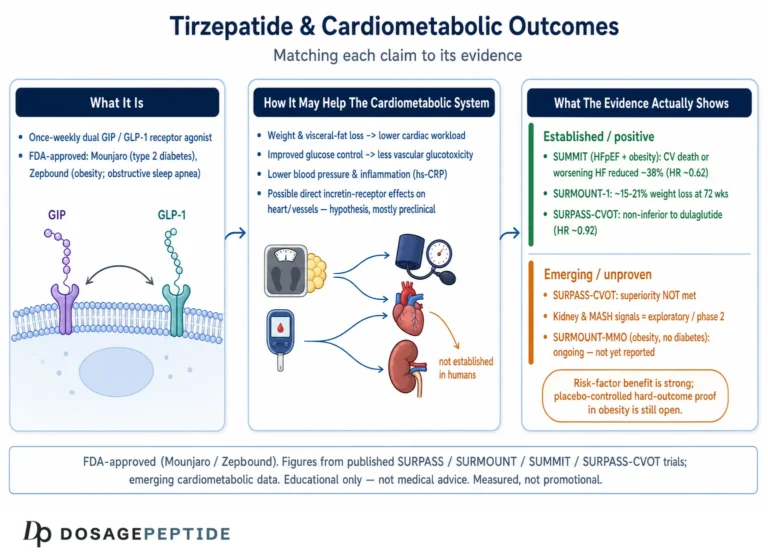
Few molecules have moved as quickly from the laboratory bench to household recognition as tirzepatide, the single-molecule dual incretin receptor agonist marketed by Eli Lilly as Mounjaro (for type 2 diabetes) and Zepbound (for chronic weight management and, more recently, obstructive sleep apnea). Unlike many compounds discussed in the peptide-research community, tirzepatide is not an experimental or preclinical agent: it has been rigorously tested in large, registrational, phase 3 randomized controlled trials, and it holds full U.S. Food and Drug Administration (FDA) approval across three separate indications.1011 That places it in a very different evidentiary category from the many peptides whose reputations rest on cell-culture experiments, rodent studies, or anecdote.
This article answers a deceptively simple question — what is tirzepatide, and how does it work? — by walking through its molecular architecture, its unusual dual-receptor pharmacology, the actual clinical trial data (stated at the level the evidence supports, not inflated), how it compares with selective GLP-1 receptor agonists, the research models used to characterize it, and its documented safety signals and regulatory boundaries. Because tirzepatide is a prescription medicine with a boxed warning, an honest account must be as clear about what is not known — long-term cardiovascular outcomes, effects across the full lifespan, and the limits of extrapolating trial populations to everyone — as it is about the headline efficacy numbers.
Everything below is written for educational and research-literacy purposes. It is not medical advice, not a protocol, and not an endorsement of any non-clinical use. Where dosing or handling is mentioned, it is described strictly in the context of how the approved product and its research analogs are characterized in the peer-reviewed and regulatory literature, and every efficacy or safety figure below is stated at the level of confidence the underlying evidence actually supports rather than the level marketing language often implies.
What Tirzepatide Is and Where It Came From
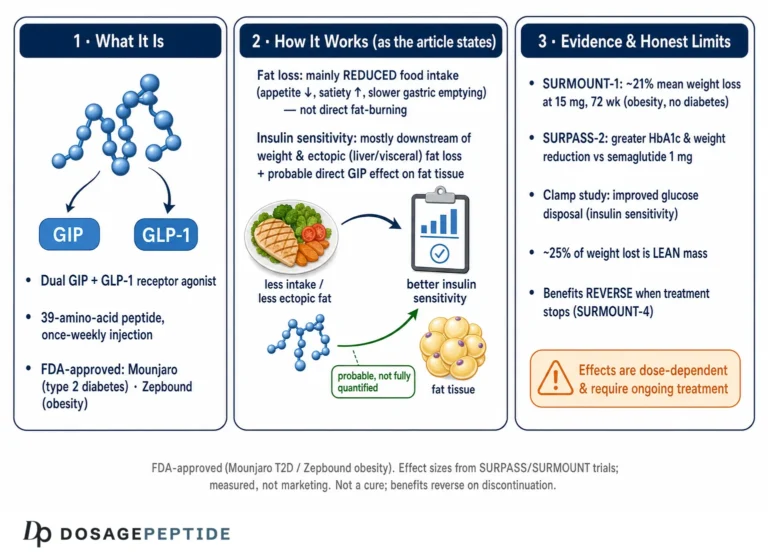
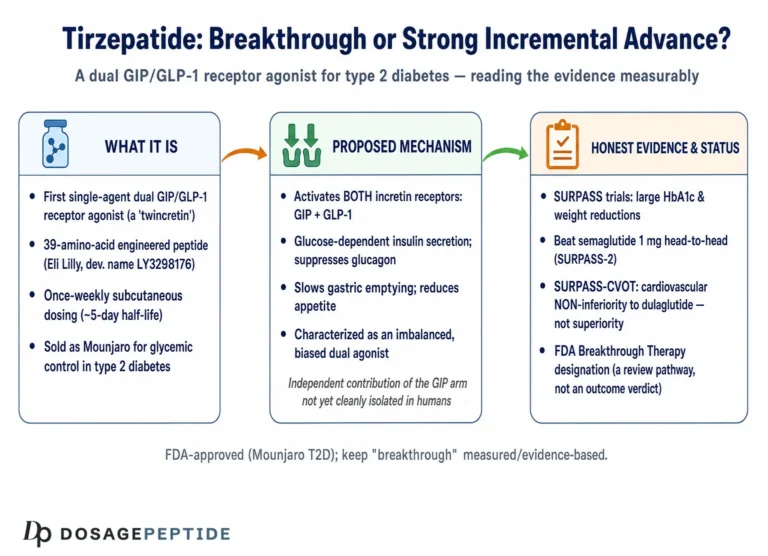
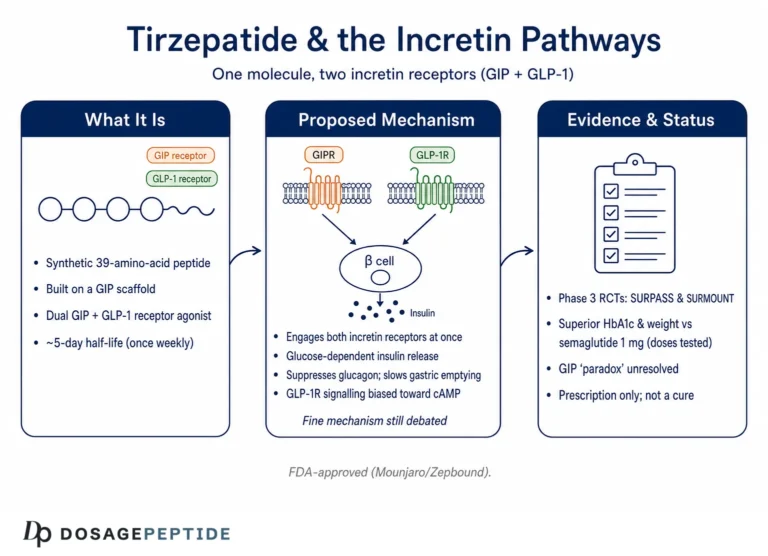
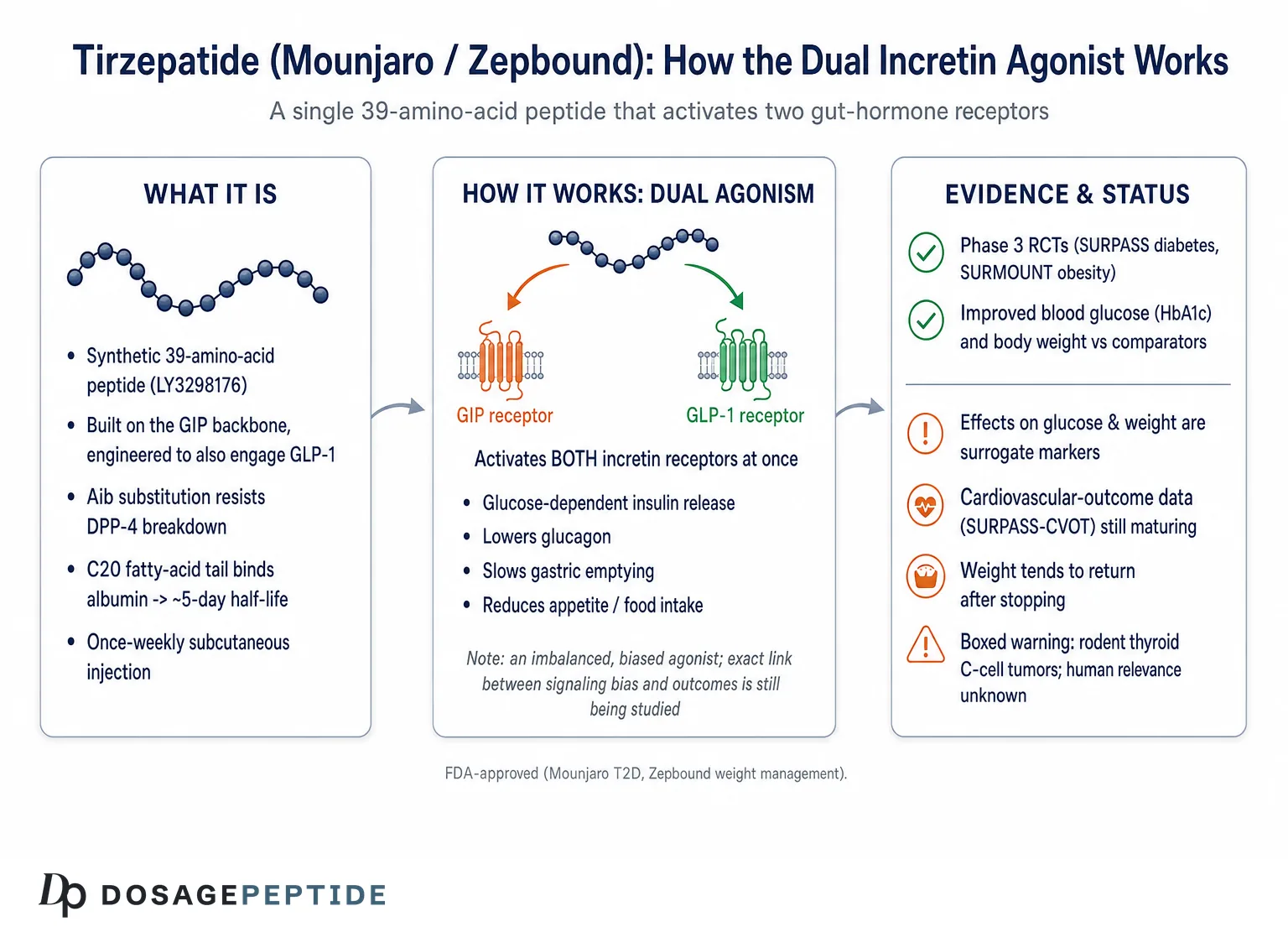
Tirzepatide (developmental code LY3298176) is a synthetic 39-amino-acid peptide engineered to activate two different hormone receptors at once: the receptor for glucose-dependent insulinotropic polypeptide (GIP) and the receptor for glucagon-like peptide-1 (GLP-1).19 Both GIP and GLP-1 belong to the family of gut-derived hormones called incretins — signals released from the intestine after eating that amplify insulin secretion in a glucose-dependent manner. For decades, drug developers focused almost exclusively on GLP-1, because GIP’s insulinotropic action appeared blunted in type 2 diabetes. Tirzepatide represents a deliberate bet that engaging both incretin pathways with one molecule would produce metabolic effects larger than either alone.
Structurally, the peptide is built on the GIP backbone rather than the GLP-1 backbone, then modified so that it can also engage the GLP-1 receptor.29 Two features are worth understanding because they explain much of the drug’s behavior. First, position 2 of the peptide carries a non-natural amino acid, alpha-aminoisobutyric acid (Aib), which blocks cleavage by the enzyme dipeptidyl peptidase-4 (DPP-4). Native incretins are destroyed by DPP-4 within a few minutes; the Aib substitution makes tirzepatide resistant to that enzyme, dramatically extending its lifespan in the body.9 Second, a lysine residue at position 20 is chemically modified (acylated) with a 20-carbon fatty di-acid (a C20 diacid) attached through a linker. This fatty “tail” binds reversibly to serum albumin, the most abundant protein in blood, effectively creating a slow-release depot that keeps the molecule circulating.9
The pharmacokinetic consequence of these two modifications is a long elimination half-life of roughly five days — commonly cited as about 4.5 to 6 days — which is what allows tirzepatide to be administered as a single weekly subcutaneous injection rather than daily.9 After a subcutaneous dose, peak plasma concentrations are reached over a wide window (roughly 8 to 72 hours), and with once-weekly dosing the drug reaches steady state after about four weeks. This slow onset is one reason the approved products are titrated upward over months rather than started at full strength: gradual escalation improves gastrointestinal tolerability.10
Historically, tirzepatide emerged from Eli Lilly’s incretin chemistry program and advanced through early-phase human studies in the late 2010s. It first demonstrated in phase 2 that dual agonism could out-perform a best-in-class selective GLP-1 agonist for glycemic control, which set the stage for the large phase 3 SURPASS (diabetes) and SURMOUNT (obesity) programs that followed.13 The FDA approved it as Mounjaro for type 2 diabetes in May 2022, then as Zepbound for chronic weight management in November 2023, and expanded the Zepbound label to include moderate-to-severe obstructive sleep apnea in adults with obesity in December 2024.101112
It is important to be precise about naming. “Mounjaro” and “Zepbound” are the same active molecule — tirzepatide — sold under two brand names tied to two different sets of approved indications. In the research and gray-market peptide space, tirzepatide is also sold as a lyophilized (freeze-dried) powder in vials labeled by milligram content, and dosagepeptide.com maintains reference pages for several of these vial sizes, including the 5 mg vial, the 10 mg vial, the 15 mg vial, and the 30 mg vial. Those vials are not FDA-approved finished drug products and are not interchangeable, in a regulatory or quality sense, with the pharmaceutical pens.
The Molecular Mechanism: A Dual Incretin Agonist
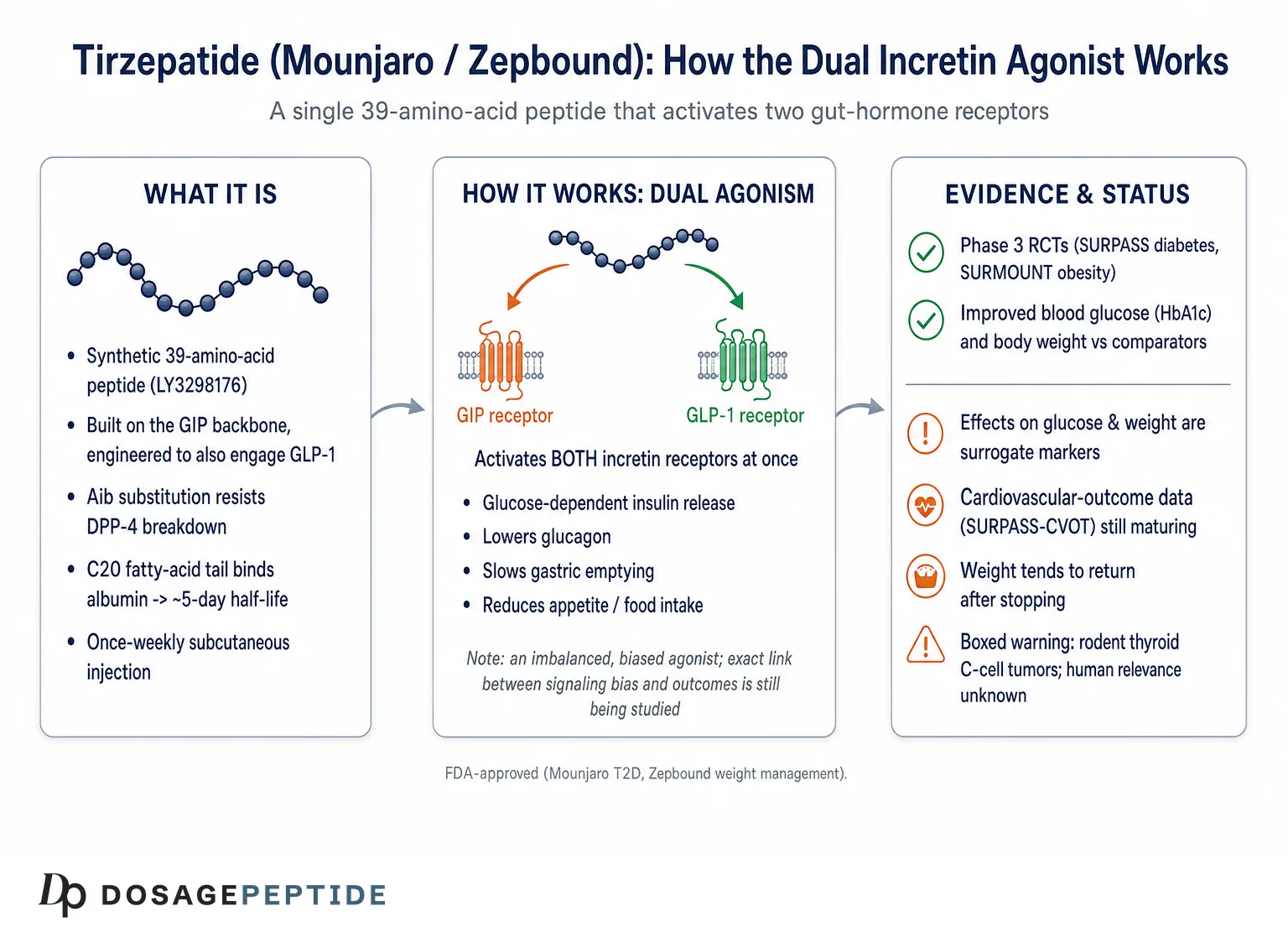
To understand how tirzepatide works, it helps to separate what each receptor does and then see how activating both simultaneously changes the picture. The GLP-1 receptor, when activated, does several things at once: it enhances glucose-dependent insulin secretion from pancreatic beta cells, suppresses inappropriate glucagon release from alpha cells, slows the rate at which the stomach empties, and acts in the brain to reduce appetite and food intake.1 Because insulin secretion is glucose-dependent, GLP-1 receptor activation tends not to cause hypoglycemia on its own — it amplifies insulin release when blood sugar is high but not when it is normal.
The GIP receptor is more nuanced. GIP is the body’s dominant incretin under normal physiology, and GIP receptor activation also enhances glucose-dependent insulin secretion and appears to improve beta-cell function and insulin sensitivity.13 GIP signaling in adipose tissue and in the central nervous system is an active area of research, and its precise contribution to weight loss when co-activated with GLP-1 is still being worked out. The central hypothesis behind tirzepatide is that combining GIP and GLP-1 agonism yields complementary and possibly synergistic effects on insulin secretion, glucagon suppression, energy intake, and body weight that exceed what a GLP-1 agonist achieves alone.13
What makes tirzepatide pharmacologically distinctive is that it is not a “balanced” dual agonist. Detailed receptor-signaling studies characterize it as an imbalanced and biased agonist.1 In practical terms: its affinity for the GIP receptor is comparable to that of native GIP, while its affinity for the GLP-1 receptor is roughly five-fold weaker than native GLP-1.1 At the GIP receptor it behaves much like the natural hormone. At the GLP-1 receptor, however, it shows signaling bias — it preferentially drives cyclic AMP (cAMP) production, the classic insulin-promoting second messenger, while recruiting less of the protein beta-arrestin and causing less receptor internalization than native GLP-1 would.1 Reduced internalization means the receptor stays available at the cell surface longer, which may sustain signaling. This biased, GIP-favoring profile is thought to contribute to the compound’s efficacy, though the exact mechanistic link between the bias and the clinical outcomes remains a subject of ongoing research rather than settled fact.
Structural biology has added resolution to this story. Cryo-electron microscopy and molecular studies of tirzepatide bound to each receptor show how the shared peptide accommodates two structurally different binding pockets, and how the fatty-acid modification and specific residues govern the differential engagement.2 These structural determinants explain why a single sequence can act as a genuine agonist at both receptors rather than a weak partial agonist at one.
The downstream physiology, integrated across both receptors, produces the metabolic signature seen in trials: improved first- and second-phase insulin secretion, better beta-cell responsiveness, reduced fasting and post-meal glucose, lowered glucagon, delayed gastric emptying, and a substantial reduction in appetite and caloric intake that drives weight loss.13 A mechanistic study using clamp techniques demonstrated that tirzepatide improved both insulin sensitivity and beta-cell function in people with type 2 diabetes, with the insulin-sensitivity improvement appearing to be largely mediated by weight loss and reduced glucose toxicity rather than a direct drug effect on muscle or liver — an important nuance often lost in marketing summaries.13
One frequently misunderstood point deserves emphasis: tirzepatide does not “burn fat” through a direct thermogenic mechanism, and it is not an amphetamine-like stimulant. Its weight effect is driven principally by reduced energy intake secondary to appetite suppression, slowed gastric emptying, and altered central signaling of satiety and reward, layered on top of its glucose-lowering actions.1 The distinction matters for anyone trying to reason about what the molecule can and cannot plausibly do.
What the Evidence Actually Shows: The SURPASS Diabetes Program
The strongest reason to take tirzepatide seriously is the size and quality of its evidence base. For type 2 diabetes, that evidence comes from the SURPASS program — a series of phase 3 randomized controlled trials that collectively enrolled thousands of adults and tested tirzepatide against placebo and against several active comparators. Every SURPASS trial met its primary glycemic endpoint.3
The most-cited of these is SURPASS-2, published in the New England Journal of Medicine in 2021. This 40-week trial randomized 1,879 adults with type 2 diabetes inadequately controlled on metformin to one of three tirzepatide doses (5, 10, or 15 mg once weekly) or to semaglutide 1 mg once weekly — at the time the leading injectable GLP-1 agonist for diabetes.3 All three tirzepatide doses produced significantly greater reductions in HbA1c (a measure of average blood glucose over roughly three months) and in body weight than semaglutide. Across the SURPASS program, HbA1c reductions in the range of roughly 1.9 to 2.6 percentage points were reported over 40 to 52 weeks, and a large proportion of participants on the higher doses reached the treatment target of HbA1c below 7%.3
These are genuinely large glycemic effects for a single agent. But several caveats keep the claim honest. First, the comparison in SURPASS-2 used semaglutide 1 mg, which is not the highest semaglutide dose later approved for weight management; head-to-head superiority against one dose of one comparator should not be read as a blanket claim of superiority in every setting. Second, the trial populations were selected — participants met specific inclusion criteria and were monitored closely — so real-world results in unselected patients with more comorbidity or lower adherence are typically more modest. Third, HbA1c is a surrogate marker: it correlates with long-term complications but is not itself a hard outcome like heart attack, stroke, kidney failure, or death.
That last point is why the dedicated cardiovascular outcomes trial, SURPASS-CVOT, matters so much. It was designed to test whether tirzepatide reduces major adverse cardiovascular events compared with an active comparator (dulaglutide, a GLP-1 agent already shown to have cardiovascular benefit) in people with type 2 diabetes and established cardiovascular disease.39 Until such outcome data are fully reported and integrated into guidelines, it is accurate to say tirzepatide robustly improves glycemic and weight surrogates, and premature to claim it definitively reduces cardiovascular death on the strength of the surrogate data alone.
The SURPASS trials also documented favorable movement in secondary cardiometabolic markers — reductions in systolic blood pressure, improvements in lipid fractions, and reductions in waist circumference — consistent with the weight loss and metabolic improvement.3 These are encouraging supporting signals, but they are secondary endpoints and should be framed as such. The disciplined way to summarize SURPASS is: in adults with type 2 diabetes, tirzepatide produced clinically meaningful, dose-dependent improvements in blood glucose and body weight that exceeded a standard-of-care GLP-1 comparator in the tested conditions, with cardiovascular-outcome confirmation being the appropriate next tier of evidence.3
Readers interested in how the milligram strengths used in trials map onto the vial products circulating in research settings can consult dosagepeptide.com’s peptide dosage index, which catalogs reference protocols across compounds. Those pages are educational references, not clinical dosing instructions, and the trial doses above are the doses actually studied under medical supervision.
Weight-Management Evidence: The SURMOUNT Program
If SURPASS built the diabetes case, the SURMOUNT program built the obesity case, and its headline numbers are what pushed tirzepatide into public consciousness. SURMOUNT-1, published in the New England Journal of Medicine in 2022, was a 72-week trial in adults with obesity, or overweight with at least one weight-related complication, who did not have type 2 diabetes.4 Participants were randomized to tirzepatide 5, 10, or 15 mg once weekly or to placebo, all alongside lifestyle counseling.
The mean weight reductions were striking: approximately 16.0% at 5 mg, 21.4% at 10 mg, and 22.5% at 15 mg, versus about 2.4% with placebo.4 Framed differently, roughly 89% of participants on the lowest dose and about 96% on the two higher doses achieved at least 5% weight loss, compared with about 28% on placebo.4 Weight loss on the order of 20% or more from a pharmacologic agent had previously been the province of bariatric surgery, which is why these results drew such attention.
| Trial | Population | Duration | Key result (highest dose) |
|---|---|---|---|
| SURPASS-23 | T2D on metformin | 40 weeks | HbA1c reduction superior to semaglutide 1 mg; greater weight loss |
| SURMOUNT-14 | Obesity, no diabetes | 72 weeks | ~22.5% mean body-weight reduction (15 mg) vs ~2.4% placebo |
| SURMOUNT-OSA5 | Obesity + moderate-severe OSA | 52 weeks | AHI reduced ~25–29 events/hr vs ~5 with placebo |
| SURMOUNT-56 | Obesity, head-to-head | 72 weeks | ~20% weight loss vs ~14% for semaglutide 2.4 mg |
The obesity story did not stop at weight. The SURMOUNT-OSA trials tested tirzepatide in adults with obesity and moderate-to-severe obstructive sleep apnea, both with and without concurrent CPAP therapy.5 The primary endpoint was the apnea-hypopnea index (AHI), the number of breathing interruptions per hour of sleep. Tirzepatide reduced AHI by roughly 25 to 29 events per hour depending on the sub-trial, versus about 5 events with placebo, alongside body-weight reductions in the high teens to about 20%.5 Those results directly supported the December 2024 expansion of the Zepbound label to include moderate-to-severe OSA in adults with obesity — the first drug therapy approved for that condition.12
More recently, the head-to-head SURMOUNT-5 trial randomized 751 adults with obesity (without diabetes) to tirzepatide or to semaglutide 2.4 mg — the full weight-management dose of semaglutide — over 72 weeks.6 Tirzepatide produced greater mean weight loss (on the order of 20% versus roughly 14% for semaglutide) and larger reductions in waist circumference, with improvements in several cardiometabolic parameters.6 This is a cleaner comparison than SURPASS-2 because it pits each drug at its approved obesity dose, and it strengthens the claim that dual agonism offers an efficacy advantage over selective GLP-1 agonism for weight loss specifically.
Two honest qualifiers apply to all of this. First, weight regain after discontinuation is well documented across the incretin class: a separate withdrawal trial (SURMOUNT-4) showed that stopping the drug led to substantial regain, underscoring that the effect is maintained only while treatment continues, much like blood-pressure medication.8 Second, the trials enrolled adults meeting specific BMI and comorbidity criteria under structured lifestyle support, so the percentages should be read as what is achievable in a trial, not a guarantee for any individual. Weight loss is also not a clinical outcome in itself; the value lies in whether it translates into reduced disease and longer, healthier life, which longer-term outcome trials are still evaluating.
How Tirzepatide Compares to Other Incretin Agents
Placing tirzepatide in context requires comparing it to the selective GLP-1 receptor agonists that preceded it — principally semaglutide (Ozempic for diabetes, Wegovy for weight management) and, earlier, liraglutide and dulaglutide. The central conceptual difference is receptor coverage: the older agents engage GLP-1 alone, whereas tirzepatide engages both GLP-1 and GIP.1 The clinical question is whether that added GIP engagement translates into meaningfully better outcomes, and the trial evidence suggests that, for glycemic control and for weight loss, it generally does — at least against the specific comparator doses tested.36
SURPASS-2 showed superior HbA1c and weight reduction versus semaglutide 1 mg in diabetes,3 and SURMOUNT-5 showed superior weight loss versus semaglutide 2.4 mg in obesity.6 Those are the two most rigorous direct comparisons, and both favored tirzepatide on the primary efficacy metric. That said, “superior on average” does not mean superior for every person or on every dimension. Individual responses vary widely; some people tolerate one agent better than the other, and cost, insurance coverage, injection experience, and supply availability all shape which agent is appropriate in practice.
| Feature | Tirzepatide | Semaglutide |
|---|---|---|
| Receptor targets | GIP + GLP-1 (dual) | GLP-1 only (selective) |
| Dosing frequency | Once weekly SC | Once weekly SC (oral form also exists) |
| Approx. half-life | ~5 days9 | ~7 days |
| Head-to-head weight loss | Greater in SURMOUNT-56 | Comparator arm |
| Cardiovascular outcome data | SURPASS-CVOT (in progress/reporting)3 | Established (SUSTAIN-6, SELECT) |
One area where semaglutide currently holds an evidentiary edge is cardiovascular outcomes. Semaglutide has completed large outcome trials demonstrating cardiovascular benefit in relevant populations, whereas tirzepatide’s dedicated cardiovascular-outcomes trial is a more recent read-out; until those data are fully mature and reflected in guidelines, it is fair to say tirzepatide has stronger surrogate data and semaglutide has a longer track record of hard-outcome data.3 This is exactly the kind of nuance that gets flattened in promotional and social-media coverage, where “tirzepatide beats semaglutide” becomes a slogan detached from the specific endpoint and dose being compared.
Tolerability comparisons are also informative. In SURMOUNT-5, gastrointestinal adverse events leading to discontinuation were somewhat less frequent with tirzepatide (about 2.7%) than with semaglutide (about 5.6%), suggesting that greater efficacy did not come at the cost of worse tolerability in that trial.6 Still, both drugs share the same class-level side-effect profile, and neither is free of the nausea, diarrhea, and constipation that characterize incretin therapy.
It is also worth distinguishing the two comparator doses to avoid a common misreading. SURPASS-2 compared tirzepatide against semaglutide 1 mg, the highest dose approved for diabetes at the time of the trial, whereas SURMOUNT-5 compared it against semaglutide 2.4 mg, the dedicated weight-management dose.36 Because those are different doses for different purposes, the two trials answer two different questions — superiority for glycemic control at diabetes-approved doses, and superiority for weight loss at obesity-approved doses. Both favored tirzepatide, which is a strong and consistent pattern, but the specificity matters: it is not the same as saying tirzepatide is superior on every conceivable endpoint, in every population, at every dose pairing. Careful readers hold the claim at exactly the resolution the trials support.
Looking ahead, tirzepatide sits within a rapidly expanding landscape of incretin-based and multi-agonist molecules — triple agonists adding glucagon-receptor activity, oral small-molecule GLP-1 agents, and amylin-based combinations are all in development. Tirzepatide is therefore best understood not as a final endpoint but as the first commercially successful proof that multi-receptor incretin agonism can outperform single-receptor agonism, opening a design space that competitors are actively exploring.
Research Models and Methodology
The evidence behind tirzepatide was generated across a hierarchy of research models, and understanding that hierarchy is essential to reading claims critically. At the most fundamental level are in vitro receptor-pharmacology assays: cell lines engineered to express the human GIP or GLP-1 receptor, used to measure binding affinity, cAMP production, beta-arrestin recruitment, and receptor internalization.1 These assays are what established tirzepatide’s imbalanced, biased signaling signature. They are precise and reproducible, but they describe molecular behavior in isolated cells, not whole-organism physiology.
Above that sit structural methods — cryo-electron microscopy and related biophysical techniques — that resolve how the peptide physically docks into each receptor. Structural studies of tirzepatide bound to the GIP and GLP-1 receptors clarified the atomic basis for dual agonism and are a good example of methodology that explains mechanism without addressing clinical benefit.2 A molecule can have an elegant, well-characterized binding mode and still fail in humans; structure supports plausibility, not proof of efficacy.
Next are animal models, principally rodents, used for pharmacokinetics, dose-finding, glucose and body-weight effects, and toxicology. Rodent studies were where the thyroid C-cell tumor signal (discussed below) first appeared, and they informed the once-weekly dosing rationale.10 The critical methodological caveat is species translation: rodents differ from humans in incretin biology and in C-cell physiology specifically, so rodent findings can over- or under-predict human effects. Regulators treat rodent carcinogenicity signals conservatively precisely because their human relevance is often uncertain.
The decisive tier is the randomized controlled trial in humans, and tirzepatide’s program is a model of how this is done well. The SURPASS and SURMOUNT trials used randomization to balance known and unknown confounders, placebo or active comparators, pre-registered primary endpoints, blinding where feasible, intention-to-treat and per-protocol analyses, and independent adjudication of key events.34 Reported analyses also distinguish between “treatment-regimen” estimands (effects regardless of adherence) and “efficacy” estimands (effects if treatment is taken as directed), which is why the same trial can generate slightly different headline numbers depending on the analytic framework.4 A careful reader checks which estimand a quoted number reflects.
Two methodological limitations recur across this literature and deserve flagging. First, most pivotal trials were sponsored and conducted by the manufacturer; this is standard for registrational studies and the trials were published in top peer-reviewed journals with rigorous review, but industry sponsorship is a factor to weigh, and independent replication and real-world evidence add important texture. Second, trial durations of 40 to 72 weeks, while long by drug-trial standards, are short relative to the many years a person with a chronic condition might take the drug; durability, very-long-term safety, and outcomes therefore rest partly on extension studies, pharmacovigilance databases, and post-marketing surveillance rather than the pivotal trials alone.9
Finally, some of the most useful post-approval evidence comes from pooled analyses and pharmacovigilance. Pooled analyses of gastrointestinal tolerability across SURPASS and across SURMOUNT-1 through -4 aggregate thousands of participants to characterize side-effect timing and dose-dependence more precisely than any single trial.78 Adverse-event reporting systems capture rare events that trials are too small to detect, at the cost of lacking a denominator and being prone to reporting bias. Neither replaces the RCT, but both extend it — and both are the appropriate places to look for signals about uncommon harms.
Safety and Tolerability
Tirzepatide is a prescription medicine with a defined and clinically important safety profile, and no honest account of “how it works” is complete without it. By far the most common adverse effects are gastrointestinal. In SURMOUNT-1, nausea was reported in roughly 24% to 33% of participants depending on dose, diarrhea in about 17% to 23%, constipation in about 11% to 17%, and vomiting in about 6% to 13%.48 These events were predominantly mild to moderate, occurred most often during dose escalation in the first weeks, and diminished over time at a given maintenance dose.8 This temporal pattern is why the approved products start low and titrate slowly, and why abruptly jumping to a high dose is both less tolerable and, in unsupervised settings, potentially hazardous.
Discontinuation due to adverse events was relatively modest in the trials. In the pooled SURMOUNT-1 through -4 analysis, discontinuation rates due to adverse events were roughly 4.3% at 5 mg, 7.1% at 10 mg, 6.2% at 15 mg, and 2.6% for placebo — meaning the great majority of participants tolerated the drug well enough to continue.8 Because insulin secretion driven by tirzepatide is glucose-dependent, the risk of hypoglycemia from tirzepatide alone is low; however, that risk rises meaningfully when it is combined with insulin or sulfonylureas, which is why co-therapy is adjusted under medical supervision.10
Beyond the common and manageable effects, several less-common but serious risks anchor the product labeling. The prescribing information carries a boxed warning — the FDA’s most prominent safety warning — regarding thyroid C-cell tumors.10 This is based on rodent studies in which tirzepatide caused dose- and duration-dependent thyroid C-cell tumors; whether this translates to humans is unknown.10 Because of this uncertainty, tirzepatide is contraindicated in people with a personal or family history of medullary thyroid carcinoma (MTC) or with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2).10
| Category | Representative findings |
|---|---|
| Very common (GI) | Nausea, diarrhea, constipation, vomiting — mostly mild/moderate, early, dose-related8 |
| Boxed warning | Rodent thyroid C-cell tumors; human relevance unknown10 |
| Contraindications | Personal/family history of MTC; MEN 210 |
| Serious (uncommon) | Acute pancreatitis, gallbladder disease, acute kidney injury (via dehydration), severe GI reactions, hypersensitivity10 |
| Interaction risks | Hypoglycemia with insulin/sulfonylureas; altered absorption of oral drugs via delayed gastric emptying10 |
Other labeled risks include acute pancreatitis (the drug has not been studied in people with a history of pancreatitis), acute gallbladder disease and gallstones, acute kidney injury — usually precipitated by dehydration from severe vomiting or diarrhea — diabetic retinopathy considerations in people with diabetes, hypersensitivity reactions, and the theoretical risk of aspiration during anesthesia due to delayed gastric emptying, which has prompted evolving peri-operative guidance.10 Delayed gastric emptying can also alter the absorption of orally administered medications, an interaction worth noting for anyone on oral drugs with narrow therapeutic windows. Tirzepatide has additionally been observed to reduce the effectiveness of oral hormonal contraceptives during dose escalation, which is a specific, practical warning in the label.10
A distinct and serious concern specific to the non-clinical market is product quality. Compounded and research-grade tirzepatide products have been the subject of FDA attention, and buying peptide powder outside the regulated supply chain removes the assurances of identity, purity, sterility, and correct concentration that pharmaceutical manufacturing provides.10 Dosing errors with such products — particularly miscalculating concentration after reconstitution — have led to documented overdoses. The safety profile summarized above is the profile of the studied, pharmaceutical-grade molecule under medical supervision; it does not automatically transfer to unverified material used without oversight.
Handling and Reconstitution in a Research Context
Because tirzepatide is widely sold to the research community as a lyophilized powder, it is worth describing how such peptides are handled — strictly as background on laboratory practice, not as a how-to for human use. Lyophilized peptides are shipped freeze-dried to maximize stability during transport and storage. A freeze-dried vial is typically stored refrigerated or frozen and protected from light; once a peptide is reconstituted into liquid, its shelf life shortens considerably and refrigeration becomes important to limit degradation.
Reconstitution is the process of dissolving the powder in a sterile diluent — commonly bacteriostatic water, which contains a small amount of benzyl alcohol as a preservative to inhibit microbial growth in a multi-use vial. The diluent is added slowly down the inside wall of the vial rather than sprayed directly onto the peptide pellet, because peptides can be denatured by shear force and foaming; the vial is then swirled gently, not shaken, until the solution clears. The concentration of the resulting solution is entirely determined by the ratio of peptide mass to diluent volume — for example, dissolving a 10 mg vial in 1 mL yields a very different concentration than dissolving it in 2 mL — which is exactly why concentration math is the single most error-prone step and the one where mistakes have real consequences.
This is where dosagepeptide.com’s reference tooling is relevant as an educational resource. The site’s peptide reconstitution guide and dosage calculator walk through the arithmetic of converting a target amount into a syringe volume given a chosen reconstitution ratio, and the per-vial pages linked earlier illustrate how different vial sizes change that math. Presenting the arithmetic transparently is a harm-reduction measure: the most dangerous scenario is someone guessing at concentration and drawing a wildly wrong volume. None of this should be read as encouragement to self-administer a molecule outside medical care; it is a description of how the calculations work so that the numbers thrown around in the community can be understood and scrutinized.
General good-practice principles that recur in the peptide-handling literature include: using sterile technique and alcohol-swabbing the vial stopper before every needle entry; not re-using needles; discarding solution that has become cloudy, discolored, or that contains particulates; labeling reconstituted vials with the concentration and date; and respecting the preservative-limited shelf life of a reconstituted multi-use vial. Freeze-thaw cycling is generally avoided because repeated temperature swings accelerate degradation. Again, these are the practices of a research setting; the pharmaceutical products (Mounjaro and Zepbound) arrive as pre-filled, pre-measured pens that require none of this reconstitution and are the only forms studied for human use.
The overarching point of this section is a cautionary one. The gap between a validated pharmaceutical pen and a reconstituted research vial is not merely one of convenience; it is a gap in identity verification, sterility assurance, concentration accuracy, and regulatory accountability. Understanding reconstitution mechanics does not close that gap. Anyone reasoning about tirzepatide should keep the two categories firmly distinct, and should treat concentration arithmetic, sterility, and material identity as the three failure points where errors are both most likely and most consequential.
Limitations and the Human-Evidence Gap
For a drug this well studied, it might seem that little is unknown — but several genuine gaps and limitations remain, and naming them honestly is part of scientific literacy. The first is duration. Even the longest pivotal trials ran about 72 weeks, and while extension and follow-up analyses now stretch to three years and beyond, that is still short relative to the multi-decade horizon over which a chronic-disease medication might be taken.4 Very-long-term safety and efficacy are extrapolated from accumulating but incomplete data.
The second gap is hard clinical outcomes. Most of tirzepatide’s celebrated numbers are surrogate markers: HbA1c, body weight, AHI, blood pressure, lipids. Surrogates are useful and generally correlate with outcomes, but the definitive questions — does tirzepatide reduce heart attacks, strokes, kidney failure, and death, and by how much? — are answered only by dedicated outcome trials, which are still maturing for tirzepatide even as they are established for some older agents.3 It is accurate to say tirzepatide dramatically improves metabolic surrogates; it is premature to claim it has been definitively shown to extend life or prevent cardiovascular death.
Third is durability and dependence on continued use. Withdrawal data show substantial weight regain after stopping, meaning the effect is a treatment effect that persists only during treatment, not a cure that resets physiology.8 This reframes tirzepatide as chronic therapy for chronic conditions rather than a short course — a framing with implications for cost, adherence, and long-term risk that individuals and health systems are still working through.
Fourth is generalizability. Trial populations met specific criteria and received structured support; effects in people who are older, frailer, have significant kidney or liver disease, are pregnant or breastfeeding (populations typically excluded and where the drug is not recommended), or who have psychiatric or eating-disorder histories are less well characterized.4 Body composition is another open area: weight loss includes loss of lean mass as well as fat, and the long-term functional consequences of that in various populations are an active research question rather than a settled matter.
Fifth is the mechanistic uncertainty that persists despite excellent structural and pharmacological characterization. The precise contribution of GIP-receptor agonism — and even whether GIP-receptor agonism versus certain forms of antagonism is optimal for weight effects — is still debated in the literature, and the causal link between tirzepatide’s biased signaling and its clinical superiority is inferred rather than fully proven.1 That the drug works is beyond doubt; exactly why it works better than selective GLP-1 agonism is still being resolved.
Finally, for the specific context of this site’s audience, there is the research-product gap already emphasized: essentially all of the human evidence above was generated with pharmaceutical-grade tirzepatide administered under supervision, and none of it validates the safety, potency, or purity of research-grade powder used without oversight. Extrapolating trial efficacy and safety to unverified material is not supported by the data. The honest summary is that tirzepatide is one of the best-evidenced metabolic drugs of its generation and that meaningful uncertainties — about very-long-term outcomes, mechanism, special populations, and non-pharmaceutical products — genuinely remain.
Regulatory Status
Unlike many compounds in the peptide-research world, tirzepatide’s regulatory status is unambiguous and well documented. In the United States it is a fully FDA-approved prescription drug, sold under two brand names for three indications, all manufactured by Eli Lilly and Company.
As Mounjaro, tirzepatide was approved in May 2022 as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes.1011 As Zepbound, it was approved in November 2023 for chronic weight management in adults with obesity, or overweight with at least one weight-related comorbidity, alongside a reduced-calorie diet and increased physical activity.11 In December 2024, the Zepbound indication was expanded to include moderate-to-severe obstructive sleep apnea in adults with obesity — the first medication ever approved for OSA.12 Both brands are supplied as pre-filled single-dose pens or vials in a range of strengths for once-weekly subcutaneous injection, with dosing titrated upward over time.10
The regulatory approvals are indication-specific and population-specific. Approval for type 2 diabetes, weight management, and OSA does not constitute approval for cosmetic use in people who do not meet the labeled criteria, for use in children outside studied populations, or for any of the off-label metabolic or “anti-aging” applications sometimes discussed online. Prescribing outside the label is a decision that rests with licensed clinicians exercising medical judgment, and it carries a correspondingly different evidence and liability profile.
Outside the U.S., tirzepatide has been authorized by other major regulators, including the European Medicines Agency, under the Mounjaro brand, generally following the same body of SURPASS and SURMOUNT evidence, though exact indications, wording, and reimbursement vary by jurisdiction. Anyone relying on regulatory status in a particular country should consult that country’s specific authorization rather than assuming the U.S. situation applies globally.
A critical regulatory distinction concerns compounded and research-grade tirzepatide. The FDA has taken action regarding compounded versions and has issued communications about quality and dosing-error risks associated with products obtained outside the approved supply chain.10 “Research use only” or “not for human consumption” labeling on peptide vials places those products in an entirely different regulatory category from the approved pharmaceuticals: they are not evaluated by the FDA for safety, efficacy, purity, or potency, and their sale for human use is not authorized. The robust evidence and defined safety profile described throughout this article attach to the approved product; they should not be read as regulatory endorsement of any unapproved source.
Frequently Asked Questions
Is tirzepatide the same thing as Mounjaro and Zepbound?
Yes. Tirzepatide is the generic name of the active molecule; Mounjaro and Zepbound are two brand names Eli Lilly uses for the same drug under different approved indications — Mounjaro for type 2 diabetes and Zepbound for chronic weight management and obstructive sleep apnea.101112 The molecule is identical; the branding and labeled uses differ.
How is tirzepatide different from Ozempic or Wegovy (semaglutide)?
Semaglutide (Ozempic/Wegovy) activates only the GLP-1 receptor, whereas tirzepatide activates both the GLP-1 and the GIP receptors — it is a dual incretin agonist.1 In head-to-head trials, tirzepatide produced greater HbA1c reduction in diabetes (SURPASS-2, versus semaglutide 1 mg) and greater weight loss in obesity (SURMOUNT-5, versus semaglutide 2.4 mg).36 Semaglutide, however, currently has a longer track record of hard cardiovascular-outcome data.
How much weight did people lose in the trials?
In SURMOUNT-1, adults with obesity (without diabetes) lost on average about 16.0%, 21.4%, and 22.5% of body weight on the 5, 10, and 15 mg doses respectively over 72 weeks, versus about 2.4% on placebo.4 These are trial averages under structured lifestyle support; individual results vary, and weight tends to return after stopping the drug.8
What are the most common side effects?
Gastrointestinal effects dominate: nausea, diarrhea, constipation, and vomiting, mostly mild to moderate, most frequent during dose escalation, and declining over time at a stable dose.8 This is why the approved products are titrated up slowly. Less common but serious risks include pancreatitis, gallbladder disease, and dehydration-related kidney injury.10
Why does tirzepatide carry a boxed warning?
Its prescribing information carries a boxed warning about thyroid C-cell tumors, based on rodent studies showing dose- and duration-dependent tumors; the relevance to humans is unknown.10 Because of this uncertainty, the drug is contraindicated in people with a personal or family history of medullary thyroid carcinoma or with Multiple Endocrine Neoplasia syndrome type 2.10
Does tirzepatide cure diabetes or obesity?
No. It manages these conditions while it is being taken. Both diabetes and obesity are chronic, and stopping tirzepatide is generally followed by rising blood glucose or weight regain, similar to stopping blood-pressure medication.8 It should be understood as ongoing therapy, not a permanent cure, and its benefit on hard long-term outcomes is still being formally established.
Is research-grade tirzepatide powder the same as the prescription pens?
No. The human evidence described here was generated with pharmaceutical-grade tirzepatide administered under medical supervision. Research-grade or compounded powder is not FDA-evaluated for identity, purity, sterility, or potency, and dosing errors after reconstitution have caused documented overdoses.10 The two are not interchangeable in a safety or regulatory sense.
How is tirzepatide dosed and administered?
The approved products are given as a once-weekly subcutaneous injection, starting at a low dose and titrating upward over months to improve tolerability, reflecting the drug’s roughly five-day half-life and four-week time to steady state.910 Specific dosing is determined by a prescriber; the reference material on this site is educational and not a substitute for medical guidance.
References
- Willard FS, Douros JD, Gabe MBN, et al. Tirzepatide is an imbalanced and biased dual GIP and GLP-1 receptor agonist. JCI Insight. 2020;5(17):e140532. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7526454/
- Sun B, Willard FS, Feng D, et al. Structural determinants of dual incretin receptor agonism by tirzepatide. Proc Natl Acad Sci USA. 2022;119(13):e2116506119. https://www.pnas.org/doi/10.1073/pnas.2116506119
- Frías JP, Davies MJ, Rosenstock J, et al. Tirzepatide versus Semaglutide Once Weekly in Patients with Type 2 Diabetes (SURPASS-2). N Engl J Med. 2021;385:503-515. https://www.nejm.org/doi/full/10.1056/NEJMoa2107519
- Jastreboff AM, Aronne LJ, Ahmad NN, et al. Tirzepatide Once Weekly for the Treatment of Obesity (SURMOUNT-1). N Engl J Med. 2022;387:205-216. https://www.nejm.org/doi/abs/10.1056/NEJMoa2206038
- Malhotra A, Grunstein RR, Fietze I, et al. Tirzepatide for the Treatment of Obstructive Sleep Apnea and Obesity (SURMOUNT-OSA). N Engl J Med. 2024;391:1193-1205. https://www.nejm.org/doi/full/10.1056/NEJMoa2404881
- Aronne LJ, Horn DB, le Roux CW, et al. Tirzepatide as Compared with Semaglutide for the Treatment of Obesity (SURMOUNT-5). N Engl J Med. 2025;392:958-971. https://www.nejm.org/doi/full/10.1056/NEJMoa2416394
- Patel H, et al. Gastrointestinal adverse events and weight reduction in people with type 2 diabetes treated with tirzepatide in the SURPASS clinical trials. Diabetes Obes Metab. 2024. https://dom-pubs.onlinelibrary.wiley.com/doi/10.1111/dom.15333
- Rubino DM, et al. Gastrointestinal tolerability and weight reduction associated with tirzepatide in the SURMOUNT-1 to -4 trials. Diabetes Obes Metab. 2025. https://dom-pubs.onlinelibrary.wiley.com/doi/full/10.1111/dom.16176
- Tirzepatide. StatPearls. National Library of Medicine (NCBI Bookshelf). https://www.ncbi.nlm.nih.gov/books/NBK585056/
- MOUNJARO (tirzepatide) injection, for subcutaneous use — U.S. Prescribing Information (FDA/DailyMed). https://pi.lilly.com/us/mounjaro-uspi.pdf
- U.S. Food and Drug Administration. FDA Approves New Medication for Chronic Weight Management (Zepbound). https://www.fda.gov/news-events/press-announcements/fda-approves-new-medication-chronic-weight-management
- Eli Lilly and Company. FDA approves Zepbound (tirzepatide) as the first and only prescription medicine for moderate-to-severe obstructive sleep apnea in adults with obesity. https://investor.lilly.com/news-releases/news-release-details/fda-approves-zepboundr-tirzepatide-first-and-only-prescription
- Thomas MK, Nikooienejad A, Bray R, et al. Dual GIP and GLP-1 Receptor Agonist Tirzepatide Improves Beta-cell Function and Insulin Sensitivity in Type 2 Diabetes. J Clin Endocrinol Metab. 2021;106(2):388-396. https://academic.oup.com/jcem/article/106/2/388/6000489
Educational and research-information disclaimer: This article is provided for scientific and educational purposes only. It is not medical advice, a treatment protocol, or a recommendation to use tirzepatide or any related compound outside of care by a qualified, licensed healthcare professional. Tirzepatide is a prescription medicine with a boxed warning and significant contraindications; decisions about its use must be made with a clinician. Research-grade or compounded peptide products are not FDA-approved and are not evaluated for safety, purity, or potency. Nothing here should be interpreted as encouraging the acquisition or self-administration of unapproved products.