The title of this article poses a question, and it is worth being clear from the outset that it remains an open question rather than a settled claim. Melanotan II (MT-II) is a synthetic melanocortin peptide that is frequently discussed in the same breath as sexual function because a closely related molecule, bremelanotide, became the first melanocortin drug approved for a female sexual disorder. That association has led some readers to assume MT-II itself “treats” hypoactive sexual desire disorder (HSDD). It does not. Melanotan II is not approved by the U.S. Food and Drug Administration (FDA) or any comparable regulator for any indication, and it has never completed a controlled clinical trial for HSDD.1
What the scientific record does contain is a plausible pharmacological rationale, a handful of small early-phase human studies focused mainly on male erectile response, extensive preclinical work in animal models, and a distinct, regulator-reviewed body of evidence for its chemical relative bremelanotide (marketed as Vyleesi) in premenopausal women.2,5 The honest framing, therefore, is not “Melanotan II treats HSDD” but rather “the melanocortin system that Melanotan II activates is implicated in sexual desire, and one specific, purpose-built melanocortin agonist has shown a modest, measurable effect in a defined female population.” Whether MT-II itself could ever occupy a similar role is unresolved and, given its safety profile, unlikely to be pursued as a therapeutic in its current form.
This article surveys the origin and chemistry of Melanotan II, the receptor biology that connects melanocortins to sexual behavior, the actual level of evidence, how MT-II compares to the approved bremelanotide, the research models used to study these questions, the documented safety concerns, and the regulatory landscape. It is written for an educational and research-literacy audience. Nothing here is medical advice, a protocol recommendation, or an endorsement of human use. Melanotan II is best understood as a research chemical with a serious risk profile, not as a candidate you should treat as a therapy.
What Melanotan II Is and Where It Came From
Melanotan II is a cyclic, seven-residue synthetic analogue of alpha-melanocyte-stimulating hormone (alpha-MSH), a naturally occurring member of the melanocortin peptide family derived from the precursor protein pro-opiomelanocortin (POMC). Its full peptide notation is Ac-Nle4-Asp5-His6-D-Phe7-Arg8-Trp9-Lys10-NH2, a structure built around the “message sequence” (His-Phe-Arg-Trp) that melanocortins use to engage their receptors.3 The molecule was designed in the 1980s by a research group at the University of Arizona led by Mac E. Hadley and Victor J. Hruby. The original goal had nothing to do with sexual function: the team was trying to create a stable, potent alpha-MSH analogue that could stimulate melanogenesis (the production of the skin pigment melanin) as a possible photoprotective strategy against ultraviolet-induced skin damage.4
To make alpha-MSH more drug-like, the chemists introduced three key modifications. A norleucine substitution at position 4 improved metabolic stability; a D-phenylalanine substitution at position 7 increased receptor potency and resistance to enzymatic breakdown; and a lactam bridge cyclized the molecule between residues 5 and 10, locking it into a conformation that binds melanocortin receptors with high affinity.3,4 The result was described in the literature as a “superpotent” cyclic melanotropic peptide with far greater activity and a longer duration of action than native alpha-MSH.3 This is the same design philosophy that produced its cousin Melanotan I (afamelanotide), a linear analogue that is far more selective for the pigmentation receptor and which later gained regulatory approval in Europe and the United States for the rare photosensitivity condition erythropoietic protoporphyria.
The pivotal and largely accidental observation came during an early human pharmacology study. In a pilot phase-I investigation of Melanotan II conducted at the University of Arizona, several male participants reported spontaneous penile erections and, in some cases, sexual arousal and yawning, effects that were not the point of the study and that the investigators had not set out to produce.3 That unexpected finding is the entire origin of the “Melanotan II and sex” narrative. It redirected an important thread of melanocortin research away from tanning and toward sexual medicine, and it is the direct ancestor of the bremelanotide program: bremelanotide is essentially a metabolite-inspired, purpose-optimized melanocortin agonist developed to keep the sexual and central nervous system effects while shedding the pigmentation-driving activity.4
It is important to separate the legitimate, peer-reviewed scientific history from how Melanotan II is used today. In the research and consumer-gray-market world, MT-II circulates almost entirely as an unregulated, non-pharmaceutical-grade lyophilized powder marketed for tanning and, informally, for libido. It is not manufactured to pharmaceutical standards, it is not quality-controlled by any regulator, and the material sold under the name may vary in purity and content. For readers who want to understand how MT-II is characterized in an educational dosing context, DosagePeptide maintains a reference page on the Melanotan II 10 mg vial protocol, but that material is explicitly research-oriented and does not establish that MT-II is safe or appropriate for human use.
The Molecular Mechanism: Melanocortins and Sexual Function
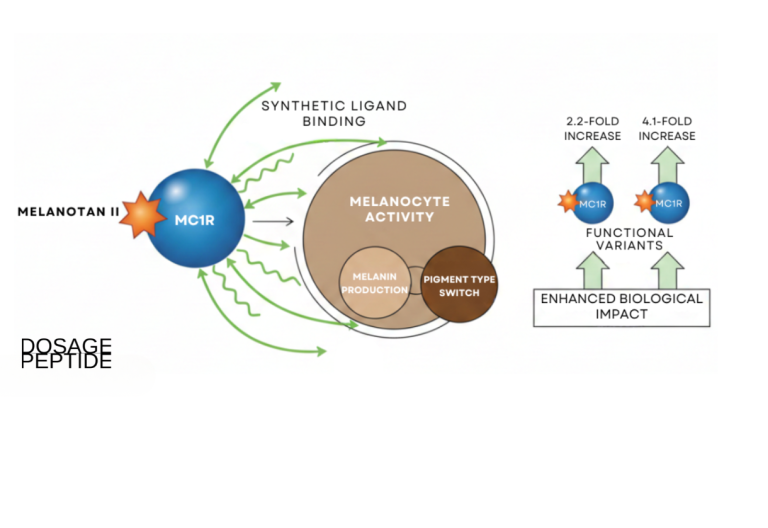
To understand why anyone connects Melanotan II to sexual desire, you have to look at the melanocortin receptor system. There are five known melanocortin receptors (MC1R through MC5R), all G-protein-coupled receptors that signal primarily by raising intracellular cyclic AMP. Each has a distinct tissue distribution and physiological role: MC1R governs skin and hair pigmentation; MC2R responds to adrenocorticotropic hormone in the adrenal cortex; MC3R and MC4R are concentrated in the central nervous system and regulate energy balance, appetite, and, relevant here, sexual behavior; and MC5R is involved in exocrine gland function.6
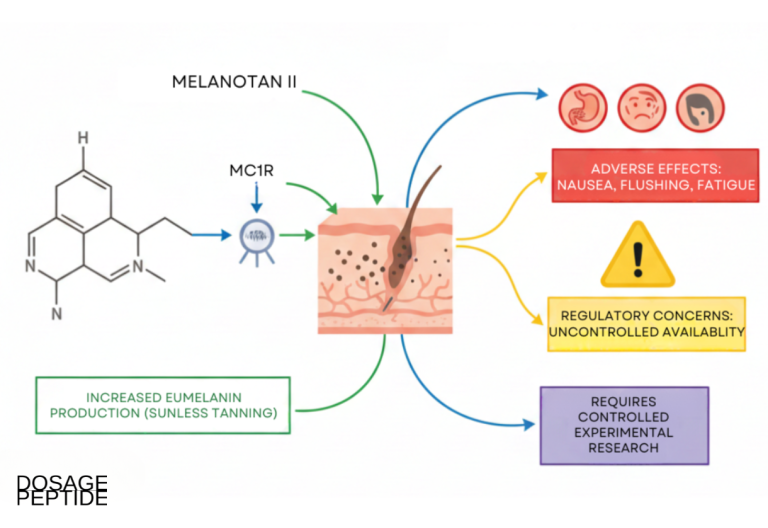
Melanotan II is a non-selective agonist. Unlike a targeted drug, it activates MC1R, MC3R, MC4R, and MC5R with meaningful potency, which is precisely why it produces such a broad spread of effects, from tanning (MC1R) to nausea, flushing, and appetite suppression, to the sexual effects that are the subject of this article.3,4 The receptor most strongly implicated in sexual behavior is MC4R, which is densely expressed in hypothalamic nuclei and in the spinal cord regions that coordinate the erectile and arousal reflexes. Activation of central MC4R is thought to act on pro-sexual neural circuits upstream of the peripheral vascular events that produce erection, meaning melanocortins are believed to work more on the “central” drive and arousal side than on the purely mechanical, blood-flow side that PDE5 inhibitors such as sildenafil target.2,7
The experimental basis for the MC4R hypothesis is reasonably well developed in animals. Reviews of the melanocortinergic control of penile erection describe how centrally administered melanocortin agonists induce erections in rodents, how this can be blocked by melanocortin receptor antagonists, and how genetically or pharmacologically manipulating MC4R shifts sexual behavior.7 In female animal models, a melanocortin receptor agonist has been shown to selectively facilitate sexual solicitation behavior in female rats, supporting the idea that the pathway is relevant to desire and not only to male erectile mechanics.18 That said, the female preclinical picture is not uniformly positive: a more recent conditioned-place-preference study in female Syrian hamsters found that bremelanotide did not enhance sexual reward and had no effect on melanocortin-receptor expression, a null result that tempers any strong claim that melanocortin agonism reliably augments female sexual motivation.8 This is the mechanistic thread that makes HSDD, a disorder defined by persistently absent or reduced sexual desire and associated distress, a theoretically coherent target for a melanocortin agonist.
There is an important caveat that regulators themselves have stated plainly. Even for the approved melanocortin drug bremelanotide, the FDA-reviewed labeling states that the precise mechanism by which it improves HSDD in women is unknown.9 In other words, we have a plausible receptor story and supportive animal data, but we do not have a validated, step-by-step account of how melanocortin activation translates into a clinically meaningful change in human sexual desire. For Melanotan II specifically, the situation is weaker still: its non-selectivity means that any hypothetical desire-related benefit from MC4R activation would arrive bundled with MC1R-driven pigmentation and the cardiovascular and gastrointestinal effects of broad melanocortin stimulation. A drug developer’s entire reason for creating a more selective successor was to escape exactly that bundling.
Readers who want the receptor-by-receptor vocabulary in plain language can consult the DosagePeptide peptide reference material, but the key mechanistic takeaway is this: Melanotan II hits the right receptor (MC4R) for a sexual effect, but it also hits several wrong ones, and even the “right” pathway’s link to clinical desire remains incompletely understood.
What the Evidence Actually Shows
Here it is essential to be precise about evidence levels, because this is where marketing most often outruns the science. The direct human evidence for Melanotan II and sexual function is small, old, and centered on male erectile response, not on female HSDD or on “desire” as a standalone outcome.
The single most-cited human study is a 1998 double-blind, placebo-controlled crossover trial by Wessells and colleagues in which ten men with psychogenic (non-organic) erectile dysfunction received Melanotan II or placebo, with erections monitored objectively using RigiScan penile tumescence recording. Clinically apparent erections developed in 8 of 10 men after MT-II, and the mean duration of tip rigidity greater than 80% was 38.0 minutes with MT-II versus 3.0 minutes with placebo.1 A follow-up study by the same group extended the observation to men with organic erectile dysfunction and additionally noted increases in self-reported sexual desire alongside the erectile effect, which is the closest the MT-II literature gets to a “desire” endpoint.10 These were genuinely important proof-of-concept findings, but the sample sizes are in the single or low double digits, the populations were men with erectile dysfunction rather than people with HSDD, and the trials were not designed or powered to evaluate a desire disorder as a treatment indication.
| Evidence source | Population | Design | Primary observation | Relevance to HSDD |
|---|---|---|---|---|
| Wessells 19981 | 10 men, psychogenic ED | Double-blind, placebo-controlled crossover, RigiScan | Erection in 8/10; tip rigidity 38.0 vs 3.0 min | Indirect (male erection, not desire) |
| Wessells 200010 | Men, organic ED | Placebo-controlled | Increased erection and self-reported desire | Indirect (desire noted, small male sample) |
| Dorr 1996 phase I3 | Healthy men | Pilot phase-I safety/pharmacology | Incidental erections; tolerability signals | Hypothesis-generating only |
| Bremelanotide RECONNECT5 | 1,247 premenopausal women, HSDD | Two randomized phase-3 RCTs | Small significant gains in FSFI-D and distress | Direct, but for bremelanotide, not MT-II |
Beyond those studies there is a large volume of preclinical and mechanistic work, plus the incidental phase-I observations that started the field.3,7 What is conspicuously absent is any randomized controlled trial of Melanotan II for HSDD in any population. There is no phase-2 or phase-3 program for MT-II in sexual desire, no regulatory submission, and no peer-reviewed efficacy dataset in women. The entire clinically robust HSDD evidence base belongs to the successor molecule, bremelanotide, and even there the effect size is modest, a point developed in the next section.
It is also worth naming the study-design weaknesses that constrain how much even the positive MT-II findings can support. The Wessells crossover trials were small enough that a single outlier could move the mean, they enrolled men rather than the female population in which HSDD is most defined, and they used objective erectile monitoring as the primary readout, a physiological signal that is meaningfully different from the subjective, distress-linked desire that HSDD requires.1,10 Crossover designs are efficient but vulnerable to carryover and to unblinding when a drug produces obvious sensations such as flushing or nausea, which melanocortin agonists reliably do, and no MT-II study was ever scaled to the hundreds or thousands of participants needed to characterize efficacy and rarer harms. None of this makes the early findings worthless; they were a legitimate signal that launched an entire drug class. It simply means they sit near the bottom of the evidence hierarchy for a treatment claim, at the level of hypothesis-generating pilot data rather than confirmatory efficacy.
So the honest summary of evidence level is: for Melanotan II specifically, the human data are limited to small early studies of male erectile response with incidental desire observations, supported by animal and receptor pharmacology. This qualifies as an interesting research signal and a legitimate open question, but it falls far short of the standard required to call MT-II a treatment for HSDD or anything else. Anyone claiming otherwise is either conflating MT-II with bremelanotide or overstating what a handful of ten-person crossover studies can establish. For a broader library of how individual compounds are characterized at the evidence level, DosagePeptide’s dosage protocol index is a useful orientation, but it is educational reference material, not clinical proof.
Melanotan II vs. Bremelanotide and Other Comparators
The most important comparison for this topic is between Melanotan II and bremelanotide, because the two are constantly conflated and because the difference explains why one is an unapproved research chemical and the other is an FDA-approved medicine. Bremelanotide (developmental name PT-141) was deliberately engineered from the melanocortin lineage that MT-II established. Chemically it is a metabolite-inspired analogue optimized to preserve the central, pro-sexual melanocortin activity while minimizing the pigmentation-driving MC1R engagement and improving the pharmacological profile for on-demand use.4 In receptor terms, bremelanotide is a non-selective melanocortin agonist as well, but its clinical development was targeted, controlled, and ultimately successful in a defined indication, whereas MT-II was never advanced as a sexual-medicine drug at all.
Bremelanotide’s pivotal evidence comes from the two RECONNECT phase-3 trials, a pair of identical randomized, double-blind, placebo-controlled studies in premenopausal women with acquired, generalized HSDD, led by Kingsberg and colleagues and published in 2019.5 Roughly 1,200 women received subcutaneous bremelanotide 1.75 mg on an as-needed basis or placebo. On the co-primary endpoints, the change in the Female Sexual Function Index desire domain (FSFI-D) and a validated distress measure, bremelanotide produced statistically significant improvements over placebo. Crucially, the magnitude was small: the integrated between-group difference in mean FSFI-D change was on the order of 0.35 points, and in FDA’s own review the responder benefit over placebo was modest (for example, improvements in desire scores reported in roughly 25% of bremelanotide users versus 17% on placebo).5,9 This is a real, regulator-validated effect, but it is a nudge, not a transformation, and it comes with meaningful side effects.
| Attribute | Melanotan II (MT-II) | Bremelanotide (Vyleesi) |
|---|---|---|
| Regulatory status | Not approved anywhere; research chemical | FDA-approved (2019) for premenopausal HSDD11 |
| Receptor selectivity | Broad MC1R/MC3R/MC4R/MC5R agonist | Non-selective, but optimized to reduce pigmentation liability |
| HSDD clinical trials | None | Two phase-3 RCTs (RECONNECT), ~1,200 women5 |
| Human sexual data | Small male erectile studies, incidental desire1,10 | Powered efficacy and safety data in HSDD5 |
| Pigmentation effect | Marked (a primary reason it is used off-label) | Minimized by design |
| Quality control | None; gray-market variability | Pharmaceutical manufacturing and labeling |
The comparison is not merely academic. It shows that the “melanocortin approach to HSDD” that succeeded was a purpose-built, quality-controlled, regulator-reviewed drug used at a defined dose and studied in the exact target population. Melanotan II shares the mechanistic family tree but almost none of the development rigor. Using MT-II as if it were a stand-in for bremelanotide ignores the deliberate engineering (reduced pigmentation liability, defined dosing, controlled purity) that made the approved drug acceptable for human use in the first place. Early combination studies also explored intranasal PT-141 with sildenafil in men with erectile dysfunction, illustrating that the sexual-medicine value of this chemical class was pursued through the optimized analogue, not through MT-II.2
Other comparators for HSDD sit outside the melanocortin class entirely. The only other FDA-approved HSDD drug, flibanserin, is a daily oral serotonergic agent with a completely different mechanism and its own tolerability and interaction constraints. Off-label transdermal testosterone is used in some postmenopausal contexts under specialist guidance. Neither is pharmacologically comparable to MT-II, and mentioning them only underscores that HSDD management is an evolving, specialist area in which an unregulated tanning peptide has no established place. Readers comparing how the melanocortin agonists relate to one another can review DosagePeptide’s PT-141 reference page alongside the MT-II material for an educational contrast.
Research Models and Methodology
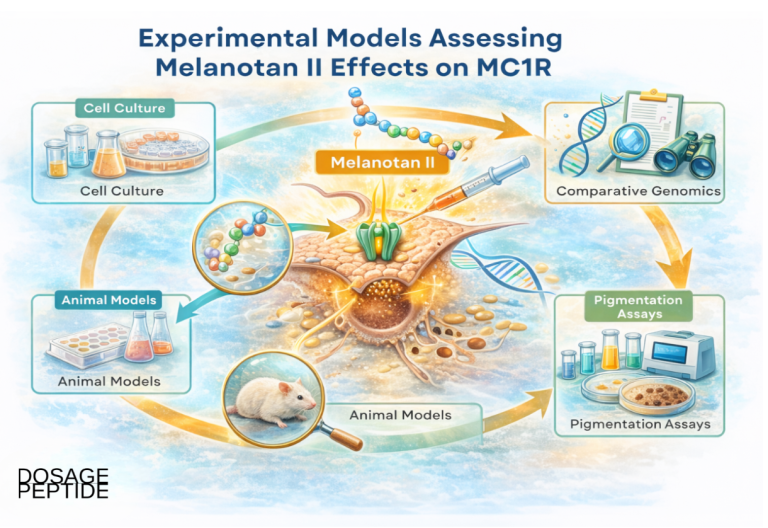
Because the human data on melanocortins and sexual desire are thin, the field leans heavily on preclinical and pharmacological models, and understanding those models is essential to reading the evidence critically. The methodological toolkit spans several levels of biological organization, each answering a different question and carrying different limitations.
At the most reductionist level are in vitro receptor-binding and functional assays. Cell lines expressing individual human melanocortin receptors are used to measure how tightly a compound binds and how strongly it triggers downstream signaling (typically cyclic AMP accumulation). These assays are how researchers established that MT-II is a broad-spectrum agonist and that bremelanotide’s activity profile differs, and they are how selectivity is quantified.4,9 Their limitation is obvious: a receptor in a dish tells you nothing about behavior, distress, or clinical benefit.
The next level is animal behavioral pharmacology. Rodent models dominate: centrally or peripherally administered melanocortin agonists are studied for their effects on penile erection reflexes in male rats and on measures of sexual motivation in females, such as solicitational behaviors and paced-mating paradigms, with antagonist co-administration used to confirm that effects are melanocortin-receptor mediated.7,18 More recently, non-rodent models have been used to probe the approved drug: a female Syrian hamster study of bremelanotide, for example, was published to test its behavioral pharmacology in a species with well-defined sexual behaviors and reported a null result, finding no enhancement of sexual reward in a conditioned-place-preference paradigm and no change in melanocortin-receptor expression.8 These models are valuable for mechanism, but translating a rat’s solicitational behavior or a hamster’s lordosis into a human’s subjective experience of “desire” and “distress” is a large and uncertain inferential leap. Sexual desire in humans is defined partly by cognition, relationship context, and self-reported distress, dimensions no animal captures.
The third level is human clinical trial methodology, which is where HSDD research becomes genuinely rigorous, and where MT-II is essentially absent. Modern HSDD trials such as RECONNECT use validated, patient-reported outcome instruments as endpoints: the Female Sexual Function Index desire domain (FSFI-D) quantifies desire, and the Female Sexual Distress Scale captures the associated distress that is a diagnostic requirement for HSDD.5 They enroll rigorously diagnosed patients, randomize against placebo, blind both participants and investigators, and pre-specify statistical analyses, precisely because sexual-desire outcomes are highly susceptible to placebo response and expectation effects. The large placebo response seen in these trials is itself a methodological lesson: in the bremelanotide studies a substantial fraction of placebo recipients reported improvement, which is exactly why uncontrolled anecdotes about MT-II “working” carry so little evidential weight.5
There is also active academic interest in the underlying receptor’s role, exemplified by investigator-initiated work registered on public trial registries examining the function of the melanocortin-4 receptor in HSDD.12 That kind of study is designed to probe mechanism in humans rather than to license a product, and it reflects the reality that even for the approved pathway, the science is still maturing. The overarching methodological point for readers is that the strength of a claim tracks the model that produced it: a receptor assay or a rodent study can justify a hypothesis, but only an adequately powered, blinded, placebo-controlled human trial can justify calling something a treatment, and no such trial exists for Melanotan II in HSDD.
Safety and Tolerability: The Central Concern
If the efficacy story for Melanotan II in HSDD is “unproven,” the safety story is “actively concerning,” and this is the part of the discussion that most decisively separates MT-II from an approved medicine. Because MT-II is a non-selective melanocortin agonist delivered without pharmaceutical quality control, its adverse effects arise both from its broad on-target pharmacology and from the unregulated nature of the products sold.
The most commonly reported acute effects, seen even in the controlled early studies and consistent with melanocortin activation, include nausea (often significant and dose-related), facial flushing, spontaneous and sometimes unwanted erections, yawning, appetite suppression, and darkening of the skin and existing moles.3,13 Transient increases in blood pressure and changes in heart rate are also characteristic of melanocortin agonism; notably, even the approved bremelanotide carries a labeled transient rise in blood pressure and a corresponding caution in people with cardiovascular risk, which underscores that this is a class effect and not merely a contaminant issue.9
More serious harms are documented in the case-report literature specific to Melanotan II. Priapism, a prolonged and painful erection that is a urological emergency capable of causing permanent tissue damage, has been reported following melanotan injection.14 A published case describes systemic toxicity with rhabdomyolysis (severe muscle breakdown) following MT-II use, a life-threatening presentation that can precipitate acute kidney injury.15 These are not theoretical risks; they are real events that reached clinical attention.
| Category | Reported effects | Nature of concern |
|---|---|---|
| Common / acute | Nausea, flushing, yawning, appetite loss, spontaneous erection | On-target melanocortin effects; often dose-related3 |
| Cardiovascular | Transient blood pressure elevation, heart-rate changes | Class effect; labeled even for approved bremelanotide9 |
| Dermatologic | Generalized skin darkening, new or changing moles | MC1R stimulation; melanoma reports raise oncologic concern13,16 |
| Serious / rare | Priapism, rhabdomyolysis, systemic toxicity | Medical emergencies documented in case reports14,15 |
| Product-related | Unknown purity, contamination, mislabeling | No quality control in gray-market supply13 |
A further layer of concern is that MT-II’s acute effects can compound one another in ways that are hard to anticipate at the individual level. Nausea and flushing may seem merely unpleasant, but combined with a transient rise in blood pressure they place additional strain on the cardiovascular system, and the same central pathway that drives arousal can drive priapism, which is not a benign side effect but an emergency requiring urgent intervention to prevent permanent damage.9,14 Because no reliable human dose-response or long-term safety dataset exists for MT-II in a libido context, there is no established margin between a dose that produces an effect and a dose that produces harm, and the unregulated supply means the actual quantity delivered by a given injection is itself uncertain. That combination, a real pharmacological potency, a narrow and undefined safety margin, and an unverified product, is exactly the scenario that regulators cite when they warn the public away from melanotan.13
The dermatologic dimension deserves particular emphasis because it connects directly to MT-II’s non-selectivity. By stimulating MC1R, MT-II drives melanin production, which is the whole reason it is used for tanning, but this also changes the appearance and behavior of pigmented lesions. Dermatology reviews of unregulated alpha-MSH analogue use have flagged darkening and proliferation of moles as a real clinical problem, and there are published reports of melanoma occurring in individuals who used melanotan, raising a biologically plausible, though not definitively causal, oncologic concern.13,16 A change in moles is precisely the kind of warning sign clinicians are trained to take seriously, and a drug that deliberately alters pigmentation complicates that surveillance.
Layered on top of the pharmacology is the supply problem. Because Melanotan II is not manufactured or tested to pharmaceutical standards, products vary in purity, actual peptide content, and potential contamination, and injecting a non-sterile or mislabeled preparation adds infection and dosing-error risks that have nothing to do with the peptide itself.13 National regulators, including the U.S. FDA and medicines agencies in the United Kingdom, Australia, and elsewhere, have issued warnings against melanotan products precisely because of this combination of pharmacological hazard and unregulated supply. The bottom line is that even if MT-II had a proven desire benefit, which it does not, its safety profile would present a serious obstacle to human use, and it is exactly this profile that a purpose-built successor was designed to improve upon.
Handling and Reconstitution in a Research Context
This section is included because Melanotan II is distributed as a lyophilized (freeze-dried) powder that must be reconstituted before it can be handled in any laboratory or research setting, and understanding that process is part of research literacy. It is presented strictly as educational and laboratory-handling information, not as an endorsement or instruction for human administration. Nothing in this section should be read as suggesting MT-II is safe to inject.
In a research context, lyophilized peptides are reconstituted by adding a sterile diluent, most commonly bacteriostatic water, to the powder to create a solution of known concentration. The diluent is added slowly down the inside wall of the vial rather than sprayed directly onto the powder, because peptides are physically delicate and vigorous agitation can shear and denature them; the vial is then gently swirled, not shaken, until the powder fully dissolves.17 The core arithmetic is straightforward: concentration equals the mass of peptide divided by the volume of diluent. For a nominal 10 mg vial, adding 3.0 mL of diluent yields a solution of approximately 3.33 mg/mL, and on a standard U-100 insulin syringe that corresponds to roughly 33.3 micrograms per “unit” marking, the kind of unit-to-microgram conversion that is central to any dosing calculation.17
| Parameter | Typical research-context value | Note |
|---|---|---|
| Vial content (nominal) | 10 mg lyophilized | Actual content varies in unregulated product |
| Diluent | Bacteriostatic water | Added slowly down vial wall |
| Example volume | 3.0 mL | Yields ~3.33 mg/mL |
| Concentration | ~3.33 mg/mL | Concentration = mass / volume |
| Unit conversion | ~33.3 mcg per U-100 unit | Depends on chosen concentration |
| Storage (powder) | Frozen, roughly -20 °C | Protect from light and moisture |
| Storage (reconstituted) | Refrigerated, 2 to 8 °C | Peptides in solution are less stable |
Stability and storage matter because peptides degrade. Lyophilized MT-II is generally stored frozen and protected from light and humidity, while a reconstituted solution is refrigerated and has a much shorter usable life, since peptides in aqueous solution are more prone to hydrolysis and aggregation over time.17 Repeated freeze-thaw cycles of a solution are avoided for the same reason. These handling principles are generic to research peptides and are covered in general terms in DosagePeptide’s peptide reconstitution guide, which walks through concentration math, syringe unit conversions, and storage considerations at an educational level.
The reason a legitimate article includes this at all is transparency: readers encounter reconstitution instructions everywhere MT-II is sold, often stripped of any safety framing, and it is better to present the arithmetic honestly while making the essential point explicit. Knowing how to calculate a concentration does not make a compound safe or approved, and none of the numbers above should be interpreted as a recommendation to administer Melanotan II to a human being. In the specific case of MT-II, the same non-selectivity and safety concerns discussed earlier apply regardless of how carefully a solution is prepared. The chemistry of reconstitution is neutral; the pharmacology and legal status are not.
Limitations and the Human-Evidence Gap
Stepping back, it is worth cataloguing explicitly what we do not know, because the gaps are large and they are the real answer to the article’s title question. The central limitation is the complete absence of controlled human trials of Melanotan II for hypoactive sexual desire disorder. There is no randomized, placebo-controlled study of MT-II in people with HSDD, in either sex, at any dose. Every confident claim that MT-II “treats HSDD” is therefore an extrapolation, and usually a conflation with the separate, approved drug bremelanotide.
The human data that do exist for MT-II are limited in population, size, and endpoint. They come from small studies of men with erectile dysfunction, with the largest and best-known enrolling only ten participants, and they measured erectile physiology rather than the desire-plus-distress construct that defines HSDD.1,10 HSDD is not erectile dysfunction; it is a disorder of desire and associated distress, most often studied and treated in premenopausal women, and inferring a desire-disorder benefit from a handful of male erection studies is not scientifically defensible. Even the incidental “increased desire” observation in the organic-ED follow-up was a secondary, self-reported note in a small trial, not a validated efficacy endpoint.10
A second limitation is placebo response and expectation. Sexual-desire outcomes are among the most placebo-sensitive endpoints in medicine, as the bremelanotide trials themselves demonstrated with substantial placebo-arm improvement.5 This means anecdotal reports of MT-II improving libido, which circulate widely, cannot distinguish a genuine pharmacological effect from expectation, context, and the well-documented tendency of desire measures to improve simply from being studied. Uncontrolled testimonials are essentially uninterpretable for a question like this.
A third limitation is the confounding of any hypothetical benefit with harm. Because MT-II is non-selective, even if MC4R activation contributed to desire, that effect would arrive inseparable from nausea, flushing, blood-pressure changes, pigmentation, and the more serious risks documented in case reports.13,14,15,16 A therapeutic candidate has to demonstrate a favorable balance of benefit and risk in the intended population; MT-II has demonstrated neither a benefit for HSDD nor an acceptable risk profile, which is why drug development moved to a more selective, better-characterized successor. There is also no reliable human pharmacokinetic, dosing, or long-term safety dataset for MT-II in a sexual-medicine context, so even the basic parameters a trial would need are not established.
Finally, there is the quality-and-identity gap: because gray-market MT-II is not standardized, even the material people study or use is of uncertain content, so results are hard to reproduce and impossible to generalize.13 Taken together, these limitations mean the appropriate scientific verdict is not “promising treatment awaiting confirmation” but “mechanistically plausible hypothesis with no controlled human efficacy evidence and significant safety liabilities.” The honest answer to whether MT-II could play a role in treating HSDD is that, on current evidence, it is an open research question that the field has largely chosen to pursue through a different, purpose-built molecule rather than through MT-II itself. For readers building general context on how compounds are grouped and stacked in educational discussions, DosagePeptide’s peptide combinations reference illustrates how melanocortin agonists are catalogued, again as education rather than endorsement.
Regulatory Status
The regulatory picture is unambiguous and is arguably the single most important fact for a reader to retain. Melanotan II is not approved as a drug by the FDA, the European Medicines Agency, or any comparable national regulator, for HSDD or for any other indication. It has no marketing authorization, no approved labeling, and no legally recognized therapeutic use. In practical terms it is sold and handled as a research chemical, and where it is marketed to consumers for tanning or libido it is doing so outside any regulatory approval.13
Multiple regulators have gone further than simply not approving it; they have actively warned against it. The FDA has cautioned that products containing melanotan peptides are unapproved and potentially unsafe, and medicines and safety agencies in the United Kingdom, Australia, Ireland, and other jurisdictions have issued public warnings about melanotan injections, citing the unregulated supply, unknown purity, and documented adverse events.13 The recurring regulatory theme is not merely bureaucratic: it reflects the case-report record of serious harms and the impossibility of assuring quality in a product that no authority oversees.
By deliberate contrast, the melanocortin approach that did clear regulatory review is bremelanotide. The FDA approved bremelanotide, under the brand name Vyleesi, on June 21, 2019, for the treatment of acquired, generalized HSDD in premenopausal women, administered as an as-needed 1.75 mg subcutaneous injection.9,11 That approval rested on the two RECONNECT phase-3 trials, a full safety database, and manufacturing to pharmaceutical standards, and even so the label reflects a modest efficacy effect and specific safety cautions, including the transient blood-pressure elevation and restrictions on use in people with uncontrolled hypertension or known cardiovascular disease.9 The existence of an approved melanocortin drug for HSDD is exactly why the topic is worth discussing seriously, and exactly why it would be misleading to let that approval rub off onto the unapproved MT-II. Approval attaches to a specific molecule, at a specific dose, for a specific population, backed by specific evidence; none of that transfers to Melanotan II.
The gap between the two molecules also illustrates a broader lesson about how melanocortin science reached the clinic. The therapeutic value of the pathway was recognized precisely because Melanotan II produced an unexpected, unmistakable signal in early human pharmacology, but recognizing a signal and delivering a usable medicine are separated by years of medicinal chemistry, dose-finding, and controlled trials. Bremelanotide represents the product of that process: a molecule reworked to shift its route, duration, and receptor emphasis, then subjected to the RECONNECT program and a full safety review before any patient could receive it as an approved product.4,5,9 Melanotan II never entered that pipeline for sexual medicine and, given its pigmentation activity and documented harms, is not a realistic candidate to do so in its current form. The regulatory distinction between them is therefore not a technicality but a faithful summary of two very different levels of evidence and oversight.
It is also worth distinguishing the two “melanotans” for regulatory clarity. Melanotan I (afamelanotide), the more MC1R-selective cousin, has been approved in the European Union and the United States for the narrow, non-sexual indication of preventing phototoxicity in erythropoietic protoporphyria, a rare inherited condition. That approval is sometimes cited to imply legitimacy for “melanotan” generally, but it applies to a different molecule for a different, dermatologic purpose and says nothing about MT-II or about sexual desire. In sum, the regulatory status of Melanotan II for HSDD is straightforward: unapproved, unregulated, warned against, and not a therapy. The approved melanocortin option for HSDD is a separate drug, and the appropriate route for anyone concerned about sexual desire is evaluation by a qualified clinician, not a research chemical.
Frequently Asked Questions
Is Melanotan II approved to treat hypoactive sexual desire disorder?
No. Melanotan II is not approved by the FDA or any comparable regulator for HSDD or for any other medical use. It has never completed a controlled clinical trial for HSDD, and there is no approved labeling, dose, or indication for it.13 The confusion usually arises because a related melanocortin drug, bremelanotide (Vyleesi), is approved for HSDD in premenopausal women, but that is a different, purpose-built molecule.9,11
What is the difference between Melanotan II and bremelanotide (PT-141)?
Both are melanocortin receptor agonists from the same research lineage, but they are distinct molecules with very different status. Bremelanotide was deliberately engineered to preserve central, pro-sexual activity while reducing pigmentation effects, and it was developed through formal clinical trials to FDA approval.4,5 Melanotan II is a broad, non-selective agonist that strongly drives tanning, was never developed as a sexual-medicine drug, and remains an unapproved research chemical.3,13
Does the research show Melanotan II increases sexual desire?
The direct human evidence is limited to small studies in men with erectile dysfunction, the largest enrolling ten participants, which primarily measured erection and only incidentally noted self-reported desire.1,10 There is no controlled trial of MT-II for desire in people with HSDD. Animal and receptor studies support a mechanistic link between melanocortins and sexual behavior, but that is a hypothesis, not proof of a desire benefit in humans, and some female-animal data are null.7,8,18
Why is Melanotan II considered unsafe?
Because it activates melanocortin receptors broadly and is sold without quality control. Documented effects include nausea, flushing, blood-pressure changes, spontaneous erections, and skin and mole darkening, while case reports describe serious events such as priapism and rhabdomyolysis, and reviews raise melanoma concerns tied to its pigmentation activity.13,14,15,16 Unregulated products also carry purity, contamination, and dosing-error risks. Regulators in several countries have issued warnings against melanotan.13
If bremelanotide is approved, why not just use Melanotan II instead?
Because approval attaches to a specific, tested molecule, not to a chemical family. Bremelanotide was studied at a defined dose in the target population with a full safety database, and it was engineered to minimize the pigmentation liability that MT-II prominently has.5,9 Substituting an unapproved, non-selective, unregulated peptide discards all of that rigor and reintroduces the exact risks the successor drug was designed to avoid.
Has Melanotan II been studied specifically in women with HSDD?
No. The MT-II human literature centers on men with erectile dysfunction, and there is no randomized or controlled study of MT-II in women with HSDD.1,10 HSDD is defined by low desire plus associated distress, most often studied in premenopausal women, and inferring a benefit for that condition from small male erectile studies is not scientifically valid.
What does “research chemical” mean for Melanotan II?
It means MT-II is distributed for laboratory and research handling rather than as an approved medicine, and it is not manufactured, tested, or labeled to pharmaceutical standards. Educational resources describe how such peptides are reconstituted and measured, but that arithmetic does not confer safety or legality.17 A research-chemical designation is not a green light for human use; it is a signal that no regulator has vouched for the product.
What is the appropriate step for someone concerned about low sexual desire?
Consult a qualified healthcare professional. Low desire can have many causes, including hormonal, psychological, relational, and medication-related factors, and diagnosis of HSDD requires that the low desire cause personal distress. Approved treatment options exist and should be evaluated by a clinician who can weigh benefits and risks, rather than self-experimenting with an unapproved peptide.9
References
- Wessells H, Fuciarelli K, Hansen J, et al. Synthetic melanotropic peptide initiates erections in men with psychogenic erectile dysfunction: double-blind, placebo controlled crossover study. Journal of Urology. 1998;160(2):389-393. https://www.auajournals.org/doi/abs/10.1016/S0022-5347(01)62903-3
- Diamond LE, Earle DC, Garcia WD, Spana C. Co-administration of low doses of intranasal PT-141, a melanocortin receptor agonist, and sildenafil to men with erectile dysfunction results in an enhanced erectile response. Urology. 2005;65(4):755-759. https://pubmed.ncbi.nlm.nih.gov/15833522/
- Dorr RT, Lines R, Levine N, et al. Evaluation of melanotan-II, a superpotent cyclic melanotropic peptide in a pilot phase-I clinical study. Life Sciences. 1996;58(20):1777-1784. https://pubmed.ncbi.nlm.nih.gov/8637402/
- Hadley ME, Dorr RT. Melanocortin peptide therapeutics: historical milestones, clinical studies and commercialization. Peptides. 2006. https://pubmed.ncbi.nlm.nih.gov/16412534/
- Kingsberg SA, Clayton AH, Portman D, et al. Bremelanotide for the Treatment of Hypoactive Sexual Desire Disorder: Two Randomized Phase 3 Trials (RECONNECT). Obstetrics & Gynecology. 2019;134(5):899-908. https://pmc.ncbi.nlm.nih.gov/articles/PMC6819021/
- Cone RD. Studies on the physiological functions of the melanocortin system. Endocrine Reviews. 2006;27(7):736-749. https://pubmed.ncbi.nlm.nih.gov/17077189/
- Molinoff PB, Shadiack AM, Earle D, et al. PT-141: a melanocortin agonist for the treatment of sexual dysfunction (review of melanocortin control of sexual behavior). Annals of the New York Academy of Sciences. 2003. https://pubmed.ncbi.nlm.nih.gov/12817821/
- Borland JM, Kohut-Jackson AL, Peyla AC, Hall MA, Mermelstein PG, Meisel RL. Female Syrian hamster analyses of bremelanotide, a US FDA approved drug for the treatment of female hypoactive sexual desire disorder (bremelanotide did not enhance sexual reward in a conditioned place-preference test and had no effect on melanocortin-receptor mRNA). Neuropharmacology. 2025;267:110307. https://pubmed.ncbi.nlm.nih.gov/39793696/
- VYLEESI (bremelanotide injection) Prescribing Information. U.S. Food and Drug Administration, 2019. https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/210557s000lbl.pdf
- Wessells H, Gralnek D, Dorr R, et al. Effect of an alpha-melanocyte stimulating hormone analog on penile erection and sexual desire in men with organic erectile dysfunction. Urology. 2000;56(4):641-646. https://www.goldjournal.net/article/S0090-4295(00)00680-4/abstract
- Vyleesi (bremelanotide) FDA Approval History. Drugs.com (FDA approval June 21, 2019). https://www.drugs.com/history/vyleesi.html
- Role of the Melanocortin-4 Receptor in Hypoactive Sexual Desire Disorder. ClinicalTrials.gov, NCT04179734. https://clinicaltrials.gov/study/NCT04179734
- Habbema L, Halk AB, Neumann M, Bergman W. Risks of unregulated use of alpha-melanocyte-stimulating hormone analogues: a review. International Journal of Dermatology. 2017;56(10):975-980. https://pubmed.ncbi.nlm.nih.gov/28266027/
- Mallory H, Lopategui D, Cordon B. Melanotan tanning injection: a rare cause of priapism. Sexual Medicine. 2021;9(1):100298. https://pubmed.ncbi.nlm.nih.gov/33460908/
- Nelson ME, Bryant SM, Aks SE. Melanotan II injection resulting in systemic toxicity and rhabdomyolysis. Clinical Toxicology (Phila). 2012;50(10):1169-1173. https://pubmed.ncbi.nlm.nih.gov/23121206/
- Hjuler KF, Lorentzen HF. Melanoma associated with the use of melanotan-II. Dermatology. 2014;228(1):34-36. https://pubmed.ncbi.nlm.nih.gov/24401718/
- Peptide Reconstitution Guide. DosagePeptide.com (educational reference). https://www.dosagepeptide.com/peptide-reconstitution-guide/
- Pfaus JG, Shadiack A, Van Soest T, Tse M, Molinoff P. Selective facilitation of sexual solicitation in the female rat by a melanocortin receptor agonist. Proceedings of the National Academy of Sciences USA. 2004;101(27):10201-10204. https://pubmed.ncbi.nlm.nih.gov/15226502/
Educational and research-use disclaimer: This article is provided solely for educational and scientific-literacy purposes. It is not medical advice, and it is not an endorsement, protocol, or recommendation to obtain, prepare, or administer Melanotan II or any other peptide. Melanotan II is not approved by the FDA or any comparable regulator for hypoactive sexual desire disorder or any other condition, and it carries documented safety risks. The related approved drug for HSDD, bremelanotide (Vyleesi), is a distinct molecule and its approval does not extend to Melanotan II. Anyone with concerns about sexual desire or sexual function should consult a qualified, licensed healthcare professional. References are provided so readers can consult primary sources directly.