The question in the title carries an assumption worth unpacking before we spend seven thousand words on the answer. The word “sustainable” can mean two very different things when applied to a weight-loss therapy. It can mean that the treatment produces durable, maintainable results for as long as a person keeps taking it — the way a blood-pressure medication sustainably controls hypertension. Or it can mean that the drug delivers a lasting change that persists after the person stops — a cure, a reset, a permanent recalibration of body weight. These two readings lead to opposite conclusions, and most confusion about semaglutide comes from sliding between them without noticing.
So this article treats the premise as a genuine research question rather than a rhetorical one. Semaglutide is not an investigational compound with a thin evidence base; it is one of the most rigorously studied weight-management agents ever developed, approved by the U.S. Food and Drug Administration as Wegovy for chronic weight management and as Ozempic and Rybelsus for type 2 diabetes.1 The pivotal trials are real, large, and largely positive. On the first reading of “sustainable” — durable results during continued treatment — the honest answer is a qualified yes, supported by two-year data.2 On the second reading — a lasting effect after discontinuation — the honest answer is a clear no, and the trial that establishes this is the STEP 1 extension, in which participants regained roughly two-thirds of their lost weight within a year of stopping.3
The rest of this piece is written for researchers, clinicians, and educated readers who want the actual data rather than either the breathless “miracle drug” framing or the reflexive backlash. We will cover what semaglutide is and where it came from, how it works at the molecular level, what the STEP clinical program actually showed, what happens when treatment stops, whether the effect holds over two years of continued use, the cardiovascular evidence, dosing and titration, the safety profile, how it compares with tirzepatide and other agents, the question of what kind of tissue is lost, and its regulatory status. Throughout, the guiding principle is precision: semaglutide is an approved and effective drug, but obesity behaves like the chronic relapsing condition it is, and no amount of enthusiasm changes the fact that the biology reasserts itself when the drug is withdrawn.
What Semaglutide Is and Where It Came From
Semaglutide is a synthetic analog of glucagon-like peptide-1 (GLP-1), an incretin hormone secreted by the enteroendocrine L-cells of the distal small intestine and colon in response to nutrient intake. Native GLP-1 is a remarkable signaling molecule — it augments glucose-dependent insulin secretion, suppresses glucagon, slows gastric emptying, and reduces appetite — but it is also almost useless as a drug in its natural form, because the enzyme dipeptidyl peptidase-4 (DPP-4) cleaves it within roughly one to two minutes of secretion.4 The entire history of GLP-1 pharmacology is, in a sense, a history of engineering around that catastrophically short half-life.
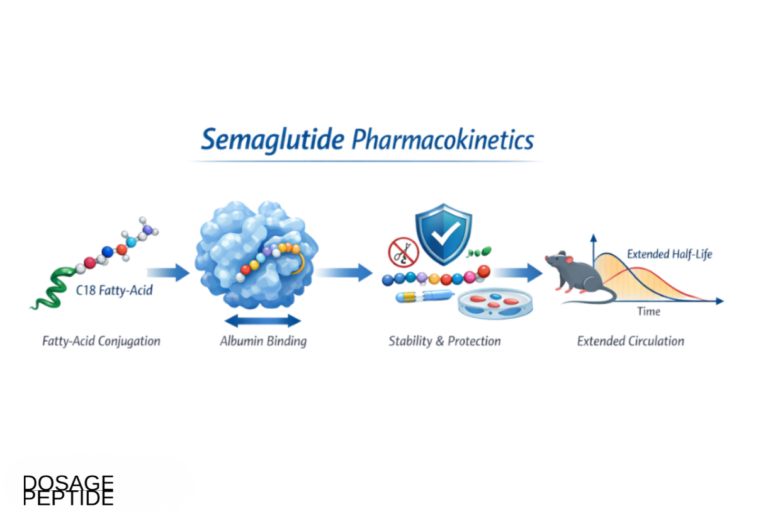
Semaglutide represents the current apex of that engineering effort. It shares about 94% sequence homology with human GLP-1, but carries three deliberate modifications that transform its pharmacokinetics.4 First, the amino acid at position 8 (alanine in native GLP-1) is substituted with alpha-aminoisobutyric acid, which sterically blocks DPP-4 cleavage. Second, lysine at position 34 is replaced with arginine. Third, and most importantly for its once-weekly dosing, a C-18 fatty diacid chain is attached via a hydrophilic glutamic-acid-and-spacer linker to a lysine at position 26. That fatty-acid tail binds reversibly and with high affinity to circulating albumin — more than 99% of the drug is albumin-bound at any moment.4 Albumin binding does two things at once: it shields the peptide from enzymatic degradation and renal clearance, and it creates a slow-release depot, because only the small unbound fraction is pharmacologically active and cleared at any time. The net result is a plasma half-life of roughly 165 to 184 hours — about a week — which is what makes a single weekly subcutaneous injection feasible.4
The developmental lineage matters. Semaglutide is the direct descendant of liraglutide, an earlier once-daily GLP-1 analog from the same manufacturer (marketed as Victoza for diabetes and Saxenda for weight).4 Liraglutide uses a shorter C-16 fatty-acid chain and binds albumin less avidly, hence its shorter half-life and daily dosing. Semaglutide was essentially liraglutide re-engineered for greater potency and duration, and the head-to-head STEP 8 trial later confirmed that the redesign produced meaningfully more weight loss.5
Semaglutide first reached the market for type 2 diabetes: subcutaneous Ozempic (up to 1.0 mg, later 2.0 mg weekly) was approved in 2017, and an oral formulation, Rybelsus, followed in 2019. The obesity indication came later. Investigators had long observed that GLP-1 agonists produced weight loss as a “side effect” in diabetes trials, and the manufacturer pursued a higher dose — 2.4 mg weekly — specifically for weight management. That dose, branded Wegovy, won FDA approval for chronic weight management in June 2021 in adults with obesity (BMI ≥30) or overweight (BMI ≥27) with at least one weight-related comorbidity, on the strength of the STEP program.1 It is worth holding onto the distinction between the molecule (semaglutide) and its branded doses and indications, because popular coverage constantly blurs “Ozempic” (a diabetes brand) with the weight-loss use, which is properly Wegovy.
For readers mapping the broader landscape of incretin-based therapeutics, semaglutide sits at one well-characterized end of a rapidly expanding family that now includes dual and triple receptor agonists; the site’s overviews of tirzepatide and retatrutide place it in that evolutionary context.
The Molecular Mechanism: How a GLP-1 Analog Curbs Appetite

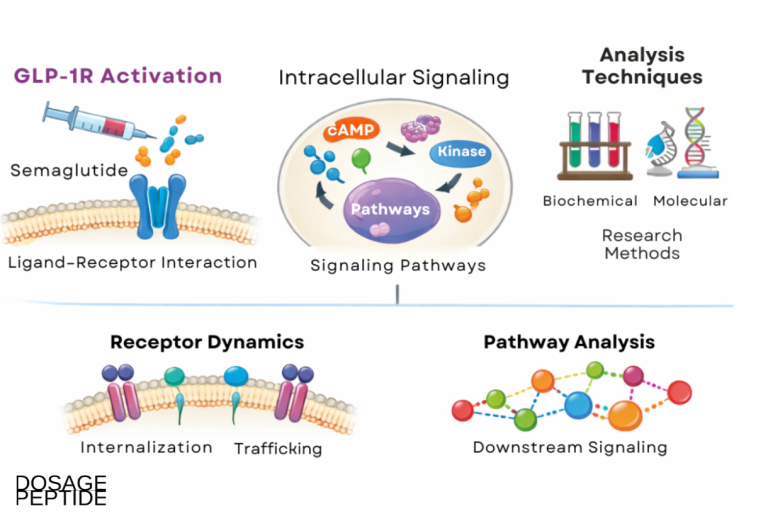
To judge whether semaglutide’s effect is sustainable, it helps to understand precisely what it does, because the mechanism itself predicts what happens when the drug is removed. Semaglutide is a selective agonist of the GLP-1 receptor (GLP-1R), a class B G-protein-coupled receptor. When it binds, it activates adenylate cyclase, raising intracellular cyclic AMP and triggering downstream signaling that varies by tissue.4 The therapeutic effects come from GLP-1 receptors distributed across several organ systems.
In the pancreatic beta cell, GLP-1R activation potentiates glucose-dependent insulin secretion — meaning it amplifies insulin release when blood glucose is elevated but tapers off as glucose normalizes, which is why GLP-1 agonists carry a low intrinsic hypoglycemia risk. It simultaneously suppresses glucagon from alpha cells. These islet effects drive the glycemic benefit in diabetes.4 But the weight-loss effect operates through different anatomy.
The dominant mechanism for weight reduction is central, in the brain. GLP-1 receptors are densely expressed in hypothalamic nuclei (notably the arcuate nucleus) and in the hindbrain (the area postrema and nucleus tractus solitarius), regions that integrate satiety and energy-balance signaling.4 By activating these circuits, semaglutide reduces hunger, increases satiety and fullness, lowers food-reward and cravings, and thereby cuts overall energy intake. In controlled feeding studies, participants on semaglutide simply eat substantially less, and self-reported control of eating improves.2 A secondary peripheral contributor is delayed gastric emptying, which prolongs the sensation of fullness after a meal and blunts post-prandial glucose excursions — though this effect appears to attenuate somewhat with continued dosing (tachyphylaxis), so it is probably not the main long-term driver of weight loss.
Here is the mechanistic key to the sustainability question. Semaglutide does not repair or reset the body’s underlying weight-regulation set point. It provides an ongoing pharmacological signal that biases the appetite system toward reduced intake. The body defends its adipose stores through a powerful homeostatic system — falling leptin, rising ghrelin, reduced energy expenditure — that responds to weight loss by increasing hunger and conserving energy. Semaglutide counteracts that defense while it is present. When the drug is withdrawn and its concentration decays over the following weeks, the counter-signal disappears, the biological drive to regain reasserts itself, and appetite returns. Nothing in the mechanism implies a durable post-treatment change, which is exactly why the discontinuation data look the way they do. This is not a failure of the drug; it is the predictable consequence of treating a chronic homeostatic condition with a reversible agonist.
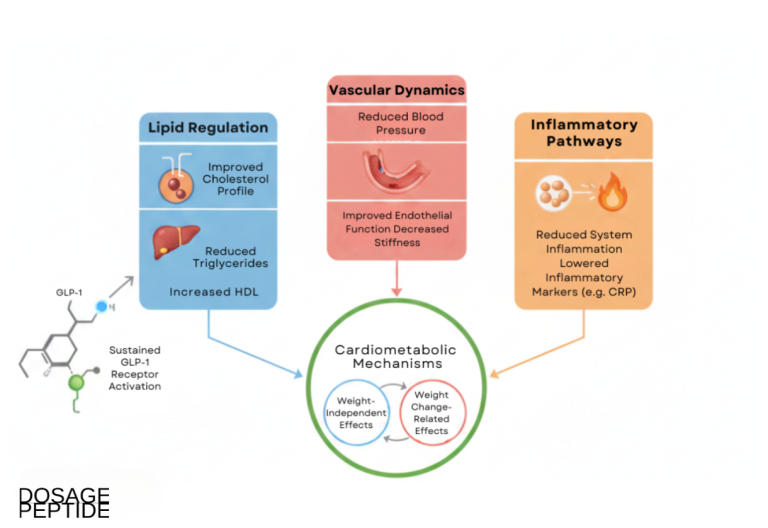
This mechanistic frame also clarifies why semaglutide’s benefits extend well beyond glucose and appetite. The same GLP-1 pathways influence vascular biology, inflammation, and lipid handling, which is why the compound has generated a distinct literature on GLP-1 signaling in lipid metabolism and arterial stiffness that we return to in the cardiovascular section.
The Pivotal Evidence: The STEP Program
The efficacy case for semaglutide in weight management rests on the STEP program (Semaglutide Treatment Effect in People with obesity), a coordinated series of phase 3 randomized controlled trials sponsored by the manufacturer. Because so much rides on these trials, it is worth being specific about what each one tested and found.
The anchor is STEP 1, published in the New England Journal of Medicine in 2021. It randomized 1,961 adults with obesity or overweight-with-comorbidity, without diabetes, to once-weekly subcutaneous semaglutide 2.4 mg or placebo, both with lifestyle counseling, for 68 weeks.2 The co-primary result was a mean body-weight change of −14.9% with semaglutide versus −2.4% with placebo — a placebo-subtracted difference of about 12.4 percentage points. Categorically, 86% of the semaglutide group lost at least 5% of body weight, roughly 69% lost at least 10%, and about 50% lost at least 15%, compared with far smaller fractions on placebo.2 A weight loss of nearly 15% from a drug had, before this, been essentially the exclusive province of bariatric surgery.
STEP 2 tested the same 2.4 mg dose in 1,210 adults who had type 2 diabetes — a population that characteristically loses less weight on any intervention. Mean weight loss was 9.6% with semaglutide 2.4 mg versus 3.4% with placebo, confirming efficacy but at a blunted magnitude in diabetes.6 STEP 3 added intensive behavioral therapy and showed roughly 16% loss, indicating that pairing the drug with structured lifestyle support squeezes out somewhat more benefit. The trials that speak most directly to sustainability — STEP 4, STEP 5, and the STEP 1 extension — get their own sections below, because they are the crux of this article.
It is also worth noting what the STEP program did not establish, because honest appraisal means marking the edges of the evidence. The trials were sponsor-designed and sponsor-funded, which is normal for pivotal drug development but warrants the usual caution about publication and interpretation incentives. The comparator was placebo plus lifestyle counseling, not an active alternative, so the trials answer “does the drug beat nothing” more cleanly than “how does it stack up against other strategies.” Follow-up in the core trials ran 68 to 104 weeks — long by weight-loss-trial standards, but short relative to a condition meant to be managed for decades. And trial populations, with their structured support and monitoring, tend to outperform real-world use, where adherence is lower and discontinuation common; large real-world cohorts have generally shown smaller average weight loss than the trials, chiefly because many people stop the drug or never reach the maintenance dose. None of this undercuts the core finding of large efficacy; it simply bounds it.
| Trial | Population | Duration | Mean weight change (sema 2.4 mg vs placebo) |
|---|---|---|---|
| STEP 1 | Obesity/overweight, no diabetes2 | 68 weeks | −14.9% vs −2.4% |
| STEP 2 | Type 2 diabetes6 | 68 weeks | −9.6% vs −3.4% |
| STEP 4 (maintenance) | Responders after 20-wk run-in7 | 68 weeks total | Continue: further −7.9%; switch to placebo: +6.9% regain |
| STEP 5 | Obesity/overweight, no diabetes8 | 104 weeks | −15.2% vs −2.6% |
| STEP 8 (vs liraglutide) | Obesity/overweight, no diabetes5 | 68 weeks | −15.8% (sema) vs −6.4% (liraglutide 3.0 mg) |
Two honest observations frame the whole program. First, the effect size is large and reproducible across trials, populations, and continents — this is not a marginal or contested finding. Second, and crucially, every one of these numbers describes weight loss during active treatment. The STEP program demonstrates conclusively that semaglutide causes substantial weight loss and maintains it as long as the drug is administered. What it does not, and cannot, show from the on-treatment numbers alone is whether that loss persists afterward. For that we have to look at what happened when the drug was taken away.
The Crux: What Happens After You Stop
If a single body of evidence should shape how anyone thinks about semaglutide and long-term weight loss, it is the discontinuation data. Two trials speak directly to it, and they point the same way.
The most decisive is the STEP 1 trial extension, published in Diabetes, Obesity and Metabolism in 2022. Researchers followed a representative subset of the original STEP 1 participants for a further year after all treatment — both semaglutide and the structured lifestyle intervention — was stopped at week 68.3 The result is the single most important sentence in this article: one year after withdrawal, participants had regained roughly two-thirds of the weight they had lost. In precise figures, the semaglutide group had lost a mean of 17.3% from baseline to week 68, then regained 11.6 percentage points over the following year, leaving a net loss of just 5.6% at week 120.3 Almost as telling, the cardiometabolic improvements achieved on treatment — better blood pressure, lipids, glycemia, and inflammatory markers — also drifted back toward baseline as the weight returned.3
The STEP 4 trial approaches the same question from the other direction, using a randomized-withdrawal design that is arguably even more rigorous. All 902 enrolled participants first took semaglutide for a 20-week open-label run-in, reaching the full 2.4 mg dose. The 803 who tolerated it were then re-randomized 2:1 either to continue semaglutide or to switch to placebo, for a further 48 weeks.7 The two groups diverged dramatically. Those who continued semaglutide lost an additional 7.9% of body weight over the maintenance phase (roughly 17.4% total across the trial). Those switched to placebo regained 6.9% over the same period.7 The only variable that differed between the groups was the presence or absence of the drug — both received identical lifestyle support — which isolates the drug as the cause of both the continued loss and, in the placebo arm, the regain.
| Scenario | Trial | Weight trajectory |
|---|---|---|
| Continue treatment past 68 wk | STEP 4 / STEP 578 | Loss maintained or deepened; plateau near 15–17% |
| Switch to placebo at wk 20 | STEP 47 | Gradual regain (+6.9% over 48 wk) |
| Full withdrawal at wk 68 | STEP 1 extension3 | ~2/3 of lost weight regained by 1 year; net ~5.6% |
The interpretation the trialists themselves reached is the honest one: these findings “confirm the chronicity of obesity and suggest ongoing treatment is required to maintain improvements in weight and health.”3 In other words, semaglutide is not a course of treatment with a finish line; it functions more like an antihypertensive or a statin, where the benefit persists only as long as the medication is taken. This is not a scandal or a failure. We do not expect blood pressure to stay low forever after a patient stops their blood-pressure pill, and it is not clear why weight should be different, given that the underlying homeostatic biology is intact. But it fundamentally reframes the marketing-friendly notion of a “solution.” Semaglutide is a management tool, not a cure, and any honest account of long-term weight loss has to center that distinction.
There is an important nuance worth adding for balance. The regain is real and substantial on average, but it is not universal or complete: at the population level participants retained a modest net loss (5.6%), and real-world cohorts show heterogeneity, with some individuals maintaining more of their loss than others through diet, activity, and behavioral change.3 The clinically meaningful takeaway is not “the drug is pointless” but “the drug’s benefits are contingent on continued exposure, and discontinuation should be understood as a return of the disease rather than a clean exit.”
Why does the biology push back so hard? The answer lies in the same homeostatic system the mechanism section described. When adipose stores shrink, leptin falls, which the hypothalamus reads as a starvation signal; the orexigenic hormone ghrelin rises; and adaptive thermogenesis lowers resting energy expenditure below what body size alone would predict. This coordinated defense — sometimes called metabolic adaptation — persists long after weight is lost and does not switch off simply because a person has reached a “healthier” weight. Semaglutide works by supplying a countervailing satiety signal strong enough to hold intake below that defended level. Withdraw the signal and the defense wins, which is precisely what the numbers show. Understood this way, weight regain after stopping is not a sign that the drug “didn’t work” or that the person lacked willpower; it is the expected physiological rebound of an intact regulatory system that was being pharmacologically overridden. This reframing matters because the moral language of failure so often attached to weight regain is both scientifically wrong and clinically counterproductive.
Two-Year Durability On Treatment: STEP 5 and the Chronic-Disease Framing
If discontinuation reverses the benefit, the natural follow-up question is whether the benefit at least holds up over longer periods of continued use, or whether the body eventually adapts and the weight creeps back even on the drug. This matters because many pharmacological weight-loss agents in history have shown exactly that pattern of escape. The relevant evidence is STEP 5, published in Nature Medicine in 2022, which extended treatment to 104 weeks — two full years.8
STEP 5 randomized 304 adults with obesity or overweight-with-comorbidity, without diabetes, to semaglutide 2.4 mg or placebo, both with lifestyle intervention, for 104 weeks. Mean weight change at two years was −15.2% with semaglutide versus −2.6% with placebo.8 The shape of the curve is as informative as the endpoint: weight loss accrued over roughly the first year and then reached a stable plateau that was maintained through the second year, rather than reversing. About two-thirds of the semaglutide group achieved at least 10% loss and roughly a third achieved at least 20% at two years.8 Improvements in cardiometabolic risk factors were likewise sustained across the two years.
Reading STEP 4, STEP 5, and the STEP 1 extension together produces a coherent and rather elegant picture. The trajectory of weight on semaglutide is: rapid loss over the first several months as the titration completes, a slowing and plateau by roughly week 60 to 68, and then stable maintenance for as long as treatment continues — demonstrated out to two years. Remove the drug at any point and weight climbs back toward baseline over the following months. This is precisely the behavior one would predict from the mechanism: a reversible appetite-suppressing signal that must be present to override the body’s defense of its fat stores. On the durability-during-treatment reading of “sustainable,” then, the answer is genuinely affirmative — the effect does not fade over two years of continued use.8 The catch, always, is the phrase “of continued use.”
This is why the professional consensus has shifted toward framing obesity explicitly as a chronic relapsing disease requiring long-term management, analogous to hypertension or type 2 diabetes, rather than a lifestyle failure to be fixed with a temporary intervention. Semaglutide fits that framing well: it is an effective long-term maintenance therapy for a chronic condition. It does not fit the older, more appealing framing of a short course that resets the body permanently, because no such therapy exists.
Beyond the Scale: Cardiovascular and Metabolic Outcomes
A weight-loss number is a surrogate; what ultimately matters to health is whether the intervention prevents the events that obesity and diabetes cause — heart attacks, strokes, and deaths. On this harder question, semaglutide has generated genuinely landmark evidence, and it is arguably more important than the weight numbers.
The pivotal trial is SELECT (Semaglutide Effects on Cardiovascular Outcomes in People with Overweight or Obesity), published in the New England Journal of Medicine in 2023. SELECT enrolled 17,604 adults aged 45 or older with a BMI of at least 27 and established cardiovascular disease but without diabetes, randomizing them to semaglutide 2.4 mg or placebo and following them for a mean of about 40 months.9 The primary composite endpoint — cardiovascular death, non-fatal myocardial infarction, or non-fatal stroke — occurred in 6.5% of the semaglutide group versus 8.0% of placebo, a 20% relative risk reduction (hazard ratio 0.80).9 This was the first demonstration that a weight-management drug reduces hard cardiovascular events in people with obesity but without diabetes, and it prompted an FDA label expansion in 2024 to include cardiovascular risk reduction. Notably, prespecified analyses suggested the cardiovascular benefit was only partly explained by weight loss itself, implying direct vascular, anti-inflammatory, or other effects of GLP-1 signaling beyond the pounds lost.9
In the diabetes population, the earlier SUSTAIN-6 trial (2016) had already shown that semaglutide (at the 0.5–1.0 mg diabetes doses) significantly reduced the composite of cardiovascular death, non-fatal MI, and non-fatal stroke versus placebo in high-risk patients with type 2 diabetes, driven substantially by a reduction in non-fatal stroke.10 Together, SUSTAIN-6 and SELECT establish cardiovascular benefit across both the diabetic and non-diabetic obese populations.
These outcomes are important for the sustainability discussion in a subtle way. Because the cardiometabolic gains largely track with the weight and with continued drug exposure — and, as the STEP 1 extension showed, revert when the drug is withdrawn3 — the cardiovascular case actually strengthens the argument for long-term rather than short-term treatment. The events prevented in SELECT accrued over years of continuous therapy. A patient who takes semaglutide for six months, loses weight, and stops would be unlikely to bank the multi-year cardiovascular protection SELECT documented. This aligns with the broader interest in how GLP-1 pathways modify vascular biology, a theme explored in the site’s discussion of GLP-1 signaling and arterial stiffness.
Dosing and Titration in the Clinical and Research Context
Semaglutide’s dosing schedule is not arbitrary; it is a direct response to the compound’s most common problem, gastrointestinal intolerance. Because GLP-1 receptor activation slows gastric emptying and stimulates nausea centers, starting at the therapeutic dose would leave most patients vomiting. The solution is a slow, stepwise escalation that lets the gut adapt.
For weight management (Wegovy), the standard subcutaneous titration begins at 0.25 mg once weekly for four weeks — a sub-therapeutic priming dose — then escalates roughly monthly through 0.5 mg, 1.0 mg, and 1.7 mg, reaching the 2.4 mg maintenance dose at around week 17.1 If a given step is poorly tolerated, the escalation is paused or stepped back down until symptoms settle. For type 2 diabetes (Ozempic), the maintenance doses are lower (0.5, 1.0, or 2.0 mg weekly), reflecting that glycemic control needs less than maximal appetite suppression. The oral formulation (Rybelsus) requires its own regimen taken on an empty stomach with minimal water, because oral bioavailability is very low and easily disrupted by food.
The table below summarizes the standard subcutaneous weight-management escalation. It is presented for educational and research context only; semaglutide is a prescription drug, and dosing decisions belong with a qualified clinician.
| Phase | Weekly dose | Typical duration | Purpose |
|---|---|---|---|
| Initiation | 0.25 mg | 4 weeks | GI priming; sub-therapeutic |
| Escalation 1 | 0.5 mg | 4 weeks | Build tolerance |
| Escalation 2 | 1.0 mg | 4 weeks | Build tolerance |
| Escalation 3 | 1.7 mg | 4 weeks | Approach target |
| Maintenance | 2.4 mg | Ongoing | Full therapeutic dose1 |
A note on the gray market is warranted for honesty. Semaglutide is widely sold outside regulated pharmacy channels as lyophilized “research” powder requiring reconstitution, often marketed to individuals seeking to avoid prescription costs. This introduces two distinct hazards beyond the pharmacology: uncertain purity, dose accuracy, and sterility of unregulated material, and the error-prone arithmetic of self-reconstitution and dosing, which has produced documented cases of accidental overdose. The technical principles of dissolving a lyophilized peptide are covered in the general peptide reconstitution guide and catalogued alongside related compounds in the dosage index, but none of that changes the core fact that the safest and best-evidenced route to semaglutide’s benefits is the regulated, titrated, clinically supervised one studied in the STEP trials.
Safety and Tolerability
Semaglutide’s safety profile is, on balance, favorable for a drug of its efficacy, but it is not benign, and honest framing requires naming both the common nuisances and the rarer serious risks.
The dominant issue is gastrointestinal. In the STEP program, GI adverse events occurred in roughly 74% of semaglutide recipients versus about 48% on placebo — nausea in around 44%, diarrhea in about 30%, vomiting in about 24%, and constipation commonly as well.11 The reassuring part is that these events were predominantly mild to moderate, transient, and concentrated during dose escalation, which is exactly why the slow titration exists. The less reassuring part is that GI intolerance nonetheless drove a meaningful minority off the drug: permanent discontinuation due to GI events occurred in about 4.3% of the semaglutide 2.4 mg group versus 0.7% on placebo in STEP 1.2
Beyond the everyday GI symptoms, several specific risks deserve mention:
- Gallbladder disease. Rapid weight loss of any kind predisposes to gallstones, and semaglutide is no exception. Cholelithiasis and cholecystitis were modestly more common on drug than placebo (gallstones roughly 2.3% vs 0.9% in some analyses).11
- Pancreatitis. Acute pancreatitis is a labeled concern for the GLP-1 class, but in pooled non-diabetes trials the observed rate was low and not clearly higher than placebo (about 0.2% vs 0.26%).11 It remains a reason to stop the drug if severe abdominal pain occurs.
- Thyroid C-cell tumors. Rodent studies showed dose-dependent medullary thyroid C-cell tumors, prompting a boxed warning; the relevance to humans is unproven, but semaglutide is contraindicated in people with a personal or family history of medullary thyroid carcinoma or MEN 2.1
- Gastroparesis and ileus. Because the drug slows gastric emptying, rare cases of severe delayed emptying and, post-marketing, ileus have been reported; this also raises aspiration considerations around anesthesia.
- Other. Increased heart rate, injection-site reactions, gallbladder-related pain, and hypoglycemia (chiefly when combined with insulin or sulfonylureas) round out the profile. Semaglutide is not recommended in pregnancy.1
One consequence that is easy to overlook and directly relevant to long-term outcomes is the composition of the weight lost, which we treat separately below. The overall reasonable reading is that semaglutide’s short- and medium-term safety is well characterized and acceptable for an approved therapy, that the GI effects are manageable with titration but non-trivial, and that because the drug is intended for indefinite use, its multi-year and truly long-term safety continues to be an active area of pharmacovigilance rather than a settled matter.
Body Composition and the Quality of Weight Lost
Not all weight loss is metabolically equal, and a candid appraisal of semaglutide has to address what kind of tissue disappears. Any substantial caloric deficit — from a GLP-1 drug, a diet, or surgery — causes loss of both fat mass and lean (predominantly skeletal-muscle) mass. The concern with the potent GLP-1 agonists is that the sheer magnitude of weight loss they produce may carry a correspondingly large absolute loss of lean tissue.
The body-composition data bear this out to a degree. In DXA substudies, a sizeable fraction of the total weight lost on semaglutide — on the order of 40% in some analyses — came from lean mass rather than fat.2 This figure is frequently cited with alarm, but it needs careful interpretation. A lean-mass fraction in that range is broadly typical of substantial weight loss by most methods, not unique to semaglutide; because heavier bodies carry more lean mass to support their fat mass, some lean loss with large weight loss is physiologically expected. Encouragingly, the proportion of lean mass relative to total body mass generally improved — that is, participants ended up leaner in composition, not just lighter.2
Nonetheless, the absolute loss of muscle is a legitimate long-term concern, particularly in older adults where sarcopenia threatens function, and it is one reason the field is actively pursuing combination approaches that pair GLP-1 agonism with muscle-preserving or complementary mechanisms. The practical mitigations are unglamorous but evidence-based: adequate dietary protein and progressive resistance exercise during weight loss substantially blunt lean-mass loss and should be considered integral to any serious weight-management program built around semaglutide, not optional add-ons. The drug reduces intake; it does not build or protect muscle, and assuming it does is a mistake.
How Semaglutide Compares
Semaglutide no longer stands alone, and understanding its place among newer agents sharpens the picture of what “sustainable” can realistically mean. The comparison also underscores that the discontinuation problem is a class property, not a semaglutide-specific flaw.
The most important comparator is tirzepatide, a dual agonist of both the GLP-1 and GIP (glucose-dependent insulinotropic polypeptide) receptors, marketed as Mounjaro and Zepbound. In its SURMOUNT program, tirzepatide produced even larger weight loss — up to roughly 20–22% at the highest dose over 72 weeks — exceeding semaglutide’s typical 15%, and an indirect and head-to-head comparison (SURMOUNT-5) favored tirzepatide on magnitude of loss.12 Critically for this article, tirzepatide shows the same weight-regain pattern on withdrawal: the SURMOUNT-4 trial found substantial regain after switching to placebo, exactly mirroring STEP 4. The site’s overview of how effective tirzepatide is in recent studies details that program.
Looking forward, retatrutide, a triple agonist adding glucagon-receptor activity, has produced even more dramatic phase 2 weight loss (approaching 24%), though it remains investigational and not FDA-approved. And cagrilintide, a long-acting amylin analog, is being combined with semaglutide (as CagriSema) to push efficacy higher while potentially improving the quality of weight lost; the site examines its metabolic profile in its coverage of whether cagrilintide can prevent diabetes in high-risk patients. Against the older liraglutide, semaglutide is simply superior: STEP 8 showed 15.8% versus 6.4% weight loss with weekly semaglutide versus daily liraglutide.5
| Agent | Mechanism | Approx. peak weight loss | Regain on stopping? |
|---|---|---|---|
| Liraglutide | GLP-1 agonist (daily) | ~6–8%5 | Yes |
| Semaglutide | GLP-1 agonist (weekly) | ~15%2 | Yes (~2/3 regained)3 |
| Tirzepatide | GLP-1 + GIP dual agonist | ~20–22%12 | Yes |
| Retatrutide (investigational) | GLP-1 + GIP + glucagon triple | ~24% (phase 2) | Not yet characterized long-term |
The pattern across the entire class is the same lesson STEP 4 taught: these are appetite-modulating maintenance therapies whose benefits are contingent on continued use. A more potent agonist produces a larger loss to maintain, but does not escape the biology of regain. Sustainability, in every case, means “durable while treated,” not “permanent after stopping.”
The comparison also reframes how “sustainable” should be judged going forward. If the goal is the largest possible loss during treatment, the dual and triple agonists are ascendant. But if the goal is a therapy someone can actually stay on for years — the true determinant of long-term outcomes given the regain data — then tolerability, cost, injection burden, and the quality of weight lost matter as much as peak efficacy. A drug that produces 22% loss but that a patient abandons after eight months due to nausea or expense may deliver worse long-term results than a better-tolerated agent producing 15% that they sustain for years. Semaglutide’s decade-plus track record in diabetes, its weekly dosing, its cardiovascular outcome data, and its comparatively mature safety profile are genuine advantages in that longer game, even as newer molecules win the headline weight-loss numbers. The right agent is the one an individual can adhere to and afford indefinitely, because indefinite is, biologically, what the treatment of obesity requires.
Regulatory Status
Semaglutide’s regulatory position is unusually clear, which is a welcome contrast to many compounds discussed in the peptide literature. It is a fully approved prescription drug, not an investigational or gray-market substance.
In the United States, the FDA has approved semaglutide under three brand names for distinct indications: Ozempic (subcutaneous, 2017) for glycemic control in type 2 diabetes and, later, cardiovascular risk reduction in diabetes; Rybelsus (oral, 2019) for type 2 diabetes; and Wegovy (subcutaneous 2.4 mg, 2021) for chronic weight management in adults with obesity or overweight-with-comorbidity, expanded in 2024 to include reduction of major adverse cardiovascular events in adults with established cardiovascular disease and obesity/overweight, and later extended to adolescents aged 12 and older.1 Comparable approvals exist through the European Medicines Agency and other major regulators. For the specific question of long-term weight management, then, semaglutide is not off-label or experimental — it is an approved, on-label therapy, and one of only a small number of drugs with that status.
Several regulatory realities nonetheless bear on how the drug is actually obtained and used. Intense demand created periodic shortages, which in the U.S. permitted pharmacy compounding of semaglutide during the official shortage period; as the shortage resolved, the FDA moved to restrict such compounding, and much of the unregulated “research-grade” and compounded material that proliferated exists in a legally and pharmaceutically precarious space. Compounded and gray-market products are not FDA-approved, may vary in purity and potency, and have been associated with dosing errors. Separately, like other GLP-1 agents, semaglutide is subject to scrutiny in competitive sport and should not be assumed permissible for tested athletes without checking current anti-doping status.
The regulatory synthesis is straightforward and, importantly, does not overstate anything: semaglutide is a genuinely approved, well-evidenced therapy for long-term weight management and diabetes, with documented cardiovascular benefit. That approval reflects demonstrated efficacy and acceptable safety during continued, supervised use. It does not, and cannot, imply that a finite course produces a permanent cure — the trials the approval rests on are the same trials that show regain on withdrawal.
Frequently Asked Questions
Does semaglutide provide permanent weight loss?
No. Semaglutide produces substantial weight loss — about 15% of body weight on average over roughly a year — and maintains it for as long as the drug is taken, demonstrated out to two years in STEP 5.8 But it is not a permanent cure. In the STEP 1 trial extension, participants regained roughly two-thirds of their lost weight within a year of stopping, ending with a net loss of only about 5.6%.3 The most accurate framing is that semaglutide is a long-term maintenance therapy for a chronic condition, like a blood-pressure or cholesterol medication, rather than a one-time fix.
How much weight do people lose on semaglutide?
In the pivotal STEP 1 trial of adults with obesity but without diabetes, mean weight loss was 14.9% with semaglutide 2.4 mg versus 2.4% with placebo over 68 weeks, and 86% of the semaglutide group lost at least 5% of body weight.2 People with type 2 diabetes tend to lose somewhat less (about 9.6% in STEP 2).6 Individual results vary widely, and behavioral factors, diet, and physical activity meaningfully influence the outcome.
What happens if I stop taking semaglutide?
Weight tends to return. Both the STEP 1 extension (full withdrawal) and the STEP 4 randomized-withdrawal trial show that discontinuing semaglutide leads to gradual weight regain over the following months, along with a reversal of the improvements in blood pressure, lipids, and blood sugar.37 This is because the drug counteracts the body’s biological drive to defend its fat stores only while it is present; removing it removes the counter-signal. The regain is on average about two-thirds of the loss, though it varies between individuals.
Is the weight-loss effect sustained if I keep taking it?
Yes, within the studied timeframe. STEP 4 showed that continuing semaglutide beyond the initial phase maintained and even deepened weight loss, while switching to placebo caused regain.7 STEP 5 extended this to 104 weeks and found the roughly 15% loss reached a stable plateau and was maintained through two years without escape.8 Truly long-term (multi-year, decade-scale) durability and safety are still being characterized through ongoing use and pharmacovigilance.
Does semaglutide reduce heart attacks and strokes?
Yes, in the studied populations. The SELECT trial in over 17,000 people with obesity and established cardiovascular disease but without diabetes found a 20% reduction in major adverse cardiovascular events (cardiovascular death, non-fatal heart attack, or non-fatal stroke) versus placebo.9 The earlier SUSTAIN-6 trial showed cardiovascular benefit in high-risk patients with type 2 diabetes.10 These benefits accrued over years of continuous treatment.
What are the most common side effects?
Gastrointestinal symptoms dominate: nausea, diarrhea, vomiting, and constipation affect a large majority of users, though they are usually mild to moderate, transient, and concentrated during dose escalation.11 More serious but less common concerns include gallbladder disease, a boxed warning for thyroid C-cell tumors (based on rodent data), rare pancreatitis and severe delayed gastric emptying, and increased heart rate. The slow, stepwise titration exists specifically to reduce GI intolerance.1
Does semaglutide cause muscle loss?
Some of the weight lost is lean tissue, as with any large weight loss. DXA substudies suggest roughly 40% of the loss can come from lean mass, although overall body composition (the proportion of lean to total mass) generally improves.2 Adequate dietary protein and resistance exercise substantially reduce muscle loss and should be treated as essential components of a semaglutide-based program, especially in older adults.
How does semaglutide compare with tirzepatide?
Tirzepatide, a dual GLP-1/GIP agonist, generally produces greater weight loss (around 20–22% versus semaglutide’s ~15%) and outperformed semaglutide in a head-to-head trial.12 However, tirzepatide shows the same weight-regain pattern after discontinuation, so it is more potent but not more “curative.” Choice between them depends on efficacy needs, tolerability, cost, availability, and individual response.
Is semaglutide FDA-approved?
Yes. Semaglutide is approved as Wegovy for chronic weight management (and cardiovascular risk reduction in obesity with established heart disease), and as Ozempic and Rybelsus for type 2 diabetes.1 Note that unregulated “research-grade” or compounded semaglutide sold outside pharmacy channels is not FDA-approved and carries risks of variable purity and dosing errors; the safest route to the benefits documented in the trials is supervised, prescribed use.
References
- U.S. Food and Drug Administration. Wegovy (semaglutide) injection: Highlights of Prescribing Information. Silver Spring, MD: FDA; 2025. https://www.accessdata.fda.gov/drugsatfda_docs/label/2025/209637s025lbl.pdf
- Wilding JPH, Batterham RL, Calanna S, et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity. N Engl J Med. 2021;384(11):989-1002. PMID: 33567185. https://www.nejm.org/doi/full/10.1056/NEJMoa2032183
- Wilding JPH, Batterham RL, Davies M, et al. Weight regain and cardiometabolic effects after withdrawal of semaglutide: The STEP 1 trial extension. Diabetes Obes Metab. 2022;24(8):1553-1564. PMCID: PMC9542252. https://pmc.ncbi.nlm.nih.gov/articles/PMC9542252/
- Knudsen LB, Lau J. The Discovery and Development of Liraglutide and Semaglutide. Front Endocrinol (Lausanne). 2019;10:155. PMCID: PMC6474072. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6474072/
- Rubino DM, Greenway FL, Khalid U, et al. Effect of Weekly Subcutaneous Semaglutide vs Daily Liraglutide on Body Weight in Adults With Overweight or Obesity Without Diabetes: The STEP 8 Randomized Clinical Trial. JAMA. 2022;327(2):138-150. PMID: 35015037. https://pmc.ncbi.nlm.nih.gov/articles/PMC8753508/
- Davies M, Fábregas BC, Buse JB, et al. Semaglutide 2.4 mg once a week in adults with overweight or obesity, and type 2 diabetes (STEP 2): a randomised, double-blind, double-dummy, placebo-controlled, phase 3 trial. Lancet. 2021;397(10278):971-984. PMID: 33667417. https://pubmed.ncbi.nlm.nih.gov/33667417/
- Rubino D, Abrahamsson N, Davies M, et al. Effect of Continued Weekly Subcutaneous Semaglutide vs Placebo on Weight Loss Maintenance in Adults With Overweight or Obesity: The STEP 4 Randomized Clinical Trial. JAMA. 2021;325(14):1414-1425. PMID: 33755728. https://pmc.ncbi.nlm.nih.gov/articles/PMC7988425/
- Garvey WT, Batterham RL, Bhatta M, et al. Two-year effects of semaglutide in adults with overweight or obesity: the STEP 5 trial. Nat Med. 2022;28(10):2083-2091. PMCID: PMC9556320. https://pmc.ncbi.nlm.nih.gov/articles/PMC9556320/
- Lincoff AM, Brown-Frandsen K, Colhoun HM, et al. Semaglutide and Cardiovascular Outcomes in Obesity without Diabetes (SELECT). N Engl J Med. 2023;389(24):2221-2232. PMID: 37952131. https://www.nejm.org/doi/full/10.1056/NEJMoa2307563
- Marso SP, Bain SC, Consoli A, et al. Semaglutide and Cardiovascular Outcomes in Patients with Type 2 Diabetes (SUSTAIN-6). N Engl J Med. 2016;375(19):1834-1844. PMID: 27633186. https://www.nejm.org/doi/full/10.1056/NEJMoa1607141
- Wharton S, Calanna S, Davies M, et al. Gastrointestinal tolerability of once-weekly semaglutide 2.4 mg in adults with overweight or obesity, and the relationship between gastrointestinal adverse events and weight loss. Diabetes Obes Metab. 2022;24(1):94-105. PMCID: PMC9293236. https://pmc.ncbi.nlm.nih.gov/articles/PMC9293236/
- Jastreboff AM, Aronne LJ, Ahmad NN, et al. Tirzepatide Once Weekly for the Treatment of Obesity (SURMOUNT-1). N Engl J Med. 2022;387(3):205-216. PMID: 35658024. https://www.nejm.org/doi/full/10.1056/NEJMoa2206038
Educational and research-use disclaimer: This article is provided solely for scientific and educational purposes and is not medical advice. Semaglutide is a prescription medication approved by the FDA (as Wegovy for chronic weight management and Ozempic/Rybelsus for type 2 diabetes); it is effective for weight loss during continued, supervised use, but the evidence shows substantial weight regain after discontinuation, and it is not a permanent cure for obesity. Nothing here is a recommendation to obtain, self-administer, or reconstitute semaglutide outside a regulated clinical setting; unapproved “research-grade” or compounded material carries risks of variable purity and dosing errors. Individuals considering semaglutide should consult a qualified healthcare professional, and any research use should occur under appropriate oversight and in compliance with applicable regulations.