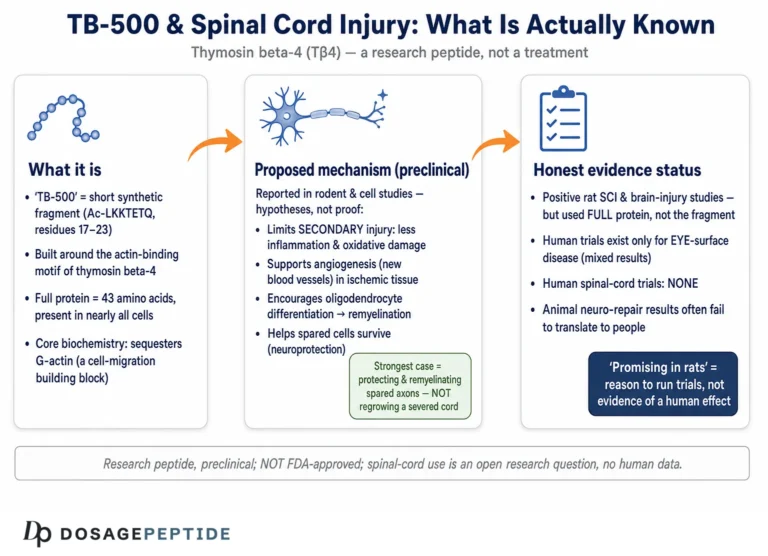
Spinal cord injury (SCI) sits among the most intractable problems in regenerative biology: the mammalian central nervous system (CNS) heals poorly, damaged axons rarely regrow across a lesion, and the fibrotic-glial scar that forms in the days after trauma becomes a lasting barrier to reconnection. Against this backdrop, a small actin-binding peptide — thymosin beta-4 (Tβ4), the parent molecule of the research compound sold as TB-500 — has attracted sustained scientific attention because it touches nearly every biological process that goes wrong after a cord is injured. This article examines the central research question honestly: what does the actual evidence show about Tβ4/TB-500 and spinal cord regeneration, and how far is it from anything resembling a human therapy? The short answer, stated up front so nothing that follows is misread: the promising findings are almost entirely preclinical — rodent SCI models, stroke and traumatic-brain-injury models, and in-vitro cell work — and there are no human clinical trials for spinal cord injury.
What makes the story worth telling in depth is that the preclinical mechanistic case is unusually coherent. Tβ4 is not a vaguely “regenerative” peptide; it has a defined molecular function (sequestering monomeric actin) that plausibly links to cell migration, angiogenesis, oligodendrocyte biology, and inflammation control — the exact levers a damaged spinal cord needs. Below we separate that mechanistic plausibility from demonstrated efficacy, keep the evidence level explicit throughout, and place the compound in its correct regulatory reality: TB-500 is not approved for human therapeutic use, is investigational only, and is prohibited in sport under the WADA code.
What makes spinal cord injuries so difficult to heal?
To understand why researchers are interested in a peptide with Tβ4’s profile, it helps to be precise about why the spinal cord fails to recover on its own. Unlike the peripheral nervous system, the adult CNS mounts a repair response that is actively hostile to regeneration. The failure is not one problem but a cascade of interacting ones.
Primary and secondary injury
The initial mechanical trauma — the “primary injury” — kills neurons, oligodendrocytes and vascular cells outright and disrupts axon tracts. What follows is arguably more damaging: a secondary injury phase unfolding over hours to weeks, driven by ischemia, glutamate excitotoxicity, oxidative stress, mitochondrial failure, and a wave of inflammation. This secondary cascade expands the lesion well beyond the original impact zone and is precisely the window in which pharmacological intervention is theoretically most useful.[2]
The glial scar and inhibitory environment
Reactive astrocytes proliferate around the lesion and, together with infiltrating fibroblasts and extracellular matrix, form a glial-fibrotic scar. This scar has a dual character — it seals off the damaged region and limits the spread of inflammation, but it also erects a physical and biochemical wall (chondroitin sulfate proteoglycans, myelin-associated inhibitors) that regenerating axons struggle to cross. A central lesion cavity often forms, further interrupting continuity of the tract.
Demyelination and limited intrinsic regrowth
Even axons that survive can lose their myelin sheath when oligodendrocytes die, and demyelinated axons conduct poorly or not at all. Compounding this, adult CNS neurons have weak intrinsic growth programs. The practical consequence is that meaningful recovery requires a multi-pronged biology — protecting surviving cells, calming inflammation, restoring blood supply, replacing lost oligodendrocytes, and remodeling the scar — rather than any single silver bullet.
- Neuronal and oligodendrocyte death produces irreversible functional loss and demyelination.
- Inflammation and glial scarring create a chemically inhibitory barrier to axon regrowth.
- Vascular disruption and ischemia starve the peri-lesional tissue of oxygen and nutrients.
- Weak intrinsic regeneration means the cord cannot rebuild lost circuitry on its own.
It is this multifactorial pathology that makes a pleiotropic agent conceptually attractive. A molecule that simultaneously nudges several of these processes in a favorable direction is, at least on paper, better matched to SCI than a narrowly targeted drug. Whether Tβ4 actually delivers on that promise is an empirical question addressed in the sections below.
What is TB-500, and how does it relate to thymosin beta-4?
Clear terminology matters here, because “TB-500” and “thymosin beta-4” are used loosely — and sometimes interchangeably — across the research-chemical marketplace, which muddies interpretation of the science.
Thymosin beta-4: the natural molecule
Thymosin beta-4 is a naturally occurring 43-amino-acid peptide found in virtually every nucleated mammalian cell and present at high concentrations in platelets and wound fluid. It is the most abundant member of the beta-thymosin family and is encoded by the TMSB4X gene. Its best-characterized biochemical job is to bind monomeric G-actin in a 1:1 complex, acting as the principal intracellular actin-sequestering protein and thereby regulating the pool of actin available for filament assembly.[7] That single function underlies its influence over cell shape, motility and directed migration.
The molecule is small and intrinsically unstructured in solution, folding into a more ordered conformation only upon binding actin. Its N-terminus is acetylated, and within the 43-residue chain sits the feature that defines the entire beta-thymosin family: a conserved central actin-binding motif. This motif is usually given as the hexapeptide LKKTET beginning at residue 17, or as the closely related heptapeptide LKKTETQ (residues 17–23); it is strongly conserved across beta-thymosins and is the segment through which Tβ4 makes its principal contact with G-actin.[11] Mutational mapping has shown that altering this motif disrupts actin binding, which is why it is treated as the functional core of the peptide rather than an incidental sequence.
Crucially for the CNS story, the same actin-binding region also carries Tβ4’s angiogenic activity. Philp and colleagues demonstrated that the seven–amino-acid actin-binding motif is essential for promoting endothelial cell migration, adhesion, tubule formation and blood-vessel sprouting — a synthetic peptide corresponding to that motif reproduced angiogenic activity, while disrupting it abolished the effect.[12] That a single short motif couples actin regulation to new vessel formation is central to why researchers regard Tβ4 as mechanistically pleiotropic rather than accidentally multifunctional: several of its downstream repair-relevant behaviors trace back to one structural element.
TB-500: the synthetic research compound
“TB-500” is a name used in the research-peptide market for a synthetic product. In practice it refers either to full-length synthetic Tβ4 or, in some descriptions, to a short fragment built around the actin-binding motif (the acetylated peptide corresponding to residues 17–23, i.e. the LKKTETQ region discussed above) that reproduces part of Tβ4’s activity. The distinction is not pedantic. A 43-residue protein and a 7-residue fragment are different molecules with potentially different stability, tissue distribution, receptor interactions and biological breadth — the fragment may capture the actin-binding/angiogenic axis while lacking whatever the rest of the sequence contributes. This ambiguity is therefore a genuine methodological caveat: virtually all of the rigorous published CNS and SCI research has used defined, full-length recombinant or synthetic Tβ4, not a loosely specified “TB-500” product, and it is often impossible to know from a product label alone which entity a given “TB-500” vial contains. When this article discusses experimental findings, the tested substance is thymosin beta-4 unless stated otherwise; readers should not assume an unspecified TB-500 product is chemically identical to the peptide used in the cited studies, nor that fragment-level data and full-length data are interchangeable.
Why an endogenous wound peptide is interesting for the CNS
One reason Tβ4 attracts regenerative interest is that it is not a foreign drug forcing an unnatural response — it is an endogenous molecule the body already deploys at sites of injury. Tβ4 is stored in high concentration in platelets and released into wound fluid, where it participates in the ordinary tissue-repair program: recruiting cells into the wound bed, supporting new blood vessel formation, and modulating the inflammatory phase of healing. This biology is well established in soft-tissue and dermal wound-healing research and is the conceptual bridge to the CNS: spinal cord injury is, in part, a wound-healing problem in a tissue that happens to heal badly. The hypothesis animating the field is that supplying additional Tβ4 might push the CNS injury response a little further toward the constructive, pro-repair phenotype seen in peripheral wounds. That framing is plausible and productive as a research direction — but it is a hypothesis about mechanism, and, as emphasized throughout, it has not been validated as a human spinal cord therapy.
For readers new to the vocabulary — G-actin, angiogenesis, oligodendrocyte, glial scar — the peptide research glossary defines these terms in plain language and is a useful companion to the mechanistic sections below.
How could thymosin beta-4 influence spinal cord regeneration? (The molecular mechanism)
The mechanistic rationale for studying Tβ4 in SCI rests on a handful of interlocking activities, each documented in the broader cell-biology and CNS-injury literature. The through-line is that a single actin-regulating peptide can plausibly act on several of the failure modes catalogued above. The logic is worth stating explicitly: because actin dynamics sit upstream of cell migration, and migration underlies angiogenesis, immune-cell trafficking, progenitor recruitment and process outgrowth, a peptide that tunes the actin monomer pool has a mechanistic route to influence many downstream repair events at once. This is why Tβ4 is best understood as pleiotropic — a network of related actions rather than one dominant mechanism.
Actin sequestration and cell migration
By binding G-actin and buffering the monomer pool, Tβ4 modulates cytoskeletal dynamics — the machinery cells use to change shape, extend processes, and migrate.[7] In the context of injury, mobilizing reparative cells (endothelial cells, progenitors, immune cells resolving inflammation) toward the lesion is a plausible upstream lever. Directed cell migration is also the cellular basis of the neurite and axonal outgrowth that neurorestorative strategies aim to promote.
Angiogenesis and revascularization
Tβ4 is angiogenic. A defined seven–amino-acid actin-binding motif is essential for this activity, and Tβ4 promotes endothelial cell migration, adhesion, tubule formation and vessel sprouting.[7] Because peri-lesional ischemia is a major driver of secondary injury, an agent that supports revascularization could improve the survival of tissue at the injury margins. In CNS-injury models, Tβ4-associated increases in vascular density accompany functional improvement.[5]
Anti-inflammatory and anti-oxidative effects
In injury models, Tβ4 dampens the pro-inflammatory response. In a compression SCI model it reduced pro-inflammatory cytokine expression, raised anti-inflammatory interleukin-10 (IL-10) messenger RNA, and lowered markers of activated microglia and macrophages.[8] Separately, Tβ4 has been shown to protect spinal-cord-derived neural stem/progenitor cells from oxidative-stress-induced injury in vitro, acting through the TLR4/MyD88 pathway to preserve cell viability under hydrogen-peroxide challenge.[3] Because oxidative stress and neuroinflammation are core secondary-injury mechanisms, these effects are directly relevant.
Oligodendrogenesis and remyelination
Perhaps the most mechanistically interesting CNS finding is that Tβ4 promotes oligodendrogenesis — the generation of new myelinating oligodendrocytes from oligodendrocyte progenitor cells (OPCs). In demyelinating models (experimental autoimmune encephalomyelitis and cuprizone-induced demyelination), Tβ4 increased newly generated oligodendrocytes and remyelinated axons, with the number of new mature oligodendrocytes correlating with functional recovery; mechanistically this was linked to activation of the epidermal growth factor receptor (EGFR) pathway.[9] Since demyelination is a key contributor to conduction failure after SCI, an OPC-differentiation effect is squarely on target.
Neuroprotection and scar/lesion modulation
Across CNS-injury paradigms, Tβ4 is described as supporting neuronal and oligodendrocyte survival and reducing lesion cavity size, tilting the balance from tissue loss toward tissue preservation.[4] Reviews from the Chopp group frame Tβ4 as a neurorestorative agent that acts on multiple parenchymal cell types to increase neurogenesis, angiogenesis, oligodendrogenesis and axonal remodeling during the recovery phase, rather than as a classic acute neuroprotectant that merely shrinks the initial lesion.[8]
Why “neurorestorative” is a meaningful distinction
This restorative-versus-protective framing is worth dwelling on because it explains an otherwise puzzling result. In the traumatic brain injury work, delayed Tβ4 treatment improved functional outcome without reducing lesion volume.[5] A classic neuroprotectant is expected to save tissue and therefore shrink the lesion; if function improves while the lesion size is unchanged, the benefit is coming from remodeling and rewiring the surviving tissue — more new vessels, more new oligodendrocytes, more axonal sprouting and plasticity — rather than from preventing the initial cell death. That distinction matters clinically because most human patients present after the acute neuroprotective window has closed. A restorative agent that acts over days to weeks, on tissue that has already been injured, is a fundamentally more realistic therapeutic concept for real-world trauma than a drug that must be given within minutes. It is one of the more genuinely encouraging features of the Tβ4 preclinical profile — while remaining, again, unproven in human spinal cord injury.

What does the scientific research actually show about TB-500 and neural recovery?
This is the section where honesty about evidence level matters most. The mechanisms above are plausible and partly demonstrated, but demonstration of a mechanism is not demonstration of clinical benefit. Here is what the literature genuinely establishes, organized by model type, with the level of evidence flagged for each.
Rodent spinal cord injury models (in vivo, preclinical)
The most directly relevant study is Cheng and colleagues (2014), which tested Tβ4 in a rat SCI model. The reported results were consistent and favorable: Tβ4-treated animals showed better motor recovery than saline controls, with histology indicating promoted neuronal survival, decreased oligodendrocyte loss and subsequent demyelination, inhibition of the early inflammatory response, and a reduced lesion cavity area.[4] This is a well-aligned dataset — the outcomes map cleanly onto the proposed mechanisms — but it is a single-species, single-lab-scale animal study, and behavioral scores in rodent SCI do not translate directly to human function.
In-vitro cell studies (mechanistic, preclinical)
At the cellular level, Li and colleagues (2019) exposed spinal-cord-derived neural stem/progenitor cells to oxidative stress and found that Tβ4 dose-dependently increased viability of the injured cells, reversed pathological changes in intracellular calcium, and lowered lactate dehydrogenase release — with the protection mediated through the TLR4/MyD88 pathway.[3] In-vitro data like this clarify how Tβ4 might protect cells but say nothing about whether an intact injured spinal cord in a living organism recovers function.
Adjacent CNS-injury models: stroke, TBI and demyelination (supporting, preclinical)
Much of the confidence in Tβ4’s CNS potential comes not from SCI alone but from a consistent signal across related injury models — a body of work driven substantially by the group of Michael Chopp, Daniel Morris and colleagues at Henry Ford Hospital in Detroit. The value of this cluster of studies is that it tests the same peptide against several distinct CNS insults, so a repeated benefit is harder to dismiss as a quirk of one lesion type.
Traumatic brain injury
In experimental traumatic brain injury, delayed Tβ4 treatment (initiated 24 hours or more post-injury) did not reduce the initial lesion volume but significantly improved functional outcome, an effect attributed to enhanced angiogenesis, neurogenesis and oligodendrogenesis and increased vascular density in injured cortex and hippocampus.[5] A companion study asked whether an earlier start helped: Tβ4 (6 or 30 mg/kg, intraperitoneal) begun 6 hours after controlled cortical impact and repeated at 24 and 48 hours produced statistically significant improvement in sensorimotor recovery and spatial learning, reduced cortical lesion volume and hippocampal cell loss, and increased cell proliferation and neurogenesis — leading the authors to describe Tβ4 as offering both neuroprotection and neurorestoration depending on timing.[13] The pattern — earlier dosing preserving tissue, later dosing improving function without shrinking the lesion — is exactly what a dual protective/restorative agent would be expected to show.
Embolic stroke
In a rat model of embolic middle-cerebral-artery stroke, Tβ4 (administered 24 hours after occlusion and then every three days) improved functional neurological outcome. Histology pointed to a neurorestorative mechanism rather than acute rescue: increased oligodendrocyte progenitor cells in the subventricular zone, striatum and corpus callosum, more mature oligodendrocytes, evidence of axonal remodeling at the ischemic boundary, and increased vessel density consistent with angiogenesis in the peri-infarct zone.[14] Because the treatment began a full day after the ischemic event, the benefit cannot be explained by preventing the initial infarct; it reflects remodeling of surviving tissue.
Demyelination and multiple-sclerosis models
Reviews summarizing this body of work report that Tβ4 improves neurological outcome across the embolic-stroke model, a mouse multiple-sclerosis model, and the TBI model.[8] The demyelination studies add the remyelination dimension discussed above — increased generation of new oligodendrocytes and remyelinated axons in both inflammatory and chemical demyelination models, driven through EGFR signaling.[9] The convergence of these independent injury models is genuinely encouraging — a common set of restorative actions (oligodendrogenesis, angiogenesis, anti-inflammatory tone, axonal remodeling) surfacing across stroke, trauma and demyelination — but every one of these studies is in animals or cell culture, and none is spinal cord injury in a human.
Human clinical evidence for spinal cord injury: none
This point cannot be overstated. There are no published human clinical trials of Tβ4 or TB-500 for spinal cord injury. Tβ4 has been evaluated in human trials for unrelated indications (for example, dermal wound healing and dry-eye/corneal repair), but SCI efficacy in humans is entirely unestablished. Consequently, the safe dose, effective dose, route, timing, and even whether any functional benefit occurs in humans are all unknown. Any claim that TB-500 “heals” or “regenerates” the human spinal cord runs far ahead of the evidence.
| Evidence type | What it shows for Tβ4 / TB-500 | Evidence level |
|---|---|---|
| In-vitro cell studies (NSPCs under oxidative stress) | Dose-dependent cytoprotection via TLR4/MyD88; preserved viability | Preclinical, mechanistic |
| Rodent SCI model (Cheng 2014) | Better motor recovery, less demyelination, smaller lesion cavity | Preclinical, in vivo (single study) |
| Rodent TBI / stroke / demyelination models | Improved functional outcome; angiogenesis, neurogenesis, oligodendrogenesis | Preclinical, supporting (adjacent injury) |
| Human SCI clinical trials | No efficacy or safety data whatsoever | None |
Are there synergistic peptides that may enhance TB-500’s regenerative effects?
A frequent question in the research-peptide space is whether combining Tβ4/TB-500 with a second regenerative peptide — most commonly BPC-157 — produces additive or synergistic effects. This is a reasonable hypothesis to investigate, and it is worth being precise about what is and is not known.
The BPC-157 rationale
BPC-157, a synthetic pentadecapeptide, has its own preclinical literature in neural and soft-tissue repair. In a rat SCI model it improved the healing course of spinal cord injury and was associated with functional recovery.[6] Its most-cited nerve result is in the peripheral nervous system: in a rat transected-sciatic-nerve model, BPC-157 applied after injury accelerated axonal regeneration and improved functional and electrophysiological (EMG, walking) recovery.[15] The theoretical appeal of pairing the two is that they are proposed to act through different primary mechanisms — BPC-157 is often described in terms of angiogenic and cytoprotective signaling, nitric-oxide-system modulation and effects on growth-factor pathways, while Tβ4’s signature action is actin sequestration and the downstream migration/angiogenesis/oligodendrogenesis effects catalogued above. There is meaningful overlap (both are described as angiogenic and cytoprotective), but also genuinely distinct axes — Tβ4’s oligodendrogenesis/remyelination effect has no clear BPC-157 counterpart, and BPC-157’s peripheral-nerve axonal-regeneration data has no clear Tβ4 counterpart. In principle, partly non-overlapping mechanisms are the ingredients for additive benefit; in practice, that remains an untested hypothesis.
What the evidence does and does not support
The critical caveat: the individual SCI studies for BPC-157 and for Tβ4 were conducted separately, in different animal experiments. There is no high-quality controlled study demonstrating that the combination outperforms either peptide alone in spinal cord injury, and certainly none in humans. Claims of synergy are, at present, mechanistic speculation layered on two separate preclinical datasets — a hypothesis, not a result. Researchers exploring co-administration in experimental models sometimes reference a fixed-ratio blend; the properties of such combinations are described on the BPC-157 and TB-500 blend research protocol page. It should be read as documentation of a research formulation, not as evidence that the blend is effective in vivo for SCI.
Which research models and methods are used to study TB-500 in spinal cord injury?
Understanding the methodology clarifies both the strengths and the limits of the current evidence, and helps a scientifically literate reader weigh how far it can be extrapolated.
Contusion, compression and transection SCI models
Most in-vivo SCI work uses standardized rodent contusion (a calibrated impact onto the exposed cord) or compression (a clip or weight applied for a defined interval) at a specific vertebral level. A third class of model, transection (partial or complete surgical cut of the cord), is more severe and more artificial but useful for asking whether a treatment supports axon growth across a cleanly defined gap. The choice matters for interpretation. Contusion and compression reproduce the primary-plus-secondary injury sequence and the fluid-filled cavity seen in most human SCI, which is caused by blunt trauma rather than laceration, and they permit graded, reproducible lesion severity — so a benefit there is arguably more clinically relevant. A complete transection, by contrast, removes all spared tissue and tests regeneration in its harshest form; functional recovery in a contusion model can be driven partly by preserving and remodeling spared tissue (the neurorestorative mechanism Tβ4 favors), a route that is unavailable after full transection. The compression paradigm is the setting in which Tβ4’s anti-inflammatory profile — reduced pro-inflammatory cytokines, elevated IL-10, fewer activated microglia — was characterized,[8] and the core rat SCI efficacy study used a contusion-type injury — meaning the published Tβ4 SCI evidence speaks to the spared-tissue, remodeling scenario rather than to bridging a complete anatomical gap.
Functional and histological outcome measures
Recovery in these models is quantified with behavioral locomotor scales (open-field walking scores, gridwalk and inclined-plane tests) and confirmed with histology: counts of surviving neurons and oligodendrocytes, myelin markers such as myelin basic protein (MBP), lesion cavity area, vascular density, and immunostaining for inflammatory and progenitor-cell markers. The Cheng study’s improvements were established by exactly this combination of behavioral and histological readouts.[4]
In-vitro and progenitor-cell systems
Cell-based work uses cultured neural stem/progenitor cells, oligodendrocyte progenitor cells, or endothelial cells, often stressed with hydrogen peroxide (to model oxidative injury) or cultured in demyelinating conditions. These systems isolate specific mechanisms — cytoprotection, OPC differentiation, endothelial tube formation — under controlled conditions but remove the complex tissue environment of a real lesion.[3]
Delivery, the blood-brain/spinal barrier, and dosing-timing windows
Two practical variables shape whether a preclinical CNS result could ever translate: how the peptide reaches the lesion, and when it is given.
Delivery and the barrier problem. In the cited animal studies Tβ4 was typically given systemically by intraperitoneal injection rather than delivered directly into the cord. For a systemically dosed peptide to act on CNS tissue it must either cross the blood-brain/blood-spinal-cord barrier or exert its effects at the vasculature and injury margin, where the barrier is transiently disrupted after trauma. This is biologically plausible — barrier breakdown is part of the injury itself, and Tβ4’s angiogenic and endothelial actions are exerted precisely at the vascular interface — but it also means the effective concentration reaching deep parenchyma from a systemic dose is uncertain, and it complicates any attempt to reason from an animal dose to a human one. It is one reason a peptide can look effective in a small rodent, where diffusion distances are short, yet behave differently in the much larger human cord.
Timing windows. The animal data suggest Tβ4 has a relatively forgiving window compared with classic acute neuroprotectants: benefit was seen with dosing started 6 hours, 24 hours, or even later after injury, repeated over subsequent days.[13] A wide, delayed window is genuinely favorable for real-world trauma, where treatment cannot begin in the first minutes. But “forgiving in a rat” is not the same as a defined human therapeutic window, and the optimal start time, dose, dosing interval and total duration for a human spinal injury are all undetermined.
Why translation is hard
Rodent SCI differs from human SCI in scale, biomechanics, immune response, and the anatomy of the descending tracts that govern function. The human cord is far larger, so diffusion and barrier penetration are more demanding; the corticospinal tract is more critical to human motor function than to rodent locomotion; and human injuries are heterogeneous in level, severity and mechanism, unlike the standardized calibrated lesions used in the lab. Treatment timing in animal studies is tightly controlled, a precision rarely matched in emergency human trauma. These are the standard reasons neurorestorative agents that look strong in rodents frequently fail to replicate in human trials — the SCI field is littered with candidates that were compelling in rats and null in people — and they are the reason the Tβ4 SCI data, however clean, must be treated as hypothesis-generating rather than as evidence of a human effect.
The remyelination mechanism in more detail
Because remyelination is one of the most therapeutically consequential effects, it is worth unpacking. In the demyelination studies, Tβ4 did not simply protect existing myelin; it increased the population of newly generated oligodendrocytes, identified by co-labeling of a proliferation marker with oligodendrocyte-lineage markers, and these new mature oligodendrocytes were shown to remyelinate axons. Critically, the magnitude of new-oligodendrocyte generation correlated with the degree of functional improvement, and the effect held in both an inflammatory model (experimental autoimmune encephalomyelitis) and a non-inflammatory chemical demyelination model (cuprizone diet), pointing to a direct action on oligodendrocyte progenitor differentiation rather than a purely anti-inflammatory side effect. The proposed molecular driver was activation of the EGFR signaling pathway.[9] For spinal cord injury specifically, where demyelinated-but-surviving axons are a recognized reservoir of recoverable function, a genuine pro-remyelination mechanism is one of the more compelling reasons the field continues to study this peptide — with the perpetual caveat that the SCI-specific human question remains open.
What a realistic translational path would require
For TB-500/Tβ4 to move from “mechanistically promising” to “evidence-based,” the field would need well-powered, independently replicated large-animal SCI studies, followed by formal toxicology and pharmacokinetic characterization in humans, and only then controlled clinical trials with objective neurological endpoints. None of that has occurred for spinal cord injury. Readers encountering marketing that compresses this long, unfinished path into a claim of “spinal cord regeneration” should recognize the gap between an interesting preclinical candidate and a proven therapy — a gap that, for SCI, is currently total.
How does TB-500 compare with other spinal cord injury research strategies?
Tβ4 does not exist in a vacuum; it is one entry in a crowded field of experimental SCI approaches. Placing it in context clarifies both what is distinctive about it and why the bar for proving any SCI therapy is so high.
Cell-based and biomaterial strategies
Much SCI research centers on transplanting cells — neural stem/progenitor cells, oligodendrocyte precursors, mesenchymal stromal cells, Schwann cells — to replace lost tissue or provide a supportive substrate, sometimes combined with engineered scaffolds that bridge the lesion. Interestingly, Tβ4 intersects with this line of work: its demonstrated ability to protect neural stem/progenitor cells from oxidative injury[3] suggests a potential role not only as a standalone agent but as an adjunct that improves the survival of transplanted cells in a hostile lesion environment. That combinatorial idea remains preclinical and speculative for SCI.
Scar-modulating and axon-growth approaches
Other strategies attack the inhibitory scar directly — enzymatically digesting chondroitin sulfate proteoglycans, blocking myelin-associated inhibitors, or activating intrinsic axon-growth programs. Tβ4’s contribution here is indirect but complementary: by reducing lesion cavity size and modulating the inflammatory milieu, it may create a less hostile terrain for whatever growth the axons can muster.[4] Its oligodendrogenesis effect is arguably its most differentiated feature, since remyelination is a distinct axis from raw axon regrowth.[9]
What makes Tβ4’s profile distinctive
Where many candidates target one mechanism, Tβ4’s appeal is breadth: a single endogenous peptide plausibly touching migration, angiogenesis, inflammation, oxidative protection and oligodendrogenesis. Breadth is double-edged, however. A pleiotropic agent is harder to dose precisely, harder to attribute effects to a single pathway, and raises broader safety questions (an agent that drives migration and angiogenesis must be studied carefully in any context involving abnormal tissue growth). The comparison underlines a recurring theme: Tβ4 is a scientifically interesting, mechanistically broad research tool for CNS repair — not a validated treatment.
Handling, reconstitution and research-dosing context
The following is provided strictly for laboratory and educational context. It is not medical advice, not a recommendation for human use, and not a protocol for self-administration. TB-500 is not approved by the FDA or any comparable regulator for human therapeutic use; it is handled as an investigational research chemical, and in the studies discussed above it was administered to animals or cells, not people.
Reconstitution basics in research settings
Synthetic peptides like TB-500 are typically supplied as a lyophilized (freeze-dried) powder that must be reconstituted before use in an experimental system. In research practice this is generally done with bacteriostatic or sterile water, added slowly against the vial wall to avoid shearing the peptide, then gently swirled rather than shaken. Reconstituted peptide is stored refrigerated and protected from light and repeated freeze-thaw cycles, which degrade peptide integrity. The general principles — solvent choice, concentration math, and stability handling — are laid out in the peptide reconstitution guide.
Concentration math and study design
Because experimental work depends on precise, reproducible concentrations, researchers calculate the delivered amount per unit volume based on the mass of peptide and the volume of solvent. A peptide dosage calculator can convert a target concentration into practical volumes and is useful for planning consistent dosing across an experimental cohort. Note that animal-study doses are expressed per body weight (for example, the intraperitoneal regimens used in the TBI literature) and are not translatable to a human dose.
Reference documentation for common vial sizes
For readers using TB-500 as a reference research compound, dosagepeptide.com maintains documentation pages for common presentations, including the TB-500 5 mg vial research protocol and the TB-500 10 mg vial research protocol. These describe reconstitution and concentration references for laboratory documentation and should be understood in the research-and-educational framing that governs this entire article — they do not constitute clinical dosing guidance.
What are the limitations and open questions?
A fair assessment of TB-500/Tβ4 in spinal cord regeneration has to foreground its limitations as prominently as its promise.
- No human SCI data. The entire efficacy case is preclinical. Human safety, dosing, and effectiveness for spinal cord injury are unknown.
- Compound identity ambiguity. Published studies used defined thymosin beta-4; commercially labeled “TB-500” products vary in whether they are full-length Tβ4 or a fragment, and in purity. Findings from research-grade Tβ4 do not automatically transfer to an arbitrary product.
- Single-study depth for SCI. The core in-vivo SCI evidence rests heavily on one rat study; independent replication at scale is limited.
- Timing and delivery unknowns. Animal benefits often depend on early, controlled administration. The optimal therapeutic window, route, and dosing schedule for a human injury are undefined.
- Mechanism vs. outcome gap. Demonstrating angiogenesis, oligodendrogenesis or cytoprotection is not the same as demonstrating durable functional recovery; adjacent-model data (TBI, stroke) support plausibility but do not close this gap for SCI.
- Long-term safety. Because Tβ4 promotes cell migration and angiogenesis, questions about effects in the context of abnormal-tissue or tumor biology warrant careful study; these are not resolved for chronic human exposure.
The honest summary is that TB-500/Tβ4 is a mechanistically compelling preclinical candidate for CNS repair with a coherent, multi-target rationale and supportive animal data — and, simultaneously, an unproven agent for human spinal cord injury that has never been tested in a controlled human SCI trial.
Is TB-500 legal, and what is its regulatory and sport status?
The regulatory picture is unambiguous and important to state plainly. TB-500 is not an FDA-approved drug and is not a lawful dietary-supplement ingredient; it occupies the “research chemical” grey zone, sold for laboratory and educational use rather than human consumption. In competitive sport, TB-500 has been on the WADA Prohibited List since 2011, banned at all times under Section S2 (peptide hormones, growth factors, related substances and mimetics), and it remains prohibited under the current list.[10] Athletes subject to anti-doping testing face sanctions for its use. None of the preclinical promise discussed in this article changes that status.
Safety and handling in research settings
In a laboratory context, standard practices apply: peptides are handled with appropriate personal protective equipment, reconstituted and stored under conditions that preserve stability (refrigeration, light protection, minimal freeze-thaw), labeled clearly, and never used outside their approved research scope. Because there is no established human safety profile for TB-500 in spinal cord injury — or, indeed, an approved human indication at all — the only defensible framing is investigational. Researchers designing experiments should rely on peer-reviewed methodology and institutional oversight rather than marketing claims, and should treat any human-facing benefit statement about spinal cord regeneration as unsupported by current evidence.
Frequently Asked Questions
Does TB-500 regenerate the human spinal cord?
There is no evidence that it does. All supportive findings come from preclinical rodent spinal cord injury models, adjacent CNS-injury models (stroke, traumatic brain injury, demyelination) and in-vitro cell studies. No human clinical trials have tested thymosin beta-4 or TB-500 for spinal cord injury, so human efficacy, safety, and dosing remain entirely unknown. Claims of human spinal cord regeneration go well beyond what the science currently supports.
What is the difference between TB-500 and thymosin beta-4?
Thymosin beta-4 is the natural 43-amino-acid actin-sequestering peptide found in nearly all cells. “TB-500” is a research-market name that refers either to synthetic full-length thymosin beta-4 or to a short actin-binding fragment of it. Importantly, the rigorous published CNS studies used defined thymosin beta-4, so results from that research do not automatically apply to every product labeled TB-500.
How does thymosin beta-4 work at the molecular level?
Its core function is binding monomeric G-actin in a 1:1 complex, which regulates cytoskeletal dynamics and cell migration. Downstream, it promotes angiogenesis, supports oligodendrocyte progenitor differentiation (oligodendrogenesis), dampens inflammation, and protects cells from oxidative stress. This combination of activities is why it is studied in multifactorial injuries like spinal cord damage, where several processes must be addressed at once.
What do the animal studies actually show for spinal cord injury?
The main rodent SCI study reported better motor recovery, reduced oligodendrocyte loss and demyelination, suppression of early inflammation, and a smaller lesion cavity in thymosin beta-4-treated animals versus controls. These are consistent, encouraging preclinical results, but they come largely from a single animal study and do not translate directly to human outcomes without controlled clinical trials.
Can TB-500 be combined with BPC-157?
The two peptides are sometimes studied together because they are proposed to act through different mechanisms, and each has separate preclinical SCI data. However, no high-quality study shows that the combination outperforms either peptide alone in spinal cord injury, and none exists in humans. Any synergy claim is currently a mechanistic hypothesis, not a demonstrated result.
Is TB-500 approved or legal?
TB-500 is not FDA-approved for any human therapeutic use and is not a lawful dietary-supplement ingredient; it is sold as a research chemical for laboratory and educational purposes. In sport it has been on the WADA Prohibited List since 2011 and is banned at all times under Section S2. It is used in the studies discussed here only in animals and cells, not as an approved human treatment.
Why is spinal cord injury so hard to treat compared with other tissues?
The central nervous system has weak intrinsic regeneration, and after injury a glial-fibrotic scar and inhibitory molecules block axon regrowth. A secondary injury cascade of ischemia, oxidative stress and inflammation expands the damage, and demyelination disrupts signal conduction. Because so many processes fail at once, a pleiotropic agent like thymosin beta-4 is conceptually attractive for research — though attractiveness in theory is not the same as proven benefit.
What is the LKKTET/LKKTETQ actin-binding motif, and why does it matter?
It is the conserved central sequence of thymosin beta-4 (a hexapeptide LKKTET starting at residue 17, or the heptapeptide LKKTETQ spanning residues 17–23) through which the peptide binds monomeric G-actin. Mutational studies show this motif is required for actin binding, and the same seven-residue motif is also essential for the peptide’s angiogenic activity. It matters because it couples the peptide’s core biochemical function (actin regulation) to a repair-relevant behavior (new blood-vessel formation), which is part of why thymosin beta-4 is described as pleiotropic. Some “TB-500” fragment products are built around this motif rather than the full 43-residue protein.
Does thymosin beta-4 cross the blood-brain or blood-spinal-cord barrier?
In the animal studies the peptide was generally given systemically (intraperitoneal injection) rather than delivered directly into the cord, and it produced CNS effects. The most plausible explanation is a combination of action at the vasculature and injury margin — where the barrier is transiently disrupted by trauma and where thymosin beta-4’s angiogenic activity is exerted — rather than free passage across an intact barrier. The exact concentration reaching deep spinal tissue from a systemic dose is uncertain, which is one of several reasons animal doses cannot be translated to humans.
Have thymosin beta-4 or TB-500 been tested in humans at all?
Yes, but not for spinal cord injury. Thymosin beta-4 has been investigated in human trials for unrelated indications such as dermal wound healing and dry-eye/corneal repair. There are no human clinical trials for spinal cord injury, traumatic brain injury or stroke that establish efficacy for those indications, so the CNS-repair case remains entirely preclinical and the human safe/effective dose for these uses is unknown.
How does thymosin beta-4 compare with BPC-157 for neural repair research?
Both are preclinical peptides with separate animal literatures. Thymosin beta-4’s distinctive CNS feature is oligodendrogenesis and remyelination in central-nervous-system models, whereas BPC-157’s most-cited nerve result is accelerated axonal regeneration in a peripheral transected-sciatic-nerve model, alongside its own rat spinal-cord-injury data. They share angiogenic and cytoprotective descriptions but act partly through different pathways. No controlled study shows the combination outperforms either alone in spinal cord injury, and none exists in humans.
References
- National Institute of Child Health and Human Development. How many people are affected by spinal cord injury? U.S. Department of Health and Human Services.
- Hellenbrand, D. J., Quinn, C. M., Piper, Z. J., Morehouse, C. N., Fixel, J. A., & Hanna, A. S. (2021). Inflammation after spinal cord injury: a review of the critical timeline of signaling cues and cellular infiltration. Journal of Neuroinflammation, 18(1), 284.
- Li, H., Wang, Y., Hu, X., Ma, B., & Zhang, H. (2019). Thymosin β4 attenuates oxidative stress-induced injury of spinal cord-derived neural stem/progenitor cells through the TLR4/MyD88 pathway. Gene, 707, 136–142.
- Cheng, P., Kuang, F., Zhang, H., Ju, G., & Wang, J. (2014). Beneficial effects of thymosin β4 on spinal cord injury in the rat. Neuropharmacology, 85, 408–416.
- Xiong, Y., Mahmood, A., Meng, Y., Zhang, Y., Zhang, Z. G., Morris, D. C., & Chopp, M. (2012). Neuroprotective and neurorestorative effects of thymosin β4 treatment following experimental traumatic brain injury. Annals of the New York Academy of Sciences, 1270(1), 51–58.
- Perović, D., Kolenc, D., Bilić, V., et al. (2019). Stable gastric pentadecapeptide BPC 157 can improve the healing course of spinal cord injury and lead to functional recovery in rats. Journal of Orthopaedic Surgery and Research, 14(1), 199.
- Goldstein AL, Hannappel E, Kleinman HK. Thymosin β4: actin-sequestering protein moonlights to repair injured tissues. Trends in Molecular Medicine. 2005;11(9):421–429.
- Morris, D. C., Zhang, Z. G., Zhang, J., Xiong, Y., Zhang, L., & Chopp, M. (2012). Treatment of neurological injury with thymosin β4. Annals of the New York Academy of Sciences, 1269(1), 110–116.
- Zhang, J., et al. (2016). Thymosin beta4 promotes oligodendrogenesis in the demyelinating central nervous system. Neurobiology of Disease.
- Banned Substances Control Group (BSCG). TB-500 — Status, Risks, and Bans in Sport and Military (WADA Prohibited List, Section S2; regulatory status).
- Van Troys, M., Dewitte, D., Goethals, M., Carlier, M. F., Vandekerckhove, J., & Ampe, C. (1996). The actin binding site of thymosin β4 mapped by mutational analysis. The EMBO Journal, 15(2), 201–210.
- Philp, D., Huff, T., Gho, Y. S., Hannappel, E., & Kleinman, H. K. (2003). The actin binding site on thymosin β4 promotes angiogenesis. The FASEB Journal, 17(14), 2103–2105.
- Xiong, Y., Zhang, Y., Mahmood, A., Meng, Y., Zhang, Z. G., Morris, D. C., & Chopp, M. (2012). Neuroprotective and neurorestorative effects of thymosin β4 treatment initiated 6 hours after traumatic brain injury in rats. Journal of Neurosurgery, 116(5), 1081–1092.
- Morris, D. C., Chopp, M., Zhang, L., Lu, M., & Zhang, Z. G. (2010). Thymosin β4 improves functional neurological outcome in a rat model of embolic stroke. Neuroscience, 169(2), 674–682.
- Gjurasin, M., Miklic, P., Zupancic, B., et al. (2010). Peptide therapy with pentadecapeptide BPC 157 in traumatic nerve injury. Regulatory Peptides, 160(1–3), 33–41.