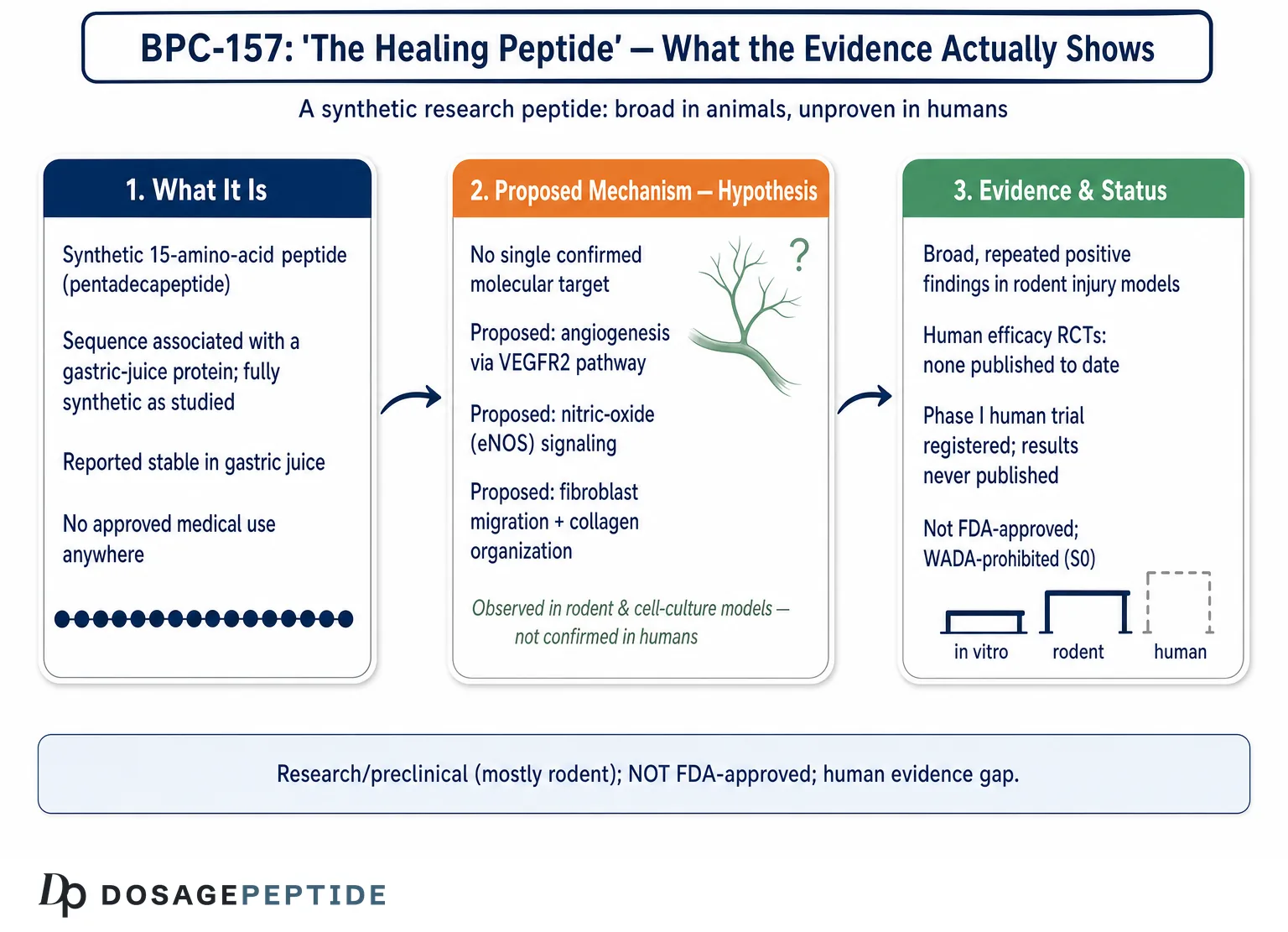
Few compounds in the peptide-research world carry as much popular momentum as BPC-157, and few carry a nickname as loaded as “the healing peptide.” That framing implies a settled fact: that a small synthetic peptide reliably repairs human tissue. The honest scientific picture is far more provisional. BPC-157 is a 15-amino-acid research peptide that has produced genuinely striking results in rodent and cell-culture experiments across tendon, muscle, gut, vascular, and nervous-system injury models. What it has not done is demonstrate those effects in adequately controlled human trials. As of 2026, there is still no published, peer-reviewed randomized controlled trial confirming that BPC-157 heals any condition in people.3
This article treats “the healing peptide explained” as an open research question rather than an established therapeutic claim. It walks through what BPC-157 actually is, where the molecule came from, the mechanisms researchers propose to explain its activity, the honest level of the evidence behind it, how it compares to related compounds, the animal models and methods that generated the data, its safety signals and gaps, handling in a laboratory context, and its regulatory status. Throughout, the goal is to separate what has been observed in controlled preclinical systems from what has been assumed, extrapolated, or marketed.
BPC-157 is best understood as an experimental substance of significant scientific interest and unresolved clinical value. It is not an approved drug, not a dietary supplement, and not a demonstrated human therapy. Reading the literature carefully rewards caution: the preclinical breadth is real, and so is the human-evidence gap. Holding both truths at once is the only intellectually honest way to discuss this compound.
What BPC-157 Is and Where It Came From
BPC-157 is a synthetic pentadecapeptide, meaning a chain of exactly fifteen amino acids. Its published sequence is Gly-Glu-Pro-Pro-Pro-Gly-Lys-Pro-Ala-Asp-Asp-Ala-Gly-Leu-Val, and its molecular weight is roughly 1419.5 daltons.1 The name is an abbreviation of “Body Protection Compound,” and the “157” reflects its designation within a research series. It was first introduced and characterized by Predrag Sikiric and colleagues at the University of Zagreb in the early 1990s, and that Zagreb group has authored a large share of the published literature on the molecule in the three decades since.1,2
The origin story that circulates online, that BPC-157 is a fragment “found in human gastric juice,” deserves a precise reading. The parent molecule, a larger protein, was described in gastric juice, and BPC-157 corresponds to a partial sequence associated with that source. Importantly, however, BPC-157 as studied is a fully synthetic peptide, and the published characterizations note that it shows no meaningful sequence homology with other known gut peptides.1 In other words, it is not a hormone or a well-established endogenous signaling molecule with a mapped receptor; it is a designed sequence whose relationship to native human physiology remains incompletely defined.
One property has driven much of the interest: stability. Most peptides are rapidly degraded in the acidic, enzyme-rich environment of the stomach, which is why peptide drugs are usually injected. BPC-157 was reported to remain stable in human gastric juice for extended periods, which is unusual and is the basis for the frequently repeated claim that it can be administered orally and still reach the gut intact.1,2 This gastric stability is a legitimate and interesting physicochemical observation. It does not, by itself, establish oral bioavailability into the systemic circulation in humans, nor does it establish that an orally delivered dose reaches distant tissues like tendon or brain at biologically meaningful concentrations. Those are separate pharmacokinetic questions that remain poorly answered in humans.
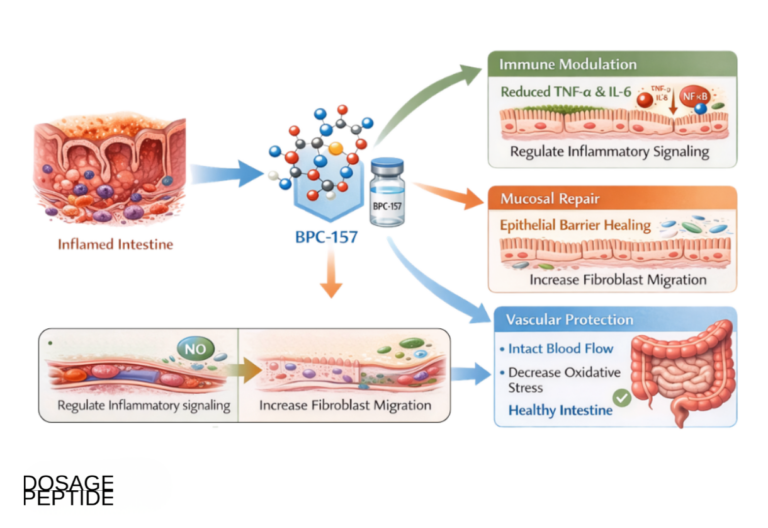
The label “cytoprotectant” appears throughout the foundational work. In the original research framing, BPC-157 was studied first for its apparent ability to protect the gastrointestinal lining against various forms of injury, including ulceration induced by chemicals, stress, and anti-inflammatory drugs in rodents.1,4 Over time, the research program expanded outward from the gut to an extraordinarily broad range of tissues and injury types, which is part of why the compound attracts both enthusiasm and skepticism. A molecule reported to help nearly everything, from tendon transection to brain injury to blood-vessel occlusion, invites the question of whether the effect is a genuine broad cytoprotective mechanism or an artifact of a single, heavily invested research lineage. That tension runs through the rest of this article.
It is also worth clarifying what BPC-157 is not, because the surrounding marketing often blurs these lines. It is not thymosin beta-4 or a fragment of it, despite frequently being sold alongside TB-500. It is not a growth hormone, a growth-hormone secretagogue, or an anabolic steroid, and it does not belong to the same regulatory or pharmacological family as those compounds. It is not a vitamin, an amino-acid supplement, or a “natural product” in the sense that a consumer supplement is, even though the “found in gastric juice” phrasing can make it sound endogenous and benign. Each of these distinctions matters because they change the questions a careful reader should ask. For a synthetic experimental peptide with no defined receptor and no approved indication, the relevant questions are about preclinical mechanism, translation to humans, product quality, and regulatory standing, not about the reassuring framing of a substance the body already makes.
To summarize the identity of the compound: BPC-157 is a stable, synthetic, fifteen-residue peptide of gastric-juice-associated origin, extensively studied in animals, with a proposed general “body-protecting” and pro-healing profile, and without an approved medical use anywhere in the world.
The Proposed Molecular Mechanism
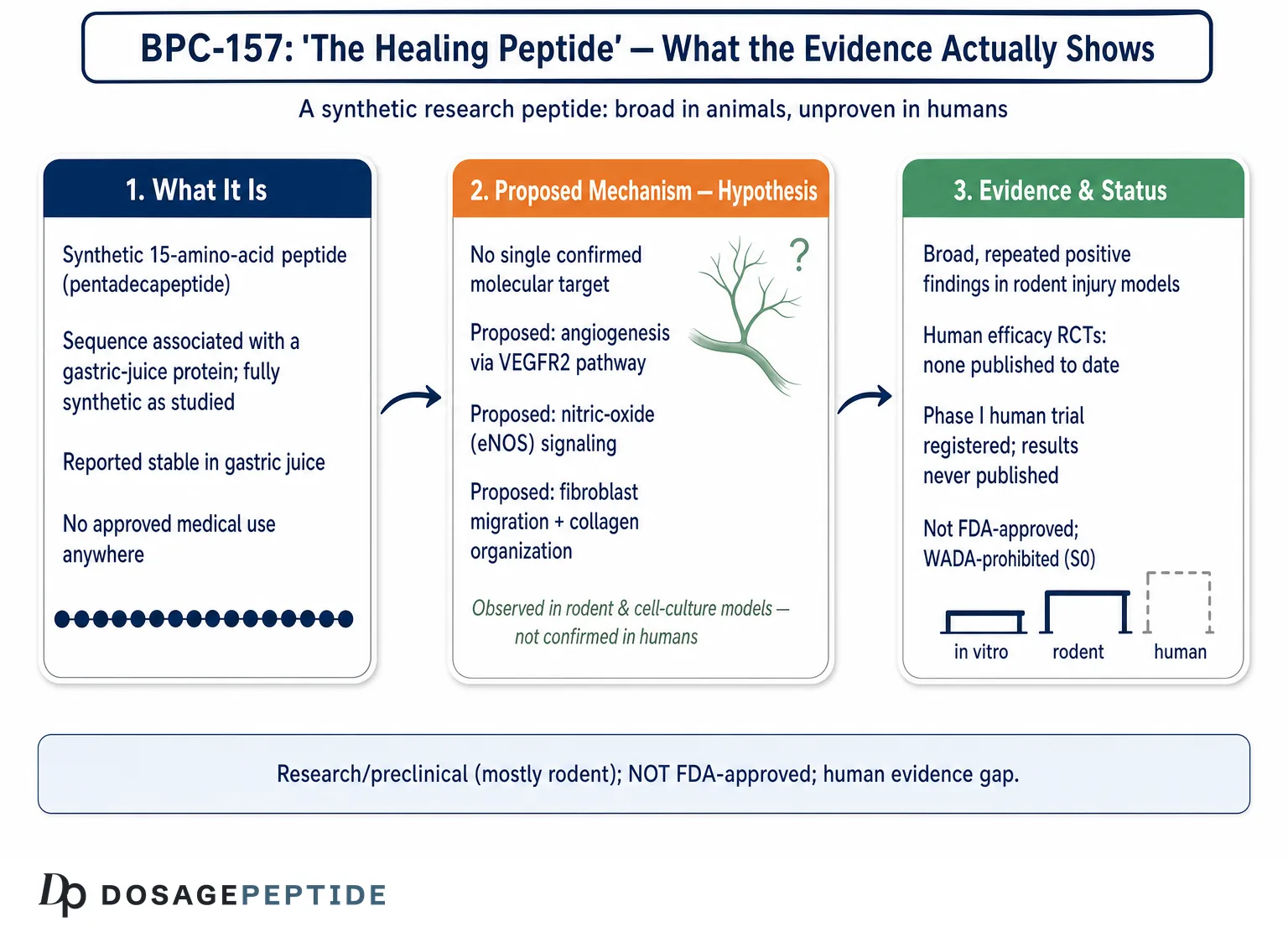
Unlike a typical drug with one well-characterized receptor, BPC-157 has no single agreed-upon molecular target. Instead, the literature describes a set of overlapping pathways that researchers propose to explain its effects. The most consistently invoked is angiogenesis, the formation of new blood vessels, because a repairing tissue needs new capillary supply to deliver oxygen and nutrients.5
Several preclinical reports center on the VEGF/VEGFR2 axis. In endothelial-cell experiments, exposure to BPC-157 has been associated with increased phosphorylation of vascular endothelial growth factor receptor 2 (VEGFR2) and activation of downstream signaling cascades such as the MAPK/ERK pathway that drive endothelial-cell proliferation and migration.5,6 In wound and injury tissue, animal studies have reported upregulation of VEGFR2 and faster ingrowth of capillaries. If these observations generalize, they would offer a plausible reason why a pro-angiogenic peptide could accelerate the vascular phase of healing.
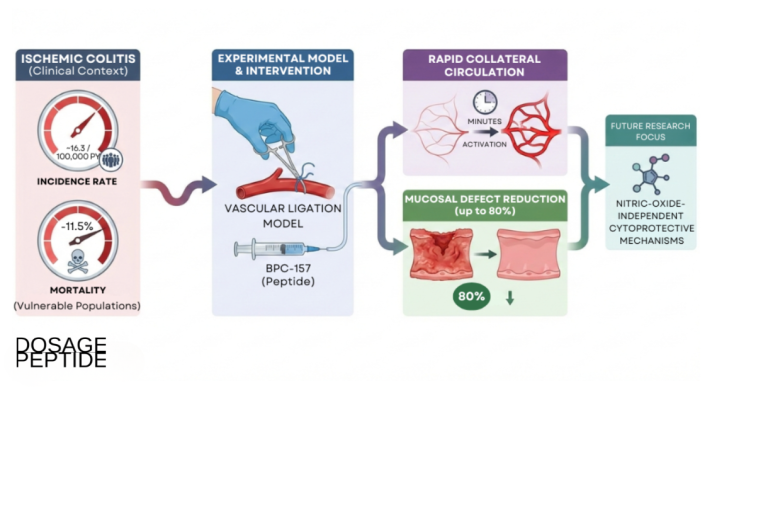
A second recurring theme is the nitric oxide (NO) system. BPC-157 has been reported to modulate NO synthesis, including via endothelial nitric oxide synthase (eNOS) and an Src-Caveolin-1-eNOS pathway that influences vascular tone and endothelial function.6 Nitric oxide is a central regulator of blood-vessel dilation, platelet behavior, and tissue perfusion, so an agent that fine-tunes NO signaling could, in principle, influence both cytoprotection and repair. Some rodent work frames BPC-157 as counteracting the harmful vascular consequences of injury, for example by helping recruit collateral circulation after a major vessel is occluded.
Beyond vasculature, the mechanistic literature describes growth-factor and matrix effects relevant to connective tissue. In tendon-fibroblast cultures, BPC-157 has been associated with increased cell migration toward an injury zone and with more organized deposition of collagen, the main structural protein of tendon and ligament.2,7 Additional angiogenic and trophic mediators such as fibroblast growth factor-2 (FGF-2) and epidermal growth factor (EGF) have been reported to rise in treated wound tissue. There are also reports of interactions with growth-hormone signaling and with the dopaminergic and serotonergic systems, which is how the compound’s proposed influence on neurological and behavioral endpoints is usually explained.2
| Proposed pathway | Reported preclinical effect | Evidence context |
|---|---|---|
| VEGFR2 / MAPK-ERK | Endothelial proliferation, migration, angiogenesis | Cell culture + rodent wound models |
| NO / eNOS (Src-Caveolin-1) | Vascular tone modulation, perfusion, cytoprotection | Rodent vascular and injury models |
| Collagen / fibroblast activity | Fibroblast migration, organized collagen deposition | Tendon-fibroblast culture, rodent tendon |
| Growth factors (FGF-2, EGF) | Upregulation in wound tissue | Rodent wound tissue analysis |
| Neurotransmitter systems | Dopamine/serotonin modulation | Rodent behavioral/neurological models |
A further mechanistic thread involves what some investigators call a “stabilizing” or homeostatic role. Rather than acting as a simple agonist that pushes one pathway in one direction, BPC-157 is described in parts of the literature as buffering systems back toward baseline, moderating both excessive and deficient signaling depending on context. This has been discussed in relation to the gut-brain axis, where the peptide is proposed to interact with vagal and enteric signaling, and in relation to the nitric-oxide system, where it is reported to counteract both the harmful effects of NO blockade and the effects of NO overload in rodent models.6 Whether this represents a genuine adaptive mechanism or an artifact of many separate experiments framed under one umbrella is unresolved. Claims of a molecule that “knows” which direction to push a system warrant particular skepticism until confirmed by independent, mechanistically controlled studies.
Two cautions are essential when reading this mechanistic map. First, the great majority of these findings come from rodents and cell cultures, not humans, and mechanisms observed in isolated systems do not automatically operate the same way, or at all, in an intact human body. Second, a compound that seems to touch angiogenesis, NO signaling, collagen biology, growth factors, and neurotransmitters simultaneously is either a remarkably pleiotropic cytoprotectant or a molecule whose reported breadth outruns its mechanistic definition. Both interpretations are live in the scientific community, and neither is resolved. The mechanistic story for BPC-157 is best described as a coherent set of preclinical hypotheses rather than an established human mechanism of action.
What the Evidence Actually Shows (An Honest Level)
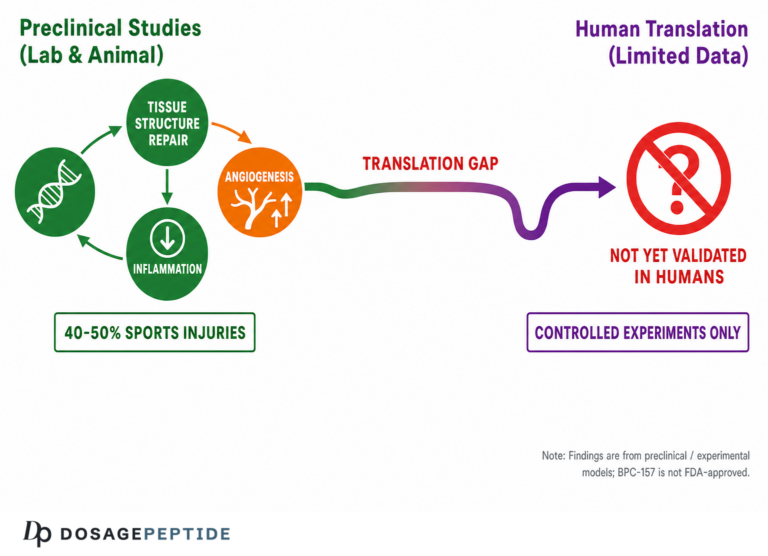
The single most important thing to understand about BPC-157 is the shape of its evidence base: broad and consistent in animals, nearly absent in humans. A 2025 systematic review of BPC-157 in orthopaedic sports medicine makes this concrete. Of 544 articles screened for that review, only one clinical study met the inclusion criteria; the remaining included studies were preclinical animal models.3 A single clinical study against dozens of animal experiments is not the profile of an established therapy. It is the profile of a compound whose translation to humans has barely begun.
What the preclinical evidence does show is worth stating fairly, because dismissing it entirely would be as inaccurate as overselling it. Across independent injury paradigms in rodents, BPC-157 has been reported to improve functional, structural, and biomechanical outcomes in muscle, tendon, ligament, and bone injuries.2,3 There are reproducible-looking reports of accelerated tendon-to-bone healing, faster closure of experimental wounds, protection of the gastric and intestinal lining against ulcerogenic insults, and recovery of function in models of vascular occlusion and organ dysfunction.1,4 The consistency across many endpoints is part of what keeps the scientific interest alive.
But several structural weaknesses limit how much weight this body of work can bear. A large fraction of it originates from a single research group, which raises the standard reproducibility concern that independent replication is needed before broad conclusions are drawn.2 Animal healing models, while useful, are simplified systems; a transected rodent tendon healing faster under peptide exposure does not establish that a human with a chronic tendinopathy would benefit. Publication and reporting patterns in this space also tend to emphasize positive results. And critically, the human pharmacokinetic foundation that would normally guide dosing, absorption, distribution, and clearance in people, is essentially missing.8
It is useful to distinguish three claims that are frequently collapsed into one in popular writing. The first claim is that BPC-157 does something biologically, which the preclinical data support: it plainly alters angiogenesis, collagen deposition, and injury markers in animal models. The second claim is that it accelerates healing in a controlled animal injury, which is also reasonably supported within the limits of those models. The third claim is that it heals or treats a condition in humans, which is not supported by any adequately controlled study. Marketing routinely uses evidence for the first two claims to imply the third. Recognizing where the evidence actually stops, at the boundary of the animal experiment, is the single most important interpretive skill when reading about this compound. Preclinical activity is a necessary precursor to a human therapy but very far from sufficient, and the history of drug development is full of compounds that healed rodents impressively and then failed in people.
The human clinical record is thin to the point of being almost anecdotal. A Phase I safety and pharmacokinetics trial of an oral BPC-157 tablet formulation (PCO-02) was registered on ClinicalTrials.gov (NCT02637284), but the sponsor cancelled submission of results, and no peer-reviewed results were ever published.8 Scattered small pilot efforts and clinic reports have appeared, but they are tiny, uncontrolled, and not the kind of evidence that supports efficacy claims. There is, to date, no adequately powered randomized controlled trial showing that BPC-157 heals a defined condition in humans.3
| Evidence tier | BPC-157 status |
|---|---|
| Cell-culture / in vitro | Multiple supportive reports (angiogenesis, fibroblast activity) |
| Rodent injury models | Broad, repeated positive findings across tissues |
| Larger-animal / PK studies | Very limited; short half-life reported in animal models |
| Human safety trials | Minimal; one Phase I registered, results unpublished |
| Human efficacy RCTs | None published to date |
The honest bottom line is that BPC-157 sits at an early, preclinical-to-translational stage. Calling it “proven” or “clinically validated” misrepresents the literature. Calling it “worthless” ignores a genuinely interesting and broad preclinical signal. The accurate description is that BPC-157 is a promising experimental peptide with an unproven human profile and an evidence base that stops well short of clinical recommendation. Anyone weighing the compound should treat the gap between rodent data and human outcomes as the central, unresolved fact, not a footnote. For those cataloguing how research schedules are described, our overview of peptide dosage protocols is presented strictly as reference material, not as evidence of efficacy.
How BPC-157 Compares to Related Research Peptides
BPC-157 is rarely discussed in isolation. In the recovery-focused corner of peptide research, it is most often compared and paired with TB-500, a synthetic fragment related to the protein thymosin beta-4. Understanding the comparison helps clarify what is distinctive about BPC-157 and what is shared marketing narrative versus shared evidence status.
TB-500 and BPC-157 are frequently framed as complementary because their proposed mechanisms differ in emphasis. BPC-157 is described primarily around angiogenesis, nitric oxide signaling, and localized collagen and fibroblast effects. TB-500, by contrast, is discussed mainly in terms of actin regulation and cell migration, with a proposed role in cell motility during tissue repair. The recovery-research community sometimes combines them on the theory that one supports vascular and collagen aspects of healing while the other supports cell migration, a rationale examined in our explainer on the BPC-157 and TB-500 recovery blend. It is essential to note that the “synergy” argument is a preclinical and theoretical construct; there is no human trial demonstrating that the combination outperforms either peptide, or placebo, for any outcome.
The critical similarity between the two is regulatory and evidentiary, not pharmacological. Both are unapproved experimental substances, both lack robust human efficacy data, and both appear on anti-doping frameworks as prohibited or non-approved compounds.9,10 A researcher comparing them is comparing two members of the same category, promising in animals, unproven in humans, rather than choosing between an established and an experimental option.
| Attribute | BPC-157 | TB-500 (thymosin beta-4 fragment) |
|---|---|---|
| Class | Synthetic pentadecapeptide | Synthetic peptide fragment |
| Emphasized mechanism | Angiogenesis, NO, collagen/fibroblast | Actin regulation, cell migration |
| Gastric stability claim | Reported stable in gastric juice | Not characterized the same way |
| Human efficacy evidence | None published (RCT) | None published (RCT) |
| Regulatory / anti-doping | Unapproved; WADA-prohibited | Unapproved; WADA-prohibited |
How does BPC-157 compare to actual approved regenerative or anti-inflammatory therapies? Unfavorably, in the specific sense that matters for medicine: approved options, whether a corticosteroid injection, a biologic, or a surgical repair, have passed controlled human trials and regulatory review, whereas BPC-157 has not. This does not mean the approved options are always better tolerated or more desirable; it means their benefits and risks are characterized in humans, and BPC-157’s are not. A fair comparison respects that asymmetry rather than treating an experimental peptide as if it belonged in the same evidence tier as a licensed drug.
Within the peptide-research literature itself, BPC-157’s distinctive selling points are its reported gastric stability and the sheer breadth of injury models in which it has shown signals. Its distinctive weakness, shared with its usual comparators, is the near-total absence of human confirmation. When researchers reference paired protocols such as a BPC-157 and TB-500 blend or a stacked TB-500 and BPC-157 protocol, they are working with combinations whose comparative advantages remain, for now, hypotheses rather than findings.
Research Models and Methodology
To read the BPC-157 literature critically, it helps to understand the experimental scaffolding that produced it. Nearly all of the influential data come from controlled laboratory systems, principally rodents (rats and mice) and cultured cells, using standardized injury paradigms designed to isolate a healing endpoint.
The tendon and musculoskeletal work is representative. Researchers surgically create a defined lesion, for example transecting a tendon, detaching a muscle from bone, or crushing a muscle, and then compare healing between treated and control animals across a fixed timeline.2 Outcomes are measured with functional tests (does the limb work), biomechanical tests (how much load the repaired tissue tolerates), and histology (what the tissue looks like under the microscope, including collagen organization and new vessel formation). The consistency of positive readouts across these independent measures is what gives the preclinical tendon and muscle data their apparent weight.2,3
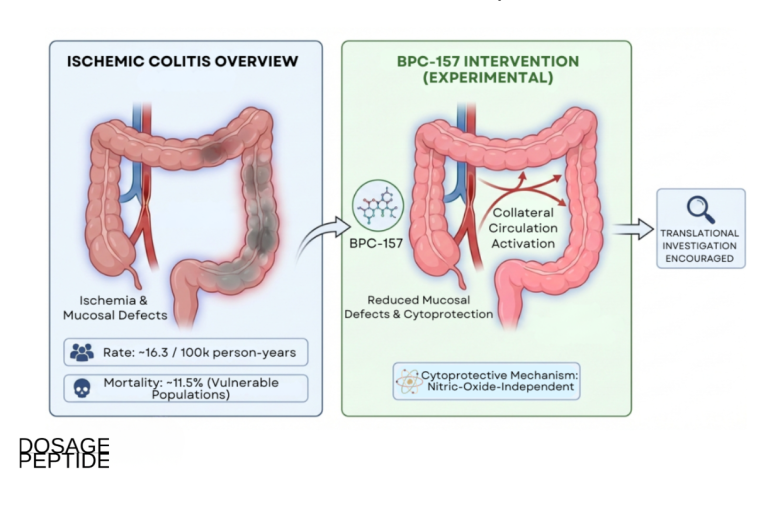
The gastrointestinal and vascular models follow a similar logic. Gastric-protection studies induce ulceration through known ulcerogenic agents, restraint stress, or NSAID exposure, then quantify the extent of mucosal damage with and without the peptide.1,4 Vascular studies use dramatic interventions such as occluding a major artery or maintaining elevated intra-abdominal pressure, then assess whether treated animals better preserve perfusion and organ function, sometimes attributing recovery to the rapid recruitment of collateral blood-flow pathways.1,13 These are legitimate, established model systems in pharmacology.
The methodological cautions, however, are substantial and are the reason careful reviewers stop short of clinical claims. Route and dose in these studies are typically parenteral (injected) and chosen for experimental convenience rather than derived from human pharmacokinetics; extrapolating an effective rodent dose to a human is not scientifically valid without bridging data, which is largely absent.3,8 Reported plasma half-life in animal models is short, on the order of well under an hour after intramuscular or intravenous administration, which complicates the story of how a rapidly cleared peptide produces durable structural changes and underscores how much remains unexplained about its pharmacokinetics.8
Model-organism limitations compound these issues. A healthy young rodent with an acute surgical lesion is a very different biological context from a middle-aged human with a chronic degenerative injury, comorbidities, and years of tissue remodeling. Acute-injury models can overstate what a compound will do in chronic disease. Study size, blinding, and independent replication also vary, and the concentration of the literature within one research program means that broad claims rest on a narrower base of independent confirmation than the raw study count suggests.2
Dose selection in the preclinical literature deserves a closer look because it is the source of much downstream confusion. Rodent studies commonly express dosing in micrograms or nanograms per kilogram of body weight, and effective ranges have been reported across a wide span. Translating any of these figures into a human context is not a matter of simple body-weight scaling; interspecies differences in metabolism, protein binding, and clearance mean that allometric conversion is an approximation at best and, without human pharmacokinetic anchoring, essentially guesswork. This is precisely why the research-reference dosing figures that circulate for BPC-157 should be understood as conventions inherited from animal work and community practice rather than validated human doses. Our reference material on related peptide protocols presents such figures strictly as documentation of how researchers describe handling, not as evidence that any dose is safe or effective in people.
The methodological takeaway is not that the animal science is invalid, it is that animal science answers animal questions. Well-designed rodent experiments can justify moving a compound toward human testing; they cannot substitute for that testing. For BPC-157, the models have done their job of generating hypotheses. The next step, adequately powered, blinded, randomized human trials, is precisely the step that has not been taken at scale, which is why every responsible summary of the methodology ends at the threshold of human application rather than crossing it.
Safety and Tolerability: What Is Known and Not Known
Safety discussion around BPC-157 tends to lean on a genuinely notable preclinical observation and then overextend it. The observation is that acute toxicity in animals appears very low. As reviewed in the foundational Sikiric-group literature, no lethal dose (no identifiable LD50 or LD1) has been established in the species tested, and those reviews recount administering doses far above standard experimental ranges without producing animal fatalities.1,11 That is a legitimate finding and suggests low acute toxicity in those models.
The overextension is treating “no LD50 in rodents” as if it meant “safe in humans.” It does not. Low acute lethality in animals says little about chronic toxicity, organ-specific effects at high cumulative exposure, immunogenicity, or delayed adverse effects, and it says nothing about safety in humans, who were not the test subjects.3 A compound can be non-lethal acutely in rats and still cause meaningful harm over months in people. The absence of a demonstrated acute-toxicity ceiling is reassuring only in the narrowest sense and should never be read as a green light.
The human safety database is thin. The registered Phase I oral trial (NCT02637284) was designed to characterize safety and pharmacokinetics, but its results were never published in peer-reviewed form, so it contributes almost nothing usable to a human risk assessment.8 Small, uncontrolled clinic reports do not establish a safety profile. This means the honest statement is that BPC-157’s human safety is essentially uncharacterized, not that it is proven safe.
Several theoretical and practical concerns deserve explicit mention. First is the angiogenesis question: a compound that promotes new blood-vessel growth raises a legitimate, unresolved concern about effects on abnormal tissue, since angiogenesis is also a feature of tumor growth. The preclinical literature does not settle this either way, and the uncertainty is a real limitation rather than a resolved point.2 Second is product-quality risk. Because BPC-157 is sold outside the regulated pharmaceutical supply chain, purity, identity, sterility, and dosing accuracy of “research” material are not guaranteed; regulatory agencies have flagged impurity and immunogenicity concerns as part of the rationale for restricting it.9,12 Contaminants and mislabeled content can pose risks entirely separate from the peptide itself.
| Safety dimension | What the data support |
|---|---|
| Acute toxicity (animal) | Very low; no LD50 identified in tested species |
| Chronic toxicity (animal) | Not well characterized |
| Human safety | Largely uncharacterized; Phase I results unpublished |
| Angiogenesis-related concern | Theoretically raised; unresolved |
| Product-quality risk | Real; unregulated supply, impurity concerns flagged |
A further practical point concerns reported adverse effects in the informal human record. Because there is no controlled trial capturing them systematically, what exists is scattered self-report: occasional mentions of injection-site reactions, transient lightheadedness, changes in blood pressure, headache, or gastrointestinal upset. These reports cannot be interpreted with any confidence. Without a placebo comparator and structured monitoring, it is impossible to know whether such effects reflect the peptide, the diluent, the injection procedure, contaminants in unregulated material, or unrelated coincidence. The absence of documented severe reactions in informal use is sometimes cited as reassurance, but absence of reported harm in an unmonitored, self-selected population is weak evidence and is not equivalent to demonstrated safety. Underreporting, short observation windows, and the healthy-user effect all bias such impressions toward the benign.
The responsible summary is that BPC-157 shows low acute toxicity in animal models but has an essentially unestablished human safety profile, with specific open questions around long-term exposure, angiogenesis, immunogenicity, and the quality of unregulated material. “Well tolerated in rats” and “safe for people” are different statements separated by exactly the human trials that have not been done. Tolerability claims that skip that distinction are not supported by the evidence.
Handling and Reconstitution in a Research Context
Because BPC-157 is distributed as a research chemical for laboratory use, questions about storage and reconstitution come up frequently. This section describes handling practices reported in the research-supply literature strictly for laboratory and educational context. It is not medical guidance, and nothing here should be read as endorsing human use of an unapproved substance.
BPC-157 is typically supplied as a lyophilized (freeze-dried) white powder in a sealed vial. In this dried state it is comparatively stable: lyophilized peptide is generally reported to remain intact for extended periods when kept frozen, with refrigeration adequate for shorter horizons and colder storage (for example around -20°C, or colder for long archival storage) preferred for periods beyond a year.14 The dried form’s stability is one reason vials are shipped without refrigeration in some cases, though minimizing warm exposure is still prudent.
Reconstitution refers to dissolving the powder into a liquid for laboratory measurement. The reagent commonly described for multi-use research handling is bacteriostatic water, which contains about 0.9% benzyl alcohol as a preservative that inhibits bacterial growth in the solution and thereby supports a longer usable window than plain sterile water.14 The standard reported technique is to add the diluent slowly down the inner wall of the vial rather than injecting it forcefully onto the powder, allowing the peptide to dissolve gently and reduce mechanical stress. The chosen diluent volume sets the final concentration, which in a research setting determines how the material would be measured; for example, our reference pages describe reconstituting a 10 mg vial with about 3.0 mL to reach roughly 3.33 mg/mL for convenient unit measurement, a purely arithmetic relationship between mass, volume, and concentration.
Once in solution, the peptide becomes more vulnerable and handling matters more. Reconstituted BPC-157 in bacteriostatic water is generally described as usable for roughly four weeks (commonly cited as up to 28 days) when refrigerated at 2 to 8°C with sterile technique.14 In solution the molecule is susceptible to oxidation, hydrolysis, and microbial contamination, so the practices reported to preserve integrity include refrigerating promptly, avoiding freeze-thaw cycling (each cycle is described as introducing mechanical and moisture stress that degrades peptide), and protecting the vial from light, since UV exposure can accelerate degradation.14 Some sources describe wrapping vials to shield them from light during storage and handling.
| State | Reported storage practice | Notes |
|---|---|---|
| Lyophilized powder | Frozen for long-term; refrigerated for short-term | Most stable form; avoid warm/humid exposure |
| Reconstitution diluent | Bacteriostatic water (0.9% benzyl alcohol) | Preservative supports multi-use window |
| Reconstituted solution | Refrigerate 2-8°C; use within ~28 days | Avoid freeze-thaw; protect from light |
For a fuller treatment of the arithmetic and technique involved, our BPC-157 vial reference page lays out concentration math in a research-reference format. Again, the framing here is laboratory handling of a research reagent. The gastric stability that makes BPC-157 interesting scientifically does not translate into solution stability once reconstituted, and none of these handling notes imply that the compound is appropriate, safe, or legal for human administration. They describe how a research material is kept chemically intact, nothing more.
Limitations and the Human-Evidence Gap
Every section above circles back to one dominant limitation, so it deserves to be stated plainly and centrally: the defining problem with BPC-157 is the chasm between its animal data and its human data. This is not a minor caveat to an otherwise solid case. It is the central fact that determines what can and cannot be responsibly said about the compound.
Consider the numbers again. A 2025 systematic review screened 544 articles and found a single clinical study meeting inclusion criteria, with essentially all the rest being animal work.3 That ratio tells you the field has generated a large hypothesis-rich preclinical literature and almost no confirmatory human literature. In evidence-based medicine, that configuration supports exactly one conclusion: BPC-157 is a candidate for human research, not a validated human intervention. No amount of rodent breadth changes that, because animal efficacy is a starting hypothesis, not proof of human benefit.
The gap has several specific dimensions. There is a pharmacokinetic gap: the absorption, distribution, metabolism, and clearance of BPC-157 in humans are not well established, and human dosing discussed online is extrapolated from animals rather than derived from human data.8 There is an efficacy gap: no published randomized controlled trial demonstrates benefit for any human condition.3 There is a long-term safety gap: chronic human exposure has not been studied, leaving questions about cumulative and delayed effects unanswered.3 And there is a reproducibility consideration: a large share of the positive preclinical literature originates from a single research lineage, so independent confirmation across laboratories remains an important unmet need.2
It is also worth naming the interpretive trap that the marketing around BPC-157 exploits. The compound’s very breadth, its apparent activity in gut, tendon, muscle, vessel, and nerve models, is presented as evidence of a powerful universal healer. But breadth without depth is a warning sign as much as a selling point. A claimed panacea that has never cleared a controlled human trial should invite more scrutiny, not less. The scientifically defensible reading of the breadth is that BPC-157 may engage some general cytoprotective and pro-angiogenic biology worth investigating, not that it reliably heals many human conditions.
A related limitation is the quality and independence of the evidence, not just its quantity. Even setting aside the human gap, the preclinical corpus would be stronger if more of it came from laboratories unconnected to the original discovery program, used pre-registered protocols, reported negative and null findings as readily as positive ones, and published complete methodological detail allowing exact replication. Concentration of a literature within a small number of closely associated groups is a recognized source of systematic bias, not because any individual study is necessarily flawed, but because independent replication is the mechanism by which science filters out artifacts, and that filter has been applied only partially here.2,3 When outside groups have looked at BPC-157, the picture has generally been more cautious than the enthusiastic framing found in consumer channels, which is itself informative.
There is also a translational-formulation gap that is easy to overlook. Much of the animal data uses injected peptide, yet a great deal of consumer interest centers on oral products, and the two routes are not interchangeable without evidence. Gastric stability, while genuine, is not the same as reliable, quantifiable systemic absorption and tissue delivery in humans. A compound can survive the stomach and still be absorbed erratically, metabolized rapidly, or fail to reach the target tissue at meaningful concentration. Because the one registered oral human trial never reported peer-reviewed results, this fundamental question, whether an oral dose does anything systemically in a person, remains genuinely open.1,8
What would actually close the gap is well understood and simply has not happened at scale: adequately powered, randomized, blinded, placebo-controlled human trials with defined endpoints, proper pharmacokinetic characterization, and independent replication. Until those exist, BPC-157’s status is fixed as experimental. Anyone describing it otherwise, as “proven,” “clinically effective,” or a “treatment,” is describing a compound that does not yet exist in the evidence. The honest, and admittedly unsatisfying, answer to “does BPC-157 heal?” is that we do not know in humans, and the current evidence does not permit the claim. That uncertainty is not a temporary rhetorical hedge; it is the accurate present state of the science.
Regulatory Status
The regulatory picture reinforces everything the evidence review implies. BPC-157 is not an approved drug anywhere. It has not been reviewed and authorized by the U.S. Food and Drug Administration, the European Medicines Agency, or any comparable national regulator for the treatment of any condition. Legally and practically, it exists as an unapproved, experimental substance.9,12
In the United States, the compounding pathway illustrates the regulatory caution well. In 2023, the FDA placed BPC-157 in Category 2 of the 503A bulk drug substances framework, the category for substances identified as presenting significant safety risks or as lacking sufficient supporting data, effectively restricting its use as a bulk substance in compounding.12 The agency’s stated concerns in this space have included impurities, immunogenicity, and limited clinical data.12 That placement should be read as of 2023: regulatory categorizations in the compounding arena have continued to be revisited procedurally through the 2024–2026 FDA and Pharmacy Compounding Advisory Committee (PCAC) review cycles, during which some peptides have been reassessed or moved between categories, so the specific bulk-substance classification can shift with review cycles. The core point, however, has held into 2026: BPC-157 remains an unapproved, non-FDA-approved substance, has not been established as a safe, effective, approved therapeutic, and its handling by regulators reflects unresolved safety and evidence questions rather than endorsement.
In sport, the position is unambiguous. The World Anti-Doping Agency added BPC-157 to its Prohibited List, and for the 2022 List it was, notably, named explicitly as an example within category S0 (Non-Approved Substances), which covers any pharmacological substance not currently approved by any governmental regulatory health authority for human therapeutic use.9,10 S0 substances are prohibited at all times, in and out of competition. Anti-doping authorities have specifically warned athletes that BPC-157 is an experimental, unapproved peptide sold in wellness products and that its use creates a doping-rule risk.9 For any competitive athlete, that alone is decisive.
The marketing workaround, labeling the product “for research use only” or “not for human consumption,” is a legal framing, not a safety or efficacy statement. That label exists precisely because the compound has not been approved for human use; it is an acknowledgment of unapproved status, not a loophole that makes the substance validated or safe. Purchasing material under that label means buying an unregulated product whose identity, purity, and sterility are not guaranteed by any regulatory authority.12
Putting the regulatory and scientific pictures together yields a consistent message from independent directions. The evidence base says: preclinically interesting, humanly unproven. The regulators say: unapproved, with open safety and quality concerns. The anti-doping authorities say: prohibited at all times as a non-approved substance. None of these bodies is treating BPC-157 as an established therapy, and neither should any accurate description of it. Its regulatory status is best summarized in one line: an unapproved experimental peptide, restricted or prohibited across the frameworks that have examined it, and lawful to discuss and study but not established, endorsed, or authorized as a treatment for anyone.
One additional consequence of this status is worth stating for readers who encounter BPC-157 in the marketplace. Because the compound is unapproved, it is manufactured and sold outside pharmaceutical good-manufacturing-practice oversight, which means there is no regulatory guarantee that a given vial contains what its label claims, in the amount claimed, at the purity claimed, or free of contaminants. Independent testing of gray-market peptide products across the industry has repeatedly found discrepancies between labeled and actual content. This quality uncertainty is not a peripheral detail; it compounds every scientific unknown discussed above, because even the animal-derived expectations assume a pure, correctly identified compound. An unregulated product introduces risks that are entirely separate from, and additional to, the intrinsic uncertainties of the molecule itself.
Frequently Asked Questions
Is BPC-157 FDA-approved?
No. BPC-157 is not approved by the FDA, the EMA, or any comparable regulator for any medical use. In 2023 the FDA placed it in Category 2 of the 503A bulk substances framework, citing significant safety concerns, and it remains an unapproved experimental substance.12 It is not a dietary supplement and not a licensed medicine.
Does BPC-157 actually heal injuries in people?
This is not established. BPC-157 has shown broad healing-related effects in rodent and cell-culture models, but a 2025 systematic review found only one clinical study among 544 screened articles, the rest being animal work.3 There is no published randomized controlled trial demonstrating that it heals any condition in humans. The accurate answer is that human efficacy is unproven.
Where does BPC-157 come from?
It is a synthetic 15-amino-acid peptide (sequence Gly-Glu-Pro-Pro-Pro-Gly-Lys-Pro-Ala-Asp-Asp-Ala-Gly-Leu-Val) first described by Sikiric and colleagues in the early 1990s. It corresponds to a partial sequence associated with a protein described in human gastric juice, but as studied it is fully synthetic and shows no meaningful homology with known gut peptides.1
How is BPC-157 thought to work?
There is no single confirmed target. Proposed mechanisms from preclinical work include promotion of angiogenesis via the VEGFR2 pathway, modulation of nitric oxide signaling through eNOS, effects on fibroblast migration and collagen organization, and upregulation of growth factors such as FGF-2 and EGF.5,6,7 These are hypotheses grounded in animal and cell studies, not a proven human mechanism of action.
Is BPC-157 safe?
Animal studies suggest low acute toxicity; as reviewed in the foundational Sikiric-group literature, no LD50 has been identified in the tested species.1,11 However, that does not establish human safety. Long-term effects, immunogenicity, and theoretical concerns such as the influence of a pro-angiogenic agent on abnormal tissue are not resolved, and human safety data are minimal.3 Unregulated product quality adds a separate, real risk.
Is BPC-157 legal, and is it banned in sport?
BPC-157 is not an approved drug, and products are typically sold labeled “for research use only,” a reflection of unapproved status rather than a safety endorsement.12 In sport it is explicitly prohibited: WADA included it by name as an example in category S0 (Non-Approved Substances) of the 2022 Prohibited List, making it banned at all times for tested athletes.9,10
How is BPC-157 different from TB-500?
Both are unapproved experimental recovery peptides often discussed together, but their emphasized mechanisms differ: BPC-157 centers on angiogenesis, nitric oxide, and collagen/fibroblast effects, while TB-500 is discussed around actin regulation and cell migration. Neither has human efficacy trials, and both are WADA-prohibited. Their proposed “synergy” is theoretical, not clinically demonstrated.2,9
Can BPC-157 be taken orally?
BPC-157 is unusual in being reported stable in gastric juice, which is the basis for oral-use claims.1 However, gastric stability does not by itself prove systemic absorption or delivery to distant tissues in humans, and the one registered oral Phase I trial never published results.8 Oral human pharmacokinetics remain poorly characterized.
References
- Sikiric P, et al. Stable Gastric Pentadecapeptide BPC 157 and Wound Healing. Frontiers in Pharmacology. 2021;12:627533. https://www.frontiersin.org/journals/pharmacology/articles/10.3389/fphar.2021.627533/full
- Multifunctionality and Possible Medical Application of the BPC 157 Peptide, Literature and Patent Review. Pharmaceuticals (MDPI). 2025;18(2):185. https://www.mdpi.com/1424-8247/18/2/185
- Vasireddi N, Hahamyan H, Salata MJ, et al. Emerging Use of BPC-157 in Orthopaedic Sports Medicine: A Systematic Review. 2025. doi:10.1177/15563316251355551. https://journals.sagepub.com/doi/abs/10.1177/15563316251355551
- Concerning BPC-157, a natural pentadecapeptide that acts as a cytoprotectant and is believed to protect the gastrointestinal tract. Inflammopharmacology. 2025. PMC12396989. https://pmc.ncbi.nlm.nih.gov/articles/PMC12396989/
- Stable Gastric Pentadecapeptide BPC 157 and Striated, Smooth, and Heart Muscle. PMC. PMC9775659. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9775659/
- Modulatory effects of BPC 157 on vasomotor tone and the activation of the Src-Caveolin-1-endothelial nitric oxide synthase pathway. PMC. PMC7555539. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7555539/
- Stable Gastric Pentadecapeptide BPC 157 as a Therapy for the Disabled Myotendinous Junction in Rats. PMC. PMC8615275. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8615275/
- PCO-02, Safety and Pharmacokinetics Trial (BPC-157 oral tablet). ClinicalTrials.gov Identifier NCT02637284. https://clinicaltrials.gov/study/NCT02637284
- U.S. Anti-Doping Agency (USADA). BPC-157: Experimental Peptide Creates Risk for Athletes. https://www.usada.org/spirit-of-sport/bpc-157-peptide-prohibited/
- World Anti-Doping Agency. Athlete Advisory: Key Changes on the 2022 WADA Prohibited List (S0 Non-Approved Substances). https://www.usada.org/athlete-advisory/key-changes-2022-prohibited-list/
- Sikiric P, Seiwerth S, Rucman R, et al. Stable Gastric Pentadecapeptide BPC 157: Novel Therapy in Gastrointestinal Tract. Current Pharmaceutical Design. 2011;17(16):1612-1632. doi:10.2174/138161211796196954. (Foundational Sikiric-group review reporting no achievable lethal dose in tested species.) https://pubmed.ncbi.nlm.nih.gov/21548867/
- U.S. Food and Drug Administration. Certain Bulk Drug Substances for Use in Compounding That May Present Significant Safety Risks (503A Category 2). https://www.fda.gov/drugs/human-drug-compounding/certain-bulk-drug-substances-use-compounding-may-present-significant-safety-risks
- Occlusion of the Superior Mesenteric Artery in Rats Reversed by Collateral Pathways Activation: Gastric Pentadecapeptide BPC 157 Therapy. PMC. PMC8229949. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8229949/
- Manning MC, Chou DK, Murphy BM, Payne RW, Katayama DS. Stability of Protein Pharmaceuticals: An Update. Pharmaceutical Research. 2010;27(4):544-575. doi:10.1007/s11095-009-0045-6. (Peer-reviewed review of peptide/protein degradation pathways—oxidation, hydrolysis, deamidation—and stabilization in aqueous solution versus the lyophilized state.) https://pubmed.ncbi.nlm.nih.gov/20143256/
Educational and research-use disclaimer: This article is provided for educational and informational purposes only and describes preclinical, experimental research on BPC-157. BPC-157 is not approved by the FDA, EMA, or any comparable regulatory authority for the diagnosis, treatment, cure, or prevention of any disease, and the great majority of the supporting evidence comes from animal and cell-culture studies rather than humans. Nothing here is medical advice or an endorsement of human use, and no claim of human efficacy or safety is made or implied. BPC-157 is prohibited in sport by WADA. Any research involving this compound should be conducted only by qualified individuals in appropriate settings and in compliance with all applicable laws and institutional requirements. Consult a licensed healthcare professional before making any health-related decision.