Search for “KLOW benefits” and you will find a remarkably confident body of copy: skin that heals faster, joints that recover overnight, gut inflammation that quiets down, collagen that rebuilds, energy that returns. The blend is marketed as a kind of all-purpose repair cocktail, and the language is fluent, specific, and reassuring. The problem is that almost none of it rests on the thing a reader would assume it rests on — a study of KLOW. This article takes the marketing claims seriously enough to check them against the actual literature, component by component, and to separate what the research genuinely supports from what has simply been asserted. The honest headline is that KLOW is an unapproved, untested research blend whose apparent evidence base is entirely borrowed from its four ingredients, and whose ingredients themselves range from cosmetically studied to almost entirely preclinical.
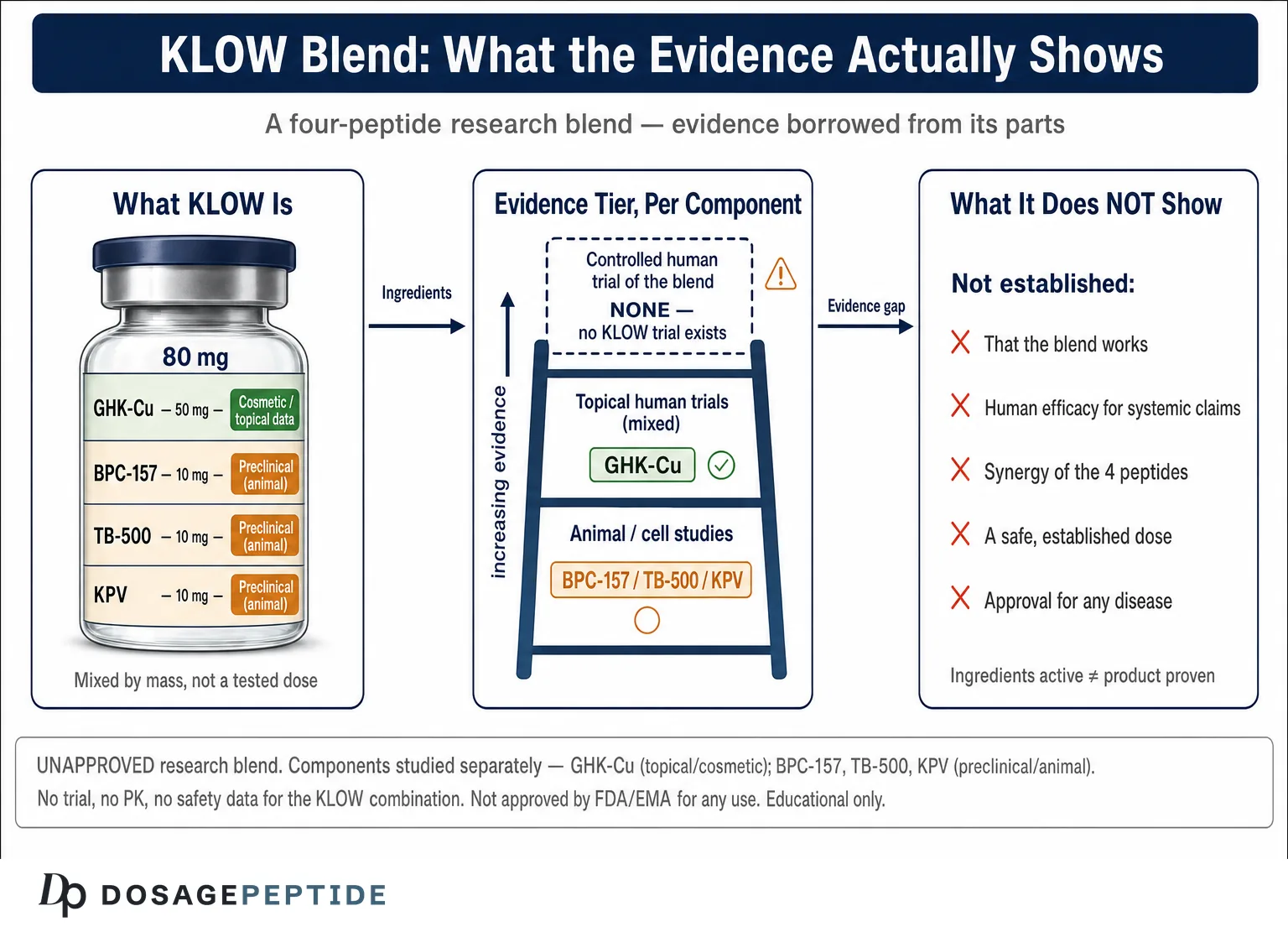
KLOW is a lyophilized four-peptide combination, most commonly sold as an 80 mg vial containing 50 mg of GHK-Cu, 10 mg of BPC-157, 10 mg of TB-500, and 10 mg of KPV.1 Each of those four molecules has its own literature, its own mechanism, and its own very different level of evidence. GHK-Cu has real cosmetic and cell-biology data behind it. BPC-157 and TB-500 have large preclinical footprints in animals but essentially no rigorous human efficacy trials. KPV has a small but genuine set of animal colitis studies and almost nothing else. What none of them has — and what the blend as a whole entirely lacks — is a single controlled clinical trial of the KLOW combination in humans, an established dose, a pharmacokinetic profile, or approval by any drug regulator for any indication. This piece is written for researchers and careful readers who want an evidence map rather than a sales pitch: what each component actually shows, what the combination does not show, and why the gap between the two is the most important fact about the product.
What KLOW Actually Is
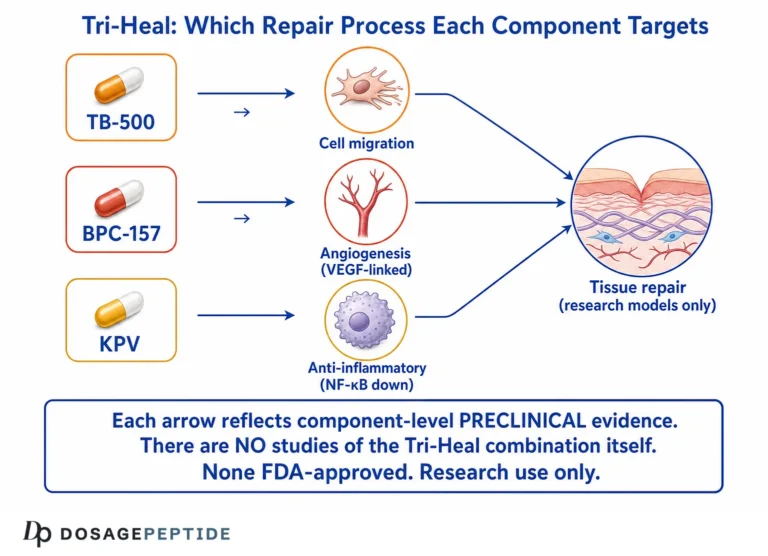
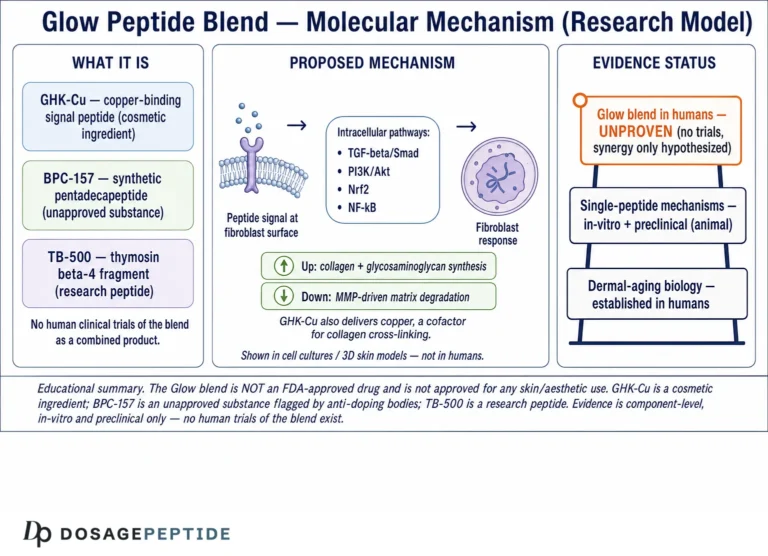
The name KLOW is a loose acronym assembled from its ingredients, and the blend is a close cousin of the older “GLOW” combination (GHK-Cu, BPC-157, TB-500) with the melanocortin-derived tripeptide KPV added. Vendors describe it as a “recovery” or “systemic repair” stack, and the marketing logic is one of convergence: four peptides that each touch some aspect of wound healing, angiogenesis, collagen, or inflammation are combined on the theory that their effects will stack or synergize. That theory is superficially appealing and, importantly, has never been formally tested. Combining four bioactive peptides is a pharmacological decision with real consequences — for dosing, for stability, for interactions, and for safety — and there is no published work establishing that this particular combination is additive, synergistic, redundant, or even mutually compatible in solution.
It helps to lay out the four components precisely, because the marketing tends to blur them into a single “healing” entity when in fact they come from four different biological worlds.
| Component | Typical amount in an 80 mg vial1 | What it is | Best-established biology |
|---|---|---|---|
| GHK-Cu | 50 mg | Copper-bound tripeptide glycyl-L-histidyl-L-lysine, isolated from human plasma in 1973 | Skin remodeling, collagen/glycosaminoglycan modulation, gene expression — largely cosmetic and cell-biology data2 |
| BPC-157 | 10 mg | Synthetic 15-amino-acid “body protection compound” sequence derived from a gastric protein fragment | Soft-tissue and gut healing in rodent models6 |
| TB-500 | 10 mg | Synthetic fragment corresponding to the actin-binding region of thymosin β4 | Cell migration and angiogenesis; animal repair models plus a few Phase 2 trials of the full protein8 |
| KPV | 10 mg | Tripeptide lysine-proline-valine from the C-terminus of α-MSH | Anti-inflammatory effects in mouse colitis models10 |
A first honest observation follows directly from the table: the blend is dominated, by mass, by GHK-Cu, the one component whose strongest evidence is topical and cosmetic. The three peptides most associated with systemic “healing” claims — BPC-157, TB-500, and KPV — each make up an eighth of the vial and each rest primarily on animal data. That composition alone should temper expectations, because the marketing narrative of deep systemic tissue repair leans hardest on the components with the thinnest human evidence. Readers who want the individual back-stories can follow the component pillars, such as the overview of what BPC-157 is and how it is studied and the review of what GHK-Cu does for skin, wrinkles, and collagen.
The Central Problem: There Is No Study of KLOW
Before examining any individual benefit, the single most important fact must be stated plainly, because it frames everything else: there is no clinical trial, no controlled preclinical study, and no published pharmacokinetic characterization of the KLOW blend itself. A literature search for the combination returns product listings and marketing pages, not primary research. Every claim you will read about “KLOW benefits” is therefore an act of extrapolation — taking evidence generated for one isolated peptide, often in animals, often by a different route of administration, and transferring it wholesale onto a four-ingredient mixture that was never studied as such.
This matters more than it might first appear, for several concrete reasons. First, combining peptides can change their behavior: copper in GHK-Cu is a redox-active metal, and its presence in the same solution as three other peptides raises legitimate, unstudied questions about oxidation, complex formation, and stability. Second, the components have wildly different pharmacokinetics — KPV is a tripeptide with a very short half-life, GHK-Cu is a small copper complex cleared quickly, and the larger peptides behave differently again — so a single injection cannot deliver all four in a coordinated way even in principle. Third, and most fundamentally, “each ingredient does something in isolation” is not evidence that “the mixture does the sum of those somethings” in a living system. Drug development is littered with rational-looking combinations that failed to add up, or actively interfered with one another.
The pharmacokinetic mismatch deserves a moment more, because it is a technical objection that few marketing pages engage with. Consider the timescales. KPV is a three-residue peptide; small peptides of this kind are typically cleared from circulation within minutes unless protected. GHK-Cu is a small copper complex that is also rapidly taken up and cleared. BPC-157 and the TB-500 fragment are larger and behave differently again, with their own absorption and distribution kinetics. A single subcutaneous injection of a blend cannot make four molecules with different sizes, charges, and clearance rates arrive at a target tissue in the same concentration window, let alone in whatever ratio would be needed for a hypothetical synergy. The vial ratio — 50:10:10:10 by mass — is a manufacturing convenience, not a pharmacologically optimized dose, and it certainly is not a ratio that any experiment identified as effective. When four molecules with divergent kinetics are combined by weight and injected together, what actually reaches any given cell is unknown and unmeasured.
So the correct scientific posture toward KLOW as a product is agnosticism about the blend and precision about the parts. When a marketer says KLOW “accelerates tissue repair,” the honest translation is: “one or more of these four peptides showed a repair-related effect in a model system, usually an animal or a cell culture, and we are assuming that carries over to this human-injected mixture.” That assumption may or may not be true; the point is that no one has checked. The rest of this article therefore does the only thing the evidence permits — it evaluates the four components individually and honestly, and then returns to what the combination as a whole can and cannot claim.
GHK-Cu: The Best-Evidenced Component — and Its Limits
GHK-Cu is the component with the deepest and most respectable literature, so it deserves the most careful treatment. It is a naturally occurring copper-binding tripeptide first isolated from human plasma, where its concentration declines markedly with age — from roughly 200 ng/mL around age 20 to about 80 ng/mL by age 60, a decline that has been linked (correlationally) to the fall in regenerative capacity that accompanies aging.2 In cell and tissue studies it does genuinely interesting things: it modulates the synthesis and breakdown of collagen and glycosaminoglycans, influences matrix metalloproteinases and their inhibitors, stimulates decorin and other proteoglycans, and, in gene-expression analyses, shifts the activity of a large number of genes in a direction associated with tissue remodeling and antioxidant defense.23 The mechanistic story is real and well documented, and it is why GHK-Cu appears widely in cosmetic dermatology.
The clinical evidence, however, is almost entirely topical and cosmetic, and it is more mixed than the marketing suggests. Small human studies of GHK-Cu creams have reported improvements in skin density, wrinkle depth, and elasticity, and it has been compared favorably in some trials to vitamin C and retinoic acid for stimulating collagen. But the countervailing data matter just as much. In a controlled trial of copper tripeptide complex applied to CO₂ laser-resurfaced skin, the GHK-Cu product produced no significant reduction in post-treatment redness and no significant objective improvement in wrinkles or overall skin quality compared with control, even though patient satisfaction was higher.4 That is an honest, instructive result: a well-designed study in which the objective endpoints did not move. It is exactly the kind of finding that vendor summaries omit.
Beyond cosmetics, GHK-Cu has a longer history in wound healing that is worth stating accurately, because it is frequently invoked as proof of “systemic repair.” The copper-peptide complex has been studied in experimental wound models and in some clinical wound settings, where it has been associated with faster re-epithelialization and improved healing of certain chronic wounds, and mechanistically it recruits immune and endothelial cells to injury sites and influences the growth factors involved in granulation.213 Its more recent scientific interest centers on gene expression: microarray analyses show that GHK-Cu can shift the activity of a large fraction of the human genome in a direction associated with tissue remodeling, anti-inflammatory signaling, and antioxidant defense, which is the basis for the “resets aging genes” language that circulates online.3 That gene-modulation work is real and intriguing, but it is largely in-vitro and does not, on its own, establish a clinical benefit for any injected human indication. It is a mechanism in search of a controlled outcome trial, not a proven therapy.
Two further limitations apply directly to KLOW. First, the vast majority of GHK-Cu evidence involves topical application to skin, whereas KLOW is a reconstituted injectable. Delivering a copper complex systemically by injection is a different pharmacological proposition from smoothing a cream onto the epidermis, with different exposure, distribution, and safety considerations, and the topical cosmetic data do not transfer automatically to that route. Second, even the topical human trials are typically small, short, and frequently industry-associated, with sparse long-term data. GHK-Cu is best described as a compound with plausible mechanisms, decent cosmetic support for topical skin appearance, and essentially no rigorous evidence for systemic injected use in humans for any medical indication. It is not FDA-approved as a drug for anything; its established home is the cosmetic shelf, not the pharmacy. For the fuller picture on the collagen-synthesis question specifically, the analysis of whether the GLOW/KLOW-type peptides support collagen synthesis pathways walks through the cell-biology in more depth.
BPC-157: Preclinical Promise, Human Void
BPC-157 is the peptide most responsible for KLOW’s “heals everything” reputation, and it is also the clearest example of a compound where preclinical enthusiasm has vastly outrun human evidence. The animal literature is genuinely substantial. In a widely cited 2003 study, systemic BPC-157 accelerated healing of a transected rat Achilles tendon and stimulated tendocyte growth in vitro, restoring biomechanical and histological parameters faster than in controls.5 Later mechanistic work showed that BPC-157 promotes the outgrowth, survival, and migration of tendon fibroblasts through the FAK-paxillin pathway and upregulates the growth-hormone receptor in tendon cells.6 Across dozens of rodent studies it has shown effects on gut ulcers, muscle-to-bone healing, ligament and tendon injury, and various vascular and anti-inflammatory endpoints. Taken together, this is a real and reproducible animal signal.
Mechanistically, BPC-157 is proposed to work through several overlapping pathways in these animal studies: modulation of the nitric-oxide system, upregulation of growth-factor and growth-hormone receptors in target cells, promotion of angiogenesis via VEGFR2 signaling, and a stabilizing effect on the gut-brain axis and vascular integrity. The peptide was originally derived from a fragment of a protein found in gastric juice and is notable for being stable in that harsh environment, which is part of what first attracted interest. These are coherent, actively researched mechanisms, and it would be unfair to dismiss the preclinical work as trivial — it is genuinely one of the more reproduced animal repair signals in the peptide field.
The honest problem is what sits on the other side of the species barrier: almost nothing. A 2025 narrative review of BPC-157 for musculoskeletal healing concluded that the overwhelming majority of the evidence is preclinical — primarily rats — with very limited human clinical data, and it explicitly flagged the gap between the animal promise and the absence of rigorous controlled trials in people.7 There is no adequately powered, randomized, placebo-controlled human trial establishing that injected BPC-157 heals tendons, joints, or gut tissue in humans at any defined dose. The compelling rat data cannot substitute for that. Animal healing models are notoriously optimistic predictors; the history of regenerative medicine is full of agents that mended rodent tissue beautifully and did nothing measurable in humans.
There is also a regulatory and safety dimension specific to BPC-157 that a candid article must include. In 2023 the U.S. FDA placed BPC-157 in the “category 2” interim group of bulk substances that may present significant safety risks for compounding, citing immunogenicity, peptide-related impurity, and insufficient human-safety concerns.11 In April 2026 the FDA removed BPC-157 (along with several other peptides) from that interim list, but it is important to read that move correctly: it was a procedural step tied to withdrawn nominations and a fresh review under the Section 503A framework, not a finding that the compound is safe or effective, and it did not add BPC-157 to the positive list of substances sanctioned for compounding. BPC-157 remained an unapproved, investigational compound, with a Pharmacy Compounding Advisory Committee review scheduled to reconsider it and related peptides. The through-line across both the 2023 restriction and the 2026 procedural reversal is the same: the human safety and efficacy profile is not established — a sharp contrast to the breezy “well tolerated” language of vendor pages. So the fair summary for BPC-157 within KLOW is: strong and interesting preclinical data, a real mechanistic rationale, and a near-total absence of the human efficacy and safety evidence that would justify confidence in the systemic claims made for it.
TB-500 / Thymosin β4: Repair Biology With a Thin Clinical Edge
TB-500 is a synthetic peptide corresponding to the actin-binding region of thymosin β4 (Tβ4), a naturally occurring 43-amino-acid protein present in most cells. Its core biology is well characterized and elegant: Tβ4 is the major intracellular actin-sequestering protein, and when released after injury it “moonlights” extracellularly as a repair signal, promoting cell migration, angiogenesis, and reduced inflammation and scarring.8 In animal models the full protein has shown benefit in dermal wounds, corneal injury, and cardiac repair after infarction, where it can activate epicardial progenitor cells and promote cardiomyocyte survival. This is a legitimate, mechanistically coherent repair story with a real preclinical footprint.
The clinical evidence is more advanced than BPC-157’s but still limited and, crucially, mostly concerns the full-length synthetic protein under pharmaceutical development names (RGN-259 for ophthalmic use, RGN-137 for dermal use) rather than the “TB-500” fragment sold in research blends. The most concrete human data are in dry-eye and ocular-surface disease: Tβ4 eye drops advanced into randomized, placebo-controlled Phase 2 trials that reported improvements in ocular discomfort and corneal staining.9 Dermal wound and cardiac programs have been explored in humans with mixed or preliminary results. But there are two large caveats for KLOW. First, injectable systemic TB-500 as used in research peptide products has not completed large-scale human efficacy trials for musculoskeletal or systemic repair; that use remains investigational and off-label. Second, the material in a blend is a fragment, not the fully studied protein, and the clinical work does not automatically transfer to it. The most useful, honest framing is that TB-500 has better repair biology than most research peptides and a genuine — if narrow — clinical toehold in ophthalmology, but no established evidence for the systemic tendon/ligament/recovery uses for which it is popularly sold. The evidence specifically on TB-500 in tendon and ligament repair is, on close reading, overwhelmingly preclinical.
The cardiac story illustrates the translation gap well. In animal models of myocardial infarction, thymosin β4 activated epicardial progenitor cells, improved cardiomyocyte survival, and promoted new-vessel formation — results striking enough to launch human cardiac programs. Those human efforts have been preliminary and mixed rather than definitively positive, which is the recurring pattern across the whole peptide-repair field: a clean, mechanistically satisfying animal result that becomes murky and inconsistent when tested in people. For the KLOW context specifically, it is worth stressing again that the ophthalmic Phase 2 data — the most solid human evidence in the Tβ4 story — concern eye drops delivering the full protein to the ocular surface.9 Extending that to systemic subcutaneous injection of a fragment, bundled with three other peptides, for tendon or general recovery is not a modest extrapolation; it crosses molecule, route, dose, and indication all at once.
KPV: The Anti-Inflammatory Tripeptide With the Narrowest Human Evidence
KPV is the newest and least-studied addition that distinguishes KLOW from the older GLOW blend. It is a tripeptide — lysine-proline-valine — corresponding to the C-terminal fragment (residues 11–13) of α-melanocyte-stimulating hormone, and its interest lies in a genuinely clever mechanism. Its anti-inflammatory effect appears to be largely independent of the melanocortin receptors and instead depends on the intestinal di/tripeptide transporter PepT1, which actively imports KPV into epithelial and immune cells where it can inhibit NF-κB signaling and dampen production of pro-inflammatory cytokines such as TNF-α, IL-1β, and IL-6.10 Because PepT1 is upregulated in inflamed colon, this offers a plausible route for targeted delivery to inflamed gut tissue.
The evidence base, however, is narrow and almost entirely preclinical. The foundational work showed that orally delivered KPV reduced the severity of DSS- and TNBS-induced colitis in mice through a PepT1-mediated mechanism, with reduced inflammatory infiltrate and improved mucosal integrity.10 A separate group independently confirmed anti-inflammatory activity in DSS and transfer-colitis mouse models, with earlier recovery, better weight regain, and lower colonic myeloperoxidase activity.12 These are real, reproducible mouse findings for gut inflammation. What they are not is human evidence, and they are especially not evidence for the systemic, injected, skin-and-joint applications implied when KPV appears in a “recovery” blend. The strongest KPV data concern oral delivery to the inflamed intestine — a specific route to a specific tissue — which is close to the opposite of the systemic injection context of KLOW. There is no controlled human trial establishing that injected KPV reduces inflammation anywhere in people, and no established human dose.
There is a subtler point buried in the KPV mechanism that undercuts its use in an injected blend. The whole elegance of KPV is that PepT1, its transporter, is enriched in the intestinal epithelium and induced further in inflamed gut — which is precisely why oral delivery targets the peptide to inflamed bowel so neatly. Remove the gut context and you remove the mechanism’s natural advantage. A systemically injected KPV does not obviously arrive at a skin or joint injury through the same targeted, transporter-driven route, so the animal colitis data cannot simply be lifted onto the systemic recovery claims. In other words, KPV’s best evidence is not just preclinical and species-limited; it is also tied to a delivery route and target tissue that KLOW does not use. That is a triple mismatch — species, route, and tissue — layered on top of the absence of any human trial.
The “Angiogenesis and Tissue Repair” Claim, Examined
The most sophisticated argument made for KLOW is mechanistic convergence: several of its components independently touch angiogenesis (the formation of new blood vessels) and tissue repair, so — the argument goes — the blend should be a powerful pro-repair agent. It is worth examining this carefully because it is the strongest case that can be made, and because it illustrates exactly where mechanistic reasoning shades into overreach.
The convergence is partly real. GHK-Cu attracts endothelial and immune cells to injury sites and influences angiogenic growth-factor expression; Tβ4 (the parent of TB-500) is a well-documented promoter of endothelial cell migration and new-vessel formation; BPC-157 has shown angiogenic and vasculo-protective effects in rodents, with proposed involvement of the nitric-oxide and VEGFR2 pathways; and KPV contributes an anti-inflammatory action that could, in principle, create a more favorable healing environment. On paper, these are complementary mechanisms, and this convergence is the honest kernel behind the blend’s design. The site’s own review of the question — what evidence supports KLOW peptides in angiogenesis and tissue repair — lays out these individual pathways in detail.
But three honest qualifications collapse the confident version of the claim. First, every strand of this angiogenesis evidence is preclinical or in-vitro; the mechanisms are demonstrated in cells and animals, not in controlled human trials of these peptides, let alone of the blend. Second, mechanistic convergence in separate experiments is not the same as demonstrated synergy in a shared solution and a shared organism — combining pro-angiogenic agents does not reliably multiply their effect, and uncontrolled angiogenesis is not an unambiguously good thing (the same vessel-forming signals that aid healing are, in other contexts, exactly what tumors exploit, which is why unsupervised pro-angiogenic stimulation is not casually assumed to be safe). Third, and decisively, no one has measured the actual repair or angiogenic output of KLOW in a human being. The convergence argument tells you why someone designed the blend; it does not tell you whether the blend works. Those are different questions, and only the first has an answer.
What the Evidence Does NOT Show
Given how much confident benefit-language surrounds this product, it is worth devoting a full section to the negative space — the things that are frequently implied but are simply not established. This is not cynicism; it is the other half of an honest evidence map, and for an unapproved blend it is arguably the more important half.
It does not show that the blend works. There is no study of KLOW. Every benefit attributed to it is inferred from component data, and the inference has never been validated for the combination. “The ingredients are active” is not “the product works.”
It does not show human efficacy for the systemic claims. For BPC-157, TB-500, and KPV, the evidence for the repair, recovery, and anti-inflammatory benefits most often advertised is preclinical — rodents and cell cultures. None of the three has an adequately powered randomized human trial supporting the systemic injected uses attached to them, and the one component with real human trials, GHK-Cu, has them almost exclusively for topical cosmetic endpoints, some of which were negative.4
It does not show that the components are additive or synergistic. Synergy is a specific, testable claim requiring a factorial experiment (each peptide alone, in combinations, and together). No such experiment exists for KLOW. The blend could be additive, redundant, or antagonistic; the copper in GHK-Cu could plausibly interact with the other peptides in solution. This is unknown, not favorable-by-default.
It does not show a safe, established dose. There is no validated human dosing regimen for the blend, no pharmacokinetic study, and no long-term safety data. Vendor “protocols” are conventions, not evidence-based dosing.
It does not show that it treats, cures, or prevents any disease. KLOW is not approved by any regulator for any medical indication. It cannot honestly be described as a therapy for injury, inflammation, aging skin, gut disease, or anything else. Preclinical activity in a disease model is not evidence of treating the disease.
It does not show route-appropriate evidence. Much of the underlying data uses routes that differ from how KLOW is used: GHK-Cu topically, KPV orally to the gut, Tβ4 as eye drops. Transposing those findings onto systemic subcutaneous injection of a mixture is an assumption, not a finding.
It does not show that “energy” or metabolic benefits are real. Some marketing extends KLOW into vague “energy” and metabolic territory. None of the four peptides has human trial evidence for improving energy or metabolic function, and the mechanistic links invoked are speculative extrapolations from cell and animal work rather than measured clinical outcomes.
The reason to be this explicit is that the internet’s KLOW content is overwhelmingly one-sided, and a reader who absorbs only the benefit claims will badly misjudge the state of the evidence. The truthful summary is that KLOW sits at the intersection of one cosmetically studied peptide and three preclinically studied peptides, combined in an untested way, with zero blend-level human data. It is worth being clear about what this verdict is and is not. It is not a claim that the components are inert or that the underlying mechanisms are fake — several are genuinely interesting and reproducible in their model systems. It is a claim about the burden of proof: extraordinary, comprehensive benefit claims for an injected human product require evidence at the level of controlled human trials, and that evidence does not exist here. The appropriate response to a well-designed-sounding but unproven combination is not enthusiasm and not dismissal, but suspended judgment paired with an accurate description of exactly how thin the human evidence is.
Claimed Versus Evidenced: A Component-by-Component Ledger
The clearest way to hold all of this together is a ledger that places the typical marketing claim next to the actual highest level of evidence for each component. The contrast is the point.
| Component | Typical marketing claim | Highest actual evidence level | Honest verdict |
|---|---|---|---|
| GHK-Cu | Rebuilds collagen, rejuvenates skin, systemic anti-aging repair | Small human topical cosmetic trials (mixed; one laser-resurfacing RCT negative on objective endpoints) plus strong cell/gene data24 | Real cosmetic-topical support; no rigorous evidence for injected systemic medical benefit |
| BPC-157 | Heals tendons, joints, gut; “body protection” | Extensive rat models; no adequately powered human RCT; FDA-flagged safety-risk history (2023 category 2; April 2026 removal procedural, not approval)5711 | Promising preclinical, unproven and safety-unestablished in humans |
| TB-500 | Accelerates recovery, repairs muscle/tendon systemically | Animal repair models; Phase 2 trials of the full Tβ4 protein in dry eye; systemic injectable use investigational89 | Good repair biology; human data narrow and not for the advertised systemic uses |
| KPV | Systemic anti-inflammatory; injury and skin recovery | Mouse colitis models via oral/PepT1 delivery; no human trials1012 | Genuine but narrow preclinical gut data; no human or systemic evidence |
| KLOW (blend) | Comprehensive systemic repair and recovery stack | No studies of any kind — no trial, no PK, no safety data | Entirely unstudied as a combination |
Reading down the “highest actual evidence” column, a pattern is unmistakable: the confident, systemic, human-benefit language of the marketing is nowhere matched by the evidence tier, which is cosmetic-topical at best and rodent-preclinical at worst, and altogether absent for the blend. That mismatch is the honest story of KLOW benefits.
Safety, Sourcing, and the Blend Problem
Safety deserves its own treatment because “natural peptide” framing tends to imply a benign profile that the evidence does not support. Several distinct issues stack up.
Unestablished human safety for the key components. The FDA’s 2023 placement of BPC-157 (and related research peptides) in the interim category of bulk substances that may present significant safety risks was based on gaps in physicochemical characterization, immunogenicity concerns, impurity risks, and a lack of human safety data.11 The FDA removed BPC-157 from that interim list in April 2026, but for procedural reasons (withdrawn nominations and a renewed 503A review) rather than because those data gaps had been filled; the compound stayed unapproved and under active reconsideration. Whatever one thinks of the regulatory process, the underlying point holds: the safety of these compounds in humans is not settled — the opposite of what “well tolerated” vendor copy implies.
The combination is itself an unknown. Even if each peptide were individually characterized, mixing four bioactive molecules — one of them a copper complex — introduces interaction, stability, and immunogenicity questions that no study has addressed. Copper is redox-active; peptides can aggregate or degrade in shared solution; and the immunogenic potential of a four-peptide injectable is entirely uncharacterized. None of this is reassured by the individual-component literature.
Product quality and sourcing. KLOW is sold as a “research use only” product outside any pharmaceutical quality system. Purity, sterility, endotoxin levels, correct peptide content, and accurate labeling all vary by supplier and are frequently not independently verified. Contamination and mislabeling are real, documented problems in the gray-market peptide supply, and they are risks that have nothing to do with the molecules’ intrinsic pharmacology and everything to do with how the material is made and handled.
Population and route mismatch. The scant favorable safety impressions for these peptides come from narrow contexts — topical creams, eye drops, oral gut delivery, short animal studies — and do not license conclusions about repeated systemic injection in humans over time. Absence of documented harm in one setting is not evidence of safety in another.
The measured conclusion is not that KLOW is necessarily dangerous, but that its safety is genuinely unknown, that at least one core component has been formally flagged for safety concerns, and that the blend, the dose, and the sourcing all add further uncharacterized risk. “Unknown safety” and “unknown efficacy” are the honest twin verdicts, and they coexist comfortably.
Handling and Reconstitution in a Research Context
Because KLOW is encountered as a lyophilized powder, a brief and strictly educational note on laboratory handling is appropriate — with the emphasis that this describes standard research-peptide practice, not a usage recommendation, and that KLOW is not an approved therapeutic for any indication. The presence of copper (in GHK-Cu) and the four-peptide composition make careful handling especially relevant, since degradation of any component changes the already-unknown composition being studied.
| Parameter | Typical research-context practice |
|---|---|
| Reconstitution diluent | Sterile or bacteriostatic water, added slowly against the vial wall |
| Mixing | Swirl gently; never shake — agitation and foaming can shear and denature peptides |
| Light and heat | Minimize exposure; both degrade peptides, and copper complexes can be light-sensitive |
| Lyophilized storage | Cool and dark; freezing favored for long-term stability before reconstitution |
| After reconstitution | Refrigerated and used within a limited window; discard if cloudy or discolored |
| Freeze-thaw | Repeated cycles degrade peptides; avoid |
The arithmetic of reconstitution is simply that a fixed mass of powder dissolved in a chosen volume of water sets the concentration — a larger volume yields a more dilute solution — and general walkthroughs of that math appear on the site’s peptide reconstitution guide. It bears repeating that meticulous technique changes nothing about the evidence question. A perfectly reconstituted, high-purity KLOW vial is still a combination with zero blend-level human data. Good handling preserves whatever activity the molecules have; it does not manufacture efficacy where none has been demonstrated.
Regulatory Status
KLOW’s regulatory picture is unambiguous in the ways that matter and murky in the ways that vendors exploit. No regulator — not the U.S. FDA, not the European Medicines Agency, nor any comparable authority — has approved KLOW, or any of its individual peptides, as a drug for the treatment, cure, or prevention of any disease. GHK-Cu’s legitimate regulatory home is as a cosmetic ingredient, a category that governs topical appearance claims, not medical efficacy. BPC-157, TB-500, and KPV are sold as “research use only” chemicals, a designation that explicitly means they are not for human use and carries no assurance of safety or efficacy.
In the United States, the compounding pathway tells the clearest story. In 2023 BPC-157 and a group of related research peptides were placed by the FDA into the interim “category 2” list of bulk drug substances that may present significant safety risks — a status reflecting immunogenicity, impurity, and human-safety concerns rather than a clean bill of health.11 In April 2026 the FDA removed BPC-157 and several other peptides from that interim list on procedural grounds (withdrawn nominations and a fresh 503A review), with a Pharmacy Compounding Advisory Committee scheduled to reconsider BPC-157, KPV, and TB-500 among others. Critically, removal from the “significant safety risks” list is not the same as addition to the positive list of sanctioned bulk substances, and it is emphatically not drug approval. The through-line is consistent: none of KLOW’s peptides has achieved recognized approval or a settled, sanctioned place in the compounding framework, and the blend as a product exists entirely outside regulated medicine. A recurring marketing sleight-of-hand deserves naming: pointing to a component’s cosmetic use, or to preclinical publications, as though either constituted medical validation. Cosmetic status speaks only to topical safety at defined exposure; a preclinical paper speaks only to a model system. Neither is drug approval, and neither should be read as one.
The synthesis is straightforward. KLOW is an unapproved, unstudied research blend of four peptides with sharply different evidence profiles, none of them approved as a medicine, one of them formally flagged for safety concerns, and the combination itself never tested in any human or controlled setting. Any legitimate exploration of these compounds belongs in properly authorized preclinical or clinical research under oversight, not in self-directed use. For readers tracking how the evidence base for these blends and their components develops, the site’s peptide glossary and its running coverage of what studies reveal about KLOW peptides follow the primary literature as it appears.
Frequently Asked Questions
Is there any clinical trial of the KLOW blend itself?
No. There is no clinical trial, no controlled preclinical study, and no published pharmacokinetic characterization of the KLOW combination. Every benefit attributed to KLOW is extrapolated from data on its four individual components — often generated in animals or in cell cultures, and often using a different route of administration than the injected blend. The combination as a product has never been formally studied, which means claims about “KLOW benefits” are inferences, not findings.
Which KLOW component has the strongest evidence?
GHK-Cu, but with an important qualifier: its strongest human evidence is topical and cosmetic, and even there the results are mixed — a controlled trial on laser-resurfaced skin found no significant objective improvement in wrinkles or redness.4 Its cell-biology and gene-expression data are genuinely substantial.2 But that evidence supports topical skin appearance, not the systemic injected medical benefits implied for the blend.
Does KLOW heal injuries, tendons, or joints?
There is no human evidence that it does. The injury- and tendon-healing reputation comes mainly from BPC-157 and TB-500, whose relevant data are overwhelmingly preclinical — rodent and cell-culture models.57 Neither has an adequately powered randomized human trial for the systemic musculoskeletal uses advertised. Animal healing results are optimistic predictors that frequently fail to translate to humans.
What about the anti-inflammatory claims from KPV?
KPV has genuine but narrow evidence: it reduced colitis severity in mice through a PepT1-transporter, NF-κB–inhibiting mechanism, confirmed by more than one group.1012 Crucially, that work used oral delivery targeting the inflamed gut, which is close to the opposite of systemic injection. There is no human trial of KPV, and no evidence it reduces inflammation systemically in people when injected.
Are the four peptides proven to work better together?
No. Synergy is a specific, testable claim that would require a factorial experiment comparing each peptide alone, in pairs, and all together. No such study exists for KLOW. The components could be additive, redundant, or even antagonistic, and the copper in GHK-Cu raises unstudied questions about chemical interactions in the shared solution. “Convergent mechanisms” explains why someone designed the blend; it does not demonstrate that the blend works.
Is KLOW approved or safe?
It is not approved by the FDA, EMA, or any comparable regulator for any indication. Its peptides are sold “research use only,” and in 2023 BPC-157 was formally placed by the FDA into an interim category of bulk substances flagged for significant safety risks, citing immunogenicity, impurities, and a lack of human safety data; an April 2026 removal from that list was procedural (withdrawn nominations and a fresh 503A review) rather than a safety clearance, and the compound stayed unapproved and under regulatory review.11 Add the unknown safety of the untested four-peptide combination and the variable quality of gray-market sourcing, and the honest verdict is that KLOW’s safety is genuinely unestablished.
Why does so much online content sound so confident about KLOW?
Because most of it is marketing, and marketing borrows the reputation of the individual ingredients while omitting the caveats — the preclinical-only status, the negative trials, the route mismatches, and the complete absence of blend-level data. When a page says KLOW “accelerates repair,” the accurate translation is that one of its peptides showed a repair-related effect in a model system, and the claim is being transferred, untested, to a human-injected mixture.
How is KLOW handled in a research setting?
As a lyophilized powder, it is reconstituted with sterile or bacteriostatic water using gentle technique (swirl, never shake), kept cool and dark, protected from freeze-thaw cycles, and used within a limited window after reconstitution — standard research-peptide practice. Handling quality preserves whatever activity the molecules have but has no bearing whatsoever on the absence of efficacy or safety data for the blend.
What would it take to actually establish KLOW’s benefits?
An entirely new research program: characterization of the blend’s stability and pharmacokinetics, controlled animal studies of the combination with appropriate endpoints, factorial experiments to test for genuine synergy, and eventually adequately powered, randomized, placebo-controlled human trials with predefined outcomes and safety monitoring — conducted under regulatory oversight. Until that work exists, any statement about KLOW benefits is hypothesis, not finding.
References
- BioLongevity Labs. KLOW Peptide Blend (GHK-Cu, BPC-157, TB-500, KPV) product specification (80 mg vial composition). 2026. https://biolongevitylabs.com/product/klow-blend-ghk-cu-bpc-157-tb-500-kpv/
- Pickart L, Vasquez-Soltero JM, Margolina A. GHK Peptide as a Natural Modulator of Multiple Cellular Pathways in Skin Regeneration. Biomed Res Int. 2015;2015:648108. PMCID: PMC4508379. https://pmc.ncbi.nlm.nih.gov/articles/PMC4508379/
- Pickart L, Margolina A. Regenerative and Protective Actions of the GHK-Cu Peptide in the Light of the New Gene Data. Int J Mol Sci. 2018;19(7):1987. PMID: 29986520. PMCID: PMC6073405. https://pmc.ncbi.nlm.nih.gov/articles/PMC6073405/
- Miller TR, Wagner JD, Baack BR, Eisbach KJ. Effects of topical copper tripeptide complex on CO2 laser-resurfaced skin. Arch Facial Plast Surg. 2006;8(4):252-259. PMID: 16847171. https://pubmed.ncbi.nlm.nih.gov/16847171/
- Staresinic M, Sebecic B, Patrlj L, et al. Gastric pentadecapeptide BPC 157 accelerates healing of transected rat Achilles tendon and in vitro stimulates tendocytes growth. J Orthop Res. 2003;21(6):976-983. PMID: 14554208. https://pubmed.ncbi.nlm.nih.gov/14554208/
- Chang CH, Tsai WC, Lin MS, Hsu YH, Pang JS. The promoting effect of pentadecapeptide BPC 157 on tendon healing involves tendon outgrowth, cell survival, and cell migration. J Appl Physiol. 2011;110(3):774-780. PMID: 21030672. https://pubmed.ncbi.nlm.nih.gov/21030672/
- Regeneration or Risk? A Narrative Review of BPC-157 for Musculoskeletal Healing. PMC. 2025. PMCID: PMC12446177. https://pmc.ncbi.nlm.nih.gov/articles/PMC12446177/
- Goldstein AL, Hannappel E, Kleinman HK. Thymosin beta4: actin-sequestering protein moonlights to repair injured tissues. Trends Mol Med. 2005;11(9):421-429. PMID: 16099219. https://pubmed.ncbi.nlm.nih.gov/16099219/
- Safety and Efficacy of Thymosin Beta 4 Ophthalmic Solution (RGN-259) in Patients With Dry Eye. ClinicalTrials.gov identifier NCT01387347. https://clinicaltrials.gov/study/NCT01387347
- Dalmasso G, Charrier-Hisamuddin L, Nguyen HTT, et al. PepT1-mediated tripeptide KPV uptake reduces intestinal inflammation. Gastroenterology. 2008;134(1):166-178. PMCID: PMC2431115. https://pmc.ncbi.nlm.nih.gov/articles/PMC2431115/
- U.S. Food and Drug Administration. Certain Bulk Drug Substances for Use in Compounding That May Present Significant Safety Risks (interim category 2 list on which BPC-157 and related peptides were placed in 2023; BPC-157 removed on procedural grounds in April 2026, pending Pharmacy Compounding Advisory Committee reconsideration — removal is not FDA approval). https://www.fda.gov/drugs/human-drug-compounding/certain-bulk-drug-substances-use-compounding-may-present-significant-safety-risks
- Kannengiesser K, Maaser C, Heidemann J, et al. Melanocortin-derived tripeptide KPV has anti-inflammatory potential in murine models of inflammatory bowel disease. Inflamm Bowel Dis. 2008;14(3):324-331. PMID: 18092346. https://pubmed.ncbi.nlm.nih.gov/18092346/
- Pickart L, Vasquez-Soltero JM, Margolina A. The human tripeptide GHK-Cu in prevention of oxidative stress and degenerative conditions of aging. Oxid Med Cell Longev. 2012;2012:324832. PMID: 22666519. https://pubmed.ncbi.nlm.nih.gov/22666519/
Educational and research-use disclaimer: This article is provided solely for scientific and educational purposes. KLOW is an unapproved research blend and is not approved by the FDA, EMA, or any comparable regulator for the treatment, cure, or prevention of any disease. No human efficacy or safety trial of the KLOW combination exists, and the evidence for its individual components ranges from cosmetic-topical (GHK-Cu) to preclinical and animal-only (BPC-157, TB-500, KPV). Nothing here is medical advice or a recommendation for human use. Its peptides are sold for research use only, and BPC-157 — though removed from the FDA’s interim category-2 compounding list on procedural grounds in April 2026 — was flagged over significant safety concerns and remains unapproved and under regulatory review. Any legitimate investigation of these compounds should occur within properly authorized preclinical or clinical research under appropriate oversight. Readers should consult qualified professionals and applicable regulations before making any decisions.