Ask around in any peptide forum and three names surface again and again: KLOW, GLOW, and Wolverine. They are spoken about the way brand names are — as if each were a single, well-characterized product with a known effect — when in reality all three are informal, community-coined combinations of individual research peptides sold by dozens of unrelated vendors at wildly varying ratios. None of them is a drug. None of them has been approved by the U.S. Food and Drug Administration, the European Medicines Agency, or any comparable regulator for any indication. None has ever been tested as a fixed-combination product in a controlled human trial. What people are really comparing when they debate “KLOW vs GLOW vs Wolverine” is not three medicines but three different recipes built from an overlapping shortlist of four peptides — BPC-157, TB-500, GHK-Cu, and KPV — each of which carries its own, mostly preclinical, evidence base.
This article takes the comparison seriously without pretending the blends are something they are not. The honest way to answer “which blend is discussed for what goal?” is to break each blend down into its components, look at what is actually known about each component, and then be candid about a fact that is easy to lose in the marketing: combining peptides does not combine their evidence. Two compounds each supported only by rodent studies do not, when mixed in a vial, produce a therapy supported by human data. If anything, stacking makes the evidence question harder, because now there are interaction effects, dosing uncertainties, and purity risks layered on top of compounds that were already investigational on their own.
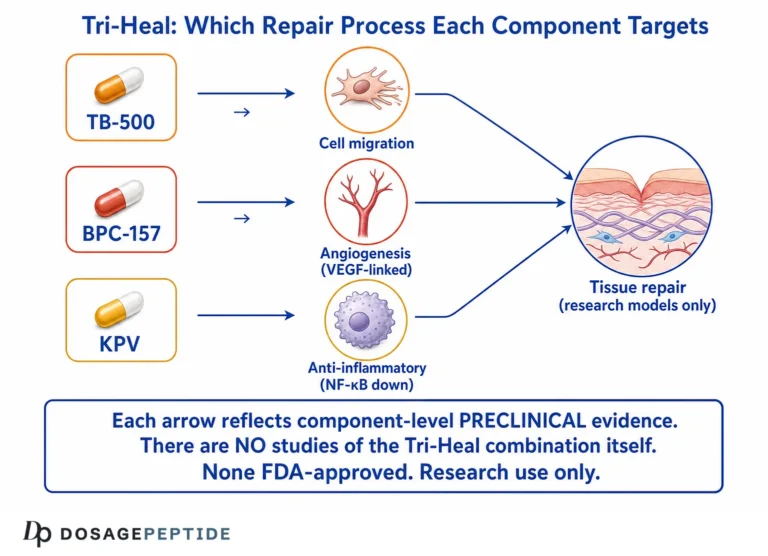
So the goal here is a map, not a sales pitch. We will define what KLOW, GLOW, and Wolverine actually contain; explain the shared “recovery backbone” of BPC-157 and TB-500 that all three are built around; examine what GHK-Cu and KPV add; lay the three recipes side by side against the goals communities discuss for them; walk through the real evidence for each ingredient (which ranges from genuine human trials for one component to animal-only data for others); and then spend real time on what the evidence does not show. Throughout, the framing is deliberate: these are compounds that people discuss for certain goals, not compounds that have been proven to achieve them.
What KLOW, GLOW, and Wolverine Actually Are
Start with the vocabulary, because the names themselves cause confusion. KLOW, GLOW, and Wolverine are nicknames that emerged from the peptide-optimization community and were then adopted, quite literally, as product titles by research-chemical vendors. They are not trademarks, not standardized formulations, and not clinical entities. Two vials labeled “GLOW” from two different suppliers may contain the same three peptides in noticeably different proportions.
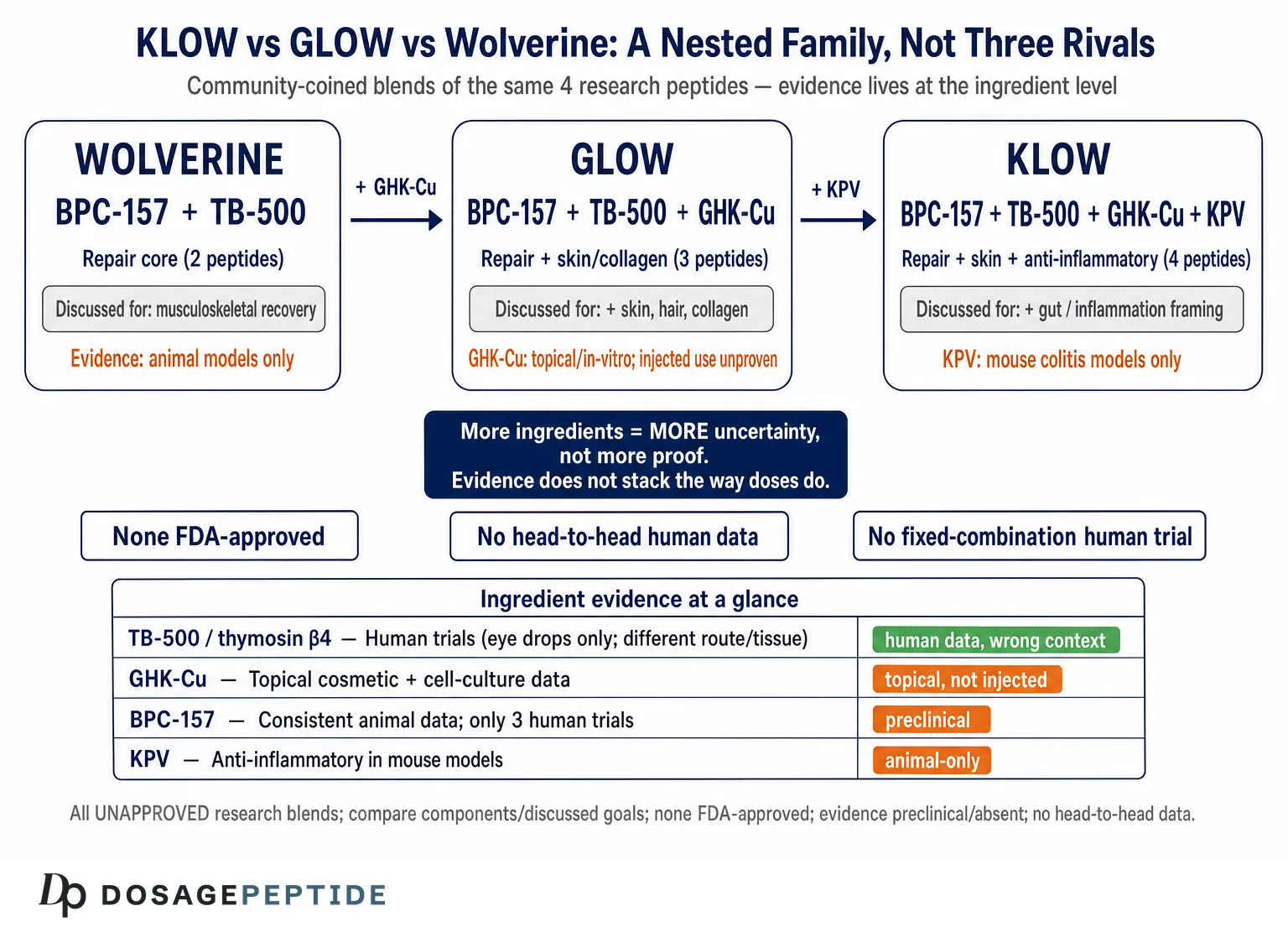
Wolverine is the simplest and the origin point. It refers to a two-peptide pairing of BPC-157 and TB-500, typically sold as roughly 10 mg of each per vial. The name is a nod to the Marvel character’s rapid self-healing — a piece of pop-culture branding, not a scientific claim. In practice, “Wolverine stack” is shorthand for “the two recovery peptides people combine most often.”
GLOW takes that same recovery pairing and adds GHK-Cu, the copper tripeptide most associated with skin and collagen. A representative GLOW blend is described as a three-peptide, roughly 50–70 mg vial in a ratio on the order of BPC-157 5 mg, TB-500 10 mg, and GHK-Cu 35–50 mg — the copper component dominating the mass. The powder often has a faint blue tint, which comes directly from the copper. The name “GLOW” signals the intended emphasis: the addition of GHK-Cu shifts the discussed goals toward skin, hair, and cosmetic appearance on top of tissue repair.
KLOW is GLOW plus a fourth peptide, KPV — a small anti-inflammatory tripeptide derived from a fragment of alpha-melanocyte-stimulating hormone (α-MSH). A typical KLOW is marketed as an 80 mg four-peptide blend: GHK-Cu 50 mg, BPC-157 10 mg, TB-500 10 mg, and KPV 10 mg. The extra letter (“K” for KPV) is the only difference in the acronym, and the extra peptide is the only difference in the vial. KLOW is therefore best understood as the “most loaded” of the three — the recovery backbone, the copper cosmetic peptide, and an inflammation-focused tripeptide, all in one.
Seen this way, the three blends form a tidy nested hierarchy rather than three unrelated products. Wolverine is the two-peptide core (repair). GLOW is Wolverine plus one (repair plus skin/collagen). KLOW is GLOW plus one more (repair plus skin plus anti-inflammatory). Every question about which blend suits which discussed goal reduces, in the end, to what each added ingredient contributes and whether that ingredient has any evidence behind it. It also means the blends are not really competitors in the way “drug A vs drug B” would be; they are points on a single spectrum of increasing complexity. That nested structure will matter later, because each added peptide also adds a new layer of uncertainty.
The Shared Backbone: BPC-157 and TB-500
Because all three blends contain both BPC-157 and TB-500, understanding this pair is the single most useful thing a reader can do. These two peptides are the reason the community groups these blends together at all, and they carry most of the “recovery and repair” reputation that the blends trade on.
BPC-157 is a synthetic pentadecapeptide — a chain of 15 amino acids — corresponding to a partial sequence of a protein identified in human gastric juice. It was first characterized by Sikiric and colleagues at the University of Zagreb, who were investigating why the stomach lining tolerates such a harsh environment. In animal models, BPC-157 has shown a striking breadth of regenerative and cytoprotective effects. It has accelerated healing of transected tendons and ligaments in rats when given by several routes, improved muscle and bone-to-tendon junction recovery, and protected gut tissue in ulcer and colitis models.23 The proposed mechanisms include promotion of angiogenesis (new blood-vessel formation), effects on the nitric-oxide system, and stimulation of fibroblast outgrowth and cell migration through signaling pathways such as FAK-paxillin.2 For a broader primer on the compound’s biology, the site’s explainer on what BPC-157 is lays out the pentadecapeptide story in more depth.
The crucial honesty here is the evidence level. A 2025 narrative review that searched six databases through March of that year found robust regenerative signals in preclinical work but only three published human clinical trials of BPC-157 — and concluded that the compound should still be considered investigational, noting the anti-doping and compounding restrictions that regulators had applied over the lack of human safety data.1 In other words, the impressive-sounding “heals everything” reputation rests almost entirely on rodents. That is not nothing — consistent effects across many animal models and delivery routes are a legitimate reason for scientific interest — but it is a long way from demonstrated efficacy in humans.
TB-500 is the other half of the backbone, and it comes with an important labeling subtlety. It is marketed as thymosin beta-4 (Tβ4), a naturally occurring 43-amino-acid actin-sequestering protein present in nearly all cell types and heavily involved in cell migration, angiogenesis, and tissue repair.4 But “TB-500” as sold in research channels is frequently a synthetic fragment of that protein rather than the full-length molecule — anti-doping chemists describe it as corresponding to a short active region of Tβ4. This distinction matters: the human clinical evidence that exists belongs to full-length thymosin beta-4 (developed as the pharmaceutical candidate RGN-259), not necessarily to the abbreviated peptide in a research vial. Conflating the two lets marketing borrow the credibility of genuine trials for a compound that may not be chemically identical.
What Tβ4 does have, uniquely among the four ingredients, is real human trial data — but for the eye, not for muscle. Thymosin beta-4 ophthalmic solution improved signs and symptoms of severe dry eye in a randomized phase 2 trial and promoted corneal healing in a randomized, placebo-controlled, double-masked phase 3 trial in neurotrophic keratopathy.56 Those are legitimate, well-designed studies. They are also about a topical eye drop for a corneal-surface disease — a completely different tissue, route, and indication from the systemic musculoskeletal recovery that TB-500 is sold for. The systemic tendon-and-muscle applications people actually stack it for remain preclinical and, in humans, unproven.
The logic of pairing the two is intuitive and is repeated everywhere: BPC-157 is cast as creating the conditions for healing (vascular supply, growth-factor signaling) while TB-500 mobilizes the cells that carry out repair. It is a tidy narrative, and it is biologically plausible. But plausible is the operative word. There is no controlled human trial of the BPC-157 + TB-500 combination, no head-to-head data, and no evidence that the pairing outperforms either peptide alone or, more to the point, outperforms nothing. The pairing is a hypothesis that many people have adopted as a conclusion.
What GHK-Cu Adds to GLOW and KLOW
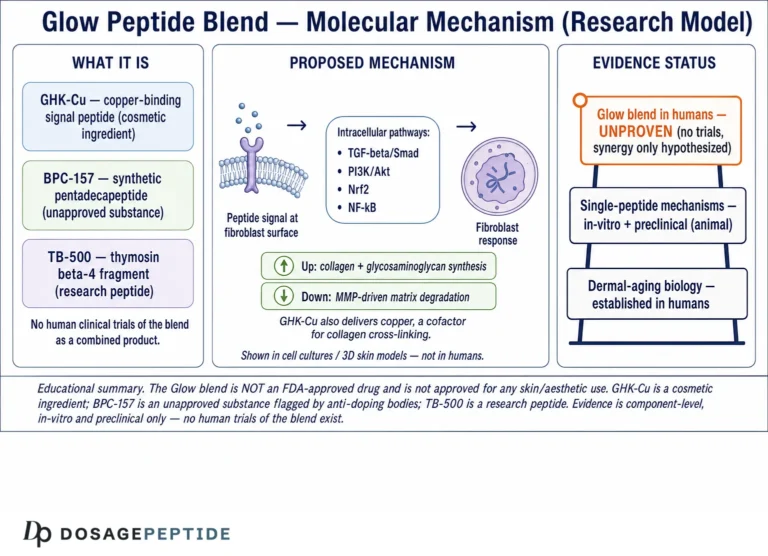
The step from Wolverine to GLOW is the addition of GHK-Cu, and it changes the character of the blend. GHK-Cu is the tripeptide glycyl-L-histidyl-L-lysine bound to a copper(II) ion. It was first isolated from human plasma in 1973 by Loren Pickart, who observed that a factor in human albumin could make aged liver tissue behave more like young tissue. Plasma levels of GHK are reported to fall with age — roughly 200 ng/mL around age 20 declining to about 80 ng/mL by 60 — a decline that parallels the body’s waning regenerative capacity.7
Of the four peptides in these blends, GHK-Cu has the most substantial cosmetic and dermatological evidence base, though it is important to be precise about what that evidence is. In fibroblast cultures, GHK-Cu stimulates the synthesis of collagen and other extracellular-matrix components; gene-expression studies suggest it can influence a large number of human genes, tilting expression toward tissue remodeling, antioxidant defense, and DNA repair.78 In topical skincare, copper-peptide formulations have shown improvements in skin firmness, elasticity, and the appearance of fine lines in a number of studies, which is why GHK-Cu is a well-established cosmetic ingredient. The site’s overview of what GHK-Cu does for skin health and collagen covers this dermatological literature, and the related discussion of whether GLOW supports collagen-synthesis pathways addresses the blend-level question directly.
Here is the honest boundary, though. Most of the credible GHK-Cu evidence is either in vitro (cell culture) or topical (creams and serums applied to skin). That evidence supports the idea that GHK-Cu can influence collagen and matrix biology and improve the look of skin when applied to it. It does not establish that injected GHK-Cu, as part of a research blend, produces systemic anti-aging, healing, or “glow” effects in humans — that is an extrapolation from topical and laboratory findings to a delivery route and set of goals that have not been studied the same way. The question of whether GHK-Cu stimulates fibroblast activity to enhance dermal elasticity in a systemic setting is best treated as an open research question for exactly this reason: the fibroblast response is well documented in culture, but what happens to it when copper tripeptide is delivered by injection alongside three other peptides is simply not on record.
What GHK-Cu contributes to the GLOW and KLOW discussion, then, is a genuine mechanistic story about collagen and matrix remodeling — the best-supported cosmetic rationale of any ingredient in these blends — alongside a real gap between the well-studied topical use and the injected, systemic use that the blends imply. It is the reason these blends are discussed for skin, hair, and connective-tissue goals, and it is also a reason to keep the word “discussed” front and center.
What KPV Adds to KLOW
KPV is the ingredient that turns GLOW into KLOW, and it is the least familiar of the four to most readers. KPV is a tripeptide — lysine-proline-valine — corresponding to the C-terminal three residues of α-MSH. That parent hormone is a known anti-inflammatory signaling molecule, and the striking finding about KPV is that it appears to retain much of the anti-inflammatory activity of the whole hormone in this tiny fragment.
The mechanistic work is interesting and, unusually for these compounds, fairly specific. KPV is taken up into cells via the peptide transporter PepT1, particularly in intestinal epithelial and immune cells; once inside, it interferes with pro-inflammatory signaling through the NF-κB and MAPK pathways, reducing the output of inflammatory cytokines.9 Importantly, this effect does not appear to require the melanocortin receptors that α-MSH normally acts through — it is a distinct, transporter-mediated route. In mouse models of inflammatory bowel disease, orally or systemically administered KPV reduced weight loss, lowered colonic myeloperoxidase activity, and improved histological markers of colitis.910
So KPV brings a plausible, mechanistically-defined anti-inflammatory rationale to KLOW, and it is the reason KLOW is discussed for gut-related and inflammatory goals more than GLOW or Wolverine are. But the evidence ceiling is the same one that limits BPC-157: this is animal-model and cell-culture data. The colitis studies are in mice. There are no controlled human trials establishing that KPV treats or prevents any inflammatory condition in people, and certainly none testing KPV as part of a four-peptide blend. The anti-inflammatory story is real as biology and unproven as therapy.
There is also a subtle point about why KPV is added at all. In a blend already containing BPC-157 (itself credited with anti-inflammatory and gut-protective effects in animals) and GHK-Cu (credited with anti-inflammatory and antioxidant gene effects), KPV is the third ingredient nominally pointed at inflammation. Whether three overlapping anti-inflammatory rationales produce additive benefit, redundant effect, or unpredictable interaction is completely unstudied. Adding an ingredient because it “also fights inflammation” assumes that more mechanisms aimed at the same target is always better — an assumption with no data behind it in this context.
Side by Side: Composition and the Goals People Discuss
With each ingredient characterized, the three blends can be laid out directly. The first table shows what is in each; the second shows the goals communities discuss for each and, crucially, the honest evidence status behind those discussions.
| Blend | Peptides (representative ratio) | Added ingredient vs simpler blend | Discussed emphasis |
|---|---|---|---|
| Wolverine | BPC-157 (~10 mg) + TB-500 (~10 mg) | — (base pairing) | Musculoskeletal recovery, injury, tissue repair |
| GLOW | BPC-157 (~5 mg) + TB-500 (~10 mg) + GHK-Cu (~35–50 mg) | + GHK-Cu (copper tripeptide) | Recovery plus skin, hair, collagen, appearance |
| KLOW | GHK-Cu (~50 mg) + BPC-157 (~10 mg) + TB-500 (~10 mg) + KPV (~10 mg) | + KPV (anti-inflammatory tripeptide) | Recovery + skin + a stronger anti-inflammatory / gut framing |
The nested structure is obvious in the composition column: each blend is the previous one plus a peptide. That is why the “which is best” question is somewhat malformed. Wolverine is not a worse GLOW; it is a narrower, simpler tool aimed only at repair. GLOW is not a worse KLOW; it simply omits the anti-inflammatory tripeptide. The right question is not which blend wins but which added ingredient’s discussed goal a person is interested in — and whether the evidence for that ingredient justifies the interest.
| Discussed goal | Driven mainly by | Best evidence that exists for that ingredient | Honest status for the blend |
|---|---|---|---|
| Tendon / ligament / muscle recovery | BPC-157, TB-500 | Animal models (BPC-157 tendon/ligament healing)23 | Preclinical only; no human blend trials |
| Gut / anti-inflammatory support | KPV, BPC-157 | Mouse colitis models (KPV)910 | Animal-only; no human data |
| Skin, wrinkles, collagen | GHK-Cu | In vitro + topical human cosmetic studies78 | Supported topically; injected/systemic use unproven |
| Hair growth | GHK-Cu | Preclinical + limited topical signals8 | Suggestive, not established |
| Wound / corneal healing | TB-500 (as Tβ4) | Human trials of Tβ4 eye drops56 | Real, but different route/tissue than the blend |
| Systemic “anti-aging” | All four (marketed) | Fragmentary, mechanism-level only8 | No blend evidence; largely aspirational |
Reading the two right-hand columns together is the whole point of this article. Every discussed goal traces to a single ingredient (or two), and for none of them does the blend as a blend have human evidence. The strongest human data in the entire set — the thymosin beta-4 eye trials — is for a route and tissue that the injectable recovery blend does not replicate. The best-supported cosmetic ingredient, GHK-Cu, is best supported topically. The gut and repair rationales are animal-only. A researcher comparing these blends is really comparing which unproven-in-combination rationale appeals most, and the community discussion around, for example, KLOW and angiogenesis or tissue repair should be read in that light — as exploration of a hypothesis, not confirmation of a result.
The Evidence Under the Hood, Component by Component
It is worth slowing down and grading the evidence for each of the four ingredients honestly, because the blends inherit exactly — and only — whatever their components have earned.
BPC-157 — strong preclinical, thin human. The animal literature is genuinely extensive and consistent: healing effects across tendon, ligament, muscle, bone, nerve, and gut models, by multiple routes of administration, from multiple laboratories.123 That consistency is why serious reviewers call the compound “of interest” rather than dismissing it. But the same 2025 review that catalogs those effects also underscores that only three human clinical trials have been published and that the compound remains investigational, with regulators having flagged it precisely because human safety and efficacy are not established.1 (As detailed in the safety section, BPC-157 was placed on the FDA’s Category 2 compounding list in 2023 and then removed from it in April 2026 on procedural grounds — a change that does not amount to approval and leaves the compound unapproved and investigational.) Evidence grade: promising in animals, unproven in humans.
TB-500 / thymosin beta-4 — real human data, wrong context. Full-length thymosin beta-4 has been through randomized, placebo-controlled human trials — but as an ophthalmic solution for dry eye and neurotrophic keratopathy, where it met efficacy endpoints.56 This is the most rigorous human evidence attached to any ingredient in these blends. The catch is threefold: the trials used a topical eye drop, not systemic injection; they targeted corneal-surface disease, not musculoskeletal recovery; and “TB-500” in research vials may be a fragment rather than the full protein studied. The site’s look at evidence for TB-500 in tendon and ligament repair keeps that systemic musculoskeletal question in the preclinical column, which is where it belongs. Evidence grade: strong for Tβ4 in ophthalmology; preclinical for the systemic recovery use the blends imply.
GHK-Cu — best cosmetic evidence, mostly topical. Decades of laboratory work show GHK-Cu influencing collagen synthesis, matrix remodeling, antioxidant defense, and a broad swath of gene expression, and topical copper-peptide products have improved measures of skin firmness and appearance in cosmetic studies.78 This is the most decision-relevant human-adjacent evidence for a skin goal. The limitation is the delivery gap: the data underpins applied-to-skin use far more than injected use. Evidence grade: solid for topical skin benefit; extrapolated for systemic/injected use.
KPV — clean mechanism, animal-only outcomes. KPV has an unusually well-defined mechanism (PepT1 uptake, NF-κB/MAPK inhibition) and reproducible anti-inflammatory effects in mouse colitis models.910 But there are no controlled human trials, and the entire outcome literature is preclinical. Evidence grade: mechanistically credible, clinically unproven.
Put together, the four ingredients span the spectrum from “real human trials in a different context” (Tβ4) through “solid topical cosmetic data” (GHK-Cu) to “strong animal, thin human” (BPC-157) and “animal-only” (KPV). Not one of them has human trial evidence for the systemic, injected, combination use that KLOW, GLOW, and Wolverine represent. That is the single most important sentence in this article, and it applies equally to all three blends.
Why Blending Makes the Evidence Question Harder, Not Easier
There is a seductive intuition behind stacking: if peptide A helps and peptide B helps, then A + B should help more. It feels like addition. In pharmacology, it rarely is that simple, and in the specific case of these blends it is worth spelling out why combining compounds actually degrades the strength of any claim rather than reinforcing it.
First, evidence does not stack the way doses do. Wolverine’s evidence is not “BPC-157’s evidence plus TB-500’s evidence.” It is the intersection of two separate preclinical literatures, studied in isolation, never together in a controlled human trial. Adding GHK-Cu to make GLOW does not import GHK-Cu’s topical cosmetic data into an injectable recovery product; it introduces a third variable whose systemic behavior in that mixture is unstudied. Every ingredient you add multiplies the uncertainty rather than dividing it.
Second, interactions are unknown and unmeasured. Peptides can compete for transporters, alter each other’s stability in solution, or act on overlapping pathways in ways that are sub-additive (redundant) or even antagonistic. KLOW, for instance, contains three ingredients with anti-inflammatory rationales (BPC-157, GHK-Cu, KPV). Whether they reinforce one another, plateau, or interfere is simply not known, because no one has run the experiment. Marketing assumes synergy; the honest word is “unknown.”
Third, dosing becomes a guess. In a fixed blend, the ratio is set by the vendor, not by any dose-finding study. GLOW’s heavy GHK-Cu load and light BPC-157 (5 mg vs 10 mg in some Wolverine vials) reflect a marketing choice, not an evidence-based ratio. There is no trial establishing that a given ratio is optimal, safe, or even sensible for any goal — and the ratios differ between vendors, so two “KLOW” vials are not interchangeable data points.
Fourth, attribution becomes impossible. If someone uses a four-peptide blend and reports an effect — better or worse — there is no way to know which ingredient (or interaction, or placebo response, or concurrent training and diet) produced it. Blends are, by construction, uncontrolled experiments with confounded variables. This is why anecdotal reports about KLOW or GLOW, however sincere, cannot substitute for evidence: the design guarantees that cause cannot be isolated. Researchers interested in the underlying biology will get cleaner answers studying single peptides — the reasoning behind resources like the site’s examination of KLOW peptides and energy metabolism, which has to decompose the blend into its parts to say anything precise at all.
The upshot is counterintuitive but important: the more ingredients a blend contains, the weaker, not stronger, any confident claim about it should be. On an evidence basis alone, Wolverine (two peptides) is the least uncertain of the three simply because it has the fewest moving parts — though “least uncertain” still means “no human combination trials.” KLOW, with four ingredients, is the most speculative precisely because it is the most complex.
What the Evidence Does NOT Show
It is worth being blunt and specific about the claims these blends cannot support, because the gap between what is marketed and what is known is where people get misled.
No blend has been tested as a blend in humans. There is no randomized controlled trial — none — of KLOW, GLOW, or Wolverine as a fixed combination. Every efficacy statement about the blends is an extrapolation from single-ingredient data, most of it from animals.
No head-to-head comparisons exist. The framing of this very article — “KLOW vs GLOW vs Wolverine” — describes a community debate, not a research finding. No study has compared the three against each other, or against placebo, for any outcome. Claims that one is “better for recovery” or “better for skin” rest on which ingredients they contain, not on comparative data.
The strongest human data does not transfer. The thymosin beta-4 eye-drop trials are real and rigorous, but they concern a topical ophthalmic product for corneal disease.56 They provide no evidence that injecting TB-500 systemically heals tendons, builds muscle, or accelerates athletic recovery. Borrowing their credibility for the blends is a category error.
GHK-Cu’s skin data is mostly topical. The collagen and appearance benefits associated with GHK-Cu come largely from creams and serums and from cell culture.78 That an injected blend containing GHK-Cu produces systemic anti-aging or “glow” is an inference across delivery routes, not a demonstrated effect.
“Regenerative” is not “proven in people.” BPC-157 and KPV have genuine, reproducible effects in animal models, and that is a legitimate reason for scientific interest.1910 But animal efficacy translating to human benefit is the exception, not the rule, in drug development. Treating “works in mice” as “works in me” skips the entire, failure-prone process that separates the two.
None treats, cures, or prevents any disease. Not inflammatory bowel disease (despite KPV’s colitis-model data), not osteoarthritis, not any injury or aging process. None of these compounds is an approved therapy for anything, and no blend has an approved indication. Discussion of a goal is not evidence of an outcome.
The recurring theme is a leap that appears in almost all blend marketing: from “the ingredients have interesting biology” to “the blend achieves the goal.” Interesting biology is where research starts, not where it concludes. For readers who want to watch how the underlying single-peptide evidence evolves, the site’s coverage of the individual peptides — for instance its review of what the research says about BPC-157’s gut and inflammation effects — tracks the single-peptide literature at the level where any real conclusions about these ingredients will be drawn.
Safety, Sourcing, and the Purity Problem
Because none of these blends is a regulated medicine, safety cannot be assessed the way it would be for an approved drug — and the risks are not only pharmacological but also about what is actually in the vial.
On the pharmacology, the honest statement is that long-term human safety data for chronic administration of any of these four peptides — individually or blended — is limited to absent. BPC-157’s human safety is described by reviewers as insufficient, which is part of why the FDA placed it on its Category 2 compounding list in 2023.111 The thymosin beta-4 eye trials characterize ocular safety of a topical product, not the systemic safety of injected TB-500. GHK-Cu’s safety profile is best characterized topically. KPV’s safety data is from animal models. Combining four compounds compounds the uncertainty: potential interactions, cumulative immunogenicity, and effects of long-term exposure are all unstudied.
The sourcing and purity problem is arguably the more immediate hazard. These blends are sold as “research chemicals” outside the pharmaceutical quality system. That means no guarantee of identity, purity, sterility, or accurate labeling. Independent testing across the peptide market has repeatedly found products that were underdosed, mislabeled, contaminated, or contained different peptides than stated. In a four-peptide blend the risk is amplified: each additional ingredient is another opportunity for an impurity, an endotoxin, or a synthesis error, and copper-containing products add their own stability and dosing considerations. Even setting the biology aside, a person cannot be confident that a given “KLOW” vial contains what the label claims, in the ratio claimed, free of contaminants.
Several practical safety-adjacent facts deserve emphasis:
- Regulatory status. None of the four peptides is an FDA-approved drug, and none of the blends is approved for any use. In 2023 the FDA placed BPC-157 in Category 2 of its 503A bulk-substances review — the group flagged as presenting significant safety risks for compounding — reflecting concerns about immunogenicity, impurities, and lack of human data. In April 2026 the agency removed BPC-157 from that Category 2 list, but this was a procedural step tied to withdrawn nominations and a fresh review cycle, not an approval or a finding of safety; the compound remains unapproved and investigational and is not on the approved 503A bulks list.11
- Sport prohibition. Both BPC-157 and TB-500 are prohibited in sport at all times by the World Anti-Doping Agency. Thymosin β4 and its derivatives (explicitly including TB-500) are listed under the S2 growth-factors category, and BPC-157 was added to the Prohibited List in 2022 under S0 (non-approved substances).12 For any tested athlete, use of Wolverine, GLOW, or KLOW would constitute an anti-doping violation regardless of pharmacology.
- Route mismatch. Much of the encouraging human-adjacent data (Tβ4 eye drops, GHK-Cu topicals) involves routes other than the subcutaneous injection typical of these research blends. Safety and efficacy do not transfer automatically across routes.
- No medical oversight. These products are used outside clinical supervision, without the monitoring, dosing standardization, or adverse-event reporting that accompanies approved therapies.
The reasonable reading is not “these are known to be dangerous” — that would overstate the evidence in the other direction — but rather that safety is genuinely uncharacterized for combined, injected, long-term use, and that product-quality risk sits on top of that biological uncertainty. Absence of documented harm in a setting no one has studied rigorously is not the same as demonstrated safety.
Practical Research-Context Considerations
For completeness, and strictly as educational context rather than usage guidance, a few practical points recur whenever these blends are discussed in a laboratory framing — with the standing caveat that none of this implies human use is appropriate.
These blends are supplied as lyophilized (freeze-dried) powder in sealed vials and are reconstituted with sterile or bacteriostatic water for handling. As with any peptide, the diluent is added gently down the vial wall and the vial is swirled rather than shaken, because agitation can degrade peptide structure. The copper-containing blends (GLOW, KLOW) carry the characteristic faint blue color of GHK-Cu, and copper complexes have their own light- and oxidation-sensitivity considerations. General reconstitution arithmetic — how a fixed mass of peptide in a chosen volume of water sets the concentration — is covered in the site’s peptide reconstitution guide, which is written for educational reference.
Two blend-specific wrinkles are worth noting. First, because the blends are fixed-ratio, the amount of any one peptide is not independently adjustable — changing the “dose” of BPC-157 in a KLOW vial necessarily changes the dose of the other three in lockstep. This is a fundamental limitation of any combination product used as a research tool: it cannot isolate variables. Second, the ratios differ by vendor, so quantitative comparisons between blends from different suppliers are unreliable. A researcher who genuinely wanted to study a mechanism — angiogenesis, collagen synthesis, anti-inflammatory signaling — would be far better served by single, well-characterized peptides at known concentrations than by a proprietary blend of uncertain composition.
None of this handling detail changes the evidence picture. A perfectly reconstituted, high-purity vial of KLOW is still a four-peptide combination with zero human combination-trial data behind it. Meticulous technique preserves whatever activity the molecules have; it does not manufacture efficacy that has not been demonstrated. That distinction — between doing the procedure carefully and having evidence that the procedure accomplishes a goal — is the one most worth carrying away.
How to Think About the Comparison
Pulling the threads together, the “KLOW vs GLOW vs Wolverine” question dissolves into a clearer set of observations once the blends are seen for what they are.
They are a nested family, not three rival drugs. Wolverine is the two-peptide repair core; GLOW adds a cosmetic/collagen ingredient; KLOW adds an anti-inflammatory one. Choosing between them, in community discussion, is really choosing how many ingredients — and which discussed goals — a person wants layered together.
The discussed goals are all traceable to individual ingredients, and the evidence lives at the ingredient level, not the blend level. Recovery talk comes from BPC-157 and TB-500 (animal data, plus Tβ4 eye trials in a different context). Skin and collagen talk comes from GHK-Cu (topical and cell-culture data). Gut and anti-inflammatory talk comes from KPV and BPC-157 (animal models). For not one of these goals does the blend itself have human evidence.
More ingredients means more uncertainty, not more proof. The evidence, the dosing rationale, the safety profile, and the ability to attribute any effect all get weaker as ingredients are added, because the number of unstudied interactions grows. If forced to rank the three by how much confident language they can support, the honest ranking runs opposite to complexity: the simplest blend permits the least-overreaching claims, and even it permits very little.
And the most important framing of all: these are compounds people discuss for certain goals, based on the interesting biology of their parts, not compounds shown to achieve those goals. That is not a dismissal — genuine, reproducible preclinical findings and real ophthalmic trials sit inside this story, and they are worth understanding. It is simply a boundary. Everything on the far side of it — systemic human efficacy of these blends for recovery, skin, inflammation, or aging — remains, as of mid-2026, unproven. The responsible way to read any “which blend is best” discussion is as a conversation about hypotheses, held to the standard that hypotheses deserve.
Frequently Asked Questions
What is the actual difference between KLOW, GLOW, and Wolverine?
They are a nested set. Wolverine is a two-peptide pairing of BPC-157 and TB-500, focused on tissue repair. GLOW is that same pairing plus GHK-Cu (a copper tripeptide associated with skin and collagen). KLOW is GLOW plus KPV (an anti-inflammatory tripeptide). So each blend is the previous one with one more ingredient added, and the discussed “goal” broadens with each addition — from recovery, to recovery plus skin, to recovery plus skin plus a stronger anti-inflammatory framing. None is a standardized product; ratios vary by vendor.
Are any of these blends FDA-approved or proven to work?
No. None of KLOW, GLOW, or Wolverine is approved by the FDA, EMA, or any comparable regulator for any use, and none has ever been tested as a fixed combination in a controlled human trial. Every efficacy claim is extrapolated from single-ingredient data, most of which is preclinical (animal or cell-culture). There are also no head-to-head studies comparing the three, so “which is best” is a community debate, not a research finding.
Which blend is best for injury recovery?
The recovery rationale comes from BPC-157 and TB-500, which all three blends contain, so on that axis they share the same (preclinical) backbone. Wolverine is the most focused option for repair because it contains only those two peptides. But “best for recovery” overstates the evidence: BPC-157’s tendon and ligament healing is documented in animal models, not established in humans,123 and there is no trial showing any of these blends accelerates recovery in people.
Which blend is best for skin and anti-aging?
GHK-Cu is the ingredient behind the skin and collagen discussion, so GLOW and KLOW (which contain it) are the ones people frame that way. GHK-Cu does have real cosmetic evidence — but mostly for topical creams and serums and in cell culture,78 not for injected use as part of a blend. So the skin rationale is the best-supported of any goal here, while still involving a significant leap from topical data to injected blends.
Does the thymosin beta-4 (TB-500) research prove these blends heal tissue?
Not for the way the blends are used. Full-length thymosin beta-4 has genuine randomized human trial data — but as an eye drop for dry eye and corneal disease, where it met endpoints.56 That is a different route (topical ocular) and a different tissue than systemic injection for muscle or tendon recovery. Also, “TB-500” sold in research vials is often a fragment rather than the full protein studied in those trials, so the credibility does not transfer cleanly.
Is it safer to use one blend over another?
Safety is genuinely uncharacterized for all of them in combined, injected, long-term use. As a general principle, fewer ingredients means fewer unknown interactions, so a two-peptide blend involves less combinatorial uncertainty than a four-peptide one — but that is not the same as being “safe.” A large, separate risk is product quality: these are unregulated research chemicals, and independent testing across the market has found mislabeled, underdosed, or contaminated products. BPC-157 and TB-500 are also both banned in sport by WADA.12
Why do blends have so many ingredients if that adds uncertainty?
Largely because combining compounds with overlapping “healing” or “anti-inflammatory” reputations makes an appealing marketing story built on assumed synergy. But synergy is assumed, not demonstrated: peptides can interact in additive, redundant, or antagonistic ways, and no study has measured what happens when these specific peptides are mixed. Each added ingredient multiplies the unknowns — interactions, dosing, purity, attribution — which is why more complex blends warrant more caution about confident claims, not less.
Can KPV in KLOW treat gut problems or inflammation?
KPV has a well-defined anti-inflammatory mechanism and reduced colitis in mouse models,910 which is why KLOW is discussed for gut and inflammatory goals. But that evidence is entirely animal-based; there are no controlled human trials showing KPV treats or prevents inflammatory bowel disease or any other condition, and certainly none testing it inside a four-peptide blend. It is a credible hypothesis, not an established therapy.
What would it take to actually prove one of these blends works?
The same thing it takes for any therapy: controlled human trials of the specific blend, at defined ratios, against placebo, with objective outcomes — ideally preceded by dose-finding and interaction studies to justify the combination. Until that work exists, statements about what KLOW, GLOW, or Wolverine “do” in people are hypotheses drawn from single-ingredient, mostly-preclinical data, and should be read that way.
References
- McGuire FP, Martinez R, Lenz A, Skinner L, Cushman DM. Regeneration or Risk? A Narrative Review of BPC-157 for Musculoskeletal Healing. Curr Rev Musculoskelet Med. 2025;18(12):611-619. PMID: 40789979. PMCID: PMC12446177. https://pmc.ncbi.nlm.nih.gov/articles/PMC12446177/
- Chang CH, Tsai WC, Lin MS, Hsu YH, Pang JH. The promoting effect of pentadecapeptide BPC 157 on tendon healing involves tendon outgrowth, cell survival, and cell migration. J Appl Physiol (1985). 2011;110(3):774-780. PMID: 21030672. https://pubmed.ncbi.nlm.nih.gov/21030672/
- Cerovecki T, Bojanic I, Brcic L, et al. Pentadecapeptide BPC 157 (PL 14736) improves ligament healing in the rat. J Orthop Res. 2010;28(9):1155-1161. PMID: 20225319. https://pubmed.ncbi.nlm.nih.gov/20225319/
- Goldstein AL, Hannappel E, Kleinman HK. Thymosin beta4: actin-sequestering protein moonlights to repair injured tissues. Trends Mol Med. 2005;11(9):421-429. PMID: 16099219. https://pubmed.ncbi.nlm.nih.gov/16099219/
- Sosne G, Dunn SP, Kim C. Thymosin β4 significantly improves signs and symptoms of severe dry eye in a phase 2 randomized trial. Cornea. 2015;34(5):491-496. PMID: 25826322. https://pubmed.ncbi.nlm.nih.gov/25826322/
- Sosne G, Kleinman HK, Springs C, Gross RH, Sung J, Kang S. 0.1% RGN-259 (Thymosin β4) Ophthalmic Solution Promotes Healing and Improves Comfort in Neurotrophic Keratopathy Patients in a Randomized, Placebo-Controlled, Double-Masked Phase III Clinical Trial. Int J Mol Sci. 2022;24(1):554. PMID: 36613994. PMCID: PMC9820614. https://pmc.ncbi.nlm.nih.gov/articles/PMC9820614/
- Pickart L, Vasquez-Soltero JM, Margolina A. GHK Peptide as a Natural Modulator of Multiple Cellular Pathways in Skin Regeneration. Biomed Res Int. 2015;2015:648108. PMID: 26236730. PMCID: PMC4508379. https://pmc.ncbi.nlm.nih.gov/articles/PMC4508379/
- Pickart L, Margolina A. Regenerative and Protective Actions of the GHK-Cu Peptide in the Light of the New Gene Data. Int J Mol Sci. 2018;19(7):1987. PMID: 29986520. https://pubmed.ncbi.nlm.nih.gov/29986520/
- Dalmasso G, Charrier-Hisamuddin L, Nguyen HT, Yan Y, Sitaraman S, Merlin D. PepT1-mediated tripeptide KPV uptake reduces intestinal inflammation. Gastroenterology. 2008;134(1):166-178. PMID: 18061177. https://pubmed.ncbi.nlm.nih.gov/18061177/
- Kannengiesser K, Maaser C, Heidemann J, et al. Melanocortin-derived tripeptide KPV has anti-inflammatory potential in murine models of inflammatory bowel disease. Inflamm Bowel Dis. 2008;14(3):324-331. PMID: 18092346. https://pubmed.ncbi.nlm.nih.gov/18092346/
- U.S. Food and Drug Administration. Certain Bulk Drug Substances for Use in Compounding That May Present Significant Safety Risks (BPC-157, Category 2). https://www.fda.gov/drugs/human-drug-compounding/certain-bulk-drug-substances-use-compounding-may-present-significant-safety-risks
- World Anti-Doping Agency. The Prohibited List. Thymosin β4 and its derivatives (e.g., TB-500) are listed under S2.3 (Growth Factors and Growth Factor Modulators); BPC-157 is listed under S0 (Non-Approved Substances). https://www.wada-ama.org/en/prohibited-list
Educational and research-use disclaimer: This article is provided solely for scientific and educational purposes. KLOW, GLOW, and Wolverine are informal, non-standardized combinations of research peptides (BPC-157, TB-500, GHK-Cu, and KPV). None of these blends, and none of their individual peptides, is approved by the FDA, EMA, or any comparable regulator for the treatment, cure, or prevention of any disease, and no blend has been tested as a fixed combination in a controlled human trial. Nothing here is medical advice or a recommendation for human use. BPC-157 and TB-500 are prohibited in sport by WADA. Product quality in the unregulated research-chemical market is not guaranteed. Any legitimate investigation of these compounds should occur within properly authorized preclinical or clinical research under appropriate oversight, and readers should consult qualified professionals and applicable regulations before making any decisions.