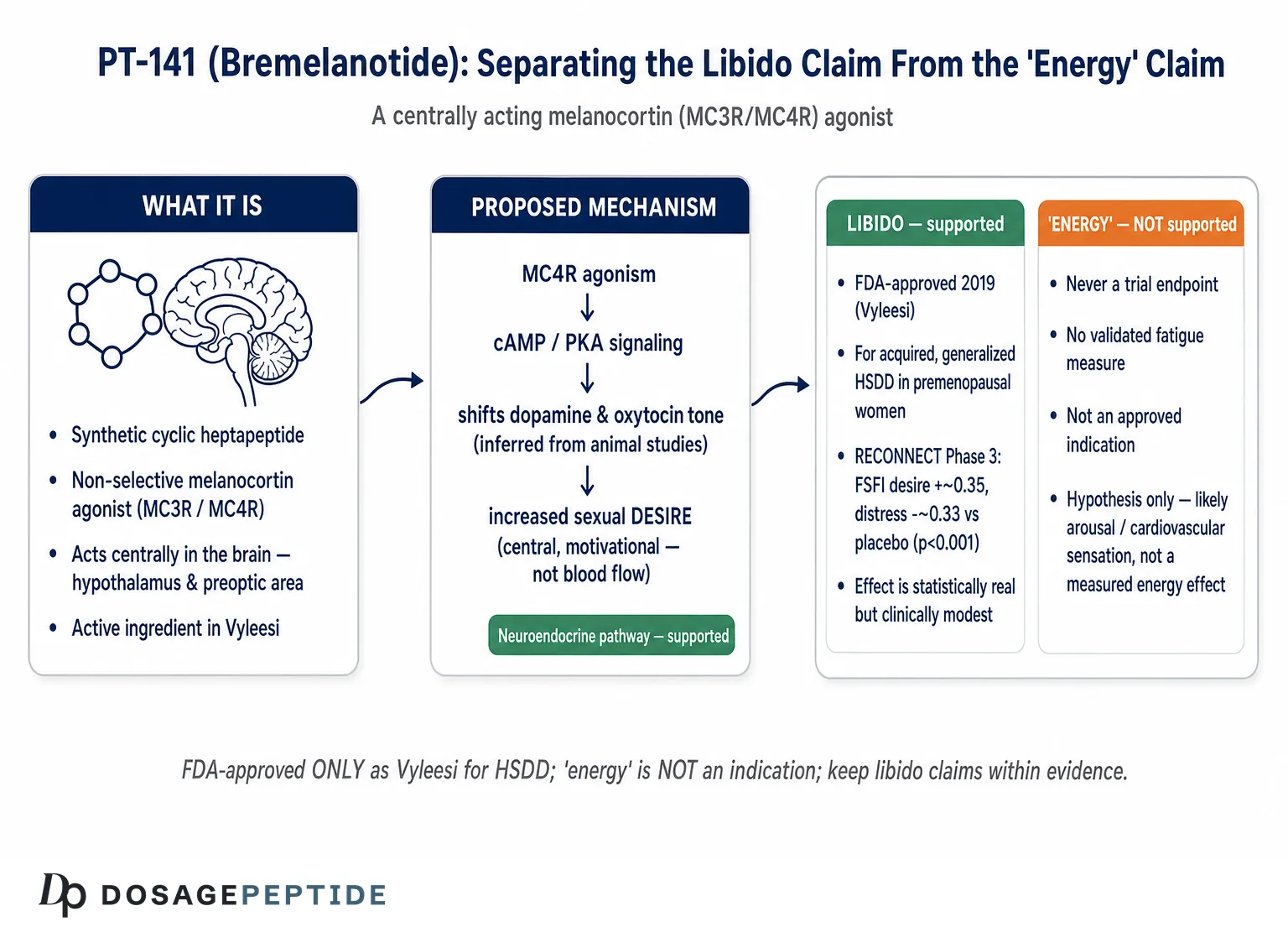
The title of this article bundles two claims together that deserve to be pulled apart before anything else is said. The first — that PT-141 (bremelanotide) acts through neuroendocrine pathways to influence libido — is on solid ground. Bremelanotide is a melanocortin-receptor agonist that works inside the brain, and it is the active ingredient in Vyleesi, a medication the U.S. Food and Drug Administration approved in 2019 for one narrowly defined condition: acquired, generalized hypoactive sexual desire disorder (HSDD) in premenopausal women.1 In the pivotal trials, it produced statistically significant improvements in sexual desire and reductions in the distress that accompanies low desire.2 So the “neuroendocrine pathways” and “libido” halves of the question map onto a real, approved, evidence-backed mechanism.
The second claim — that the same peptide enhances “energy” — is a different animal entirely. Energy is not an approved indication for bremelanotide. It was never a primary or secondary endpoint in the registration program. There is no randomized trial showing that bremelanotide raises energy levels, reduces fatigue, or improves vitality as a stand-alone outcome. The word “energy” has migrated into the compound’s popular reputation largely by association — because sexual arousal feels energizing, because the melanocortin system also touches metabolism and appetite, and because wellness marketing tends to blur “feels invigorating” into “boosts energy.” This article treats the energy premise as an open, and largely unstudied, research question rather than an established effect, and it will say so plainly wherever the evidence runs out.
What follows is an honest map for researchers and scientifically literate readers: where bremelanotide came from, what the central melanocortin system actually is, how the peptide engages it, what the human trials genuinely demonstrated for desire, why the “energy” framing outruns the data, how the compound compares with other agents, what its safety profile looks like, and where it sits with regulators. Throughout, the guiding rule is proportion: state the approved, well-supported libido effect at full strength, and refuse to inflate the unproven energy claim beyond what any study can bear.
What PT-141 (Bremelanotide) Is and Where It Came From
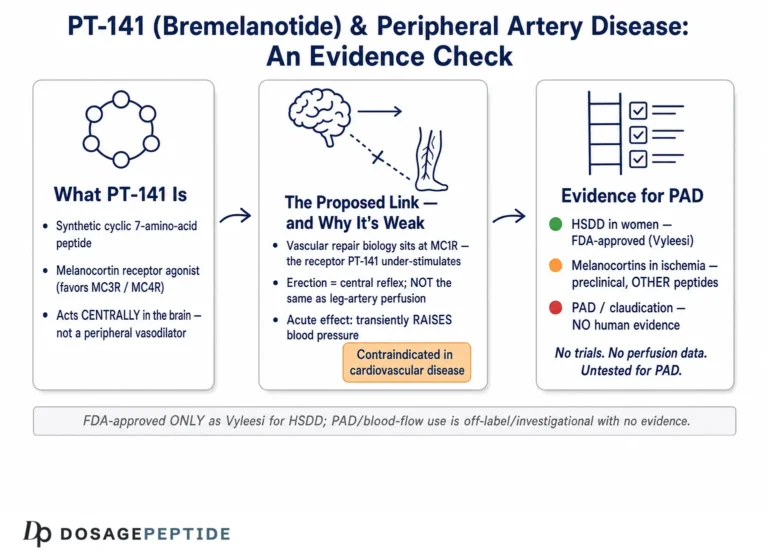
Bremelanotide is a synthetic cyclic heptapeptide — a seven-amino-acid ring — that behaves as a non-selective agonist at melanocortin receptors, with its clinically relevant activity concentrated at the melanocortin-3 and melanocortin-4 receptor subtypes (MC3R and MC4R). Its lineage is unusual and worth telling accurately, because the history explains both the mechanism and several of the safety caveats that follow.
The story begins with Melanotan II, an α-melanocyte-stimulating hormone (α-MSH) analog originally synthesized at the University of Arizona and studied as a potential sunless-tanning agent, since melanocortin signaling drives melanin production in the skin. During early human testing, an unexpected side effect appeared: male volunteers reported spontaneous erections. That serendipitous observation redirected an entire research program away from pigmentation and toward sexual function.3 Palatin Technologies licensed the melanocortin chemistry and developed bremelanotide as a metabolite-derived, ring-modified successor to Melanotan II, optimized as a drug candidate for sexual dysfunction rather than tanning. Readers interested in the parent molecule can compare the mechanistic accounts of how Melanotan II influences erectile performance and its debated role in hypoactive sexual desire disorder, which share the same melanocortin backbone as bremelanotide.
The early clinical development of bremelanotide targeted erectile dysfunction in men and used an intranasal spray formulation. Double-blind, placebo-controlled work in healthy males and in men with mild-to-moderate erectile dysfunction did show pharmacodynamic effects consistent with central pro-erectile activity.4 But the intranasal program ran into a wall that has shadowed the compound ever since: transient increases in blood pressure. The nasal route produced rapid absorption and blood-pressure spikes that were judged unacceptable for a lifestyle indication, and that development track was halted. The program was later reconstituted around a subcutaneous, on-demand formulation and re-aimed at female HSDD, where the pivotal trials eventually succeeded and led to the 2019 approval.1
Three points from this history bear directly on how to read the compound today. First, bremelanotide is, at its core, a central nervous system agent: its sexual effects were discovered as brain-mediated phenomena, not as peripheral vascular ones, and that distinction runs through the entire mechanistic story below. Second, the blood-pressure signal is intrinsic to melanocortin agonism, not an artifact of one formulation — it reappears, in milder form, with the approved subcutaneous product. Third, the compound’s identity has always been sexual function; “energy” was never the target of any development program, which is one reason the energy literature is essentially empty.
A useful habit when reasoning about bremelanotide is to keep three layers distinct: the endogenous ligand (α-MSH and related melanocortins, which the body makes), the receptor family (five melanocortin receptors, MC1R through MC5R, each with different tissue distributions and jobs), and the drug (bremelanotide, a synthetic agonist that hits several of those receptors at once). Much of the confusion in popular writing comes from collapsing these layers — attributing to the drug every effect associated with any melanocortin receptor anywhere in the body. Keeping them separate is the single most useful discipline for thinking clearly about what this peptide can and cannot do.
The Central Melanocortin System: The Neuroendocrine Substrate
To evaluate the “neuroendocrine pathways” claim in the title, you have to understand what the central melanocortin system actually is, because it is one of the better-characterized neuroendocrine circuits in the mammalian brain. It is not a single receptor or a single behavior; it is an integrative hub that helps the brain translate signals about the body’s internal state into coordinated outputs.6
At its center are two populations of neurons in the arcuate nucleus of the hypothalamus. One set makes pro-opiomelanocortin (POMC), a precursor protein that is cleaved into α-MSH and other melanocortins; these neurons are, broadly, catabolic and satiety-promoting. The opposing set makes agouti-related peptide (AgRP), an endogenous antagonist/inverse agonist at MC4R; these neurons are orexigenic, driving food intake. Downstream, MC4R is expressed in the paraventricular nucleus of the hypothalamus, the medial preoptic area, and other limbic and brainstem sites. Through this architecture the melanocortin system regulates energy homeostasis, appetite, and body weight, and it also participates in autonomic control, including sympathetic outflow to the cardiovascular system.6 That last function is the anatomical reason a central melanocortin agonist raises blood pressure — the pathway is wired into sympathetic tone, not just sexual circuitry.
The system’s role in sexual behavior sits alongside its metabolic role, mediated largely by MC4R (with a contribution from MC3R) in hypothalamic and preoptic nodes. Decades of preclinical work established that melanocortin agonists acting centrally can facilitate sexual motivation and erectile responses in rodent models, and that these effects are dissociable from direct peripheral vasodilation — they involve the brain’s motivational and autonomic circuitry rather than smooth-muscle relaxation in genital tissue.5 This is the crucial mechanistic pivot that separates a melanocortin agonist from a PDE5 inhibitor such as sildenafil: one works top-down on desire and central arousal, the other works bottom-up on penile blood flow.
The division of labor between the two relevant receptor subtypes is worth spelling out, because popular accounts tend to treat “MC3R/MC4R” as an undifferentiated pair. MC4R is the dominant player: it is densely expressed in the paraventricular nucleus and preoptic area, it is the receptor whose loss-of-function mutations are the most common monogenic cause of human obesity, and it is the subtype most directly implicated in the sexual and autonomic effects that matter here.6 MC3R is more restricted in distribution and appears to play a modulatory, presynaptic role in energy balance and in the timing of feeding rather than a primary role in sexual motivation. Bremelanotide hits both, but the therapeutically relevant — and the most heavily studied — target is MC4R, which is why the imaging and mechanistic literature increasingly describes the drug as an “MC4R agonist” even though its pharmacology is broader. That broader pharmacology, extending to MC1R in the skin, is what accounts for the pigmentation side effects discussed later; the receptor that produces the wanted effect and the receptor that produces the unwanted one belong to the same family the drug engages indiscriminately.
The phrase “neuroendocrine” is accurate for this system in the strict sense — it is a neural circuit that both responds to hormonal signals (leptin, insulin, and other peripheral cues converge on POMC/AgRP neurons) and shapes endocrine and autonomic output. But it is worth being precise about what “neuroendocrine” does not mean here. Bremelanotide is not a sex hormone, does not act on the testosterone or estrogen axes directly, and does not work by raising circulating gonadal hormones. Its neuroendocrine action is upstream and central: it nudges a hypothalamic motivational circuit, and any downstream hormonal or autonomic consequences follow from that central nudge. Conflating “neuroendocrine peptide” with “hormone replacement” is a common error, and it matters for both mechanism and safety.
How Bremelanotide Engages the Pathway
At the molecular level, bremelanotide binds melanocortin receptors that are G-protein-coupled and signal predominantly through the stimulatory G-protein Gs. Receptor activation raises intracellular cyclic adenosine monophosphate (cAMP), which activates protein kinase A (PKA) and, through downstream phosphorylation cascades, changes the excitability and firing of the neurons that express the receptor.5 In the hypothalamic and preoptic circuits relevant to sexual behavior, this increased melanocortin tone is thought to shift the balance of downstream neurotransmission — notably engaging dopaminergic signaling associated with reward and motivation and oxytocinergic signaling associated with arousal and social/sexual bonding. The net physiological read-out in the well-studied rodent models is increased pro-sexual behavior and central arousal.35
Two features of this mechanism deserve emphasis because they are frequently misrepresented. First, the effect is motivational and central, not primarily hemodynamic. Bremelanotide is best understood as acting on the “desire” side of the sexual-response system — the appetitive, wanting phase — rather than as a vasodilator that mechanically produces an erection or engorgement. This is precisely why it was pursued for a desire disorder (HSDD) rather than positioned as a direct competitor to erectile-blood-flow drugs. For readers exploring the blood-flow question specifically, the separate discussion of whether PT-141 can enhance blood flow in peripheral artery disease is a useful counterpoint: it illustrates how thin the direct-vascular evidence is compared with the central-desire evidence, and why the two should not be conflated.
Second, the receptor promiscuity of the drug cuts both ways. Because bremelanotide is a non-selective agonist, it activates MC1R (pigmentation) and contributes to autonomic effects through central MC4R in addition to producing the intended sexual-motivation effect. The same pharmacology that drives desire therefore also drives the characteristic side effects — skin hyperpigmentation via MC1R, nausea and flushing, and the transient blood-pressure rise via central sympathetic engagement. Mechanistically, these are not unrelated nuisances; they are the fingerprints of the very melanocortin agonism that produces the wanted effect. A cleaner, MC4R-selective molecule is a long-standing goal precisely because it might separate the desire effect from the pigmentary and cardiovascular ones.
It is also worth being candid about how much of the fine-grained mechanism is extrapolated from animal work rather than measured in humans. The dopaminergic and oxytocinergic downstream steps — the idea that melanocortin tone in the preoptic area recruits reward-associated dopamine and arousal-associated oxytocin — rest heavily on rodent neurochemistry and lesion studies, not on direct human neurotransmitter measurement.5 The human evidence establishes that the drug engages central sexual-processing circuits and improves reported desire; the precise neurochemical choreography that connects receptor binding to that outcome is inferred from a well-developed but species-limited preclinical literature. This is an honest boundary that should temper confident mechanistic storytelling: the direction of the effect is well supported, but the step-by-step causal chain in the human brain is a reasonable model rather than a fully mapped fact.
It is also worth stating what the mechanism does not obviously predict: a robust, stand-alone boost in physical energy or wakefulness. The melanocortin system’s metabolic arm regulates appetite and energy homeostasis — the balancing of intake and expenditure — which is a very different thing from acutely making a person feel more energetic. Nothing in the cAMP/PKA-to-motivation cascade described above translates cleanly into “more energy” as most people use the phrase. Any energizing sensation reported after dosing is at least as plausibly a downstream feature of heightened arousal, dopaminergic tone, or the cardiovascular response as it is a genuine, measurable increase in usable energy. That gap between mechanism and marketing is the theme of a later section.
Defining the Condition: What HSDD Actually Is
Because bremelanotide’s only approved use is HSDD, and because the “libido” claim stands or falls on that indication, it helps to be precise about the diagnosis. HSDD is not simply “low sex drive” in the colloquial sense. In the framework used by sexual-medicine specialists, it is characterized by a persistent or recurrent deficiency of sexual/erotic thoughts, fantasies, and desire for sexual activity, which causes clinically significant personal distress and is not better explained by another disorder, a medication, a relationship problem, or a substance.11 The distress criterion is essential: low desire that does not bother the person is not a disorder.
The approved indication is narrower still. Vyleesi is indicated specifically for acquired, generalized HSDD in premenopausal women — acquired meaning the person previously had normal desire and later lost it, and generalized meaning it is not limited to a specific partner or situation.1 It is explicitly not indicated to enhance sexual performance, not indicated in postmenopausal women, and not indicated in men. The professional process-of-care guidance emphasizes a biopsychosocial assessment first — screening for relationship factors, mood disorders, medication effects (antidepressants are a common culprit), and medical contributors — before any pharmacologic option is considered.11 This matters for honest interpretation: bremelanotide is one narrowly positioned tool within a much larger diagnostic and management framework, not a general-purpose libido or vitality enhancer.
Keeping the diagnosis in view also guards against a subtle overreach. Demonstrating that a drug helps a distressing, diagnosed desire disorder in a specific population is not the same as demonstrating that it “boosts libido” in people without the disorder. The trials enrolled women who met strict HSDD criteria; they say little about what the compound does in someone with normal baseline desire, and nothing at all about “energy” in any population.
The Libido Evidence: What the Human Trials Actually Showed
The libido case for bremelanotide is genuinely strong by the standards of sexual-medicine pharmacology, and it is worth laying out in the order the evidence accumulated.
The earliest signal in women came from a proof-of-concept study using an intranasal dose in premenopausal women with sexual arousal disorder. More women reported moderate-to-high sexual desire after bremelanotide than after placebo, and among those who attempted intercourse within 24 hours, more were satisfied with their arousal.7 This was a small, early study with an intranasal formulation that was later abandoned, but it established the central hypothesis: a melanocortin agonist could move subjective desire in women.
The definitive evidence is the RECONNECT program: two identically designed, randomized, double-blind, placebo-controlled, multicenter Phase 3 trials that together enrolled roughly 1,250 premenopausal women with acquired, generalized HSDD, who self-administered 1.75 mg of subcutaneous bremelanotide on demand over a 24-week core phase.2 The trials met both co-primary endpoints. On the Female Sexual Function Index (FSFI) desire domain, bremelanotide improved scores by approximately 0.35 points more than placebo, and on the relevant item of the Female Sexual Distress Scale (FSDS-DAO item 13, measuring bother from low desire), it reduced distress by about 0.33 points more than placebo — both statistically significant (P < 0.001 in the integrated analysis).2 A 52-week open-label extension in 684 participants found that improvements were sustained over a year of as-needed use, with no new safety signals emerging over the longer horizon.9 Prespecified and integrated subgroup analyses subsequently reported that the desire and distress benefits were broadly consistent across age groups, baseline severity, and other subpopulations within the enrolled cohort.10
Two honest qualifications belong right next to those results. First, the effect sizes are statistically robust but clinically modest. A 0.35-point shift on the FSFI desire domain is a real, reproducible signal, not a dramatic transformation; many treated women did not reach a responder threshold, and placebo responses in HSDD trials are notably large. Second, the co-primary endpoints measured desire and distress — not the number of satisfying sexual events, which did not separate as convincingly from placebo. The fair summary is that bremelanotide reliably and safely produces a modest improvement in desire and its associated distress in the studied population, which is exactly the claim the FDA approval supports — no more, no less.
The large placebo response in HSDD trials deserves its own sentence, because it is central to interpreting the numbers honestly. Sexual desire is a subjective, context-sensitive outcome that improves substantially with attention, expectation, and study participation alone; placebo groups in these trials routinely report meaningful gains. That is precisely why the between-group difference — the increment attributable to the drug over and above placebo — is the figure that matters, and why a statistically significant but modest 0.35-point desire advantage is the appropriate summary rather than the larger raw improvement seen within the treated arm.2 Any account that quotes the total change in bremelanotide-treated women without subtracting the placebo response overstates the drug’s specific contribution, and the same discipline should be applied — even more strictly — to any anecdotal “energy” report, where no placebo control exists at all.
| Study / dataset | Design | Key libido finding |
|---|---|---|
| Diamond et al. 2006 (women) | Early proof-of-concept, intranasal, premenopausal women with arousal disorder | More women reported moderate/high desire vs placebo; greater arousal satisfaction7 |
| RECONNECT (two Phase 3 RCTs) | Randomized, double-blind, placebo-controlled; 1.75 mg SC on demand; ~1,250 women; 24 weeks | FSFI desire +~0.35 and FSDS-DAO distress −~0.33 vs placebo (P < 0.001)2 |
| Open-label extension | 52 weeks, 684 participants, no placebo arm | Sustained desire/distress improvement; no new safety signals9 |
| Integrated subgroup analyses | Prespecified pooling of RECONNECT data | Benefit broadly consistent across subgroups10 |
| Energy / vitality | — | No trial; not an endpoint; no data |
The Brain-Imaging Evidence: Watching the Neuroendocrine Effect
If the RECONNECT trials showed that bremelanotide improves self-reported desire, a later functional-MRI study offered a mechanistic look at how — and it is the most direct human evidence that the effect is genuinely central and neuroendocrine rather than peripheral or purely subjective.
In a randomized, double-blind, placebo-controlled crossover study, 31 premenopausal women with HSDD underwent functional MRI while viewing erotic visual stimuli, on separate occasions after receiving 1.75 mg subcutaneous bremelanotide or placebo.8 MC4R agonism significantly increased participant-reported sexual desire compared with placebo for up to 24 hours, and, critically, it altered brain activation in regions involved in sexual processing — providing objective neural correlates for the subjective effect. This was the first trial to image the effect of MC4R agonism on sexual brain processing in women with HSDD.8
The imaging study matters for the title’s framing in two ways. It substantiates the “neuroendocrine pathways” claim with direct evidence that the drug changes activity in central sexual-processing circuits, not merely in the periphery. And it reinforces the boundary of what has been demonstrated: the measured outcome was sexual brain processing and desire, imaged under erotic stimuli. The study offers no read-out on generalized energy, alertness, or fatigue, and it should not be cited — as it sometimes is — as evidence that the drug “activates the brain” in some diffuse, energizing way. It activated sexual-processing circuitry in a desire-disorder population, which is a specific and appropriately narrow finding.
The “Energy” Question: Examining a Premise the Evidence Does Not Support
Now to the harder half of the title. Does bremelanotide enhance energy? The scientifically honest answer is that there is no direct evidence it does, and the framing conflates several distinct phenomena that ought to be kept apart.
Start with what is absent. Across the registration program — the Phase 3 RECONNECT trials, the long-term extension, and the subgroup analyses — energy, vitality, fatigue, and vigor were not co-primary or key secondary endpoints, and no validated fatigue instrument was the basis of any efficacy claim.29 The FDA-approved labeling for Vyleesi describes an indication for HSDD and says nothing about energy enhancement.1 There is, in short, no pivotal-trial evidence that bremelanotide raises energy as an outcome in its own right. It is worth adding the converse observation, too: fatigue, asthenia, and somnolence did not emerge as prominent treatment-emergent adverse events in the RECONNECT dataset, where the common reactions were instead nausea, flushing, injection-site reactions, and headache.19 A compound with a genuine, robust stimulant-like action on wakefulness would be expected to leave some fingerprint on either the efficacy or the tolerability record; bremelanotide leaves neither, which is itself weak evidence against a meaningful stand-alone energy effect rather than evidence for one.
Why, then, does the energy claim circulate so persistently? Several plausible, non-exclusive explanations, none of which amount to demonstrated efficacy:
- Arousal feels energizing. Heightened sexual desire and central arousal are subjectively activating states. A person who feels more interested, more motivated, and more physically aroused may describe that as feeling “more energetic,” but that is a facet of the arousal effect, not an independent energy mechanism.
- The melanocortin system touches metabolism. Because the same receptor family regulates appetite and energy homeostasis, it is tempting to reason that a melanocortin drug must affect “energy.” But energy homeostasis (the long-run balance of intake and expenditure) is not the same as acute felt energy or reduced fatigue, and bremelanotide was not developed or dosed to modulate metabolism.6
- Cardiovascular activation. The transient rise in blood pressure and shift in autonomic tone after dosing could produce a sensation of stimulation in some users. That is a side effect of sympathetic engagement, not a therapeutic energy benefit — and it is a reason for caution, not enthusiasm.
- Marketing drift. In wellness and gray-market contexts, “libido” and “energy” are routinely bundled into a single vitality narrative. That bundling is commercial, not clinical.
There is a more clinically serious version of the energy question worth separating out: fatigue as a symptom of illness, where low libido and low energy travel together. In chronic diseases, depression, and endocrine disorders, desire and vitality are often simultaneously depressed by shared upstream drivers — inflammation, HPA-axis dysregulation, poor sleep, medication effects. Whether a desire-directed melanocortin agonist could indirectly help the libido component of such syndromes is a legitimate research question, explored in the discussion of whether PT-141 can improve fatigue and libido dysregulation in chronic illness and, relatedly, whether it might modulate inflammatory responses in autoimmune disorders. But “might address the libido arm of an illness that also causes fatigue” is a far cry from “enhances energy,” and both of those explorations are hypothesis-generating rather than trial-proven. The responsible position is that bremelanotide’s energy effects are, at present, unestablished, mechanistically unmotivated as a stand-alone claim, and confounded by the arousal and cardiovascular responses that could masquerade as “energy.”
Dosing and Administration in the Clinical and Research Context
Because bremelanotide is an approved drug with a defined label, its dosing is better specified than that of most research peptides — and that specificity is itself informative about the compound’s constraints.
The approved regimen is 1.75 mg administered subcutaneously in the abdomen or thigh, on demand, at least 45 minutes before anticipated sexual activity.1 The label sets a ceiling of one dose per 24 hours and no more than eight doses per month. These limits are not arbitrary; they exist because the side-effect burden — nausea, blood-pressure elevation, and cumulative pigmentation risk with frequent dosing — scales with exposure. The on-demand, capped design reflects a drug whose benefit is modest and whose tolerability is the binding constraint, which is why it is dosed episodically rather than continuously.
Several administration details follow from the pharmacology. The 45-minute pre-dose interval reflects the time to central engagement rather than an instantaneous effect. The subcutaneous route was chosen specifically because the earlier intranasal formulation produced unacceptable blood-pressure spikes; the slower subcutaneous absorption blunts that peak.4 The label also directs that a dose should be avoided if it would coincide with situations where a transient blood-pressure rise is hazardous. For anyone handling lyophilized research-grade peptide rather than the pre-filled autoinjector, the general principles of reconstitution and sterile handling are the same as for any peptide and are covered in the site’s peptide reconstitution guide; terminology used throughout this article is defined in the peptide glossary. It cannot be overstated, however, that reconstitution technique changes nothing about the evidence: a perfectly prepared vial does not create an energy benefit that trials never measured, and material sold outside regulated channels carries purity, sterility, and dosing-accuracy risks entirely separate from the molecule’s intrinsic pharmacology.
How Bremelanotide Compares With Other Options
Placing bremelanotide beside the agents it is most often confused with clarifies what makes it distinctive — a centrally acting, on-demand desire drug — and what it is not.
| Agent | Mechanism | Approved use / status | Key contrast with bremelanotide |
|---|---|---|---|
| Bremelanotide (Vyleesi) | Central melanocortin (MC3R/MC4R) agonist; acts on desire circuitry5 | FDA-approved 2019 for acquired, generalized HSDD in premenopausal women1 | — |
| Flibanserin (Addyi) | 5-HT1A agonist / 5-HT2A antagonist; daily central serotonergic modulation | FDA-approved for HSDD in premenopausal women; taken daily | Daily dosing, weeks to effect, alcohol interaction — vs on-demand melanocortin |
| Sildenafil / PDE5 inhibitors | Peripheral vasodilation via cGMP; increases genital blood flow | Approved for erectile dysfunction (men) | Peripheral “plumbing” vs central “desire”; does not address low desire |
| Transdermal testosterone (off-label) | Androgen replacement affecting the hormonal substrate of desire | Not FDA-approved for female HSDD; used off-label in some settings | Hormonal axis vs non-hormonal central neuromodulation |
| Melanotan II | Non-selective melanocortin agonist (parent-class compound) | Not approved for any indication; unregulated | Shared receptor class, but no controlled desire-disorder evidence base |
The comparison highlights bremelanotide’s actual niche. Against flibanserin — the other FDA-approved HSDD drug — the differences are practical: flibanserin is a daily serotonergic agent requiring weeks of continuous use and carrying an alcohol-interaction warning, whereas bremelanotide is taken only when wanted and works through an entirely different (melanocortin) system.2 Against PDE5 inhibitors, the contrast is mechanistic and often misunderstood: sildenafil improves the hardware of erection by increasing blood flow but does nothing for desire, while bremelanotide targets desire and central arousal and is not a blood-flow drug. Against off-label testosterone, the distinction is that bremelanotide is non-hormonal and does not manipulate the gonadal-steroid axis. And against its own parent, Melanotan II, the lesson is cautionary: they share a receptor class, but only bremelanotide has been through controlled desire-disorder trials and regulatory review; Melanotan II remains unapproved and unstandardized.
Notably, none of these comparators are energy drugs, and bremelanotide’s supposed edge in “energy” does not appear in any head-to-head or single-agent comparison because the outcome was never measured. The honest competitive framing is desire-versus-desire and mechanism-versus-mechanism, not vitality.
Safety and Tolerability
Bremelanotide’s safety profile is well characterized from the Phase 3 program and reflected in its labeling, and it is the area where honest counseling matters most, because the tolerability burden is substantial for a modest-benefit, quality-of-life drug.
The most common adverse reaction, by a wide margin, is nausea: roughly 40% of treated women experienced nausea in the RECONNECT trials, versus about 1% on placebo, and a meaningful minority required an anti-nausea medication or discontinued because of it.1 Flushing (about 20%), injection-site reactions (about 13%), and headache (about 11%) were the next most frequent.1 These are consequences of broad melanocortin agonism and central autonomic engagement.
Two label warnings deserve particular attention:
- Transient blood-pressure increase and heart-rate decrease. Each dose produces a transient rise in blood pressure (on the order of a few mmHg systolic in healthy users, peaking a few hours post-dose) and a small fall in heart rate, typically resolving within about 12 hours.1 Because of this, the label directs consideration of cardiovascular risk before initiation, advises that blood pressure be controlled, and contraindicates use in people with uncontrolled hypertension or known cardiovascular disease. This is the mature, subcutaneous echo of the very signal that killed the intranasal ED program.4
- Focal hyperpigmentation. Because bremelanotide activates MC1R (the pigmentation receptor), it can cause darkening of the skin and gums, including the face and breasts. This was reported in about 1% of patients dosed up to eight times per month, with higher risk in people with darker skin and with more frequent dosing, and it did not always fully resolve after stopping.1 This is the monthly-dose cap’s central justification.
The compound is not associated with clinically apparent liver injury, and dedicated pharmacovigilance summaries classify the hepatotoxicity risk as low, consistent with its peptide nature and episodic dosing.12 The label also notes reduced efficacy and increased nausea when taken with alcohol in some contexts, and interactions with certain orally administered drugs whose absorption bremelanotide can slow. Importantly, the entire safety database is drawn from premenopausal women dosed on demand for HSDD; it does not license conclusions about long-term daily use, use in men, use in postmenopausal or medically complex populations, or — the recurring theme — use for “energy,” a setting in which the risk-benefit calculus has simply never been evaluated. A tolerability profile acceptable for a distressing, diagnosed desire disorder is not automatically acceptable for an unproven vitality claim in an unstudied population.
Limitations and the Evidence Gaps
Pulling the threads together, the limitations cluster into two very different tiers depending on which half of the title you are asking about.
For libido, the limitations are the ordinary ones of a real but modestly effective drug. The effect size is small; placebo responses in HSDD are large; the benefit was demonstrated on desire and distress rather than on the frequency of satisfying events; and the entire evidence base is confined to premenopausal women with a specific, distress-defined diagnosis.2 Extrapolating the desire benefit to men, to postmenopausal women, or to people without HSDD is unsupported by controlled data, even though the mechanism is plausible in those groups. These are the normal boundaries of an approved indication, not signs that the core claim is unsound.
For energy, the limitation is more fundamental: there is essentially no evidence at all. No pivotal trial measured energy or fatigue as an efficacy outcome; no validated instrument grounds an energy claim; and the mechanism does not straightforwardly predict a stand-alone energy effect. Every statement that bremelanotide “boosts energy” is therefore inference or marketing rather than finding, and the most likely explanations for the perception — arousal-linked activation and cardiovascular stimulation — are as much cautions as they are benefits. On this half of the title, the appropriate scientific posture is not skepticism-for-its-own-sake but simple accuracy: the question is open and largely unstudied.
A cross-cutting limitation applies to both halves: much of the bremelanotide that circulates in research and wellness settings is not the pharmaceutical product but unregulated material of variable purity and dosing accuracy. Even well-designed observations made with such material are confounded, and safety expectations calibrated on the pharmaceutical formulation and its capped regimen do not transfer to unstandardized use. For readers tracking how the broader peptide evidence base evolves, the site’s dosing references and educational catalog under the dosages index are organized for study rather than as guidance for human use.
Regulatory Status
Bremelanotide’s regulatory picture is unusually clear compared with most research peptides, and that clarity is worth stating precisely because it is so often blurred.
An approved drug — for one thing. The FDA approved bremelanotide as Vyleesi in June 2019 for acquired, generalized HSDD in premenopausal women, making it the second approved pharmacotherapy for female HSDD (after flibanserin) and the first approved for on-demand use.1 The approval is specific: it is not for postmenopausal women, not for men, not for sexual-performance enhancement, and emphatically not for energy, vitality, or fatigue. Any use outside acquired, generalized HSDD in premenopausal women is off-label.
Not approved for men, despite the origins. Although bremelanotide’s earliest development targeted erectile dysfunction in men, that program did not result in an approval; the male-ED and intranasal tracks were discontinued after the blood-pressure findings.4 Contemporary use in men is therefore off-label and unsupported by a completed registration program, notwithstanding the plausible shared mechanism.
No approval anywhere for “energy.” No regulator has recognized an energy, fatigue, or vitality indication for bremelanotide, and no such indication has been sought, because no adequate and well-controlled trials support one. Marketing that implies otherwise is making a claim the regulatory record does not sustain.
Gray-market realities. A large share of the “PT-141” sold online is research-grade or compounded material outside the approved product and its labeling. Such material is not subject to the manufacturing, purity, and pharmacovigilance controls that underpin the safety statements above, and its use for any purpose — libido or the unproven “energy” — sits outside the evidence and the regulatory framework alike. The appropriate path for any legitimate exploration beyond the approved indication is a properly controlled clinical trial, not off-label or unregulated use.
The regulatory synthesis, then, mirrors the scientific one: a real, approved, narrowly bounded libido drug with a well-documented but demanding safety profile, and no regulatory footing whatsoever for the energy claim embedded in the popular framing.
Frequently Asked Questions
Is PT-141 (bremelanotide) FDA-approved, and for what?
Yes, but narrowly. The FDA approved bremelanotide as Vyleesi in 2019 for acquired, generalized hypoactive sexual desire disorder (HSDD) in premenopausal women, given as a 1.75 mg subcutaneous injection on demand.1 It is not approved for postmenopausal women, not approved for men, not approved to enhance sexual performance, and not approved for energy, fatigue, or vitality. Any other use is off-label.
Does bremelanotide actually work through neuroendocrine pathways?
Yes. It is an agonist at central melanocortin receptors (mainly MC3R and MC4R) in hypothalamic and preoptic circuits that regulate sexual motivation, and it signals through cAMP/PKA to shift downstream dopaminergic and oxytocinergic tone.56 A functional-MRI study in women with HSDD showed it changes activity in sexual-processing brain regions, providing direct evidence that the effect is genuinely central and neuroendocrine rather than peripheral.8
Does it enhance energy?
There is no direct evidence that it does. Energy, fatigue, and vitality were not endpoints in the pivotal trials, no validated fatigue measure supports an energy claim, and the mechanism does not clearly predict a stand-alone energy effect.12 Any energizing sensation is most plausibly a facet of heightened arousal or of the transient cardiovascular activation the drug produces — not a demonstrated therapeutic benefit. On the energy question, the honest answer is that it is unstudied.
How strong is the libido effect?
Statistically robust but clinically modest. In the RECONNECT Phase 3 trials, bremelanotide improved the FSFI desire domain by about 0.35 points and reduced desire-related distress by about 0.33 points more than placebo (P < 0.001 integrated), with benefits sustained over a 52-week extension.29 These are real, reproducible improvements, but they are moderate in size, and placebo responses in HSDD trials are large.
How is it different from Viagra or flibanserin?
PDE5 inhibitors like sildenafil act peripherally to increase genital blood flow and do nothing for desire; bremelanotide acts centrally on desire and arousal circuitry and is not a blood-flow drug.5 Flibanserin is the other FDA-approved HSDD drug but works on serotonin receptors, must be taken daily for weeks, and carries an alcohol-interaction warning, whereas bremelanotide is a melanocortin agonist taken on demand.2
What are the main side effects?
Nausea is by far the most common, affecting about 40% of treated women, followed by flushing (~20%), injection-site reactions (~13%), and headache (~11%).1 Each dose causes a transient rise in blood pressure and a small drop in heart rate, so it is contraindicated in uncontrolled hypertension or cardiovascular disease, and repeated dosing can cause focal skin and gum hyperpigmentation via MC1R, which does not always fully resolve.1
Can it be used in men?
Not on an approved basis. Bremelanotide’s earliest development targeted erectile dysfunction in men, but that program was discontinued after blood-pressure concerns, and no approval for men was granted.4 The mechanism is plausibly relevant to male desire and erection, but current use in men is off-label and not backed by a completed registration program.
Why is it prescribed as an on-demand injection with a monthly cap?
Because the benefit is modest and the tolerability is the limiting factor. The label caps dosing at once per 24 hours and eight times per month largely to limit cumulative nausea, blood-pressure effects, and pigmentation risk, which scale with exposure.1 The episodic design fits a quality-of-life drug whose risk-benefit favors occasional, as-needed use over continuous dosing.
Is the “PT-141” sold online the same as Vyleesi?
Often not. Much online “PT-141” is research-grade or compounded material outside the approved product and its manufacturing, purity, and safety controls. The efficacy and safety data described here come from the pharmaceutical formulation dosed within its labeled regimen; they do not transfer to unregulated material used off-label, and certainly not to unstudied uses such as “energy.”
References
- U.S. Food and Drug Administration. VYLEESI (bremelanotide injection) prescribing information. Initial U.S. approval 2019. https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/210557s000lbl.pdf
- Kingsberg SA, Clayton AH, Portman D, Williams LA, Krop J, Jordan R, Lucas J, Simon JA. Bremelanotide for the Treatment of Hypoactive Sexual Desire Disorder: Two Randomized Phase 3 Trials. Obstet Gynecol. 2019;134(5):899-908. PMID 31599840. https://pubmed.ncbi.nlm.nih.gov/31599840/
- Molinoff PB, Shadiack AM, Earle D, Diamond LE, Quon CY. PT-141: a melanocortin agonist for the treatment of sexual dysfunction. Ann N Y Acad Sci. 2003;994:96-102. PMID 12851303. https://pubmed.ncbi.nlm.nih.gov/12851303/
- Diamond LE, Earle DC, Rosen RC, Willett MS, Molinoff PB. Double-blind, placebo-controlled evaluation of the safety, pharmacokinetic properties and pharmacodynamic effects of intranasal PT-141, a melanocortin receptor agonist, in healthy males and patients with mild-to-moderate erectile dysfunction. Int J Impot Res. 2004;16(1):51-59. PMID 14963471. https://pubmed.ncbi.nlm.nih.gov/14963471/
- King SH, Mayorov AV, Balse-Srinivasan P, Hruby VJ, Vanderah TW, Wessells H. Melanocortin receptors, melanotropic peptides and penile erection. Curr Top Med Chem. 2007;7(11):1098-1106. PMID 17584130. https://pubmed.ncbi.nlm.nih.gov/17584130/
- Cone RD. Anatomy and regulation of the central melanocortin system. Nat Neurosci. 2005;8(5):571-578. PMID 15856065. https://pubmed.ncbi.nlm.nih.gov/15856065/
- Diamond LE, Earle DC, Heiman JR, Rosen RC, Perelman MA, Harning R. An effect on the subjective sexual response in premenopausal women with sexual arousal disorder by bremelanotide (PT-141), a melanocortin receptor agonist. J Sex Med. 2006;3(4):628-638. PMID 16839319. https://pubmed.ncbi.nlm.nih.gov/16839319/
- Thurston L, Hunjan T, Ertl N, et al. Melanocortin 4 receptor agonism enhances sexual brain processing in women with hypoactive sexual desire disorder. J Clin Invest. 2022;132(19):e152341. PMID 36189794. https://pubmed.ncbi.nlm.nih.gov/36189794/
- Simon JA, Kingsberg SA, Portman D, Williams LA, Krop J, Jordan R, Lucas J, Clayton AH. Long-Term Safety and Efficacy of Bremelanotide for Hypoactive Sexual Desire Disorder. Obstet Gynecol. 2019;134(5):909-917. PMID 31599847. https://pubmed.ncbi.nlm.nih.gov/31599847/
- Simon JA, Kingsberg SA, Portman D, Jordan R, Lucas J, Sadiq A, Krop J, Clayton AH. Prespecified and Integrated Subgroup Analyses from the RECONNECT Phase 3 Studies of Bremelanotide. J Womens Health (Larchmt). 2022;31(3):391-400. PMID 35230162. https://pubmed.ncbi.nlm.nih.gov/35230162/
- Clayton AH, Goldstein I, Kim NN, et al. The International Society for the Study of Women’s Sexual Health Process of Care for Management of Hypoactive Sexual Desire Disorder in Women. Mayo Clin Proc. 2018;93(4):467-487. PMID 29545008. https://pubmed.ncbi.nlm.nih.gov/29545008/
- LiverTox: Clinical and Research Information on Drug-Induced Liver Injury. Bremelanotide. National Institute of Diabetes and Digestive and Kidney Diseases; Bethesda (MD). NBK573221. https://www.ncbi.nlm.nih.gov/books/NBK573221/
Educational and research-use disclaimer: This article is provided solely for scientific and educational purposes. Bremelanotide (PT-141) is approved by the FDA only as Vyleesi for acquired, generalized hypoactive sexual desire disorder in premenopausal women; it is not approved for use in men, in postmenopausal women, for sexual-performance enhancement, or for any “energy,” fatigue, or vitality indication, and no adequate controlled trials support an energy effect. Nothing here is medical advice or a recommendation for human use, and much material sold as “PT-141” is unregulated and of uncertain purity. Any use outside the approved indication is off-label, and any legitimate investigation beyond it should occur within properly authorized clinical research under appropriate medical and regulatory oversight. Readers should consult qualified healthcare professionals before making any decisions.