Almost everything written about retatrutide leads with the headline: up to roughly 24% body-weight reduction in its Phase 2 trial, one of the largest figures ever reported for an investigational obesity drug candidate. Far less gets said about the other side of that same trial. At the top dose studied, roughly 6 in 10 participants reported nausea. That is not a reason to panic, and it is not a reason to dismiss the molecule either, but it is the number you actually need in order to understand retatrutide’s safety picture.
This article walks through what the published clinical research reports about retatrutide’s side effects: which ones are common, which are dose-dependent, which tend to fade, and which are still genuinely unknown because the long-term trials are not finished. It is a research summary, not a how-to. Retatrutide is an investigational compound. It is not FDA-approved for any use, and nothing here is medical advice or a guide to taking it.
Research-use-only notice. The information below summarizes published clinical trial data for educational and research purposes only. It is not medical advice, not a recommendation to use retatrutide, and not a dosing guide. Retatrutide is an investigational drug that has not been approved by the FDA. Consult a qualified clinician before making any personal health decision.

The honest summary: retatrutide’s side-effect profile in one paragraph
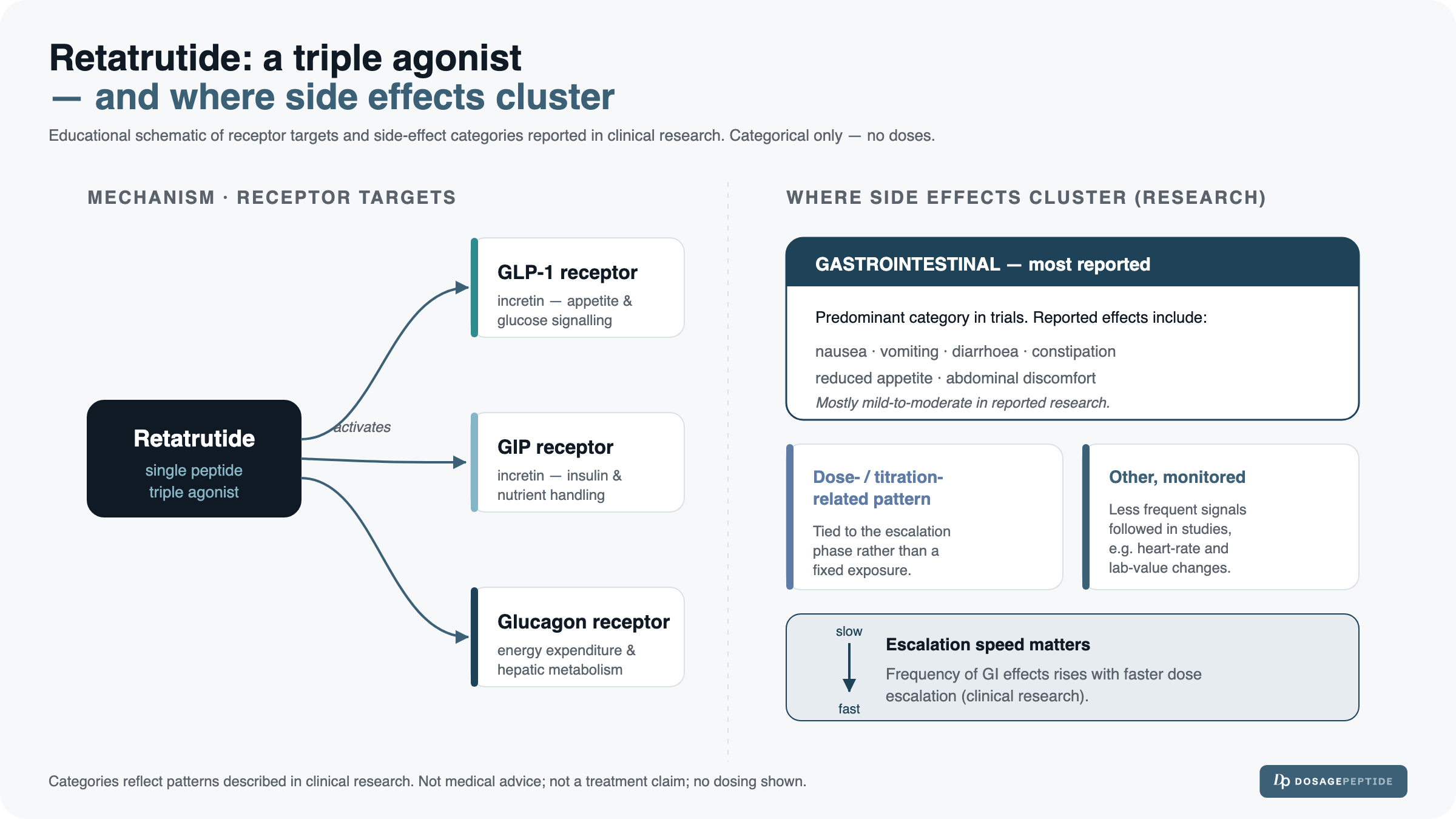
In the Phase 2 evidence available so far, retatrutide’s side effects are overwhelmingly gastrointestinal, clearly dose-dependent, and mostly rated mild-to-moderate. Nausea, vomiting, diarrhea, and constipation are the most frequently reported events, and they cluster during the period when the dose is being escalated. Beyond the gut, the most-watched signal is a modest increase in resting heart rate at higher doses. Serious adverse events were relatively uncommon in the reported short-term data, and no drug-related deaths were highlighted. The large caveat is duration: these findings come from a 48-week Phase 2 trial in a screened population, so the long-term human safety profile remains unestablished pending later-stage results.
What retatrutide is, in one paragraph
Retatrutide is a single-molecule triple-receptor agonist, engineered to activate three metabolic pathways at once: the GIP, GLP-1, and glucagon receptor systems. That triple action is what distinguishes it from the dual GIP/GLP-1 agonist tirzepatide and the single GLP-1 agonist semaglutide, and it is the mechanism researchers believe underlies the large weight-change figures reported in early trials. For the full mechanism and background, see our full retatrutide overview. The point that matters for a safety article: retatrutide is investigational and not FDA-approved, so every figure below describes what happened in a controlled trial, not an established real-world profile.
Where this data comes from: the Phase 2 evidence base
The anchor for the numbers in this article is the published Phase 2 obesity trial: Jastreboff AC, Kaplan LM, Frías JP, and colleagues, “Triple–Hormone-Receptor Agonist Retatrutide for Obesity — A Phase 2 Trial,” published in the New England Journal of Medicine in 2023. It was a randomized, double-blind, placebo-controlled study of 338 adults with obesity, run over 48 weeks, testing weekly subcutaneous doses of 1, 4, 8, and 12 mg against placebo. A separate Phase 2 trial in adults with type 2 diabetes, reported by Rosenstock and colleagues in The Lancet in 2023, offers corroborating signals on the gastrointestinal and heart-rate findings.
Trial-sourced numbers matter here because the alternative — forum anecdotes and vendor claims — cannot tell you how common an effect is, whether it tracked with dose, or how it compared to placebo. A placebo-controlled trial can. Where this article states a percentage, it comes from that published trial data; where a claim reflects a broader drug class rather than retatrutide specifically, that distinction is made explicit.
The most common side effects are gastrointestinal, with the actual trial percentages
Gastrointestinal events were the dominant side-effect category in the Phase 2 obesity trial, and their frequency rose with dose. The table below summarizes the adverse-event rates the trial reported at the 12 mg weekly dose, the highest studied, alongside placebo for context.
| Side effect (as reported) | Placebo | 12 mg weekly (highest dose) |
|---|---|---|
| Nausea | ~9% | ~60% |
| Vomiting | ~2% | ~26% |
| Diarrhea | ~9% | ~15% |
| Constipation | ~6% | ~16% |
Source: Jastreboff et al., NEJM 2023 (Phase 2 obesity trial, n=338). Percentages are approximate, reflect the highest-dose group, and are rounded.
The trial reported a clear dose-dependent gradient rather than a flat rate. Nausea, for example, rose from roughly 14% of participants at the lowest 1 mg dose toward roughly 60% at the 12 mg dose. Importantly, the study characterized these gastrointestinal events as predominantly mild-to-moderate in severity, and they were concentrated during the dose-escalation phase rather than persisting evenly across the whole 48 weeks.
Nausea, vomiting, diarrhea, constipation: the dose-dependent pattern
The practical takeaway from the trial data is that the higher the dose group, the more likely a participant was to report a gut-related event, and nausea was consistently the single most common complaint. Vomiting was less frequent than nausea but still notably more common at the top dose than on placebo. Diarrhea and constipation appeared at both ends of the spectrum, which is typical of how the broader GLP-1 receptor-agonist class affects gastrointestinal motility. None of this establishes what any individual would experience; it describes the distribution across a trial population.
Why side effects cluster during dose escalation
The reason these events concentrate early is the titration design itself. In the trial, participants did not start at their target dose; they stepped up gradually. Tolerance to the gastrointestinal effects of receptor agonists in this class tends to build over time, so the window when the dose is being raised is also the window when nausea and vomiting are most likely to appear, then ease. This is why the investigators emphasized that gastrointestinal events were front-loaded around escalation. It is also precisely the kind of detail that turns into a dosing question, and dosing is not something this article will answer. How the research doses are structured and stepped up is covered on the retatrutide dosage protocol page, not here.
Cardiovascular signals: the heart-rate question
After the gut, the most discussed retatrutide safety signal is its effect on heart rate. This is worth understanding precisely, because it is easy to overstate in either direction.
The resting heart-rate increase: size and time course
The Phase 2 obesity trial reported a mean increase in resting heart rate of roughly 5 to 7 beats per minute at the higher doses. Just as important as the size is the time course: the increase peaked around week 24, then declined toward weeks 36 to 48. In other words, the trial data described a heart-rate signal that rose and then partially settled over the study period rather than climbing continuously. An increase in heart rate is a recognized feature of the GLP-1 receptor-agonist class generally, so this finding is consistent with what has been seen in related molecules, but the magnitude and trajectory here are specific to what this trial measured.
Blood pressure, and why the trials excluded people with significant cardiovascular disease
Alongside the heart-rate data, the trial tracked blood pressure, and reductions in blood pressure have been reported in this class as weight decreases. The critical context, however, is who was studied. The Phase 2 program excluded participants with significant cardiovascular disease. That exclusion is standard for early-phase trials, but it has a direct consequence for interpretation: the trial cannot tell us how retatrutide behaves in people with established heart disease, because those people were not enrolled. Class-level cardiovascular safety for retatrutide is therefore not yet established, and readers should not generalize the reassuring short-term signals to populations the trial deliberately left out.
Metabolic and other signals
Beyond the gut and the heart, the trial and the class literature point to several other effects worth noting, again framed as trial observations rather than established outcomes:
- Glucose effects. Consistent with its mechanism, retatrutide lowered glucose measures in study participants; the diabetes Phase 2 trial reported meaningful reductions in blood-sugar markers. Because glucagon-receptor activity can influence glucose, it is one of the parameters monitored in the ongoing research program.
- Appetite and energy-intake reduction. The weight change is driven largely by reduced food intake, a shared feature of receptor agonists in this family. This is a mechanism of action, not a side effect, but it explains why nausea and reduced appetite often travel together.
- Injection-site reactions. As a subcutaneously injected compound, injection-site reactions were among the reported events, generally minor in the trial data.
- Gallbladder-related events. Gallbladder and biliary events are a recognized consideration across the GLP-1 receptor-agonist class, often linked to rapid weight loss. This is discussed further below as a class-level consideration rather than a confirmed retatrutide-specific outcome.
Discontinuations: how many people stopped because of side effects
A useful way to gauge how tolerable a drug was in a trial is to ask how many participants stopped taking it because of adverse events. In the Phase 2 obesity trial, discontinuations attributed to adverse events were reported in a single-digit percentage range. The trial reported this as an observed figure in a specific study population, so it is best read as “this is what happened in this trial” rather than a precise universal rate that will hold everywhere.
Two further points from the reported data: the trial did not highlight any drug-related deaths, and it did not report unexpected serious safety signals over its 48 weeks. Both are genuinely reassuring within the limits of the study, but those limits are the whole point. This is short-term data from a screened population, so the absence of a signal over 48 weeks is not the same as a clean long-term safety record.
Serious adverse events, and what the trial could and couldn’t rule out
Serious adverse events did occur in the trial, as they do in essentially every study of an active drug, but the published Phase 2 report did not describe an unexpected pattern of serious harm tied specifically to retatrutide over the study period. What a 48-week Phase 2 trial with a few hundred participants can do is characterize common and moderately common events and flag obvious safety signals. What it cannot do is reliably detect rare events, or effects that only emerge after years of exposure. Rare adverse events, by definition, need much larger and longer trials to surface. That gap between “no signal seen so far” and “proven safe long-term” is the single most important idea for a reader evaluating retatrutide’s safety honestly.
The big caveat: what we still don’t know
Everything above comes from Phase 2. The larger, longer Phase 3 program, known as TRIUMPH, and the cardiovascular-outcomes work associated with it were still underway, with full long-term results pending as of writing. That means several things remain genuinely unknown:
- Long-term human safety beyond roughly a year of exposure has not been characterized.
- Cardiovascular outcomes — not just the heart-rate number, but hard endpoints like cardiovascular events — are the subject of dedicated ongoing study and are not yet established.
- Excluded populations — most notably people with significant cardiovascular disease — were not represented in the Phase 2 data, so findings cannot be extended to them.
Until those data mature, retatrutide’s safety story is genuinely incomplete, and any confident long-term claim, positive or negative, runs ahead of the evidence.
GLP-1 class context: what applies to the family, not necessarily to retatrutide
Because retatrutide acts partly through the GLP-1 receptor, it is reasonable to look at what regulators and labels flag for the broader GLP-1 receptor-agonist class. These are class-level considerations under study for retatrutide, not confirmed retatrutide-specific outcomes, and the distinction matters:
- Gallbladder events. FDA and EMA labeling for approved GLP-1 receptor agonists notes gallbladder-related events, often associated with rapid weight loss.
- Pancreatitis monitoring. Pancreatitis is monitored across the class, and approved-drug labeling advises attention to it, though a causal picture specific to retatrutide has not been established in the published trial data.
- Thyroid C-cell / MTC boxed warning. Several approved GLP-1 receptor agonists carry a boxed warning related to thyroid C-cell tumors and medullary thyroid carcinoma, based largely on rodent data. This is class-level regulatory context, not a demonstrated retatrutide-specific finding, and it is one of the questions later-stage research is positioned to address.
Transient vs. persistent: a quick framing
Effects that typically faded in the trial (mostly during titration): nausea, vomiting, diarrhea, and constipation. These were front-loaded around dose escalation and were characterized as predominantly mild-to-moderate.
Effects monitored over a longer horizon: resting heart rate (rose, then partially declined by weeks 36–48), glucose parameters, and the class-level considerations above. These are the signals that longer trials are designed to track.
How tolerability was managed in the trials, and where dosing questions belong
In the clinical trials, the main lever used to manage tolerability was the gradual dose-escalation schedule described earlier — the reason gastrointestinal events clustered early and then eased. That is a description of trial design, not a personal protocol. This article deliberately does not tell anyone what dose to use, how to titrate, or how to medically manage side effects, because those are clinical decisions that depend on an individual and belong with a qualified professional. For how the research doses are structured and reconstituted, see the retatrutide dosage protocol. If you are working with a vial in a research context, our reconstitution guide and dosage calculator cover the mechanics of preparing and calculating concentration — again, as reference tools, not as medical instruction.
The context anchor: reading safety against efficacy
Side-effect data only means something next to what the drug was doing. For context, the Phase 2 obesity trial reported a mean body-weight reduction of about 24.2% at the 12 mg dose versus about 2.1% on placebo at 48 weeks. That is context, not the focus of this article and not a dosing endorsement, but it explains why the drug is being studied so intensively despite a demanding gastrointestinal profile. A high nausea rate reads differently against a large, sustained metabolic effect than it would against a marginal one. Both numbers come from the same trial, and an honest safety read holds them together.
Bottom line
On the published evidence, retatrutide is a powerful investigational agent with a predominantly gastrointestinal, dose-driven side-effect profile and an incomplete long-term record. The common events — nausea above all — were frequent at higher doses but mostly mild-to-moderate and concentrated during escalation. The heart-rate signal was modest and partially self-limiting over the trial. Serious harms were not flagged as an unexpected pattern in Phase 2, but Phase 2 is short and screened. Retatrutide remains investigational and is not FDA-approved, its Phase 3 (TRIUMPH) and cardiovascular-outcome data were still pending as of writing, and its long-term safety is not yet known. This is not a guide to taking retatrutide, and no one should read it as one.
FAQ
Does retatrutide cause nausea?
In the Phase 2 obesity trial (Jastreboff et al., NEJM 2023), nausea was the most commonly reported side effect and was dose-dependent, reported by roughly 60% of participants at the highest 12 mg dose versus about 9% on placebo. The trial characterized it as predominantly mild-to-moderate and concentrated during dose escalation.
Is retatrutide safe?
The short-term Phase 2 data did not highlight unexpected serious safety signals or drug-related deaths, but that is not the same as being established as safe. Retatrutide is investigational, long-term and cardiovascular-outcome data are still pending, and the trials excluded people with significant cardiovascular disease. Safety in the full sense has not yet been established, and any decision about it is a matter for a qualified clinician.
Does retatrutide raise heart rate?
The Phase 2 trial reported a mean resting heart-rate increase of roughly 5 to 7 bpm at higher doses, peaking around week 24 and then declining toward weeks 36 to 48. An increase in heart rate is a recognized feature of the GLP-1 receptor-agonist class.
Is retatrutide FDA approved?
No. Retatrutide is an investigational drug and is not approved by the FDA for any use. Its Phase 3 TRIUMPH program and associated cardiovascular-outcome studies were still ongoing as of writing.
How does retatrutide compare to tirzepatide on side effects?
Both are gastrointestinal-dominant. Because no trial has directly compared them head-to-head, any comparison draws on separate trials with different populations and doses and should be read cautiously. For a fuller side-by-side, see retatrutide vs tirzepatide.
References
- Jastreboff AC, Kaplan LM, Frías JP, et al. Triple–Hormone-Receptor Agonist Retatrutide for Obesity — A Phase 2 Trial. N Engl J Med. 2023;389(6):514–526. doi:10.1056/NEJMoa2301972.
- Rosenstock J, et al. Retatrutide, a GIP/GLP-1/glucagon receptor triple agonist, in adults with type 2 diabetes: a randomized, double-blind, placebo-controlled and active-comparator, parallel-group Phase 2 trial. The Lancet. 2023.
- ClinicalTrials.gov. Retatrutide Phase 3 (TRIUMPH) program listings — supporting the pending long-term and cardiovascular-outcome status.
- U.S. Food and Drug Administration and European Medicines Agency labeling for GLP-1 receptor agonists — cited for class-level context (gallbladder events, pancreatitis monitoring, and the thyroid C-cell / medullary thyroid carcinoma boxed warning), distinguished from retatrutide-specific proven outcomes.
- Published Phase 2 safety analyses and clinical reviews summarizing dose-dependent adverse-event rates for retatrutide.
Disclaimer: This article is for research and educational purposes only. It is not medical advice and is not a recommendation to use retatrutide or any other compound. Retatrutide is an investigational drug that is not approved by the FDA, and products referenced on this site are intended for laboratory and research use only, not for human consumption. Nothing here should be used to diagnose, treat, or prevent any condition, and no dose or self-management strategy is prescribed. Always consult a qualified healthcare professional before making any personal medical decision.