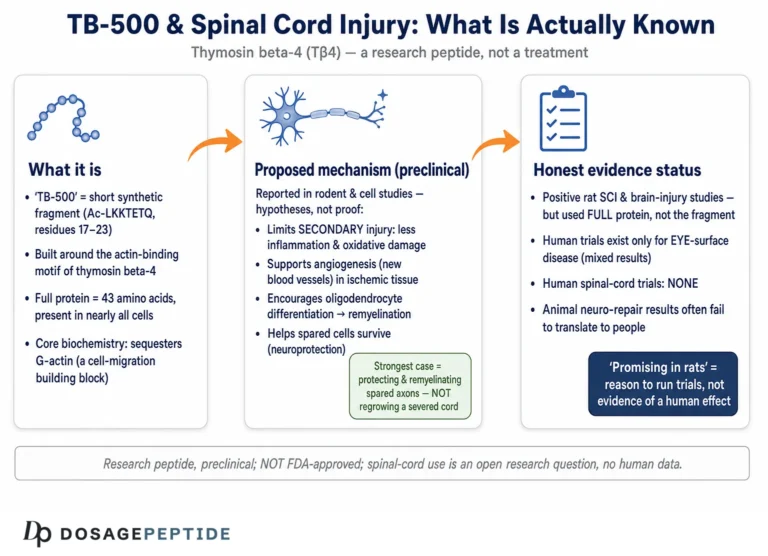
TB-500 is one of the most talked-about compounds in the “recovery peptide” conversation, routinely described in forums and vendor copy as a near-miraculous accelerator of tissue repair. The reality that emerges from the peer-reviewed literature is more measured and, in some ways, more interesting. TB-500 is a synthetic peptide built around the actin-binding domain of thymosin beta-4 (Tβ4), a small protein that virtually every cell in the mammalian body already produces. The parent molecule, Tβ4, has a genuine and substantial research pedigree spanning cardiac, dermal, corneal, and neurological injury models, along with several completed human safety and early-efficacy trials.12 The synthetic fragment sold as “TB-500,” by contrast, has almost no clinical data of its own, and the distinction between the two is the single most important thing to understand before interpreting any claim about what TB-500 “does.”
This article walks through what the research literature actually says about thymosin beta-4 and its actin-binding fragment in the context of tissue repair and healing. It covers the molecular origin of the peptide, the mechanistic hypotheses that make it biologically plausible, the strongest lines of preclinical and clinical evidence, honest comparisons with related compounds such as BPC-157, the animal and in-vitro models the field relies on, the safety record as it currently stands, practical handling considerations in a laboratory setting, the very real gap between animal findings and human proof, and the regulatory reality that TB-500 is not an approved drug anywhere.
Throughout, the goal is calibration rather than hype. Where the evidence is strong, this article says so. Where it is preclinical, in-vitro, or entirely absent for the specific fragment, it says that too. TB-500 remains an investigational research compound, not a medicine, and nothing below should be read as a claim that it treats, cures, or prevents any condition in humans.
What TB-500 Is and Where It Comes From
Thymosin beta-4 is a 43-amino-acid, roughly 4.9 kDa polypeptide first isolated from calf thymus tissue in the early 1980s. Despite the “thymosin” name, which reflects its historical discovery, it is not a thymic hormone in any meaningful sense; it is instead one of the most abundant and ubiquitous intracellular proteins in the body, present in nearly every cell type except red blood cells and at especially high concentrations in platelets, neutrophils, and wound fluid.13 Its principal, well-characterized biochemical job is to bind and sequester monomeric G-actin, and it is quantitatively the major actin-sequestering molecule in most eukaryotic cells. That single function places Tβ4 at the center of the machinery cells use to migrate, reorganize their cytoskeleton, and rebuild tissue after injury.1
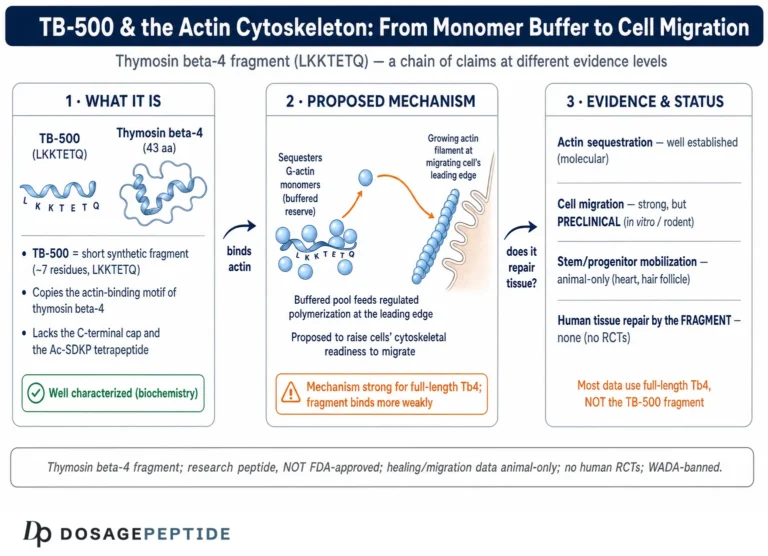
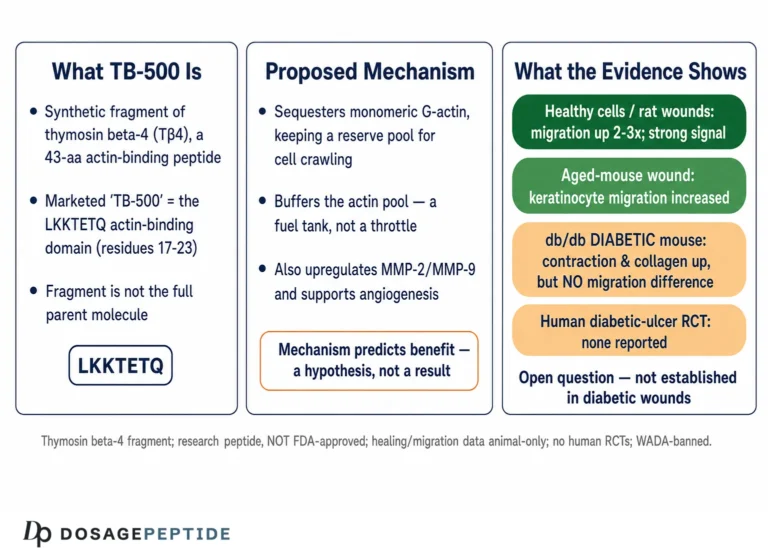
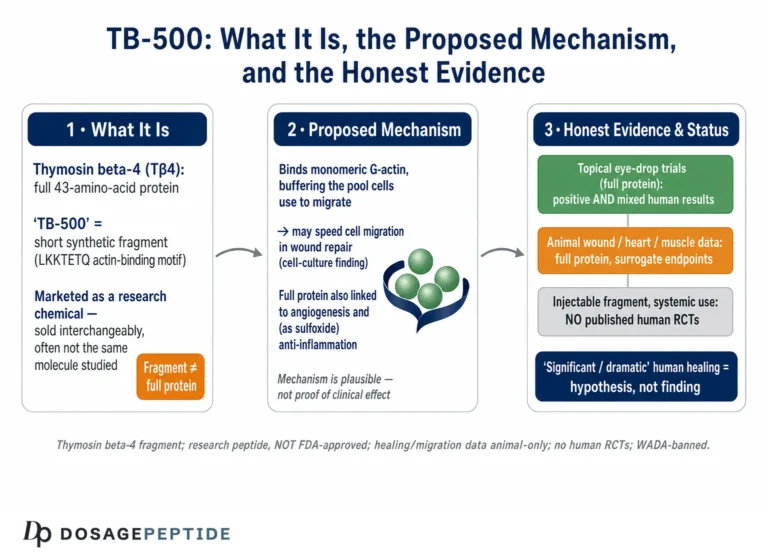
The active core of that actin-binding capacity lies in a short, conserved motif. Structural and competition studies mapped the actin-contact region to a seven-residue sequence, LKKTETQ, sitting near the center of the molecule (residues 17 through 23).4 This heptapeptide is the conceptual basis for “TB-500.” The compound distributed under that name is generally described as a synthetic, N-terminally acetylated peptide corresponding to that actin-binding domain, most precisely written as Ac-LKKTETQ. In other words, TB-500 is meant to be a minimized synthetic fragment that reproduces the actin-binding motif of the natural protein rather than the whole 43-residue molecule.
Here an important honesty flag is warranted, because the marketplace is genuinely muddled. Some products labeled “TB-500” are sold as, or are believed to actually contain, full-length synthetic thymosin beta-4 rather than the short LKKTETQ fragment, while others contain the heptapeptide or acetylated variants of it. These are chemically distinct entities. They differ in molecular weight, in three-dimensional behavior, in how long they persist in circulation, and in the breadth of biological activity they can exert, since the full protein carries additional functional regions beyond the actin-binding core. Almost the entire body of rigorous published research, including every completed human trial, was performed with full-length thymosin beta-4 (frequently the clinical-grade material formulated by RegeneRx as RGN-259, RGN-137, or RGN-352), not with the abbreviated research-market “TB-500.”28 This means that when a vendor cites a cardiac or wound-healing study to sell “TB-500,” the study almost certainly used the parent protein, and the assumption that findings transfer cleanly to a heptapeptide fragment is exactly that: an assumption, not a demonstrated fact.
For readers who want to see how the research-market compound is characterized and handled in practice, the compound-specific reference on this site is the TB-500 (10mg vial) dosage protocol page, which frames the material strictly as a research peptide. The practical takeaway of this section is simple but easy to lose: “TB-500” and “thymosin beta-4” are related but not interchangeable, and keeping the distinction in view is the difference between reading the evidence accurately and being misled by it.
The Molecular Mechanism: Actin Sequestration and Beyond
The mechanistic story of thymosin beta-4 begins with actin dynamics. Inside a cell, actin exists in equilibrium between free monomers (G-actin) and polymerized filaments (F-actin). Tβ4 binds G-actin monomers in a 1:1 complex and holds them in reserve, acting as a buffer that maintains a large pool of unpolymerized actin ready to be deployed.1 When a cell receives a signal to move, spread, or extend a leading edge, monomers are released from Tβ4 and fed into growing filaments, driving the shape changes and locomotion that underlie cell migration. Because coordinated cell migration is fundamental to closing wounds, regrowing epithelium, forming new blood vessels, and repopulating damaged tissue with reparative cells, this actin-buffering role provides a coherent first-principles explanation for why the molecule keeps appearing in tissue-repair contexts.1 The LKKTETQ motif that TB-500 reproduces is the part of the protein that physically contacts actin, which is why the fragment is hypothesized to retain at least this core activity.4
Actin sequestration, however, is only the opening chapter, and the “and more” is where the biology becomes rich. Research on the full protein has implicated Tβ4 in a striking range of additional activities that plausibly contribute to repair: promotion of angiogenesis (new blood-vessel formation), stimulation of endothelial and other cell migration, upregulation of matrix-remodeling enzymes such as matrix metalloproteinase-2, recruitment and activation of progenitor and stem cells, suppression of inflammatory signaling, reduction of apoptosis (programmed cell death) in stressed cells, and modulation of fibrosis and scarring.356 A widely cited concept, from a review by Goldstein, Hannappel, and Kleinman, framed the protein as an actin-sequestering molecule that “moonlights” to repair injured tissue, capturing the idea that a housekeeping cytoskeletal protein appears to have been co-opted for a much broader regenerative role.1
At the level of intracellular signaling, one of the best-characterized pathways comes from cardiac work. Thymosin beta-4 was shown to form a functional complex with the adaptor protein PINCH and integrin-linked kinase (ILK), leading to activation of the pro-survival kinase Akt.7 Akt activation is a canonical anti-apoptotic, pro-survival signal, and this PINCH-ILK-Akt axis offered a molecular explanation for how Tβ4 could keep stressed or ischemic cells alive after injury, distinct from its purely structural actin role.7 Separate work localized the pro-angiogenic activity to the actin-binding site itself, suggesting that the same short motif responsible for actin contact also contributes to blood-vessel formation.4 Additional research pointed to a role in cell migration via matrix metalloproteinase-2-mediated cleavage of laminin-5, and to the generation of an anti-inflammatory oxidized derivative, thymosin beta-4 sulfoxide.36
Two cautions keep this mechanistic picture honest. First, most of these downstream activities were mapped using the full 43-residue protein; how faithfully a seven-residue fragment reproduces angiogenic, anti-apoptotic, anti-inflammatory, and stem-cell-recruiting effects, as opposed to just the actin-binding step, is not firmly established for the research-market compound. Second, a plausible mechanism is not the same as a demonstrated clinical benefit. A molecule can buffer actin, activate Akt in a dish, and accelerate endothelial migration on a plate while still failing to produce meaningful, reproducible healing in an intact organism at a tolerable dose. Mechanistic elegance is a reason to investigate, not a substitute for outcome data. The gap between “this molecule does something biochemically interesting” and “this molecule reliably improves healing in a living patient” is exactly where most promising preclinical compounds fail, and thymosin beta-4 has not yet definitively crossed it for any tissue-repair indication.
What the Research Actually Shows on Tissue Repair
The strongest way to summarize the evidence is by level. Thymosin beta-4 has an extensive and genuinely impressive body of preclinical data, a modest set of completed human safety and early-efficacy trials, and essentially no confirmatory, approval-grade efficacy trials that established it as a treatment for any tissue-repair indication. TB-500, the specific fragment, sits several rungs lower still, with its reputation resting almost entirely on extrapolation from the parent protein rather than on studies of the fragment itself.
On the preclinical side, full-length Tβ4 has repeatedly accelerated repair across multiple injury models. In dermal wound-healing studies it increased the rate of wound closure, enhanced angiogenesis and collagen deposition, and promoted keratinocyte and endothelial migration.5 In corneal injury models it sped epithelial healing and reduced inflammation. In rodent hair-follicle studies it activated follicle stem cells and increased hair growth, a finding tied to its stem-cell-migration and angiogenic activities.6 In neurological injury models, including stroke and traumatic brain injury, it improved functional recovery and promoted neurovascular remodeling in animals.2 This breadth, across skin, eye, heart, and nervous tissue, is what makes the molecule scientifically compelling and explains why it attracted sustained academic and commercial interest.
The table below sketches the evidence tiers, which is more useful than any single headline result.
| Evidence tier | What exists for thymosin beta-4 | What exists for the TB-500 fragment |
|---|---|---|
| In vitro / mechanistic | Extensive: actin sequestration, Akt activation, endothelial migration, MMP-2 induction17 | Limited; actin-binding motif is shared but fragment-specific data are sparse |
| Animal injury models | Broad: cardiac, dermal, corneal, neurological, hair follicle256 | Minimal peer-reviewed, fragment-specific published data |
| Human safety (Phase 1) | Completed: IV thymosin beta-4 well tolerated to high doses9 | None specific to the marketed fragment |
| Human efficacy (Phase 2) | Several: dermal ulcers, dry eye, corneal wounds; mixed/early signals810 | None |
| Confirmatory (Phase 3) / approval | None; not approved for any indication | None; not approved |
The honest reading of this table is that thymosin beta-4 is a legitimately investigated molecule that has cleared early human hurdles for safety and shown encouraging but non-definitive Phase 2 signals in a few narrow indications, while never reaching the confirmatory trials that would make it a proven therapy.810 The synthetic research fragment “TB-500” borrows the credibility of that research program without having generated an equivalent evidence base of its own. When you read a confident claim that “TB-500 heals tendons” or “TB-500 repairs muscle,” it is worth asking which molecule was actually studied, in which species, at what level of evidence, and whether any of it was the fragment in a human being. In nearly every case the answer traces back to animal or in-vitro work on the parent protein.
Cardiac and Vascular Repair Models
The cardiac literature is where thymosin beta-4 built much of its scientific reputation, and it is worth examining closely because it illustrates both the promise and the ceiling of the evidence. In a landmark 2004 study published in Nature, Bock-Marquette and colleagues reported that thymosin beta-4 promoted migration and survival of cardiac cells, activated the integrin-linked kinase and Akt pathway, and improved cardiac function after coronary artery ligation in mice, with reduced scar volume and better ejection fraction when treatment began around the time of injury.7 The proposed mechanism, preservation of ischemic cardiomyocytes through PINCH-ILK-Akt-mediated survival signaling combined with enhanced cell migration, gave the finding a satisfying mechanistic backbone rather than a black-box result.7
Subsequent animal work extended the story. Later studies reported that thymosin beta-4 was cardioprotective when administered after myocardial infarction, that systemic dosing could confer benefit following ischemic myocardial injury, and that the peptide modulated inflammation and fibrosis in cardiac tissue, in part by influencing the PINCH-1-ILK-alpha-parvin complex and suppressing pro-inflammatory NF-kappaB signaling.27 A particularly intriguing thread suggested Tβ4 could reactivate dormant epicardial progenitor cells, hinting at a regenerative rather than merely protective mechanism. Collectively, this made the heart one of the most thoroughly explored organs in the Tβ4 field and generated genuine enthusiasm about post-infarction repair.
That enthusiasm is precisely why the human translation matters, and here the record is sobering. A clinical trial was registered to study injectable thymosin beta-4 for acute myocardial infarction (ClinicalTrials.gov identifier NCT01311518), reflecting a real effort to move the compelling animal data into patients.11 Despite the strength of the preclinical signal, thymosin beta-4 did not go on to become an approved cardiac therapy, and no large, positive, confirmatory human efficacy trial established clinical benefit in myocardial infarction. This is a recurring and instructive pattern in cardiac regenerative medicine: many interventions that look transformative in rodent infarct models fail to reproduce the effect at scale in humans, whose hearts, disease timelines, comorbidities, and treatment backgrounds differ enormously from a young inbred mouse subjected to a clean surgical ligation.
For the reader interested specifically in tissue repair of tendons, muscle, and connective tissue, the relevance of the cardiac work is largely mechanistic rather than direct. The cardiac studies demonstrate that Tβ4 can promote cell survival and migration and blunt fibrosis in an injured, hypoxic tissue, which are exactly the processes one would want in a healing tendon or muscle. But they are cardiac studies, in mice, with the parent protein. Extrapolating from an improved murine ejection fraction to faster human tendon recovery with an injected heptapeptide fragment is a long chain of assumptions, each link of which is currently unproven. The cardiac chapter is best read as a proof of biological principle for the molecule’s regenerative machinery, not as evidence that TB-500 repairs musculoskeletal injuries in people.
Dermal, Corneal, and Ophthalmic Wound-Healing Data
If any indication brought thymosin beta-4 closest to real-world tissue-repair use, it was topical wound healing, and this is also where the only genuinely controlled human data live. It is worth separating the dermal (skin) program from the ophthalmic (eye) program, because they reached somewhat different endpoints.
On the dermal side, preclinical studies showed that Tβ4 promoted dermal healing by enhancing keratinocyte migration, angiogenesis, and collagen deposition, and by accelerating wound closure in animal models.5 RegeneRx developed a topical thymosin beta-4 formulation, RGN-137, and advanced it into human trials. Phase 2, blinded, placebo-controlled, dose-response trials were conducted in chronic pressure ulcers and venous stasis ulcers, and a separate Phase 2 program studied wound healing in the rare blistering disease epidermolysis bullosa.8 The consistent safety finding across these trials was encouraging: RGN-137 was reported as safe and well tolerated at the doses tested, with no drug-related serious adverse events. On efficacy, the results were more nuanced. Reports indicated that an intermediate (“mid”) dose level appeared to be the most active and to induce more rapid initiation of wound healing compared with placebo, an interesting non-monotonic dose-response pattern, but the trials did not deliver a clean, decisive efficacy verdict, and the program did not culminate in an approved product.8
The ophthalmic program arguably produced the most quantitatively striking human signals. Thymosin beta-4 eye drops (RGN-259) were evaluated for severe dry eye and corneal wound healing, indications registered on ClinicalTrials.gov. In a physician-sponsored Phase 2 randomized, double-masked, vehicle-controlled trial in severe dry eye reported by Sosne and colleagues, Tβ4-treated patients showed a 35.1% reduction in ocular discomfort versus vehicle (p=0.0141 at day 56) and a 59.1% reduction in total corneal fluorescein staining versus vehicle (p=0.0108 at day 56), along with improvements in tear-film breakup time, and the drops were safe and well tolerated.10 These are statistically significant, directionally consistent results in a real patient population, which places them among the more credible pieces of human efficacy evidence for the molecule.
Even so, the appropriate framing is cautious optimism, not vindication. These were relatively small Phase 2 studies in narrowly defined indications, using a topical formulation of the full protein delivered directly to the wounded surface (skin ulcer or ocular surface). None of that establishes that a systemically injected fragment accelerates the healing of a torn tendon, a strained muscle, or a joint injury, which are the uses most people associate with “TB-500.” The dermal and corneal data are the best human evidence the Tβ4 field has, and they are genuinely worth respecting, but they are also the clearest illustration of how narrow, indication-specific, and formulation-specific the credible evidence actually is. Readers exploring the recovery-oriented use case should treat those extrapolations as unproven, a point reinforced in the site’s discussion of the BPC-157 and TB-500 recovery blend.
TB-500 vs Thymosin Beta-4 vs BPC-157: Comparisons
Three comparisons matter most for anyone trying to make sense of TB-500: how the fragment relates to its parent protein, how it relates to recombinant clinical-grade thymosin beta-4, and how it differs from BPC-157, the peptide with which it is most often paired and confused.
The first comparison, fragment versus full protein, was introduced earlier but deserves restating because it is the crux. Full-length thymosin beta-4 is a 43-residue protein with multiple functional regions and the entire published research record behind it. TB-500 is intended to be the short acetylated actin-binding motif, Ac-LKKTETQ. The fragment may retain the core actin-binding activity but cannot be assumed to reproduce the full protein’s angiogenic, anti-apoptotic, anti-inflammatory, and stem-cell-recruiting behaviors, and it has different pharmacokinetics and stability. Marketing that cites Tβ4 studies to characterize TB-500 is quietly performing an unvalidated substitution.
The second comparison contrasts research-market TB-500 with clinical-grade thymosin beta-4 such as RegeneRx’s RGN-259, RGN-137, and RGN-352.28 The clinical material was manufactured under regulated conditions, characterized for identity and purity, and dosed in registered trials with defined formulations and routes. Research-market “TB-500” from a peptide vendor is a laboratory chemical of variable and often unverified identity, purity, and even molecular content, explicitly labeled for research use only and never intended for administration to humans. Even where the underlying amino-acid sequence overlaps, the regulatory, quality, and evidentiary contexts are worlds apart. It is a category error to cite a RegeneRx Phase 2 trial as evidence for a vendor’s research vial, yet that substitution happens constantly in marketing copy, and it is one of the most common ways readers are led to overestimate the evidence behind the compound they can actually buy.
The third comparison, TB-500 versus BPC-157, is the one researchers ask about most, because the two are frequently stacked. They are mechanistically distinct. BPC-157 is a 15-amino-acid peptide derived from a gastric protein and is most associated in the animal literature with local angiogenesis, growth-factor and nitric-oxide signaling, and direct effects on tendon and ligament fibroblasts, with the widely quoted rodent Achilles-tendon transection studies being its signature dataset. TB-500 (thymosin beta-4) is associated with actin regulation, systemic cell migration, and a broader, more diffuse regenerative profile drawn largely from muscle and cardiac models. In shorthand, BPC-157 has the more direct animal evidence for tendon and ligament, while TB-500’s supporting data lean cardiac and muscular.
| Attribute | TB-500 (thymosin beta-4 fragment) | BPC-157 |
|---|---|---|
| Origin | Actin-binding domain (LKKTETQ) of thymosin beta-4 | Fragment of a gastric protective protein (BPC) |
| Size | ~7-residue fragment (parent protein 43 residues) | 15 amino acids |
| Primary hypothesized mechanism | Actin sequestration, cell migration, angiogenesis, Akt survival signaling17 | Local angiogenesis, growth-factor/NO pathways, fibroblast effects |
| Strongest animal data | Cardiac, dermal, corneal, neurological25 | Tendon, ligament, gut |
| Human efficacy trials | Only for full protein, narrow indications; none for the fragment810 | No completed controlled efficacy trials |
| Approval status | Not approved; research only | Not approved; research only |
Crucially, no head-to-head human trial has ever compared these two peptides, so any claim that one is “better” for tendons, muscles, or recovery is not scientifically grounded, however confidently it is stated. The frequent pairing of the two, discussed in the site’s overview of BPC-157 + TB-500 blends and the corresponding TB-500 and BPC-157 stack, reflects a theoretical logic of combining a “systemic” and a “local” repair agent, but that rationale rests on unproven assumptions and has never been validated in a controlled human study.
Research Models and Methodology
To interpret the TB-500 and thymosin beta-4 literature responsibly, it helps to understand the toolbox researchers actually used, because the choice of model shapes what a result can and cannot tell you. The field spans four broad tiers: molecular and biochemical assays, cell-culture work, animal injury models, and human clinical trials.
At the biochemical level, the foundational studies characterized how Tβ4 binds G-actin, measured binding stoichiometry and affinity, and mapped the actin-contact site to the LKKTETQ motif using competition experiments with other actin-binding proteins.14 These assays are precise and reproducible, and they are the reason the actin-sequestration mechanism is considered well established. Their limitation is that they describe molecular behavior in isolation and say nothing directly about healing in a living organism.
Cell-culture (in vitro) studies form the next tier. Researchers used keratinocyte, endothelial, cardiomyocyte, and stem-cell cultures to test whether Tβ4 accelerates migration in scratch-wound assays, promotes tube formation as a proxy for angiogenesis, activates survival kinases such as Akt, or upregulates matrix-remodeling enzymes.67 These experiments established plausible cellular mechanisms and are relatively cheap and fast. Their weakness is well known across biology: a monolayer of cells in a dish, bathed in a controlled concentration of peptide, is a poor model of the crowded, vascularized, immunologically active environment of a real wound, and effects seen in vitro routinely fail to reproduce in vivo.
Animal injury models carry most of the field’s translational weight. Researchers induced controlled injuries, coronary artery ligation for infarction, full-thickness excisional or incisional skin wounds, corneal abrasions, stroke and traumatic brain injury models, and measured whether Tβ4 improved objective outcomes such as scar size, wound-closure rate, ejection fraction, or functional recovery.257 These models are far more informative than cell culture because they test the molecule in an intact organism. Yet they carry systematic biases that inflate apparent efficacy: animals are typically young, genetically uniform, healthy apart from the experimental injury, and free of the age, comorbidity, and polypharmacy that define human patients. Injuries are clean, standardized, and treated immediately, unlike the messy, chronic, variably timed injuries seen clinically. Small-animal healing physiology also differs from human physiology. These factors are a major reason so many regenerative interventions shine in rodents and disappoint in people.
Human clinical trials are the top tier and the scarcest. For thymosin beta-4 these include the completed Phase 1 intravenous safety study in healthy volunteers and the Phase 2 dermal-ulcer, dry-eye, and corneal programs described earlier.8910 Registered trials on ClinicalTrials.gov (for example NCT00832091 for venous stasis ulcers, NCT00311766 for epidermolysis bullosa, NCT00598871 for corneal wounds, and NCT01311518 for acute myocardial infarction) document the seriousness of the clinical effort.811 The overriding methodological point for TB-500 specifically is that essentially none of this human work used the research-market fragment. The evidence pyramid is broad and reasonably tall for the parent protein but nearly empty at the fragment level, which is the single most important methodological caveat in the entire topic.
Safety and Tolerability in the Research Record
Safety data, like efficacy data, come overwhelmingly from thymosin beta-4 rather than from the marketed fragment, and the available human safety record for the parent protein is reassuring within its limits. In a randomized, placebo-controlled, single- and multiple-dose Phase 1 study, intravenous thymosin beta-4 was administered to healthy volunteers across ascending single doses spanning roughly 42 to 1260 mg, with dosing over a 14-day multiple-dose period.9 The peptide was reported to be safe and well tolerated, with adverse events infrequent and generally mild to moderate, and with no dose-limiting toxicities or serious drug-related adverse events observed even at the highest dose tested. Pharmacokinetics were dose-proportional, with a half-life that increased at higher doses.9 A separate first-in-human Phase 1 study of a recombinant human thymosin beta-4 in healthy volunteers likewise reported that adverse events were mild to moderate with no dose-limiting toxicities or serious adverse events.12 Across the topical dermal and ophthalmic Phase 2 trials, the tolerability picture was similar: safe and well tolerated at the doses studied, with no drug-related serious adverse events attributed to the peptide.810
Those are real, encouraging data, but they must be read within tight boundaries. The Phase 1 safety findings apply to a defined, pharmaceutical-grade formulation of full-length thymosin beta-4, administered by a controlled route, in a small number of screened healthy adults, over short study durations. They do not characterize long-term safety over months or years, do not reflect use in people with underlying disease, and do not address the research-market fragment “TB-500,” whose actual identity, purity, and contaminant profile in a given vial are typically unverified. Short-term tolerability in a controlled trial of a clean molecule is not a guarantee of safety for an unregulated laboratory chemical self-administered outside medical supervision.
Several theoretical safety considerations warrant explicit mention in the interest of honesty. Because thymosin beta-4 promotes cell migration and angiogenesis, a recurring conceptual concern in the literature is whether such activity could, in principle, be undesirable in the context of malignancy, since tumors also exploit migration and blood-vessel formation. This remains a hypothesis-level consideration rather than a demonstrated clinical harm, but it is a reasonable reason for caution and for excluding anyone with a cancer history from casual use. Additional generic risks attach to any injectable research peptide independent of the molecule itself: injection-site reactions, infection or abscess from non-sterile technique, immune or allergic responses to peptide or excipients, and exposure to endotoxin or synthesis-related impurities in material not manufactured to pharmaceutical standards. The parent protein’s clean Phase 1 record is meaningful, but it should not be transferred wholesale onto an unregulated fragment used in uncontrolled conditions.
The accurate summary is that thymosin beta-4 has shown a favorable short-term tolerability profile in the limited human trials conducted to date, that no serious drug-related toxicity signal emerged in those studies, and that this record nonetheless says little about the long-term safety of the marketed TB-500 fragment used outside a clinical setting. Absence of evidence of harm in a handful of small, short trials is not the same as evidence of long-term safety.
Handling and Reconstitution in a Research Context
Because TB-500 is supplied strictly as a research chemical rather than a medicine, handling considerations are framed here purely for laboratory accuracy and reproducibility, not as instructions for human use. Peptides of this class are typically distributed as a lyophilized (freeze-dried) white powder in a sealed vial, quantified in milligrams, and are reconstituted into solution before any in-vitro or animal-model work.
In a research setting, lyophilized peptide is generally reconstituted with sterile or bacteriostatic water added slowly down the inside wall of the vial rather than directly onto the powder, allowing the solid to dissolve gently without excessive foaming or shear, which can degrade fragile peptides. The vial is swirled, not vigorously shaken, until the solution is clear. The resulting concentration is a matter of simple arithmetic: total peptide mass divided by the volume of diluent added yields the concentration per unit volume, and getting that math right is the single most important step for any downstream measurement to be meaningful. A worked reconstitution walkthrough for this specific compound is maintained on the TB-500 dosage protocol page, and general dosing-math principles are covered in the site’s blend and stack references such as the KLOW dosage protocol guide.
Stability and storage matter because peptides are chemically delicate. Lyophilized TB-500 is typically most stable stored frozen and protected from light and moisture, while reconstituted solution is generally refrigerated and used within a limited window, since peptides in aqueous solution are more susceptible to hydrolysis, oxidation, and microbial contamination than the dry powder. Repeated freeze-thaw cycles of solution are usually avoided because they can promote aggregation and loss of activity. Using bacteriostatic rather than plain sterile water for solutions intended to be stored for more than a single use is a common laboratory practice, as the benzyl alcohol content inhibits microbial growth. These are standard peptide-handling conventions rather than anything unique to TB-500, and they exist to preserve the integrity of the material so that experimental results reflect the peptide’s actual behavior rather than artifacts of degradation.
Two points keep this section honest and appropriately bounded. First, none of the above should be read as endorsement or instruction for administering TB-500 to a human being; it describes bench handling of a research reagent. Second, the entire exercise of careful reconstitution and storage is undermined at the source if the vial’s contents are not what the label claims. Independent analyses of research-market peptides have repeatedly found discrepancies between labeled and actual content, including underfilled mass, degradation products, and, in the case of “TB-500” specifically, uncertainty about whether a given vial contains the short fragment, full-length protein, or a mixture. No amount of careful pipetting can correct for an unverified starting material, which is why identity and purity verification is the foundation of any rigorous research use.
Limitations and the Human-Evidence Gap
If a single idea should survive from this article, it is the size and shape of the gap between what is claimed for TB-500 and what has actually been demonstrated. That gap is not a minor caveat; it is the central fact of the topic.
Start with the fragment-versus-protein problem. The overwhelming majority of the encouraging research, cardiac protection, dermal and corneal healing, hair-follicle activation, neurological recovery, was conducted with full-length thymosin beta-4, frequently a pharmaceutical-grade formulation, not with the LKKTETQ fragment sold as “TB-500.”278 Every time that research is invoked to describe TB-500, an unvalidated assumption is smuggled in: that a seven-residue fragment reproduces the full activity of a 43-residue protein. That assumption may be partly true for actin binding and largely untested for everything else.
Next, consider the species-and-model gap. The most impressive tissue-repair results come from animal injury models with all the built-in optimism biases described earlier: young, uniform, healthy animals; clean, standardized, immediately treated injuries; short timelines; and small-animal physiology. The history of regenerative medicine is littered with interventions that produced beautiful rodent data and null human results, and thymosin beta-4’s own cardiac program, spectacular in mice, never delivering an approved human cardiac therapy despite a registered infarction trial, is a case study in exactly that pattern.711
Then there is the indication gap. Even the credible human data, the dermal-ulcer and dry-eye Phase 2 trials, addressed narrow, specific conditions with topical formulations applied directly to the injured surface.810 They provide essentially no evidence for the uses most people actually have in mind for TB-500: systemic acceleration of tendon, ligament, muscle, or joint recovery via injection. There are no completed controlled human trials demonstrating that TB-500, or even full thymosin beta-4, meaningfully speeds musculoskeletal injury healing in people. That specific, popular claim is supported by extrapolation and anecdote, not by human outcome data.
Finally, there is the quality-and-verification gap. Research-market peptides are not manufactured to pharmaceutical standards, are labeled for laboratory use only, and vary in identity, purity, and content between suppliers and even between batches. This means that even the extrapolated animal evidence cannot be cleanly applied, because the material a person actually obtains may not match the molecule that was studied. Anecdotal user reports, which fill the vacuum where trials should be, are additionally confounded by the placebo effect, by concurrent rest and rehabilitation, by the natural time course of healing, and by frequent co-administration of other compounds such as BPC-157, making it impossible to attribute any perceived benefit to TB-500 itself. The intellectually honest position is that TB-500 is a biologically plausible, mechanistically interesting, but clinically unproven research compound, and that anyone treating it as an established therapy is well ahead of the evidence.
Regulatory Status
The regulatory picture is unambiguous and worth stating plainly. TB-500 is not an approved drug. It has not been approved by the U.S. Food and Drug Administration, the European Medicines Agency, or any comparable regulator for any indication, in any country, for human use. It has no marketing authorization, no approved label, and no recognized therapeutic indication. It is sold and distributed as a research chemical, typically marked “for research use only, not for human consumption,” and that designation is a legal and scientific description of its actual status, not a marketing formality.
Full-length thymosin beta-4 has been the subject of legitimate, registered clinical investigation, appearing in ClinicalTrials.gov entries and progressing through Phase 1 and Phase 2 studies under formulations such as RGN-259, RGN-137, and RGN-352.8911 Investigational status is precisely that, however: it means a compound is being studied, not that it has been proven safe and effective and cleared for use. Being “in trials,” historically or currently, is not approval, and the parent protein never advanced to approved-drug status for tissue repair.
For athletes and anyone in tested sport, the anti-doping status is a separate and important layer. Thymosin beta-4 and its fragments fall under the World Anti-Doping Agency Prohibited List within category S2 (peptide hormones, growth factors, related substances, and mimetics), which is prohibited at all times, both in and out of competition.13 TB-500 attracted early anti-doping attention in part through its use in animal sport, and it is also prohibited in horse racing under racing-medication rules. The practical consequence is that use of TB-500 by a competitive athlete subject to WADA-code testing constitutes a doping violation and can result in sanctions, entirely independent of the drug-regulatory question.
Putting the layers together yields a clear compliance summary: TB-500 is an investigational research compound and is not approved as a medicine anywhere; the credible human research belongs to the full parent protein and did not reach approval; and the fragment is a banned substance in tested sport. None of this is a comment on the molecule’s scientific interest, which is real, but it is the essential legal and ethical context for any discussion of it. Anyone considering the compound outside a properly authorized research setting should understand that they are working with an unapproved substance of unverified quality and unproven human benefit.
Frequently Asked Questions
Is TB-500 approved by the FDA for healing or tissue repair?
No. TB-500 is not approved by the FDA or any other major regulator for any use. It is sold as a research chemical labeled for laboratory use only, not for human consumption. Full-length thymosin beta-4 has been studied in registered human trials, but investigational status is not approval, and neither the protein nor the TB-500 fragment ever reached approved-drug status for tissue repair.811
Is TB-500 the same thing as thymosin beta-4?
Not exactly, and the distinction matters a great deal. Thymosin beta-4 is the full 43-amino-acid protein. TB-500 is generally a synthetic fragment built around its actin-binding motif (Ac-LKKTETQ), and confusingly, some products sold as “TB-500” may actually contain the full protein instead.14 Because nearly all rigorous research used the full protein, findings do not automatically transfer to the fragment, and any such transfer is an assumption rather than a proven fact.
Does the research show TB-500 heals tendons or muscle in humans?
There are no completed controlled human trials demonstrating that TB-500 accelerates tendon, muscle, ligament, or joint healing. The most relevant human data for thymosin beta-4 come from narrow topical indications such as dermal ulcers and dry eye, not from systemic musculoskeletal repair.810 Claims about tendon and muscle recovery rest on animal and in-vitro data on the parent protein plus anecdote, which is not the same as human proof.
What is the strongest evidence that thymosin beta-4 works at all?
The most credible human signals are the Phase 2 ophthalmic trials, where thymosin beta-4 eye drops produced statistically significant improvements in ocular discomfort and corneal staining in severe dry eye, and the Phase 1 studies showing the intravenous protein was safe and well tolerated at high doses.910 These are genuine, respectable data, but they are small, indication-specific, and based on the full protein rather than the marketed fragment.
How does TB-500 compare with BPC-157?
They are mechanistically different peptides. BPC-157 has more direct animal evidence for tendon and ligament repair, while TB-500 (thymosin beta-4) is associated with actin regulation, systemic cell migration, and cardiac and dermal repair models.27 No head-to-head human trial has ever compared them, so claims that one is definitively better for recovery are not scientifically grounded, and the rationale for stacking them is theoretical.
Is TB-500 banned in sports?
Yes. Thymosin beta-4 and its fragments are prohibited at all times under category S2 of the WADA Prohibited List, and TB-500 is also banned in horse racing.13 Any athlete subject to WADA-code testing who uses TB-500 commits an anti-doping violation, independent of the drug-approval question.
What are the known safety concerns with TB-500?
In short human trials of the full protein, thymosin beta-4 was well tolerated with only mild-to-moderate adverse events and no serious drug-related toxicity, but those data are short-term, use pharmaceutical-grade material, and do not cover the unregulated fragment.912 Theoretical concerns include the implications of a pro-migration, pro-angiogenic molecule in the context of malignancy, plus generic injectable-peptide risks such as contamination, impurities, and unverified vial contents.
Why is the identity of TB-500 in a given vial uncertain?
Research-market peptides are not manufactured to pharmaceutical standards, and independent testing has repeatedly found discrepancies between labeled and actual content. For “TB-500” specifically, vials may contain the short fragment, full-length thymosin beta-4, or a mixture, with variable purity.1 This is why identity and purity verification is considered the foundation of any legitimate research use, since unverified material makes every downstream result and safety assumption unreliable.
References
- Goldstein AL, Hannappel E, Kleinman HK. Thymosin beta4: actin-sequestering protein moonlights to repair injured tissues. Trends Mol Med. 2005;11(9):421-429. PubMed 16099219. https://pubmed.ncbi.nlm.nih.gov/16099219/
- Morris DC, Chopp M, Zhang L, et al. Treatment of neurological injury with thymosin beta-4. PMC3471669. https://pmc.ncbi.nlm.nih.gov/articles/PMC3471669/
- Sosne G, Qiu P, Goldstein AL, Wheater M. Biological activities of thymosin beta4 defined by active sites in short peptide sequences. FASEB J. 2010;24(7):2144-2151. PubMed 20179146. https://pubmed.ncbi.nlm.nih.gov/20179146/
- Philp D, Goldstein AL, Kleinman HK. The actin binding site on thymosin beta4 promotes angiogenesis. PubMed 14500546. https://pubmed.ncbi.nlm.nih.gov/14500546/
- Ehrlich HP, Hazard SW III. Thymosin beta4 promotes dermal healing. Ann N Y Acad Sci. PubMed 27450738. https://pubmed.ncbi.nlm.nih.gov/27450738/
- Philp D, Nguyen M, Scheremeta B, et al. Thymosin beta4 increases hair growth by activation of hair follicle stem cells. FASEB J. 2004;18(2):385-387. PubMed 14657002. https://pubmed.ncbi.nlm.nih.gov/14657002/
- Bock-Marquette I, Saxena A, White MD, Dimaio JM, Srivastava D. Thymosin beta4 activates integrin-linked kinase and promotes cardiac cell migration, survival and cardiac repair. Nature. 2004;432(7016):466-472. PubMed 15565145. https://pubmed.ncbi.nlm.nih.gov/15565145/
- Study of Thymosin Beta 4 in Patients With Venous Stasis Ulcers (RGN-137). ClinicalTrials.gov NCT00832091. https://clinicaltrials.gov/study/NCT00832091
- Ruff D, Crockford D, Girardi G, Zhang Y. A randomized, placebo-controlled, single and multiple dose study of intravenous thymosin beta4 in healthy volunteers. Ann N Y Acad Sci. 2010;1194:223-229. https://onlinelibrary.wiley.com/doi/10.1111/j.1749-6632.2010.05474.x
- Sosne G, Dunn SP, Kim C. Thymosin beta4 significantly improves signs and symptoms of severe dry eye in a phase 2 randomized trial. Cornea. 2015;34(5):491-496. PubMed 25826322. https://pubmed.ncbi.nlm.nih.gov/25826322/
- A Study of the Safety and Efficacy of Injectable Thymosin Beta 4 for Treating Acute Myocardial Infarction. ClinicalTrials.gov NCT01311518. https://classic.clinicaltrials.gov/ct2/show/NCT01311518
- First-in-human, randomized, double-blind, single- and multiple-dose, Phase I study of recombinant human thymosin beta4 in healthy Chinese volunteers. PMC8419156. https://pmc.ncbi.nlm.nih.gov/articles/PMC8419156/
- World Anti-Doping Agency. The 2026 Prohibited List, Section S2 (Peptide Hormones, Growth Factors, Related Substances and Mimetics). https://www.wada-ama.org/en/prohibited-list
Disclaimer: This article is provided for educational and research-information purposes only and does not constitute medical advice, a treatment recommendation, or an endorsement of use. TB-500 is an investigational research compound that is not approved by the FDA, EMA, or any other regulator for human use, and it is prohibited in tested sport. Nothing here should be interpreted as a claim that TB-500 or thymosin beta-4 treats, cures, or prevents any disease or injury in humans. Any handling described refers strictly to laboratory research contexts. Consult a qualified healthcare professional regarding any health condition, and comply with all applicable laws and anti-doping regulations.