The question as posed — what evidence shows TB-500’s effectiveness in tendon and ligament repair after injury — carries a quiet assumption that deserves to be surfaced before we examine a single study. It presumes that TB-500 is an established or at least demonstrated repair agent for tendon and ligament, and that the task ahead is merely to catalog how well it works. That framing gets ahead of the science. TB-500 is a synthetic peptide sold for laboratory and research use; it is not an approved therapeutic for any orthopedic indication, and the evidence that bears most directly on tendon and ligament healing is preclinical — cell culture, rodent surgery, and tissue-engineering scaffolds — not controlled human trials. There are, as of mid-2026, no published randomized controlled trials of TB-500 or its parent peptide in human tendon or ligament injury.
So rather than treat effectiveness as settled and grade it, this article treats the premise itself as the open research question. What, precisely, does the evidence show? The honest answer is a layered one: a genuinely interesting and reasonably well-characterized molecular mechanism; a scattering of positive animal and in-vitro results, some of them directly in ligament and tendon models; and a near-total absence of the human interventional data that would be required to call any of this “effective” in the clinical sense the question implies. Holding those three layers apart — mechanism, preclinical signal, and human proof — is the entire discipline of reading this literature correctly.
This piece is written for researchers, clinicians, and educated readers who want a candid map rather than a marketing brochure. We will work through what TB-500 and thymosin beta-4 actually are, the actin-based mechanism that gives the molecule its regenerative reputation, why tendon and ligament are biologically stubborn tissues to repair, exactly what the preclinical tendon and ligament studies did and did not demonstrate, how the compound is handled in research settings, how it compares with the other repair peptide it is most often mentioned alongside, its safety profile, and its regulatory and anti-doping status. Throughout, the governing rule is restraint: nothing here should be read as a claim that TB-500 treats, cures, or prevents any injury or disease, because no such claim is supported by the current human evidence.
What TB-500 and Thymosin Beta-4 Actually Are
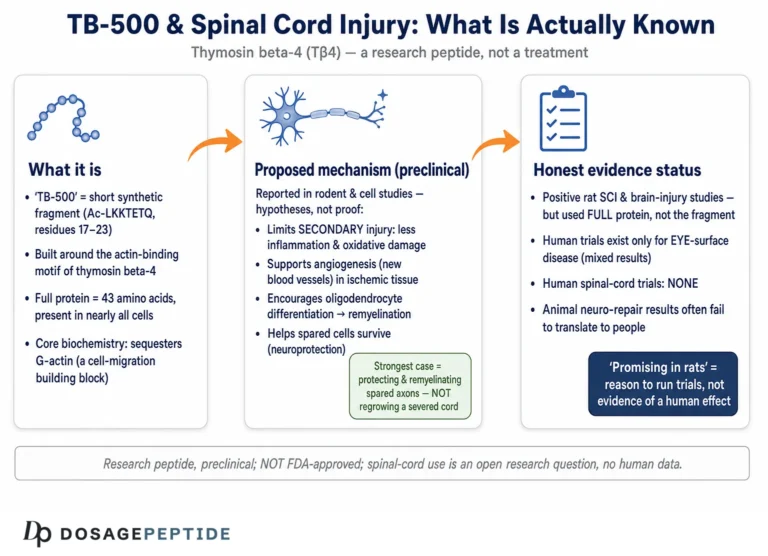
To evaluate TB-500 fairly you first have to be precise about what the label refers to, because the term is used loosely in ways that inflate its evidentiary pedigree. Thymosin beta-4 (Tβ4) is a naturally occurring 43-amino-acid polypeptide found in nearly every cell type in the body, and one of the most abundant intracellular proteins in mammalian tissue. It was first isolated from thymic tissue, which is where its name comes from, but the “thymic hormone” framing is largely historical; the peptide’s dominant biology is that of an intracellular actin-regulating protein present far beyond the thymus.1 Decades of work have characterized Tβ4 as a multifunctional regenerative peptide involved in cell migration, survival, angiogenesis, and the modulation of inflammation and fibrosis.1
TB-500, by contrast, is a commercial designation. It is generally described as a synthetic peptide corresponding to the biologically active region of thymosin beta-4 — frequently the actin-binding domain that contains the seven-residue motif responsible for much of the molecule’s cell-migration and angiogenic activity.3 In practice, material sold as “TB-500” on the research-chemical market is variously represented as either full-length Tβ4 or as a fragment of it, and purity and exact composition are not guaranteed outside regulated manufacturing. This matters more than it may seem: almost the entire peer-reviewed evidence base — the wound-healing studies, the cardiac studies, the ligament study — was generated with characterized thymosin beta-4, not with vials labeled “TB-500.” When a vendor cites a Tβ4 paper to support a claim about TB-500, it is borrowing the credibility of the natural peptide for a product whose identity and quality may differ. A researcher reading this literature should mentally translate “TB-500” back to “thymosin beta-4” and then ask whether the specific product in question is actually the same molecule that was studied.
The distinction between a naturally abundant endogenous peptide and a synthetic research chemical also frames the safety and regulatory discussion later on. Because Tβ4 is ubiquitous and normally present at appreciable concentrations, one intuition is that supplementing it should be innocuous. But endogenous abundance under tight physiological control is not the same as safety when a synthetic analog is injected at supraphysiologic doses from an unregulated source, and the leap from “the body makes this” to “injecting more of it is safe and helpful” is exactly the kind of inference the evidence does not license. For readers building a broader picture of this compound’s biology beyond the musculoskeletal question, the site’s discussion of whether TB-500 is a promising therapy for chronic inflammatory conditions covers the same peptide from the inflammation angle.
The Molecular Mechanism: Actin, Migration, and Angiogenesis
The reason thymosin beta-4 is taken seriously as a regenerative molecule at all comes down to a single, well-established biochemical fact: it is the major intracellular G-actin–sequestering peptide in mammalian cells. Actin exists in two interconvertible forms — monomeric globular actin (G-actin) and polymerized filamentous actin (F-actin) — and the dynamic balance between them drives cell shape, motility, and migration. Tβ4 binds monomeric G-actin in a roughly one-to-one ratio and holds it in a sequestered, unpolymerized pool.1 That buffered reserve of monomer is what allows a cell to rapidly assemble new filaments at the leading edge when it needs to move, which is precisely the demand placed on cells during tissue repair, when fibroblasts, endothelial cells, and progenitor cells must migrate into a wound.
From that core actin-buffering role, several downstream effects have been documented that are directly relevant to healing. First, cell migration: Tβ4 promotes the directed movement of keratinocytes, endothelial cells, and fibroblasts, and a seven-amino-acid actin-binding motif within the peptide has been shown to be essential for this activity. In endothelial migration and vessel-sprouting assays, Tβ4 and the isolated actin-binding motif displayed near-identical activity at nanomolar concentrations, whereas peptides missing any part of that motif were inactive — strong evidence that the actin-binding site is the functional heart of the molecule’s pro-migratory and angiogenic behavior.3 Second, angiogenesis: by promoting endothelial migration and tube formation, Tβ4 supports the formation of new blood vessels in injured and ischemic tissue, a prerequisite for delivering oxygen and nutrients to a healing site.3
Third, and demonstrated most rigorously in the heart, Tβ4 promotes cell survival through a defined signaling pathway. In a landmark 2004 study, Tβ4 was shown to form a complex with PINCH and integrin-linked kinase (ILK), activating the survival kinase Akt; systemic or local Tβ4 enhanced cardiomyocyte survival and migration and improved cardiac function after coronary artery ligation in mice.2 The ILK/Akt survival axis is not tendon-specific, but it illustrates that Tβ4’s effects extend beyond passive actin buffering into active pro-survival signaling — a plausible contributor to preserving cells in a hostile post-injury environment.
Fourth, Tβ4 modulates inflammation and fibrosis. It has been reported to reduce inflammatory cytokine signaling and, in several organ models, to influence the transforming growth factor-beta (TGF-β) pathway that governs scar formation, in some settings limiting excess fibrosis while still supporting matrix organization.11 A related line of work found that Tβ4 can organize connective tissue during repair and reduce the appearance of myofibroblasts, the contractile cells associated with scarring and contracture.9 For tendon and ligament, where the quality and alignment of the collagen matrix largely determine mechanical strength, an agent that improves matrix organization rather than simply adding bulk scar is at least mechanistically attractive.
A fifth thread worth separating from the others is the peptide’s reported influence on progenitor-cell recruitment. Beyond simply enabling migration through actin buffering, Tβ4 has been shown to increase proliferation of mesenchymal stem cells through an interleukin-8–dependent mechanism, with neutralization of IL-8 blunting the effect.7 If the healing of a hypocellular tissue is rate-limited by how many reparative cells can be recruited and expanded at the injury, a signal that both draws cells in and encourages their proliferation is, in principle, addressing two bottlenecks at once. This is again a mechanistic argument — demonstrated in cell systems, not in a healing tendon — but it rounds out why the molecule attracts regenerative interest rather than being dismissed as a mere cytoskeletal housekeeping protein.
Taken together, the mechanistic case is genuine and multi-pronged: buffer actin to enable migration, recruit and keep alive the cells that build new tissue, grow the blood supply, and temper disorganized fibrosis. This is a coherent story for how a molecule could aid connective-tissue repair. But mechanism is a hypothesis generator, not proof of clinical effect — a coherent mechanism explains why a compound might work, not whether it does, at what dose, by what route, or with what magnitude of benefit in an actual injured tendon. The history of regenerative medicine is full of molecules with impeccable mechanistic credentials that nonetheless failed to move hard clinical endpoints, precisely because living tissue is more complicated than the sum of a few validated pathways. That gap between plausible mechanism and demonstrated effectiveness is where most of the honest tension in this topic lives, and it is the reason the sections that follow weigh the actual data rather than resting on the theory.
Why Tendon and Ligament Are Difficult Tissues to Repair
To judge whether any peptide meaningfully helps tendon and ligament healing, it helps to understand why these tissues are so notoriously slow and imperfect to repair in the first place, because the biology sets the bar that a candidate agent must clear.
Tendons and ligaments are dense, highly organized connective tissues built primarily of type I collagen arranged in tightly aligned, hierarchically bundled fibers. That alignment is what gives them tensile strength, and it is exactly what is hardest to reconstruct after injury. Both tissues are relatively hypovascular and hypocellular compared with muscle or skin: they have a sparse blood supply and comparatively few resident cells (tenocytes and ligament fibroblasts). Low vascularity means limited delivery of oxygen, nutrients, and reparative cells; low cellularity means fewer cells available to lay down and remodel matrix. The result is slow healing that, in many cases, produces mechanically inferior scar tissue rather than true regeneration of the original aligned architecture.
The natural repair sequence proceeds through overlapping phases — an initial inflammatory phase, a proliferative phase in which cells migrate in and deposit a disorganized, largely type III collagen matrix, and a prolonged remodeling phase during which that matrix is gradually reorganized and cross-linked toward stronger, more aligned type I collagen. Remodeling can take months and rarely restores full pre-injury strength; healed tendon and ligament frequently retain elevated type III collagen, disordered fiber alignment, and a persistent strength deficit that predisposes to re-injury. Comorbidities make this worse: diabetes, for example, is associated with altered expression of growth and inflammatory mediators during Achilles tendon repair and with compromised healing, illustrating how systemic metabolic state can degrade an already marginal repair process.11
Read against that biology, the mechanistic profile of thymosin beta-4 lines up unusually well with the specific deficits of tendon and ligament healing. The tissues are poorly vascularized — Tβ4 promotes angiogenesis. They are hypocellular and depend on cells migrating in — Tβ4 promotes migration and survival of fibroblasts and progenitor cells. Their functional outcome depends on collagen organization — Tβ4 has been reported to improve matrix organization and limit disorganized fibrosis. This alignment between mechanism and pathology is the strongest a-priori argument for studying the peptide here, and it is why the preclinical work that does exist targeted exactly these endpoints. It is also, however, a reason for caution: a mechanism that fits the theory neatly can create confirmation bias, making weak or preliminary data feel more conclusive than it is. The discipline is to let the actual studies, not the elegance of the rationale, set the confidence level.
What the Preclinical Tendon and Ligament Evidence Actually Shows
Here is the core of the matter. When you strip away the vendor copy and look for controlled experiments in which thymosin beta-4 or TB-500 was administered as an intervention in a tendon or ligament model with objective outcomes, the peer-reviewed literature is real but thin, and it is entirely preclinical.
The single most relevant primary study is Xu and colleagues’ 2013 work on medial collateral ligament (MCL) injury in rats.5 The investigators transected the MCL in rats and placed a fibrin sealant containing 1 microgram of Tβ4 into the ligament gap, comparing healing against control animals that received the sealant alone. At four weeks, the healing tissue was evaluated by histology (hematoxylin and eosin staining), transmission electron microscopy of collagen fibrils, and biomechanical testing of the femur–MCL–tibia complex. The Tβ4-treated group showed significantly better biomechanical properties than controls, and histologically their healing tissue displayed uniform, evenly spaced collagen fiber bundles, whereas control fibers were irregularly spaced. Electron microscopy found that collagen fibril diameters within the granulation tissue were significantly larger in the treated animals.5 This is a genuine, objective, positive result for a ligament-healing endpoint — the kind of data a serious case would be built on. It is also a small, single-timepoint rodent study using a locally delivered microgram dose in fibrin sealant, an experimental design far removed from a human patient injecting reconstituted peptide subcutaneously.
On the tendon side, the most informative work comes from tissue engineering rather than simple injection. Wu and colleagues (2019) fabricated electrospun Tβ4-loaded PLGA/PLA nanofiber/microfiber hybrid yarns designed as scaffolds for tendon tissue engineering.6 The scaffolds released Tβ4 in a sustained fashion over 28 days, and human adipose-derived mesenchymal stem cells cultured on the Tβ4-loaded yarns showed enhanced migration, proliferation, and — importantly — upregulation of tendon-specific genes including scleraxis (SCX), tenascin C (TNC), collagen I and III (COL1A1, COL3A1), and tenomodulin (TNMD) relative to scaffolds without the peptide.6 Tenogenic differentiation — nudging stem cells toward a tendon-cell phenotype and a tendon-like matrix program — is a meaningful in-vitro endpoint. But it is exactly that: an in-vitro, scaffold-delivered result about gene expression and cell behavior in a dish, not evidence that a systemically or locally injected peptide heals a torn tendon in a living animal, let alone a person.
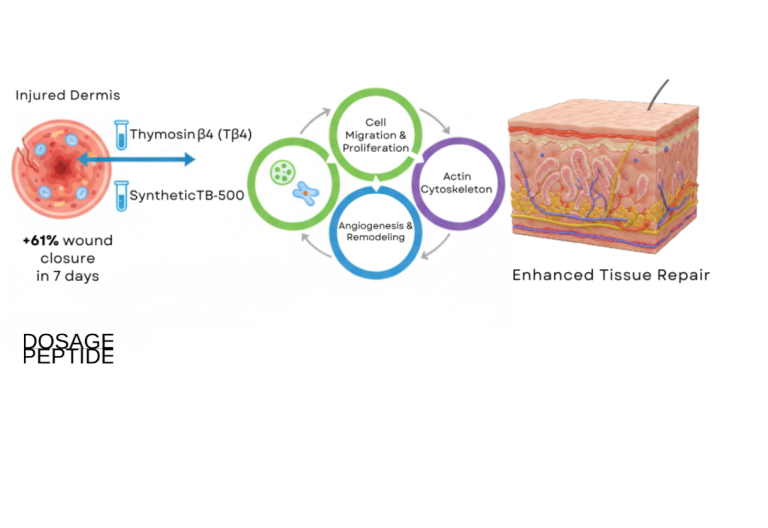
Supporting these tissue-specific findings is a broader body of Tβ4 regenerative biology that is relevant by extension but not tendon-specific. The peptide accelerates dermal wound healing in rodents, increasing reepithelialization and collagen deposition and stimulating keratinocyte migration.4 It promotes proliferation of mesenchymal stem cells through an interleukin-8–dependent mechanism, a pathway plausibly relevant to recruiting reparative cells.7 Reviews of animal studies catalog Tβ4 activity across skin, cornea, heart, and other tissues.8 And a 2026 scoping review specifically surveying thymosin beta-4 and TB-500 in tissue healing and musculoskeletal repair concluded that the musculoskeletal evidence, while promising and mechanistically coherent, is dominated by heterogeneous preclinical models and that the clearest gap is the absence of direct human interventional studies.10
It is also worth being explicit about what these preclinical models can and cannot tell us, because the design details carry the interpretation. Rodent ligament and tendon models heal faster and often more completely than human tissue, use young healthy animals without the comorbidities that degrade real-world healing, and employ delivery routes — local sealant, engineered scaffold — that concentrate a known dose exactly where it is needed. A positive four-week biomechanical result in a rat MCL is genuinely meaningful as proof of biological activity, but the leap from that to “a human injecting reconstituted peptide subcutaneously will heal a chronic Achilles tendinopathy faster” crosses differences in species, tissue, dose, delivery, timing, and patient health all at once. Each of those is a place where an effect can shrink, vanish, or reverse. This is not a reason to ignore the preclinical data; it is the reason preclinical data are treated as hypothesis-supporting rather than practice-changing until human trials are done.
The honest synthesis is therefore threefold.
There is at least one objective positive ligament study and one informative tenogenic tissue-engineering study, which is more direct tendon/ligament data than exists for many marketed “repair” peptides. There is a large, credible surrounding literature on Tβ4 as a pro-migratory, pro-angiogenic, matrix-organizing regenerative peptide. And there is no human tendon or ligament trial of any kind. Effectiveness, in the sense the title’s premise implies, has not been demonstrated in people. For context on how a related repair peptide has been examined specifically for tendon problems, the site’s analysis of whether scientific evidence supports BPC-157 as a long-term tendonitis therapy walks through the same evidentiary distinctions for a different molecule.
| Study / model | Design & delivery | Key finding | Evidence level |
|---|---|---|---|
| Xu et al. 2013 — rat MCL transection5 | 1 µg Tβ4 in fibrin sealant, local, 4-week endpoint | Improved biomechanics; more uniform, larger-diameter collagen fibrils | Preclinical, in vivo (rodent), single timepoint |
| Wu et al. 2019 — tendon scaffold6 | Tβ4-loaded electrospun yarns, 28-day release, human stem cells | Enhanced migration/proliferation; upregulated SCX, TNC, COL1A1, COL3A1, TNMD | Preclinical, in vitro (cell + scaffold) |
| Malinda et al. 1999 — dermal wound4 | Topical/IP Tβ4, rat full-thickness wounds | +42–61% reepithelialization; increased collagen & angiogenesis | Preclinical, in vivo (rodent); skin, not tendon |
| Bock-Marquette et al. 2004 — cardiac2 | Tβ4, mouse coronary ligation | ILK/Akt-mediated cell survival & migration; improved function | Preclinical, in vivo (rodent); heart, not tendon |
| Human tendon/ligament RCTs | — | None published | Absent |
The Human-Evidence Gap
This section is deliberately blunt, because the gap between preclinical promise and human proof is the crux of the entire question and the point most often obscured in popular writing.
There are no published randomized controlled trials — and, as far as the indexed literature reveals, no controlled human interventional studies of any design — testing TB-500 or thymosin beta-4 for the repair of tendon or ligament injury. The human clinical experience with thymosin beta-4 that does exist lies in other domains entirely: dermal wound healing and, notably, ophthalmology, where Tβ4-based formulations have been evaluated in clinical trials for corneal and ocular surface repair such as dry eye and neurotrophic keratopathy. Those programs are genuine clinical research, but they concern the eye and skin, use defined pharmaceutical-grade preparations, and tell us nothing about whether injected TB-500 heals a partially torn Achilles tendon or a sprained knee ligament.
What flows from this absence is important to state precisely. First, there is no established effective human dose, route, frequency, or duration for tendon or ligament repair, because the trials that would define those parameters have not been run. Any “protocol” circulating for such use is extrapolated from animal studies, vendor convention, and anecdote, not from clinical evidence. Second, there is no human efficacy magnitude to cite — no percentage improvement in healing, re-rupture rate, return-to-activity time, or strength recovery attributable to the peptide, because no controlled human study has measured them. Third, there is no long-term human safety data specific to this use.
It is worth being equally clear about what this absence does not mean. It does not mean TB-500 has been tested and failed in human tendon repair; it means it has not been properly tested at all. Absence of evidence is not evidence of absence of effect. The mechanistic rationale and the rodent ligament data make it a legitimately interesting research candidate. But “interesting research candidate” and “effective therapy” are separated by exactly the body of human trials that does not yet exist, and no amount of mechanism or animal work can substitute for it. The correct scientific posture is neither dismissal nor endorsement but calibrated agnosticism: a promising hypothesis awaiting the clinical test that would confirm or refute it.
Dosing and Delivery in a Research Context
Because the practical question “how is TB-500 used in studies?” inevitably arises, a brief and strictly educational description of the research context is warranted — with the emphatic caveat that none of this constitutes a validated human dosing regimen, and that no dose has been shown effective for tendon or ligament repair in people.
The published tendon and ligament work used delivery methods quite unlike the way the compound is used informally. Xu’s ligament study delivered 1 microgram of Tβ4 locally, embedded in fibrin sealant placed directly in the ligament gap.5 The tendon tissue-engineering work delivered Tβ4 from an implanted scaffold engineered for sustained 28-day release.6 Cardiac and wound studies used intraperitoneal, intravenous, intramuscular, or topical routes at doses scaled to rodents.24 Each of these is a controlled experimental delivery, chosen to place a known quantity of characterized peptide at a defined site, and none maps cleanly onto subcutaneous self-injection of reconstituted research-chemical powder.
The doses quoted in non-clinical, informal use — typically expressed in milligrams per week with an initial “loading” period followed by less frequent maintenance — derive from vendor convention and community practice rather than from any clinical trial or pharmacokinetic study establishing an effective and safe human regimen. The absence of validated pharmacokinetic data in humans means the relationship between an injected dose and tissue exposure at an injured tendon is genuinely unknown. Reconstitution arithmetic — dissolving a fixed mass of lyophilized peptide in a chosen volume of diluent to set a concentration — is the same for any peptide and is covered in general terms in the peptide reconstitution guide, but knowing how to calculate a concentration says nothing about whether that concentration does anything useful or is safe. The gap here is not one of arithmetic; it is one of missing clinical evidence, and no dosing table can close it.
How TB-500 Compares With Other Repair Approaches
TB-500 is rarely discussed in isolation. In the recovery and research-peptide conversation it is almost always paired with BPC-157, and it competes conceptually with established, evidence-based orthopedic interventions. Placing it alongside these clarifies where it actually stands.
BPC-157, a synthetic peptide derived from a gastric protein, is the compound most often stacked with or compared to TB-500 for connective-tissue repair. Its preclinical tendon-and-ligament literature is arguably somewhat larger than TB-500’s, with multiple rodent studies reporting accelerated tendon-to-bone and ligament healing, but it shares TB-500’s central limitation exactly: the evidence is overwhelmingly animal, and rigorous human tendon trials are lacking. The two peptides are frequently marketed as complementary — TB-500 for systemic migration and angiogenesis, BPC-157 for local angiogenic and tendon-fibroblast effects — but the “synergy” framing is a hypothesis, not a demonstrated clinical fact, and no controlled human study has tested the combination for tendon or ligament repair. Readers weighing the two can consult the site’s overview of what BPC-157 is and how the healing-peptide claims are supported and its examination of whether BPC-157 is the missing link in treating inflammation and joint pain, both of which apply the same evidence-grading discipline used here.
Against this stand the interventions that actually have human evidence for tendon and ligament injury. Structured rehabilitation and progressive loading — eccentric and heavy slow-resistance exercise for tendinopathy — is the best-supported, guideline-endorsed approach, with randomized human trials behind it. Surgical repair is established for complete ruptures and unstable ligament tears. Injectable options such as corticosteroids offer short-term symptom relief (with known downsides for tendon integrity), while biologic injections like platelet-rich plasma have been extensively studied in humans with genuinely mixed results. The instructive point is not that these are perfect — tendinopathy remains hard to treat and even well-studied biologics disappoint — but that they have all been put through human trials. TB-500 has not. A candidate with an appealing mechanism and rodent ligament data occupies a different evidentiary tier than an intervention that has, for better or worse, faced controlled human testing.
| Approach | Primary rationale for tendon/ligament | Human evidence for tendon/ligament repair |
|---|---|---|
| Progressive loading / eccentric rehab | Mechanotransduction drives collagen remodeling & alignment | Multiple RCTs; guideline first-line for tendinopathy |
| Surgical repair | Restores continuity in complete ruptures/unstable tears | Established standard of care where indicated |
| Platelet-rich plasma (PRP) | Concentrated growth factors delivered locally | Extensively studied in humans; mixed/inconsistent results |
| BPC-157 | Angiogenesis, tendon-fibroblast effects (preclinical) | Preclinical only; no rigorous human tendon RCTs |
| TB-500 / thymosin beta-4 | Actin-driven migration, angiogenesis, matrix organization | Preclinical only; no human tendon/ligament trials |
Nothing in this comparison rules TB-500 out; the migration-and-angiogenesis mechanism is legitimately well matched to the deficits of connective-tissue healing, as discussed earlier. It simply locates the compound accurately: a mechanistically promising, preclinically supported research candidate sitting one full tier of evidence below the interventions that have actually been tested in patients. Researchers cataloging where it fits among related compounds can browse the broader dosage and compound index, which is organized for educational reference rather than as clinical guidance.
Safety and Tolerability
Discussion of TB-500 safety must begin by distinguishing what has been characterized from what has merely been assumed. Thymosin beta-4 is an endogenous, ubiquitously expressed peptide, and in the animal and early human studies conducted with defined, pharmaceutical-grade Tβ4 — predominantly in wound-healing and ophthalmic contexts — it has generally been reported to be well tolerated over the durations studied, without prominent acute toxicity. That is a reasonable statement about characterized Tβ4 in controlled settings. It is not a clean bill of health for injected research-chemical “TB-500” used long-term for orthopedic purposes, and several caveats separate the two.
- Population and indication mismatch. Human safety experience with Tβ4 comes largely from topical ocular and dermal use and short study durations. It does not characterize the safety of repeated subcutaneous injection over months for tendon repair, which is how the compound is used informally.
- Product quality and provenance. Material sold as TB-500 is a research chemical of variable and often unverified purity. Impurities, incorrect peptide content, endotoxin contamination, and mislabeling are real, documented risks of the unregulated peptide market that have nothing to do with the intrinsic properties of the molecule and everything to do with sourcing. Non-sterile or contaminated injectables carry infection and immunogenicity risks independent of any peptide effect.
- The angiogenesis double edge. Pro-angiogenic and pro-migratory activity is helpful for healing but is theoretically a concern in the context of malignancy or proliferative disease, since tumors also depend on angiogenesis and cell migration. This is a mechanistic caution, not a demonstrated cancer risk in humans, but it is a reason that indiscriminate long-term self-administration is not obviously benign.
- Absent long-term data. There is no long-term human safety dataset for TB-500 used for musculoskeletal repair. Rare or delayed adverse effects would not have been captured by the short studies that exist.
- Anti-doping and regulatory hazard. For any athlete, use carries a near-certain sanction risk that is a serious practical harm regardless of pharmacology, discussed below.
The measured conclusion is that characterized thymosin beta-4 has not thrown up major short-term toxicity signals in the limited, mostly non-orthopedic settings studied, and its endogenous nature is mildly reassuring — but that this provides no assurance about long-term injection of unregulated product for an unproven use. Absence of demonstrated harm and absence of demonstrated benefit coexist here, and neither should be mistaken for its opposite.
Handling and Reconstitution in a Laboratory Setting
Because TB-500 is typically supplied as a lyophilized (freeze-dried) powder in a sealed vial, a brief educational note on standard research-peptide handling is appropriate — framed explicitly as laboratory practice, not a usage recommendation, and with the reminder that meticulous handling does nothing to change the compound’s unproven status for tendon or ligament repair.
Lyophilized peptides are generally reconstituted with sterile or bacteriostatic water. The diluent is directed slowly down the inside wall of the vial rather than sprayed onto the powder, and the vial is gently swirled rather than shaken, because vigorous agitation can shear peptide bonds and denature the material and foaming can cause loss. The volume of diluent chosen simply sets the concentration: a fixed mass of peptide in a larger volume yields a lower concentration per unit volume, the arithmetic behind any reconstitution chart. General handling parameters that recur across the peptide literature are summarized below and treated in more depth in the site’s peptide research glossary.
| Parameter | Typical research-context practice |
|---|---|
| Lyophilized storage | Cool, dark; long-term stability favored by freezing |
| After reconstitution | Refrigerated; used within a limited window |
| Diluent | Sterile or bacteriostatic water; aseptic technique |
| Light & heat | Minimize exposure; both degrade peptides |
| Agitation | Swirl gently; avoid shaking and foaming |
| Freeze-thaw | Repeated cycles degrade peptides; avoid |
It bears emphasizing that good technique preserves whatever biological activity the molecule has; it does not create clinical efficacy where none has been demonstrated. A perfectly reconstituted, high-purity vial of TB-500 is still a compound with no human tendon or ligament trial behind it.
Regulatory and Anti-Doping Status
The regulatory picture is unambiguous and frequently misrepresented, so precision matters.
No therapeutic approval. TB-500 is not approved by the U.S. Food and Drug Administration, the European Medicines Agency, or any comparable major regulator as a drug for tendon repair, ligament repair, or any other indication. It is sold and labeled for laboratory and research use only, a designation that expressly means it is not intended for human diagnostic or therapeutic use and has not been evaluated for safety or efficacy as a medicine. Thymosin beta-4–based pharmaceuticals have been investigated in formal clinical trials for specific indications such as ocular surface and dermal wounds, but those investigational programs do not confer approval on research-chemical TB-500 for musculoskeletal use.
Compounding and supplement status. In the United States, peptide products in this general class have faced regulatory caution, and TB-500/thymosin beta-4 is not an established, sanctioned compounded medication for orthopedic use. It is likewise not a lawful dietary supplement ingredient. Marketing that presents it as a legitimate “healing” product for consumer use is operating ahead of, and frequently against, the regulatory reality.
Prohibited in sport. This is the sharpest and most consequential point for many readers. Thymosin beta-4 and its derivatives, explicitly including TB-500, are prohibited by the World Anti-Doping Agency at all times — both in and out of competition — under section S2 of the Prohibited List, which covers peptide hormones, growth factors, related substances, and mimetics.12 The relevant subsection addresses substances affecting muscle, tendon, or ligament protein synthesis and regeneration — language that directly captures the very repair effects TB-500 is marketed for. WADA-accredited laboratories can detect the substance by liquid chromatography–tandem mass spectrometry, and an adverse finding carries substantial sanctions.12 For any athlete subject to anti-doping testing, use should be assumed to constitute an anti-doping rule violation regardless of intent, and this regulatory hazard is a concrete, near-certain harm that exists entirely apart from the unresolved question of whether the peptide even works.
The regulatory synthesis is straightforward: TB-500 is an unapproved research chemical, not a medicine; it has no sanctioned therapeutic use for tendon or ligament injury; and it is banned in sport. Any legitimate exploration of its repair potential belongs in properly authorized preclinical and clinical research under regulatory oversight, not in off-label or informal use. The same peptide’s investigational profile in other repair contexts, such as the exploratory work on whether TB-500 can support regeneration in spinal cord injuries, is similarly preclinical and similarly unapproved.
Reading the Evidence Honestly: A Synthesis
Pulling the threads together, the answer to the title’s question — what evidence shows TB-500 effectiveness in tendon and ligament repair post-injury — is best given in layers, because collapsing them is exactly how the topic gets distorted.
At the level of mechanism, the evidence is solid and specific. Thymosin beta-4 is the principal cellular G-actin sequestrant; it promotes cell migration through a defined actin-binding motif, drives angiogenesis, supports cell survival via ILK/Akt signaling, and modulates fibrosis and matrix organization.1239 These mechanisms map unusually well onto the specific deficits of hypovascular, hypocellular, alignment-dependent connective tissue. This is a legitimately strong mechanistic case.
At the level of preclinical data, the evidence is real but limited and non-clinical. A rat MCL study showed objective biomechanical and collagen-organization improvements with local Tβ4;5 a tendon tissue-engineering study showed Tβ4-driven tenogenic differentiation of stem cells;6 and a large surrounding literature documents Tβ4-mediated wound healing, angiogenesis, and stem-cell proliferation.47810 This is enough to justify continued research; it is not enough to establish clinical effectiveness.
At the level of human proof, the evidence is absent. There are no randomized controlled trials, and no controlled human interventional studies of any design, testing TB-500 or thymosin beta-4 for tendon or ligament repair. There is no validated human dose, no measured human efficacy, and no long-term human safety dataset for this use. Effectiveness in the clinical sense the question presumes has not been demonstrated.
The responsible conclusion, then, is neither the enthusiastic “proven healing peptide” of marketing copy nor a reflexive dismissal. It is that TB-500 is a mechanistically compelling, preclinically supported, but clinically unproven research candidate for connective-tissue repair — a good hypothesis awaiting the human trials that alone could confirm it, and one that is meanwhile unapproved as a therapy and banned in sport. Anyone who tells you the evidence shows TB-500 “works” for tendon and ligament repair in humans is describing a study that has not been done.
Frequently Asked Questions
Is TB-500 proven to repair tendons and ligaments in humans?
No. There are no published randomized controlled trials, and no controlled human interventional studies of any kind, testing TB-500 or thymosin beta-4 for tendon or ligament repair. The supportive evidence is preclinical — cell culture and rodent surgery — including a rat medial collateral ligament study5 and a tendon tissue-engineering scaffold study.6 These are genuinely encouraging results, but they do not establish effectiveness in people, and no validated human dose or efficacy figure exists.
What is the difference between TB-500 and thymosin beta-4?
Thymosin beta-4 is a natural 43-amino-acid peptide found in nearly all cells and is the molecule studied in the peer-reviewed literature.1 TB-500 is a commercial research-chemical designation typically described as a synthetic version or an active fragment of thymosin beta-4. The distinction matters because most cited studies used characterized thymosin beta-4, whereas material sold as “TB-500” is of variable and often unverified composition and purity.
How is TB-500 thought to help healing at the molecular level?
Its best-characterized action is sequestering monomeric G-actin, buffering the actin pool that cells use to migrate and remodel.1 Through a seven-residue actin-binding motif it promotes cell migration and angiogenesis,3 supports cell survival via integrin-linked kinase and Akt signaling,2 and can improve collagen organization while limiting disorganized fibrosis.9 These mechanisms fit the deficits of tendon and ligament healing well, which is why the compound is studied — but mechanism is not the same as demonstrated clinical benefit.
What did the rat ligament study actually find?
Xu and colleagues transected the medial collateral ligament in rats and placed 1 microgram of thymosin beta-4 in fibrin sealant into the gap. At four weeks, treated ligaments had significantly better biomechanical properties and more uniform, larger-diameter collagen fibrils than controls.5 It is an objective positive result, but it is a small, single-timepoint rodent study using local microgram delivery — not evidence about subcutaneous use in humans.
Is TB-500 legal, and is it banned in sports?
TB-500 is not an approved medicine anywhere and is sold for research use only. It is explicitly prohibited by the World Anti-Doping Agency at all times, in and out of competition, under section S2 covering peptide hormones and growth factors.12 Any athlete subject to testing should assume use is an anti-doping rule violation carrying substantial sanctions.
Is TB-500 safe?
Characterized thymosin beta-4 has generally been reported as well tolerated in the short-term, mostly ophthalmic and dermal studies conducted with pharmaceutical-grade peptide, and it is an endogenous molecule. But there is no long-term human safety data for injected TB-500 used for tendon or ligament repair, research-chemical product quality is unregulated and variable, and the pro-angiogenic mechanism is a theoretical concern in the setting of malignancy. Absence of demonstrated harm is not proof of safety for this unapproved use.
How does TB-500 compare with BPC-157 for tendon repair?
Both are research peptides marketed for connective-tissue repair, and both share the same core limitation: the evidence is overwhelmingly preclinical, with no rigorous human tendon trials. BPC-157 has a somewhat larger rodent tendon-and-ligament literature, and the two are often combined in informal practice, but any synergy is hypothetical rather than clinically demonstrated. Neither has established human effectiveness for tendon or ligament repair.
What is the best-supported way to heal a tendon or ligament injury?
For tendinopathy, progressive loading and eccentric or heavy slow-resistance rehabilitation is the most robustly evidenced, guideline-endorsed approach in humans, and complete ruptures or unstable tears may require surgical repair. These have human trial support that TB-500 lacks. Anyone with an actual injury should work with a qualified clinician rather than substitute an unproven, unapproved research chemical for evidence-based care.
References
- Goldstein AL, Hannappel E, Sosne G, Kleinman HK. Thymosin β4: a multi-functional regenerative peptide. Basic properties and clinical applications. Expert Opin Biol Ther. 2012;12(1):37-51. PMID: 22074294. https://pubmed.ncbi.nlm.nih.gov/22074294/
- Bock-Marquette I, Saxena A, White MD, Dimaio JM, Srivastava D. Thymosin beta4 activates integrin-linked kinase and promotes cardiac cell migration, survival and cardiac repair. Nature. 2004;432(7016):466-472. PMID: 15565145. https://pubmed.ncbi.nlm.nih.gov/15565145/
- Philp D, Huff T, Gho YS, Hannappel E, Kleinman HK. The actin binding site on thymosin beta4 promotes angiogenesis. FASEB J. 2003;17(14):2103-2105. PMID: 14500546. https://pubmed.ncbi.nlm.nih.gov/14500546/
- Malinda KM, Sidhu GS, Mani H, et al. Thymosin beta4 accelerates wound healing. J Invest Dermatol. 1999;113(3):364-368. PMID: 10469335. https://pubmed.ncbi.nlm.nih.gov/10469335/
- Xu B, Yang M, Li Z, et al. Thymosin β4 enhances the healing of medial collateral ligament injury in rat. Regul Pept. 2013;184:1-5. PMID: 23523891. https://pubmed.ncbi.nlm.nih.gov/23523891/
- Wu S, Zhou R, Zhou F, Streubel PN, Chen S, Duan B. Electrospun thymosin beta-4 loaded PLGA/PLA nanofiber/microfiber hybrid yarns for tendon tissue engineering application. Mater Sci Eng C Mater Biol Appl. 2019;106:110268. PMID: 31753373. https://pubmed.ncbi.nlm.nih.gov/31753373/
- Jeon BJ, Yang Y, Shim SK, Yang HM, Cho D, Bang SI. Thymosin beta-4 promotes mesenchymal stem cell proliferation via an interleukin-8-dependent mechanism. Exp Cell Res. 2013;319(16):2526-2534. doi:10.1016/j.yexcr.2013.04.014. https://pubmed.ncbi.nlm.nih.gov/23608463/
- Philp D, Kleinman HK. Animal studies with thymosin beta, a multifunctional tissue repair and regeneration peptide. Ann N Y Acad Sci. 2010;1194:81-86. PMID: 20536453. https://pubmed.ncbi.nlm.nih.gov/20536453/
- Ehrlich HP, Hazard SW 3rd. Thymosin beta4 enhances repair by organizing connective tissue and preventing the appearance of myofibroblasts. Ann N Y Acad Sci. 2010;1194:118-124. PMID: 20536458. https://pubmed.ncbi.nlm.nih.gov/20536458/
- Thymosin beta-4 and TB-500 in tissue healing, regeneration, and musculoskeletal repair: a scoping review. Appl Sci. 2026;16(12):6202. https://www.mdpi.com/2076-3417/16/12/6202
- Ahmed AS, Schizas N, Li J, et al. Expressional changes in growth and inflammatory mediators during Achilles tendon repair in diabetic rats: new insights into a possible basis for compromised healing. Cell Tissue Res. 2014;357(1):109-117. PMID: 24816987. https://pubmed.ncbi.nlm.nih.gov/24816987/
- World Anti-Doping Agency. The Prohibited List (Section S2: Peptide Hormones, Growth Factors, Related Substances and Mimetics; thymosin-β4 and its derivatives, e.g., TB-500). https://www.wada-ama.org/en/prohibited-list
Educational and research-use disclaimer: This article is provided solely for scientific and educational purposes. TB-500 (thymosin beta-4 fragment) is a research chemical that is not approved by the FDA, EMA, or any comparable regulator for the treatment, cure, or prevention of tendon injury, ligament injury, or any other condition, and its effectiveness for tendon or ligament repair has not been demonstrated in controlled human trials. The supportive evidence discussed here is preclinical (cell-culture and animal) only. Nothing in this article is medical advice or a recommendation for human use. TB-500 is prohibited in sport by the World Anti-Doping Agency. Any legitimate investigation of this compound should occur within properly authorized preclinical or clinical research under appropriate oversight. Individuals with an injury should consult a qualified healthcare professional and rely on evidence-based care.