
Tirzepatide adds a second target: glucose-dependent insulinotropic polypeptide (GIP), another incretin hormone, alongside GLP-1. The working theory is that engaging both incretin pathways produces complementary metabolic effects. Marketed as Zepbound for obesity (and Mounjaro for type 2 diabetes), it is FDA-approved and, like semaglutide, backed by large human trials.
Retatrutide — triple GIP + GLP-1 + glucagon agonist
Retatrutide goes one further, adding glucagon-receptor activity to GIP and GLP-1 — a “triple agonist.” The glucagon arm is hypothesized to raise energy expenditure in addition to the appetite and glycemic effects of the other two pathways. Retatrutide is investigational: it is not FDA-approved for any use, and its efficacy and long-term safety in people are still being established in ongoing trials. Every figure you will read about it below comes from research, not approved-use guidance.
The master comparison table (mechanism · research stage · regulatory status · headline trial result)
Takeaway: This table is the whole article in one view. Read the “regulatory status” and “head-to-head data” rows as carefully as the weight-loss row — they are what separate an approved medicine from a research candidate.
| Semaglutide | Tirzepatide | Retatrutide | |
|---|---|---|---|
| Receptor target | GLP-1 | GIP + GLP-1 | GIP + GLP-1 + glucagon |
| Drug-class shorthand | Single agonist | Dual agonist | Triple agonist |
| Regulatory status | FDA-approved for obesity (Wegovy) | FDA-approved for obesity (Zepbound) | Investigational — not approved |
| Most advanced research stage | Approved / post-marketing | Approved / post-marketing | Phase 3 (TRIUMPH) ongoing |
| Headline weight-loss result (trial · dose · duration) | −14.9% mean; STEP-1, 68 weeks | Up to −22.5%; SURMOUNT-1, 15 mg, 72 weeks | Up to −24.2%; phase 2, 12 mg, 48 weeks (topline phase 3 ~28% — see below) |
| Direct head-to-head data | Yes — vs. tirzepatide (SURMOUNT-5) | Yes — vs. semaglutide (SURMOUNT-5) | None yet |
Notice the trap the table defuses: retatrutide’s numbers look the biggest, but they carry the phrases “investigational,” “phase 2/topline,” and “none yet” beside them. The approved drugs’ numbers come with years of follow-up and a direct head-to-head. That context is the comparison.
What the studies actually show
Takeaway: Each drug’s headline number comes from a specific, named trial at a specific dose over a specific duration. Line them up and you will see why you cannot just read the three percentages as a leaderboard.
Semaglutide — the STEP program (STEP-1: −14.9% at 68 weeks)
In STEP-1, the pivotal obesity trial for semaglutide, adults with overweight or obesity lost a mean of −14.9% of body weight at 68 weeks, versus −2.4% for placebo, and 86% achieved at least 5% weight loss (Wilding et al., New England Journal of Medicine, 2021). This is mature, peer-reviewed human evidence from a large randomized trial — the kind of foundation retatrutide does not yet have.
Tirzepatide — the SURMOUNT program (SURMOUNT-1: up to −22.5% at 72 weeks)
SURMOUNT-1, tirzepatide’s pivotal obesity trial, reported dose-dependent mean weight reductions of −16.0%, −21.4%, and −22.5% at the 5, 10, and 15 mg doses over 72 weeks (Jastreboff et al., NEJM). That upper figure is why tirzepatide is often described as the more potent of the two approved options — a characterization that gained direct support in the head-to-head trial described further down.
Retatrutide — phase 2 NEJM (up to −24.2% at 48 weeks) and the 2025–2026 phase 3 TRIUMPH readouts
Retatrutide’s most-cited human data come from a phase 2 randomized trial (Jastreboff et al., NEJM, 2023; NEJMoa2301972), which enrolled 338 participants over 48 weeks. Least-squares mean weight changes were −8.7% (1 mg), −17.1% (4 mg), −22.8% (8 mg), and −24.2% (12 mg) versus −2.1% for placebo, and 83% of the 12 mg group achieved at least 15% loss.
Two caveats are essential and easy to miss. First, this is phase 2 — an earlier, smaller stage than the phase 3 trials that supported the approvals of the other two. Second, it ran 48 weeks, shorter than the 68–72-week approved-drug trials, so the −24.2% is not a like-for-like figure against the numbers above.
Moving into 2025–2026, retatrutide entered its phase 3 TRIUMPH program — roughly eight pivotal trials with about 5,800+ participants, plus a large cardiovascular-outcomes trial reported to enroll on the order of 10,000 patients. Topline releases have described TRIUMPH-1 at roughly 28.3% average weight loss at the 12 mg dose over 80 weeks, with about 45.3% of participants achieving at least 30% loss, and TRIUMPH-4 at approximately 28.7% over 68 weeks (Eli Lilly topline releases, with coverage in outlets such as AJMC and The Pharmaceutical Journal). These figures are promising, but they remain investigational: an FDA submission has been estimated for roughly Q4 2026–Q1 2027, and retatrutide is not yet approved. Topline company releases also precede full peer-reviewed publication, so treat them as preliminary until the complete trial reports are available.
Head-to-head where it exists: SURMOUNT-5 (tirzepatide vs. semaglutide)
Takeaway: There is exactly one direct, randomized head-to-head among these three, and it did not involve retatrutide. In SURMOUNT-5, tirzepatide outperformed semaglutide — but even this gold-standard comparison only speaks to two of the three.
SURMOUNT-5 (NEJM, 2025; NEJMoa2410819) was an open-label randomized trial of roughly 750 adults over 72 weeks that compared the two approved drugs directly. Tirzepatide produced a mean weight reduction of −20.2% versus −13.7% for semaglutide. About 50% of the tirzepatide group achieved at least 20% loss versus 27.3% on semaglutide, and roughly one-third versus 16.1% reached at least 25%.
Because both arms were studied in the same trial — same population, same duration — this is a genuine apples-to-apples result, the only one in this comparison. It is the reason “tirzepatide tends to outperform semaglutide” is a defensible research statement, while any claim about retatrutide relative to either remains an inference. For a closer look at the two-drug picture, see our deeper retatrutide vs. tirzepatide comparison.
Why there is NO head-to-head trial including retatrutide yet
No published randomized trial has directly compared retatrutide against tirzepatide or against semaglutide. Head-to-head trials typically arrive after a compound has cleared its own pivotal program; retatrutide is still in that program. Until such a trial is run and published, every retatrutide-versus-the-others number is a cross-trial comparison — different participants, doses, durations, and trial designs — and cannot be read as a true head-to-head. A −24.2% (or a topline ~28%) from a retatrutide trial and a −22.5% from SURMOUNT-1 were never measured against each other.
Research stage matters more than the headline number
Takeaway: The single most important variable here is not the weight-loss percentage — it is how much human evidence stands behind it. Approval reflects an accumulated safety and efficacy record that an investigational compound, by definition, does not yet have.
FDA-approved vs. investigational — what that means for evidence and safety data
Semaglutide (Wegovy) and tirzepatide (Zepbound) are FDA-approved for chronic weight management. Approval means each cleared phase 3 trials, underwent regulatory review of efficacy and safety, and now accumulates real-world, post-marketing data across large populations over years.
Retatrutide is investigational. Its phase 2 results are encouraging and its phase 3 topline numbers are eye-catching, but it has not completed the full regulatory process, its long-term safety profile in broad populations is still being characterized, and no regulator has authorized it for use. A larger short-term percentage from an earlier-stage trial does not outweigh the deeper, longer, regulator-reviewed evidence behind an approved drug. Stage is not a footnote to the comparison — it is arguably the comparison.
Side-effect profiles in the research (GI-dominant, discontinuation rates)
Takeaway: Efficacy never travels alone. Across all three, the most common adverse effects in trials were gastrointestinal, and tolerability differences show up in how many people stopped treatment.
In the trials, all three compounds were GI-dominant: the most frequently reported adverse effects were nausea, vomiting, diarrhea, and constipation, typically most pronounced during dose escalation. In SURMOUNT-5, discontinuation specifically due to GI adverse events was 2.7% on tirzepatide versus 5.6% on semaglutide — a tolerability signal alongside the efficacy difference. Retatrutide’s phase 2 data were likewise GI-dominant and, notably, showed a dose-dependent increase in heart rate, a signal that is part of why continued study of the triple agonist matters before any conclusions about its safety can be drawn. None of this is a tolerability verdict for any individual; it is a description of what the trials reported at a group level.
How to read cross-trial comparisons responsibly (different populations, doses, durations)
Takeaway: When trials were not run against each other, lining up their numbers is a rough sketch, not a scoreboard. Four variables quietly change what a percentage means.
Cross-trial literacy — read before ranking any numbers:
- Population. Baseline BMI, age, sex mix, and whether participants had type 2 diabetes all shift the results — trials that enroll different people are measuring different starting points.
- Dose. A drug’s “headline” number usually comes from its highest studied dose; comparing a top dose of one against a mid dose of another is not a fair match.
- Duration. A 48-week result and a 72-week result are not the same measurement — weight-loss curves are still changing at those timepoints.
- Trial design. Blinding, placebo vs. active comparator, lifestyle support, and dropout handling all move the numbers before the drug does.
When two drugs were compared inside one trial (as in SURMOUNT-5), those variables are controlled and the comparison is trustworthy. When they were not, treat any side-by-side percentage as directional at best.
Where to go deeper (hand-off to individual explainers and protocol pages)
Takeaway: This hub is the map; the detailed pages are the terrain. For anything specific — mechanism deep-dives or the numbers themselves — follow the links below rather than acting on figures in this overview.
- The two-drug picture in depth: our retatrutide vs. tirzepatide comparison.
- The individual explainers: what retatrutide is, what tirzepatide is, and how semaglutide works.
- Concept and terminology: what a GLP-1 is and the full peptide glossary.
- Research-context dosing information — not stated in this article by design — lives on the retatrutide dosage protocol page. Route every “how much / how often” question there.
- Handling references for research contexts: the peptide reconstitution guide and the dosage calculator.
Frequently asked questions
Which of the three produces the most weight loss in the research?
On the raw headline numbers, retatrutide’s trials show the largest percentages (phase 2 up to −24.2% at 48 weeks; phase 3 topline around 28%), followed by tirzepatide (up to −22.5% at 72 weeks) and semaglutide (−14.9% at 68 weeks). But those come from separate trials at different doses and durations, so they are cross-trial comparisons, not a true ranking. The only direct head-to-head — SURMOUNT-5 — found tirzepatide (−20.2%) ahead of semaglutide (−13.7%).
Is retatrutide “better” than the other two?
The research cannot answer that yet. Retatrutide is investigational, has no head-to-head trial against either approved drug, and its phase 3 program is still reporting out. Larger early-stage percentages do not outweigh the deeper, regulator-reviewed evidence behind semaglutide and tirzepatide.
Are all three FDA-approved?
No. Semaglutide (Wegovy) and tirzepatide (Zepbound) are FDA-approved for chronic weight management. Retatrutide is investigational and not approved for any use; an FDA submission has been estimated for roughly late 2026 to early 2027, but timelines can change.
Has retatrutide ever been tested directly against tirzepatide or semaglutide?
Not in any published randomized trial. Every retatrutide-versus-the-others figure is a cross-trial comparison. SURMOUNT-5 is the only direct head-to-head among the three, and it compared tirzepatide with semaglutide only.
What are the main side effects seen in the trials?
All three were GI-dominant in the research — nausea, vomiting, diarrhea, and constipation were the most common adverse effects, usually worst during dose escalation. Retatrutide’s phase 2 data additionally showed a dose-dependent heart-rate increase. This is group-level trial data, not a personal safety assessment.
Where can I find dosing information?
Not in this article — by design. Research-context dosing details are handed off to the retatrutide dosage protocol page, and general handling is covered in the peptide reconstitution guide and dosage calculator. None of that is a recommendation to use any compound.
The bottom line — research-use-only, not medical advice
Takeaway: The fair reading is not “retatrutide wins.” It is that semaglutide and tirzepatide are approved medicines with mature human evidence and a direct head-to-head (tirzepatide ahead), while retatrutide is an investigational triple agonist whose early numbers are striking but whose story is not finished. Stage of evidence, trial design, and cross-trial caveats matter more than any single percentage.
This has been a comparison of the research landscape — mechanism, evidence stage, regulatory status, and what named trials found. It is explicitly not a recommendation of which compound to take, whether to take any of them, or at what dose. If you are weighing metabolic-health decisions, that is a conversation for a qualified healthcare professional who knows your history — not a blog comparison.
References
- Wilding JPH, et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity (STEP-1). New England Journal of Medicine, 2021 (NEJMoa2032183). — Semaglutide −14.9% at 68 weeks.
- Jastreboff AM, et al. Tirzepatide Once Weekly for the Treatment of Obesity (SURMOUNT-1). New England Journal of Medicine. — Tirzepatide up to −22.5% at 72 weeks.
- Jastreboff AM, et al. Triple–Hormone-Receptor Agonist Retatrutide for Obesity — Phase 2 Trial. New England Journal of Medicine, 2023 (NEJMoa2301972). — Up to −24.2% at 48 weeks; n=338.
- SURMOUNT-5: Tirzepatide vs. Semaglutide head-to-head trial. New England Journal of Medicine, 2025 (NEJMoa2410819; PubMed 40353578). — Tirzepatide −20.2% vs. semaglutide −13.7% at 72 weeks.
- Eli Lilly TRIUMPH phase 3 topline releases, with coverage in AJMC and The Pharmaceutical Journal (TRIUMPH-1 ~28.3%; TRIUMPH-4 ~28.7%) — retatrutide research-stage/status.
- ClinicalTrials.gov — TRIUMPH program registrations (phase 3 ongoing; ~5,800 participants across pivotal trials plus a cardiovascular-outcomes trial).
- U.S. Food and Drug Administration — approval status: semaglutide (Wegovy) and tirzepatide (Zepbound) approved for chronic weight management; retatrutide investigational and not approved.
Disclaimer: This article is for informational and research-use-only purposes and is not medical advice. It does not diagnose, treat, or recommend any product, and it does not tell any reader which compound to use or at what dose. Retatrutide is investigational and not approved by the FDA or any regulator; semaglutide and tirzepatide are prescription medicines. Products referenced by research-supply vendors are intended for laboratory and research use only and not for human consumption. Trial percentages are group-level research findings from specific studies and do not predict any individual outcome. Always consult a qualified healthcare professional before making any health decision.