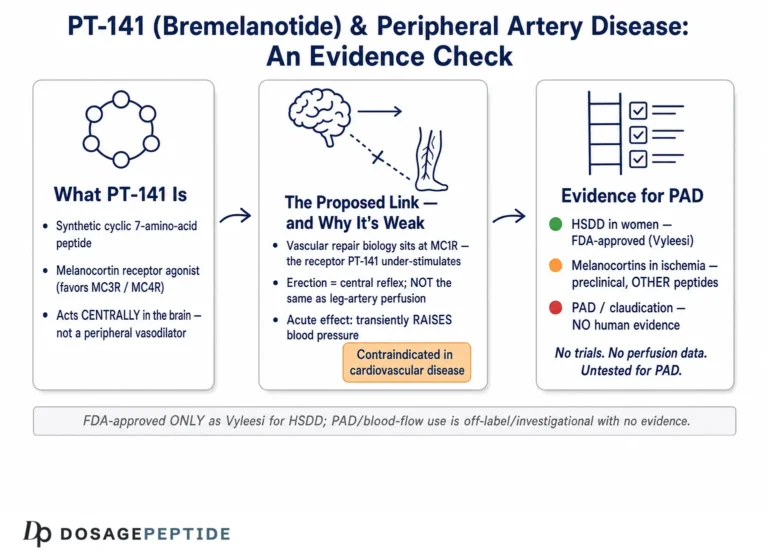
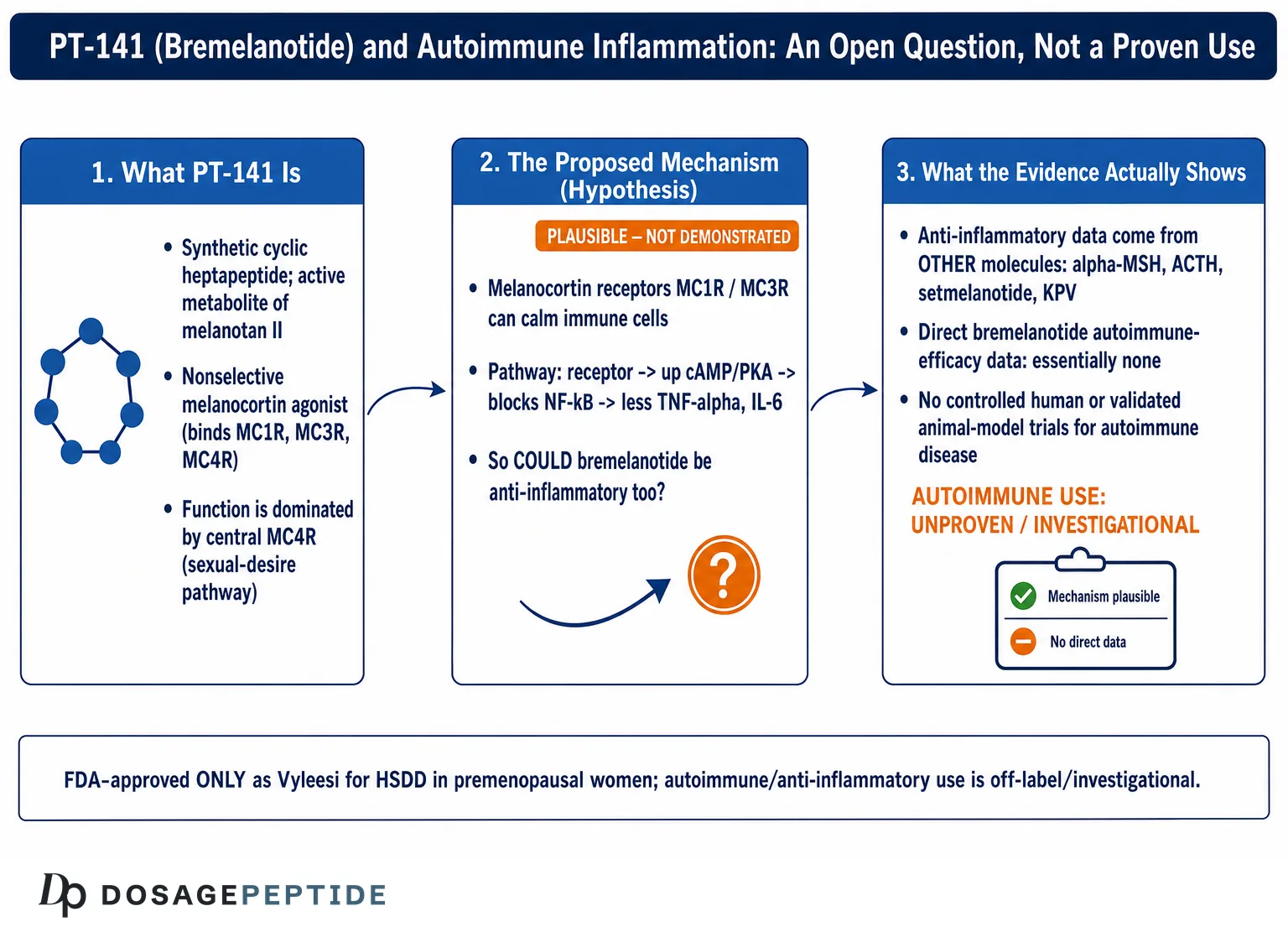
PT-141, known by its International Nonproprietary Name bremelanotide, is a synthetic cyclic heptapeptide that reaches the general public through a very specific door: it is the active ingredient in Vyleesi, a drug-device combination approved by the U.S. Food and Drug Administration in 2019 for one narrow indication — acquired, generalized hypoactive sexual desire disorder (HSDD) in premenopausal women.1 That approved use has almost nothing to do with the question posed in this article’s title. The reason the question gets asked at all is that bremelanotide belongs to a receptor family — the melanocortin system — that immunologists have studied for decades as a native brake on inflammation. From that overlap grows a tempting inference: if melanocortin receptor activation calms immune cells, and if bremelanotide activates melanocortin receptors, might bremelanotide “modulate inflammatory responses in autoimmune disorders”?
This article treats that inference as an open research question, not a settled fact, because that is what the literature supports. There is a genuine, well-documented body of preclinical and mechanistic work showing that the melanocortin system regulates inflammation. There is also a striking absence of direct, controlled evidence that bremelanotide specifically improves any autoimmune condition in humans or even in validated animal disease models. Most of the anti-inflammatory melanocortin data come from other molecules — the natural ligands alpha-melanocyte-stimulating hormone (α-MSH) and adrenocorticotropic hormone (ACTH), the MC1R/MC3R-focused analogs, and selective agonists such as setmelanotide — whose receptor preferences differ meaningfully from bremelanotide’s.2,3 Conflating “the melanocortin system is anti-inflammatory” with “bremelanotide treats autoimmune disease” is precisely the kind of leap this page exists to resist.
What follows is an evidence-cautious walkthrough for readers and researchers who want to understand where the hypothesis comes from, why it is biologically plausible, and — just as importantly — why plausibility is not proof. Nothing here is medical advice, a protocol, or an endorsement of any off-label use. Bremelanotide is not an approved, established, or evidence-supported treatment for rheumatoid arthritis, multiple sclerosis, inflammatory bowel disease, lupus, uveitis, or any other autoimmune disorder. The goal is to map the science honestly, flag the gaps loudly, and let the size of the human-evidence deficit speak for itself.
What PT-141 (Bremelanotide) Is, and Where It Came From
Bremelanotide is a synthetic, cyclic seven-amino-acid peptide (a heptapeptide) built on the pharmacophore shared by all melanocortin peptides: the core His-Phe-Arg-Trp sequence that natural α-MSH uses to engage melanocortin receptors. Its lineage is direct and worth understanding, because the lineage is what created its receptor personality. Bremelanotide is the primary active metabolite of melanotan II (MT-II), a superpotent, cyclic α-MSH analog originally synthesized in the 1980s and 1990s during university efforts to develop a “sunless tanning” agent by activating the pigmentation receptor MC1R.4 Researchers noticed that MT-II produced unexpected effects on sexual arousal in early human studies, and attention shifted from tanning to that off-target behavioral effect. Bremelanotide is essentially MT-II with its C-terminal amide replaced by a free carboxylic acid — a small change that removes some of the pigmentary drive and yields a molecule with a shorter, more manageable pharmacokinetic profile.4,5
The commercial development path was rocky and is instructive for anyone weighing bremelanotide’s evidence base. Palatin Technologies first pursued an intranasal formulation for male and female sexual dysfunction. That program was halted in 2008 after intranasal dosing was associated with clinically meaningful increases in blood pressure in some study participants.6 The company then reformulated bremelanotide as a subcutaneous autoinjector, ran the Phase 3 RECONNECT trials in premenopausal women with HSDD, and obtained FDA approval for Vyleesi on June 21, 2019.1,7 The approved product delivers 1.75 mg subcutaneously, self-administered at least 45 minutes before anticipated sexual activity, with hard caps of one dose per 24 hours and eight doses per month.1 Those caps exist largely because of the same cardiovascular signal that ended the intranasal program — a detail that matters when anyone imagines chronic, anti-inflammatory-style dosing.
It is important to separate the two identities the molecule carries. As Vyleesi, bremelanotide is a regulated pharmaceutical with a defined indication, a full prescribing label, and a pharmacovigilance trail. As “PT-141,” the same molecule circulates in the research-chemical and gray markets, sold as a lyophilized powder “for research use only,” where it is discussed in connection with an ever-expanding list of unapproved uses: erectile function in men, general libido, fat loss, neuroprotection, blood-flow enhancement, and — the subject here — inflammation and autoimmunity. None of those research-chemical uses carry the evidentiary weight of the HSDD approval. When you see the string “PT-141” attached to an anti-inflammatory claim, you are looking at the speculative identity, not the regulated one. Our compound-specific overview, the PT-141 (10 mg vial) dosage protocol, lays out the vial-handling and reconstitution context that the research-chemical form is typically discussed in, and it, too, is framed around the approved and studied uses rather than the speculative ones.
Structurally, bremelanotide’s cyclic lactam bridge locks the peptide into a conformation that presents the His-Phe-Arg-Trp motif to the receptor in a constrained way. That constraint is the origin of both its potency and its receptor selectivity, and it is the reason bremelanotide cannot simply be treated as an interchangeable stand-in for α-MSH or ACTH in immunological reasoning. The natural ligands and the therapeutic analogs that dominate the anti-inflammatory melanocortin literature differ from bremelanotide in exactly the dimension — receptor subtype preference — that determines whether a melanocortin will act on immune tissue or on the central circuits that govern arousal and appetite.
The Melanocortin System: Molecular Basis for an Anti-Inflammatory Hypothesis
To understand why bremelanotide gets mentioned near autoimmunity at all, you need the melanocortin system itself, because the anti-inflammatory reputation belongs to the system, not to any single peptide. Melanocortins are a family of peptide hormones — α-, β-, and γ-MSH and ACTH — all cleaved from a single precursor protein, proopiomelanocortin (POMC). They act on five G-protein-coupled receptors, MC1R through MC5R, which are distributed across very different tissues and carry out very different jobs.2 MC1R sits on melanocytes and immune cells and governs pigmentation and macrophage behavior; MC2R is the adrenal ACTH receptor that drives cortisol release; MC3R and MC4R are concentrated in the central nervous system, where they regulate energy balance, feeding, and, relevant to bremelanotide, sexual arousal; MC4R and MC5R appear on additional peripheral and immune populations.2,8
The anti-inflammatory story centers mostly on MC1R and MC3R. Across decades of work, α-MSH and ACTH acting through these receptors have been shown to suppress the master pro-inflammatory transcription factor NF-κB. The mechanism is cAMP-driven: melanocortin receptor activation raises intracellular cyclic AMP, activates protein kinase A, and blocks TNF-α-induced NF-κB activation in a dose- and time-dependent manner.2 Downstream, this translates into reduced production of TNF-α, IL-1β, IL-6, and IL-8, and increased production of the anti-inflammatory cytokine IL-10.2 On macrophages, MC3R activation reduces phagocytosis, dampens chemokine release, and cuts neutrophil accumulation at inflamed sites — the cellular signature of an immune “off switch.”2,3
It also helps to appreciate why evolution built anti-inflammatory logic into a pigmentation-and-appetite hormone family at all. The melanocortin system is one of the body’s endogenous “resolution” circuits — part of the machinery that not only starts but actively terminates inflammation once a threat is cleared. α-MSH is produced locally by immune cells themselves, not merely delivered from the pituitary, and this local production creates a feedback loop in which an inflamed tissue can generate its own braking signal.2 That biology is genuinely elegant and is a large part of why the melanocortin system has attracted serious pharmaceutical interest as a source of “steroid-sparing” anti-inflammatory agents that might calm immune activation without the broad metabolic toll of glucocorticoids.3 The catch, again, is that harvesting this biology therapeutically has favored selective and fragment agonists engineered for immune receptors — not broad central agonists like bremelanotide. The promise of the system is real; the question is which molecule can capture it cleanly.
Two additional threads round out the picture. First, ACTH’s oldest therapeutic use is as an anti-inflammatory. Repository corticotropin injection (Acthar Gel) has been FDA-approved since 1952 and is used across a striking range of autoimmune and inflammatory conditions — infantile spasms, multiple sclerosis relapses, rheumatoid arthritis, and systemic lupus — historically assumed to work only by triggering adrenal cortisol release, but now understood to also exert glucocorticoid-independent anti-inflammatory effects through direct MC3R signaling on immune cells.2 Second, the anti-inflammatory activity survives fragmentation of the parent peptide: the C-terminal tripeptide of α-MSH, KPV (Lys-Pro-Val), retains much of the anti-inflammatory effect while shedding the pigmentary action, which is why KPV has become a distinct object of study in its own right.2 For readers tracking that adjacent thread, our KPV (10 mg vial) dosage protocol covers the α-MSH fragment that carries the cleanest anti-inflammatory melanocortin signal.
Here is where the hypothesis for bremelanotide is born and where it starts to strain. The system-level story is real and reasonably robust: melanocortin receptors, especially MC1R and MC3R, are legitimate anti-inflammatory nodes, and the field has explored MC1R- and MC3R-selective agonists precisely to exploit this without the appetite, arousal, or pigmentation effects of broad agonism.3 But bremelanotide is not an MC1R- or MC3R-selective anti-inflammatory analog. It was engineered and selected for central MC4R-driven behavioral effects. The next section examines exactly how its receptor profile lines up — and fails to line up — with the receptors that matter most for immune modulation.
How Bremelanotide’s Receptor Profile Maps Onto Immune Signaling
The decisive question for the inflammation hypothesis is not “does bremelanotide touch melanocortin receptors” — obviously it does — but “does it engage the specific receptors, on the specific cells, that produce anti-inflammatory effects, at concentrations that are achievable and safe.” On each of those sub-questions the picture is more complicated than promotional material suggests.
Bremelanotide is a nonselective melanocortin agonist. The FDA-approved Vyleesi label characterizes it as activating multiple receptor subtypes with an order of potency of MC1R ≥ MC4R ≥ MC3R > MC5R > MC2R.1 Notably, the label itself lists MC1R at the top of that potency order — the very receptor most tied to macrophage anti-inflammatory activity — which is one reason the anti-inflammatory conversation is not baseless. At the same time, much of the pharmacology and clinical-review literature emphasizes that bremelanotide’s functional and behaviorally relevant activity is dominated by central MC4R (and to a lesser extent MC3R) engagement, since MC4R is the receptor through which it produces its approved effect on sexual desire.5,8 The two framings are not contradictory: potency at a receptor in a transfected assay is not the same as physiologically dominant signaling in a living animal, where receptor density, tissue distribution, and drug exposure at the relevant site all intervene.
This gap between “binds MC1R in a dish” and “produces MC1R-mediated anti-inflammatory effects in tissue” is the crux. The macrophage and microglial anti-inflammatory effects catalogued in the melanocortin literature are demonstrated primarily with α-MSH, NDP-α-MSH, MC1R-selective agonists, and MC3R-directed compounds — molecules chosen or engineered for immune-cell receptors.2,3 Bremelanotide has not been the workhorse of that literature. When immunologists want to probe MC1R or MC3R anti-inflammatory biology, they reach for tool compounds with cleaner selectivity, not for a centrally acting MC4R agonist optimized for a behavioral endpoint.
There is a plausible peripheral-signaling counterargument worth stating fairly. Because bremelanotide does have measurable MC1R and MC3R affinity, one can hypothesize that at some dose it could engage immune-cell melanocortin receptors and nudge them toward an anti-inflammatory phenotype. The setmelanotide literature makes the general idea more credible: setmelanotide, an MC4R-selective agonist approved for rare genetic obesity, was shown in a 2019 study to reduce TNF-α/IFN-γ-induced chemokines (CCL2, CXCL10) and to raise IL-6 and IL-11 in MC4R-overexpressing human astrocytes, shifting neighboring macrophages toward an M2 (anti-inflammatory) phenotype — effects blocked by an MC4R antagonist, confirming receptor specificity.9 That study establishes that even an MC4R-centric agonist can have anti-inflammatory actions in the right cellular context. But it studied setmelanotide, in engineered astrocytes, using micromolar concentrations — not bremelanotide, not in an autoimmune animal model, and not at exposures matched to the approved 1.75 mg human dose.
The honest synthesis is this: bremelanotide’s receptor profile makes an anti-inflammatory effect conceivable rather than demonstrated. It hits receptors that, in other hands and with other molecules, do anti-inflammatory work. Whether bremelanotide itself, at tolerable doses, meaningfully engages those pathways in autoimmune tissue is an empirical question that the existing data do not answer. The receptor map is an invitation to research, not a substitute for it.
Key Evidence: What Actually Exists, and Its Honest Level
If we grade the evidence for the specific claim — “bremelanotide modulates inflammatory responses in autoimmune disorders” — the honest grade is very low, and largely indirect. It is worth being explicit about the tiers of evidence so the gap is unmistakable.
Tier 1 — System-level and other-molecule evidence (moderate and real, but not about bremelanotide). The strongest melanocortin-inflammation evidence concerns α-MSH, ACTH/Acthar, MC1R/MC3R agonists, and setmelanotide. In these bodies of work, melanocortin agonism reduces neutrophil influx and joint swelling in models of arthritis, shows MC3R-dependent benefit in models of gouty arthritis, ameliorates experimental autoimmune encephalomyelitis (the standard multiple sclerosis model) by limiting central and peripheral inflammation, and shows protective effects in models of uveitis, colitis, sepsis, and reperfusion injury.2,3,9 This tier is legitimate preclinical and, for ACTH, clinical science — but it does not feature bremelanotide as the tested agent.
Tier 2 — Mechanistic plausibility for bremelanotide (weak, inferential). Bremelanotide binds MC1R, MC3R, and MC4R, all of which have anti-inflammatory roles in the broader literature.1,8 The setmelanotide astrocyte data show an MC4R agonist can be anti-inflammatory in a defined system.9 These support a hypothesis; they are not evidence of an effect from bremelanotide.
Tier 3 — Direct bremelanotide anti-inflammatory or autoimmune data (essentially absent). This is the tier that would actually answer the title question, and it is close to empty. Bremelanotide was historically explored in preclinical work on hemorrhagic shock and ischemia-reperfusion — contexts involving inflammatory cascades — but that development program was discontinued and did not yield an approved or well-substantiated anti-inflammatory indication.6 There is no robust, peer-reviewed, controlled body of work demonstrating that bremelanotide improves rheumatoid arthritis, multiple sclerosis, lupus, IBD, or any autoimmune disorder in animals bred to model those diseases, let alone in patients. The clinical trial record for bremelanotide is overwhelmingly about sexual dysfunction (the RECONNECT program) and, more recently, exploratory metabolic endpoints.7,10
| Evidence tier | What it shows | Concerns bremelanotide directly? | Strength |
|---|---|---|---|
| System / other molecules | Melanocortin agonism (α-MSH, ACTH, MC1R/MC3R agonists, setmelanotide) is anti-inflammatory across many models | No | Moderate (preclinical) to established (ACTH/Acthar clinical) |
| Mechanistic plausibility | Bremelanotide binds MC1R/MC3R/MC4R, receptors implicated in anti-inflammatory signaling | Partially (binding only) | Weak / inferential |
| Direct autoimmune data | Bremelanotide improves an autoimmune disorder | Yes — but essentially no such data exist | Absent |
It is worth dwelling on why the historical hemorrhagic-shock work does not rescue the autoimmune claim, since vendors sometimes cite it as if it did. Hemorrhagic shock and ischemia-reperfusion injury are acute, sterile inflammatory events driven by sudden loss and restoration of blood flow — a very different biology from the chronic, antigen-driven, adaptive-immune-mediated process of an autoimmune disease like rheumatoid arthritis or multiple sclerosis. A signal in an acute reperfusion model, even if it had been robust and successfully developed (it was not), would say little about whether the same molecule could restrain a self-sustaining autoimmune attack over months or years. The two problems differ in their triggering mechanisms, the immune-cell populations involved, the required duration of intervention, and the endpoints that define success. Borrowing an acute-injury rationale to support a chronic-autoimmune claim is a second layer of extrapolation stacked on top of the molecule-and-species gaps already discussed — and each layer multiplies the uncertainty rather than adding to the evidence.
The practical takeaway is that anyone citing “melanocortin anti-inflammatory research” to justify bremelanotide for autoimmune conditions is borrowing credibility from Tier 1 and spending it on a Tier 3 claim that has not been earned. The molecules that carry the anti-inflammatory data are not bremelanotide, and the receptor-selectivity differences are not cosmetic. Until a study administers bremelanotide in a validated autoimmune model and measures disease-relevant outcomes against controls, the title question remains genuinely open.
Comparisons: Bremelanotide vs. Other Melanocortin and Anti-Inflammatory Peptides
Placing bremelanotide beside the peptides that actually anchor the anti-inflammatory melanocortin literature clarifies why it is a poor fit for the autoimmune hypothesis despite belonging to the same family. The comparison is not about which molecule is “better” — it is about which molecule’s design and evidence base match the claim being made.
| Agent | Class / origin | Receptor emphasis | Anti-inflammatory evidence | Regulatory status |
|---|---|---|---|---|
| Bremelanotide (PT-141) | Synthetic cyclic heptapeptide; MT-II metabolite | Nonselective; MC1R/MC4R/MC3R, functionally MC4R-dominant | Essentially none directly for autoimmunity | FDA-approved (Vyleesi) for HSDD only |
| α-MSH | Endogenous POMC-derived peptide | MC1R, MC3R, MC4R, MC5R | Extensive preclinical anti-inflammatory data | Not an approved drug |
| ACTH (Acthar Gel) | Endogenous corticotropin / repository injection | MC2R (cortisol) + MC3R (direct) | Clinical use in MS relapse, RA, lupus, infantile spasms | FDA-approved since 1952 |
| Setmelanotide | Synthetic MC4R-selective agonist | MC4R-selective | Preclinical anti-inflammatory (astrocytes, macrophages) | FDA-approved for rare genetic obesity |
| KPV | C-terminal tripeptide of α-MSH | Anti-inflammatory core, minimal pigmentary action | Preclinical anti-inflammatory (e.g., colitis models) | Not an approved drug |
Several contrasts jump out. ACTH is the only melanocortin with an actual autoimmune track record in humans, and it works substantially through adrenal cortisol release plus direct MC3R signaling — a mechanism bremelanotide does not share, since bremelanotide has minimal MC2R activity and therefore does not meaningfully drive the adrenal axis.1,2 Setmelanotide is the melanocortin whose anti-inflammatory cell biology is best characterized in modern receptor-defined systems, and it is MC4R-selective — but it is used for obesity, not autoimmunity, and its anti-inflammatory data remain preclinical.9 KPV and its relatives are the fragments deliberately engineered to keep the anti-inflammatory action while discarding pigmentation and behavioral effects, which is exactly why researchers interested in inflammation gravitate to them rather than to a full agonist like bremelanotide.2
The comparison also underscores a design mismatch. Bremelanotide’s development history selected relentlessly for a central behavioral endpoint — sexual desire — and its dosing, formulation, and safety caps are all built around intermittent, on-demand use. Anti-inflammatory therapy, by contrast, generally requires sustained or repeated exposure to keep immune activation suppressed. A molecule capped at eight doses per month for cardiovascular-safety reasons is structurally ill-suited to the pharmacological pattern an autoimmune indication would demand.1 Readers exploring how peptides are grouped and compared for different research goals may find our peptide dosages catalog and peptide stacks overview useful context for how compound selection is normally reasoned about — matching a molecule’s characterized biology to the question, rather than assuming family membership transfers.
None of this means bremelanotide is uniquely disqualified in principle; it means that if one were designing a serious research program on melanocortin modulation of autoimmunity, bremelanotide would not be the obvious first choice, and the field’s own behavior reflects that. The peptides carrying the anti-inflammatory hopes of the melanocortin community are the selective and fragment agonists, not the approved sexual-desire drug.
Research Models and Methodology in Melanocortin Immunology
Understanding how melanocortin-inflammation research is done makes it easier to judge what any given claim is worth — and to see how far removed most of that methodology is from a demonstration involving bremelanotide. The field relies on a layered set of models, each answering a different question and each with characteristic limitations.
In vitro cell systems are the entry point. Researchers stimulate a defined cell type — macrophages, microglia, astrocytes, chondrocytes, or a monocyte line — with a pro-inflammatory trigger such as lipopolysaccharide (LPS), TNF-α, or IFN-γ, then apply a melanocortin agonist and measure changes in cytokine and chemokine output, NF-κB activation, and cAMP/CREB signaling. The setmelanotide study is a clean example: it used MC4R-overexpressing human astrocytoma cells, stimulated with TNF-α/IFN-γ, and read out CCL2, CXCL10, IL-6, and IL-11, then used the MC4R antagonist SHU9119 to confirm the effect was receptor-mediated.9 The strength of these systems is mechanistic precision; the weakness is that they often use receptor-overexpressing cells and micromolar drug concentrations that may not reflect physiological receptor density or achievable in-vivo exposure.
Animal disease models are the next tier and the one that most directly tests a therapeutic hypothesis. Each autoimmune disease has one or more canonical models: experimental autoimmune encephalomyelitis (EAE) for multiple sclerosis, collagen-induced arthritis and monosodium-urate models for rheumatoid and gouty arthritis, experimental autoimmune uveitis for uveitis, and dextran-sulfate or TNBS colitis for inflammatory bowel disease.2,3 In these, an agonist is dosed and investigators track clinical disease scores, histology, immune-cell infiltration, and cytokine profiles. Melanocortin agonists — α-MSH, NDP-MSH, MC1R/MC3R-directed compounds — have shown benefit across several of these, and knockout or receptor-antagonist experiments have been used to pin the effect to specific receptors (for example, MC3R-dependence in gouty arthritis and MC5R-dependence in some uveitis protection).2,3 The crucial methodological point for this article: these disease-model demonstrations were, in the main, not performed with bremelanotide.
Human tissue and genetic studies add a translational layer. Investigators examine post-mortem or biopsy tissue for melanocortin receptor expression at disease sites — the setmelanotide work found MC4R immunoreactivity elevated in active multiple sclerosis lesions — and population studies probe whether melanocortin receptor gene polymorphisms track with inflammatory traits and disease susceptibility.9,11 These strengthen the biological case that the melanocortin system is engaged in human autoimmune pathology, but they are associational and cannot establish that dosing any particular agonist changes outcomes.
Human clinical trials are the top of the pyramid and the tier where bremelanotide’s autoimmune record is blank. Bremelanotide’s registered trials cluster around sexual dysfunction (notably the RECONNECT Phase 3 studies) and exploratory metabolic work, not autoimmune disease.7,10 For the melanocortin system as a whole, the closest thing to autoimmune clinical validation is ACTH/Acthar’s long regulatory history — a different molecule with a partly different mechanism.2 A researcher evaluating the title question should therefore ask, of any cited study, three questions: Which molecule? Which model tier? Which receptor was implicated? For bremelanotide-and-autoimmunity specifically, the answers rarely survive scrutiny, because the direct studies simply have not been done.
Safety and Tolerability: What Is Known From the Approved Indication
Because there are no controlled autoimmune-use safety data for bremelanotide, the only rigorous tolerability information comes from its approved on-demand HSDD use — and that profile is directly relevant to why chronic anti-inflammatory dosing would be problematic. This section summarizes what the label and pharmacovigilance record actually show; it is descriptive, not a clearance for any off-label use.
In the Vyleesi trials, the most common adverse reactions were nausea (reported by roughly 40% of users, most pronounced with the first injection and sometimes severe enough to warrant an antiemetic), flushing (about 20%), injection-site reactions (about 13%), headache (about 11%), and vomiting.1,12 Nausea led a meaningful minority of participants to discontinue. These are on-demand, single-dose figures; the frequency and cumulative burden under the repeated dosing an anti-inflammatory strategy would imply are simply unknown.
The cardiovascular signal is the most consequential. Each bremelanotide dose produces a transient increase in blood pressure (on the order of 6 mmHg systolic and 3 mmHg diastolic on average, peaking a few hours post-dose) and a compensatory decrease in heart rate, effects that typically resolve within about 12 hours.1 This is precisely why the label restricts use to no more than one dose per 24 hours and eight per month, contraindicates the drug in people with uncontrolled hypertension or known cardiovascular disease, and warns against use in anyone at high cardiovascular risk.1 Any hypothetical anti-inflammatory regimen — which would presumably require far more frequent dosing than eight times a month — runs headlong into the exact safety limit that shaped the approved product.
Two additional effects deserve emphasis. First, focal hyperpigmentation: bremelanotide can darken the skin (especially the face, gums, and breasts), an effect more likely with more frequent dosing, and this pigmentation may be permanent even after stopping.1,12 This is a direct consequence of MC1R activation — the same receptor arm that fuels the anti-inflammatory hypothesis — and it illustrates that the receptors of interest do not come with an off switch for their other effects. Second, bremelanotide can transiently reduce the absorption of orally administered drugs by slowing gastric emptying, which was shown to lower exposure to a co-administered oral medication and is flagged as a clinically relevant interaction.1 The LiverTox database records bremelanotide as not associated with clinically apparent liver injury at approved doses, a reassuring but narrow statement tied to the approved use.13
The overarching safety message is that bremelanotide’s known profile was characterized under intermittent, low-frequency, short-term use in a specific population (premenopausal women, cardiovascularly screened). Extrapolating tolerability to the sustained dosing, mixed populations, and comorbidity burden typical of autoimmune disease is unsupported and potentially hazardous. The cardiovascular and pigmentary effects in particular scale in the wrong direction for a chronic anti-inflammatory concept. Nothing in the safety record makes bremelanotide look like a plausible long-term immunomodulator; if anything, it argues the opposite.
Handling and Reconstitution in a Research Context
Because “PT-141” circulates as a lyophilized research powder, and because handling questions come up whenever a peptide is discussed, this section describes the standard laboratory context — strictly as reference information for legitimate research settings, not as instructions for human use. Bremelanotide for any autoimmune purpose is not an approved therapy, and reconstituting a research chemical does not convert it into one.
Research-grade bremelanotide is typically supplied as a lyophilized (freeze-dried) powder in a sealed vial, most commonly in 10 mg quantities, and is reconstituted with bacteriostatic water (water containing 0.9% benzyl alcohol, which permits multi-day storage) rather than sterile water for single-use contexts. A common approach for a 10 mg vial is to add about 3.0 mL of diluent, yielding a concentration near 3.33 mg/mL; on a U-100 insulin syringe, one “unit” mark (0.01 mL) then corresponds to roughly 33 mcg, which is how researchers translate volume marks into peptide quantity.14 The approved Vyleesi product, by contrast, is a fixed 1.75 mg dose in a prefilled autoinjector and requires no reconstitution at all — a reminder that the research-powder workflow is a feature of the gray market, not of the regulated drug. Our PT-141 (10 mg vial) protocol walks through this reconstitution math in the same reference-only spirit.
General handling principles that appear throughout the peptide research literature include reconstituting by directing the diluent stream against the vial wall rather than blasting the powder directly, swirling gently instead of shaking vigorously (peptides can be shear-sensitive and prone to aggregation), protecting the solution from light and heat, and storing the reconstituted material refrigerated at roughly 2–8 °C while keeping lyophilized powder frozen for long-term stability. Reconstituted peptide has a finite shelf life measured in weeks, and any cloudiness, precipitate, or discoloration is a signal to discard. These practices reflect general good laboratory technique; they are not endorsements of self-administration and do not substitute for the controlled, sterile, and regulated conditions any human use would require. Comparable handling logic is discussed in our BPC-157 and TB-500 blend explainer, again as research-context reference.
It bears repeating in this section specifically, because handling guides are so often misread as permission: the existence of a reconstitution procedure says nothing about whether a compound works for a given purpose. You can reconstitute bremelanotide flawlessly and still have zero evidence that it modulates autoimmune inflammation. Purity, sterility, and endotoxin content of gray-market “research chemicals” are also frequently unverified, which introduces an entirely separate set of risks orthogonal to the peptide’s own pharmacology. For the autoimmune question, the handling details are essentially a distraction from the central fact that the efficacy evidence does not exist.
Limitations and the Human-Evidence Gap
This section states plainly the gap that the rest of the article has been circling, because it is the single most important thing a reader should take away. The distance between “biologically interesting hypothesis” and “supported clinical claim” for bremelanotide in autoimmune disease is very large, and several specific deficits define it.
No direct efficacy data. There is no body of controlled trials — and, as far as the accessible literature shows, not even a robust set of validated animal-model studies — testing bremelanotide as a treatment for any autoimmune disorder.7,10 The anti-inflammatory melanocortin evidence rests on other molecules. This is not a case of “early but promising” data for bremelanotide; it is a case of borrowed data from receptor cousins.
Receptor-selectivity mismatch. The anti-inflammatory action of the melanocortin system is concentrated on MC1R and MC3R immune-cell signaling, and the field’s tool compounds and drug candidates are selected accordingly. Bremelanotide is a nonselective agonist whose functionally dominant activity is central MC4R-mediated behavior, and whose MC1R activity brings pigmentary side effects rather than a clean anti-inflammatory readout.1,3,8 Family membership does not guarantee that the specific molecule delivers the family’s most-hoped-for effect.
Dosing and safety incompatibility. Bremelanotide’s approved use is intermittent and capped for cardiovascular safety; anti-inflammatory therapy typically demands sustained suppression of immune activation. The pharmacological patterns are close to opposite, and the transient hypertension and cumulative pigmentation that limit bremelanotide’s approved dosing would be expected to worsen under a chronic regimen.1
Model-to-human translation. Even the strong melanocortin anti-inflammatory data from other molecules sit largely at the in-vitro and animal-model tiers. The history of immunology is full of agents that suppressed cytokines in a dish or improved scores in a mouse and then failed in human autoimmune disease. Extrapolating from α-MSH or setmelanotide cell studies to a human bremelanotide effect requires crossing both the molecule gap and the species gap simultaneously.2,9
Publication and marketing bias. Much of the online content connecting PT-141 to inflammation originates from vendors and interest-driven sources that selectively cite the encouraging system-level literature while omitting the receptor-selectivity and evidence-tier caveats. Primary sources — the FDA label, peer-reviewed reviews, and mechanistic papers — are far more circumspect than the secondary framing suggests.1,2,3
What would it take to close the gap? At minimum: dose-ranging studies of bremelanotide in validated autoimmune animal models with disease-relevant endpoints and receptor-antagonist controls to establish causality; pharmacokinetic work confirming that anti-inflammatory receptor engagement is achievable at tolerable exposures; and, only then, cautious human trials in a defined condition. None of that has happened. Until it does, “Can PT-141 modulate inflammatory responses in autoimmune disorders?” should be read as a question mark, not a claim — an interesting direction for basic research, not a basis for use. Readers comparing how better-substantiated peptides are discussed can contrast this thin record with entries like our Tesamorelin protocol, where an approved indication anchors the discussion.
Regulatory Status
The regulatory picture is the cleanest and least ambiguous part of this entire topic, and it should function as the anchor for everything else. Bremelanotide has exactly one approved identity, and it is narrow.
In the United States, bremelanotide is approved by the FDA as Vyleesi, indicated solely for the treatment of acquired, generalized hypoactive sexual desire disorder in premenopausal women. The approval was granted on June 21, 2019, following the RECONNECT Phase 3 program, and the product is a 1.75 mg subcutaneous autoinjector for on-demand use.1,7 “Acquired” means the low desire developed after a period of normal function; “generalized” means it is not limited to certain situations or partners; and the indication explicitly excludes low desire due to a coexisting medical or psychiatric condition, relationship problems, or medication effects.1 This is a tightly bounded approval, and it is the only claim about bremelanotide that carries the FDA’s evidentiary imprimatur.
Every other use — autoimmune and anti-inflammatory applications, erectile dysfunction in men, general libido enhancement, fat loss, neuroprotection, blood-flow or “vascular” claims, and fatigue — is off-label or purely investigational. Off-label prescribing is legal for licensed clinicians in many jurisdictions, but off-label status is precisely a signal that the FDA has not evaluated safety and efficacy for that purpose; it is not a hidden endorsement. For autoimmune indications specifically, there is no approval, no completed pivotal trial, and no established standard of care involving bremelanotide anywhere.1,13
The “research chemical” market adds a further regulatory wrinkle. PT-141 sold as a lyophilized powder “for research use only” is not manufactured, tested, or released under the standards that govern the approved Vyleesi product. Such material is not FDA-approved for any human use, its purity and sterility are frequently unverified, and marketing it with disease claims can itself run afoul of drug-marketing law. The “for research use only” label is a regulatory boundary, not a wink toward human use. Internationally, regulatory status varies, but no major regulator has approved bremelanotide for an autoimmune or anti-inflammatory indication.
It is also worth noting how the approval itself was reached, because it frames how much weight the single indication can bear. The RECONNECT trials measured desire and distress using validated patient-reported instruments and found statistically significant but clinically modest improvements over placebo — enough to support approval for a symptom-based condition, but firmly within the domain of a behavioral, centrally mediated effect.1,7 Nothing in that evidence base examined immune function, inflammatory markers, or autoimmune outcomes, because those were never the endpoints. An approval, in other words, is only as broad as the questions the pivotal trials actually asked. Reading an anti-inflammatory capability into a sexual-desire approval is not a cautious extrapolation; it is a category error.
The bottom line for readers is simple and worth internalizing: the gap between bremelanotide’s one narrow approval and the sprawling list of speculative uses is exactly the gap between what has been proven and what has merely been hypothesized. On the question this article addresses, the regulatory record and the scientific record agree — both say “unproven.” Treat any source that blurs that line, or that presents an anti-inflammatory or autoimmune use as established, as a source to distrust.
Frequently Asked Questions
Is PT-141 (bremelanotide) approved to treat autoimmune or inflammatory conditions?
No. Bremelanotide is FDA-approved only as Vyleesi for acquired, generalized hypoactive sexual desire disorder in premenopausal women.1 It is not approved — anywhere — for rheumatoid arthritis, multiple sclerosis, lupus, inflammatory bowel disease, uveitis, or any other autoimmune or inflammatory disorder. Any such use is off-label or investigational and is not supported by controlled human evidence.
If the melanocortin system is anti-inflammatory, doesn’t that mean PT-141 is too?
Not necessarily, and this is the central error to avoid. The anti-inflammatory reputation belongs mainly to MC1R- and MC3R-directed signaling and to specific molecules — α-MSH, ACTH, MC1R/MC3R agonists, KPV, and setmelanotide.2,3,9 Bremelanotide is a nonselective agonist whose functionally dominant activity is central MC4R-mediated behavior. Sharing a receptor family does not mean it delivers the family’s anti-inflammatory effects at safe, achievable doses; that is an untested empirical question.
Has bremelanotide ever been studied in inflammation research?
Historically, bremelanotide was explored in preclinical work on hemorrhagic shock and ischemia-reperfusion injury — contexts that involve inflammatory cascades — but that development program was discontinued and did not produce an approved or well-substantiated anti-inflammatory indication.6 There is no robust body of controlled studies testing bremelanotide in validated autoimmune-disease models or in patients with autoimmune conditions.
What is the difference between Vyleesi and “PT-141” sold online?
They contain the same molecule but are worlds apart in regulation. Vyleesi is an FDA-approved, quality-controlled 1.75 mg autoinjector with a full safety label.1 “PT-141” sold as a research powder is not FDA-approved for human use, is labeled “for research use only,” and often has unverified purity and sterility. The research-chemical form is where speculative autoimmune claims circulate; the approved form carries none of them.
Which melanocortin compounds actually have autoimmune evidence?
ACTH (as Acthar Gel) is the melanocortin with a real human autoimmune track record, used in multiple sclerosis relapses, rheumatoid arthritis, lupus, and infantile spasms — working partly through cortisol release and partly through direct MC3R signaling.2 Preclinically, α-MSH, MC1R/MC3R agonists, setmelanotide, and the fragment KPV carry most of the anti-inflammatory data.2,3,9 Bremelanotide is not among the compounds anchoring this evidence.
Are there safety reasons bremelanotide would be a poor chronic anti-inflammatory agent?
Yes. Each dose transiently raises blood pressure and lowers heart rate, which is why the approved label caps use at one dose per 24 hours and eight per month and contraindicates it in cardiovascular disease.1 Anti-inflammatory therapy usually needs sustained dosing, which conflicts directly with that cap. Frequent dosing also increases the risk of focal skin and gum hyperpigmentation, which can be permanent.1,12
Could future research change this picture?
Potentially. The melanocortin system is a legitimate anti-inflammatory target, and the receptor biology makes a bremelanotide effect conceivable in principle. Closing the gap would require dose-ranging studies in validated autoimmune models with receptor-antagonist controls, pharmacokinetic confirmation that anti-inflammatory receptor engagement is achievable at tolerable exposures, and only then cautious human trials.2,9 None of that has been done, so today the honest answer remains “unproven.”
Is this article medical advice?
No. This is educational, research-oriented content. It does not recommend, endorse, or provide instructions for using bremelanotide or any peptide to treat, cure, or prevent any disease. Decisions about diagnosing or managing autoimmune conditions should be made with a qualified, licensed healthcare professional using approved, evidence-based therapies.
References
- U.S. Food and Drug Administration. VYLEESI (bremelanotide injection) Highlights of Prescribing Information, NDA 210557, 2019. accessdata.fda.gov/drugsatfda_docs/label/2019/210557s000lbl.pdf
- Wang W, Guo DY, Lin YJ, Tao YX, et al. Melanocortin Regulation of Inflammation. Frontiers in Endocrinology. 2019;10:683. doi:10.3389/fendo.2019.00683
- Spana C, Taylor AW, Yee DG, Makhlina M, Yang W, Dodd J. Probing the Role of Melanocortin Type 1 Receptor Agonists in Diverse Immunological Diseases. Frontiers in Pharmacology. 2018;9:1535. doi:10.3389/fphar.2018.01535 (PMC6339910)
- Molinoff PB, Shadiack AM, Earle D, et al. PT-141: a melanocortin agonist for the treatment of sexual dysfunction. Annals of the New York Academy of Sciences. 2003;994:96-102.
- Kingsberg SA, Clayton AH, Portman D, et al. Bremelanotide for the Treatment of Hypoactive Sexual Desire Disorder: Two Randomized Phase 3 Trials. Obstetrics & Gynecology. 2019;134(5):899-908. doi:10.1097/AOG.0000000000003500 (PMC6819021)
- Palatin Technologies, Inc. Regulatory and development history of bremelanotide: discontinuation of the intranasal program following blood-pressure findings (2008) and reformulation to a subcutaneous product; corroborated by the U.S. FDA Multi-Discipline Review, NDA 210557 (2019). Palatin Technologies press releases / SEC filings and accessdata.fda.gov/drugsatfda_docs/nda/2019/210557Orig1s000MultidisciplineR.pdf
- U.S. FDA Multi-Discipline Review, NDA 210557 (bremelanotide), 2019; RECONNECT Phase 3 program (ClinicalTrials.gov NCT02333071, NCT02338960). accessdata.fda.gov/drugsatfda_docs/nda/2019/210557Orig1s000MultidisciplineR.pdf
- Bremelanotide (DB11653). DrugBank — mechanism of action and melanocortin receptor pharmacology.
- Kamermans A, Verhoeven T, van het Hof B, Koning JJ, Borghuis L, Witte M, van Horssen J, de Vries HE, Rijnsburger M. Setmelanotide, a Novel, Selective Melanocortin Receptor-4 Agonist Exerts Anti-inflammatory Actions in Astrocytes and Promotes an Anti-inflammatory Macrophage Phenotype. Frontiers in Immunology. 2019;10:2312. doi:10.3389/fimmu.2019.02312
- Spana C, Jordan R, Fischkoff S. Effect of bremelanotide on body weight of obese women: Data from two phase 1 randomized controlled trials. Diabetes, Obesity and Metabolism. 2022;24(6):1084-1093.
- Polymorphism of Melanocortin Receptor Genes — Association with Inflammatory Traits and Diseases. Diseases (MDPI). 2025;13(9):305. (PMC12468675)
- Vyleesi (bremelanotide) Side Effects and Safety. Drugs.com professional monograph and FDA label adverse-reaction data.
- Bremelanotide. LiverTox: Clinical and Research Information on Drug-Induced Liver Injury. National Institute of Diabetes and Digestive and Kidney Diseases; NCBI Bookshelf NBK573221.
- DosagePeptide.com. PT-141 (10 mg Vial) Dosage Protocol — reconstitution reference (bacteriostatic water, ~3.33 mg/mL, U-100 syringe conversion).
Educational and research-only disclaimer: This article is provided solely for educational and scientific-reference purposes. It is not medical advice and must not be used to diagnose, treat, cure, or prevent any disease. Bremelanotide (PT-141) is approved only as Vyleesi for acquired, generalized hypoactive sexual desire disorder in premenopausal women; all other uses, including any autoimmune, anti-inflammatory, or immune-modulating application, are unapproved and investigational, with little or no supporting human evidence. Nothing here endorses or provides instructions for human use of any research compound. “Research use only” materials are not intended for human or veterinary use. Always consult a qualified, licensed healthcare professional regarding any medical condition and rely on approved, evidence-based therapies.