The question in the title carries an assumption worth pausing on before we chase the evidence: it presumes there is a settled body of “research” describing what BPC-157 does to the gut and to inflammation, as though the healing effects were an established fact and the only task left were to summarize them. That framing is half right and half misleading, and untangling the two halves is the honest starting point for anyone trying to understand this peptide. The half that is right: BPC-157 does have a genuine, three-decade research record, and the gastrointestinal tract is unambiguously its best-studied territory — the place where the strongest and most internally consistent signals appear.1 The half that is misleading: essentially all of that record is preclinical, conducted in rats and mice, and the human clinical efficacy of BPC-157 for gut disease or inflammation has never been confirmed in a published, peer-reviewed controlled trial.2
So this article does not treat “BPC-157 heals the gut” as a premise to be defended. It treats it as a research claim to be examined at its actual level of evidence. We will look closely at what the rodent studies genuinely show — and they show a great deal that is interesting — while being equally precise about the boundary those studies cannot cross without human data. The compound’s name is itself a claim: BPC stands for “Body Protection Compound,” and 157 designates a specific pentadecapeptide (a 15-amino-acid chain) said to be a partial sequence derived from a protein found in human gastric juice.1 That gastric origin is not a marketing flourish; it is the historical and biological reason the gut is where the science is deepest.
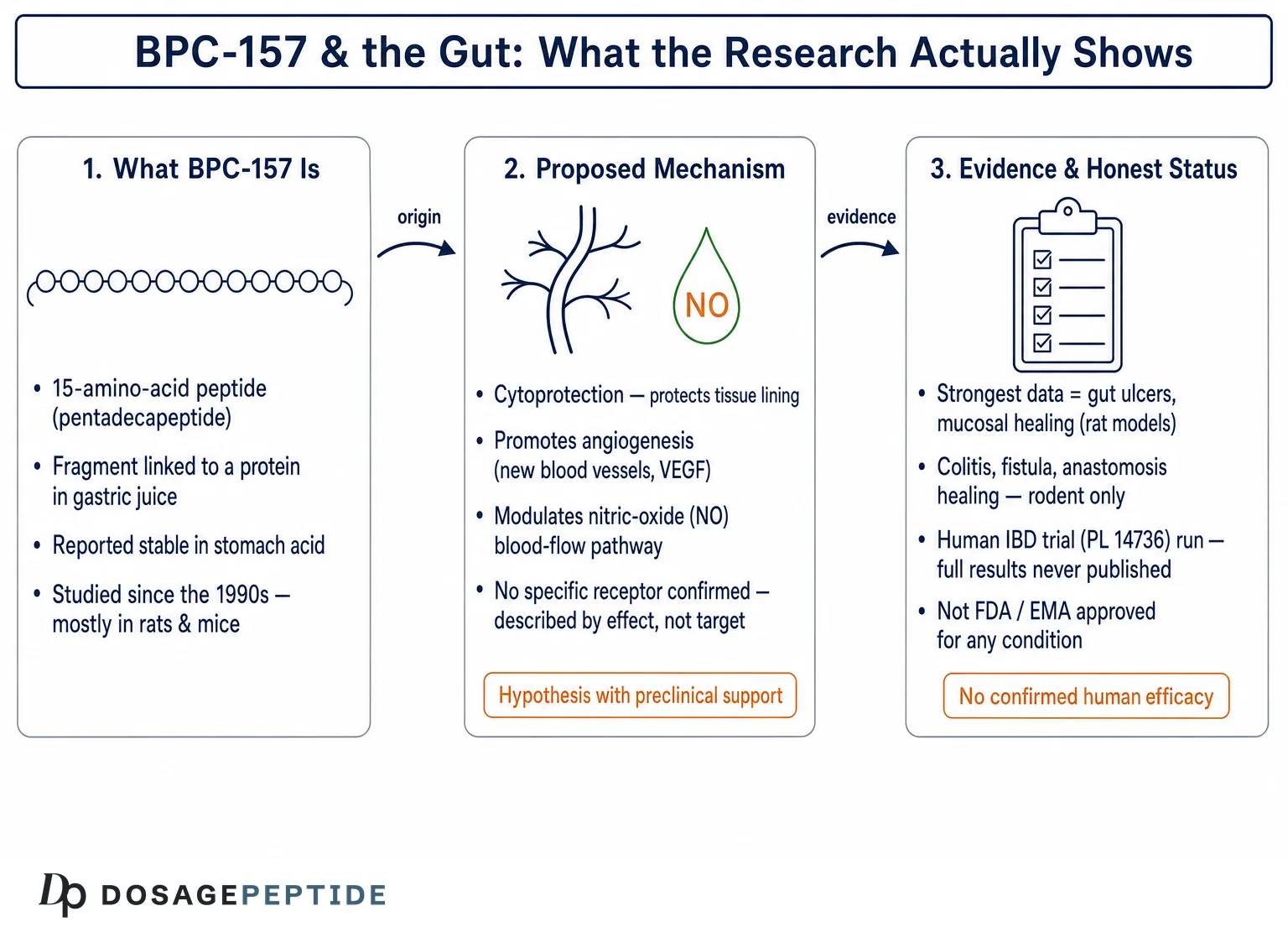
This piece is written for researchers, clinicians curious about the peptide literature, and educated readers who want a map that distinguishes what is demonstrated from what is hypothesized from what is simply asserted online. We will cover the compound’s identity and origin, the proposed cytoprotective and angiogenic mechanisms, the ulcer and mucosal-healing models, the inflammatory-bowel-disease work and the human trial that was run but never fully published, the surgical-healing studies in anastomoses and short bowel, the NSAID-injury data that most directly speaks to inflammation, a candid accounting of what “anti-inflammatory” can and cannot mean here, comparisons with established gut therapies, handling in a research context, safety and sourcing, and regulatory status. Throughout, the guiding discipline is to neither dismiss a rich preclinical literature nor inflate it into clinical proof it has not earned. BPC-157 is not approved by any major regulator to treat, cure, or prevent any gastrointestinal or inflammatory disease, and nothing here should be read as suggesting otherwise.
What BPC-157 Is and Where the Story Begins
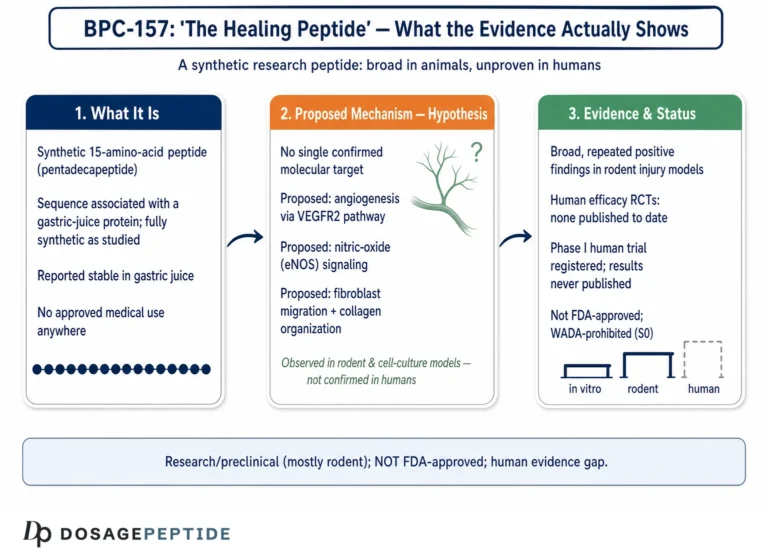
BPC-157 is a synthetic peptide of fifteen amino acids, with the sequence Gly-Glu-Pro-Pro-Pro-Gly-Lys-Pro-Ala-Asp-Asp-Ala-Gly-Leu-Val. It was described by its originators as a fragment corresponding to a portion of a larger “body protection compound” isolated from human gastric juice, and the synthetic pentadecapeptide reproduces the biologically active core.1 Unlike many peptides, it carries no formulation carrier and is reported to be unusually stable — notably, stable in human gastric juice for more than 24 hours, a property that matters enormously for a molecule proposed to act along the digestive tract, because it implies the peptide can survive the very environment that destroys most proteins.1
The research program behind BPC-157 is closely associated with Predrag Sikiric and colleagues at the University of Zagreb in Croatia, whose group has published the large majority of the primary studies since the early 1990s. The foundational work framed BPC-157 as an anti-ulcer agent and, more ambitiously, as a mediator of what pharmacologists call cytoprotection — the capacity to protect the cells lining an organ against injury by mechanisms that go beyond simply reducing stomach acid.1 The very first widely cited demonstration compared BPC-157 against a panel of standard agents in three classic rat models of gastroduodenal injury: 48-hour restraint stress, subcutaneous cysteamine (which reliably produces duodenal ulcers), and intragastric 96% ethanol (which produces acute hemorrhagic gastric lesions). BPC-157 was reported to be consistently protective across all three, and to outperform H2-receptor antagonists, dopamine agents, and several gut peptides used as comparators.3
Commercially, the compound has traveled under several development codes — PL-10, PLD-116, and PL 14736 — the last of which was advanced by the Croatian pharmaceutical company Pliva specifically as a candidate therapy for inflammatory bowel disease.5 That development history is a crucial and often-omitted piece of context: BPC-157 is not merely an underground “research chemical” that appeared on the internet. It was, at one point, a formally sponsored pharmaceutical asset taken into early human testing. What happened to that program — and what did not get published — is central to any honest evidence assessment, and we return to it below.
It helps to hold three distinct ideas apart when thinking about this molecule, because popular writing routinely blurs them. First, there is the claimed origin: a fragment related to a protective protein in gastric juice. Second, there is the proposed mechanism: cytoprotection through angiogenesis, growth-factor and nitric-oxide modulation, and effects on the gut-brain axis. Third, there is the evidence level: overwhelmingly rodent, with human data thin to absent. Confident online summaries tend to collapse all three into a single reassuring sentence — “a gastric peptide that heals the gut” — when in reality the origin is a specific historical claim, the mechanism is a set of hypotheses with preclinical support, and the evidence level is the part that most needs stating plainly. For a broader orientation to the compound and its research framing, the site’s pillar explainer, what BPC-157 is and how it is studied, provides useful background.
The Proposed Mechanism: Cytoprotection, Angiogenesis, and Nitric Oxide
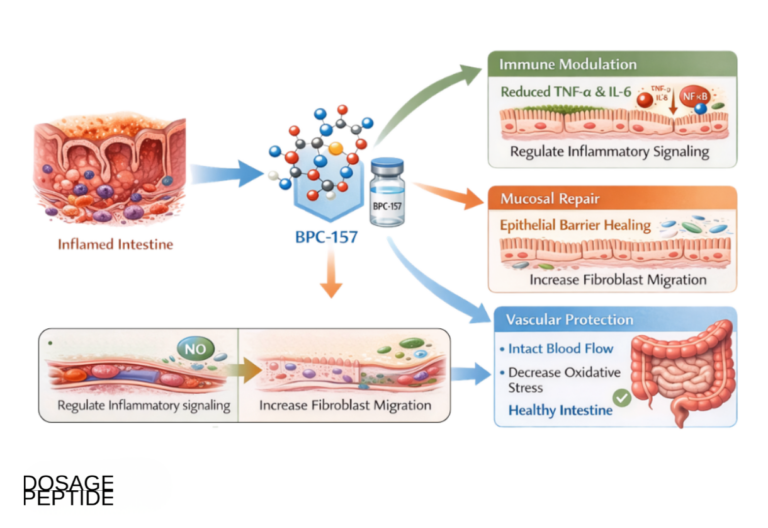
To evaluate the gut-healing claim, one has to understand the mechanistic story its proponents tell, because the plausibility of the claim rests on whether that story is coherent and supported. The mechanism most consistently invoked is angiogenesis — the formation of new blood vessels. Wound healing anywhere in the body depends on re-establishing blood supply to injured tissue; without angiogenesis, granulation tissue cannot form, oxygen and nutrients cannot reach the repair site, and healing stalls. The BPC-157 literature reports that the peptide promotes angiogenesis and up-regulates vascular endothelial growth factor (VEGF) signaling, and that this pro-angiogenic action is a recurring thread across the many tissues in which the peptide has been tested.4
Closely linked is the nitric oxide (NO) system. Nitric oxide is a signaling molecule central to blood-vessel tone, mucosal blood flow, and cytoprotection in the stomach. A distinctive feature of the BPC-157 work is that the peptide is described as a bidirectional modulator of the NO pathway: in experiments that pit BPC-157 against L-NAME (an inhibitor of NO synthesis) and L-arginine (an NO precursor), the peptide is reported to counteract the harmful effects of NO-blockade while interacting productively with NO-donation.4 Much of the mechanistic case is in fact built on these L-NAME/L-arginine designs, which are a standard pharmacological way to implicate the NO system in an observed effect. The interpretation offered is that BPC-157 helps maintain endothelial integrity and mucosal blood flow through NO-related mechanisms rather than by acting as a simple NO donor or blocker.4
Beyond vessels, the peptide has been reported to influence several growth-factor and cytoprotective pathways relevant to epithelial repair, to affect the expression of genes involved in cell survival and extracellular-matrix remodeling, and to interact with the gut-brain axis — the bidirectional communication between the enteric nervous system and the brain that shapes gut motility, sensation, and mucosal function.59 This gut-brain framing is one reason the same research group has extended BPC-157 claims from the intestine outward to the nervous system; readers interested in that separate and considerably more speculative direction can review the site’s discussion of BPC-157 and nerve and brain research, keeping in mind that the neurological claims rest on an even thinner evidence base than the gastrointestinal ones.
Two honest caveats belong right here, because they temper the mechanistic enthusiasm that vendor pages rarely qualify. First, a great deal of the mechanistic detail circulating online — precise receptor identities, exact percentage changes in tight-junction proteins, specific cytokine fold-reductions — is stated with a confidence the primary literature does not support, and often traces to commercial rather than peer-reviewed sources. The robust, repeatedly reported findings are broad and functional: better blood flow, more granulation tissue, faster epithelial coverage, reduced lesion area. The molecular fine print is genuinely less settled than the internet implies. Second, no defined high-affinity receptor for BPC-157 has been established in the way it has for, say, GLP-1 or the opioid peptides. The compound is best understood mechanistically as a pleiotropic cytoprotective and angiogenic modulator whose downstream effects are better characterized than its proximal molecular target. That is not a fatal flaw — many useful agents predate a known receptor — but it is a real limit on how mechanistically “proven” the story is, and it should be named.
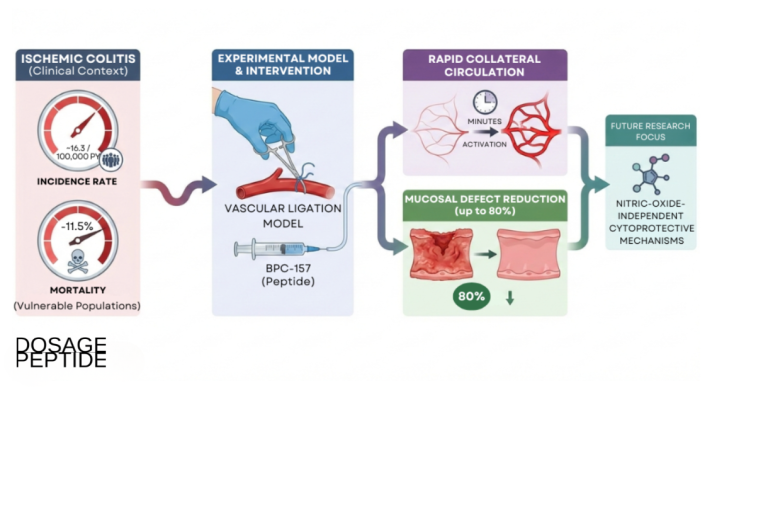
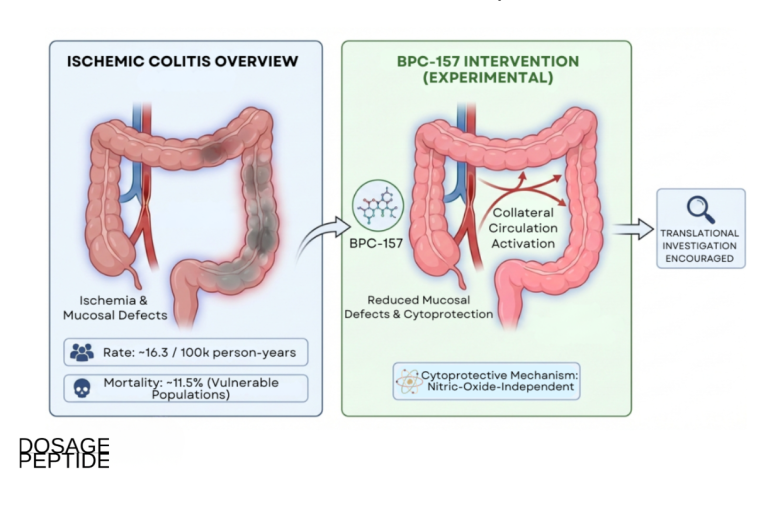
There is one more mechanistic strand worth naming because it recurs across the newer literature: the proposal that BPC-157 acts partly by rapidly recruiting alternative or “bypassing” blood-flow pathways when a vessel is occluded or a tissue is ischemic. In several vascular-injury models the peptide is reported to restore perfusion quickly by activating collateral circulation, an effect the originating group ties back to the same angiogenic and NO-related machinery.4 Applied to the gut, this framing is attractive because so much mucosal injury — stress ulcers, NSAID gastropathy, ischemic anastomoses — is fundamentally a blood-flow problem: tissue starved of perfusion cannot defend or repair itself. A peptide that improved microvascular supply to a compromised mucosa would, in principle, help across many of the injury types described in this article through a single unifying route. That said, the same caution applies. The perfusion-recovery claims are, like the rest, preclinical, and the leap from “restores collateral flow in a rat vascular model” to “protects the human gut in disease” is exactly the kind of extrapolation this article is at pains not to make on the reader’s behalf.
The reasonable mechanistic summary is therefore this: BPC-157 has a coherent, repeatedly observed functional signature — pro-angiogenic, NO-modulating, cytoprotective — that plausibly explains why injured gut tissue would heal faster in a rodent given the peptide. What it lacks is a fully resolved molecular target and, more importantly, any demonstration that the same signature operates at meaningful magnitude in a human gut.
The Gut as Home Turf: Ulcer and Mucosal-Healing Models
If any organ system deserves to be called BPC-157’s strongest, it is the gastrointestinal tract, and the reason is partly historical — the peptide was born as an anti-ulcer agent — and partly the sheer density of concordant rodent studies. The foundational ethanol, cysteamine, and restraint-stress models mentioned earlier are worth dwelling on because each isolates a different mechanism of gut injury, and BPC-157 was reported protective across all of them.3
Consider what these three models actually test. 96% ethanol instilled into the stomach causes direct chemical necrosis of the mucosa and acute hemorrhagic erosions — a model of caustic, blood-flow-dependent injury. Cysteamine reliably produces duodenal ulcers and is a classic model for the kind of penetrating ulceration seen in the proximal small bowel. Restraint stress produces gastric lesions through a neurogenic, stress-hormone-mediated pathway, engaging exactly the gut-brain axis the mechanism section described. A single agent reported to protect across chemical, ulcerative, and stress-driven injury is, at minimum, doing something broad to mucosal resilience rather than blocking one narrow pathway.3 This breadth is the origin of the “cytoprotection” label: the effect does not look like acid suppression, because it appears in models where acid is not the driver, and in the cysteamine work the peptide protected even in the setting of removed stomach acid influence.
Later reviews from the originating group consolidated these observations into the claim that BPC-157 is effective throughout the entire gastrointestinal tract — esophagus, stomach, duodenum, small intestine, and colon — and can promote the healing of ulcers, fistulas, and mucosal lesions at multiple levels simultaneously.1 The wound-healing literature adds the mechanistic connective tissue: improved angiogenesis, better-organized granulation tissue, and favorable collagen deposition at the healing site, with the peptide effective when given alone and without a delivery scaffold.4 The functional endpoints in these studies are the ones that matter for a healing claim — reduced lesion area, faster epithelial coverage, restored tissue architecture on histology.
Here is where honesty must sharpen the picture. Every study in the previous two paragraphs is a rodent study, and the great majority originate from a single research group. That does not make the findings wrong — the internal consistency across models is genuinely notable, and independent reviewers have acknowledged that the reported healing effects are strikingly uniform.2 But it does mean the evidence has not been broadly replicated across independent laboratories at the scale one would want before treating it as established, and it has not been tested in the human stomach or intestine in any published controlled way. The correct reading is that BPC-157 has a strong, coherent preclinical ulcer- and mucosal-healing signal — the best in its entire evidence portfolio — and that this signal remains, for now, a rodent phenomenon awaiting human confirmation. Anyone comparing it against agents with decades of human trial data should keep the broader dosage and compound index framing in mind: preclinical promise and clinical proof are different currencies.
Inflammatory Bowel Disease: the Models and the Human Trial That Vanished
Inflammatory bowel disease — ulcerative colitis and Crohn’s disease — is the indication for which BPC-157 came closest to becoming an actual medicine, and it is also where the gap between preclinical enthusiasm and human proof is most instructive. On the preclinical side, the peptide has been tested in standard rodent colitis models. Trinitrobenzene sulfonic acid (TNBS) colitis produces transmural inflammation resembling Crohn’s disease; dextran sodium sulfate (DSS) colitis produces epithelial-barrier-driven inflammation used to model ulcerative colitis; cysteamine can be used to induce colitis as well. Across such models the originating group has reported that BPC-157 reduces inflammation and accelerates mucosal healing.1
The peptide’s IBD credentials were formalized when it entered clinical development as PL 14736. The rodent studies from that era are explicit about the connection: papers describe BPC-157 as the agent “in trials for inflammatory bowel disease” and demonstrate, for example, that it heals ileoileal anastomoses — surgically joined segments of small intestine — in rats, with the nitric oxide system implicated in the effect.5 A companion line of work showed BPC-157 healing colocutaneous fistulas (abnormal tracts between colon and skin, a serious complication of Crohn’s disease) in rats, again with an NO-system mechanism.6 Fistula healing is a demanding endpoint because it requires simultaneous repair of two different tissues along an abnormal tract; a reported effect there is not trivial.
Now the part that most online summaries omit. PL 14736 did reach human testing. A Phase I program in healthy volunteers examined safety, tolerability, and pharmacokinetics, and a Phase II study of a BPC-157/PL 14736 enema in patients with mild-to-moderate ulcerative colitis was undertaken. But the crucial fact for evidence assessment is this: the full results of that Phase II ulcerative-colitis trial were never published in a standalone, peer-reviewed clinical paper. The development program did not proceed to approval, and the clinical outcome data are not available for independent scrutiny in the way a published randomized trial would provide.1 This is a profound limitation. It means that the single most relevant piece of human evidence — a controlled trial in the actual target disease — exists in a form that cannot be properly evaluated, cited for efficacy, or independently verified. Reviewers outside the originating group have specifically noted that human clinical efficacy remains unconfirmed.2
So the honest IBD verdict has two parts that must be held together. The preclinical colitis and fistula data are real, peer-reviewed, and mechanistically coherent, and they were serious enough to justify a pharmaceutical development program.56 Yet the human trial that would convert that promise into evidence was either never completed to publication or its results were never released, leaving BPC-157 in an unusual limbo: a compound that was clinically interesting enough to test in patients, but whose test results the field cannot read. Treating “it was in IBD trials” as if it meant “it works for IBD” is precisely the inference the missing publication forbids.
Surgical Gut Healing: Anastomoses, Fistulas, and Short Bowel
A distinct and unusually consistent slice of the gastrointestinal literature concerns surgical healing — the repair of intestine that has been cut, rejoined, or largely removed. These models matter because they test structural, load-bearing healing rather than surface mucosal repair, and because the endpoints (anastomotic bursting pressure, leak rates, adaptation of remaining bowel) are quantitative and surgically meaningful.
In anastomosis studies, rat intestinal segments are surgically joined and the strength and integrity of the join are measured. BPC-157 has been reported to improve the healing of several types of gut anastomosis — ileoileal, colocolonic, and esophagogastric among them — with better anastomotic integrity and reduced leakage relative to controls.5 A recent review dedicated specifically to BPC-157 and intestinal anastomoses in rats catalogs this body of work and its recurring findings across surgical models.7 The fistula work described in the IBD section belongs to the same family: healing an abnormal tract is, mechanically, a demanding variant of the same challenge.6
The most striking surgical model is short bowel syndrome. After massive small-intestinal resection, the remaining bowel must adapt — villi lengthen, crypts deepen, and the muscular wall thickens — to compensate for lost absorptive surface. In a rat short-bowel model, BPC-157 was reported not only to support anastomotic healing but to enhance this adaptive response, with greater villus height, crypt depth, and muscular-layer thickness in treated animals, alongside counteraction of the concomitant deterioration seen in gut, liver, and brain.8 If real and translatable, an agent that accelerated intestinal adaptation would be genuinely valuable, because short bowel syndrome is a difficult clinical problem with few good options.
The pattern across these surgical models reinforces the mechanistic story: healing that depends heavily on angiogenesis and organized tissue remodeling is exactly what a pro-angiogenic cytoprotective agent would be expected to help, and the surgical endpoints are harder to fake than a subjective inflammation score. But the same two limitations recur without exception. First, these are rodent studies, concentrated in one research tradition. Second — and this is the load-bearing point for the whole article — there is no published human surgical trial of BPC-157 for anastomotic healing, fistula closure, or short bowel adaptation. The compound’s surgical-healing record is impressive on paper and entirely preclinical in reality.
NSAID-Induced Gut Injury and the Inflammation Question
Because the title specifically raises inflammation, the studies most directly on point are those in which BPC-157 was tested against injury driven by non-steroidal anti-inflammatory drugs (NSAIDs). This is a clarifying body of work, and it also exposes a common conceptual confusion about what “anti-inflammatory” means for this peptide.
NSAIDs such as indomethacin, aspirin, ibuprofen, and diclofenac damage the gastrointestinal tract by inhibiting cyclooxygenase and depleting protective prostaglandins, producing gastric and small-intestinal ulcers, bleeding, and increased permeability. In an early and important study, BPC-157 was reported to counteract both NSAID-induced gastrointestinal lesions and, separately, adjuvant-induced arthritis in rats — a striking pairing, because it suggested the peptide could protect the gut from an anti-inflammatory drug while itself showing benefit in an inflammatory joint model.10 Later work extended this to specific NSAIDs and to a broader “toxicity” framing. Chronic ibuprofen produced not only gastric lesions but hepatomegaly and hepatic encephalopathy in rats, and BPC-157 was reported to counteract this constellation.11 A parallel diclofenac model produced combined gastrointestinal, liver, and brain lesions, and BPC-157 — given intraperitoneally or in drinking water — was reported to be strongly protective.12
Here is the conceptual clarification that matters. When people say BPC-157 is “anti-inflammatory,” they usually imagine it suppresses the immune system the way a corticosteroid or a TNF-blocker does. The NSAID studies suggest a different and more specific picture: the peptide appears to protect and heal tissue under inflammatory or toxic stress — preserving mucosal integrity, maintaining blood flow, limiting lesion formation — rather than broadly immunosuppressing. Its reported benefit in adjuvant arthritis and in colitis is consistent with dampening the consequences of inflammation on tissue while the animal’s underlying immune response is not shut down.10 This distinction is not pedantic. A cytoprotective, pro-healing agent and an immunosuppressant are different tools with different risk profiles; conflating them leads to overstated claims in both directions. For readers weighing the peptide against inflammatory joint conditions specifically, the site’s discussion of BPC-157, inflammation, and joint pain examines that adjacent question, and the same evidence-level caveats apply there as here.
It is also worth being precise about the direction of the inflammation evidence, because it is easy to overclaim. The strongest NSAID findings concern the gut: prevention and healing of drug-induced gastric and intestinal lesions. The claims that reach further — that the peptide benefits a systemic inflammatory disease such as arthritis, or that it broadly “reduces inflammation” body-wide — rest on fewer studies and a single classic adjuvant-arthritis report, and they should be weighted accordingly.10 A responsible reading keeps the confident conclusion local (BPC-157 protects rodent gut tissue against NSAID injury) and treats the systemic-inflammation extrapolation as a weaker, secondary hypothesis rather than a co-equal finding. This graded weighting — strongest for gut cytoprotection, weaker for systemic anti-inflammatory action, absent for human effect — is the kind of internal calibration that separates an honest evidence summary from a promotional one.
The NSAID literature is, in one sense, the most decision-relevant part of the gut story, because NSAID gastropathy is an enormous real-world clinical problem and any agent that reliably prevented it would matter. But once again the ceiling is the same: these are rat models, and there is no published human trial showing that BPC-157 prevents or heals NSAID-induced ulcers in people. The mechanistic logic — restore blood flow and prostaglandin-independent cytoprotection to a mucosa stripped of its prostaglandin defenses — is elegant, and the rodent data are consistent. Elegance and consistency in rodents are reasons to run a human trial, not substitutes for one.
What the Evidence Actually Supports — A Level-of-Proof Table
Because the BPC-157 conversation so often flattens wildly different evidence levels into one enthusiastic claim, it is worth laying the gut-and-inflammation findings side by side with an explicit, honest rating of how strong each really is. The point of the table is not to dismiss the work but to show where each claim actually sits.
| Gut / inflammation claim | Model & endpoint | Honest evidence level |
|---|---|---|
| Protects against acute gastric & duodenal ulcers | Rat ethanol, cysteamine, restraint-stress lesions3 | Consistent preclinical; multiple models; rodent only |
| Accelerates mucosal / wound healing via angiogenesis | Rodent wound & GI models; VEGF, granulation4 | Strong, repeated preclinical signal; no human data |
| Reduces colitis severity | Rat TNBS / DSS / cysteamine colitis1 | Preclinical; mostly one research group |
| Heals intestinal fistulas & anastomoses | Rat colocutaneous fistula, ileoileal anastomosis56 | Preclinical; quantitative surgical endpoints; rodent only |
| Supports short-bowel adaptation | Rat massive-resection model8 | Single-context preclinical; not replicated at scale |
| Counteracts NSAID-induced GI injury | Rat indomethacin/ibuprofen/diclofenac101112 | Consistent preclinical; no human trial |
| Treats human IBD (ulcerative colitis / Crohn’s) | PL 14736 Phase II enema1 | Trial run; full results never published — unverifiable |
| Broad “anti-inflammatory” immunosuppression in humans | — | Not demonstrated; misreads cytoprotection |
The shape of the table is the real message. The preclinical rows are populated and internally consistent; the human row is either empty or, in the one case where a trial existed, unreadable. That is an unusual and important evidence profile: not “no research” and not “proven therapy,” but a deep rodent literature sitting atop an almost bare human record. Honest communication about BPC-157 lives entirely in respecting that shape.
How BPC-157 Compares With Established Gut Therapies
Placing BPC-157 beside treatments that are actually used for gut disease clarifies both what is distinctive about it and how far it stands from clinical validation. The comparison is not a competition — BPC-157 has never entered the clinical arena these agents occupy — but it shows what a validated gut therapy looks like in terms of evidence.
| Agent / class | Primary mechanism in the gut | Evidence level for gut use |
|---|---|---|
| Proton-pump inhibitors (omeprazole, etc.) | Suppress gastric acid secretion | Extensive human RCTs; approved for ulcers/GERD |
| 5-ASA / mesalamine | Topical mucosal anti-inflammatory in colon | Approved first-line for ulcerative colitis; large trials |
| Anti-TNF biologics (infliximab, adalimumab) | Neutralize TNF-α; immunosuppressive | Approved for moderate-severe IBD; pivotal RCTs |
| Sucralfate | Physical mucosal barrier; cytoprotective | Approved for ulcers; human trials |
| Misoprostol (prostaglandin analog) | Restores prostaglandin-mediated mucosal defense | Approved to prevent NSAID ulcers; human trials |
| BPC-157 | Cytoprotection, angiogenesis, NO modulation | Preclinical (rodent) only; not approved anywhere |
Two lessons fall out of the comparison. First, the established agents span exactly the mechanistic space BPC-157 occupies: acid suppression (PPIs), mucosal barrier and cytoprotection (sucralfate, misoprostol), and anti-inflammatory action (5-ASA, anti-TNF). BPC-157’s proposed profile most resembles the cytoprotective agents — sucralfate and misoprostol — in that it aims to protect and heal the mucosa rather than to suppress acid or immunity. Conceptually, misoprostol is an especially apt comparator: it restores prostaglandin-mediated defense that NSAIDs strip away, and BPC-157 is proposed to achieve a similar protective end through prostaglandin-independent, angiogenesis- and NO-based routes.410 That is a genuinely interesting mechanistic niche.
Second, and decisively, every agent in the table except BPC-157 earned its place through human randomized controlled trials and regulatory review. BPC-157 has neither. It is the only row whose evidence column reads “preclinical only.” This is the difference between a compound that is mechanistically interesting and one that is clinically established, and it cannot be papered over by the volume of rodent papers, however consistent they are. A researcher choosing what to study may find BPC-157’s cytoprotective niche compelling; a patient or clinician deciding what to use has, in the approved agents, options backed by human evidence that BPC-157 simply does not have.
Dosing and Handling in a Research Context
Because BPC-157 is encountered almost entirely as a lyophilized (freeze-dried) powder in sealed vials sold for laboratory use, a brief and strictly educational note on how it is handled in research is warranted — with the explicit understanding that this is not a usage recommendation, that no human therapeutic dose has been established, and that the compound is not an approved medicine for any condition.
The rodent studies used a wide range of doses and, notably, a wide range of routes — intraperitoneal injection, and delivery in drinking water, being common, alongside local application in some models.12 The effective doses in these studies are frequently reported in micrograms or even nanograms per kilogram, and the peptide’s reported activity across such a broad dose range is itself one of the more unusual features of the literature.3 A critical translational caveat follows directly: rodent milligram-per-kilogram or microgram-per-kilogram figures do not convert into human doses by simple arithmetic, and the oral or drinking-water efficacy reported in rats cannot be assumed to hold in humans, whose gastrointestinal physiology, transit, and enzymatic environment differ. There is no validated human dosing regimen, because there is no completed, published human efficacy trial from which one could be derived.
For the laboratory handling of research peptides generally, standard practice is well described: lyophilized material is reconstituted with sterile or bacteriostatic water directed gently against the vial wall, the vial is swirled rather than shaken (vigorous agitation can shear and denature peptides), and the reconstituted solution is refrigerated, protected from light and heat, and not subjected to repeated freeze-thaw cycles. The site’s peptide reconstitution guide walks through the arithmetic by which a fixed mass of peptide in a chosen diluent volume yields a given concentration, and the peptide glossary defines the technical terms used throughout this literature. None of this handling detail, it must be said plainly, changes the evidence question: meticulous reconstitution preserves whatever activity the molecule has but creates no human efficacy where none has been demonstrated.
Safety, Purity, and the Sourcing Problem
Safety discussion of BPC-157 must be carefully bounded, because the reassuring statements one reads are almost all derived from rodent studies and cannot be transferred wholesale to human use. Within the preclinical literature, the compound is repeatedly described as having a notably favorable safety profile: no lethal dose (LD1) was established in the toxicology reported by the originating group, and the peptide was reported to be well tolerated across a wide dose range.1 The Phase I human program conducted during the PL 14736 development is likewise reported to have found the agent safe and well tolerated in healthy volunteers at the doses studied.1 Independent reviewers acknowledge the consistently benign safety picture in animals while stressing that human clinical data remain limited and efficacy unconfirmed.2
Several caveats are essential and are routinely omitted from promotional writing:
- Short duration and small human exposure. Human safety data come from limited Phase I exposure in healthy volunteers, not from long-term administration to patients with disease. Chronic-use safety in humans is uncharacterized.
- Pro-angiogenic action cuts both ways. The very mechanism proposed to heal tissue — promotion of new blood-vessel growth — is one that warrants caution in any setting where unwanted angiogenesis is a concern, such as malignancy. This is a theoretical flag, not a documented human harm, but it is the kind of consideration a serious safety assessment cannot ignore.
- Immunogenicity and impurities. As a peptide manufactured outside regulated pharmaceutical channels, real-world BPC-157 raises concerns about peptide-related impurities and potential immune reactions — concerns that regulators have explicitly cited.13
- Sourcing and purity. Much material sold as “research chemical” BPC-157 is of unverified purity and provenance. Mislabeling, under- or over-dosing, endotoxin contamination, and inconsistent salt forms are genuine hazards that have nothing to do with the molecule’s intrinsic pharmacology and everything to do with an unregulated supply chain.
The honest safety synthesis is that BPC-157 has a clean short-term profile in rodents and in limited healthy-volunteer exposure, that no major acute toxicity signal has been reported, and that this is emphatically not the same as an established human safety record for therapeutic use. Absence of demonstrated harm in small, short studies is not evidence of long-term safety, and it is certainly not evidence of efficacy. A discussion of the peptide’s proposed durability in one specific indication, tendon and joint use, appears in the site’s review of whether evidence supports BPC-157 as a long-term therapy, and reaches the same measured conclusion the gut evidence forces here.
Regulatory Status
BPC-157’s regulatory position is frequently misrepresented, so precision matters. The single most important fact is that BPC-157 is not approved as a drug for any indication by any major regulator — not by the U.S. Food and Drug Administration, not by the European Medicines Agency, and not by comparable authorities. There is no approved gastrointestinal or anti-inflammatory indication, and therefore nothing that could be extended to gut disease or inflammation on the basis of an existing approval. The PL 14736 pharmaceutical development program that took the peptide into early human testing did not culminate in approval.1
In the United States, BPC-157 has been the subject of specific regulatory attention within the drug-compounding framework. The FDA reviewed BPC-157 as a bulk drug substance nominated for use in compounding under Section 503A and identified significant safety concerns — including insufficient characterization, questions about the peptide’s properties and impurities, immunogenicity potential, and a lack of adequate safety data for the proposed uses — placing it in the interim “Category 2” of substances that may present significant risks rather than the category of substances permitted for compounding.13 Regulatory categories in this area have continued to evolve: as of 2026 the FDA removed BPC-157 from Category 2 after the compounding nominations were withdrawn, but it was not moved to Category 1 (the list of bulk substances permitted for compounding), and it has no recognized USP/NF monograph. The net effect is a regulatory gray zone — BPC-157 is neither an approved drug nor an authorized compounding substance — and none of these procedural shifts amounts to an efficacy endorsement or a therapeutic approval for gut or inflammatory disease. The practical meaning is unchanged: BPC-157 has never been sanctioned as a treatment for any condition, and its removal from a “significant-risk” list is an administrative reclassification, not a safety clearance and certainly not a finding that it works.
A recurring public confusion deserves explicit correction. The existence of a former pharmaceutical development code (PL 14736) and of early human trials is sometimes cited as though it demonstrated that BPC-157 “was a drug” or “passed trials.” It demonstrates neither efficacy nor approval. Entering Phase I and Phase II testing means a sponsor judged a compound worth investigating in humans; it says nothing about whether the trials succeeded, and in this case the pivotal efficacy results were never published and the program did not reach approval.1 Similarly, the fact that BPC-157 is widely sold for “research use only” is a statement about how it is marketed and shipped, not a regulatory judgment that it is safe or effective for people.
The regulatory synthesis is straightforward: BPC-157 is an investigational compound with a substantial preclinical record, an incomplete and largely unpublished clinical record, no marketing approval anywhere, and active regulatory caution in at least one major jurisdiction. Any legitimate exploration of its gut-healing or anti-inflammatory potential belongs in properly designed, published human trials conducted under regulatory oversight — not in off-label or informal use.
Frequently Asked Questions
Does research show BPC-157 heals the gut?
Research shows this in animals, not yet in humans. There is a substantial and internally consistent preclinical literature — concentrated in rat models — reporting that BPC-157 protects against gastric and duodenal ulcers, accelerates mucosal and wound healing, reduces experimental colitis, and heals intestinal fistulas and anastomoses.135 What does not exist is a published, peer-reviewed human controlled trial confirming these gut-healing effects in people. So the accurate statement is that BPC-157 has a strong preclinical gut-healing signal whose human efficacy remains unconfirmed.2
Is BPC-157 an anti-inflammatory drug?
Not in the way that word is usually meant. The evidence suggests BPC-157 acts primarily as a cytoprotective, pro-healing agent that limits the tissue damage caused by inflammatory or toxic insults — for example protecting the gut against NSAID injury — rather than as a broad immunosuppressant like a steroid or a TNF-blocker.1012 It is also not an approved anti-inflammatory drug for any condition. Describing it as “anti-inflammatory” without that distinction overstates and mischaracterizes what the preclinical data show.
Was BPC-157 ever tested in humans for inflammatory bowel disease?
Yes, but the results were never fully published. Under the code PL 14736, the peptide went through a Phase I safety program in healthy volunteers and a Phase II study of an enema formulation in mild-to-moderate ulcerative colitis. The complete Phase II efficacy results were never released in a standalone peer-reviewed clinical paper, and the program did not lead to approval.1 This means the single most relevant piece of human evidence cannot be independently evaluated — a major gap, not a proof of efficacy.
How is BPC-157 thought to work?
The most consistently proposed mechanisms are promotion of angiogenesis (new blood-vessel formation, linked to VEGF signaling) and modulation of the nitric oxide system, together producing a broad cytoprotective effect that maintains mucosal blood flow and supports tissue repair.4 It has also been studied in the context of the gut-brain axis.9 Importantly, no specific high-affinity receptor for BPC-157 has been firmly established, so the mechanism is better described functionally (what it does to tissue) than molecularly (its precise target).
Why is so much of the research from one group?
The majority of BPC-157 primary studies originate from Predrag Sikiric and colleagues at the University of Zagreb, who have driven the field since the 1990s. This concentration is a genuine limitation: independent, multi-laboratory replication at scale is what would most strengthen the evidence, and reviewers outside the group have noted both the consistency of the reported effects and the fact that the work comes from relatively few investigators.2 The findings are not thereby wrong, but they are less independently corroborated than a naive reading of the paper count suggests.
Is BPC-157 approved or legal to use?
It is not approved as a drug for any condition by the FDA, EMA, or other major regulators, and there is no approved gut or anti-inflammatory indication.1 In the United States, the FDA reviewed BPC-157 for compounding and flagged significant safety concerns, declining to permit it.13 It is widely sold “for research use only,” which is a marketing and shipping designation, not a finding of safety or efficacy for people.
Can BPC-157 be taken orally for gut problems?
In rodents, oral and drinking-water administration produced effects in some models, and the peptide’s reported stability in gastric juice is often cited to argue that oral dosing is plausible for a gut target.112 But rodent oral efficacy does not automatically translate to humans, no human oral dose has been validated in a published efficacy trial, and self-administration of an unapproved compound of uncertain purity carries real risks. There is no evidence-based human oral regimen.
What would it take to actually prove BPC-157 heals the human gut?
It would require what the field currently lacks: adequately powered, randomized, double-blind, placebo-controlled human trials in defined gut conditions (for example ulcerative colitis, NSAID gastropathy, or post-surgical anastomotic healing), with objective endpoints such as endoscopic mucosal healing, ulcer rates, or leak rates — and, crucially, full publication of the results for independent scrutiny. Ideally this would include independent laboratories beyond the originating group. Until such trials exist and are published, every human-facing claim about BPC-157 and the gut remains an extrapolation from rodents.2
References
- Sikiric P, Seiwerth S, Rucman R, et al. Stable gastric pentadecapeptide BPC 157: novel therapy in gastrointestinal tract. Curr Pharm Des. 2011;17(16):1612-1632. PMID: 21548867. https://pubmed.ncbi.nlm.nih.gov/21548867/
- Gwyer D, Wragg NM, Wilson SL. Gastric pentadecapeptide body protection compound BPC 157 and its role in accelerating musculoskeletal soft tissue healing. Cell Tissue Res. 2019;377(2):153-159. PMID: 30915550. https://pubmed.ncbi.nlm.nih.gov/30915550/
- Sikiric P, Seiwerth S, Grabarevic Z, et al. The beneficial effect of BPC 157, a 15 amino acid peptide BPC fragment, on gastric and duodenal lesions induced by restraint stress, cysteamine and 96% ethanol in rats. Life Sci. 1994;54(5):PL63-68. PMID: 7904712. https://pubmed.ncbi.nlm.nih.gov/7904712/
- Seiwerth S, Milavic M, Vukojevic J, et al. Stable Gastric Pentadecapeptide BPC 157 and Wound Healing. Front Pharmacol. 2021;12:627533. PMID: 34267654; PMCID: PMC8275860. https://pmc.ncbi.nlm.nih.gov/articles/PMC8275860/
- Vuksic T, Zoricic I, Brcic L, et al. Stable gastric pentadecapeptide BPC 157 in trials for inflammatory bowel disease (PL-10, PLD-116, PL14736, Pliva, Croatia) heals ileoileal anastomosis in the rat. Surg Today. 2007;37(9):768-777. PMID: 17713731. https://pubmed.ncbi.nlm.nih.gov/17713731/
- Klicek R, Sever M, Radic B, et al. Pentadecapeptide BPC 157, in clinical trials as a therapy for inflammatory bowel disease (PL14736), is effective in the healing of colocutaneous fistulas in rats: role of the nitric oxide-system. J Pharmacol Sci. 2008;108(1):7-17. PMID: 18818478. https://pubmed.ncbi.nlm.nih.gov/18818478/
- Sikiric P, Seiwerth S, Kolenc D, et al. Stable Gastric Pentadecapeptide BPC 157 and Intestinal Anastomoses Therapy in Rats—A Review. Pharmaceuticals (Basel). 2024;17(8):1081. PMID: 39204186. https://pmc.ncbi.nlm.nih.gov/articles/PMC11357423/
- Sever M, Klicek R, Radic B, et al. Gastric pentadecapeptide BPC 157 and short bowel syndrome in rats. Dig Dis Sci. 2009;54(10):2070-2083. PMID: 19093208. https://pubmed.ncbi.nlm.nih.gov/19093208/
- Sikiric P, Seiwerth S, Rucman R, et al. Brain-gut Axis and Pentadecapeptide BPC 157: Theoretical and Practical Implications. Curr Neuropharmacol. 2016;14(8):857-865. PMID: 27138887; PMCID: PMC5333585. https://pmc.ncbi.nlm.nih.gov/articles/PMC5333585/
- Sikiric P, Seiwerth S, Grabarevic Z, et al. Pentadecapeptide BPC 157 positively affects both non-steroidal anti-inflammatory agent-induced gastrointestinal lesions and adjuvant arthritis in rats. J Physiol Paris. 1997;91(3-5):113-122. PMID: 9403784. https://pubmed.ncbi.nlm.nih.gov/9403784/
- Ilic S, Drmic D, Zarkovic K, et al. Ibuprofen hepatic encephalopathy, hepatomegaly, gastric lesion and gastric pentadecapeptide BPC 157 in rats. Eur J Pharmacol. 2011;667(1-3):322-329. PMID: 21645505. https://pubmed.ncbi.nlm.nih.gov/21645505/
- Ilic S, Drmic D, Franjic S, et al. Pentadecapeptide BPC 157 and its effects on a NSAID toxicity model: diclofenac-induced gastrointestinal, liver, and encephalopathy lesions. Life Sci. 2011;88(11-12):535-542. PMID: 21295044. https://pubmed.ncbi.nlm.nih.gov/21295044/
- U.S. Food and Drug Administration. Certain Bulk Drug Substances for Use in Compounding That May Present Significant Safety Risks (BPC-157 review under Section 503A). https://www.fda.gov/drugs/human-drug-compounding/certain-bulk-drug-substances-use-compounding-may-present-significant-safety-risks
Educational and research-use disclaimer: This article is provided solely for scientific and educational purposes. BPC-157 is not approved by the FDA, EMA, or any comparable regulator for the treatment, cure, or prevention of gastrointestinal ulcers, inflammatory bowel disease, NSAID-induced injury, or any other disease, and its gut-healing and anti-inflammatory effects have been demonstrated only in preclinical (rodent) research, with no published human efficacy trial confirming them. Nothing here is medical advice or a recommendation for human use. Material sold as BPC-157 is generally supplied “for research use only” and may vary in purity and provenance. Any legitimate investigation of this compound should occur within properly authorized preclinical or clinical research under appropriate oversight. Readers should consult qualified professionals and applicable regulations before making any decisions.