The question in this article’s title deserves an honest answer before the first section even begins: there is no approved use of PT-141 (bremelanotide) for fatigue, and there is no rigorous human trial demonstrating that it corrects the fatigue or the libido changes that accompany chronic illnesses such as multiple sclerosis, lupus, chronic kidney disease, or myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS). Bremelanotide is FDA-approved for exactly one narrow indication, marketed as Vyleesi: the on-demand treatment of acquired, generalized hypoactive sexual desire disorder (HSDD) in premenopausal women.1 Everything else, including the premise that it might “improve fatigue and libido dysregulation in chronic illnesses,” is an open research question rather than an established fact.
That reframing matters because the melanocortin system PT-141 acts on is genuinely interesting to fatigue and sexual-function researchers. The melanocortin-4 receptor (MC4R) sits at the crossroads of energy balance, inflammation, and sexual motivation in the central nervous system, and that biological overlap is exactly what makes speculation about “fatigue plus libido” so tempting.78 But biological plausibility is not clinical evidence. A pathway being involved in fatigue does not mean a drug that touches that pathway treats fatigue, and the leap from receptor biology to a therapeutic claim is precisely where marketing and wishful thinking tend to outrun the data.
This article walks through what PT-141 actually is, how it works at the receptor level, what the human evidence does and does not support, why chronic-illness fatigue and libido are so entangled, how the compound compares to alternatives, how it is studied, its safety profile, handling considerations in a research setting, the limits of the evidence, and its regulatory status. The goal throughout is education, not endorsement. Nothing here is medical advice, and none of it should be read as encouragement to use an unapproved compound for an unapproved purpose.
What PT-141 (Bremelanotide) Is and Where It Came From
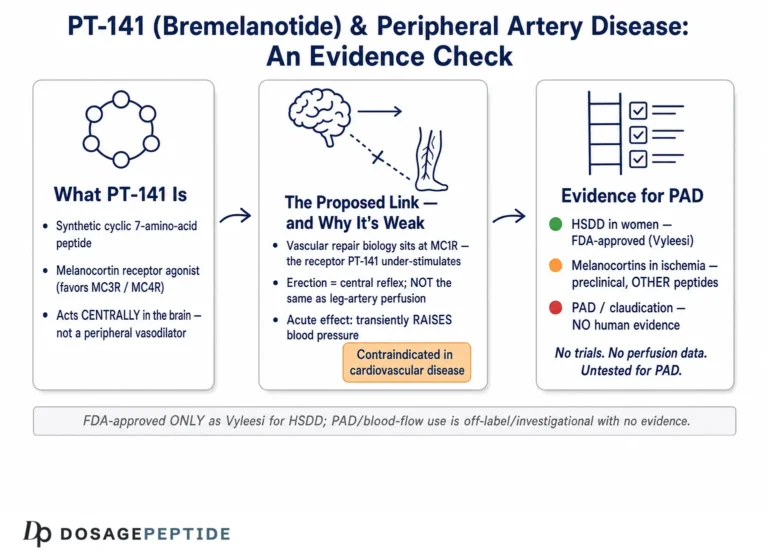
PT-141 is a research and development code name for bremelanotide, a synthetic cyclic heptapeptide that acts as an agonist at melanocortin receptors, with relative selectivity for the melanocortin-4 receptor (MC4R).110 Its full chemical description is a cyclic seven-amino-acid lactam analogue of the naturally occurring hormone alpha-melanocyte-stimulating hormone (alpha-MSH), with the sequence Ac-Nle-cyclo[Asp-His-D-Phe-Arg-Trp-Lys]-OH.10 The cyclization and the incorporation of a D-phenylalanine residue are not cosmetic; they make the peptide far more resistant to enzymatic breakdown than native alpha-MSH and shift its receptor-binding profile, which is why bremelanotide behaves differently from the endogenous hormone it is modeled on.
The molecule’s lineage is worth understanding because it explains both the enthusiasm and the caution around it. Bremelanotide descends from Melanotan II, a melanocortin agonist developed at the University of Arizona in the 1990s and originally studied as a synthetic tanning agent, since MC1R activation drives skin pigmentation.9 During early human work on Melanotan II, investigators noticed an unexpected effect: spontaneous erections and heightened sexual arousal in some male participants, an effect that appeared to be central rather than vascular. Palatin Technologies isolated and refined that arousal-related activity into a cleaner molecule with reduced MC1R affinity and greater MC4R engagement, and named it PT-141, later bremelanotide.9
The early clinical ambition was broad and, importantly, initially aimed at men. Bremelanotide was first developed as an intranasal spray for erectile dysfunction. That program ran into trouble: the nasal route produced higher and less predictable plasma concentrations, and with them dose-dependent increases in blood pressure. In 2007 the FDA placed a clinical hold on the intranasal erectile-dysfunction program over these cardiovascular signals.9 Palatin subsequently pivoted to a subcutaneous formulation and to a different indication entirely, HSDD in premenopausal women, a condition that had no approved pharmacotherapy at the time. That pivot, not the original male-ED vision, is what eventually reached approval in June 2019.5
This history is directly relevant to the fatigue-and-libido question. The compound was never developed for fatigue, never developed for chronic-illness populations, and its one successful indication is the product of a narrow, carefully bounded trial program in otherwise healthy premenopausal women. The origin story shows a molecule repeatedly reshaped by safety constraints and regulatory feedback, and it explains why claims that stray far from the approved use rest on very thin ground. Readers who want the practical framing of how the compound is handled can review the site’s PT-141 (10 mg vial) dosage protocol, which is written for a research-education context rather than as clinical direction.
A final point about naming: “PT-141” and “bremelanotide” are the same molecule, but the contexts differ. “Bremelanotide” and “Vyleesi” refer to the FDA-reviewed, pharmaceutical-grade product with a defined dose, formulation, and label. “PT-141,” as it circulates in the research-chemical and gray markets, refers to lyophilized powder of variable purity, provenance, and concentration that has not been through that regulatory process. Conflating the two, treating a research-chemical vial as if it carried the evidence base of the approved drug, is one of the most common and most misleading errors in this space.
The Molecular Mechanism: Melanocortin Receptors and the MC4R Question
The melanocortin system consists of five G-protein-coupled receptors (MC1R through MC5R), their peptide agonists derived from proopiomelanocortin (POMC), and endogenous antagonists such as agouti-related peptide (AgRP). These receptors are distributed across skin, adrenal cortex, immune cells, and, critically for this discussion, the central nervous system.78 Bremelanotide is a non-selective agonist across several melanocortin receptors but is generally described as acting on sexual function primarily through MC4R and, to a lesser extent, MC3R in the brain.110
MC4R is the most highly expressed melanocortin receptor in the CNS, concentrated in the hypothalamus and limbic structures. Its best-established physiological role is in energy homeostasis and appetite regulation; loss-of-function MC4R mutations are among the most common monogenic causes of human obesity, and MC4R agonists such as setmelanotide are approved for specific genetic obesity syndromes.7 The same receptor population is implicated in sexual motivation, autonomic tone, nociception, and neuro-inflammatory signaling. It is this multi-functionality, one receptor family touching energy, mood, immune tone, and sexual drive, that generates the speculative bridge to fatigue.
For the approved indication, the honest mechanistic statement is that the mechanism is not fully known. The FDA label states plainly that the way Vyleesi improves HSDD “is unknown.”1 The leading hypothesis is that bremelanotide activates MC4R-expressing neurons in the hypothalamus and limbic system, enhancing central neural responses to sexual cues and lowering the cognitive-emotional threshold for desire, rather than acting on genital blood flow the way a PDE5 inhibitor does.11 In other words, it is thought to work “upstream,” on motivation and central arousal circuitry, not “downstream” on the vasculature. This central-motivational model is precisely why some have speculated it might touch the low-drive, low-motivation phenotype seen in chronic-illness fatigue, but speculation is all it is.
The anti-inflammatory arm of melanocortin biology is real and well documented, and it is worth stating carefully so it is not overread. Melanocortin peptides, including alpha-MSH and ACTH, reduce pro-inflammatory cytokine production and have been studied in inflammatory bowel disease, pulmonary inflammation, and atherosclerosis models.8 Much of this anti-inflammatory action runs through MC1R and MC3R on immune cells rather than the MC4R that bremelanotide is thought to use for sexual effects. So even if one accepts that melanocortin signaling can dampen inflammation, and that inflammation contributes to sickness-behavior fatigue, it does not follow that bremelanotide, with its particular receptor profile, dose, and pharmacokinetics, would deliver a meaningful anti-fatigue effect. The receptor subtype, the tissue, the dose, and the timing all matter, and the alignment required for a real clinical benefit is far from established.
Pharmacologically, bremelanotide is short-acting. After subcutaneous injection it reaches peak plasma concentration at roughly one hour, with a mean terminal half-life of about 2.7 hours (range roughly 1.9 to 4.0 hours) and near-complete bioavailability.6 This is an “on-demand” pharmacology: a transient pulse of receptor activation, not sustained receptor occupancy. That is well suited to an on-demand sexual indication but is a poor fit, at least intuitively, for a chronic, persistent symptom like the fatigue of a long-term illness, which would presumably require sustained rather than episodic intervention. The mismatch between an on-demand drug and a chronic symptom is one of several reasons the fatigue hypothesis should be treated skeptically.
What the Human Evidence Actually Shows (and Its One Approved Use)
The human evidence for bremelanotide is essentially the evidence for its approved indication. The pivotal data come from two identically designed Phase 3 trials collectively branded RECONNECT (Study 301 and Study 302), which enrolled 1,247 premenopausal women with acquired, generalized HSDD, randomized to bremelanotide 1.75 mg subcutaneously on demand or placebo over 24 weeks.2 These are the trials that support the label, and they are the appropriate yardstick for what “evidence” means for this compound.
The results were statistically significant but modest in absolute terms, and it is important to represent them accurately rather than in the inflated form common on vendor pages. On the co-primary endpoints, bremelanotide improved the Female Sexual Function Index (FSFI) desire-domain score by about 0.35 points more than placebo, and reduced distress associated with low desire.2 On the global assessment questionnaire in the RECONNECT trials, responder rates were roughly 58% for bremelanotide versus roughly 36% for placebo, a real difference, but one against a high placebo response.2 Notably, the trials did not demonstrate an increase in the number of satisfying sexual events, an endpoint many would consider clinically central.
| Domain | What the RECONNECT trials tested | Result |
|---|---|---|
| Population | Premenopausal women with acquired, generalized HSDD | 1,247 randomized2 |
| Primary endpoint (desire) | Change in FSFI desire-domain score vs placebo | ~+0.35 points, P<0.0012 |
| Primary endpoint (distress) | Reduction in desire-related distress | Statistically significant2 |
| Satisfying sexual events | Change in event frequency | No significant increase2 |
| Fatigue in chronic illness | Not studied | No data3 |
Long-term safety was assessed in an open-label extension in which participants could continue for up to 52 additional weeks; this study characterized tolerability over time but did not expand the efficacy claims beyond HSDD.3 Across the entire clinical development program, the evidence base is HSDD in premenopausal women. There is no comparable body of randomized, controlled data for postmenopausal women, for men, for erectile dysfunction (the original nasal program never reached approval), or for any fatigue-related or chronic-illness indication.
On the specific question this article addresses, the evidentiary record is not “weak,” it is essentially empty. A search of the trial and literature record does not reveal randomized controlled trials of bremelanotide for fatigue, for ME/CFS, for cancer-related fatigue, for multiple-sclerosis fatigue, or for the sexual dysfunction that accompanies chronic disease.3 Claims that PT-141 “boosts energy,” “restores vitality,” or “corrects illness-related fatigue” are not supported by any trial designed to test them. The strongest defensible statement is a negative one: we do not know, because the studies have not been done.
This is the crux of the honesty problem. It is entirely possible for a compound to have a legitimate, approved effect in one narrow population and simultaneously be the subject of unsupported claims in adjacent populations. Bremelanotide’s real, FDA-recognized effect on desire in premenopausal women with HSDD does not transfer, evidentially, to the fatigue and libido changes of someone with lupus or chronic kidney disease. Treating the approved data as if it “covers” those uses is a category error, and it is the error that most PT-141 fatigue marketing depends on.
Fatigue and the Melanocortin System: Biological Plausibility vs. Proof
To evaluate the title’s hypothesis fairly, it helps to separate three distinct claims that are often blurred together: (1) that melanocortin signaling is involved in fatigue biology; (2) that MC4R agonism could plausibly influence fatigue; and (3) that bremelanotide does improve fatigue in people with chronic illness. The first is defensible, the second is speculative, and the third is unsupported. Keeping them separate is the entire discipline of reading this literature honestly.
On the first claim, there is a genuine biological rationale. Chronic-illness fatigue is increasingly understood through the lens of “sickness behavior,” a coordinated response to inflammation in which pro-inflammatory cytokines act on the brain to produce lethargy, reduced motivation, anhedonia, and social withdrawal. The melanocortin system is one of the CNS pathways that modulates this response, and MC4R sits at the intersection of energy sensing, inflammatory signaling, and motivated behavior.78 Melanocortin peptides have measurable anti-inflammatory effects in preclinical models, and disordered energy homeostasis is a hallmark of MC4R biology.7 So it is not unreasonable to say the melanocortin system participates in the machinery of fatigue.
The second claim, that MC4R agonism could therefore be leveraged against fatigue, is where the reasoning becomes speculative and where several complications appear. MC4R signaling is bidirectional and context-dependent: the same receptor family involved in anti-inflammatory tone is also central to anorexigenic (appetite-suppressing) and, in some models, catabolic and stress-associated pathways. Overactivation of central melanocortin signaling is associated with cachexia and weight loss in illness, not with restored vigor. In fact, MC4R antagonists, not agonists, have been explored for cancer- and disease-associated cachexia and anorexia. That is close to the opposite of what a naive “MC4R agonist fights fatigue” story would predict, and it is a strong reason to distrust simple narratives.
The third claim, that bremelanotide specifically improves chronic-illness fatigue, has no direct human evidence at all.3 Even setting aside the receptor-direction problem, bremelanotide’s on-demand pharmacology (a roughly 2.7-hour half-life, a transient pulse of activation) is poorly matched to a persistent symptom that would require sustained modulation.6 Any anecdotal report of “more energy” after a dose is confounded by the intense placebo responses seen even in the controlled HSDD trials, by the subjective and fluctuating nature of fatigue, by expectancy effects, and by the transient autonomic changes (flushing, blood-pressure shifts) the drug produces, which a person might misread as “activation.”
There is also a plausible indirect route worth naming precisely so it is not overstated. If a chronically ill person’s fatigue is intertwined with the demoralization of losing sexual function, and if a compound genuinely improved sexual desire, one could imagine a secondary lift in mood and perceived energy. But this is a hypothesis about a downstream, quality-of-life effect in a specific subgroup, not a demonstration that the drug acts on the biology of fatigue, and it has not been tested in any chronic-illness population. Readers exploring the broader landscape of compounds studied for cognitive and energy-related endpoints can compare, for context only, the site’s overview pages such as the Semax protocol; the comparison is educational and implies no equivalence of evidence.
Libido Dysregulation in Chronic Illness: What We Know and Don’t
Sexual dysfunction is genuinely common in chronic illness, and it is one of the most under-addressed dimensions of long-term disease. Conditions such as chronic kidney disease, diabetes, multiple sclerosis, cardiovascular disease, depression, and autoimmune disorders are all associated with elevated rates of low desire, arousal difficulty, and reduced sexual satisfaction. The causes are typically multifactorial: the illness itself, its inflammatory and hormonal consequences, fatigue and pain, medication side effects (antidepressants and antihypertensives are frequent contributors), vascular and neurological changes, and the psychological burden of chronic disease. This is a real clinical problem that deserves serious attention, which is different from saying bremelanotide is the answer to it.
The tempting logic runs: bremelanotide is a desire drug that works centrally; chronically ill people often have low desire; therefore bremelanotide should help. The flaw is that the approved evidence comes from a deliberately curated population, otherwise healthy premenopausal women with acquired, generalized HSDD and, importantly, no confounding medical explanation for their low desire.2 The RECONNECT trials specifically studied a condition defined by the absence of a medical or medication cause. Chronic-illness libido dysregulation is, almost by definition, the opposite situation: desire is low because of an underlying disease, its inflammatory milieu, or its treatment. Extrapolating an effect measured in the former group to the latter is exactly the kind of population mismatch that invalidates confident predictions.
There are also specific safety reasons the extrapolation is risky rather than merely unproven. Bremelanotide transiently raises blood pressure and lowers heart rate, and it is contraindicated in uncontrolled hypertension and in known cardiovascular disease.1 Many chronic-illness populations, people with kidney disease, diabetes, or cardiovascular conditions, carry exactly the cardiovascular risk profile the label warns against. A drug’s theoretical benefit is meaningless if the population most likely to be targeted is also the population in whom it is most cautioned. This is not a minor footnote; it is a structural reason why the “chronic illness” framing is more fraught, not less, than the approved use.
It is worth stating what responsible management of libido dysregulation in chronic illness actually looks like, so the contrast is clear. Evidence-based approaches begin with reviewing and adjusting causative medications, optimizing treatment of the underlying disease and its inflammation, addressing depression and relationship factors, evaluating hormonal status, and considering approved therapies appropriate to the specific diagnosis and sex. These are unglamorous, individualized, clinician-guided steps. They are also where the real evidence lives. An unapproved, off-label injection promoted as a shortcut around that work is not a substitute for it, and framing it as one does a disservice to people managing difficult illnesses.
None of this means the underlying scientific question is uninteresting. A properly designed trial, bremelanotide versus placebo for sexual dysfunction in a defined chronic-illness population, with careful cardiovascular screening and validated fatigue and sexual-function endpoints, would be a legitimate and welcome study. The honest position is that such trials have not been done, and until they are, “PT-141 for chronic-illness libido” remains a hypothesis dressed up, in much online content, as a conclusion.
How PT-141 Compares to Related Compounds and Approaches
Placing bremelanotide next to its neighbors clarifies both what is distinctive about it and how narrow its evidence base is relative to the breadth of claims made for it. The comparison below is descriptive and educational, not a ranking or a recommendation, and it deliberately foregrounds evidence level rather than mechanism hype.
| Compound / approach | Primary mechanism | Approved use | Relevance to fatigue/libido in chronic illness |
|---|---|---|---|
| Bremelanotide (PT-141) | Central MC4R agonism1 | HSDD in premenopausal women (US only)1 | No trial evidence in chronic-illness fatigue or libido3 |
| PDE5 inhibitors (e.g., sildenafil) | Peripheral vasodilation | Erectile dysfunction; pulmonary hypertension | Act on genital blood flow, not central desire; not fatigue drugs |
| Flibanserin (Addyi) | Central serotonergic/dopaminergic modulation | HSDD in premenopausal women | Daily dosing, alcohol interaction; also studied only in HSDD |
| Setmelanotide | MC4R agonist | Specific genetic obesity syndromes | Same receptor family, different indication; illustrates MC4R breadth7 |
| Melanotan II | Non-selective melanocortin agonist | None (not approved) | Ancestor of PT-141; unregulated, notable safety concerns9 |
The most important comparison for the title’s premise is the one against its own ancestor, Melanotan II, and against PDE5 inhibitors. Melanotan II is a cautionary example of a melanocortin agonist that circulated widely without approval and accumulated safety concerns including pigmentary changes, nausea, and case reports of adverse events; bremelanotide’s development was in part an effort to build a cleaner, more selective, better-characterized molecule.9 The contrast with PDE5 inhibitors is instructive in a different way: sildenafil and its relatives act peripherally on blood flow and have a large, well-defined evidence base for erectile dysfunction, but they are not desire drugs and are not fatigue drugs, which highlights how mechanism-specific these agents are. No approved agent in this table is an “energy” drug.
Within its own drug class, bremelanotide is distinguished by being the melanocortin agonist that reached approval for a sexual-desire indication, and by its on-demand subcutaneous route. Flibanserin, the other approved HSDD therapy, works through an entirely different central mechanism and requires daily dosing with a notable alcohol interaction; the two are sometimes discussed together only because they share an indication, not a mechanism. Setmelanotide, another MC4R agonist, is approved for rare genetic obesity, a vivid reminder that “MC4R agonist” is not a therapeutic category by itself, the same receptor supports drugs with completely different clinical purposes.7
The practical lesson from this landscape is that mechanism-level similarity tells you very little about clinical effect. A reader tempted by the reasoning “PT-141 hits MC4R, MC4R is involved in energy, therefore PT-141 fights fatigue” should notice that setmelanotide also hits MC4R and is used to increase satiety and reduce weight in specific syndromes, a completely different clinical outcome from the same receptor. Receptor pharmacology is necessary but nowhere near sufficient to predict a therapeutic effect, and the diversity of outcomes across this class is the proof. For those mapping how the site organizes these compounds, the broader dosage index and the peptide stacks overview catalog protocols across many mechanisms; none of these listings should be read as endorsing off-label fatigue use.
Research Models and Methodology
Understanding how bremelanotide is studied clarifies why the fatigue-and-libido claims are so poorly supported: the methods used to build its evidence base were designed to answer a specific question, and that question was not about fatigue. Its development followed a conventional pharmaceutical arc, preclinical receptor pharmacology and animal behavioral models, then early human safety and pharmacokinetics, then randomized controlled efficacy trials in the target indication.5
Preclinically, melanocortin agonists have been characterized through receptor-binding and functional assays that quantify affinity and potency at MC1R through MC5R, and through animal behavioral paradigms. Rodent models of sexual behavior, measuring proceptive and receptive behaviors in females and erectile responses in males, provided the original signal that a melanocortin agonist could influence sexual motivation centrally rather than peripherally. It is these central-behavior models, not any fatigue or chronic-illness model, that shaped the drug’s development. More recent non-clinical work has continued to probe melanocortin behavioral pharmacology, but the translational chain that led to approval was specifically a sexual-motivation chain.
The clinical methodology that matters most is the Phase 3 design: randomized, double-blind, placebo-controlled, parallel-group trials with pre-specified co-primary endpoints (validated desire and distress instruments), fixed dose (1.75 mg subcutaneously, on demand), and a defined 24-week duration in a tightly screened population.2 Several methodological features are worth flagging because they bound what the data can support. The endpoints were patient-reported outcomes on validated but subjective scales, which are appropriate for a desire indication but are highly sensitive to placebo and expectancy effects, and indeed the placebo response in these trials was substantial.4 The population was curated to exclude medical and medication causes of low desire, which maximizes internal validity for HSDD but sharply limits generalizability to chronically ill people.
For anyone genuinely interested in whether bremelanotide affects fatigue or chronic-illness libido, the methodological gap is glaring: none of the endpoints in the approved program measured fatigue, none of the populations included chronic-illness cohorts, and no validated fatigue instrument (such as the Multidimensional Fatigue Inventory or the FACIT-Fatigue scale) was a pre-specified outcome.3 A study that does not measure fatigue cannot provide evidence about fatigue, no matter how large or well-conducted it is for its actual purpose. This is not a subtle statistical point; it is the difference between having data and not having it.
A properly designed study to test the title’s hypothesis would look quite different from anything run to date. It would enroll a defined chronic-illness population (say, adults with a specific autoimmune or metabolic condition and clinically significant fatigue), screen carefully for the cardiovascular contraindications the label specifies, randomize against placebo, use validated co-primary endpoints for both fatigue and sexual function, and follow participants long enough to distinguish a genuine effect from placebo and regression to the mean. Until studies of that design exist, the correct methodological verdict is that the question is unanswered. In the research-education framing this site uses, methodology is not a formality, it is the reason a claim can or cannot be trusted, and here the methodology needed to support the claim simply has not been executed.
Safety and Tolerability
Bremelanotide’s safety profile is reasonably well characterized within its approved use and dosing limits, and that qualifier is essential, because most of the reassurance in the safety literature applies specifically to on-demand dosing capped at one dose per 24 hours and no more than eight doses per month.1 Outside those bounds, the picture changes for the worse, which is directly relevant to any speculative “chronic” or higher-frequency use for fatigue.
The most common adverse effects in the controlled trials were gastrointestinal and vasomotor. Nausea was strikingly frequent, reported by roughly 40% of bremelanotide users versus about 1% on placebo, and was severe enough that a minority of participants required anti-nausea medication or discontinued.4 Flushing (around 20%), headache (around 11%), and injection-site reactions were also more common than with placebo.4 These are not trivial for a symptomatic population: a person already burdened by chronic-illness fatigue and nausea is a poor candidate for a drug whose most common effect is more nausea.
| Adverse effect | Bremelanotide | Placebo | Note |
|---|---|---|---|
| Nausea | ~40%4 | ~1% | Most common; sometimes severe |
| Flushing | ~20%4 | ~1% | Vasomotor |
| Headache | ~11%4 | ~2% | Common |
| Injection-site reaction | ~5%4 | ~0.5% | Local |
| Focal hyperpigmentation | ~1% at label dosing12 | — | >1/3 with daily dosing; may be permanent |
The cardiovascular signal is the most clinically important. Bremelanotide transiently increases systolic blood pressure by roughly 6 mmHg and diastolic by roughly 3 mmHg, peaking around 30 to 60 minutes after a dose and generally resolving within a few hours, accompanied by a transient reduction in heart rate.1 Because of this, it is contraindicated in uncontrolled hypertension and known cardiovascular disease, and is not recommended for people at high cardiovascular risk.1 This is the same signal that halted the original intranasal erectile-dysfunction program, and it is the reason the daily/monthly dosing caps exist. For chronic-illness populations, who disproportionately carry cardiovascular and renal comorbidity, this contraindication overlaps heavily with the very people a fatigue-and-libido claim would target.
The pigmentation risk deserves special emphasis because it scales with frequency of dosing, and speculative fatigue use would likely involve more frequent dosing than the label allows. Focal hyperpigmentation of the face, gums, or breasts occurred in about 1% of subjects at label-compliant dosing but in more than a third of subjects who received up to sixteen consecutive daily doses, and the discoloration may not resolve after stopping.12 This is a concrete, potentially permanent harm that becomes substantially more likely under exactly the high-frequency, chronic dosing pattern that a “fatigue” or “energy” use case would tend to encourage. Additional caution applies to people with darker skin who may be more prone to pigmentary changes.
Hepatic safety appears generally reassuring at label doses, with no clear signal of clinically significant liver injury in the approved-use data.13 But the honest summary is that the favorable safety statements are tethered to a specific, low-frequency, on-demand regimen in a screened, otherwise-healthy population. None of that reassurance transfers automatically to unapproved gray-market PT-141 of uncertain purity, used at unvalidated frequencies, in people with the comorbidities common to chronic illness. Safety, like efficacy, is indication- and dose-specific, and extending it beyond the studied conditions is not warranted.
Handling and Reconstitution in a Research Context
Because PT-141 circulates widely as a lyophilized research chemical, a brief, strictly educational note on handling is warranted, framed entirely around laboratory and research context rather than human use. This section describes how such peptides are conventionally handled in vitro; it is not instruction for self-administration, and the compound’s only legitimate human use is the FDA-approved product under medical supervision.
Research-grade peptides are typically supplied as a lyophilized (freeze-dried) white powder in a sealed vial, often with a stated nominal mass such as 10 mg. Reconstitution in a research setting generally uses bacteriostatic or sterile water, added slowly against the vial wall rather than injected forcefully onto the powder, and the vial is swirled rather than shaken, since aggressive agitation can shear and degrade peptide structure. The chosen diluent volume determines the resulting concentration, which is why any research protocol pairs a nominal vial mass with a defined reconstitution volume to yield a known concentration for accurate measurement. The site’s PT-141 protocol page lays out these conventions, and a general reconstitution guide covers the shared principles across compounds.
Stability and storage are the practical variables that most affect a research peptide’s integrity. Lyophilized bremelanotide is generally more stable and is typically stored refrigerated and protected from light; once reconstituted, aqueous peptide solutions are less stable and are conventionally kept refrigerated and used within a limited window, with bacteriostatic water (containing benzyl alcohol) preferred over plain sterile water when multiple withdrawals from a vial are anticipated, for its antimicrobial property. Freeze-thaw cycling of reconstituted solution is generally avoided because it degrades peptides. These are ordinary laboratory-handling considerations, not endorsements of use.
A central caveat dominates this entire topic: research-chemical PT-141 is not the approved drug. It has not undergone the identity, purity, potency, sterility, and endotoxin testing that a regulated pharmaceutical product requires. Independent analyses of gray-market peptides across the industry have repeatedly found discrepancies between labeled and actual content, contaminants, and inconsistent concentrations. This means that even the modest, indication-specific safety and efficacy data discussed earlier, which pertain to pharmaceutical-grade Vyleesi, cannot be assumed to apply to a research vial of unknown provenance. The uncertainty compounds: an unapproved use, of an unapproved-for-that-purpose molecule, in an unverified formulation.
Anyone approaching PT-141 in a genuine research context, in vitro or in a properly authorized preclinical study, would work within institutional oversight, use analytically characterized material, and never treat handling instructions as a bridge to human use. For any question about a person’s own fatigue, libido, or chronic illness, the appropriate path is a qualified clinician who can evaluate the underlying disease and the evidence-based options for it. The tools this site provides, including a dosage calculator, exist to make research-context concentration math accurate and transparent, not to encourage unsupervised use.
Limitations and the Human-Evidence Gap
It is worth consolidating, in one place, the full scope of what is not known, because the gaps are the real answer to the title’s question. The central limitation is simple and decisive: there are no randomized controlled trials of bremelanotide for fatigue or for libido dysregulation in any chronic-illness population.3 Every efficacy statement that can be made with confidence pertains to acquired, generalized HSDD in premenopausal women, and even there the effect size is modest and does not extend to the frequency of satisfying sexual events.2
Beyond the absence of fatigue trials, several specific gaps compound the uncertainty. First, the studied population was deliberately free of medical and medication causes of low desire, the exact opposite of the chronic-illness scenario, so external validity to ill populations is essentially unestablished.2 Second, the drug’s on-demand pharmacology is a conceptual mismatch for a chronic, persistent symptom, and no data address whether or how it might be used for a sustained condition.6 Third, the receptor pharmacology cuts in ambiguous directions: MC4R agonism is associated with satiety and, in some contexts, catabolic and anorexia-related pathways, so the naive “agonism equals energy” story is not merely unproven but arguably contradicted by the broader biology.
There are also population-safety gaps. The cardiovascular contraindications overlap heavily with the comorbidity profile of many chronic-illness groups, yet no trials have specifically evaluated bremelanotide’s cardiovascular safety in those higher-risk populations.1 Long-term data exist only for the approved on-demand regimen; there are no long-term data for the higher-frequency dosing that a fatigue use case would likely involve, where the pigmentation risk in particular rises sharply.12 And essentially all of the reassuring data pertain to pharmaceutical-grade product, not to the research-chemical PT-141 that most speculative use would actually involve.
Methodologically, even the anecdotal reports that circulate are weak evidence. Fatigue and libido are subjective, fluctuating, and heavily influenced by expectation, making them among the endpoints most vulnerable to placebo effects, and the HSDD trials themselves showed large placebo responses.4 A person who injects an unapproved compound hoping for more energy and then reports feeling better has produced a data point almost entirely confounded by expectancy, natural symptom variability, and possibly the misattribution of transient autonomic effects (flushing, blood-pressure changes) to “vitality.” Uncontrolled self-report cannot distinguish a real drug effect from these confounds, which is precisely why controlled trials exist.
The intellectually honest conclusion is not “PT-141 does nothing for fatigue,” nor “PT-141 helps fatigue,” but rather “the question has not been tested, the biology is ambiguous, the pharmacology is a poor fit, the safety overlap with chronic-illness populations is unfavorable, and the burden of proof has not been met.” Filling that gap would require the specific, well-designed trials described earlier. Absent them, any confident claim in either direction, and especially any therapeutic claim, outruns the evidence.
Regulatory Status
Bremelanotide’s regulatory position is narrow and unambiguous, and it is the single most important fact for a reader trying to calibrate the claims in this space. In the United States, the FDA approved bremelanotide (Vyleesi) in June 2019 for one indication only: the treatment of acquired, generalized hypoactive sexual desire disorder in premenopausal women.15 The approval is explicitly limited by patient population (premenopausal women), disorder type (acquired and generalized, not lifelong or situational), and it is not indicated to enhance sexual performance, is not for postmenopausal women, and is not for men.1
Every other use is, in regulatory terms, off-label or investigational. That includes any use for fatigue, for chronic-illness-associated symptoms, for erectile dysfunction in men (the original nasal program for which was halted and never approved), for general “libido enhancement,” and for the anti-inflammatory or metabolic applications that melanocortin biology might theoretically suggest.9 “Off-label” does not by itself mean unsafe or unreasonable in the hands of a physician exercising judgment for an individual patient, but it does mean the use has not been reviewed or approved by a regulator and is not backed by the trial evidence that supported the on-label indication. For the specific uses in this article’s title, off-label is not even the right word, because there is no substantial evidence base to be “off” of.
Internationally, the situation is more restrictive still. Bremelanotide is not approved by the European Medicines Agency, and as of the most recent information there is no EMA-approved pharmacotherapy for HSDD in the European Union.14 This means that outside the United States, even the one indication for which bremelanotide has robust evidence generally lacks a regulatory home. A compound with a single approved use in one jurisdiction, and no approval in another major jurisdiction, is not a compound whose broad off-label promotion rests on regulatory endorsement anywhere.
The research-chemical dimension adds a further legal and quality layer. Material sold as “PT-141” for “research use only” is not an approved drug, is not manufactured or tested to pharmaceutical standards, and is explicitly not intended or authorized for human consumption. Marketing such material with therapeutic claims, for fatigue, libido, or anything else, would run counter to its stated status and to the regulatory reality that no such uses are approved. The gap between “an FDA-approved on-demand desire drug for a specific group of women” and “an energy-and-libido peptide for chronic illness” is not a gray area; it is the difference between an approved indication and an untested claim.
The practical takeaway is that regulatory status functions here as a reality check on enthusiasm. Bremelanotide is a real drug with a real, if modest, approved effect in a narrowly defined population. It is also the subject of expansive claims that its regulatory record does not support. Anyone weighing information about PT-141 should keep that boundary firmly in view, and should treat therapeutic claims about fatigue and chronic illness as hypotheses awaiting evidence, not as established facts. Decisions about symptoms in the context of a real illness belong with a qualified clinician, not with a research-chemical vendor’s marketing copy.
Frequently Asked Questions
Is PT-141 (bremelanotide) approved to treat fatigue?
No. Bremelanotide is FDA-approved only as Vyleesi for acquired, generalized hypoactive sexual desire disorder in premenopausal women.1 It has no approval for fatigue, and there are no randomized controlled trials showing it improves fatigue in any population, including chronic-illness populations.3 Claims that it “boosts energy” are not supported by trial evidence.
If the melanocortin system is involved in fatigue, doesn’t that mean PT-141 should help?
Not necessarily. The melanocortin system does participate in energy balance and inflammation, but MC4R agonism is also linked to satiety and, in some contexts, to catabolic and anorexia-related pathways, so the biology does not point cleanly toward an anti-fatigue effect.78 A pathway being involved in fatigue is not the same as a drug touching that pathway treating fatigue. That gap can only be closed by trials, which have not been done.
Can PT-141 help sexual problems caused by a chronic illness?
There is no direct evidence for this. The approving trials studied otherwise-healthy premenopausal women whose low desire had no medical or medication cause, essentially the opposite of chronic-illness libido dysregulation.2 Extrapolating from that population to chronically ill people is not supported, and several chronic-illness groups carry the cardiovascular risk profile the drug’s label specifically cautions against.1
How well does bremelanotide actually work for its approved use?
The effect is statistically significant but modest. In the Phase 3 RECONNECT trials it improved the FSFI desire-domain score by about 0.35 points more than placebo and reduced desire-related distress, but it did not significantly increase the number of satisfying sexual events, and the placebo response was substantial.24 It is a meaningful but limited effect, not a dramatic one.
What are the main safety concerns?
Nausea is very common (about 40% versus 1% on placebo), along with flushing and headache.4 The drug transiently raises blood pressure and lowers heart rate and is contraindicated in uncontrolled hypertension and known cardiovascular disease.1 Focal hyperpigmentation of the face, gums, or breasts can occur and becomes much more likely with frequent daily dosing, and it may be permanent.12
Is “research-chemical” PT-141 the same as the approved drug?
No. Gray-market PT-141 sold for “research use only” is not manufactured or tested to pharmaceutical standards, may vary in purity and concentration, and is not authorized for human use. The safety and efficacy data discussed here pertain to pharmaceutical-grade Vyleesi and cannot be assumed to apply to unregulated material of uncertain provenance.
Is bremelanotide approved outside the United States?
Generally no. It is not approved by the European Medicines Agency, and there is no EMA-approved pharmacotherapy for HSDD in the European Union as of the most recent information.14 Its approval is essentially limited to the US indication.
What should someone with chronic-illness fatigue or low libido do instead?
Speak with a qualified clinician. Evidence-based management focuses on treating the underlying disease and its inflammation, reviewing medications that may lower desire or energy, addressing depression and relationship factors, evaluating hormonal status, and considering approved therapies appropriate to the specific diagnosis. An unapproved off-label injection is not a validated substitute for that individualized evaluation.
References
- U.S. Food and Drug Administration. VYLEESI (bremelanotide injection) Prescribing Information, 2019. accessdata.fda.gov/drugsatfda_docs/label/2019/210557s000lbl.pdf
- Kingsberg SA, Clayton AH, Portman D, et al. Bremelanotide for the Treatment of Hypoactive Sexual Desire Disorder: Two Randomized Phase 3 Trials. Obstet Gynecol. 2019;134(5):899-908. pmc.ncbi.nlm.nih.gov/articles/PMC6819021
- Simon JA, Kingsberg SA, Portman D, et al. Long-Term Safety and Efficacy of Bremelanotide for Hypoactive Sexual Desire Disorder. Obstet Gynecol. 2019;134(5):909-917. pubmed.ncbi.nlm.nih.gov/31599847
- Clayton AH, Kingsberg SA, Portman D, et al. Safety Profile of Bremelanotide Across the Clinical Development Program. J Womens Health. 2022;31(2):171-182. journals.sagepub.com/doi/full/10.1089/jwh.2021.0191
- Dhillon S, Keam SJ. Bremelanotide: First Approval. Drugs. 2019;79(14):1599-1606. researchgate.net/publication/335242211
- Rooney KL, et al. Bremelanotide for the Treatment of Female Hypoactive Sexual Desire Disorder. Neurol Int. 2022;14(1):6. pmc.ncbi.nlm.nih.gov/articles/PMC8788464
- Krashes ML, Lowell BB, Garfield AS. Melanocortin-4 receptor-regulated energy homeostasis. Nat Neurosci. 2016;19(2):206-219. pmc.ncbi.nlm.nih.gov/articles/PMC5244821
- Wang W, et al. Melanocortin Regulation of Inflammation. Front Endocrinol. 2019;10:683. pmc.ncbi.nlm.nih.gov/articles/PMC6794349
- Palatin Technologies. FDA Approves New Drug Application for Vyleesi (bremelanotide injection) — company history and development background. palatin.com press release
- PubChem / structural and pharmacologic summary of bremelanotide (Ac-Nle-cyclo[Asp-His-D-Phe-Arg-Trp-Lys]-OH). See FDA label ref. 1 and: en.wikipedia.org/wiki/Bremelanotide (secondary summary)
- Palatin / VYLEESI clinical mechanism materials; DailyMed Label: VYLEESI- bremelanotide injection. dailymed.nlm.nih.gov (Vyleesi)
- FDA Prescribing Information, Warnings and Precautions — focal hyperpigmentation with repeated daily dosing (ref. 1); also summarized in Clayton et al. 2022 (ref. 4).
- National Institute of Diabetes and Digestive and Kidney Diseases. Bremelanotide. LiverTox: Clinical and Research Information on Drug-Induced Liver Injury. NCBI Bookshelf NBK573221. ncbi.nlm.nih.gov/books/NBK573221
- European Medicines Agency — regulatory status (no EMA marketing authorization for bremelanotide/HSDD as of latest available information). ema.europa.eu
Educational and research-use disclaimer: This article is provided for general educational and research-information purposes only and does not constitute medical advice, diagnosis, or treatment, nor an endorsement or recommendation of any compound. PT-141 (bremelanotide) is approved by the FDA only as Vyleesi for acquired, generalized hypoactive sexual desire disorder in premenopausal women; all other uses, including for fatigue or libido changes in chronic illness, are unapproved and investigational, with little or no supporting human evidence. Nothing here should be interpreted as claiming that PT-141 treats, cures, or prevents any disease. Research-chemical material is not intended for human consumption. Always consult a qualified, licensed healthcare professional before making any decision related to a medical condition or symptom.