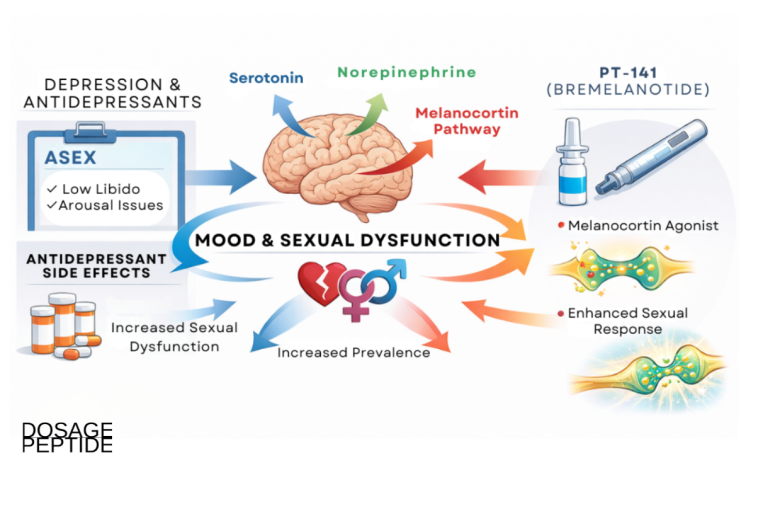
PT-141, known generically as bremelanotide, occupies an unusual position among research peptides: unlike most compounds studied only in cell cultures or animal models, it carries a genuine clinical evidence base and an approved human indication. As a synthetic melanocortin receptor agonist that acts centrally within the brain rather than peripherally on blood vessels, it offers a mechanistically distinct approach to sexual motivation, one that intersects with the same neural circuitry that chronic stress and hypothalamic-pituitary-adrenal (HPA) axis activation are known to disrupt. This article examines what the peptide actually is, how its melanocortin mechanism links to stress-sensitive motivation circuits, what the clinical trials genuinely demonstrated, and where the “stress-induced sexual motivation” framing is supported by evidence versus where it remains speculative.
Because sexual desire is generated centrally, in dopaminergic and melanocortinergic circuits of the hypothalamus and limbic system, a compound that engages those circuits invites the question of whether it can address desire deficits that arise specifically from stress rather than from vascular, hormonal, or primary mood pathology. The honest answer, developed throughout this piece, is that the mechanistic plausibility is real and the human safety and efficacy data for hypoactive sexual desire disorder (HSDD) are substantial, but no trial has yet been designed to test a discrete “stress-induced” indication.
What Is PT-141 (Bremelanotide) and What Is Its Regulatory Status?
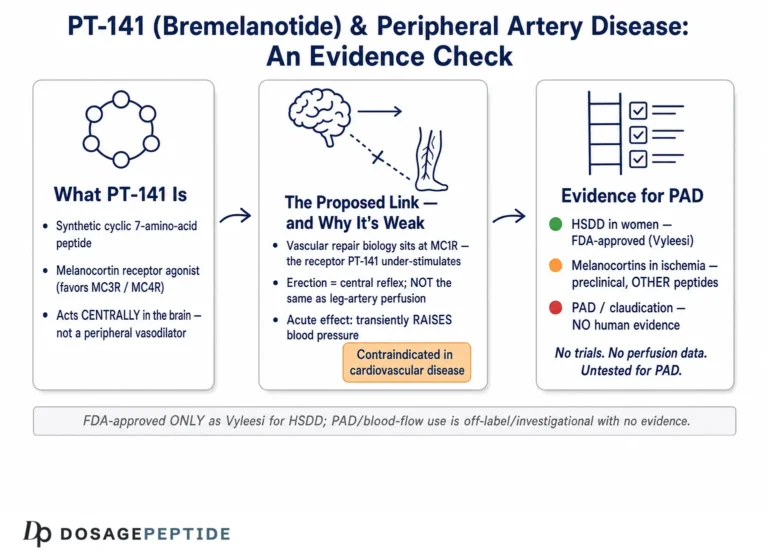
PT-141 is a synthetic cyclic heptapeptide analogue of alpha-melanocyte-stimulating hormone (alpha-MSH). It is a metabolite of Melanotan II and functions as a non-selective agonist across the melanocortin receptor family, with functional activity at the melanocortin-3 (MC3R) and melanocortin-4 (MC4R) receptors considered most relevant to its effects on sexual arousal and motivation.[1] The generic name assigned to the compound is bremelanotide, and understanding that PT-141 and bremelanotide are the same molecule is essential to reading its literature accurately, because the clinical and regulatory record is filed under the generic name.
Bremelanotide is not merely an investigational research chemical. On June 21, 2019, the United States Food and Drug Administration approved it under the brand name Vyleesi for the treatment of acquired, generalized hypoactive sexual desire disorder (HSDD) in premenopausal women, characterized by low sexual desire that causes marked distress or interpersonal difficulty and is not attributable to a co-existing medical or psychiatric condition, relationship problems, or medication effects.[2] This approval places bremelanotide in a small category of peptides with a rigorously characterized human efficacy and safety profile.
The specificity of the approved indication is worth reading closely because each qualifier carries meaning. “Acquired” means the low desire developed after a period of normal function, distinguishing it from lifelong low desire. “Generalized” means the deficit is not limited to a particular partner or situation. And the requirement that the low desire cause “marked distress” is what elevates a personal characteristic into a clinical disorder: a person with low desire who is untroubled by it does not have HSDD. These boundaries were not incidental; they defined the population studied in the pivotal trials and therefore define the population in whom efficacy was actually demonstrated. Understanding them is the difference between reading the evidence accurately and over-generalizing it.
Approved Use Versus Investigational Use
The distinction between what bremelanotide is approved for and what it has merely been studied for is critical and frequently blurred. The approved indication is narrow and specific: acquired, generalized HSDD in premenopausal women, administered as a 1.75 mg subcutaneous injection on an as-needed basis at least 45 minutes before anticipated sexual activity, with no more than one dose in 24 hours and no more than eight doses per month.[2]
Bremelanotide has also been investigated for male erectile dysfunction (ED) and for female sexual arousal disorder, but it is not approved for either male ED or for any stress-related indication. Its earliest human studies used an intranasal formulation for ED; that route was ultimately abandoned in favor of subcutaneous delivery. Any framing of PT-141 as a treatment for “stress-induced sexual motivation disorders” describes a research hypothesis, not an approved use. For readers examining research-scale material, the practical dosing context is documented separately in the PT-141 10 mg vial dosage protocol, which is intended for laboratory reference rather than clinical guidance.
Why the Distinction From Melanotan II Matters
PT-141 is structurally related to Melanotan II but is not identical, and the pharmacological difference is meaningful. Melanotan II is a broader, less-refined melanocortin agonist marketed illicitly for tanning; bremelanotide was developed specifically to exploit the sexual-motivation effects mediated through central melanocortin receptors while being deployed as a defined, on-demand therapeutic rather than a chronic tanning agent.[1] The two compounds are compared in more detail in a later section and in the combined Melanotan II and PT-141 dosage protocol.
The Development History Behind the Approval
The path from laboratory concept to approved product is instructive because it explains many of the compound’s defining features. PT-141 emerged from a program aimed at harnessing the sexual-behavior effects of alpha-MSH that had been observed for decades but were considered clinically intractable because the parent hormone was too broadly active and too short-lived to be useful. Investigators recognized that the sexual effects of melanocortin peptides were mediated centrally, through receptors in the brain, rather than peripherally, which distinguished this class from every other approach to sexual dysfunction then in development. That insight defined the entire subsequent research program: rather than trying to improve peripheral blood flow, the goal became to selectively engage the central receptors responsible for sexual motivation.
The early clinical development pursued an intranasal spray for erectile dysfunction, a route chosen for convenience and rapid onset. When that formulation produced clinically meaningful erectile responses but also elevated blood pressure more than was acceptable for an on-demand sexual medicine, the developers pivoted twice: away from the nasal route toward subcutaneous injection, and away from the male ED indication toward female HSDD, where the unmet need was greater and no comparable central agent existed. This history matters because it explains why the approved product is a subcutaneous injection for women rather than a nasal spray for men, and why the compound’s cardiovascular signal remains its most closely watched safety attribute. It also underscores that the “sexual motivation” framing is not marketing language layered onto a vascular drug; it is the founding mechanistic premise of the entire program.
How Does the Melanocortin System Drive Central Sexual Motivation?
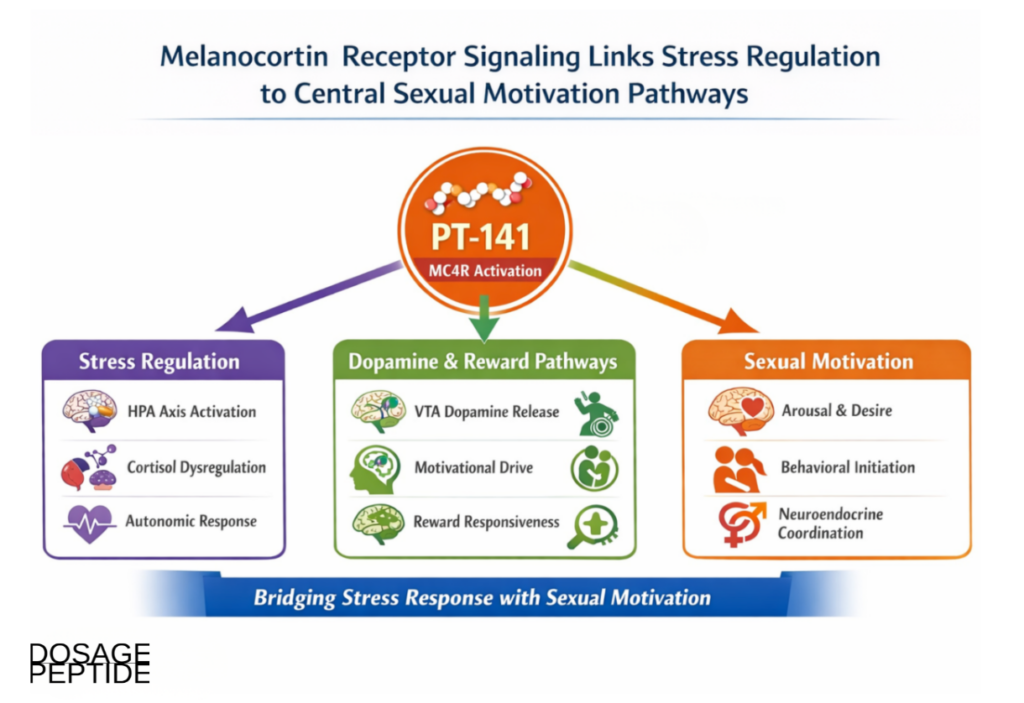
To understand why PT-141 is discussed in the context of motivation rather than mechanics, one must understand where it acts. The melanocortin system is an ancient neuroendocrine signaling network built around five G-protein-coupled receptors (MC1R through MC5R) and their endogenous ligands, the melanocortin peptides derived from proopiomelanocortin (POMC). Within the brain, MC3R and MC4R are the dominant subtypes, and MC4R in particular is densely expressed in hypothalamic and limbic structures that govern appetite, autonomic tone, and sexual behavior.
Where in the Brain PT-141 Acts
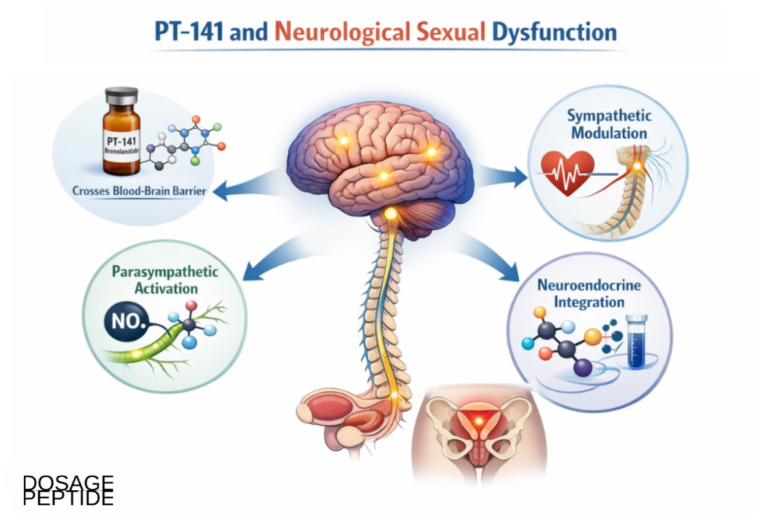
Foundational preclinical work established that systemic administration of PT-141 activates neurons in the hypothalamus, demonstrated by increased c-Fos immunoreactivity (a marker of neuronal activation), and produces penile erection in rats and non-human primates through a centrally initiated pathway rather than a direct vascular action.[1] The key regions implicated are the paraventricular nucleus and the medial preoptic area of the hypothalamus, both of which are integrative hubs where hormonal, autonomic, and motivational signals converge to shape sexual behavior.
When bremelanotide binds MC4R on these neurons, it activates a Gs-coupled cascade that raises intracellular cyclic AMP (cAMP), changing neuronal firing patterns in circuits that initiate the motivational, or “wanting,” component of sexual arousal. This is distinct from the reflexive, peripheral component that governs genital blood flow.
The Dopamine Link
The bridge between melanocortin signaling and motivation is dopamine. Activation of hypothalamic MC4R populations modulates downstream dopaminergic neurotransmission in mesolimbic reward circuits that originate in the ventral tegmental area and project to the nucleus accumbens and other forebrain targets. Dopamine release in these pathways generates incentive salience, the neural currency of desire and approach behavior, which is conceptually separable from the physical arousal response.
This dopaminergic coupling is why bremelanotide is framed as acting on sexual motivation specifically. It does not directly dilate blood vessels or raise circulating sex hormones; instead, it nudges the reward circuitry that decides whether a sexual stimulus is worth pursuing. Readers unfamiliar with terms such as incentive salience, MC4R, or POMC can consult the site peptide research glossary for concise definitions.
The Wanting-Versus-Liking Distinction
A concept from affective neuroscience clarifies why a motivation-targeting compound is conceptually distinct from a performance-targeting one. Reward researchers separate “wanting” (the motivational drive to pursue a reward, mediated heavily by mesolimbic dopamine) from “liking” (the hedonic pleasure derived once the reward is obtained, mediated by other neurochemical systems). Sexual desire disorders are, in this framework, largely disorders of wanting: the capacity for physical response and pleasure may be intact, but the motivational engine that initiates pursuit is under-driven. Because bremelanotide acts on the melanocortin-dopamine interface that governs wanting, its mechanism maps onto exactly the component that desire disorders implicate, which is a large part of why the RECONNECT endpoints were built around desire and desire-related distress rather than around orgasm or physical arousal alone.
Receptor Selectivity and Why It Shapes the Side-Effect Profile
Bremelanotide’s non-selective binding across the melanocortin family is a double-edged attribute. Its therapeutic effect is attributed principally to MC3R and MC4R engagement in the central nervous system, but the same molecule also engages MC1R, the receptor on melanocytes that controls pigmentation. This is not an off-target contaminant effect; it is intrinsic to the compound’s pharmacology. The consequence is that the very receptor promiscuity that makes melanocortin agonists effective on sexual motivation also makes them capable of driving skin and mucosal pigmentation, autonomic responses such as flushing, and the nausea characteristic of central melanocortin activation. Understanding this trade-off is essential for interpreting the safety data honestly: the common adverse effects are on-target melanocortin phenomena, not signs of impurity or improper handling, and they scale with the degree and frequency of receptor activation.
Central Versus Vascular: Why This Is Not a PDE5 Inhibitor
The most important conceptual contrast is between bremelanotide and phosphodiesterase-5 (PDE5) inhibitors such as sildenafil and tadalafil. PDE5 inhibitors act peripherally: they prevent the breakdown of cyclic GMP in the smooth muscle of the corpus cavernosum, enhancing the vasodilation that produces an erection once arousal has already begun. They do essentially nothing to generate desire; they facilitate the plumbing of an arousal that must be initiated by other means.
Bremelanotide operates one level upstream. By engaging central melanocortin and dopaminergic circuits, it targets the origination of sexual motivation itself. This is why the two mechanisms are complementary rather than redundant, and why bremelanotide has been of interest for desire disorders (where the deficit is in wanting) whereas PDE5 inhibitors address performance disorders (where the deficit is in physical response). The two are compared in detail later in this article.
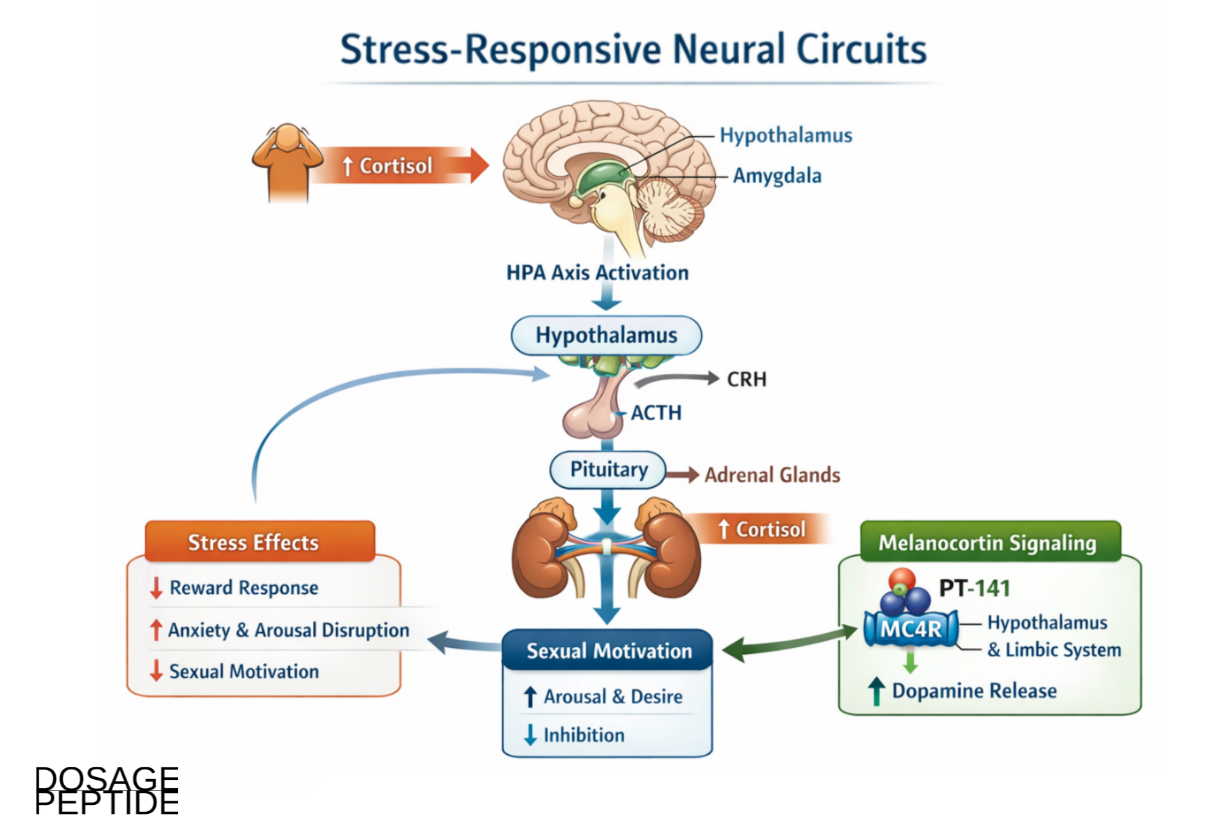
How Do Stress and the HPA Axis Intersect With Sexual Motivation?
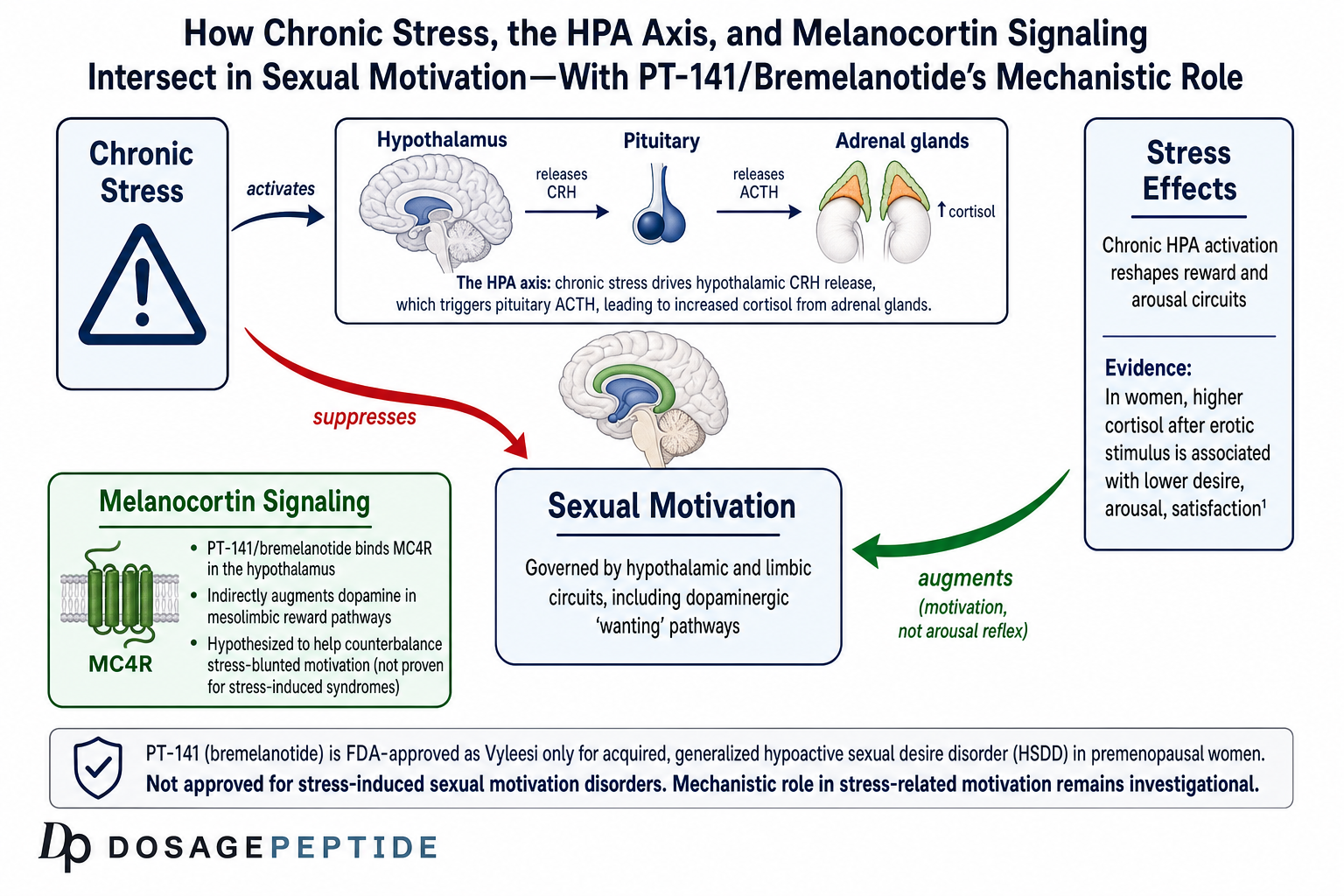
The premise that stress can suppress sexual motivation independently of a diagnosable mood disorder is well grounded, and it is the honest anchor for any discussion of PT-141 in a stress context. The hypothalamic-pituitary-adrenal (HPA) axis is the body’s central stress-response system: perceived threat drives the hypothalamus to release corticotropin-releasing hormone, which triggers pituitary adrenocorticotropic hormone (ACTH) release, which in turn stimulates adrenal cortisol secretion. Under acute conditions this is adaptive; under chronic conditions the sustained activation reshapes the very reward and arousal circuits that sexual motivation depends on.
What the Cortisol Evidence Actually Shows
Direct human evidence for a cortisol-arousal relationship comes from controlled laboratory work. In a study of premenopausal women exposed to erotic stimuli, most participants showed a decrease in salivary cortisol, but a subset showed a cortisol increase, and those women with rising cortisol scored significantly lower on the arousal, desire, and satisfaction domains of the Female Sexual Function Index.[3] This is important because it demonstrates, in humans, that a stress-linked endocrine response tracks with reduced sexual function, and it does so at the level of desire and arousal rather than physical capacity.
It is worth being precise about what this study does and does not establish. It shows an association between an acute cortisol response and lower sexual function scores; it does not demonstrate that chronic stress causes a discrete clinical syndrome, nor does it test any melanocortin intervention. The finding supports the plausibility of a stress-sensitive motivation deficit, not a proven “stress-induced sexual motivation disorder” as a formal diagnosis.
Where Melanocortin Signaling Fits In
The mechanistic case for linking melanocortin signaling to stress physiology rests on anatomical and circuit overlap rather than on a demonstrated causal loop. The hypothalamic and limbic regions rich in MC4R are the same regions that integrate HPA-axis signals and process reward. Chronic stress and elevated glucocorticoid exposure are associated with blunted mesolimbic dopamine responsiveness, which manifests behaviorally as reduced motivation and anhedonia across many appetitive domains, including sexual approach behavior.
Because bremelanotide augments dopaminergic tone in these same mesolimbic circuits, a reasonable hypothesis is that melanocortin activation could partially counterbalance stress-induced motivational suppression. This is a mechanistic conjecture supported by convergent anatomy, not a proven therapeutic effect. Critically, bremelanotide is not a cortisol-lowering agent, is not an anxiolytic, and does not suppress HPA-axis output; it does not treat stress itself. Any interaction with stress-related physiology is indirect, operating downstream on the motivation circuit rather than upstream on the stress response.
How Chronic Stress Reshapes Reward Circuitry
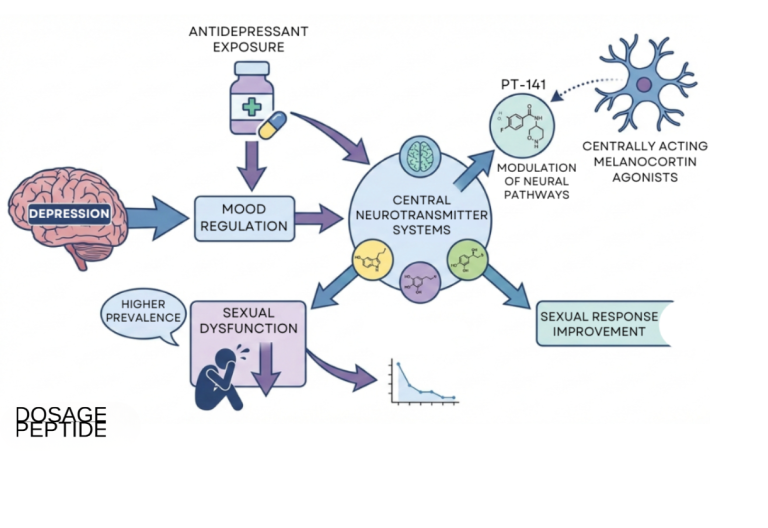
The biological plausibility of a stress-to-desire pathway rests on a substantial body of reward neuroscience. Chronic stress and sustained glucocorticoid exposure are associated with adaptations in the mesolimbic dopamine system that reduce its responsiveness to appetitive cues. Behaviorally, this manifests as anhedonia and reduced motivation across many reward domains: food, social interaction, novelty, and sexual approach behavior. The reduction is not primarily a loss of the physical capacity to respond but a dampening of the drive to initiate. Because sexual motivation is one appetitive behavior among several that share the mesolimbic substrate, it is vulnerable to the same stress-induced blunting that affects the others, which is one reason low desire so often co-travels with generalized low motivation during periods of prolonged stress.
This framing helps explain why stress-related low desire is conceptually distinct from a primary mood disorder even though the two frequently overlap. A person can experience stress-linked motivational blunting without meeting criteria for major depression, and the cortisol-arousal association observed in laboratory settings supports the existence of a stress-sensitive component to sexual function that operates through endocrine and reward pathways rather than through mood pathology alone.[3]
The Bidirectional Nature of the Relationship
The relationship between stress and sexual motivation is not one-directional. Just as stress can suppress desire, unsatisfying or absent sexual function can itself become a source of distress that feeds back into the stress system, producing a self-reinforcing loop. This is precisely why the HSDD construct pairs low desire with the requirement of marked distress: the distress is not incidental but central to the disorder, and it is one of the endpoints the pivotal trials measured directly. A compound that improves desire could, in principle, interrupt this loop by reducing the distress that arises from the desire deficit, an effect the RECONNECT trials captured through the Female Sexual Distress Scale. Whether this distress reduction reflects a genuine downstream easing of stress physiology or simply the relief of a specific worry is not something the trials were designed to resolve.
| System | Primary node | Effect of chronic stress | Relationship to PT-141 |
|---|---|---|---|
| HPA axis | Hypothalamus, pituitary, adrenal | Sustained cortisol elevation | Not modulated by PT-141 |
| Mesolimbic dopamine | VTA to nucleus accumbens | Blunted reward responsiveness | Augmented indirectly via MC4R |
| Melanocortin (MC4R) | Paraventricular nucleus, medial preoptic area | Not the primary stress target | Direct agonist target of PT-141 |
| Sexual motivation circuit | Hypothalamic and limbic integration | Reduced incentive salience | Hypothesized point of counterbalance |
What Does the Clinical Evidence Show?
The strength of bremelanotide’s evidence base is what separates it from typical research peptides, and it deserves careful, non-inflated presentation. The pivotal data come from two identical phase 3 trials, collectively known as the RECONNECT program, alongside earlier erectile-function work that established the compound’s central mechanism in humans.
The RECONNECT Phase 3 HSDD Trials
The RECONNECT program comprised two identically designed, randomized, double-blind, placebo-controlled, multicenter phase 3 studies (identified as Study 301 and Study 302). Premenopausal women with acquired, generalized HSDD were randomized one-to-one to 24 weeks of treatment with subcutaneous bremelanotide 1.75 mg as needed or placebo.[4] The co-primary endpoints were change in sexual desire, measured by the Female Sexual Function Index desire domain, and change in the distress associated with low desire, measured by the Female Sexual Distress Scale.
Both studies met their co-primary endpoints: bremelanotide significantly improved sexual desire and significantly reduced the distress related to low desire compared with placebo.[4] The reported effect sizes were modest but statistically robust, approximately 0.3 across the desire and distress measures, with individual study values ranging from about 0.29 to 0.42, which is characteristic of centrally acting agents for desire disorders and comparable to other approved therapies in the space. An open-label extension study subsequently supported the longer-term safety and tolerability of the compound over up to 52 additional weeks of as-needed use.[5]
The identical-replicate design of the two RECONNECT trials is a particular strength worth emphasizing. Running two independent studies with the same protocol, rather than a single larger trial, provides internal replication: a finding that holds in both is far less likely to be a chance result or an artifact of one study population. That both Study 301 and Study 302 reached the same co-primary endpoints, in the same direction, with comparable effect sizes, is precisely the pattern regulators look for as evidence of a reproducible drug effect. The trials also ran their treatment phase over 24 weeks, long enough to characterize repeated as-needed use rather than a single-dose response, which is important for a compound intended for recurrent, on-demand administration.
Earlier Erectile-Function Studies
Before its development for female HSDD, bremelanotide was studied for male erectile dysfunction. A double-blind, placebo-controlled evaluation examined the safety, pharmacokinetics, and pharmacodynamic effects of intranasal PT-141 in healthy males and in men with mild-to-moderate erectile dysfunction, and reported statistically significant improvements in erectile response versus placebo.[6] These findings confirmed that the central melanocortin mechanism could translate into a measurable sexual response in humans, not only in animal models.
However, the intranasal route produced clinically relevant elevations in blood pressure, and this cardiovascular signal, combined with variable bioavailability, led developers to abandon nasal delivery. The eventual subcutaneous formulation was associated with a more manageable, transient blood-pressure effect, which is part of why the female HSDD program advanced to approval while male ED development did not culminate in an approved product.
Limits of the Evidence
Several honest limitations frame all of the above. First, none of the pivotal trials stratified participants by stress exposure or measured stress biomarkers; the “stress-induced” framing is a mechanistic interpretation layered onto trials designed around desire and distress endpoints, not stress endpoints.[4] Second, the approved efficacy data are specific to premenopausal women with HSDD; extrapolation to men, to postmenopausal women, or to other populations is not supported by approval-grade evidence. Third, the effect sizes, while real, are moderate, and the trials measured self-reported desire and distress rather than any objective physiological marker of a “corrected” stress state.
Interpreting the Effect Sizes Honestly
The effect sizes reported in RECONNECT deserve careful, non-inflated interpretation because they are frequently either overstated or dismissed. An effect size of approximately 0.3 on desire and distress measures, with individual study values ranging from about 0.29 to 0.42, is best described as small-to-moderate. In the context of desire disorders, where the outcome is inherently subjective and placebo responses tend to be substantial, an effect of this magnitude that separates cleanly from placebo across two independent, identically designed trials is a meaningful and reproducible signal, and it was sufficient to support approval. It is not, however, a dramatic transformation, and it should not be presented as one. The honest reading is that bremelanotide produces a real but modest average improvement in desire and a real reduction in the associated distress, with considerable individual variability in response.
It is also worth noting the high placebo response typical of this field. Sexual desire is sensitive to expectation, attention, and context, so a portion of any observed improvement in both arms reflects those factors rather than the pharmacology. The value of the randomized, double-blind, placebo-controlled design is precisely that it isolates the drug-specific increment above this backdrop, which is why the reproducibility of the effect across two trials carries more weight than the absolute magnitude in either one.
The Onset and Duration Profile
The approved product is used on demand rather than continuously, which reflects the compound’s pharmacology and distinguishes it from chronically dosed agents for low desire. It is administered ahead of anticipated activity because the central mechanism requires time to engage the relevant circuits, and it is not intended to build a sustained baseline effect through daily accumulation. This on-demand, event-linked profile is a defining practical feature: it means the compound is studied and used as an acute motivational intervention rather than as a maintenance therapy that reshapes baseline desire over weeks. In research terms, this event-driven paradigm is what allows investigators to isolate acute motivational effects without the confound of sustained neurochemical alteration.
What Is the Safety and Tolerability Profile?
Because bremelanotide is an approved drug, its adverse-event profile is unusually well characterized for a compound often discussed in research-peptide circles. The prescribing information and trial data document a consistent and largely predictable set of effects.[2]
Common Adverse Effects
- Nausea is the most common effect, reported by roughly 40% of treated women and typically most pronounced with the first dose.
- Flushing occurs in approximately 20% of users, consistent with melanocortin activity.
- Injection-site reactions are reported by around 13% of users.
- Headache affects roughly 11% of users.
Most of these events are mild to moderate and self-limiting, which was reflected in the favorable overall tolerability seen across the RECONNECT program.[4]
Cardiovascular Considerations
A transient increase in blood pressure and a corresponding decrease in heart rate occur after each dose and typically resolve within about 12 hours. Because of this effect, the labeling contraindicates use in patients with uncontrolled hypertension or known cardiovascular disease, and warns against use in those at high cardiovascular risk.[2] This is the single most important safety consideration and the reason blood-pressure status is central to any discussion of the compound.
Focal Hyperpigmentation
Because melanocortin receptors include MC1R, the pigmentation receptor, bremelanotide can cause focal hyperpigmentation. This was reported in about 1% of women receiving up to eight doses per month and involved sites including the face, gingiva (gums), and breasts. The risk is higher with darker skin and with more frequent dosing, and resolution after discontinuation was not confirmed in all affected individuals.[2] This risk is directly attributable to the compound’s melanocortin activity and is one of the clearest illustrations of why receptor selectivity matters across this peptide class.
Nausea, flushing, and spontaneous erections are also the classic effects seen with the parent compound Melanotan II, underscoring that these are shared, on-target melanocortin phenomena rather than idiosyncratic reactions.
Managing the Nausea Signal
Nausea deserves specific attention because it is both the most common effect and the one most likely to affect real-world tolerability. In the trials, nausea was most pronounced with the first dose and tended to diminish with subsequent exposures, a pattern consistent with the central melanocortin mechanism and with the body’s adaptation to repeated activation. A minority of participants found the nausea significant enough to discontinue, which is reflected in the discontinuation rates seen in the pivotal program. The practical implication is that the compound’s tolerability is front-loaded: the first experience is often the most challenging, and the profile improves for those who continue. This is an important nuance because a single first-dose experience may not represent the steady-state tolerability of the compound.
Long-Term Safety Considerations
The open-label extension work provided reassurance on longer-term tolerability across up to roughly a year of additional as-needed use, with no new safety signals emerging beyond those seen in the controlled phase.[5] The most important open long-term question concerns cumulative pigmentation, since focal hyperpigmentation did not reliably resolve after discontinuation in all affected individuals and the risk rises with more frequent dosing. This is why the approved dosing caps monthly exposure and why frequency, not just per-dose amount, is the relevant variable for pigmentation risk. It is a concrete example of how the melanocortin mechanism’s benefits and risks are governed by the same receptor engagement.
How Does PT-141 Compare With PDE5 Inhibitors and Melanotan II?
Placing bremelanotide alongside the two most relevant comparators, PDE5 inhibitors on the mechanism axis and Melanotan II on the chemistry axis, clarifies both what it is and what it is not.
PT-141 Versus PDE5 Inhibitors
The contrast here is fundamental and mechanistic. PDE5 inhibitors are peripheral vasodilators that facilitate the physical erectile response once desire and arousal are present; they do not create desire. Bremelanotide is a central agent that acts on the motivation circuit itself, upstream of the vascular response. In practical research terms, they address different links in the chain: desire and arousal initiation for the melanocortin agonist, physical performance for the PDE5 inhibitor.
| Feature | PT-141 (bremelanotide) | PDE5 inhibitors (sildenafil, tadalafil) |
|---|---|---|
| Site of action | Central (CNS, hypothalamus/limbic) | Peripheral (penile vasculature) |
| Primary mechanism | MC4R agonism, dopaminergic modulation | PDE5 inhibition, cGMP preservation |
| Target of effect | Sexual motivation and desire | Physical erectile response |
| Approved indication | HSDD in premenopausal women | Erectile dysfunction, PAH |
| Key safety concern | Transient BP rise, hyperpigmentation, nausea | Hypotension, nitrate interaction |
PT-141 Versus Melanotan II
Melanotan II is the broader parent melanocortin agonist from which bremelanotide is derived; PT-141 is a metabolite (the C-terminal des-amide analogue) of Melanotan II. Both engage central MC4R and share the characteristic melanocortin effects of nausea, flushing, and spontaneous erection, and both engage MC1R sufficiently to drive pigmentation. The key difference is one of development and intended use: Melanotan II is an unapproved, non-selective compound most associated with illicit tanning, whereas bremelanotide was refined and clinically developed as a defined, on-demand sexual-motivation agent and carries an approved human indication.[1] Research contexts that examine the two together are documented in the combined Melanotan II and PT-141 protocol reference.
It is also worth situating both compounds against a third relative, afamelanotide (Melanotan I, marketed as Scenesse). Afamelanotide is a more MC1R-selective linear analogue that is approved for a rare light-sensitivity disorder, erythropoietic protoporphyria, and its selectivity for the pigmentation receptor is precisely why it is used for a skin indication rather than a sexual one. Comparing the three clarifies a general principle of this peptide class: the balance of receptor subtype activity determines the dominant clinical effect. A compound biased toward MC1R behaves like a pigmentation agent; a compound with meaningful central MC3R and MC4R activity behaves like a sexual-motivation agent; and a broad, non-selective compound like Melanotan II produces the full spectrum of melanocortin effects with correspondingly less predictability.
| Compound | Receptor bias | Dominant effect | Regulatory status |
|---|---|---|---|
| Bremelanotide (PT-141) | Central MC3R/MC4R active, also MC1R | Sexual motivation | FDA-approved (Vyleesi) for HSDD in women |
| Melanotan II | Broad, non-selective | Tanning plus sexual and autonomic effects | Unapproved |
| Afamelanotide (Melanotan I) | MC1R-selective | Pigmentation | Approved (Scenesse) for erythropoietic protoporphyria |
What Research Models and Methodology Underpin PT-141 Studies?
The evidence for PT-141 spans a well-defined progression of model systems, each answering a different question, and appreciating that progression is central to interpreting the compound rigorously.
Preclinical Models
The earliest and most mechanistically informative work used rodent and non-human primate models. In rats, systemic PT-141 produced penile erection and, importantly, activated hypothalamic neurons as shown by increased c-Fos immunoreactivity, providing anatomical evidence that the effect originated centrally.[1] These models established the central mechanism and localized it to the hypothalamus before any human exposure, which is precisely the order in which a mechanistic claim should be built.
Early Human Pharmacology
The transition to humans came through pharmacokinetic and pharmacodynamic studies, initially by the intranasal route in men with erectile dysfunction, which established that the central mechanism could produce a measurable clinical response and simultaneously surfaced the blood-pressure signal that shaped subsequent development.[6] These studies emphasized safety, exposure profiles, and tolerability, using healthy volunteers and mild-to-moderate ED patients rather than individuals selected for stress-related pathology.
Pivotal Efficacy Trials
The definitive efficacy data came from the randomized, double-blind, placebo-controlled RECONNECT trials, which used validated, self-reported instruments (the Female Sexual Function Index desire domain and the Female Sexual Distress Scale) as endpoints.[4] This design is the gold standard for a subjective outcome such as desire, but it also defines a boundary: because the endpoints were desire and distress, not stress biomarkers, the trials cannot speak directly to a stress-specific mechanism. Any researcher designing a study to test the “stress-induced” hypothesis would need to add stress stratification, cortisol or HPA-axis measures, and appropriate control conditions that the existing trials did not include.
Why Validated Instruments Matter for a Subjective Outcome
The choice of endpoint instruments is not a technicality; it is central to the credibility of any desire-disorder study. Sexual desire cannot be measured with a blood test or an imaging biomarker, so the field relies on psychometrically validated questionnaires that have been tested for reliability and for the ability to detect change. Using the Female Sexual Function Index desire domain and the Female Sexual Distress Scale, both established instruments in the field, allowed the RECONNECT program to quantify a subjective experience in a reproducible way and to compare results against placebo on a common scale. A study that invented its own unvalidated desire measure would be far less interpretable, which is one reason the pivotal program’s use of established instruments strengthens confidence in its findings.
What a Stress-Specific Study Would Require
To move the “stress-induced sexual motivation” hypothesis from plausible conjecture to tested claim, a purpose-built study would need several features absent from the existing record. It would enroll participants selected or stratified by validated stress measures rather than by desire criteria alone. It would incorporate objective stress physiology, such as cortisol profiles, diurnal HPA-axis rhythm, or heart-rate variability, alongside the subjective desire and distress endpoints. It would ideally include a comparison against an intervention known to reduce stress directly, to distinguish a melanocortin-specific motivational effect from generalized stress relief. Until such a study exists, the honest position is that the mechanistic overlap is real and interesting but the specific clinical claim is untested.
How Is PT-141 Handled and Reconstituted in a Research Context?
The following describes standard laboratory handling practice for research-grade lyophilized peptides and is provided strictly as educational and methodological context. It is not medical advice, not a dosing recommendation, and not a protocol for human administration. The approved clinical product Vyleesi is supplied as a prefilled autoinjector and should never be conflated with research material.
Reconstitution Basics
Research-grade PT-141 is typically supplied as a lyophilized (freeze-dried) powder that must be reconstituted with bacteriostatic water before it can be handled in solution. The core methodological considerations, choice of diluent, gentle introduction of the diluent against the vial wall rather than directly onto the peptide pellet, avoidance of vigorous agitation, and appropriate cold storage of the reconstituted solution, are common to the peptide class and are described in the general peptide reconstitution guide. Concentration is determined by the ratio of peptide mass to diluent volume, and small errors in that ratio propagate directly into every subsequent measurement.
Peptides are physically fragile relative to small-molecule compounds. The gentle handling emphasized above is not fussiness: mechanical shear from vigorous shaking, exposure to heat, and repeated freeze-thaw cycles can degrade a peptide’s structure and reduce the fraction of intact, active molecule in solution. Because melanocortin peptides act at small quantities, even modest degradation can meaningfully change the effective concentration in a way that is invisible without analytical testing. This is why documented, consistent handling is treated as part of experimental rigor rather than as an afterthought, and why storage temperature and time-in-solution are recorded variables in careful work.
Concentration and Measurement
Because melanocortin peptides are active at small quantities, accurate concentration math matters more than with many other compounds. Researchers commonly use a reconstitution and dosage calculator to convert a target quantity into a syringe volume for a given vial size and diluent amount, reducing the arithmetic errors that are the most common source of variability in peptide work. Compound-specific handling parameters for the 10 mg vial format are documented in the PT-141 10 mg vial dosage protocol. Consistent, documented reconstitution and storage practice is what allows one experiment to be compared meaningfully against another.
What Are the Limitations and Open Questions?
A rigorous account of PT-141 must be as clear about what remains unknown as about what is established.
The Stress Framing Is a Hypothesis, Not an Indication
The central limitation of the “stress-induced sexual motivation disorder” framing is that no approved indication and no pivotal trial has been built around it. The mechanistic story, HPA-axis activation blunts mesolimbic dopamine, melanocortin activation augments mesolimbic dopamine, therefore melanocortin activation might counterbalance stress-related motivation deficits, is internally coherent and anatomically plausible, but it has not been directly tested in a stress-stratified clinical trial.[3] The cortisol-arousal association in women is real, and the RECONNECT efficacy is real, but the two have never been connected in a single controlled study.
Population and Route Boundaries
The approval-grade evidence is confined to premenopausal women with acquired, generalized HSDD, using the subcutaneous route.[2] Male efficacy was demonstrated in early studies but never carried to approval, and the intranasal cardiovascular signal illustrates that route matters. Extrapolating efficacy or safety across populations and routes is not warranted from the existing record.
Modest Effect Sizes and Subjective Endpoints
The pivotal efficacy, while statistically significant and clinically meaningful for an approved indication, reflected moderate effect sizes on self-reported measures of desire and distress.[4] There is no objective biomarker that confirms a “corrected” motivation state, and the durability of benefit beyond the studied windows, as well as long-term consequences of repeated melanocortin activation such as cumulative pigmentation risk, remain areas where more data would strengthen the picture.[5]
Frequently Asked Questions
Is PT-141 the same thing as bremelanotide?
Yes. PT-141 is the research and development designation, and bremelanotide is the assigned generic name for the identical molecule, marketed as Vyleesi. The clinical trial and regulatory record is filed under bremelanotide, so anyone researching the compound should search both terms to find the full body of evidence, including the FDA approval and the RECONNECT phase 3 trials.
Is PT-141 approved to treat stress or stress-induced sexual problems?
No. Bremelanotide is FDA-approved only for acquired, generalized hypoactive sexual desire disorder in premenopausal women. There is no approved indication for stress, anxiety, or a discrete “stress-induced sexual motivation disorder.” The connection between stress and melanocortin signaling is a mechanistic hypothesis based on overlapping brain circuitry, not a tested or approved clinical indication.
Does PT-141 lower cortisol or reduce HPA-axis activity?
No. Bremelanotide does not act as a cortisol-lowering agent or an anxiolytic, and it does not suppress hypothalamic-pituitary-adrenal axis output. It acts downstream on melanocortin and dopaminergic motivation circuits. Any interaction with stress physiology is indirect, operating on the reward and motivation pathway rather than on the stress-response system itself.
How is PT-141 different from Viagra or Cialis?
PDE5 inhibitors like sildenafil (Viagra) and tadalafil (Cialis) act peripherally on penile blood vessels to facilitate the physical erectile response once arousal exists. PT-141 acts centrally in the brain on melanocortin receptors to influence sexual desire and motivation itself. They target different links in the chain, which is why their mechanisms are considered complementary rather than interchangeable.
What are the most common side effects of bremelanotide?
In the phase 3 trials, nausea was the most frequent effect, reported by roughly 40% of users and usually worst with the first dose, followed by flushing (about 20%), injection-site reactions (about 13%), and headache (about 11%). A transient rise in blood pressure occurs after each dose, and focal hyperpigmentation can develop, particularly with darker skin and more frequent dosing.
Why can’t bremelanotide be used by people with high blood pressure?
Each dose causes a transient increase in blood pressure and a decrease in heart rate that usually resolves within about 12 hours. Because of this predictable cardiovascular effect, the prescribing information contraindicates use in people with uncontrolled hypertension or known cardiovascular disease. Blood-pressure status is the most important safety consideration when the compound is discussed.
Is PT-141 approved for men?
No. Although bremelanotide was studied for male erectile dysfunction in early trials, including intranasal formulations that showed efficacy but produced blood-pressure elevations, it was never approved for male use. The only approved indication is hypoactive sexual desire disorder in premenopausal women, delivered by subcutaneous injection.
How strong is the evidence for PT-141 compared with other research peptides?
Considerably stronger. Unlike most research peptides, which are supported only by animal or in-vitro data, bremelanotide has completed two large randomized, double-blind, placebo-controlled phase 3 trials and holds an FDA approval. Its efficacy for desire disorders is modest but statistically robust, and its safety profile is well characterized, which is unusual in this compound class.
Why does PT-141 cause skin darkening?
Bremelanotide activates melanocortin receptors non-selectively, which includes MC1R, the receptor on pigment-producing melanocytes. Stimulating MC1R promotes melanin production, so focal hyperpigmentation of areas such as the face, gums, and breasts can occur. The risk is greater in people with darker skin and with more frequent dosing, and in the trials it did not always resolve after stopping, which is why monthly dosing frequency is capped.
Is PT-141 the same as Melanotan II?
No, though they are closely related. PT-141 (bremelanotide) is a metabolite (the C-terminal des-amide analogue) of Melanotan II and shares its central melanocortin activity. The difference is one of development and refinement: Melanotan II is an unapproved, broadly non-selective compound associated with illicit tanning, whereas bremelanotide was developed as a defined, on-demand sexual-motivation agent and carries an FDA approval for HSDD in premenopausal women.
References
- Molinoff PB, Shadiack AM, Earle D, Diamond LE, Quon CY. PT-141: a melanocortin agonist for the treatment of sexual dysfunction. Annals of the New York Academy of Sciences. 2003;994:96-102. https://nyaspubs.onlinelibrary.wiley.com/doi/abs/10.1111/j.1749-6632.2003.tb03167.x
- U.S. Food and Drug Administration. VYLEESI (bremelanotide injection) prescribing information. NDA 210557; 2019. https://dailymed.nlm.nih.gov/dailymed/fda/fdaDrugXsl.cfm?setid=8c9607a2-5b57-4a59-b159-cf196deebdd9 (also available at accessdata.fda.gov)
- Hamilton LD, Rellini AH, Meston CM. Cortisol, sexual arousal, and affect in response to sexual stimuli. Journal of Sexual Medicine. 2008;5(9):2111-2118. https://pubmed.ncbi.nlm.nih.gov/18624961/
- Kingsberg SA, Clayton AH, Portman D, et al. Bremelanotide for the treatment of hypoactive sexual desire disorder: two randomized phase 3 trials. Obstetrics & Gynecology. 2019;134(5):899-908. https://pubmed.ncbi.nlm.nih.gov/31599840/
- Simon JA, Kingsberg SA, Portman D, et al. Long-term safety and efficacy of bremelanotide for hypoactive sexual desire disorder. Obstetrics & Gynecology. 2019;134(5):909-917. https://pubmed.ncbi.nlm.nih.gov/31599847/
- Diamond LE, Earle DC, Rosen RC, Willett MS, Molinoff PB. Double-blind, placebo-controlled evaluation of the safety, pharmacokinetic properties and pharmacodynamic effects of intranasal PT-141, a melanocortin receptor agonist, in healthy males and patients with mild-to-moderate erectile dysfunction. International Journal of Impotence Research. 2004;16(1):51-59. https://pubmed.ncbi.nlm.nih.gov/14963471/