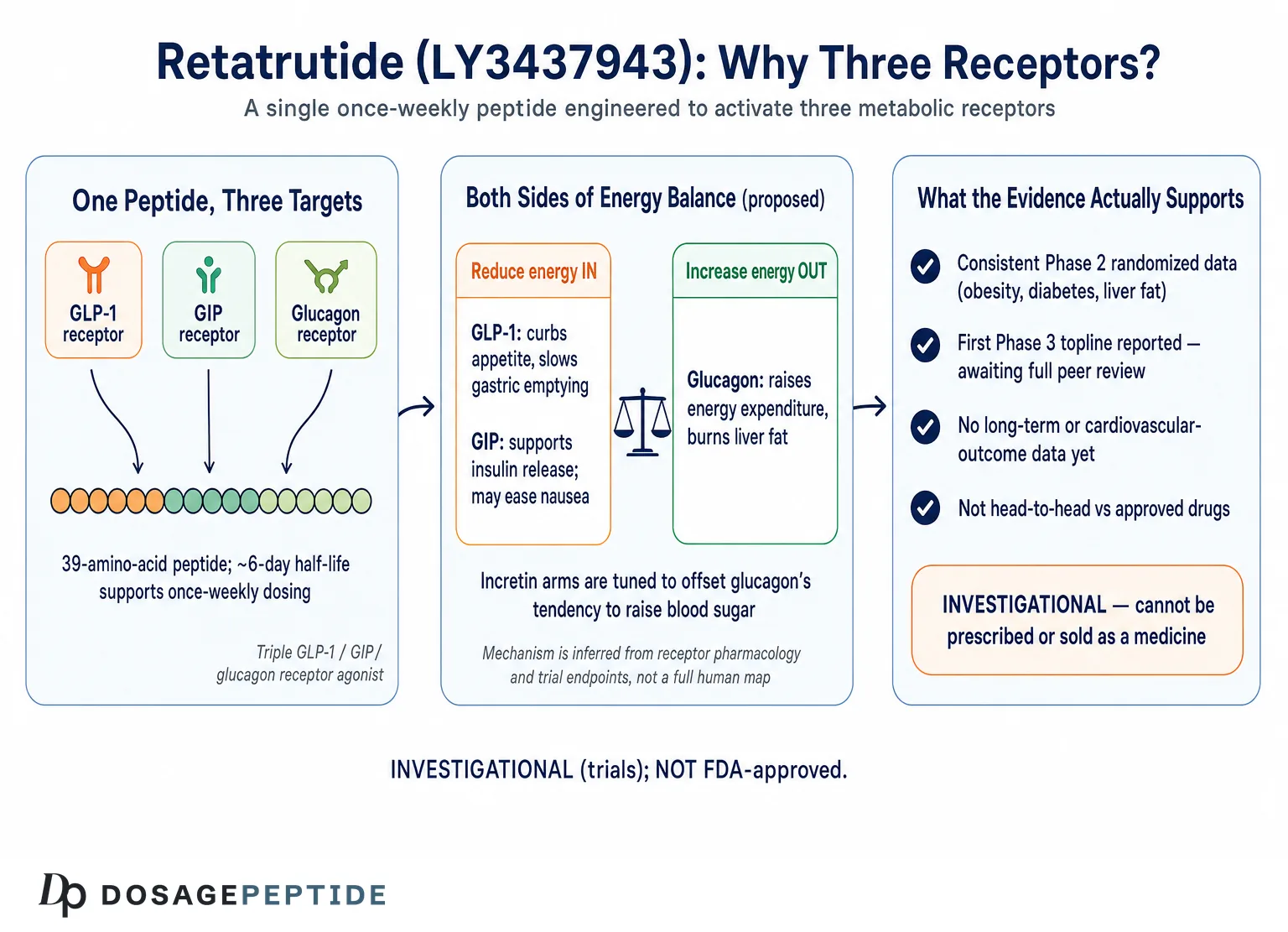
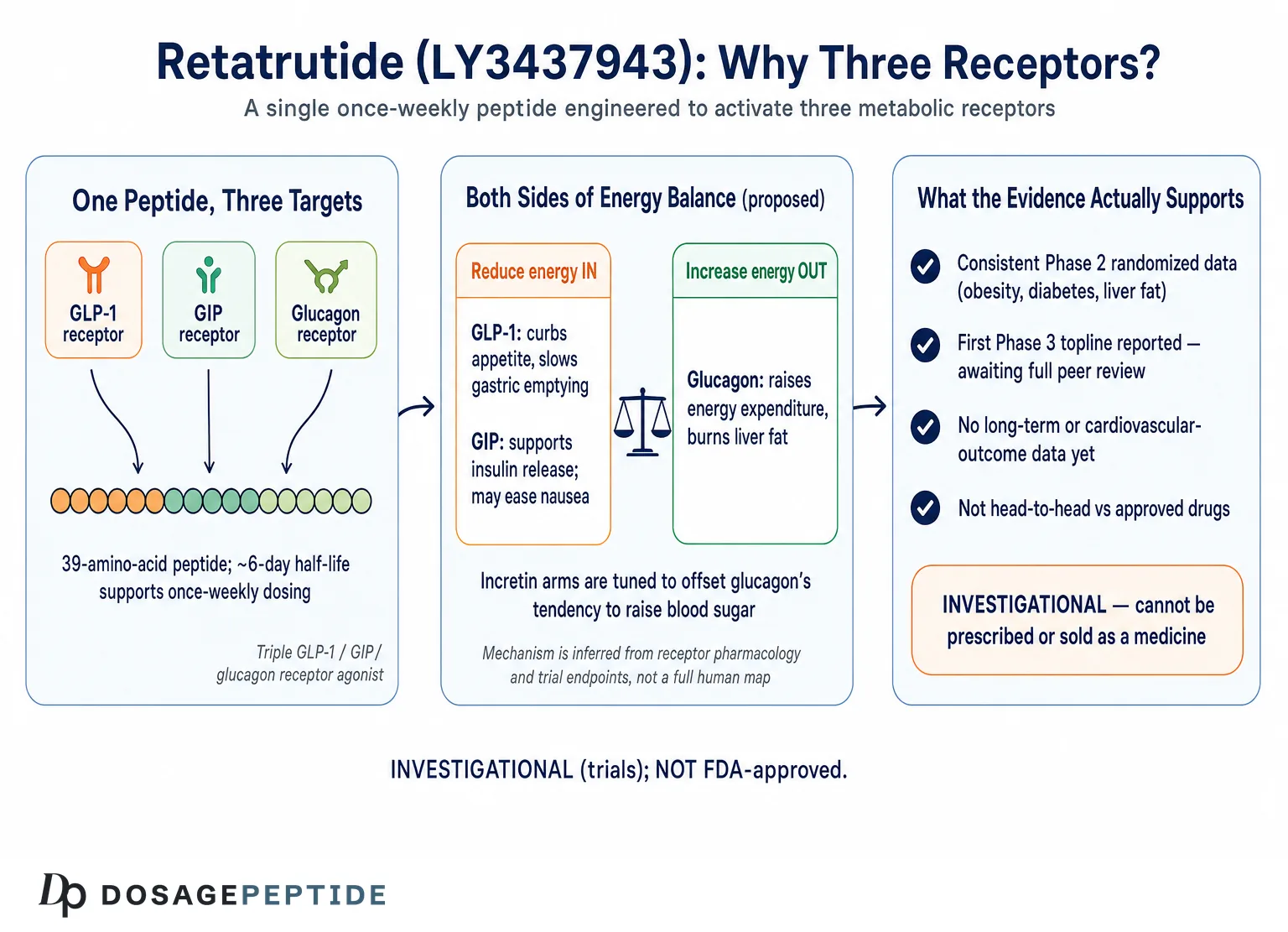
Retatrutide (development code LY3437943) is one of the most closely watched molecules in metabolic medicine, and the title of this article deliberately frames a question rather than a conclusion. It is a single synthetic peptide engineered to activate three different hormone receptors at once — the glucagon-like peptide-1 receptor (GLP-1R), the glucose-dependent insulinotropic polypeptide receptor (GIPR), and the glucagon receptor (GCGR). That “triple agonist” design has produced some of the largest body-weight reductions ever recorded in a pharmacological weight-management trial. It is easy to see why the popular framing calls it a therapy that is “reshaping weight-loss treatment.”1
The honest scientific position, however, is more measured. As of mid-2026, retatrutide is investigational. It is not approved by the U.S. Food and Drug Administration (FDA), the European Medicines Agency (EMA), or any other major regulator, and it cannot be lawfully prescribed or sold as a finished medicine.7 Its manufacturer, Eli Lilly, has completed a large Phase 2 program and reported the first positive Phase 3 topline results in 2026, but the full pivotal dataset, the safety database required for approval, and the long-term cardiovascular outcomes trial are not yet complete.5,6 In other words, the premise that retatrutide is “reshaping weight-loss therapies” is best treated as an open research question: the early-phase signal is genuinely remarkable, but the evidence is not yet the evidence of an approved therapy.
This article summarizes what the peer-reviewed primary literature and regulatory record actually establish about retatrutide — what the molecule is, how it is thought to work, the honest level of evidence behind the headline numbers, how it compares with other incretin agents, how it is studied in a research setting, its documented tolerability signals, and the substantial gaps that remain. It is written for an educational and research audience and does not provide medical advice. Nothing here should be read as a recommendation to obtain or use retatrutide outside of an authorized clinical trial.
What Retatrutide Is and Where It Came From
Retatrutide is a synthetic, single-chain peptide agonist that engages three distinct incretin-family and metabolic receptors simultaneously. It was discovered and developed by Eli Lilly, and its foundational pharmacology was published by Coskun and colleagues in Cell Metabolism in 2022 under the title “LY3437943, a novel triple glucagon, GIP, and GLP-1 receptor agonist for glycemic control and weight loss: from discovery to clinical proof of concept.”4 The molecule builds conceptually on two earlier waves of incretin science: first the single GLP-1 receptor agonists (such as liraglutide and semaglutide), then the dual GIP/GLP-1 receptor agonist tirzepatide. Retatrutide adds a third arm — glucagon-receptor agonism — to that lineage.4,10
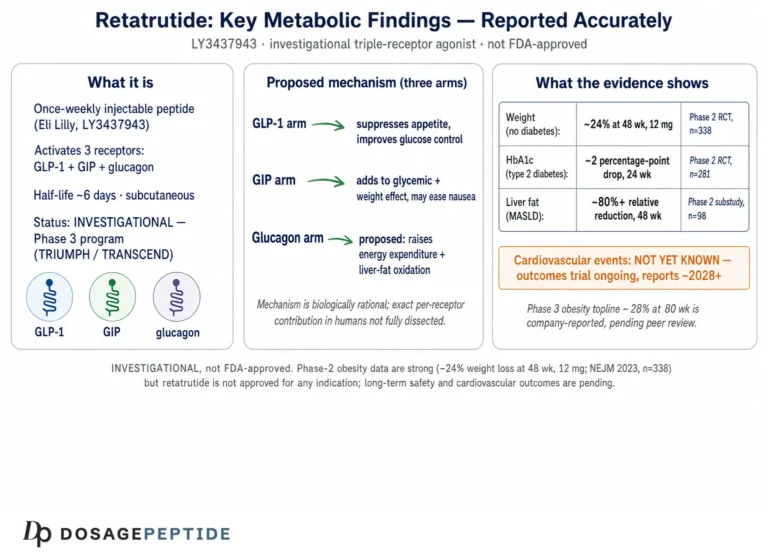
Structurally, retatrutide is a 39-amino-acid peptide backbone derived from the GIP sequence and modified with a C20 fatty-diacid moiety. That lipidation binds the peptide to circulating albumin, which slows renal clearance and proteolytic degradation and extends the half-life to roughly six days — long enough to support convenient once-weekly subcutaneous dosing.4 The engineering challenge was not simply to hit three receptors, but to hit them in a deliberately imbalanced ratio. The published receptor-activity profile describes relatively balanced potency at the glucagon and GLP-1 receptors with comparatively greater activity at the GIP receptor, a tuning intended to capture the metabolic upside of glucagon signaling (energy expenditure and hepatic fat handling) while avoiding the hyperglycemia that unopposed glucagon agonism would otherwise cause.4
The clinical name “retatrutide” follows the standard nomenclature for these agents, where the “-tide” stem denotes a peptide and the “glutide/trutide” family signals an incretin mechanism. Some commentators informally call it a “GLP-3” or “triple-G” agonist, but those are marketing shorthand, not pharmacological classifications. The precise and accurate description is a GLP-1/GIP/glucagon triple receptor agonist.1,4
It is worth emphasizing what retatrutide is not. It is not a naturally occurring hormone, not a compounded version of an approved drug, and not interchangeable with tirzepatide or semaglutide despite belonging to the same broad family. Each of those molecules has a distinct receptor profile, distinct pharmacokinetics, and its own separate regulatory dossier. Research-facing reference material such as the retatrutide 12 mg vial protocol overview exists because the compound is distributed as a lyophilized research peptide in a variety of vial masses, but that distribution channel is entirely separate from the regulated pharmaceutical product that Lilly is developing. The material sold for laboratory use has not been through the manufacturing, purity, and safety controls that define an approved medicine.7
The scientific interest in the compound stems from a simple hypothesis: if activating one incretin receptor (GLP-1) produces meaningful weight loss, and activating two (GIP + GLP-1) produces more, then adding a third complementary mechanism — one that increases energy expenditure rather than only reducing intake — might push efficacy further still. The trials described below were designed to test exactly that hypothesis, and the early results are the reason retatrutide is discussed at all.
The historical arc is worth appreciating because it frames how quickly this field has moved. GLP-1 biology was elucidated over decades, and the first GLP-1 receptor agonists reached the clinic for type 2 diabetes before their weight-management potential was fully appreciated. The recognition that these agents produced substantial, sustained weight loss reoriented an entire therapeutic area and created intense scientific and commercial interest in “unimolecular” multi-agonists — single peptides engineered to hit several receptors at once rather than combining separate drugs. Retatrutide is a product of that unimolecular design philosophy, and it represents, at least conceptually, the current frontier of how many complementary metabolic targets a single well-tolerated molecule can engage. Whether three targets is the optimal number, or whether the added glucagon arm justifies its own distinct risk considerations, is exactly what the ongoing development program is designed to determine.4,10
The Molecular Mechanism: Why Three Receptors
To understand retatrutide, it helps to consider what each of its three targets does on its own. The three receptors regulate overlapping but distinct arms of metabolic physiology, and the therapeutic thesis is that combining them produces effects that no single- or dual-receptor agonist fully replicates.1,4
The GLP-1 receptor is the best-characterized target. GLP-1 is an incretin hormone released from the gut after eating. Agonism at GLP-1R enhances glucose-dependent insulin secretion from pancreatic beta cells, suppresses inappropriate glucagon release, slows gastric emptying, and acts on hypothalamic and hindbrain circuits to reduce appetite and food intake. This is the mechanism responsible for the satiety and glycemic benefits shared across the entire incretin drug class.4,10
The GIP receptor is the second incretin target. GIP also potentiates glucose-dependent insulin secretion, and there is evidence that GIPR agonism improves the tolerability of the GLP-1 component — potentially blunting nausea — while contributing independently to metabolic and adipose-tissue effects. The precise contribution of GIP agonism remains an area of active scientific debate, but its inclusion is central to the tirzepatide and retatrutide designs.4
The glucagon receptor is what distinguishes retatrutide from every currently approved incretin drug. Glucagon is usually thought of as the hormone that raises blood sugar, which sounds counterproductive in a diabetes or obesity agent. But glucagon also increases resting energy expenditure, stimulates hepatic fat oxidation (breaking down fat stored in the liver), and promotes lipolysis. The design goal is to harness those catabolic, energy-burning effects while the simultaneous GLP-1 and GIP activity keeps blood glucose controlled and offsets glucagon’s hyperglycemic tendency.1,4 In effect, the GLP-1/GIP arms and the glucagon arm are engineered to counterbalance one another so that the net result is weight loss plus improved — not worsened — glycemic control.
This mechanistic combination is why retatrutide is theorized to act on both sides of the energy-balance equation. GLP-1-mediated appetite suppression and delayed gastric emptying reduce energy intake, while glucagon-driven thermogenesis and fat oxidation increase energy output. Most weight-management drugs work almost entirely through reduced intake; the added energy-expenditure component is the mechanistic novelty that its developers argue explains the unusually large weight reductions seen in trials.1,3,4
The liver is a particularly instructive tissue for understanding this mechanism. Glucagon-receptor agonism directly promotes hepatic lipid clearance, which may explain why retatrutide produced dramatic reductions in liver fat in dedicated imaging studies — effects larger and faster than would be expected from weight loss alone.3 That observation, discussed in the evidence section below, is one of the strongest pieces of support for the idea that the glucagon arm contributes something mechanistically distinct rather than simply amplifying GLP-1 biology.
A useful way to picture the design is as a system of complementary and partly opposing forces. The GLP-1 arm reduces how much energy enters the body by curbing appetite and slowing the rate at which the stomach empties, so meals feel more filling and are eaten in smaller amounts. The GIP arm reinforces glucose-dependent insulin release and appears to soften the gastrointestinal burden of GLP-1 activity, which may allow higher effective dosing than a GLP-1-only agent could tolerate. The glucagon arm then acts on the output side of the ledger, nudging resting energy expenditure upward and mobilizing stored lipid, particularly in the liver. Because glucagon on its own would raise blood glucose, the simultaneous incretin activity is what keeps that liability in check; the whole point of the imbalanced tuning is to let the beneficial glucagon effects surface while the GLP-1 and GIP components neutralize its hyperglycemic tendency.1,4
This balance is delicate, and it is the reason the specific ratio of receptor potencies matters so much. Too much glucagon activity relative to the incretin arms, and glycemic control would deteriorate; too little, and the added energy-expenditure benefit that differentiates retatrutide from tirzepatide would be lost. The published pharmacology suggests Lilly’s medicinal chemists spent considerable effort tuning this ratio, and the fact that the diabetes trial showed improved — not worsened — glycemic control alongside weight loss is the clinical evidence that the balance was, at least in that population and timeframe, achieved.2,4
It is important to note that this mechanistic account is built on preclinical pharmacology, receptor-binding assays, and inference from clinical endpoints — not on a complete, tissue-by-tissue map of drug action in humans. The receptor-level story is well supported; the precise quantitative contribution of each arm to the overall clinical effect in people is still being worked out. In particular, the role of GIP-receptor agonism remains scientifically contested across the incretin field, with some evidence favoring GIP-receptor agonism and other lines of work exploring GIP-receptor antagonism — a reminder that even within an approved-adjacent class, fundamental mechanistic questions are unresolved.4,10
The Key Evidence: What the Trials Actually Show
The evidence base for retatrutide is best described as a strong and internally consistent Phase 2 program, followed by the first — but not yet complete — Phase 3 readouts. Framing the evidence level honestly matters: Phase 2 trials establish proof of concept and dose response; they do not carry the statistical power, duration, or breadth of an approval-grade dataset.
The landmark study is the Phase 2 obesity trial by Jastreboff and colleagues, published in the New England Journal of Medicine in June 2023.1 This randomized, double-blind, placebo-controlled trial enrolled 338 adults with obesity (BMI ≥30) or overweight (BMI 27–30 with a weight-related condition). Participants received once-weekly subcutaneous retatrutide at 1, 4, 8, or 12 mg, or placebo, for 48 weeks. The least-squares mean percentage change in body weight was as follows.
| Weekly dose (Phase 2, 48 weeks) | Mean body-weight change |
|---|---|
| Placebo | −2.1% |
| 1 mg | −8.7% |
| 4 mg (combined) | −17.1% |
| 8 mg (combined) | −22.8% |
| 12 mg | −24.2% |
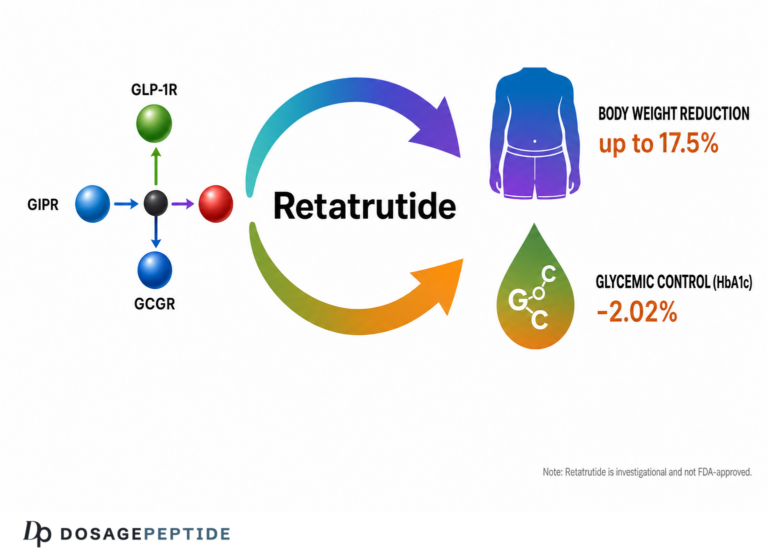
The 24.2% mean reduction at the 12 mg dose was, at the time of publication, among the largest weight reductions reported for any pharmacological agent, and notably the weight-loss curve had not clearly plateaued by week 48 at the higher doses — suggesting the ceiling had not been reached.1 Those numbers are the origin of nearly every “reshaping weight loss” headline about this compound.
A parallel Phase 2 type 2 diabetes trial by Rosenstock and colleagues was published in The Lancet in 2023.2 It enrolled 281 adults with type 2 diabetes (mean HbA1c 8.3%, mean BMI 35.0) and tested retatrutide doses from 0.5 to 12 mg over 36 weeks against both placebo and the active GLP-1 comparator dulaglutide 1.5 mg. HbA1c fell by up to about 2.2%, with an HbA1c below 6.5% achieved in up to 82% of participants, and body weight fell by up to 16.9% at 36 weeks — again without a clear plateau.2
A third pillar is the MASLD (fatty-liver) substudy published by Sanyal and colleagues in Nature Medicine in 2024.3 Among 98 participants with metabolic dysfunction-associated steatotic liver disease (≥10% liver fat by MRI-PDFF), retatrutide produced relative reductions in liver-fat content of roughly 81–82% at the 8 and 12 mg doses at 24 weeks, versus essentially no change on placebo. Normal liver fat (<5%) was reached by the large majority of participants on the higher doses — approximately 79% at the 8 mg dose and 86% at the 12 mg dose by 24 weeks.3 These were among the most pronounced pharmacological liver-fat reductions reported in a clinical study.
The most recent development is Phase 3. In 2026 Eli Lilly reported positive topline results from TRIUMPH-1, a large pivotal obesity trial of roughly 2,300 participants, in which all studied doses met their primary and key secondary endpoints; the company reported an average weight reduction at the highest dose in the high-20s percent range, with a substantial proportion of participants losing 30% or more of body weight.5 These are press-release topline figures pending full peer-reviewed publication and regulatory review, and they should be read as promising interim confirmation rather than final, scrutinized results.5,6
A dedicated body-composition substudy in the type 2 diabetes program added an important layer of detail. Rather than reporting only total scale weight, it used imaging to partition the weight change into fat mass and lean mass, addressing a common and legitimate concern about potent weight-loss agents: whether the loss is predominantly fat or whether it also strips away muscle.8 This kind of granular endpoint is exactly what distinguishes a rigorous program from a headline-weight-loss story, and it is one reason the retatrutide dataset is taken seriously by the metabolic research community even at the Phase 2 stage.
Beyond the individual trials, a systematic review and meta-analysis of retatrutide randomized controlled trials has attempted to pool the available evidence and quantify effects with greater precision.9 Meta-analyses of this kind are valuable because they aggregate data and formalize uncertainty, but they inherit the limitations of the underlying trials: pooling short, Phase 2 studies cannot manufacture the long-term or outcome data that those studies never collected. A meta-analysis of early-phase trials sharpens the estimate of a short-term effect; it does not upgrade the evidence to the level of a completed Phase 3 program.9
Taken together, the honest evidence level is: consistent, high-quality Phase 2 randomized data across three metabolic indications, plus early positive Phase 3 topline data. That is a genuinely strong early signal. It is not the same as a completed, regulator-reviewed body of evidence, and it does not establish long-term safety or hard clinical outcomes such as reduced heart attacks, strokes, or deaths. The distinction is not pedantic: many compounds with impressive Phase 2 results have failed to replicate or have revealed safety problems in larger, longer trials, which is precisely why the regulatory system requires Phase 3 and outcomes data before a drug is called a therapy.
How Retatrutide Compares With Other Incretin Agents
Retatrutide is best understood by placing it alongside the incretin agents that preceded it. The clearest way to compare is by receptor mechanism and by the magnitude of weight change reported in each drug’s pivotal trials — while remembering that cross-trial comparisons are indirect and should be interpreted cautiously, because trial populations, durations, and designs differ.
| Agent | Receptor mechanism | Regulatory status (mid-2026) | Representative weight change |
|---|---|---|---|
| Semaglutide | GLP-1 (single) | Approved | ~15% (obesity Phase 3) |
| Tirzepatide | GIP + GLP-1 (dual) | Approved | ~21% (obesity Phase 3, high dose) |
| Retatrutide | GLP-1 + GIP + glucagon (triple) | Investigational | ~24% (Phase 2, 12 mg, 48 wk) |
The pattern is a stepwise increase in apparent efficacy as receptor targets are added, which is the central narrative behind the “next-generation” framing.1,10 But several caveats deserve emphasis. First, the retatrutide figure comes from a 48-week Phase 2 trial, whereas the semaglutide and tirzepatide figures come from larger, longer Phase 3 trials that formed the basis for approval. Comparing a Phase 2 result against Phase 3 results systematically flatters the newer, less-tested drug. Second, the trials enrolled different populations under different protocols, so numeric differences cannot be attributed cleanly to the drugs themselves. Only a head-to-head randomized trial could settle relative efficacy, and no such definitive comparison has been published.1,2
The mechanistic distinction is real, however. Semaglutide is a pure GLP-1 receptor agonist. Tirzepatide adds GIP agonism. Retatrutide adds glucagon agonism on top of both. The glucagon arm is the genuinely novel element, and it is the plausible mechanistic explanation for two observations that set retatrutide apart in its trials: the unusually large liver-fat reductions and the fact that the weight-loss curves had not plateaued at 48 weeks.1,3
That added mechanism also carries a distinctive trade-off. Because glucagon agonism raises energy expenditure and can transiently affect heart rate, retatrutide’s cardiovascular tolerability profile is not identical to that of the pure GLP-1 or dual GIP/GLP-1 agents, and it requires its own dedicated evaluation rather than assuming class equivalence (see the safety section).1 Similarly, the glucagon component means retatrutide’s effect on glycemic control had to be demonstrated directly — which the Phase 2 diabetes trial did — rather than assumed.2
A final comparative point concerns positioning within the treatment landscape. Because semaglutide and tirzepatide are already approved and widely used, they define the standard against which retatrutide will be judged — not against placebo. For retatrutide to change practice, it will ultimately need to demonstrate not just large weight loss versus placebo, but a favorable overall benefit-risk profile relative to therapies that are already available, affordable in some markets, and backed by years of post-marketing safety data. That is a higher bar than a Phase 2 placebo-controlled result clears, and it is another reason the “reshaping therapy” framing is premature until head-to-head and long-term data exist.1,10 For research-facing readers comparing dosing formats across the incretin class, the general reconstitution and unit-conversion principles are broadly similar across these lyophilized peptides, and a general orientation is available through the dosage-protocol index. But similarity in handling should not be mistaken for equivalence in pharmacology, approval status, or evidence base. Retatrutide sits at a fundamentally earlier and less-validated point in the development pipeline than its approved cousins.
Research Models and Trial Methodology
The retatrutide evidence base was built through a conventional, well-designed drug-development sequence, and understanding that methodology is essential to interpreting the results honestly. The trials share the design features that make randomized evidence credible: randomization, blinding, placebo control, pre-specified endpoints, and dose-ranging arms.
The preclinical foundation came first. Coskun and colleagues characterized LY3437943 in receptor-binding and functional assays and in animal models, establishing the imbalanced triple-agonist profile and demonstrating glycemic control and weight loss before any human dosing.4 This is the standard bridge from molecule to clinic: in vitro receptor pharmacology, then rodent and other animal metabolic models, then first-in-human safety and pharmacokinetic work.
The Phase 2 trials were the pivotal proof-of-concept step. Both the obesity and diabetes trials used a randomized, double-blind, placebo-controlled, parallel-group design with multiple active dose arms — the design most capable of establishing a causal, dose-dependent drug effect while minimizing bias.1,2 The diabetes trial added an active comparator (dulaglutide), which strengthens interpretation by benchmarking retatrutide against an established therapy rather than against placebo alone.2 Both trials used gradual dose-escalation (titration) schedules — starting low and stepping up — specifically to characterize how tolerability and efficacy evolve with dose, and the obesity trial directly tested whether a lower 2 mg starting dose improved tolerability versus a 4 mg start.1
Endpoint measurement was rigorous and, importantly, often objective rather than self-reported. Body weight was measured directly; HbA1c is a laboratory biomarker of average glycemia; and the liver-fat substudy used MRI-PDFF, a validated quantitative imaging technique, rather than a proxy such as liver enzymes.1,2,3 A separate body-composition substudy used imaging to distinguish fat-mass from lean-mass changes in participants with type 2 diabetes, adding granularity that simple scale weight cannot provide.8 The reliance on objective, instrument-based endpoints is a meaningful strength of the program.
The Phase 3 TRIUMPH program represents the scale-up needed for regulatory approval. It comprises multiple large pivotal trials enrolling several thousand participants across obesity and diabetes indications, plus a separate, large, long-duration cardiovascular outcomes trial (CVOT) designed to test whether the drug affects hard endpoints such as heart attack, stroke, and cardiovascular death.5,6 The CVOT is methodologically the most important piece for long-term safety, because Phase 2 trials are simply too small and too short to detect rare but serious outcomes. Additional registered trials examine specific populations, including a study of renal function in people with overweight or obesity and chronic kidney disease.6
The methodological limitations are equally important to state. Phase 2 trials, however well designed, are relatively small (hundreds, not thousands, of participants) and relatively short (36–48 weeks). They typically exclude people with significant cardiovascular or other serious comorbidities, which limits how far their safety findings can be generalized. And they are powered to detect weight and glycemic effects, not to detect rare adverse events or to prove durability over years. These are not flaws in the trials; they are inherent properties of the Phase 2 stage that make the ongoing Phase 3 program indispensable before any firm conclusion about the drug’s real-world role can be drawn.1,2,9
Safety and Tolerability Signals
The safety data available for retatrutide come almost entirely from the Phase 2 program and from early Phase 3 topline reporting. They should be read as an early, incomplete tolerability picture, not as a settled safety profile. Within that limitation, the signals are broadly consistent with the incretin class, with some features specific to the glucagon arm.
The most common adverse events were gastrointestinal — nausea, diarrhea, vomiting, and constipation — occurring more frequently with retatrutide than with placebo.1 These events were clearly dose-related, mostly mild to moderate in severity, occurred predominantly during dose escalation, and were partially mitigated by using a lower starting dose. Reported nausea rates ranged from roughly 14% at the 1 mg dose to around 60% at the 12 mg dose.1 Adverse events leading to discontinuation of the study drug occurred in approximately 6–16% of retatrutide participants across dose groups, versus none on placebo — a meaningful discontinuation signal that scales with dose.1
| Safety domain (Phase 2) | Reported signal |
|---|---|
| Gastrointestinal events | Most common; dose-related; mostly mild-moderate; worst during titration |
| Nausea (range across doses) | ~14% (1 mg) to ~60% (12 mg) |
| Discontinuation for adverse events | ~6–16% on retatrutide; 0% on placebo |
| Resting heart rate | Dose-dependent rise, peaked ~24 weeks, then declined |
| Blood pressure / triglycerides | Reductions reported at higher doses |
The most mechanism-specific signal is the effect on heart rate. Retatrutide produced a dose-dependent increase in resting heart rate that peaked at around 24 weeks and then declined thereafter.1 Reported increases were modest in magnitude (on the order of a few beats per minute, larger at higher doses), and are consistent with the known cardiovascular effects of both GLP-1 receptor agonism and glucagon signaling. At the same time, the trials reported favorable changes in some cardiovascular risk markers, including reductions in systolic blood pressure and triglycerides at higher doses.1 The Phase 2 data did not show a clear dose-dependent arrhythmia signal, but — critically — Phase 2 trials are not powered to detect rare cardiac events, and they generally excluded higher-risk cardiovascular patients.1
This is precisely why the ongoing cardiovascular outcomes trial matters so much. The net cardiovascular effect of a drug that both lowers blood pressure and modestly raises heart rate cannot be inferred from surrogate markers; it must be measured directly in a large, long trial with adjudicated hard endpoints. Until that trial reports, statements about retatrutide’s cardiovascular safety must remain provisional.5,6
Several other categories of risk remain uncharacterized in the public data. Long-term effects (beyond one to two years) are unknown. Effects during pregnancy and lactation have not been established, and incretin agents are generally contraindicated in pregnancy. As with other GLP-1-based agents, the class carries labeled attention to concerns such as pancreatitis, gallbladder events, and — based on rodent data for the class — a theoretical thyroid C-cell tumor consideration; whether and to what degree these apply specifically to retatrutide will be defined by its own complete safety database, not by class assumption.1,9
One further tolerability nuance deserves mention: the glucagon arm’s tendency to mobilize hepatic energy stores and raise metabolic rate means that laboratory parameters such as glucose handling, lipids, and markers of liver and kidney function are logically important to monitor, which is one reason dedicated substudies and a renal-function trial were built into the program.3,6,8 A drug that reduces liver fat so dramatically is clearly doing significant work on hepatic metabolism, and characterizing whether that work is uniformly beneficial across diverse patients — including those with pre-existing liver or kidney disease who were largely excluded from the early trials — is a live scientific question rather than a settled one.
Because the compound is investigational, there is also no established, regulator-reviewed dosing regimen, no approved patient-selection criteria, and no professional monitoring framework for use outside a trial. Any handling of research-grade material occurs entirely outside the safety infrastructure — medical supervision, pharmacovigilance, quality-controlled manufacturing — that surrounds an approved medicine. That absence is itself a safety consideration, and arguably the most important one: the trial results that make retatrutide interesting were generated under carefully controlled conditions with screening, titration, and monitoring that simply do not exist outside a clinical study. Extrapolating those results to unsupervised settings is not supported by any evidence.
Handling and Reconstitution in a Research Context
This section is included because retatrutide is commonly distributed to laboratories as a lyophilized (freeze-dried) research peptide, and questions about reconstitution are among the most frequently searched. It is provided strictly as general laboratory-handling information for authorized research settings. It is not dosing guidance, not a protocol for human use, and not an endorsement of self-administration, which would be unsafe and, for an unapproved compound, outside any lawful therapeutic framework.
Research-grade retatrutide is typically supplied as a white lyophilized powder in sealed vials of varying nominal mass. The powder is generally reconstituted with bacteriostatic water for research purposes; the volume of diluent added determines the final concentration. The core relationship is straightforward: concentration = peptide mass ÷ diluent volume. For example, reconstituting a vial with more solvent yields a lower concentration per unit volume, and vice versa. This arithmetic, and the conversion between milligrams, micrograms, and the unit markings on an insulin-style syringe, are the source of most handling errors and are the reason vial-specific reference material exists for different masses.
Because vials are sold in a range of sizes, the same target concentration requires different diluent volumes for each. Reference overviews organized by vial mass — for example the 6 mg vial overview, the 10 mg vial reconstitution reference, the 20 mg vial overview, and the 30 mg vial overview — exist precisely because the reconstitution math differs by vial size even when the underlying peptide is identical.
General handling principles that apply to lyophilized peptides of this type include: introducing diluent slowly against the vial wall rather than directly onto the powder pellet; allowing the peptide to dissolve without vigorous shaking, since aggressive agitation can shear peptide structure; inspecting the reconstituted solution for clarity and absence of particulates; and storing the material under cold-chain conditions. Lyophilized peptide is generally stored frozen; once reconstituted, it is typically refrigerated and used within a limited window, as the aqueous form is less stable than the dry powder. Bacteriostatic water contains a preservative that supports multi-use handling, but sterility and stability still degrade over time.
Two honest caveats dominate this topic. First, the purity and identity of any research-grade material cannot be assumed. Unlike an approved medicine, research peptides are not manufactured under the same regulatory quality systems; content, purity, and even correct identity can vary between suppliers, and independent third-party analytical testing (such as mass spectrometry and HPLC) is the only meaningful check. Second, none of this handling information changes the compound’s status: retatrutide is investigational, and reconstitution technique has nothing to do with whether use is safe, appropriate, or lawful outside a clinical trial. The presence of detailed handling references reflects demand, not endorsement.
For orientation across different vial masses without implying any human-use protocol, the consolidated 24 mg vial reference illustrates how the same reconstitution logic scales with vial size. Again, these are laboratory-arithmetic references, not therapeutic instructions.
Limitations and the Human-Evidence Gap
It is worth stating the limitations of the retatrutide evidence base directly and without softening, because the gap between the enthusiasm surrounding the compound and the maturity of its evidence is the single most important thing for a reader to understand.
First, the pivotal efficacy data are still Phase 2. The widely cited 24.2% weight-loss figure comes from a 338-person, 48-week Phase 2 trial.1 Phase 2 trials are designed to establish proof of concept and to select doses for Phase 3; they are not designed to be the final word on efficacy or safety. The first Phase 3 topline results are encouraging but are, as of this writing, press-release figures awaiting full peer-reviewed publication and regulatory scrutiny.5 Topline announcements report headline numbers without the full dataset, subgroup analyses, and adverse-event detail that peer review and regulatory review demand.
Second, duration is short relative to the intended use. Obesity and type 2 diabetes are chronic conditions that may involve years or decades of treatment, yet the published trials span 36–48 weeks. Whether the weight loss is durable, whether it is regained after discontinuation (as it is with other incretin agents), and how the drug behaves over multi-year exposure are simply unknown from the current data.1,2
Third, hard clinical outcomes have not been demonstrated. The trials measured weight, HbA1c, liver fat, and blood-pressure markers — all intermediate or surrogate endpoints. They did not show that retatrutide reduces heart attacks, strokes, kidney failure, or death. Those outcomes are the purpose of the ongoing cardiovascular outcomes and renal-function trials, and until they report, any claim that retatrutide improves long-term health outcomes is unproven.5,6
Fourth, the studied populations were selective. Trial participants were enrolled under specific inclusion and exclusion criteria that generally screened out people with significant cardiovascular disease and other serious comorbidities. Real-world populations are more heterogeneous, and safety and efficacy can differ substantially outside the controlled trial setting.1,9
Fifth, and most importantly for the framing of this article, retatrutide is not an established therapy. It cannot be prescribed. There is no approved indication, no approved dose, no approved label, and no regulatory determination that its benefits outweigh its risks for any patient population. The material available through research channels is not a medicine and has not passed the manufacturing and safety controls that define one. Descriptions of retatrutide as something that is already “reshaping weight-loss therapy” run ahead of the evidence: what the data actually show is a compound with an exceptional early-phase signal that is still being tested to determine whether it can become such a therapy.7
None of this is meant to diminish the science. The Phase 2 program is genuinely strong, the mechanism is elegant, and the early Phase 3 signal is promising. But strong early evidence and an approved therapy are different things, and conflating them is exactly the error a responsible, evidence-cautious summary must avoid. The correct posture is calibrated interest: this is one of the most interesting molecules in metabolic research, and its ultimate role remains an open question pending the completion and review of its Phase 3 program.9
Regulatory Status
As of mid-2026, retatrutide is an investigational drug that is not approved by any major regulatory agency. It has not received marketing authorization from the FDA in the United States, the EMA in Europe, or comparable regulators elsewhere. It cannot be lawfully marketed, prescribed, or dispensed as a finished pharmaceutical product, and any such product does not exist in the regulated market.7
The development pathway is well advanced but incomplete. Eli Lilly has completed its Phase 2 program across obesity, type 2 diabetes, and MASLD, and in 2026 reported the first positive Phase 3 topline results from the TRIUMPH obesity program.5 The company has publicly indicated an intention to file a New Drug Application (NDA) with the FDA, with the pivotal obesity trials forming the core of the efficacy package.5,6 Public reporting as of this writing indicates the NDA had not yet been filed and that no Fast Track or Breakthrough Therapy designation had been publicly confirmed; independent commentary generally projects potential approval no earlier than 2027–2028 assuming the remaining trials read out favorably and are accepted on review.7 These timelines are projections, not commitments, and can shift with trial results, regulatory questions, or manufacturing considerations.
Because retatrutide is unapproved, the material sold through research-chemical and peptide-supply channels occupies a very different regulatory category from a medicine. Such material is typically labeled — and lawfully permitted only — for laboratory research use, explicitly not for human consumption. It is not manufactured under the pharmaceutical quality systems that govern approved drugs, is not subject to the same purity, potency, sterility, and labeling requirements, and is not accompanied by regulator-reviewed prescribing information or pharmacovigilance. Purchasing, possessing, or using such material for human purposes falls outside any approved therapeutic framework and outside the safety protections that regulation exists to provide.7
The practical upshot is simple. The scientifically legitimate way to receive retatrutide is through enrollment in an authorized clinical trial, where dosing, monitoring, and safety oversight are provided under an approved protocol and ethical review. Everything else — including research-grade vials distributed for laboratory use — sits outside the medical system, and the regulatory status is not a technicality but a direct reflection of the fact that the drug’s benefit-risk balance for any human indication has not yet been formally established.7,9
Frequently Asked Questions
Is retatrutide FDA approved?
No. As of mid-2026, retatrutide is investigational and is not approved by the FDA, the EMA, or any other major regulator. It cannot be lawfully prescribed or sold as a finished medicine. Eli Lilly has reported positive Phase 3 topline data and has stated an intention to file for approval, but no approval had been granted at the time of writing.5,7
What makes retatrutide a “triple agonist”?
Retatrutide is a single peptide that simultaneously activates three receptors: the GLP-1 receptor, the GIP receptor, and the glucagon receptor. Adding glucagon-receptor agonism — which increases energy expenditure and hepatic fat oxidation — is what distinguishes it from single-receptor GLP-1 agonists and dual GIP/GLP-1 agonists.1,4
How much weight loss did retatrutide produce in trials?
In the Phase 2 obesity trial, the highest dose (12 mg weekly) produced a mean body-weight reduction of about 24.2% at 48 weeks, versus 2.1% on placebo, and the curve had not clearly plateaued.1 Early Phase 3 topline reporting described average reductions in the high-20s percent range at the top dose, pending full publication.5 These are trial results, not outcomes to expect outside a supervised trial.
How does retatrutide compare with semaglutide and tirzepatide?
Semaglutide targets one receptor (GLP-1), tirzepatide targets two (GIP + GLP-1), and retatrutide targets three (adding glucagon). Reported weight reductions increase across that progression, but retatrutide’s figures come from Phase 2 trials while the others come from Phase 3 approval trials, so the comparison is indirect and cannot establish which is truly superior without a head-to-head study.1,10
What are the main side effects seen in trials?
The most common were gastrointestinal — nausea, vomiting, diarrhea, and constipation — which were dose-related, mostly mild to moderate, and worst during dose escalation. A dose-dependent, transient increase in resting heart rate was also observed. Adverse events led some participants (roughly 6–16% depending on dose) to discontinue.1 Long-term and cardiovascular-outcome safety remain under investigation.
Does retatrutide help with fatty liver disease?
In a Phase 2a substudy, retatrutide produced large reductions in liver fat measured by MRI — on the order of 80% or more at higher doses at 24 weeks, with most higher-dose participants reaching normal liver-fat levels.3 This is a promising but early finding in a specific research population; it does not constitute an approved treatment for liver disease.
Can I buy retatrutide?
Retatrutide is not available as an approved prescription medicine. Material sold through research-chemical channels is labeled for laboratory research use only, not for human consumption, and is not manufactured under pharmaceutical quality standards. The only legitimate way to receive retatrutide for a health purpose is through enrollment in an authorized clinical trial.7
Why does the weight-loss curve “not plateau” — is that good?
In the 48-week Phase 2 trials, weight was still declining at the higher doses when the trials ended, meaning maximum effect may not have been reached.1,2 That suggests substantial potency, but it is not automatically “good” without longer data: it also underscores that durability, plateau point, and long-term safety over years are still unknown and are the reason the Phase 3 program is essential.
References
- Jastreboff AM, Kaplan LM, Frías JP, et al. Triple–Hormone-Receptor Agonist Retatrutide for Obesity — A Phase 2 Trial. New England Journal of Medicine. 2023;389(6):514–526. doi:10.1056/NEJMoa2301972. PMID:37366315. https://www.nejm.org/doi/full/10.1056/NEJMoa2301972
- Rosenstock J, Frias J, Jastreboff AM, et al. Retatrutide, a GIP, GLP-1 and glucagon receptor agonist, for people with type 2 diabetes: a randomised, double-blind, placebo and active-controlled, parallel-group, phase 2 trial conducted in the USA. The Lancet. 2023;402(10401):529–544. doi:10.1016/S0140-6736(23)01053-X. https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(23)01053-X/abstract
- Sanyal AJ, Kaplan LM, Frias JP, et al. Triple hormone receptor agonist retatrutide for metabolic dysfunction-associated steatotic liver disease: a randomized phase 2a trial. Nature Medicine. 2024;30:2037–2048. doi:10.1038/s41591-024-03018-2. https://www.nature.com/articles/s41591-024-03018-2
- Coskun T, Urva S, Roell WC, et al. LY3437943, a novel triple glucagon, GIP, and GLP-1 receptor agonist for glycemic control and weight loss: from discovery to clinical proof of concept. Cell Metabolism. 2022;34(9):1234–1247. doi:10.1016/j.cmet.2022.07.013
- Eli Lilly and Company. Lilly’s triple agonist, retatrutide, delivered powerful weight loss in pivotal Phase 3 obesity trial. News release, May 21, 2026 (TRIUMPH-1 topline results; also distributed via PR Newswire). https://investor.lilly.com/news-releases/news-release-details/lillys-triple-agonist-retatrutide-delivered-powerful-weight-loss
- ClinicalTrials.gov. A Study of Retatrutide (LY3437943) on Renal Function in Participants With Overweight or Obesity and Chronic Kidney Disease (NCT05936151); TRIUMPH Phase 3 program registrations. https://clinicaltrials.gov/study/NCT05936151
- U.S. Food and Drug Administration. Drugs@FDA: FDA-Approved Drugs (searchable approvals database). A search for retatrutide returns no approved product as of mid-2026, directly confirming its investigational status; corroborated by the ongoing Phase 3 TRIUMPH-program records on ClinicalTrials.gov (see reference 6). https://www.accessdata.fda.gov/scripts/cder/daf/
- Effects of retatrutide on body composition in people with type 2 diabetes: a substudy of a phase 2, double-blind, parallel-group, placebo-controlled, randomised trial. The Lancet Diabetes & Endocrinology. 2025. https://www.thelancet.com/journals/landia/article/PIIS2213-8587(25)00092-0/abstract
- Efficacy and safety of retatrutide, a novel GLP-1, GIP, and glucagon receptor agonist for obesity treatment: a systematic review and meta-analysis of randomized controlled trials. PMC. 2025. https://pmc.ncbi.nlm.nih.gov/articles/PMC12026077/
- Katsi V, Koutsopoulos G, Fragoulis C, et al. Retatrutide — A Game Changer in Obesity Pharmacotherapy. Biomolecules. 2025;15(6):796. doi:10.3390/biom15060796. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12190491/
Educational and research-only disclaimer: This article is provided solely for scientific education and reference. It is not medical advice, not a recommendation, and not an endorsement of use. Retatrutide is an investigational compound that is not approved by the FDA or any major regulator; it is not a treatment for obesity, diabetes, liver disease, or any other condition, and no claim here should be read as stating that it treats, cures, or prevents disease. Any research-grade material is intended for authorized laboratory research use only and not for human consumption. Individuals with health concerns should consult a qualified, licensed healthcare professional and, if interested in retatrutide, should consider only participation in an authorized clinical trial.