Prostamax is one of the many so-called “peptide bioregulators” that have migrated out of a specific Russian research lineage and into the international research-chemical market, where it is sold as a lyophilised powder and marketed loosely for “prostate health.” In its most rigorously defined form, Prostamax is a short synthetic peptide with the amino-acid sequence Lys-Glu-Asp-Pro (abbreviated KEDP) that belongs to the family of ultrashort peptides associated with Vladimir Khavinson and the St. Petersburg Institute of Bioregulation and Gerontology.1 It is conceived as the defined-sequence descendant of an older generation of bovine-prostate tissue extracts — clinically used in Russia under the names Prostatilen and Vitaprost — that were the actual subjects of most of the human clinical work in this area.6 Understanding Prostamax therefore means holding two separate things in mind at once: a modern, single-sequence research peptide with almost no independent literature of its own, and a much older extract-based product line with a real but geographically confined clinical history.
This distinction matters because a great deal of the marketing copy surrounding Prostamax quietly borrows credibility from the extract studies while presenting the synthetic tetrapeptide as if it were equally well characterised. It is not. The extracts were complex mixtures of peptides isolated from animal prostate tissue; the synthetic KEDP peptide is a single defined molecule. Data generated on one do not automatically transfer to the other, and the transfer is exactly where the honest reader should slow down. As with the pineal peptide Epithalon or the vascular tripeptide sold as Vesugen, the specific synthetic sequence marketed as Prostamax rests on a body of work that is dominated by a single research school, largely preclinical, and essentially unreplicated by independent Western laboratories.3
This article is an evidence-cautious explainer, not a protocol and not an endorsement. It walks through what Prostamax is claimed to be, the mechanism its originators propose, the actual level of the evidence, how it compares with related compounds, the laboratory models used to study it, what is and is not known about safety, how researchers handle the material, the substantial gap between animal work and human outcomes, and its regulatory status. Throughout, the aim is to describe the science plainly and to be candid when the science simply is not there. Prostamax is an experimental, unapproved research compound. Nothing here should be read as a claim that it treats, prevents, or cures any prostate disease.
What Prostamax Is and Where It Came From
Prostamax sits inside a Soviet- and Russian-era research tradition that begins in the 1970s, when Vladimir Khavinson and Vladimir Morozov described a way to isolate low-molecular-weight peptide fractions from animal tissues, which they termed “cytomedines.”2 The governing idea was that each organ produces its own set of short regulatory peptides that help maintain the function of that specific tissue, and that supplying a matching peptide fraction could, in their framework, help a corresponding organ restore normal activity. From this program came a whole catalogue of tissue-named products: thymus peptides (Thymalin), pineal peptides (Epithalamin, later the synthetic Epithalon), brain peptides (Cortexin), retinal peptides, and — relevant here — prostate peptides.
The first prostate-directed products in this lineage were extracts, not defined single molecules. Prostatilen is described as a purified polypeptide complex obtained from the prostate gland of young cattle, and it has been used in Russian urology for decades, later reformulated and marketed as Vitaprost in rectal-suppository and oral-tablet forms.6 These extract products, not Prostamax, are what most of the human clinical papers actually studied. When a vendor page says Prostamax “has 30 years of clinical use,” it is almost always describing this extract lineage rather than the synthetic KEDP peptide that is shipped in the vial.
The synthetic tetrapeptide Lys-Glu-Asp-Pro (KEDP) is the more recent, “designed” iteration. It follows the same design philosophy that produced Khavinson’s other ultrashort peptides: take a tissue-associated peptide motif, reduce it to a very short defined sequence, and manufacture it by solid-phase peptide synthesis so that every batch is a single, characterisable molecule rather than a biological extract.1 The logic is that a defined tetrapeptide is reproducible, patentable, free of the batch-to-batch variability of tissue extracts, and — in the originators’ theory — carries the “informational” core responsible for the tissue effect. Whether KEDP genuinely reproduces the biology of the older extracts is an open scientific question rather than an established fact.
There is a broader historical point that helps make sense of the whole category. The cytomedine program emerged in a specific scientific and institutional environment — Soviet military and gerontological medicine — where the emphasis was on practical, deployable interventions and where the publication ecosystem was largely domestic and in Russian. That context shaped the evidence in ways that still matter today: much of the foundational literature is difficult to access, is not indexed in the major English-language databases, and was produced before the modern conventions of pre-registration, blinding, and independent replication became standard. This does not make the work worthless, but it does mean that a Western reader encountering Prostamax for the first time is looking at the visible tip of a literature whose bulk is hard to inspect and even harder to independently verify. Enthusiastic vendor summaries tend to treat that inaccessibility as if it were depth; the more sober reading is that inaccessibility is itself a limitation.2
It is worth being precise about naming, because the market is inconsistent. “Prostamax” is a trade-style name applied by research-chemical vendors; it is not a compendial drug name in the United States or European Union. Different suppliers may attach the name to slightly different presentations, and some marketing conflates the synthetic peptide with the natural extract. The most defensible technical description is the one used on careful reference pages: Prostamax is a synthetic short peptide, sequence Lys-Glu-Asp-Pro, sold as a research-only lyophilised powder, typically in a 20 mg vial.1 Anyone evaluating the compound should confirm from a certificate of analysis exactly what sequence and purity they are actually looking at, because the label word “Prostamax” does not, by itself, guarantee a particular molecule.
The intended research context is prostate biology broadly: age-related prostate changes, chronic non-bacterial (abacterial) inflammation of the prostate, and the general “restore normal function” narrative common to the whole bioregulator category. Vendors frequently gesture at benign prostatic hyperplasia and chronic prostatitis, but it is important to separate the disease areas the extracts were studied in from the far thinner evidence base for the synthetic peptide. For readers exploring the broader family, our overview pages on Vesugen and Livagen describe two other Khavinson-class peptides that share this same “tissue-specific short peptide” framing, and the same evidentiary caveats apply to all of them.
The Molecular Mechanism Khavinson’s Group Proposes
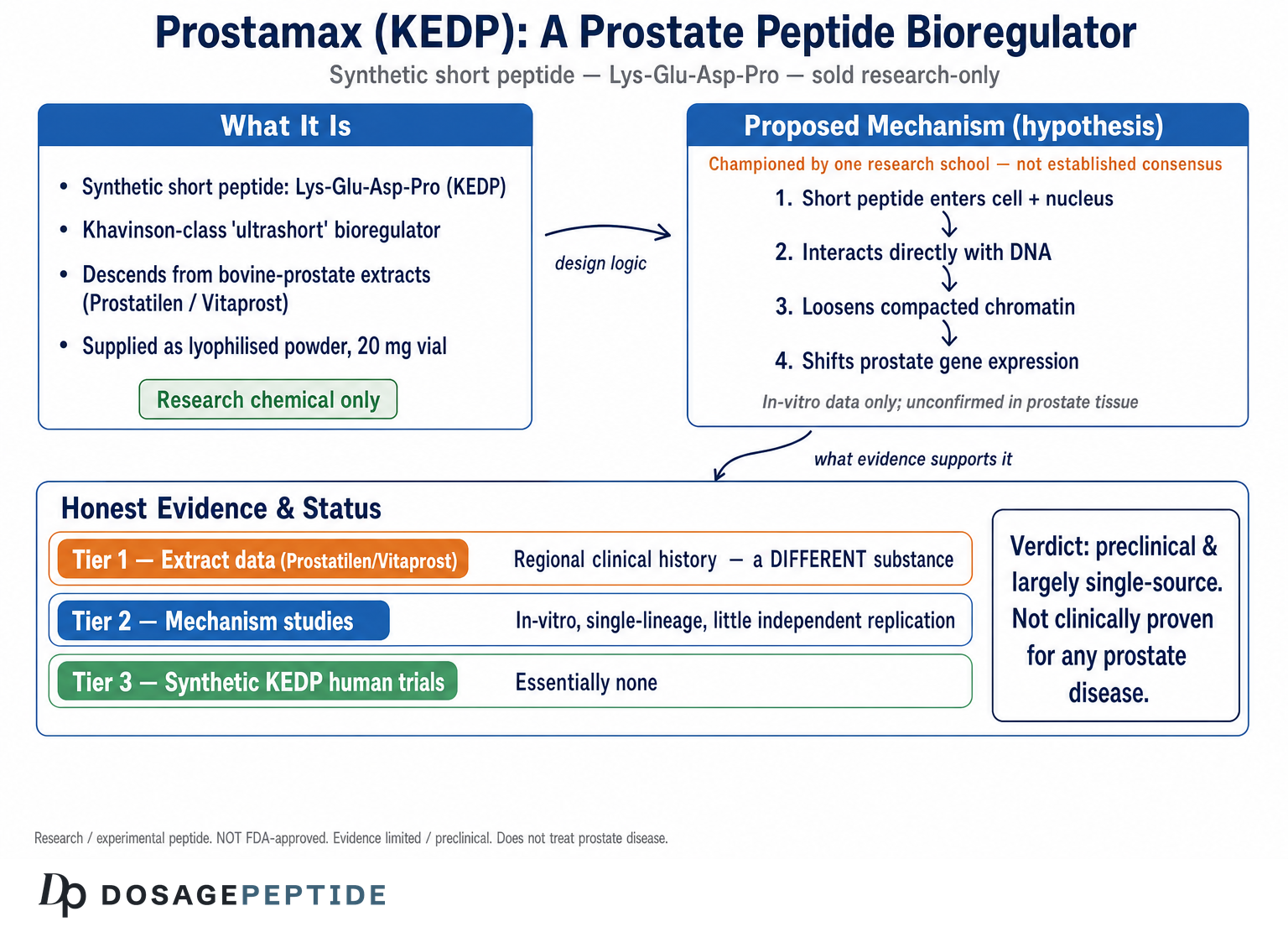
The proposed mechanism for Prostamax is inseparable from the general mechanistic hypothesis that Khavinson and colleagues advance for all of their ultrashort peptides, and it is important to flag from the outset that this is a hypothesis championed largely by one research school rather than an established, textbook consensus. The core claim is that di-, tri- and tetrapeptides are small enough to cross the cell membrane and the nuclear membrane, enter the nucleus, and interact directly with DNA — modulating gene expression rather than acting through a classical cell-surface receptor.3 On this model, a peptide like KEDP is not a hormone or a growth factor; it is described as an “epigenetic” signal that changes which genes are read in a target tissue.
Two more specific sub-claims sit underneath this. The first is a chromatin argument: that short peptides can loosen tightly packed, transcriptionally silent chromatin (heterochromatin), effectively “de-condensing” it and allowing previously suppressed genes to become active again.4 Papers from the group report that short peptides interact with DNA and with histone-associated structures, and that adding these peptides to cell cultures shifts the thermal denaturation behaviour of chromatin and changes the expression of particular genes.4 The narrative applied to Prostamax specifically is that, in prostate cells, this de-condensation restores expression of genes involved in normal prostate cell maintenance.
The second sub-claim is sequence specificity through complementarity. The group proposes that each short peptide sequence is “complementary” to particular DNA promoter regions, binding in the major groove via electrostatic and hydrogen-bond interactions, and thereby influencing a defined subset of genes rather than acting indiscriminately.3 This is the theoretical basis for the claim that KEDP is “prostate-specific” while a different sequence such as KED (Vesugen) is “vessel-specific.” Much of the supporting evidence here is molecular-docking and modelling work plus in-vitro assays generated within the same research lineage.3
An honest reader should register several caveats about this mechanistic story. It is internally coherent and has generated real publications, including systematic reviews of peptide effects on gene expression.3 But direct, independent, Western replication of the specific “peptide enters nucleus and docks onto a named promoter to change prostate gene expression” claim is essentially absent, and the leap from “a short peptide can bind DNA in a tube” to “this tetrapeptide reorganises prostate tissue in a living organism in a controlled, beneficial way” is very large. The chromatin-remodeling and gene-activation findings that vendors cite for Prostamax are frequently drawn from lymphocyte or generic cell-culture systems, not from prostate tissue in a diseased organism.4
A further complication is that the mechanistic model, as stated, is unusually permissive: because almost any tissue effect can be framed as “the peptide normalised gene expression,” the hypothesis is difficult to falsify with the kinds of experiments typically reported. A robust mechanistic claim makes specific, testable predictions — this peptide should upregulate these named genes, in this cell type, at this concentration, and blocking that interaction should abolish the downstream effect. Much of the Prostamax-adjacent literature instead offers correlative observations: a peptide was added, some genes changed, inflammation decreased. Correlation of that kind is a reasonable starting point, but it is a long way from a mechanistically closed loop, and it is the sort of evidence that independent replication is specifically designed to stress-test. That stress-testing has, for the most part, not happened for KEDP.3
It is also worth naming what the mechanism is not. There is no well-characterised, named prostate receptor for KEDP; there is no established pharmacokinetic model describing how an injected tetrapeptide distributes to, and is taken up by, human prostate tissue; and there is no consensus dose-response curve tied to a validated biomarker. The mechanism, in short, is a plausible and interesting hypothesis with supportive in-vitro data from its originators, not a settled account of how — or whether — the molecule produces meaningful effects on the prostate in humans. That gap between an elegant molecular story and demonstrated clinical effect recurs throughout the bioregulator field and is the single most important thing to keep in view.
What the Evidence Actually Shows (and Its Level)
The most useful way to think about the Prostamax evidence base is to sort it into three tiers, because collapsing them is exactly how the compound gets oversold. Tier one is the extract literature (Prostatilen/Vitaprost). Tier two is the general Khavinson short-peptide mechanistic literature. Tier three is direct, independent, human evidence specifically for the synthetic KEDP peptide. The tiers get progressively thinner, and tier three is very nearly empty.
Tier one is where the real clinical data live, and even here it is geographically and methodologically confined. The bovine-prostate extract Prostatilen, and its later formulation Vitaprost, accumulated decades of Russian urological use for chronic prostatitis and benign prostatic conditions.6 Published Russian trials report that oral Vitaprost roughly halved the probability of chronic abacterial prostatitis exacerbations over follow-up,7 and that in men with benign prostatic hyperplasia complicated by chronic bacterial prostatitis, combination regimens including the extract reduced symptom scores and residual urine volume.8 These are genuine clinical signals — but they describe a tissue-extract drug, mostly in studies conducted by investigators within the originating research tradition, and often without the double-blind, placebo-controlled, independently audited design that Western regulators expect.
| Evidence tier | What it covers | Strength | Applies to synthetic KEDP? |
|---|---|---|---|
| 1. Extract clinical data | Prostatilen / Vitaprost in chronic prostatitis and BPH | Moderate but regionally confined; largely non-blinded, single-lineage | Only by inference; different substance |
| 2. Short-peptide mechanism | In-vitro DNA binding, chromatin, gene-expression models | Consistent within one school; little independent replication | Partially; mostly non-prostate cell systems |
| 3. Synthetic KEDP human data | Controlled trials of Prostamax (KEDP) in men | Essentially absent | Directly — and this tier is empty |
Tier two is the mechanistic material discussed in the previous section: DNA-interaction studies, chromatin de-condensation assays, and gene-expression modelling.3,4 This work is real and indexed, but it is generic to the peptide platform rather than being a demonstration that Prostamax fixes a prostate problem. Reduced prostate inflammation, less vascular congestion, and less immune-cell infiltration are reported in animal models of prostatitis for prostate-directed peptide preparations,2,6 and this is genuinely the most on-target preclinical signal in the whole file. But animal-model inflammation data are hypothesis-generating, not confirmatory, and they cannot establish a clinical benefit.
Tier three — controlled human trials of the specific synthetic KEDP molecule marketed as Prostamax — is where candour is essential: there are, to date, no Western randomized controlled trials of synthetic KEDP, and no independent replication of its specific effects outside the originating institute.3 Searching the primary databases for the exact synthetic tetrapeptide returns essentially no independent, peer-reviewed human efficacy studies. That is a striking absence for a compound sold with confident health framing. The overall verdict is therefore straightforward and unflattering: the evidence level for Prostamax as a synthetic peptide is preclinical and largely single-source, and the more clinically substantial data belong to a related-but-different extract. Anyone who tells you Prostamax is “clinically proven” for prostate disease is, at best, importing the extract’s reputation onto a molecule that has not earned it.
Prostamax Versus Related Compounds
Placing Prostamax next to its neighbours clarifies both its family resemblance and how modest its own dossier is. The most instructive comparisons are with the extracts it descends from, with other Khavinson short peptides, and with the conventional agents actually used for prostate conditions.
Against Prostatilen and Vitaprost, the difference is composition and evidence. The extracts are multi-peptide biological preparations with a real, if regionally bounded, clinical track record in chronic prostatitis and BPH.6,7 Prostamax (KEDP) is a single defined peptide with a strong mechanistic narrative but little direct clinical validation. In other words, the extract has the data but not the molecular tidiness; the synthetic peptide has the molecular tidiness but not the data. Marketing tends to fuse the two into a single flattering picture, which is precisely the move to resist.
Against other Khavinson peptides, Prostamax is a mid-pack member of a large family that all share the same design logic and the same evidentiary limitations. The pineal peptide Epithalon (Ala-Glu-Asp-Gly) is probably the most-studied member and has a comparatively larger literature, including reviews of its proposed telomerase and circadian effects, yet even it lacks robust independent human outcome trials.9 The vascular tripeptide KED (Vesugen) is another relatively better-indexed sequence, but its clinical claims again trace back to the same investigators.3 Prostamax has less of a distinct literature than either of those, which is saying something. The table below sketches the family relationships without implying that any of them is a validated therapy.
| Compound | Sequence / type | Associated tissue | Relative evidence depth |
|---|---|---|---|
| Prostamax | Lys-Glu-Asp-Pro (KEDP), synthetic | Prostate | Thin; mostly extract-borrowed + mechanism |
| Prostatilen / Vitaprost | Bovine prostate peptide extract | Prostate | Largest in this niche; regionally confined |
| Vesugen | Lys-Glu-Asp (KED), synthetic | Vasculature | Modest; better-indexed than Prostamax |
| Epithalon | Ala-Glu-Asp-Gly (AEDG), synthetic | Pineal / systemic | Most-studied bioregulator; still preclinical-heavy |
| Livagen | Lys-Glu-Asp-Ala (KEDA), synthetic | Liver | Sparse |
Against conventional prostate medicine, the contrast is stark and worth stating plainly for perspective. Standard management of benign prostatic hyperplasia and of chronic prostatitis/chronic pelvic pain syndrome rests on agents and approaches with large, independent, blinded, regulator-reviewed trial programs — alpha-blockers and 5-alpha-reductase inhibitors for BPH, and multimodal symptom-directed strategies for chronic prostatitis, all classified within frameworks such as the NIH consensus categories of prostatitis.10 Prostamax has nothing remotely comparable. It should not be positioned as an alternative to evaluated care, and it does not belong in the same evidentiary sentence as approved therapies.
One additional comparison is worth making explicitly, because it is where the most consequential mistakes happen: Prostamax versus doing nothing but proper medical evaluation. For a man with prostate symptoms, the realistic alternatives are not “Prostamax versus another peptide” but “an unproven research chemical versus a clinical work-up that could identify a treatable and sometimes serious condition.” Framed that way, the opportunity cost of relying on Prostamax is not neutral. Symptoms attributed vaguely to “aging prostate” can reflect benign hyperplasia, infection, inflammation, or malignancy, and only the last of these is time-sensitive in a way that makes delay genuinely dangerous. No mechanistic elegance offsets the risk of substituting an unevaluated compound for a diagnostic process. This is the comparison the marketing never draws, and it is arguably the most important one.10
For readers mapping the wider landscape, our library page on Epithalon and our explainer on Ovagen, the liver bioregulator peptide illustrate the same pattern at work across the bioregulator category: coherent tissue-specific stories, a shared originating school, and a persistent shortage of independent human trials.
Research Models and Methodology
Because Prostamax has no meaningful independent clinical trial base, the “how it is studied” question is really a question about the preclinical and in-vitro methods used across the bioregulator platform, plus the extract-era animal and clinical work. Knowing the models is important, because the strengths and weaknesses of those models largely determine how much weight the resulting claims can bear.
The mechanistic backbone comes from cell-free and cell-culture systems. Researchers in the Khavinson lineage have used DNA-binding assays, thermal denaturation of DNA and chromatin, fluorescence and spectroscopic methods, and molecular docking to argue that short peptides interact with specific nucleotide sequences and alter chromatin state.3,4 Gene-expression readouts — sometimes via microarray or targeted expression panels — are then used to claim tissue-relevant transcriptional changes. These are legitimate laboratory techniques, and they can convincingly show that a peptide can bind DNA or shift gene expression in a dish. Their limitation is external validity: a binding event in a cuvette or a transcript change in cultured lymphocytes does not establish a coordinated, beneficial physiological effect in an intact prostate.
The most prostate-relevant preclinical work sits in animal models of prostatitis and age-related prostate change. Here, prostate-directed peptide preparations have been reported to reduce inflammatory infiltration, oedema, and vascular congestion, and to support tissue architecture in rodent models of chronic abacterial prostatitis.2,6 Rodent prostatitis models are the standard way to probe candidate anti-inflammatory prostate agents, and a reduction in histological inflammation is a reasonable, on-target endpoint. But several methodological cautions apply: much of this work uses extract preparations rather than the isolated KEDP peptide; group sizes and blinding are frequently not reported to modern standards; and the endpoints are histological and biochemical surrogates rather than symptomatic or functional outcomes that matter to patients.
| Model type | Typical endpoints | What it can show | What it cannot show |
|---|---|---|---|
| Cell-free DNA / chromatin assays | Binding, denaturation shifts | A peptide can physically interact with DNA | That this changes prostate physiology |
| Cell culture (often lymphocytes) | Gene expression, proliferation | Transcriptional changes are possible | Tissue-specific, in-vivo benefit |
| Rodent prostatitis models | Inflammation, oedema, histology | On-target anti-inflammatory signal | Human symptom or disease outcomes |
| Extract clinical series | Symptom scores, exacerbations | Possible clinical benefit of the extract | Anything about synthetic KEDP directly |
A recurring methodological theme across all tiers is the single-lineage problem. Independent replication — different investigators, different institutions, different countries, ideally pre-registered and blinded — is the mechanism by which science filters robust findings from artefacts and enthusiasm. For Prostamax specifically, that independent replication layer is largely missing.3 This is not an accusation of misconduct; it is a statement about the maturity of the evidence. Findings that have been reproduced only within the group that generated them, using surrogate endpoints, in models that do not use the exact marketed molecule, are precisely the findings that responsible readers treat as provisional.
It is also worth understanding why the field has not simply run the obvious study. A well-designed, independent, placebo-controlled trial of synthetic KEDP in men with, say, chronic abacterial prostatitis — with validated symptom-score endpoints and adequate follow-up — would settle much of the uncertainty in one stroke. Several structural factors explain the absence of such trials: the compound is unpatentable in its basic sequence and therefore commercially unattractive to sponsors who would fund large trials; the originating institutions publish largely within their own ecosystem; and the research-chemical market can sell the product profitably without ever generating clinical evidence, since “research use only” labelling sidesteps the requirement to prove anything. The result is a self-perpetuating situation in which demand exists, product exists, mechanistic papers exist, and the one thing that would actually resolve the question — rigorous independent human trials — has no natural funder. Readers should recognise that the evidence gap is structural, not merely a matter of the science being “early.”
Methodology also shapes how one should read vendor claims. When a product page says Prostamax “reduces prostate inflammation” or “regenerates prostate tissue,” the underlying citations, where they exist at all, almost always point to extract animal studies or to platform-level in-vitro work — not to controlled human trials of the peptide in the vial. Recognising which model a claim comes from is the single most useful skill for evaluating this compound honestly.
Safety and Tolerability Signals
Safety discussion for Prostamax has to begin with an uncomfortable admission: there is no adequate, independent human safety dataset for the synthetic KEDP peptide, so any statement about its tolerability is an inference rather than a demonstrated fact. What exists is indirect — general observations from the broader ultrashort-peptide class, and tolerability notes from the older prostate extracts — and neither of those can substitute for controlled safety evaluation of the actual compound at the doses and routes people use.
From the class-level literature, ultrashort peptides are often described by their proponents as low-toxicity because they are small, are composed of standard amino acids, and are used at low absolute masses.2 The extract products (Prostatilen/Vitaprost) have a long marketed history in Russia with a generally benign reported tolerability profile in that setting.6 These points are frequently cited to imply that Prostamax “is safe.” That inference is weak for several reasons: extract tolerability does not certify the synthetic peptide; a long marketing history is not the same as rigorous pharmacovigilance; and “low toxicity in a rodent or in short Russian clinical use” does not characterise the risks of self-administered injectable material of uncertain purity used outside medical supervision.
The more decision-relevant risks for Prostamax as it actually circulates are not really about the peptide’s intrinsic pharmacology at all — they are about the research-chemical supply chain and the route of administration. Injectable products reconstituted and used outside a controlled setting carry generic, well-established hazards: contamination and endotoxin from non-sterile handling, infection or injection-site reactions, dosing errors from home reconstitution math, and — importantly — impurities or mislabelling, since research-chemical vendors are not held to pharmaceutical manufacturing standards. A certificate of analysis mitigates but does not eliminate these concerns, and identity/purity can vary between suppliers selling under the same “Prostamax” name.
| Risk domain | What is known | Honest assessment |
|---|---|---|
| Intrinsic peptide toxicity | No adequate independent human data for KEDP | Unknown; class claims of low toxicity are unverified for this molecule |
| Product quality | Unregulated market; purity varies by supplier | Material risk; COA advisable but not a guarantee |
| Sterility / injection | Generic hazards of non-clinical injectable use | Real and preventable-only-in-part outside medical settings |
| Drug interactions | Not characterised for KEDP | Unknown; no interaction studies exist |
| Long-term effects | No long-term human follow-up for the peptide | Unknown; a genuine data gap, not a clean bill of health |
There is also a category-specific concern worth naming for anything marketed around the prostate: the prostate is an organ where the most important conditions — benign hyperplasia, prostatitis, and prostate cancer — can present with overlapping symptoms, and where cancer specifically requires timely, evidence-based evaluation. A mechanism narrative built around “restoring normal prostate cell function” and “stimulating tissue activity” should prompt caution rather than reassurance, because effects on cell proliferation in prostate tissue are exactly the kind of thing that has not been safety-characterised for this peptide. The absence of data here is not neutral; it is a reason for restraint.
The correct summary is therefore not “Prostamax appears safe.” It is: the intrinsic safety of synthetic Prostamax in humans is uncharacterised, the supply-chain and injection risks are real, and the most prostate-relevant long-term questions are simply unstudied. Absence of reported harm in a thin, non-independent record is not evidence of safety.
Handling and Reconstitution in a Research Context
This section describes how the material is handled in laboratory and research settings for completeness and for reader safety literacy; it is explicitly not dosing guidance, and it is not a suggestion that anyone administer this compound. Prostamax is supplied strictly as a research chemical, “not for human consumption,” and that framing should govern every handling decision.
Physically, Prostamax ships as a white lyophilised (freeze-dried) powder in a sealed glass vial, most commonly labelled at 20 mg, and typically stored refrigerated and protected from light until use, with the sealed lyophilised powder being the most stable form for longer-term storage.1 Lyophilised short peptides are generally more stable as dry powder than in solution, which is why reconstitution is done shortly before use in a research protocol and the reconstituted solution is kept cold and used within a limited window. As with the rest of the bioregulator class, the reconstitution medium described in research write-ups is bacteriostatic water, chosen because the benzyl alcohol it contains suppresses microbial growth in a multi-use vial.
Reconstitution in a research context is simply a dilution calculation: a volume of sterile diluent is added down the vial wall (not sprayed directly onto the powder), the vial is swirled rather than shaken to avoid shearing the peptide and generating foam, and the resulting concentration is powder mass divided by diluent volume. For a 20 mg vial, adding a given volume of bacteriostatic water yields a proportional concentration — the arithmetic is the same for any peptide and is covered generically in our peptide reconstitution and calculation resources rather than repeated as a protocol here. The general concepts of concentration, drawing accuracy, and vial handling are described in a compound-neutral way in the dosage and reconstitution reference library, and the compound-specific reference sheet lives on the Prostamax dosage protocol page.
Several handling caveats deserve emphasis precisely because the material is unregulated. First, identity and purity are only as trustworthy as the accompanying certificate of analysis; without third-party mass-spectrometry and HPLC data, the vial’s true contents are unverified. Second, sterility cannot be assumed — reconstitution should use aseptic technique, and even bacteriostatic diluent does not make a non-sterile process safe. Third, lyophilised peptides are hygroscopic and light- and heat-sensitive; repeated warming, freeze-thaw cycling of solutions, and prolonged room-temperature exposure degrade them. Fourth, accurate low-volume measurement is genuinely error-prone, and reconstitution math mistakes are one of the most common and consequential errors in amateur handling.
None of this handling detail should be read as normalising human use. The reason to understand reconstitution and storage is to be an informed reader of the research literature and to recognise how much can go wrong outside a controlled laboratory — not to enable self-experimentation with a compound whose human safety and efficacy are unestablished. In any legitimate research setting, work with a material like this would occur under institutional oversight, with proper documentation, and with no assumption that laboratory findings translate to human benefit.
Limitations and the Human-Evidence Gap
The single most important thing to understand about Prostamax is the size and character of the gap between its marketing and its evidence. This section names that gap directly, because it is easy to lose it amid the confident mechanistic language that surrounds the compound.
The first limitation is the substance-substitution problem. Most of the credible clinical signal in this niche belongs to bovine-prostate extracts, not to the synthetic KEDP peptide sold as Prostamax.6,7,8 These are not interchangeable. The extract is a complex mixture; the peptide is one molecule. Presenting the extract’s clinical history as if it validated the synthetic peptide is a category error, and it is the most common way Prostamax is oversold.
The second limitation is the single-lineage problem. Nearly all of the mechanistic and clinical claims for the bioregulator platform originate from, or are closely tied to, one research school.1,3 Independent replication by unaffiliated laboratories — the ordinary immune system of science against error and bias — is largely absent for the specific Prostamax molecule. Findings that have not survived independent, blinded reproduction are provisional by definition, however internally consistent they appear.
The third limitation is the surrogate-endpoint problem. The preclinical data that do exist rely on binding assays, gene-expression readouts, and rodent histology.3,4 These are hypothesis-generating surrogates. They can suggest a plausible pathway; they cannot demonstrate that a man with a prostate condition experiences a meaningful, durable, safe benefit. The chain from “peptide binds DNA in vitro” to “clinically useful prostate outcome in humans” has many missing links, and none of the missing links has been filled by controlled human trials of the compound.
| Question a patient would care about | State of evidence for synthetic Prostamax |
|---|---|
| Does it improve urinary symptoms in men? | No controlled human trials of KEDP; unknown |
| Does it reduce prostatitis symptoms durably? | Only extract data exist; peptide unproven |
| Is it safe over months or years? | No long-term human data; unknown |
| How does it compare to approved therapy? | No head-to-head data; not comparable in evidence |
| What is the right dose? | No validated human dose-response; unknown |
The fourth limitation is the pharmacology gap. There is no established human pharmacokinetic profile for injected KEDP — no clear picture of absorption, distribution to prostate tissue, metabolism, or elimination — and no validated biomarker to titrate against. Without that, even the concept of a “correct dose” is undefined for humans. The figures that circulate in protocols are conventions borrowed across the peptide class, not values derived from human dose-finding studies.
Taken together, these limitations mean Prostamax should be understood as an early-stage experimental compound with an interesting hypothesis and a conspicuously thin human record. It has not been shown to treat benign prostatic hyperplasia, chronic prostatitis, prostate cancer, or any other prostate disease, and it should not be used as a substitute for evaluation and care by a qualified clinician. Men with prostate symptoms — urinary changes, pelvic pain, or anything raising concern about cancer — need proper medical assessment, not an unapproved peptide.
Regulatory Status
Prostamax has no marketing authorisation as a medicine in the major Western regulatory systems, and its legal character is that of an unapproved research chemical rather than an approved drug or a lawful dietary supplement. This is not a technicality; it defines what is and is not known, and it defines what claims may lawfully be made.
In the United States, the synthetic KEDP peptide marketed as Prostamax is not an FDA-approved drug for any indication. It has not been through the investigational-new-drug and new-drug-application process that generates the independent efficacy and safety record required for approval, which is precisely why the honest evidentiary verdict above is “preclinical and unreplicated.” It is also not a recognised dietary-supplement ingredient — injectable peptides of this kind fall outside the dietary-supplement framework — so it cannot lawfully be sold for human use as a supplement either. In practice it circulates through the research-chemical channel, labelled “for research use only, not for human consumption,” a designation that exists precisely because the material has not been evaluated or authorised for people. The FDA has, more broadly, scrutinised many peptides sold through compounding and research channels, and several peptides have been flagged as not meeting the standards for use in compounded human drugs.11
In the European Union, the situation is analogous: there is no EMA authorisation for a synthetic KEDP prostate peptide, and no approved medicinal product corresponds to the “Prostamax” research compound. The extract lineage (Prostatilen/Vitaprost) has a regulatory and clinical history primarily within Russia and some neighbouring markets;6 that regional status does not confer approval elsewhere and, again, does not apply to the synthetic peptide.
The regulatory framing has direct consequences for how the compound should be discussed. Because it is unapproved, no seller may lawfully claim it diagnoses, treats, cures, or prevents any prostate disease, and readers should treat any such claim as a red flag rather than as information. “Research use only” is not a marketing flourish; it is a statement that the compound lacks the demonstrated safety and efficacy that approval requires. It also means the ordinary consumer protections that attach to approved medicines — manufacturing standards, mandated adverse-event reporting, dosing labels validated in humans — do not apply.
For orientation, it helps to compare the categories. Approved prostate therapies sit in a fully regulated space with independent trial evidence and pharmacovigilance. Traditional/regional extract products occupy a middle zone with regional authorisation and some clinical history. Prostamax, as a synthetic research peptide, sits in the least-regulated tier, with the least independent evidence and the fewest protections. That placement is the most reliable single summary of where the compound actually stands. Readers who want to see how the same regulatory pattern recurs across the family can compare the framing on our Livagen and Vesugen reference pages, both of which carry the identical “research-only, unapproved” status.
Frequently Asked Questions
Is Prostamax an FDA-approved treatment for prostate problems?
No. Prostamax is not approved by the FDA (or the EMA) for any indication. It is sold as a research chemical labelled “not for human consumption,” and it has not completed the clinical trials that approval requires.11 It should not be used as a treatment for benign prostatic hyperplasia, prostatitis, prostate cancer, or any other condition, and men with prostate symptoms should be evaluated by a qualified clinician using established, evidence-based care.
What exactly is Prostamax — an extract or a synthetic peptide?
The name is used loosely, which is part of the confusion. The most defensible technical description of Prostamax is a synthetic short peptide with the sequence Lys-Glu-Asp-Pro (KEDP), part of the Khavinson family of ultrashort “bioregulator” peptides.1 It is conceptually descended from older bovine-prostate tissue extracts (Prostatilen/Vitaprost), but the extract and the synthetic peptide are different substances, and most of the clinical data belong to the extracts, not to the synthetic peptide.6
Does Prostamax actually work for prostate health?
There is no good evidence that the synthetic Prostamax peptide works for prostate health in humans. There are no independent, controlled human trials of KEDP for any prostate outcome.3 The clinical signals that vendors cite generally come from the related tissue extracts studied mostly in Russia,7,8 or from platform-level laboratory experiments on gene expression that do not demonstrate a real-world benefit.4 The honest answer is: unproven.
How is Prostamax supposed to work at the molecular level?
Its originators propose that short peptides enter cells and the nucleus and interact with DNA, loosening compacted chromatin and changing which genes are expressed in a tissue-specific way — an “epigenetic” model rather than classical receptor signalling.3,4 This is an interesting hypothesis with supportive in-vitro data from one research school, but it has not been independently confirmed for the prostate, and a molecular mechanism in a dish does not prove a clinical effect in a person.
Is Prostamax safe?
Its safety in humans is not established. There is no adequate, independent human safety dataset for the synthetic KEDP peptide, so claims that it is “safe” are inferences, not demonstrated facts. In addition, because it is an unregulated injectable research chemical, there are real supply-chain risks (variable purity, possible contamination) and injection risks that exist regardless of the peptide itself. The most prostate-relevant long-term questions are simply unstudied.
How does Prostamax compare with Vitaprost or Prostatilen?
Vitaprost and Prostatilen are bovine-prostate peptide extracts with a decades-long, if regionally confined, clinical history in chronic prostatitis and BPH.6,7 Prostamax is a single synthetic peptide with a strong mechanistic story but little direct clinical data. The extracts have more human evidence; the synthetic peptide has more molecular definition. They are not interchangeable, and the extract’s history does not validate the synthetic peptide.
Can Prostamax treat or prevent prostate cancer?
No, and this is important: there is no evidence that Prostamax treats or prevents prostate cancer, and a mechanism centred on stimulating prostate cell activity has not been safety-characterised in that context. Prostate cancer requires timely, specialist, evidence-based evaluation and care. Using an unproven peptide in place of proper assessment could be harmful by delaying diagnosis.
Where does the “500 mcg” figure some sources mention come from?
Figures like that are conventions carried across the ultrashort-peptide class rather than values derived from human dose-finding studies of Prostamax specifically. Because there is no validated human pharmacokinetic profile or dose-response data for KEDP, there is no established “correct” human dose. Any number circulating in protocols should be read as a research-community convention, not as evidence-based dosing.
References
- Khavinson VK. Peptides and Ageing. Neuroendocrinology Letters. 2002;23(Suppl 3):11-144.
- Khavinson VK, Kuznik BI, Ryzhak GA. Peptide bioregulators: a new class of geroprotectors. Report of analytical research. Advances in Gerontology. 2013. Available at: https://khavinson.info/assets/files/2013-Khavinson_Kuznik.pdf
- Khavinson V, Popovich I, Linkova N, et al. Peptide Regulation of Gene Expression: A Systematic Review. Molecules. 2021;26(22):7053. doi:10.3390/molecules26227053. PMID: 34834147.
- Fedoreyeva LI, Kireev II, Khavinson VKh, Vanyushin BF. Short Peptides Regulate Gene Expression. Bulletin of Experimental Biology and Medicine. 2016. doi:10.1007/s10517-016-3596-7
- Khavinson VK, Linkova NS, Diatlova AS, Trofimova SV. Peptide Regulation of Cell Differentiation. Stem Cell Reviews and Reports. 2020.
- Kuzmin IV, Borovets SYu, Gorbachev AG, Al-Shukri SKh. Prostatic bioregulatory polypeptide prostatilen: pharmacological properties and 30-year experience of clinical application in urology. Urology Reports (St. Petersburg). Eco-Vector. Available at: https://journals.eco-vector.com/uroved/article/view/42472
- Lopatkin NA, et al. Administration of oral vitaprost for prevention of exacerbations of chronic abacterial prostatitis. Urologiia. 2009. PMID: 19432231.
- Treatment of prostatic adenoma with concomitant chronic bacterial prostatitis (vitaprost). Urologiia. PMID: 21500490.
- Overview of Epitalon — Highly Bioactive Pineal Tetrapeptide with Promising Properties. PMC. 2024. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11943447/
- Krieger JN, Nyberg L Jr, Nickel JC. NIH consensus definition and classification of prostatitis. JAMA. 1999;282(3):236-237.
- U.S. Food and Drug Administration. Bulk Drug Substances Used in Compounding Under Section 503A of the FD&C Act. Available at: https://www.fda.gov/drugs/human-drug-compounding/bulk-drug-substances-used-compounding-under-section-503a-fdc-act
Educational and research-use disclaimer. This article is provided for educational and informational purposes only and describes an experimental, unapproved research compound. Prostamax is not approved by the FDA, the EMA, or any comparable regulator for the diagnosis, treatment, cure, or prevention of any disease, and it is sold and handled strictly as a research chemical that is not for human consumption. Nothing here is medical advice, a treatment recommendation, or a dosing protocol, and nothing here should be used to guide self-experimentation. The available evidence for synthetic Prostamax (KEDP) is limited, largely preclinical, and drawn mostly from a single research lineage without independent replication or controlled human trials; claims of prostate-health benefit are unproven. Men with urinary symptoms, pelvic pain, or any concern about prostate disease — including prostate cancer — should seek evaluation and care from a qualified, licensed healthcare professional and should not substitute an unapproved peptide for evidence-based medical assessment. Always comply with the laws and institutional regulations that apply in your jurisdiction.