The tri-heal peptide blend is a single research vial that combines three separate peptides — TB-500 (25 mg), BPC-157 (10 mg) and KPV (10 mg) — each of which has been studied independently in preclinical tissue-repair and anti-inflammatory models. The core research question this article addresses is deceptively simple: what does the laboratory literature actually say about these three molecules, and what does it emphatically not say about the combination product that carries them together? The honest short answer is that every peptide here has its own body of animal, in-vitro or cell-culture data, but there is no published controlled study of the three-peptide mixture itself.
This distinction matters more than any marketing headline. In the discussion below, each claim is tagged to its real evidence tier — preclinical animal, in-vitro, or theoretical — and the article states plainly, repeatedly, that none of these compounds is FDA-approved for any human indication and that the Tri-Heal combination has zero combination-specific data behind it. This is a reference for how researchers describe and handle these materials, not guidance for human use.
Research Context: What Is the Tri-Heal Peptide Blend?
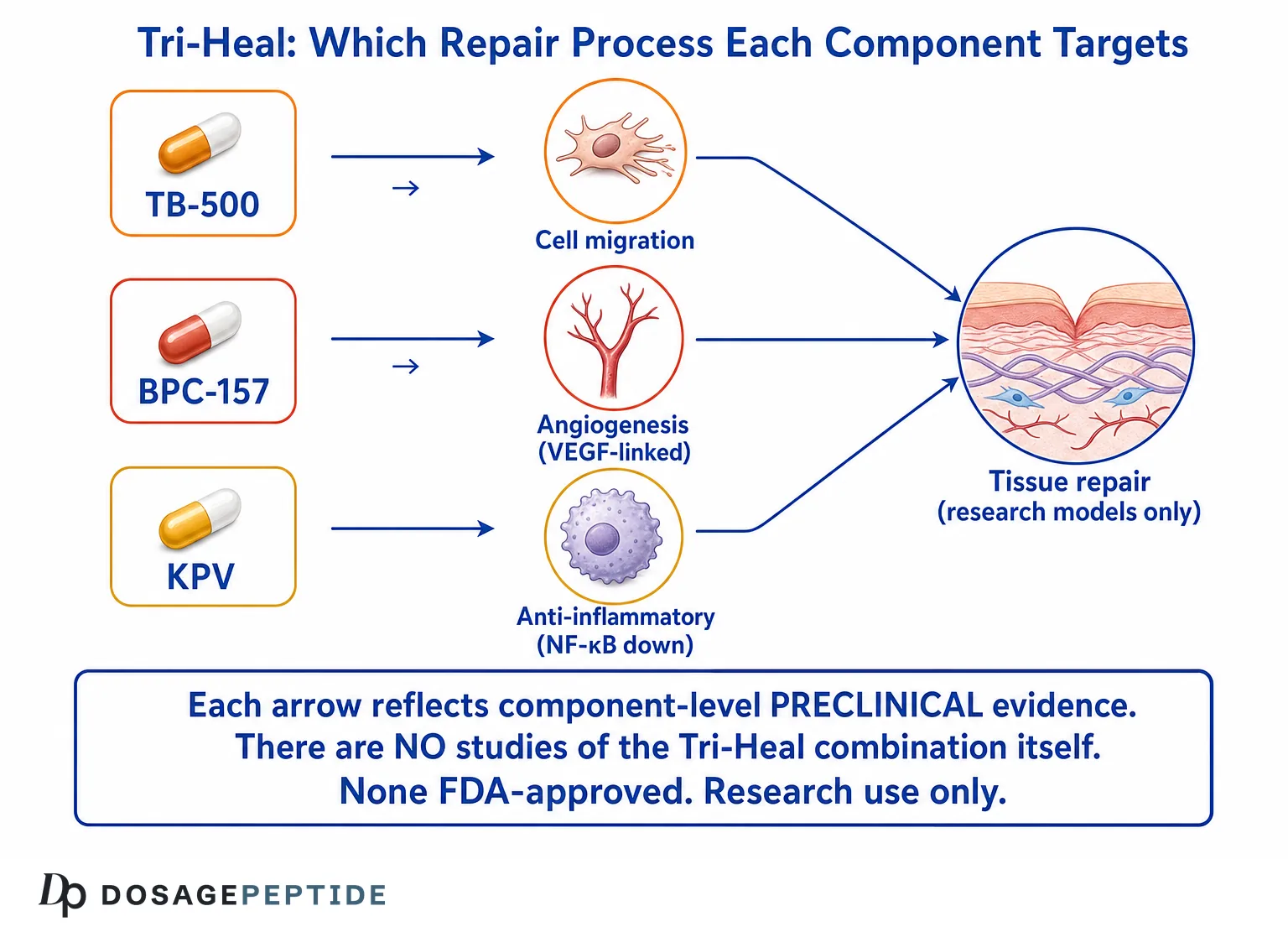
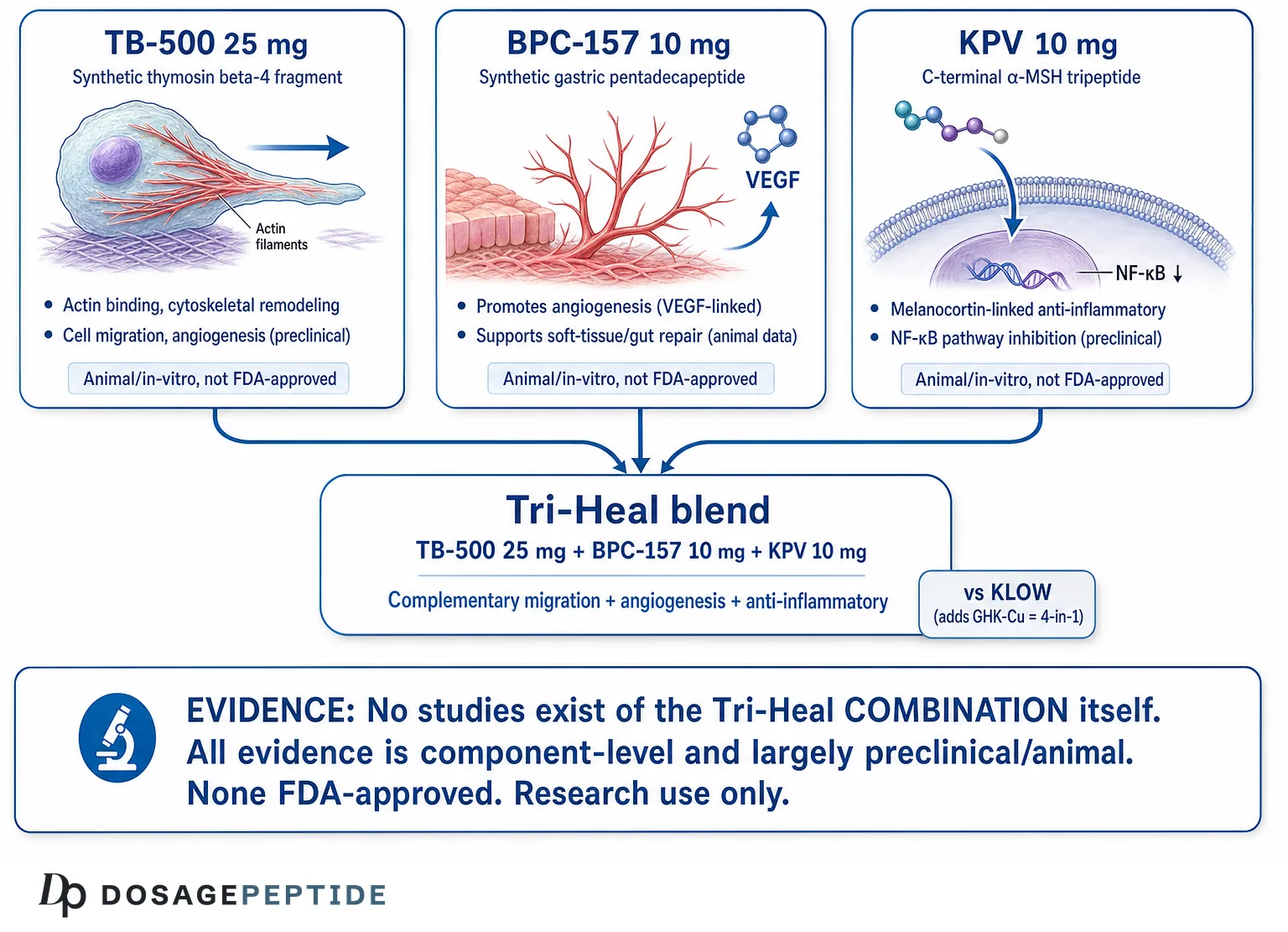
Tri-Heal is a compounded research blend — a “3-in-1” healing peptide blend in the informal vocabulary of the peptide research community — that co-formulates three distinct peptides in a single lyophilized vial. The typical labeled composition is TB-500 at 25 mg, BPC-157 at 10 mg and KPV at 10 mg, giving a nominal 45 mg of total peptide per vial. The rationale offered for co-formulation is that each component targets a different, theoretically complementary node of the tissue-repair cascade: cell migration and cytoskeletal remodeling (TB-500), angiogenesis and growth-factor signaling (BPC-157), and melanocortin-linked anti-inflammatory signaling (KPV).
It is essential to frame what “blend” means here. A blend is a physical mixture of already-characterized research chemicals; it is not a novel, separately-validated drug. When a study is cited in this article, it studied one of these peptides in isolation, usually in rodents or in cultured cells. No investigator has published a randomized, controlled, or even descriptive preclinical experiment on the TB-500 + BPC-157 + KPV mixture as a unit. Readers evaluating the Tri-Heal TB-500 25 mg / BPC-157 10 mg / KPV 10 mg vial reference page should treat the combination as an empirically unstudied arrangement of individually-studied parts.
Where the Name Comes From
The “Tri” simply denotes three peptides, and “Heal” reflects the shared preclinical theme of the components: each has appeared in wound-healing, gut-injury, tendon, or anti-inflammatory literature. The naming is descriptive rather than a regulatory or clinical designation. There is no monograph, no pharmacopeia entry, and no clinical trial registry record for a product called Tri-Heal. That absence is itself an important data point about the evidence tier.
Why Researchers Distinguish Blends From Single Agents
In pharmacology, combining agents introduces the possibility of additive, synergistic, or antagonistic interaction, plus shared-solvent stability questions and altered pharmacokinetics. None of these interaction parameters has been measured for Tri-Heal. Anyone reasoning about the blend is therefore extrapolating from single-agent data and assuming the components behave in a mixture the same way they behave alone — an assumption that is untested. For single-agent grounding, the component deep-dives on what BPC-157 is and what research says about TB-500 for tissue repair are the appropriate starting references.
It also helps to place Tri-Heal in the wider landscape of “recovery” blends that have appeared in the research-chemical market. These products generally take two or more peptides with overlapping preclinical healing literature and package them together under a name that signals the intended theme — recovery, repair, or healing. The appeal is convenience and the narrative of “covering more bases” with one vial. The scientific reality is that bundling does not generate new evidence: a blend inherits the (largely preclinical) strengths and the (substantial) weaknesses of each of its parts, and then adds fresh uncertainty about interactions that no one has measured. Understanding this pattern is more useful than memorizing any single product, because the same evidentiary logic applies to every multi-peptide blend in the category.
What Are the Three Components in a Tri-Heal Vial?
Before discussing mechanisms, it helps to define each molecule precisely, because loose naming causes much of the confusion in this space. The table below summarizes the three peptides, their molecular identity, and their strongest published evidence tier as of the current literature.
| Component | What it actually is | Typical Tri-Heal load | Strongest evidence tier | FDA status |
|---|---|---|---|---|
| TB-500 | A synthetic fragment marketed as related to thymosin beta-4 (Tβ4), a naturally occurring 43-amino-acid actin-sequestering peptide | 25 mg | Preclinical (animal + in-vitro wound/cardiac/corneal models) | Not approved; research chemical |
| BPC-157 | A synthetic pentadecapeptide (15 amino acids) derived from a partial sequence of a human gastric juice protein | 10 mg | Preclinical (rodent gut, tendon, ligament, vascular models) | Not approved; research chemical |
| KPV | Lysine-Proline-Valine, the C-terminal tripeptide (residues 11–13) of α-melanocyte-stimulating hormone (α-MSH) | 10 mg | Preclinical/in-vitro (IBD models, epithelial cell anti-inflammatory assays) | Not approved; research chemical |
A Note on the TB-500 / Tβ4 Distinction
“TB-500” is a research-market label, not a clean scientific synonym for thymosin beta-4. Much of the peer-reviewed literature studies full-length Tβ4 or its actin-binding domain, whereas material sold as TB-500 is often described as a fragment. When this article cites Tβ4 studies, it is citing the molecule the academic literature actually examined; the degree to which a given TB-500 preparation reproduces those findings depends on its exact sequence and purity, which vary by source and are rarely independently verified. This is a real limitation of translating the published science onto the vial.
KPV Is a Genuine Fragment of α-MSH
KPV is unusual among the three because it is a well-defined, naturally occurring tripeptide corresponding to the C-terminal end of α-MSH. That precise identity is why its anti-inflammatory literature is relatively coherent: multiple independent groups have studied the same three-residue sequence. The dedicated reference on KPV as an anti-inflammatory peptide for gut, skin and beyond covers this melanocortin lineage in more depth.
Mechanisms Studied: How Might Each Peptide Work?
This section walks through the mechanism-of-action research for each component. Every mechanism described below is drawn from preclinical or in-vitro studies unless otherwise stated, and none has been demonstrated for the Tri-Heal combination. The word “may” is doing real work throughout — these are studied hypotheses, not established human effects.
TB-500 / Thymosin Beta-4: Actin Binding and Cell Migration
The best-characterized biochemical role of thymosin beta-4 is as the principal intracellular G-actin–sequestering peptide in mammalian cells. By binding monomeric actin, Tβ4 helps regulate the pool of actin available for polymerization, which is central to cytoskeletal remodeling — the machinery a cell uses to change shape and migrate.[1] In wound-healing models, this actin-regulating activity has been linked experimentally to accelerated keratinocyte and endothelial cell migration into a wound bed.
In one frequently cited dermal study, topical or injected Tβ4 accelerated wound closure and increased collagen deposition and angiogenesis in rodent models compared with controls.[2] Separate corneal-injury work reported that Tβ4 promoted epithelial cell migration and suppressed inflammatory signaling, including reduced NF-κB activation in the injured cornea.[3] Taken together, the preclinical Tβ4 literature describes three recurring themes: cell migration, angiogenesis (new blood-vessel formation), and modulation of inflammation. All of it is animal or cell-based; there is no approved human tissue-repair indication.
It is worth understanding why actin sequestration connects to migration in the first place, because it explains the theoretical logic of putting Tβ4-related material in a healing blend. Cell migration depends on the coordinated assembly and disassembly of actin filaments at the leading and trailing edges of a moving cell. By buffering the pool of free actin monomers, Tβ4 participates in the regulated availability of building blocks for that process. A migrating keratinocyte closing a wound, or an endothelial cell sprouting a new capillary, both rely on this cytoskeletal choreography. This is the biochemical bridge between a “housekeeping” actin protein and the tissue-level phenomenon of wound closure that the studies report.
Beyond the actin story, some Tβ4 research has explored anti-fibrotic and anti-apoptotic angles — that is, reducing excessive scarring and protecting cells from programmed death in the stressed environment of an injury. The cardiac-injury literature in particular generated interest in Tβ4 as a signaling peptide that might support progenitor-cell activity. As with everything in this section, these are hypotheses supported by animal and cell data, not established human mechanisms, and the material sold as TB-500 is not guaranteed to reproduce the exact molecule these studies used.
BPC-157: Angiogenesis and Growth-Factor Signaling
BPC-157 is a stable synthetic pentadecapeptide whose preclinical signature is angiogenesis and soft-tissue repair. Reviews of the vascular literature describe BPC-157 promoting the formation of new blood vessels in injury models, an effect several authors have connected to the vascular endothelial growth factor (VEGF) pathway and endothelial nitric oxide signaling.[4] Because angiogenesis restores blood supply to damaged tissue, it is a plausible upstream driver of the healing effects reported across BPC-157 studies.
In tendon and ligament models, BPC-157 has been reported to enhance the outgrowth, survival and migration of tendon fibroblasts in culture, and to influence growth-hormone receptor expression in those cells.[5] A widely referenced functional study found that BPC-157 accelerated the healing of transected rat Achilles tendon and improved biomechanical and functional outcomes relative to controls.[6] The peptide is perhaps best known for gastrointestinal-protection experiments, where rodent models of gastric and intestinal injury showed reduced lesion severity.[7]
Several authors have also proposed that BPC-157 interacts with the nitric oxide (NO) system and may stabilize or upregulate pathways involved in endothelial function, and some rodent work describes effects on the vascular endothelial growth factor receptor 2 (VEGFR2) signaling axis as a route to the angiogenic response. In injury settings, the peptide has been described as promoting the formation of new microvessels around a wound and as supporting the recruitment of the cells needed to rebuild connective tissue. These are mechanistically coherent observations, but they remain descriptions of what happened in a controlled animal preparation rather than validated human pathways.
A distinctive feature of the BPC-157 literature is its breadth: beyond tendon and gut, rodent studies have touched on ligament, muscle, bone, nerve, and even effects framed around the brain–gut axis.[14] Breadth can look impressive, but it is also a reason for caution — a peptide reported to help almost every tissue in almost every model invites careful scrutiny of study design, controls, blinding, and independent replication. The most defensible summary is narrow: in specific rodent injury models, BPC-157 improved specific reparative endpoints, plausibly through angiogenesis and fibroblast support.
The consistent caveat, repeated by the authors themselves, is that this is animal and in-vitro work. There is no completed, published, adequately powered human clinical trial establishing efficacy for any of these indications, and BPC-157 is not FDA-approved. A fuller treatment of the single agent lives in the BPC-157 healing peptide explainer.
KPV: Melanocortin-Linked, NF-κB–Directed Anti-Inflammatory Signaling
KPV occupies a different mechanistic niche from its two vial-mates. As the C-terminal tripeptide of α-MSH, it retains a portion of the anti-inflammatory activity attributed to the parent hormone but without the pigmentary (melanocyte-stimulating) effects of the full molecule.[8] The melanocortin system — and α-MSH–derived peptides in particular — has been studied as a brake on pro-inflammatory transcription.
The most-cited KPV mechanism is inhibition of the NF-κB pathway, a master regulator of inflammatory gene expression. In intestinal epithelial and immune cell models, KPV reduced the activation of NF-κB and downstream pro-inflammatory cytokine production.[9] Notably, one influential study reported that KPV is taken up into intestinal epithelial cells via the peptide transporter PepT1, and that this uptake was associated with reduced inflammation in murine colitis models.[9] A companion body of work in murine inflammatory bowel disease models found that the melanocortin-derived tripeptide KPV had measurable anti-inflammatory potential.[10]
Broader reviews of α-MSH–related peptides frame KPV within a class of small molecules with anti-inflammatory and immunomodulating activity in vitro and in animal models.[11] Again, the tier is preclinical/in-vitro; KPV is not an approved anti-inflammatory drug, and its human pharmacology is essentially uncharacterized in the peer-reviewed literature.
Two features make KPV interesting to researchers relative to the full α-MSH molecule. First, because it is only three residues, it is small, comparatively stable, and cheap to synthesize, and it can enter certain cells through the di/tri-peptide transporter PepT1 rather than depending solely on the classical melanocortin receptors. Second, it appears to retain anti-inflammatory activity while shedding the pigment-stimulating effect of the parent hormone, which is why some authors describe it as separating the “anti-inflammatory” function of α-MSH from its “melanocyte” function. Whether KPV’s effects are strictly receptor-mediated, transporter-mediated, or a combination is still debated in the preclinical literature.
Mechanistically, the NF-κB story is the through-line. NF-κB is a transcription factor that, when activated, switches on genes for many pro-inflammatory cytokines and mediators. By interfering with this activation — reported in intestinal epithelial cells and in models of colitis — KPV is described as lowering the inflammatory output of the tissue. In the context of a healing blend, the theoretical role is not to build tissue directly but to reduce the inflammatory “noise” that can prolong injury and impair repair. That is a plausible complementary function, but its contribution to any combined healing effect has never been isolated experimentally.
Why Combine These Three? The Theoretical Rationale
The stated logic behind Tri-Heal is that the three peptides address non-overlapping steps of tissue repair, so a mixture might, in theory, cover more of the cascade than any single component. It is worth laying out that theory explicitly — while stressing that it is a hypothesis constructed from single-agent data, not a finding.
The Complementary-Node Hypothesis
- Migration and cytoskeletal remodeling (TB-500/Tβ4): supplies the actin-regulating activity linked to cell movement into a wound.
- Angiogenesis and growth-factor signaling (BPC-157): supplies the new-vessel-formation and fibroblast-support activity that could restore perfusion to repairing tissue.
- Anti-inflammatory tone (KPV): supplies NF-κB–directed dampening of inflammation, which in principle could limit collateral tissue damage during repair.
On paper, migration + angiogenesis + anti-inflammation is a tidy narrative that maps onto the classical phases of wound healing (inflammation, proliferation, remodeling). That narrative is exactly why the blend exists. But a tidy narrative is not evidence. The proposition that these three activities combine additively — let alone synergistically — when the peptides are co-administered has never been tested in any published model.
What Synergy Would Require to Demonstrate
To claim genuine combination benefit, a study would need at minimum: a control group, single-agent arms for each peptide, the combination arm, and a quantitative endpoint, with statistical analysis for interaction (for example, tests distinguishing additive from synergistic effects). No such experiment appears in the literature for Tri-Heal. Until it exists, the “complementary node” rationale should be read as a design intention, not a demonstrated property. The comparably-marketed two-peptide product is discussed in the BPC-157 + TB-500 recovery blend explainer, which faces the identical evidence gap at the combination level.
The Fixed-Ratio Problem
A blend commits to a fixed ratio — here 25:10:10 by mass. In genuine combination pharmacology, the optimal ratio of two or more agents is an empirical question answered by dose-response experiments, and the best ratio for one endpoint may be wrong for another. Tri-Heal’s ratio was not derived from any such experiment; it reflects a manufacturing choice, not an optimized finding. This means even if one accepted the (untested) premise that the peptides act complementarily, there is no basis for asserting that this particular ratio is the one that would maximize any complementary effect. A researcher reasoning rigorously would treat the ratio as arbitrary until data justify it.
Potential for Interaction, Not Just Addition
Co-formulation also raises the possibility of chemical interaction in the vial and biological interaction in the tissue. Peptides in shared solvent can, in principle, affect one another’s stability or aggregation, and there is no published stability study for this specific mixture. Biologically, an anti-inflammatory component (KPV) and pro-angiogenic components (BPC-157, Tβ4) are not guaranteed to be neutral toward each other, since inflammation and angiogenesis are intertwined processes. Whether the net interaction is additive, synergistic, or partially self-cancelling is simply unknown — and “unknown” is the accurate word, not “synergistic.”
How Does Tissue Repair Work, and Where Would Each Peptide Fit?
To evaluate the blend’s logic fairly, it helps to have the biology of wound healing in view. Classical tissue repair is described in overlapping phases, and the Tri-Heal narrative maps each component onto one or more of them. Laying this out makes the theoretical appeal clear while also exposing where the reasoning outruns the data.
The Phases of Repair
- Hemostasis: immediately after injury, the body forms a clot to stop bleeding and creates a provisional matrix. None of the three peptides is primarily a hemostatic agent.
- Inflammation: immune cells clear debris and pathogens; controlled inflammation is necessary, but excessive or prolonged inflammation impairs healing. This is the phase KPV’s NF-κB–directed activity theoretically modulates.
- Proliferation: new tissue is built — fibroblasts lay down collagen, keratinocytes migrate to close the surface, and angiogenesis restores blood supply. This is where Tβ4’s migration activity and BPC-157’s angiogenic and fibroblast-supporting activity are theoretically relevant.
- Remodeling: the new matrix matures and reorganizes over weeks to months, and scar tissue is refined. Anti-fibrotic signaling attributed to Tβ4 in some models would sit here.
The Map Is Elegant — and Unproven
On this scaffold, the blend looks almost purpose-built: an anti-inflammatory for the inflammatory phase, two pro-migration/pro-angiogenesis agents for the proliferative phase, and a possible anti-fibrotic touch for remodeling. This is exactly the story that makes a “3-in-1 healing blend” sound rational. But mapping single-agent activities onto a textbook diagram is a thought experiment, not evidence. The phases overlap in time, the peptides were never studied together across those phases, and the actual kinetics of a co-administered mixture in a single tissue are unmeasured. The map should be read as an illustration of the intended logic, not as a demonstrated mechanism of the product.
Why Overlap Complicates the Story
Because inflammation and proliferation overlap rather than occur in neat sequence, an agent that suppresses inflammation and an agent that drives angiogenesis are acting on the same tissue at the same time. In some contexts inflammatory signaling actually promotes early angiogenesis, so dampening it is not unambiguously helpful for vessel formation. This is precisely the kind of interaction that only a real combination study could resolve. It is a concrete example of why the neat phase-map, however appealing, cannot substitute for data on the mixture itself.
Current Evidence Level: What Does the Research Actually Show?
This is the section that the primary keyword — tri-heal peptide blend — most needs, because the honest evidence assessment is the whole point. Here it is, stated as plainly as possible.
Combination-Specific Evidence: None
There are zero clinical trials of Tri-Heal. There are also zero published preclinical (animal or in-vitro) studies of the specific TB-500 + BPC-157 + KPV combination. A search of the biomedical literature and clinical-trial registries returns no controlled experiment on the three-peptide mixture as a unit. Every mechanistic and outcome claim that could be attached to Tri-Heal is, in reality, an extrapolation from studies of the individual peptides administered alone. This is the single most important fact in the article, and no amount of component-level data changes it.
Component-Level Evidence: Preclinical, Not Approved
The table below grades where each component actually sits. “Preclinical” means animal and/or cell-based studies without adequate human efficacy trials. None of the three has an FDA approval for any indication relevant to the blend.
| Component | Highest evidence tier reached | Human clinical efficacy trials? | FDA-approved indication? |
|---|---|---|---|
| TB-500 / Tβ4 | Preclinical animal + in-vitro; limited early-phase human safety exploration of Tβ4 in specific conditions (not the TB-500 research chemical) | No adequate efficacy trials for general tissue repair | No |
| BPC-157 | Preclinical animal + in-vitro only | No completed, published, adequately powered efficacy trials | No |
| KPV | Preclinical animal + in-vitro only | No | No |
| Tri-Heal (combination) | No studies of any tier | No | No |
How to Read Preclinical Data Responsibly
Preclinical promise is common; clinical confirmation is rare. Across drug development, a large majority of compounds that look effective in rodent models fail to show benefit or safety in humans. Rodent wound-healing kinetics, dosing scaled to body weight, controlled injury models, and the absence of human comorbidities all limit how far animal results transfer. When a source describes a peptide “accelerating healing,” the accurate translation is “accelerated a defined endpoint in a specific animal or cell model,” not “heals people.” That discipline is the correct lens for every claim in this article.
There is a further, subtler point about how single-agent evidence gets transferred to a blend. Even if one fully accepted every BPC-157, Tβ4, and KPV study at face value, those studies used their own doses, routes, timing, and endpoints. The blend fixes a single ratio and a single administration event for all three at once. Nothing guarantees that a dose of BPC-157 shown to help in one rat tendon study corresponds to the amount delivered by a Tri-Heal vial at whatever volume it is reconstituted to, or that the timing that worked in isolation is right when the other two peptides are present. So the transfer from “the components have data” to “the blend should work” involves several unstated leaps, each of which is itself unvalidated.
Tri-Heal vs KLOW: How Do the Blends Differ?
A common comparison in the research-blend space is Tri-Heal (three peptides) versus KLOW (four peptides). The comparison is worth making precisely, because the difference is one added component — and that component changes the theoretical profile.
The Compositional Difference
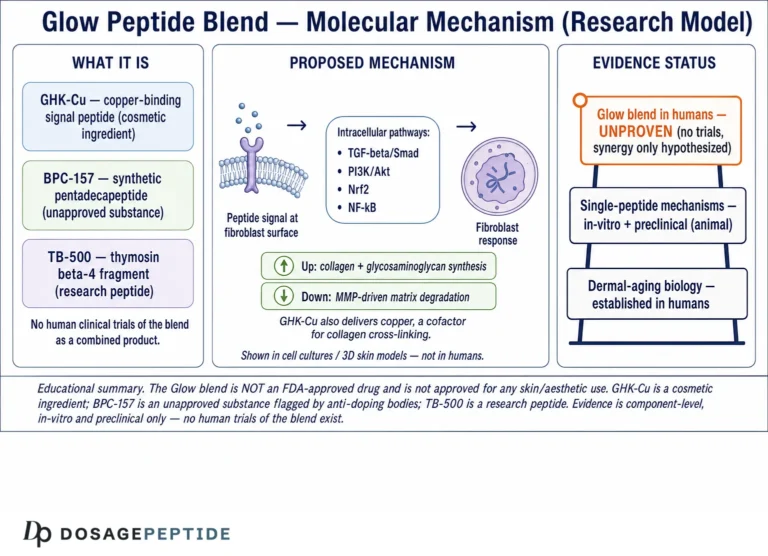
KLOW is generally described as a 4-in-1 blend adding GHK-Cu (a copper-binding tripeptide) to the KPV, TB-500 and BPC-157 trio, so the two products share three of their components. GHK-Cu (glycyl-L-histidyl-L-lysine copper complex) is a naturally occurring copper-peptide studied preclinically for skin remodeling, antioxidant activity, and modulation of genes involved in tissue regeneration.[12]
| Feature | Tri-Heal (3-in-1) | KLOW (4-in-1) |
|---|---|---|
| TB-500 | Yes | Yes |
| BPC-157 | Yes | Yes |
| KPV | Yes | Yes |
| GHK-Cu | No | Yes (added component) |
| Theoretical extra node | — | Copper-peptide skin-remodeling / antioxidant signaling |
| Combination-specific studies | None | None |
The Evidence Gap Is Identical
The crucial point of the comparison is that adding GHK-Cu does not add combination evidence. KLOW, like Tri-Heal, has no published study of its specific multi-peptide mixture; the extra component simply adds one more single-agent literature (GHK-Cu’s) to extrapolate from. So the choice between the two blends cannot be made on combination data, because none exists for either. Researchers comparing them are comparing theoretical compositions, not measured outcomes. The dedicated KLOW peptide blend explainer lays out the four-component version with the same honesty applied here.
What GHK-Cu Adds to the Theory
GHK-Cu is a naturally occurring copper-binding tripeptide (glycyl-L-histidyl-L-lysine complexed with copper) whose preclinical literature centers on skin remodeling, extracellular-matrix modulation, and antioxidant activity. Pickart and colleagues have described GHK and GHK-Cu as influencing the expression of a broad set of genes involved in tissue regeneration and as supporting the synthesis of collagen and other matrix components in skin models.[12] In the KLOW rationale, GHK-Cu is meant to reinforce the matrix-remodeling and antioxidant side of the story, complementing the migration, angiogenesis, and anti-inflammatory nodes already covered by the other three. The copper-carrying property is also the reason GHK-Cu is often discussed in cosmetic and dermatological research contexts specifically.
Choosing on Theory Is Not Choosing on Evidence
Someone deciding between Tri-Heal and KLOW is, in practice, choosing between three theoretical nodes and four. It is tempting to assume “more peptides equals more benefit,” but that is not a defensible inference. Adding a component adds complexity, potential interactions, and another unverified single-agent literature to lean on — without adding a single study of how the enlarged mixture behaves. A rigorous researcher would note that the four-way blend is, if anything, further from being characterized than the three-way blend, because the number of possible interactions grows with each component. Neither product can claim outcome data; the comparison is entirely at the level of intended design.
What Does Preclinical Research Say About Tissue Repair Models?
To give the reader a fair picture of the underlying science — without overstating it — this section summarizes the kinds of tissue-repair endpoints the individual components have been studied against. These are the experiments that motivate the blend concept.
Soft-Tissue and Tendon Models (Primarily BPC-157)
Much of the musculoskeletal interest in BPC-157 comes from rodent studies of tendon, ligament and muscle transection or crush injury, where treated animals showed improved functional recovery and histological repair relative to controls.[13] The proposed mechanism ties back to angiogenesis and fibroblast support. These are consistent findings across several groups, which is a point in the peptide’s favor at the preclinical tier — but consistency in rodents is not the same as human efficacy.
Wound, Corneal and Cardiac Models (Primarily Tβ4)
Thymosin beta-4 has been studied in dermal wound healing, corneal epithelial repair, and cardiac injury models, with recurring reports of accelerated cell migration, angiogenesis, and reduced inflammatory signaling.[2][3] The cardiac work in particular generated substantial academic interest in Tβ4 as a regenerative signaling peptide, though translating that into approved human therapy has not occurred.
Gut and Mucosal Inflammation Models (Primarily KPV)
KPV’s tissue-repair relevance is mostly framed through inflammation control rather than direct structural repair. In murine colitis, KPV administration — including oral delivery leveraging PepT1 transport — was associated with reduced inflammatory markers and mucosal damage.[9][10] The theoretical contribution to a healing blend is that lower inflammatory tone could create a more favorable environment for the reparative activities of the other two peptides — a reasonable hypothesis that, once more, has not been tested in the combination.
Putting the Models Together
Notice that the three peptides were studied in different tissues, species strains, injury models, and delivery routes. There is no common experimental platform on which all three were compared head-to-head, let alone combined. So even the “complementary” story is stitched together from methodologically heterogeneous studies. This heterogeneity is a limitation, not a strength, when reasoning about a fixed-ratio blend.
To make the heterogeneity concrete: BPC-157’s marquee results are in rat gastrointestinal and Achilles-tendon models with the peptide given by injection or in drinking water; Tβ4’s are in dermal, corneal, and cardiac models, sometimes topical, sometimes systemic; KPV’s are largely in murine colitis and in cultured epithelial or immune cells, with oral and local delivery. These differ in species, injury type, dosing schedule, and the very definition of a successful outcome. Assembling them into a single “healing” narrative requires ignoring how little the experimental contexts have in common. The narrative can be a useful way to organize the hypotheses, but it must not be mistaken for evidence that the three effects co-occur when the peptides are given together in one preparation.
What a Convincing Combination Study Would Look Like
If a laboratory wanted to actually test Tri-Heal, a credible design would take a single, standardized injury model (say, a defined rodent tendon or excisional wound), and run parallel arms: vehicle control, each peptide alone at matched doses, the full three-peptide blend at its labeled ratio, and ideally several alternative ratios. Blinded, quantitative endpoints (tensile strength, closure rate, histology, vessel density, inflammatory markers) measured at fixed timepoints would then reveal whether the blend outperforms its best single component and whether the interaction is additive or synergistic. Nothing resembling this exists in the published record for Tri-Heal, which is why every statement about the blend’s combined effect remains hypothesis rather than result.
How Is Tri-Heal Described and Handled in Research Settings?
This section is reference material on how the blend is characterized and handled by laboratories, framed strictly for research settings. It is not a dosing protocol and contains no human-use instructions. For the specific labeled composition and handling reference, see the Tri-Heal vial reference page.
Reconstitution and Stability Considerations
Lyophilized research peptides are typically reconstituted with bacteriostatic or sterile water for laboratory handling, and the resulting concentration is a function of the total peptide mass and the solvent volume added. Because Tri-Heal contains three peptides at different loads (25/10/10 mg), the concentration of each component in the reconstituted solution differs proportionally — a point researchers note when characterizing aliquots. Peptides are generally sensitive to repeated freeze-thaw cycles, light, and elevated temperature; stability of a three-peptide mixture in shared solvent is not independently documented for this blend, which is itself an open question.
Purity and Identity Verification
A recurring problem in the research-chemical market is the gap between labeled and actual content. Independent analytical verification — for example mass spectrometry and HPLC purity analysis — is the only way to confirm that a vial contains the stated peptides at the stated masses. For a blend, this is more complex than for a single agent because each component must be resolved and quantified. Any reasoning about the blend that assumes label accuracy without analytical confirmation is making an unverified assumption. Purity also matters beyond identity: synthesis byproducts, truncated sequences, residual solvents, and endotoxin are all quality variables that a certificate of analysis from an independent lab would address and that a label alone does not.
Because the three peptides carry different masses in the same vial, researchers characterizing the material typically calculate each component’s concentration separately after reconstitution rather than treating the vial as a single “45 mg” unit. This matters for any analytical or documentation work, since the three peptides also differ in their solubility, isoelectric behavior, and susceptibility to degradation, meaning they may not age identically in shared solvent. The practical consequence is that the ratio printed on the label describes the dry powder, not necessarily the ratio of intact, active peptide in a solution that has been stored for some time — another reason the blend’s real-world composition is an empirical question rather than a given.
Why “Handling Reference” Is Not “Dosing Advice”
Describing how a material is reconstituted and stored in a laboratory is categorically different from recommending that a person administer it. None of these peptides is approved for human use, no human dosing has been established in adequate trials, and this article makes no human-use recommendation of any kind. The handling notes exist so that the research context is complete, not to imply a protocol for people.
Limitations: What the Evidence Cannot Tell Us
A dedicated limitations section is warranted because the limitations here are unusually severe — they define the topic more than the positive findings do.
No Combination Data at Any Tier
The overriding limitation, stated a final time for clarity: there is no study — clinical or preclinical — of the Tri-Heal combination. Every inference about the blend is extrapolation. Interactions among the three peptides (pharmacodynamic or chemical) are unmeasured. Whether co-administration changes the activity, stability, or safety of any component is unknown.
Single-Agent Data Is Itself Preclinical and Uneven
- Species and model gaps: most findings are in rodents or cultured cells, which translate poorly to humans.
- Sequence and purity ambiguity: particularly for TB-500 versus academic Tβ4, the material studied and the material sold are not guaranteed to be identical.
- Publication and reporting factors: a portion of the BPC-157 literature comes from a small number of overlapping research groups, which is a recognized consideration when weighing independent replication.
- Absent human pharmacokinetics: for KPV and BPC-157 especially, human absorption, distribution, metabolism and excretion are essentially uncharacterized in peer-reviewed work.
Regulatory and Safety Unknowns
Because none of the components is FDA-approved, there is no regulatory safety review, no established adverse-event profile from controlled human study, and no manufacturing quality standard applied to the blend. Long-term safety data do not exist. The absence of reported problems in short rodent studies is not evidence of human safety. The unmeasured interaction question compounds this: even if each peptide had a benign profile alone, a mixture’s combined and interacting effects would need their own evaluation, which has never been performed here.
What Would Change the Picture
The evidence level would meaningfully improve only with: (1) analytical confirmation of blend composition, (2) preclinical studies of the specific combination against single-agent and control arms, and (3) eventually, properly designed human trials. None of these currently exists. Until they do, Tri-Heal remains a research blend built on component-level, largely preclinical rationale.
What Questions Should Researchers Ask Before Trusting Blend Claims?
Because Tri-Heal sits at the intersection of genuine preclinical science and unregulated marketing, a short checklist of critical questions helps separate what is known from what is asserted. Each question below has a defensible answer grounded in the evidence discussed above.
Is the claim about the blend or about a component?
This is the first and most important filter. Almost every favorable statement one encounters about Tri-Heal is actually a statement about one of its components studied alone. When a claim is attached to the blend, ask for the specific study of the three-peptide mixture. There is none. Reassigning single-agent results to the combination is the central rhetorical move to watch for, and it is not valid.
What tier of evidence supports it?
For each component claim, identify whether the underlying data are in-vitro (cells in a dish), animal, or human, and whether the study had proper controls. The honest tiering here is: BPC-157 and Tβ4/TB-500 — animal and in-vitro; KPV — animal and in-vitro; the combination — nothing. No claim in this space currently rests on adequate human efficacy data.
Does the material match what was studied?
Especially for TB-500, the research-market product may not be identical to the Tβ4 molecule in the academic papers. Without analytical confirmation (mass spectrometry, HPLC) of a specific vial, one cannot assume the contents match either the label or the studied compound. For a three-peptide blend, that verification is harder and rarely available to the end user.
Who ran the studies, and were they replicated?
Independent replication across multiple groups strengthens a finding. Part of the BPC-157 literature originates from a concentrated set of collaborating authors, which is a reason to weigh independent confirmation carefully rather than treating volume of publications as if it were breadth of independent evidence. The KPV colitis findings, by contrast, have contributions from more than one group, which is a modest point in their favor at the preclinical tier.
Is there a regulatory or safety framework behind it?
None of these peptides has undergone the controlled human safety evaluation that FDA approval entails, so there is no established adverse-event profile, no approved manufacturing standard for the blend, and no long-term human safety data. Absence of reported harm in brief rodent experiments is not the same as demonstrated human safety. This question alone places Tri-Heal firmly in the research-only category.
Safety and Regulatory Status in a Research Context
To close the substantive discussion, the regulatory posture deserves an explicit statement. TB-500, BPC-157 and KPV are research chemicals. None is an approved drug in the United States for the indications implied by a healing blend, and the combination has no regulatory recognition whatsoever. Materials of this kind are generally labeled for laboratory research use only and are not intended for diagnosis, treatment, cure, or prevention of any disease. Additionally, some of these peptides appear on sport anti-doping prohibited lists, which is a further reason the research community treats them as controlled laboratory materials rather than consumer products. Nothing in this article should be read as endorsing human administration.
Frequently Asked Questions
What is the Tri-Heal peptide blend?
Tri-Heal is a research-market vial that combines three separately-studied peptides — TB-500 (25 mg), BPC-157 (10 mg) and KPV (10 mg) — in one lyophilized product. The rationale is that each targets a different node of tissue repair: cell migration, angiogenesis, and anti-inflammatory signaling. It is a physical mixture of research chemicals, not an approved drug, and it has no combination-specific studies of any kind.
Are there any clinical trials of Tri-Heal?
No. There are no clinical trials of the Tri-Heal combination, and there are also no published preclinical (animal or in-vitro) studies of the specific three-peptide mixture. All available evidence is component-level, meaning it studied TB-500, BPC-157, or KPV individually. Any claim about the blend as a unit is an extrapolation from single-agent data, not a tested finding.
Is Tri-Heal FDA-approved?
No. None of the three components — TB-500, BPC-157, or KPV — is FDA-approved for the tissue-repair or anti-inflammatory uses implied by the blend, and the combination has no regulatory recognition at all. These are research chemicals labeled for laboratory use only, without an established human safety profile from controlled trials.
What is the difference between Tri-Heal and KLOW?
Tri-Heal is a 3-in-1 blend (TB-500, BPC-157, KPV). KLOW is a 4-in-1 blend that adds GHK-Cu, a copper-binding peptide studied preclinically for skin remodeling and antioxidant activity. The two share three components. Importantly, neither blend has any combination-specific research, so the difference is compositional and theoretical rather than a difference backed by outcome data.
What does KPV do in the blend?
KPV is the C-terminal tripeptide (Lysine-Proline-Valine) of α-MSH. In preclinical and in-vitro studies, it has shown anti-inflammatory activity linked to inhibition of the NF-κB pathway, notably in murine models of inflammatory bowel disease. In the blend’s theory, KPV contributes an anti-inflammatory tone. This role is preclinical only; KPV is not an approved anti-inflammatory drug.
How is TB-500 related to thymosin beta-4?
TB-500 is a research-market label for material described as related to thymosin beta-4 (Tβ4), a natural 43-amino-acid actin-sequestering peptide. Much peer-reviewed research studied full-length Tβ4 or its actin-binding domain, while TB-500 is often a fragment. Whether a given TB-500 preparation reproduces the published Tβ4 findings depends on its exact sequence and purity, which vary and are rarely independently verified.
Is there evidence the three peptides work synergistically?
No. There is no published experiment testing whether TB-500, BPC-157 and KPV act additively, synergistically, or antagonistically when combined. Demonstrating synergy would require a study with control, single-agent, and combination arms plus interaction analysis — and no such study exists for Tri-Heal. The “complementary node” rationale is a design hypothesis, not a measured property.
Can Tri-Heal be used to treat an injury or condition?
This article makes no human-use recommendation. The components are unapproved research chemicals with no established human efficacy or safety, and the combination has no data at all. All discussion here is educational and framed for research settings. Questions about any actual health condition should go to a qualified, licensed medical professional, not a research-chemical reference.
Why do sources describe these peptides as “healing” if the evidence is only preclinical?
The “healing” framing comes from animal and cell-culture studies where the individual peptides improved defined endpoints — wound closure, tendon repair, reduced colitis markers. The accurate translation is “improved a specific endpoint in a specific model,” not “heals people.” Most preclinical successes never translate to proven human benefit, which is why the evidence tier must always be stated explicitly.
References
- Goldstein AL, Hannappel E, Kleinman HK. Thymosin β4: actin-sequestering protein moonlights to repair injured tissues. Trends Mol Med. 2005;11(9):421–429.
- Malinda KM, Sidhu GS, Mani H, et al. Thymosin β4 accelerates wound healing. J Invest Dermatol. 1999;113(3):364–368.
- Sosne G, Qiu P, Christopherson PL, Kurpakus-Wheater M. Thymosin beta 4 suppression of corneal NFκB: a potential anti-inflammatory pathway. Exp Eye Res. 2007;84(4):663–669.
- Seiwerth S, Brcic L, Vuletic LB, et al. BPC 157 and blood vessels. Curr Pharm Des. 2014;20(7):1121–1125.
- Chang CH, Tsai WC, Hsu YH, Pang JHS. Pentadecapeptide BPC 157 enhances the growth hormone receptor expression in tendon fibroblasts. Molecules. 2014;19(11):19066–19077.
- Chang CH, Tsai WC, Lin MS, Hsu YH, Pang JHS. The promoting effect of pentadecapeptide BPC 157 on tendon healing involves tendon outgrowth, cell survival, and cell migration. J Appl Physiol. 2011;110(3):774–780.
- Sikiric P, Seiwerth S, Rucman R, et al. Stable gastric pentadecapeptide BPC 157: novel therapy in gastrointestinal tract. Curr Pharm Des. 2011;17(16):1612–1632.
- Brzoska T, Luger TA, Maaser C, Abels C, Böhm M. α-melanocyte-stimulating hormone and related tripeptides: biochemistry, antiinflammatory and protective effects. Endocr Rev. 2008;29(5):581–602.
- Dalmasso G, Charrier-Hisamuddin L, Nguyen HTT, et al. PepT1-mediated tripeptide KPV uptake reduces intestinal inflammation. Gastroenterology. 2008;134(1):166–178.
- Kannengiesser K, Maaser C, Heidemann J, et al. Melanocortin-derived tripeptide KPV has anti-inflammatory potential in murine models of inflammatory bowel disease. Inflamm Bowel Dis. 2008;14(3):324–331.
- Luger TA, Brzoska T. α-MSH related peptides: a new class of anti-inflammatory and immunomodulating drugs. Ann Rheum Dis. 2007;66(Suppl 3):iii52–iii55.
- Pickart L, Margolina A. Regenerative and protective actions of the GHK-Cu peptide in the light of the new gene data. Int J Mol Sci. 2018;19(7):1987.
- Gwyer D, Wragg NM, Wilson SL. Gastric pentadecapeptide body protection compound BPC 157 and its role in accelerating musculoskeletal soft tissue healing. Cell Tissue Res. 2019;377(2):153–159.
- Sikiric P, Seiwerth S, Rucman R, et al. Brain-gut axis and pentadecapeptide BPC 157: theoretical and practical implications. Curr Neuropharmacol. 2016;14(8):857–865.
Research-use-only disclaimer: This article is an educational reference summarizing preclinical and in-vitro literature on individual peptides. TB-500, BPC-157 and KPV are unapproved research chemicals, the Tri-Heal combination has no combination-specific studies of any tier, and none of these materials is FDA-approved for human use. Nothing here is medical advice or a recommendation for human administration. Consult a qualified, licensed healthcare professional regarding any health condition.