The question in the title carries a quiet assumption worth pausing over before we accept it: that tirzepatide “improves fat loss and insulin sensitivity” as settled, demonstrated fact. For most compounds discussed on this site, that framing would be a red flag — a premise inflated well beyond the evidence. Tirzepatide is the unusual case where the premise is, broadly, supported. It is a dual glucose-dependent insulinotropic polypeptide (GIP) and glucagon-like peptide-1 (GLP-1) receptor agonist that the U.S. Food and Drug Administration approved as Mounjaro for type 2 diabetes in May 2022 and as Zepbound for chronic weight management in November 2023, on the strength of large, randomized, placebo- and active-comparator-controlled trials.12 Within those approved indications, it produces some of the largest reductions in body weight and the clearest improvements in glycemic control and insulin sensitivity of any pharmacological agent studied to date.
So this article does not have to debunk the premise. But it does have to discipline it. “Improves fat loss and insulin sensitivity in clinical research” is true in a specific, bounded sense, and the honest job here is to draw those boundaries precisely: in whom, by how much, through what mechanisms, with what caveats, and — crucially — how much of the insulin-sensitivity benefit is a direct pharmacological effect versus a downstream consequence of weight loss itself. That last distinction is where a great deal of loose writing goes wrong, implying a direct insulin-sensitizing action that the data only partly support.
There is also a temptation, whenever a drug performs this well, to let enthusiasm outrun the evidence: to imply it “reverses” diabetes, that the weight loss is durable without continued treatment, or that the fat lost is exclusively adipose tissue with lean mass spared. None of those stronger claims survives contact with the trial data. Tirzepatide’s benefits are real and large; they are also conditional, dose-dependent, accompanied by meaningful loss of lean mass alongside fat, and substantially reversed when treatment stops.7 This piece is written for researchers and educated readers who want the actual shape of the evidence — the pivotal trials, the mechanisms, the effect sizes, and the limits — rather than either hype or reflexive skepticism. Readers wanting an orientation to the compound itself may find the site’s overview of what tirzepatide is and how it works a useful companion.
What Tirzepatide Is: A Single Molecule, Two Incretin Receptors
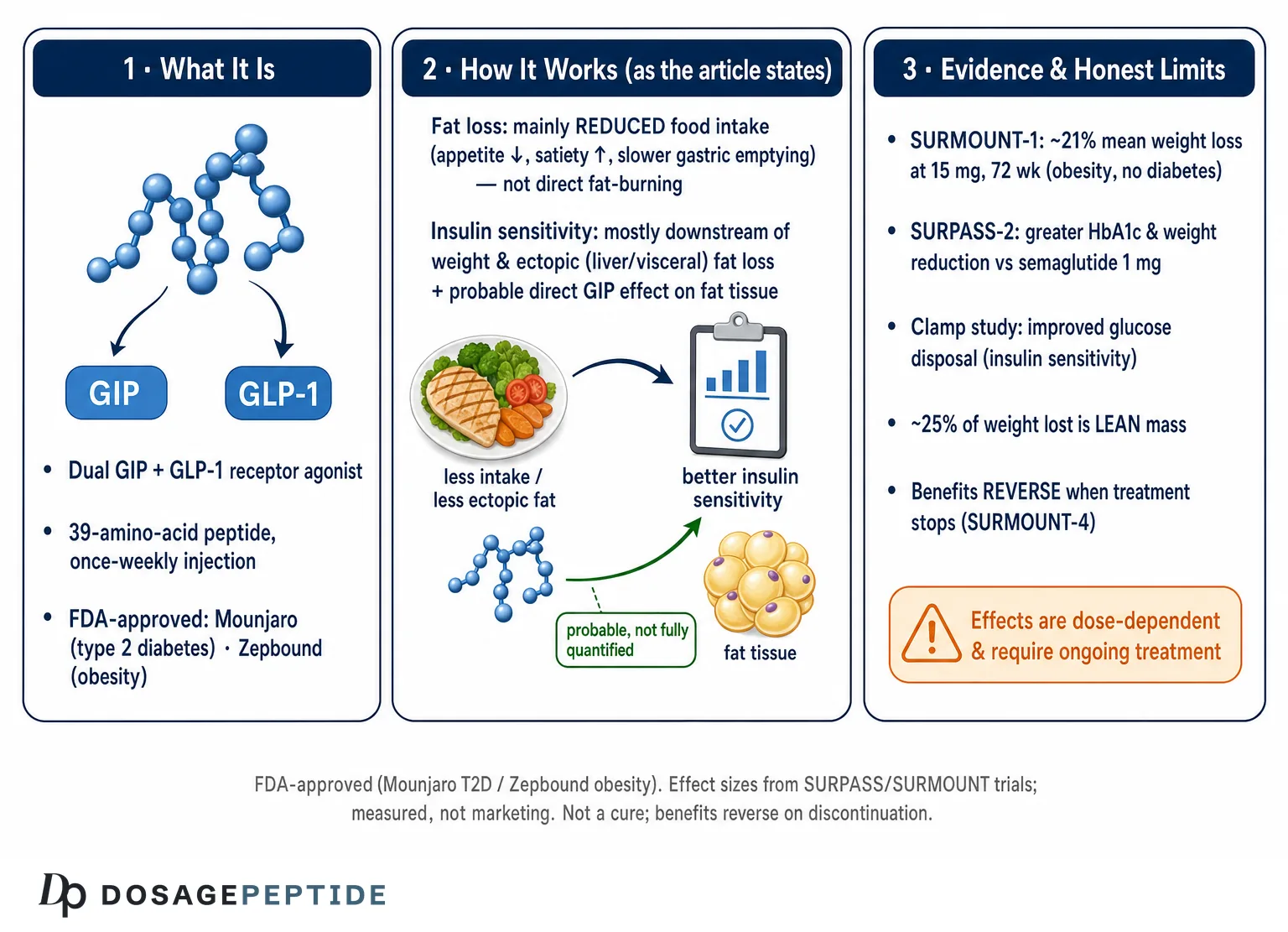
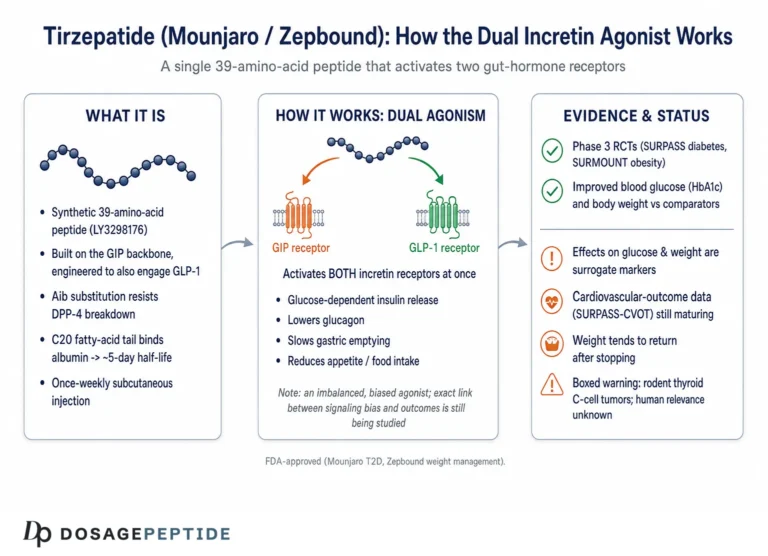
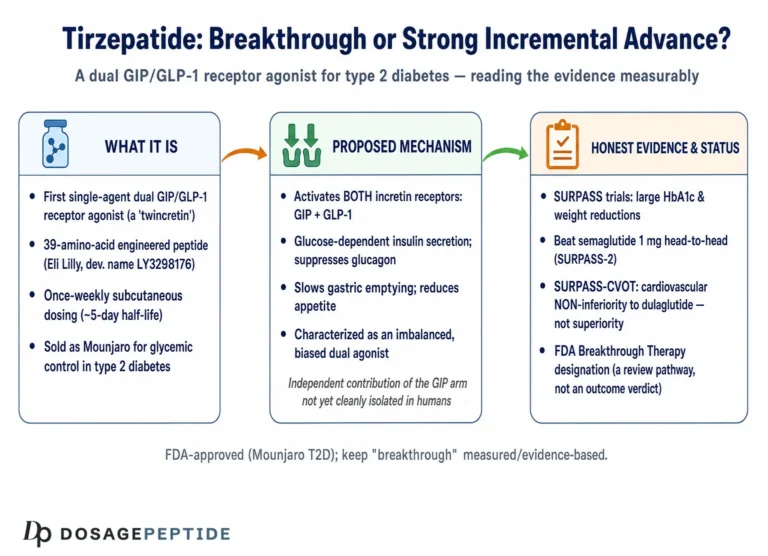
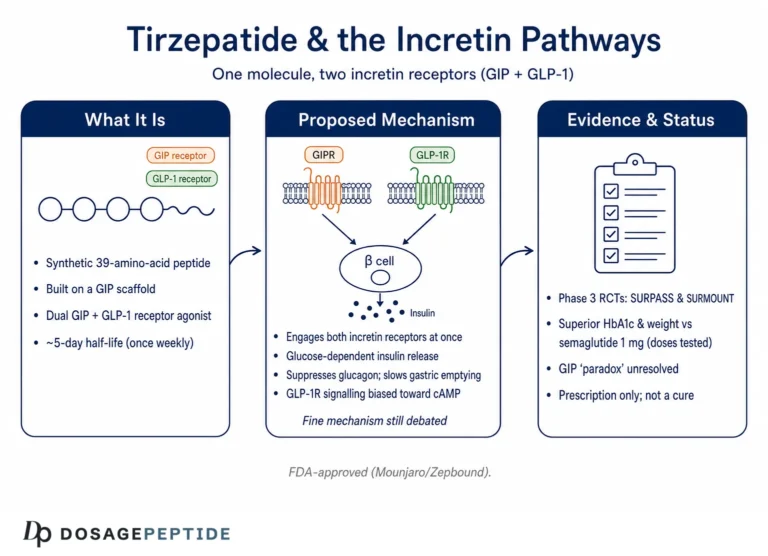
Tirzepatide (development code LY3298176) is a synthetic 39-amino-acid peptide engineered to activate two distinct incretin receptors at once: the GIP receptor and the GLP-1 receptor.3 Incretins are gut hormones released after eating that amplify insulin secretion in a glucose-dependent manner — they help the pancreas respond proportionately to a meal. GLP-1 receptor agonists such as semaglutide had already established that pharmacologically sustaining one incretin signal produces weight loss and glycemic improvement. Tirzepatide’s design premise was that adding GIP-receptor activity to GLP-1-receptor activity in a single molecule might do more than either alone.
The molecule is built on a modified GIP peptide backbone with a C20 fatty-diacid moiety attached, which binds albumin and slows clearance enough to permit once-weekly subcutaneous dosing.3 Its receptor pharmacology is deliberately lopsided. In the original discovery work, tirzepatide bound the GIP receptor with an affinity comparable to native GIP, but bound the GLP-1 receptor with roughly five-fold weaker affinity than native GLP-1.3 For this reason it is often described as an “imbalanced” or “biased” dual agonist — not a symmetric co-activation of both pathways, but a GIP-favoring molecule with tempered GLP-1 activity. That imbalance is not a footnote; it is central to ongoing debate about why tirzepatide outperforms pure GLP-1 agonists, a question we return to below because the honest answer is that it is not fully resolved.
It helps to keep three levels distinct when reasoning about this compound, because popular writing routinely collapses them. First, there is the molecular pharmacology: what tirzepatide does at each receptor in vitro. Second, there is the integrated physiology: how those receptor actions translate into effects on appetite, gastric emptying, insulin secretion, and fat and glucose handling in a living organism. Third, there is the clinical outcome: what happens to weight, HbA1c, and insulin-sensitivity markers in actual trials. A mechanism demonstrated at level one does not automatically explain an outcome at level three, and much of the confident causal storytelling around tirzepatide skips the middle level entirely. For a deeper look at the incretin biology underpinning all of this, the site’s discussion of how tirzepatide influences incretin pathways unpacks the receptor signaling in more detail.
Regulatory Status: What Tirzepatide Is Actually Approved For
Because tirzepatide’s evidence base is unusually strong, it is important to state precisely what regulators have and have not sanctioned, so that legitimate approved uses are not blurred into unproven ones.
Tirzepatide is marketed under two brand names for two distinct indications. As Mounjaro, it was approved by the FDA in May 2022 as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes.1 As Zepbound, it was approved in November 2023 for chronic weight management in adults with obesity (body mass index ≥30) or overweight (BMI ≥27) with at least one weight-related comorbidity, again as an adjunct to reduced-calorie diet and increased physical activity.2 In late 2024, Zepbound also received approval for moderate-to-severe obstructive sleep apnea in adults with obesity. These are the approved uses; both are supported by dedicated pivotal trials.
What tirzepatide is not approved to do is equally important. It is not approved for type 1 diabetes, not approved for cosmetic weight loss in people without obesity or a qualifying comorbidity, and not approved as a “metabolic optimizer” for otherwise healthy adults. The phrase “improves insulin sensitivity” is a description of a measurable pharmacodynamic effect within the studied populations — not a standalone approved indication, and not a license to treat insulin resistance as a disease target in people outside the trial criteria. Much of the peptide sold outside regulated pharmacy channels as “research tirzepatide” is of unverified purity and is not the FDA-approved product; provenance and quality are real and separate concerns from the pharmacology discussed here.
The distinction between an approved indication and a demonstrated pharmacodynamic effect is worth dwelling on, because it is the exact seam where legitimate science gets stretched into marketing. Regulators approve a drug for a disease and a population after weighing benefit against risk in adequate trials. They do not approve individual mechanisms. So the fact that tirzepatide measurably improves insulin sensitivity does not mean it is sanctioned — or wise — to take it purely to improve insulin sensitivity in someone who does not meet the criteria for diabetes or obesity treatment. The risk-benefit calculus that justifies the drug in a person with a BMI of 35 and type 2 diabetes is simply not the same calculus for a metabolically healthy person seeking marginal optimization, and the trials provide no data on the latter. Honest communication keeps “the drug does X to physiology” firmly separated from “the drug is approved and appropriate for person Y,” because conflating them is how a legitimate therapy becomes an unregulated lifestyle product.
How Tirzepatide Drives Fat Loss: The Mechanistic Story
The dominant, best-supported mechanism by which tirzepatide reduces fat mass is not a direct “fat-burning” action on adipocytes. It is a reduction in energy intake driven by central and gastrointestinal effects on appetite and satiety.311 Both GLP-1 and GIP receptors are expressed in brain regions that regulate appetite, including the hypothalamus and hindbrain. Agonism at these receptors reduces hunger, increases satiety, slows gastric emptying, and lowers overall caloric consumption. The resulting energy deficit is what mobilizes stored fat — the same fundamental route by which any effective weight-loss intervention works, but pharmacologically sustained in a way that lifestyle change alone rarely achieves.
This matters for honest framing. Tirzepatide does not conjure fat loss out of nowhere or override the energy balance equation; it shifts appetite and intake so that a person eats substantially less without the compensatory hunger that normally sabotages caloric restriction. Describing it as making the body “burn fat” misplaces the primary action. The fat oxidation that follows is downstream of eating less, not a direct lipolytic command to fat cells.
The GIP component adds a genuinely interesting and still-debated layer. GIP receptor signaling appears to have direct effects on adipose tissue, including the enhancement of insulin-stimulated glucose uptake into fat cells and modulation of adipocyte nutrient handling and lipid buffering.13 The theory is that healthier, more insulin-responsive adipose tissue can store lipid appropriately rather than spilling it into liver and muscle, which in turn improves whole-body metabolism. There is mechanistic and preclinical support for GIP receptor agonism improving adipose insulin sensitivity and lipid metabolism.13 But how much of tirzepatide’s clinical fat loss is attributable specifically to this adipocyte-level GIP action, versus to the central appetite effects shared with GLP-1, remains an open question rather than a settled one.
A useful discipline here is to separate the quantity question (how much fat is lost) from the mechanism question (through what pathway). The quantity is well documented by trials. The mechanistic partitioning — how much central appetite suppression versus peripheral adipose effects versus altered energy expenditure — is far less resolved, and any source that assigns confident percentages to each pathway is overstating what the data show.
The energy-expenditure question deserves its own note of caution because it is a frequent site of overclaiming. It is sometimes asserted that tirzepatide “boosts metabolism” and raises the number of calories the body burns at rest. The reality is more nuanced. During active weight loss, resting energy expenditure typically falls as body mass falls — this is the well-known metabolic adaptation that makes sustained weight loss difficult with any method. Whether tirzepatide blunts this adaptation, leaves resting expenditure appropriate for the new lower body size, or has some modest independent thermogenic effect via GIP-mediated actions is not firmly established in humans, and preclinical signals do not translate cleanly to clinical energy-expenditure outcomes. The safe conclusion is that the dominant driver of fat loss is reduced intake, and that any contribution from increased expenditure is, at most, secondary and not well quantified.
It is also worth being precise about what “appetite suppression” means physiologically, because the phrase can sound like a blunt override of hunger. What the incretin receptors appear to do is shift the homeostatic and hedonic set points that govern eating: participants report reduced hunger, earlier and stronger satiety during meals, diminished preoccupation with food, and in some cases reduced reward-driven eating. Slowed gastric emptying contributes to the sense of fullness, especially early in treatment, though this effect tends to attenuate over time as the gut adapts. The net result is a spontaneous, sustained reduction in caloric intake that does not depend on conscious willpower to the same degree that unaided dieting does — which is precisely why the weight loss is larger and more durable during treatment than lifestyle change typically achieves. None of this changes the underlying arithmetic of energy balance; it changes the ease with which a person maintains a deficit.
The Fat-Loss Evidence: SURMOUNT and SURPASS
Tirzepatide’s weight-reduction evidence is among the strongest for any anti-obesity pharmacotherapy, and it is worth quoting the pivotal numbers precisely rather than in the rounded, inflated form that circulates online.
The landmark obesity trial is SURMOUNT-1, a 72-week, randomized, double-blind, placebo-controlled study of 2,539 adults with obesity or overweight without diabetes.2 At the maximum 15 mg weekly dose, mean weight reduction from baseline was 20.9% (some analyses cite up to 22.5% in completers), compared with roughly 3.1% for placebo; the 5 mg and 10 mg doses produced approximately 15% and 19.5% reductions respectively.2 More than half of participants on the higher doses lost at least 20% of their body weight — a magnitude previously associated mainly with bariatric surgery. Waist circumference, blood pressure, and lipid and glycemic markers all improved alongside weight.
In people with type 2 diabetes, weight loss is characteristically more modest, and the trials reflect this. In SURPASS-2, a 40-week head-to-head against semaglutide 1 mg on a background of metformin in 1,879 participants, tirzepatide 15 mg reduced body weight by about 11.2 kg versus 5.7 kg with semaglutide, alongside superior HbA1c reduction.4 The gap between the diabetic and non-diabetic populations is a consistent and honest caveat: the headline “20%+” figures come from people without diabetes, and quoting them as generic is misleading.
| Trial | Population | Duration | Top-dose weight change | Comparator |
|---|---|---|---|---|
| SURMOUNT-12 | Obesity/overweight, no diabetes (n=2,539) | 72 wk | −20.9% (15 mg) | −3.1% placebo |
| SURPASS-24 | Type 2 diabetes on metformin (n=1,879) | 40 wk | −11.2 kg (15 mg) | −5.7 kg semaglutide 1 mg |
| SURMOUNT-210 | Obesity + type 2 diabetes (n=938) | 72 wk | −14.7% (15 mg) | −3.2% placebo |
| SURPASS-3 MRI5 | Type 2 diabetes (MRI substudy, n=296) | 52 wk | Liver fat −8.09% (pooled 10/15 mg) | −3.38% insulin degludec |
Two honest observations follow from this table. First, the effect sizes are genuinely large and consistent across independent trials and populations — this is not a fragile or cherry-picked signal. Second, the magnitude depends heavily on population and dose: obesity without diabetes yields the largest percentages, diabetes yields less, and the numbers are top-dose figures that not every participant tolerated or reached. Readers wanting the fuller trial-by-trial picture can consult the site’s summary of how effective tirzepatide is according to recent clinical studies.
Body Composition: Fat Loss Is Not the Whole Story
A frequent and important omission in casual coverage is the composition of the weight lost. It is not pure fat. Rapid, large-magnitude weight loss from any modality — diet, surgery, or incretin pharmacotherapy — carries away lean mass alongside adipose tissue, and tirzepatide is no exception.
The clearest data come from a dual-energy X-ray absorptiometry (DXA) substudy of SURMOUNT-1, in which 160 participants were scanned at baseline and week 72.6 With tirzepatide, total body weight fell by about 21.3%, fat mass by 33.9%, and lean mass by 10.9%; the placebo group lost 5.3% weight, 8.2% fat, and 2.6% lean mass.6 Expressed as a proportion, roughly 75% of the weight lost was fat and about 25% was lean mass — a ratio that, notably, was similar between the drug and placebo groups, suggesting the fat-to-lean loss ratio reflects the physiology of weight loss itself rather than a drug-specific catabolic effect.
| Compartment (SURMOUNT-1 DXA substudy, wk 72) | Tirzepatide (pooled) | Placebo |
|---|---|---|
| Total body weight | −21.3% | −5.3% |
| Fat mass | −33.9% | −8.2% |
| Lean mass | −10.9% | −2.6% |
| Approx. fat : lean ratio of loss | ~75% : 25% | ~75% : 25% |
How should this be read? The reassuring interpretation is that the proportion of lean loss is broadly in line with what non-pharmacological weight loss produces, and that overall body composition — fat as a fraction of total mass — improves. The cautious interpretation is that a 10.9% absolute reduction in lean mass is not trivial, particularly in older adults for whom muscle preservation bears directly on function and metabolic health, and that trials measure lean mass by DXA rather than muscle strength or physical performance. The site’s discussion of whether the evidence supports tirzepatide as a breakthrough therapy touches on where such caveats fit into the overall risk-benefit picture. The honest summary is that tirzepatide reduces fat mass substantially and improves body composition on balance, while also reducing lean mass to a degree that resistance exercise and adequate protein intake are widely recommended to mitigate — a mitigation strategy, it should be noted, that has not been rigorously tested in combination with the drug in the pivotal trials.
How Tirzepatide Improves Insulin Sensitivity: Direct and Indirect Routes
Insulin sensitivity — the efficiency with which a given amount of insulin lowers blood glucose by driving uptake into muscle, fat, and liver — improves substantially with tirzepatide. But the mechanism is a genuine mixture of direct pharmacological effects and indirect consequences of weight and ectopic-fat loss, and separating the two is where careful reading pays off.
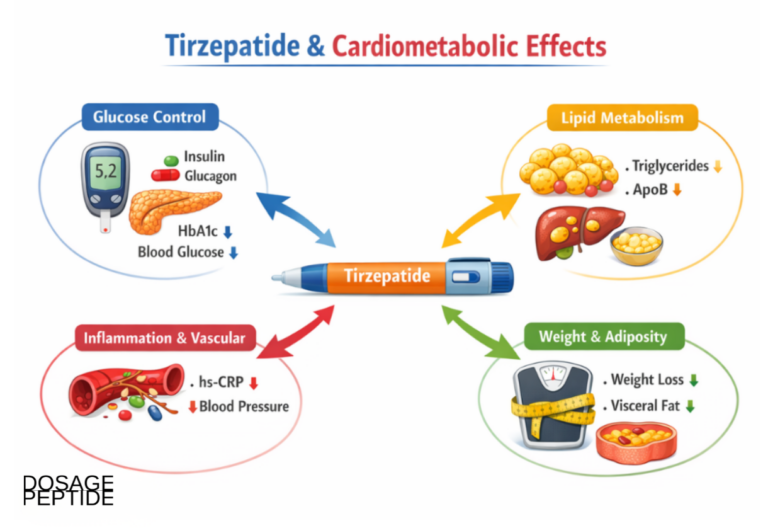
The indirect route is the larger and less controversial contributor. Insulin resistance in type 2 diabetes and obesity is driven substantially by excess adiposity, especially visceral fat and ectopic lipid deposited in the liver and skeletal muscle. When tirzepatide reduces total fat, visceral fat, and liver fat, it removes major drivers of insulin resistance almost mechanically. The SURPASS-3 MRI substudy demonstrated this directly: tirzepatide markedly reduced liver fat content and both visceral and subcutaneous abdominal adipose tissue, whereas the insulin comparator increased them.5 Less ectopic fat means less lipotoxic interference with insulin signaling in the tissues that matter, and therefore better insulin sensitivity — a benefit that would accrue, in principle, to any intervention achieving comparable fat loss.
The direct route is more subtle and is where the GIP component is invoked. Beyond weight loss, GIP receptor agonism may improve adipose-tissue insulin sensitivity and lipid buffering directly, helping fat tissue act as a proper metabolic sink rather than an inflamed, insulin-resistant source of circulating lipids.13 There is also the glucose-dependent enhancement of insulin secretion — an effect on the beta cell rather than on peripheral sensitivity per se, but one that improves overall glucose handling. Mechanistic clamp work suggests tirzepatide improves both insulin secretion and insulin sensitivity, and the two together produce a large improvement in the “disposition index,” a composite of secretion and sensitivity.8 Even as monotherapy in early type 2 diabetes, tirzepatide improved fasting-derived markers of both beta-cell function and insulin sensitivity relative to placebo in the SURPASS-1 program.9
It is worth being specific about which tissues become more insulin-sensitive, because “insulin sensitivity” is not a single number but a composite of effects in liver, skeletal muscle, and adipose tissue. Hepatic insulin sensitivity improves as liver fat falls: a fatty liver over-produces glucose and resists insulin’s suppression of that output, so de-fatting the liver restores appropriate glucose regulation. Skeletal-muscle insulin sensitivity — the largest sink for post-meal glucose — improves as intramuscular lipid decreases and as overall metabolic load lightens. Adipose insulin sensitivity is where the direct GIP hypothesis is most relevant: healthier fat tissue suppresses lipolysis appropriately in response to insulin and buffers dietary lipid rather than releasing a damaging flux of free fatty acids into the circulation.13 The clamp studies measure whole-body disposal, which is dominated by muscle, so they capture the muscle and, indirectly, the systemic picture, but they do not neatly isolate the adipose-specific contribution.
The intellectually honest position, and the one supported by careful reviews, is that tirzepatide’s insulin-sensitivity benefit is predominantly mediated by weight and ectopic-fat loss, with a probable but harder-to-quantify direct component attributable to incretin signaling and especially to GIP effects on adipose tissue.11 Claims that tirzepatide is a powerful direct insulin sensitizer independent of weight loss overreach the evidence; claims that the benefit is purely a weight-loss artifact probably understate the direct incretin contribution. The truth sits, as it often does, in the messier middle. A clean experimental resolution would require comparing tirzepatide against a matched degree of weight loss achieved by other means — a difficult study to run — and until such data exist, the partitioning remains an informed estimate rather than a measured fact.
The Insulin-Sensitivity Evidence: Clamps, HOMA, and Ectopic Fat
Two complementary bodies of evidence quantify the insulin-sensitivity effect: gold-standard clamp studies and trial-embedded surrogate markers such as HOMA-IR.
The most rigorous evidence comes from a phase 1 mechanistic study by Heise and colleagues, which used the hyperinsulinemic-euglycemic clamp — the reference method for measuring insulin sensitivity — in adults with type 2 diabetes.8 After 28 weeks, tirzepatide 15 mg produced a substantial increase in the clamp-derived glucose disposal rate (M-value), indicating markedly improved insulin sensitivity, along with improved beta-cell function; the combined effect drove a large increase in the clamp disposition index relative to placebo and to semaglutide.8 Because a clamp measures insulin action directly and independently of the confounds that plague fasting surrogates, this is the strongest single piece of evidence that tirzepatide improves insulin sensitivity — though even here, the 28-week timeframe means weight loss had already occurred and cannot be fully disentangled from any direct effect.
Trial-embedded surrogate data reinforce the picture. In analyses derived from SURPASS-2, tirzepatide across its dose range reduced HOMA2-IR (a fasting insulin-resistance index) by roughly 15.5% to 24.0%, compared with about 5.1% for semaglutide 1 mg, alongside greater improvements in markers of beta-cell function.12 Fasting insulin, fasting glucagon, and C-peptide also moved in favorable directions.12 Similar directional improvements in insulin-sensitivity and beta-cell markers were seen in post hoc analyses extending to people with obesity and prediabetes or normoglycemia in SURMOUNT-1.2
| Measure | Method | Tirzepatide effect | Comparator |
|---|---|---|---|
| Glucose disposal (M-value)8 | Hyperinsulinemic-euglycemic clamp, 28 wk | Substantial increase (15 mg) | > placebo and > semaglutide |
| HOMA2-IR12 | Fasting surrogate, SURPASS-2 | −15.5% to −24.0% | −5.1% semaglutide 1 mg |
| Liver fat content5 | MRI, SURPASS-3, 52 wk | −8.09% (pooled 10/15 mg) | −3.38% insulin degludec |
| Beta-cell function (HOMA2-B)12 | Fasting surrogate, SURPASS-2 | Greater increase vs comparator | Semaglutide 1 mg |
A necessary caveat about surrogates: HOMA-IR and HOMA-B are fasting-state estimates and are influenced by concurrent changes in weight, glucose, and insulin. They are useful for showing direction and rough magnitude but are not equivalent to a clamp. The convergence of clamp data and surrogate data pointing the same way is what makes the insulin-sensitivity conclusion robust; neither alone would be decisive. It is also worth noting that these are effects on markers and physiology — improved insulin sensitivity is a mechanism and an intermediate outcome, not itself a hard clinical endpoint like cardiovascular events, which are being evaluated in dedicated outcome trials that were still maturing as of this writing.
The GIP Question: Does the Second Receptor Actually Earn Its Keep?
One of the most scientifically interesting and least resolved questions about tirzepatide is why it outperforms selective GLP-1 receptor agonists. The intuitive answer — “because it hits a second receptor, GIP” — is plausible but not fully proven, and it deserves an honest airing precisely because it is so often stated as settled.
The puzzle is that GIP biology is genuinely paradoxical. In native physiology, GIP is often associated with fat storage, and in type 2 diabetes the beta cell can become relatively resistant to GIP’s insulinotropic action. Historically, some researchers argued that GIP receptor antagonism, not agonism, might be metabolically beneficial. Yet tirzepatide, a GIP receptor agonist, produces superior outcomes. Several explanations have been proposed: that sustained pharmacological GIP agonism resensitizes or biases GIP signaling in a favorable way; that GIP agonism improves adipose-tissue insulin sensitivity and lipid buffering, complementing GLP-1’s central appetite effects; that GIP acts centrally to potentiate GLP-1’s satiety signal or to reduce nausea, allowing more effective net dosing; or that tirzepatide’s specific “biased” signaling profile at the GLP-1 receptor contributes independently of GIP.313
What can be said honestly is that head-to-head clinical superiority over semaglutide is established (SURPASS-2), and that mechanistic and preclinical work supports meaningful metabolic contributions from GIP receptor agonism, particularly in adipose tissue.413 What cannot yet be said with confidence is a clean, quantified attribution of tirzepatide’s clinical advantage to GIP agonism specifically, as opposed to differences in GLP-1 receptor pharmacology, dosing, or exposure. This is an active area of investigation, and readers should be wary of sources that present the GIP explanation as a closed case. For a broader view of how such dual- and triple-agonist strategies are evolving, the site’s coverage of retatrutide and the triple-receptor approach shows where the field is heading next.
Dosing in a Research and Clinical Context
Tirzepatide dosing in the pivotal trials followed a deliberate, gradual escalation, and understanding that structure clarifies both the efficacy and the tolerability data. This section is descriptive of how the trials and approved labeling handle dosing; it is not guidance for use.
In the clinical program, tirzepatide is administered by once-weekly subcutaneous injection, initiated at a low 2.5 mg dose that is explicitly a non-therapeutic starting point intended only to acclimate the gastrointestinal tract. The dose is then escalated at four-week intervals — 2.5, 5, 7.5, 10, 12.5, up to a maximum of 15 mg — with the intent of reaching an effective maintenance dose while minimizing nausea and vomiting.1 This slow titration is not incidental; the gastrointestinal adverse effects that dominate the safety profile are largely dose- and titration-rate-dependent, and the escalation schedule is a central reason the drug is tolerable at doses that produce large effects.
The efficacy data are dose-dependent in a fairly orderly way: 5 mg produces smaller effects than 10 mg, which produces smaller effects than 15 mg, across weight, glycemia, and insulin-sensitivity markers. This dose-response is itself evidence that the effects are pharmacological rather than incidental. It also means that quoting only the 15 mg figures, as marketing frequently does, overstates the average result, since not every participant tolerates or requires the top dose.
For researchers handling reference material, tirzepatide is typically supplied as a lyophilized powder requiring reconstitution with a sterile diluent, with the concentration set by the diluent volume — the same arithmetic that underlies any peptide reconstitution. General handling principles for research peptides are covered in the site’s peptide reconstitution guide. It bears emphasizing that material obtained outside regulated pharmacy channels is not the FDA-approved product, may vary in purity and content, and carries risks unrelated to the pharmacology described here.
Safety, Tolerability, and the Limits of the Evidence
No honest account of tirzepatide can present the efficacy without the corresponding safety and limitation profile, which is substantial even for an approved drug.
The dominant adverse effects are gastrointestinal: nausea, diarrhea, vomiting, constipation, and dyspepsia, occurring in a meaningful minority of participants and driving most treatment discontinuations.24 These are generally mild-to-moderate, most common during dose escalation, and tend to attenuate over time, but they are the principal tolerability limit. Beyond the gastrointestinal profile, several considerations warrant emphasis:
- Lean-mass loss. As discussed, roughly a quarter of the weight lost is lean mass; the long-term functional consequences, especially in older adults, are not fully characterized in the trials.6
- Boxed warning. Tirzepatide carries a boxed warning regarding thyroid C-cell tumors based on rodent data; it is contraindicated in people with a personal or family history of medullary thyroid carcinoma or multiple endocrine neoplasia syndrome type 2. The relevance of the rodent finding to humans is uncertain but the contraindication is precautionary and firm.1
- Pancreatitis and gallbladder disease. As with GLP-1-based therapies, acute pancreatitis and gallbladder events have been reported and require vigilance.
- Hypoglycemia. Low on its own because insulinotropy is glucose-dependent, but the risk rises when combined with insulin or sulfonylureas.
- Population limits. Efficacy and safety are established in the studied populations (type 2 diabetes; obesity/overweight with comorbidity). Use in type 1 diabetes, pregnancy, or otherwise healthy individuals is not supported by these trials.
- Durability. The benefits require ongoing treatment; stopping the drug substantially reverses them, as detailed below.7
A further limitation that rarely appears in enthusiastic coverage concerns the endpoints themselves. The pivotal trials measured weight, HbA1c, body composition by DXA, and insulin-sensitivity surrogates — all intermediate or physiological outcomes. Dedicated large cardiovascular-outcome trials, which test whether the drug reduces hard events such as heart attack, stroke, and cardiovascular death, were still maturing at the time of writing. This matters because history is full of metabolic drugs that improved surrogate markers without delivering, or even while worsening, the hard outcomes that ultimately matter. Tirzepatide’s effects on weight, ectopic fat, blood pressure, and lipids all point in a favorable direction and make cardiovascular benefit plausible, but plausibility from surrogates is not the same as a demonstrated reduction in events, and the honest reader should hold the two apart until the outcome data are complete.
The reasonable synthesis is that tirzepatide has a well-characterized, manageable safety profile within its approved uses, dominated by gastrointestinal effects and hedged by a precautionary thyroid warning, but that this favorable profile was established in specific populations over trial-length durations and does not license casual use in people outside those criteria or extrapolation to indefinite lifelong exposure without ongoing monitoring.
How Tirzepatide Compares With Other Incretin Therapies
Placing tirzepatide beside its neighbors clarifies both its strengths and the honest limits of its advantage.
| Agent | Receptor targets | Approval / status | Representative top-line weight effect |
|---|---|---|---|
| Tirzepatide24 | GIP + GLP-1 dual agonist | FDA-approved (T2D; obesity; OSA) | ~21% (obesity, no diabetes, 15 mg, 72 wk) |
| Semaglutide 2.4 mg | GLP-1 agonist | FDA-approved (obesity; T2D at other doses) | ~15% (obesity, 68 wk) |
| Semaglutide 1 mg4 | GLP-1 agonist | FDA-approved (T2D) | ~5.7 kg (T2D, SURPASS-2 comparator) |
| Retatrutide14 | GIP + GLP-1 + glucagon triple agonist | Investigational (phase 3) | ~24% in phase 2 (obesity, 48 wk) — not yet approved |
Two honest points frame this comparison. First, tirzepatide’s superiority over semaglutide 1 mg in type 2 diabetes is established by a direct head-to-head trial (SURPASS-2), which is a high evidentiary bar; its apparent edge over semaglutide 2.4 mg for obesity rests substantially on cross-trial comparison and a later dedicated head-to-head, and cross-trial comparisons are always weaker than randomized ones.4 Second, retatrutide’s larger phase 2 numbers are precisely that — phase 2, investigational, and not FDA-approved — and should not be treated as an established superior option until phase 3 outcomes and regulatory review are complete. Newer or bigger numbers are not the same as better-established ones. The site’s overview of how GLP-1 pathways regulate lipid metabolism gives further context on how this drug class affects the broader metabolic profile beyond weight and glucose alone.
Durability and Weight Regain: The Honest Limitation
Perhaps the single most important caveat for anyone reading enthusiastic coverage is that tirzepatide’s benefits are contingent on continued treatment. This is not a cure that resets metabolism; it is an ongoing pharmacological intervention whose effects substantially reverse when it stops.
The evidence is direct. In SURMOUNT-4, participants first received tirzepatide for 36 weeks (achieving mean weight reduction of about 20.9%), then were randomized either to continue the drug or to switch to placebo, with lifestyle support maintained in both arms.7 Those who continued tirzepatide lost additional weight; those switched to placebo regained a substantial fraction of what they had lost. In the withdrawal arm, a large majority regained more than a quarter of the lost weight within a year, and about half regained more than half of it.7 Subsequent analyses showed that the regained weight was accompanied by a corresponding reversal of the cardiometabolic improvements — blood pressure, lipids, glycemia, and, by implication, insulin sensitivity — that the drug had produced.7
This has direct bearing on the article’s title question. The improvements in fat mass and insulin sensitivity are real and large while treatment continues, but they are not a permanent metabolic reprogramming. They are held in place by the drug. That reflects the underlying biology of obesity and insulin resistance as chronic, relapsing conditions rather than any failure of the compound — but it means that framing tirzepatide as a one-time fix, or implying the insulin-sensitivity gains persist independently after discontinuation, misrepresents the evidence. The clinical reality is closer to long-term, possibly indefinite, therapy.
There is a second, subtler concern embedded in the regain data that is easy to miss. When weight is regained after stopping the drug, it is not guaranteed to return in the same body-composition proportions in which it was lost. A person who lost roughly a quarter of their weight as lean mass may regain a larger share as fat, particularly without a structured resistance-training program during and after treatment. Over repeated cycles of loss and regain — the “yo-yo” pattern that intermittent or interrupted access to these drugs can produce — the theoretical risk is a gradual worsening of body composition even if scale weight returns to baseline. The trials were not designed to test repeated on-off cycling, so this remains a reasoned concern rather than a documented outcome, but it is a reason to think carefully about treatment as a sustained commitment rather than a short course. For readers tracking how the trial evidence continues to evolve, the site follows new data in its coverage of what the latest clinical trials reveal about tirzepatide.
Frequently Asked Questions
Does tirzepatide actually improve insulin sensitivity, or just lower blood sugar?
Both, and they are related but distinct. Tirzepatide lowers blood glucose through several routes, and one genuine component is improved insulin sensitivity — the efficiency with which insulin clears glucose into tissues. Gold-standard hyperinsulinemic-euglycemic clamp studies show a substantial increase in glucose disposal rate after treatment, and fasting surrogate markers such as HOMA2-IR improve by roughly 15–24% in trial analyses.812 Much of this improvement follows from weight loss and reduced ectopic (liver and visceral) fat, with a probable additional direct contribution from incretin signaling, especially GIP effects on adipose tissue. So it is not just glucose lowering, but the sensitivity gain is substantially, though not entirely, a downstream effect of fat loss.
How much of the insulin-sensitivity benefit is just from losing weight?
The most defensible interpretation is that the majority of the insulin-sensitivity improvement is mediated by weight loss and the reduction of ectopic fat in liver and muscle, since these are dominant drivers of insulin resistance and tirzepatide reduces them markedly.511 There is a probable additional direct effect from GIP and GLP-1 receptor signaling on adipose tissue and the beta cell, but its exact magnitude has not been cleanly quantified. Sources claiming tirzepatide is a powerful weight-independent insulin sensitizer are overstating the evidence.
How much fat does tirzepatide help people lose?
It depends heavily on population and dose. In adults with obesity but without diabetes, the 15 mg dose produced about 21% mean total-body-weight reduction over 72 weeks in SURMOUNT-1, of which roughly two-thirds to three-quarters was fat mass by DXA.26 In people with type 2 diabetes, weight loss is smaller — on the order of 11 kg at the top dose in SURPASS-2.4 The widely quoted “20%+” figures come from the non-diabetic obesity population at the maximum tolerated dose and should not be generalized.
Is the weight I lose all fat, or do I lose muscle too?
You lose both. In the SURMOUNT-1 DXA substudy, about 75% of the weight lost was fat and about 25% was lean mass — a ratio similar to placebo-driven and diet-driven weight loss.6 Lean-mass loss of roughly 11% is meaningful, especially for older adults, which is why resistance exercise and adequate protein intake are commonly recommended alongside treatment. That combination, however, has not been rigorously tested within the pivotal trials.
Is tirzepatide FDA-approved, and for what?
Yes. It is approved as Mounjaro for type 2 diabetes (2022) and as Zepbound for chronic weight management in adults with obesity or overweight plus a weight-related comorbidity (2023), and for obstructive sleep apnea in adults with obesity (2024).12 It is not approved for type 1 diabetes, for cosmetic weight loss in people without qualifying criteria, or as a general metabolic enhancer.
Why does tirzepatide seem to work better than semaglutide?
In type 2 diabetes, superiority over semaglutide 1 mg is established by the head-to-head SURPASS-2 trial on both HbA1c and weight.4 The mechanistic reason is debated: adding GIP receptor agonism to GLP-1 receptor agonism likely contributes, possibly through improved adipose insulin sensitivity and central potentiation of satiety, but the precise attribution of the advantage to GIP specifically versus other pharmacological differences is not fully resolved.313
Will the fat loss and insulin-sensitivity gains last if I stop taking it?
Largely no. The SURMOUNT-4 trial showed that stopping tirzepatide leads to substantial weight regain — most people regained more than a quarter of lost weight within a year — accompanied by reversal of the associated cardiometabolic improvements.7 The benefits are maintained by continued treatment, consistent with obesity and insulin resistance being chronic conditions, and are not a permanent reset.
Does tirzepatide reduce liver fat?
Yes, and this is one of the better-documented mechanistic findings. In the SURPASS-3 MRI substudy, tirzepatide reduced liver fat content substantially more than insulin degludec, and also reduced visceral and subcutaneous abdominal fat, whereas the insulin comparator increased them.5 Reduced liver fat is closely tied to improved insulin sensitivity, though tirzepatide is not approved as a treatment for fatty liver disease specifically.
Is “research” tirzepatide the same as the prescription product?
Not necessarily. Material sold outside regulated pharmacy channels as research peptide is not the FDA-approved product and may differ in purity, content, and sterility. The efficacy and safety data discussed here derive from the pharmaceutical-grade product studied under trial conditions; nothing here endorses use of unregulated material, and quality and provenance are serious, separate concerns.
References
- U.S. Food and Drug Administration. Mounjaro (tirzepatide) prescribing information and approval, May 2022. https://www.accessdata.fda.gov/scripts/cder/daf/
- Jastreboff AM, Aronne LJ, Ahmad NN, et al. Tirzepatide once weekly for the treatment of obesity (SURMOUNT-1). N Engl J Med. 2022;387(3):205-216. PMID 35658024. https://www.nejm.org/doi/full/10.1056/NEJMoa2206038
- Coskun T, Sloop KW, Loghin C, et al. LY3298176, a novel dual GIP and GLP-1 receptor agonist for the treatment of type 2 diabetes mellitus: from discovery to clinical proof of concept. Mol Metab. 2018;18:3-14. PMID 30473097. PMCID PMC6308032. https://pmc.ncbi.nlm.nih.gov/articles/PMC6308032/
- Frías JP, Davies MJ, Rosenstock J, et al. Tirzepatide versus semaglutide once weekly in patients with type 2 diabetes (SURPASS-2). N Engl J Med. 2021;385(6):503-515. PMID 34170647. https://www.nejm.org/doi/full/10.1056/NEJMoa2107519
- Gastaldelli A, Cusi K, Fernández Landó L, et al. Effect of tirzepatide versus insulin degludec on liver fat content and abdominal adipose tissue in people with type 2 diabetes (SURPASS-3 MRI). Lancet Diabetes Endocrinol. 2022;10(6):393-406. PMID 35468325. https://pubmed.ncbi.nlm.nih.gov/35468325/
- Look M, Dunn JP, Kushner RF, et al. Body composition changes during weight reduction with tirzepatide in the SURMOUNT-1 study of adults with obesity or overweight. Diabetes Obes Metab. 2025. PMID 39996356. https://pubmed.ncbi.nlm.nih.gov/39996356/
- Aronne LJ, Sattar N, Horn DB, et al. Continued treatment with tirzepatide for maintenance of weight reduction in adults with obesity: the SURMOUNT-4 randomized clinical trial. JAMA. 2024;331(1):38-48. PMID 38078870. https://jamanetwork.com/journals/jama/fullarticle/2812936
- Heise T, Mari A, DeVries JH, et al. Effects of subcutaneous tirzepatide versus placebo or semaglutide on pancreatic islet function and insulin sensitivity in adults with type 2 diabetes: a multicentre, randomised, double-blind, parallel-arm, phase 1 clinical trial. Lancet Diabetes Endocrinol. 2022;10(6):418-429. DOI 10.1016/S2213-8587(22)00085-7. https://www.thelancet.com/journals/landia/article/PIIS2213-8587(22)00085-7/abstract
- Lee CJ, Mao H, Thieu VT, Fernández Landó L, Thomas MK. Tirzepatide as monotherapy improved markers of beta-cell function and insulin sensitivity in type 2 diabetes (SURPASS-1). J Endocr Soc. 2023;7(5):bvad056. PMCID PMC10157777. https://pmc.ncbi.nlm.nih.gov/articles/PMC10157777/
- Garvey WT, Frias JP, Jastreboff AM, et al. Tirzepatide once weekly for the treatment of obesity in people with type 2 diabetes (SURMOUNT-2). Lancet. 2023;402(10402):613-626. PMID 37385275. https://pubmed.ncbi.nlm.nih.gov/37385275/
- Corrao S, Pollicino C, Maggio D, Torres A, Argano C. Tirzepatide against obesity and insulin-resistance: pathophysiological aspects and clinical evidence. Front Endocrinol (Lausanne). 2024;15:1402583. PMCID PMC11228148. https://www.frontiersin.org/journals/endocrinology/articles/10.3389/fendo.2024.1402583/full
- Frías JP, De Block C, Brown K, Wang H, Thomas MK, et al. Tirzepatide improved markers of islet cell function and insulin sensitivity in people with type 2 diabetes (SURPASS-2). J Clin Endocrinol Metab. 2024;109(7):1745-1753. PMCID PMC11180500. https://academic.oup.com/jcem/article/109/7/1745/7585180
- Regmi A, Aihara E, Christe ME, et al. Tirzepatide modulates the regulation of adipocyte nutrient metabolism through long-acting activation of the GIP receptor. Cell Metab. 2024;36(7):1534-1549. https://www.cell.com/cell-metabolism/fulltext/S1550-4131(24)00186-4
- Jastreboff AM, Kaplan LM, Frías JP, et al. Triple–hormone-receptor agonist retatrutide for obesity — a phase 2 trial. N Engl J Med. 2023;389(6):514-526. PMID 37366315. https://www.nejm.org/doi/full/10.1056/NEJMoa2301972
Educational and research-use disclaimer: This article is provided solely for scientific and educational purposes and is not medical advice. Tirzepatide is an FDA-approved prescription medicine (marketed as Mounjaro for type 2 diabetes and Zepbound for chronic weight management and obstructive sleep apnea) and should be used only under the supervision of a qualified healthcare professional and within its approved indications. The improvements in fat mass and insulin sensitivity described here were demonstrated in specific trial populations, are dose-dependent, are accompanied by loss of lean mass and gastrointestinal side effects, and substantially reverse when treatment is discontinued; they do not constitute a cure for obesity or diabetes. Tirzepatide is not approved for type 1 diabetes, pregnancy, or use in otherwise healthy individuals, and material sold outside regulated pharmacy channels is not the approved product. Nothing here should be construed as encouraging use of unregulated substances. Consult qualified professionals and applicable regulations before making any medical decisions.