Human chorionic gonadotropin (HCG) occupies an unusual place in male endocrinology: it is a placental hormone, an FDA-approved drug, a fertility agent, and — increasingly — an off-label companion to testosterone replacement therapy (TRT). The central research question this article examines is a practical one for anyone studying the literature: what does the clinical evidence actually show about HCG’s ability to raise testosterone, preserve or restore fertility, and protect testicular function, and where does that evidence stop and off-label practice begin? HCG earns its clinical relevance because it behaves like luteinizing hormone (LH) at the receptor level, and by doing so it can drive the testis to make testosterone from the inside — a distinction that turns out to matter enormously for sperm production.
This is an educational review of the published literature and regulatory record, not medical advice. It does not tell any reader how to dose HCG for themselves. Where dosing appears, it is reported as it exists in clinical trials, guidelines, and drug labels. Nothing here should be read as a prescription, and material sold as “research-grade” HCG is not the FDA-approved pharmaceutical product discussed in the clinical trials below.
What is HCG, and why does it behave like luteinizing hormone?
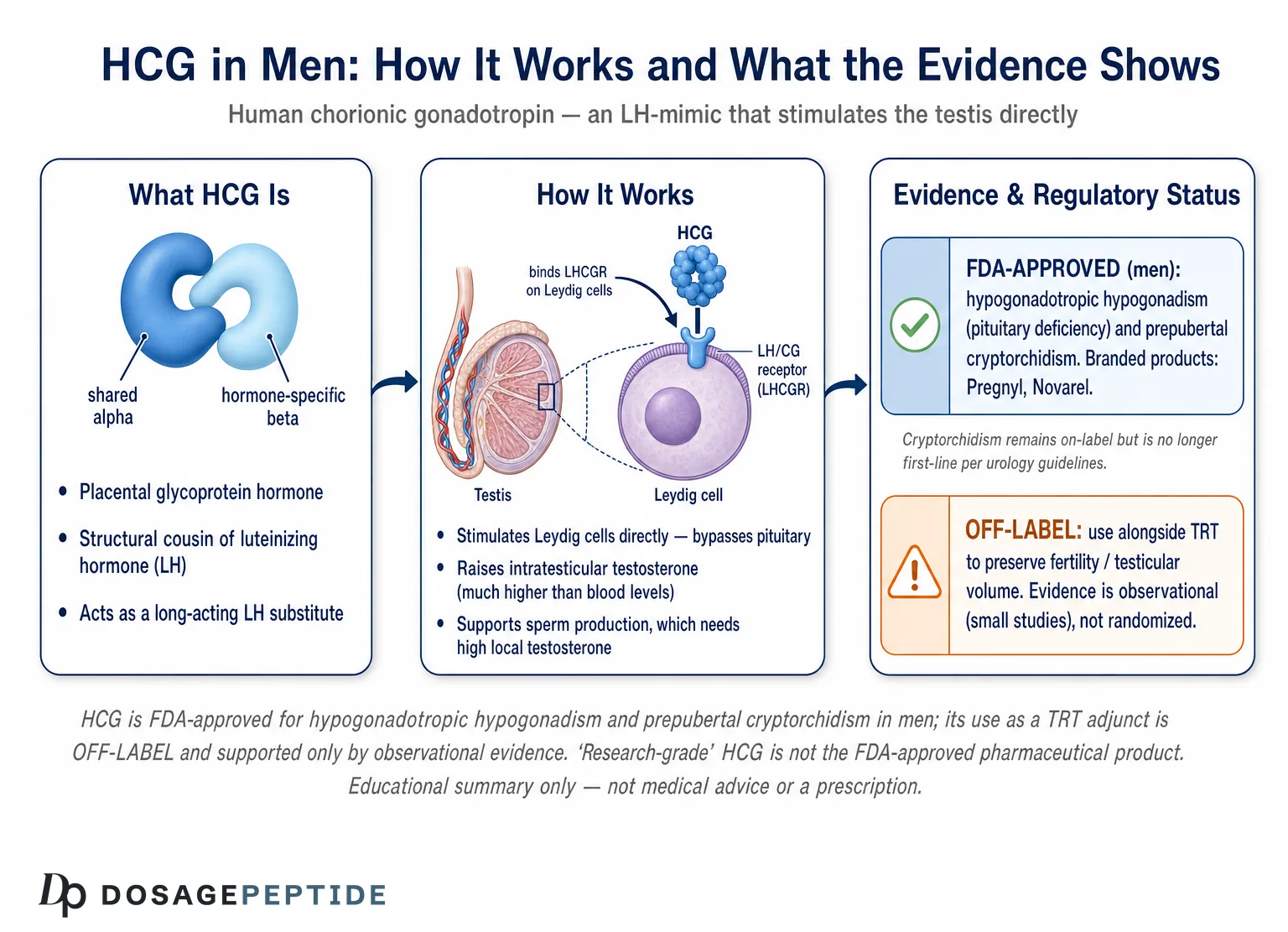
Human chorionic gonadotropin is a glycoprotein hormone produced physiologically by the syncytiotrophoblast of the placenta during pregnancy, where its best-known job is to rescue the corpus luteum and sustain progesterone production. Its relevance to male physiology comes from a quirk of molecular evolution: HCG is a close structural cousin of luteinizing hormone, and it binds and activates the same receptor. In clinical use for men, HCG is essentially borrowed from pregnancy biology and repurposed as a long-acting LH substitute.
HCG and LH belong to the same family of pituitary and placental glycoprotein hormones, which also includes follicle-stimulating hormone (FSH) and thyroid-stimulating hormone (TSH). All four are heterodimers built from two non-covalently linked subunits.
The glycoprotein structure: a shared alpha subunit and a hormone-specific beta subunit
Every member of the glycoprotein hormone family shares an identical alpha subunit; biological specificity comes entirely from the beta subunit, which differs between LH, FSH, TSH, and HCG. LH and HCG are the two most similar: their beta subunits are highly homologous, which is precisely why HCG can act as an LH mimic at the gonad.[1] The most conspicuous structural difference is that the HCG beta subunit carries an extended carboxy-terminal peptide, heavily decorated with sialic-acid-rich carbohydrate chains. That extra glycosylation is functionally important: it slows renal clearance and gives HCG a substantially longer circulating half-life than pituitary LH, which is why a single injection produces a prolonged rise in testosterone rather than the short pulses that native LH generates.
Both hormones circulate not as single uniform molecules but as mixtures of differentially glycosylated isoforms, and these isoforms differ in half-life and potency at the receptor.[1] For the reader, the practical takeaway is simpler than the biochemistry: HCG is a heterodimeric glycoprotein whose beta subunit lets it dock onto the LH receptor and whose sugar chains let it linger there far longer than LH itself.
Biased agonism: why HCG is not simply “LH in a vial”
It is tempting to describe HCG as interchangeable with LH, but the pharmacology is more nuanced. Detailed signaling studies using recombinant human LH and recombinant human HCG at the same receptor have shown that the two hormones are biased agonists — they activate the identical receptor but trigger quantitatively and qualitatively different downstream signals inside the cell.[1] In these experiments, HCG showed a higher steroidogenic potential — a stronger drive toward cyclic-AMP signaling and testosterone synthesis — while LH preferentially favored proliferative and anti-apoptotic (cell-survival) pathways.[1]
This helps explain a clinical observation: HCG is a very effective tool for switching on Leydig-cell testosterone production, which is exactly what most male applications require. Readers who want plain-language definitions of the endocrine terms used throughout this article can consult the peptide and hormone glossary. The distinction between LH and HCG is not academic hair-splitting — it is part of why HCG, rather than recombinant LH, became the workhorse gonadotropin for stimulating the testis.
How does the HPG axis normally regulate testosterone and sperm?
To understand what HCG does, it helps to understand the control system it plugs into: the hypothalamic-pituitary-gonadal (HPG) axis. In the healthy male, the hypothalamus releases gonadotropin-releasing hormone (GnRH) in pulses. GnRH prompts the anterior pituitary to secrete two gonadotropins — LH and FSH — into the bloodstream. LH travels to the testis and stimulates the Leydig cells (in the interstitial tissue between the seminiferous tubules) to produce testosterone. FSH acts on the Sertoli cells inside the tubules to support sperm maturation. Testosterone, in turn, feeds back negatively on both the hypothalamus and pituitary, dialing down GnRH and LH so the system self-regulates.
HCG enters this circuit at the level of the testis. Because it mimics LH, it acts directly on Leydig cells and bypasses the hypothalamus and pituitary entirely. That is a crucial property: in a man whose pituitary cannot make enough LH — for example, in hypogonadotropic hypogonadism — HCG can substitute for the missing signal and coax the testis to work. It is also why HCG behaves so differently from oral agents such as clomiphene or enclomiphene, which work higher up the axis by increasing the brain’s own gonadotropin output.
Serum versus intratesticular testosterone: the roughly 100-fold gradient
One of the most important and most under-appreciated facts in male reproductive endocrinology is that the testosterone concentration inside the testis is vastly higher than the concentration measured in a blood test. Intratesticular testosterone (ITT) is on the order of one to two orders of magnitude higher than serum testosterone, and this high local concentration is what normal spermatogenesis actually requires.[2] Sperm production is not driven by the testosterone your lab reports; it is driven by the far larger reservoir of testosterone bathing the seminiferous tubules.
This single fact explains the central paradox of testosterone therapy. When a man takes exogenous testosterone, his serum testosterone rises — but that external testosterone suppresses the pituitary’s LH output through negative feedback, the Leydig cells stop being stimulated, and intratesticular testosterone collapses. Exogenous testosterone raises the number on the lab slip while starving the testis of the local androgen concentration sperm production depends on, which is why testosterone therapy is a well-documented, and preventable, cause of male infertility.[2] HCG’s clinical rationale flows directly from this gradient: by stimulating the Leydig cells directly, HCG keeps intratesticular testosterone up even when the pituitary has gone quiet.
How does HCG signal at the LH/CG receptor on Leydig cells?
The molecular target for both LH and HCG is the luteinizing hormone/choriogonadotropin receptor (LHCGR), a G-protein-coupled receptor with the classic seven-transmembrane architecture and a large extracellular domain that binds the hormone with high affinity. In men, the LHCGR sits on the surface of the testicular Leydig cells, where its job is to regulate androgen production in response to circulating LH.[1]
When HCG binds the extracellular domain of the LHCGR, the receptor changes shape and couples to intracellular G proteins — chiefly Gs, which activates adenylyl cyclase and raises cyclic AMP. Rising cyclic AMP activates protein kinase A, which drives the enzymatic machinery of steroidogenesis: cholesterol is transported into the mitochondria by the steroidogenic acute regulatory (StAR) protein and converted, through a cascade of cytochrome-P450 and hydroxysteroid-dehydrogenase enzymes, into testosterone. The net result of HCG binding is a sustained increase in Leydig-cell testosterone output, concentrated exactly where spermatogenesis needs it — inside the testis.
Because the LHCGR is the shared receptor for LH and HCG, and because HCG has a longer half-life and higher steroidogenic potency, a modest, infrequent dose of HCG can maintain robust androgen production. This receptor-level mechanism is the throughline connecting every clinical application discussed below, from fertility induction to TRT-adjunct use. It also underlies the compound’s most direct off-label rationale, detailed in the HCG 5000 IU dosage protocol resource, which frames HCG explicitly as a Leydig-cell stimulant.
What are HCG’s established, FDA-approved clinical roles?
HCG is a genuinely approved drug with a long regulatory history, and it is important to separate what is on-label from what is off-label. Branded chorionic-gonadotropin products such as Pregnyl and Novarel are FDA-approved; historically, Ovidrel (choriogonadotropin alfa) is a recombinant version. According to the FDA-approved Pregnyl label, chorionic gonadotropin is indicated in males for two conditions: prepubertal cryptorchidism not due to anatomical obstruction, and selected cases of hypogonadotropic hypogonadism secondary to pituitary deficiency.[3] (In women, HCG is approved to induce ovulation, but that is outside this article’s scope.)
Hypogonadotropic hypogonadism in men
Hypogonadotropic hypogonadism (also called secondary or central hypogonadism) is a condition in which the testes are fundamentally capable of working, but the pituitary fails to send the LH and FSH signals that would drive them. The cause can be congenital — as in congenital hypogonadotropic hypogonadism and Kallmann syndrome — or acquired, from pituitary tumors, trauma, or, notably, from exogenous androgen use. Because the defect is a missing upstream signal rather than a broken testis, replacing that signal with HCG can restore testosterone production.
A crucial caveat governs all of this: HCG only works if the testis can respond. The condition it treats — secondary (central) hypogonadism — means the testis is intact but understimulated, so supplying the missing LH-like signal fixes the problem. In primary hypogonadism, where the testicular tissue itself is damaged (for example, Klinefelter syndrome or prior chemotherapy or radiation), the Leydig cells cannot answer the signal, and HCG will be ineffective no matter the dose. This is why clinicians characterize the axis before choosing HCG: an LH-substitution strategy is only rational when a functioning testis is waiting on the other end of the signal. The detailed mechanism and this responsive-testis prerequisite are laid out further in the HCG 5000 IU dosage protocol resource.
This is the clearest example of HCG doing on-label work. The FDA label for Pregnyl specifies HCG for selected cases of hypogonadotropic hypogonadism arising from pituitary deficiency, and it lays out concrete dosing regimens — for instance, 500 to 1000 units three times weekly for three weeks followed by a reduced twice-weekly schedule, among alternative protocols described in the label.[3] Those figures are reproduced here strictly as the regulatory record, not as a recommendation. The key conceptual point is that in central hypogonadism, HCG is treating the actual pathophysiology — supplying the LH-like signal the pituitary cannot.
Fertility induction: HCG combined with FSH
The most compelling evidence for HCG in men is in restoring fertility in hypogonadotropic hypogonadism. Because LH activity (supplied by HCG) drives intratesticular testosterone and FSH activity supports the Sertoli cells, gonadotropin therapy can literally switch on spermatogenesis in men who were previously azoospermic. In practice, treatment typically begins with HCG alone to normalize intratesticular testosterone and grow the testes, followed by the addition of an FSH preparation — either human menopausal gonadotropin (hMG) or recombinant FSH.[4]
The results are impressive by the standards of male-infertility medicine. Reviews of combined gonadotropin therapy report that treatment over roughly 12 to 24 months promotes testicular growth in nearly all patients, induces spermatogenesis in approximately 80 percent, and achieves pregnancy rates in the range of about 50 percent, with combined HCG plus FSH generally outperforming HCG alone.[4] Predictors of success include post-pubertal (rather than prepubertal) onset, absence of prior undescended testes, larger baseline testicular volume, and higher baseline inhibin B.[4] This is one of the rare situations in andrology where a medication can convert an infertile man into a fertile one, and HCG is at the center of it.
Cryptorchidism: approved, but no longer first-line
The second male indication on the label — prepubertal cryptorchidism (undescended testis) — is a useful case study in how “FDA-approved” does not automatically mean “currently recommended.” The rationale is that HCG-driven androgen production might encourage testicular descent, and the Pregnyl label describes pediatric regimens for this purpose.[3] In modern practice, however, hormonal therapy has fallen out of favor. The American Urological Association’s guideline on cryptorchidism advises against hormonal therapy to induce testicular descent, citing low success rates, and positions surgical orchidopexy as the standard of care.[5] For an honest review, this is an important nuance: an indication can remain on a decades-old label while specialty guidelines have moved on. The label reflects historical approval; the guideline reflects current best evidence.
Why is HCG used alongside TRT — the testicular-atrophy and fertility problem?
The fastest-growing use of HCG in men is entirely off-label: as an adjunct to testosterone replacement therapy. Understanding why requires returning to the intratesticular-testosterone gradient. When a man starts TRT, exogenous testosterone suppresses pituitary LH and FSH. Deprived of LH stimulation, the Leydig cells go dormant, intratesticular testosterone plummets, the testes shrink (testicular atrophy), and sperm production falls — often to azoospermia. Reviews estimate that a large share of reproductive-age men on testosterone are unaware of this effect, and testosterone-induced suppression of spermatogenesis is now a recognized clinical problem.[6]
The off-label idea is to add low-dose HCG to TRT. Because HCG stimulates the Leydig cells directly, it can keep intratesticular testosterone elevated even while exogenous testosterone suppresses the pituitary — in effect, keeping the testicular “factory” running so that testicular volume and sperm production are preserved. This is a clinical decision made with a physician, weighing goals such as future fertility, testicular volume, and how the man subjectively feels. It is not something to self-administer, and it sits well outside the FDA-approved indications. Men interested in the broader endocrine toolkit sometimes also encounter GnRH-analog approaches, discussed in the gonadorelin 2 mg dosage protocol resource, which work by a different mechanism covered later in this article.
What the intratesticular-testosterone studies show
The mechanistic cornerstone for TRT-adjunct HCG is a study by Coviello and colleagues published in The Journal of Clinical Endocrinology & Metabolism in 2005. The investigators gave healthy men weekly testosterone enanthate (to suppress their own gonadotropins, mimicking TRT) together with either placebo or one of three low HCG doses — 125, 250, or 500 IU every other day — and then directly measured intratesticular testosterone via testicular aspiration.[7] The finding was elegant: intratesticular testosterone rose in a dose-dependent, essentially linear fashion with HCG dose, and even relatively low HCG doses maintained intratesticular testosterone within the normal range despite full gonadotropin suppression from the exogenous testosterone.[7]
This is proof of concept at the level that matters — the actual androgen concentration inside the testis, not just a blood level. It established that co-administered low-dose HCG can defend the intratesticular environment that spermatogenesis depends on, even in the face of TRT. The Coviello study is small and short, and it measured a biochemical surrogate rather than pregnancies, but it remains the key physiological evidence underpinning the entire TRT-plus-HCG strategy.
What the TRT-plus-HCG cohort data show
The most cited clinical (as opposed to purely mechanistic) evidence comes from Hsieh and colleagues, published in the Journal of Urology in 2013. This was a retrospective review of hypogonadal men treated with testosterone replacement plus concomitant low-dose intramuscular HCG (500 IU every other day). Across the cohort, no patient became azoospermic during combined therapy, and semen parameters were maintained; notably, several men in the group went on to contribute to a pregnancy with their partner during follow-up.[8] The authors concluded that low-dose HCG appears to maintain semen parameters in hypogonadal men on TRT and that concurrent use may preserve fertility in men who want to stay fertile while treating their hypogonadism.[8]
The honest framing here is essential. Hsieh’s study is retrospective and observational — there was no randomized control group receiving TRT without HCG — and the sample was modest. It provides encouraging real-world signal, but it does not carry the evidentiary weight of a randomized controlled trial. Taken together, Coviello (mechanism) and Hsieh (clinical outcomes) form a coherent but limited evidence base: biologically plausible, supported by direct intratesticular measurement, and backed by observational fertility data, yet still short of definitive proof. That is exactly why TRT-adjunct HCG remains an off-label, individualized clinical decision rather than a guideline mandate.
Can HCG restore fertility after testosterone or anabolic steroid use?
A distinct but related question is not about preventing infertility during TRT, but about reversing it after a man has already suppressed his own axis — whether from prescribed testosterone or from non-prescribed anabolic-androgenic steroids (AAS). Here HCG is used as part of a “restart” or recovery protocol, typically after the offending androgen is stopped.
The logic is that the dormant Leydig cells need to be re-awakened. HCG supplies the LH-like stimulus to restart intratesticular testosterone, and it is frequently combined with a selective estrogen receptor modulator (such as clomiphene) to restore the man’s own pituitary LH and FSH output, and sometimes with an aromatase inhibitor or an FSH analog. A retrospective case series by Wenker, Ramasamy, and colleagues focusing on HCG for recovery of spermatogenesis after exogenous testosterone reported that HCG — in the studied protocols dosed around 3,000 IU every other day, combined with clomiphene, tamoxifen, anastrozole, or an FSH analog — was associated with restoration of spermatogenesis in the large majority of men, on average within roughly four to five months.[9] Recovery time also depends on the testosterone formulation used and the duration of prior exposure, with transdermal-gel users in some series taking longer to recover than injectable users.[2]
It is worth being candid about the quality of this evidence too. Data on natural recovery of spermatogenesis after stopping TRT or AAS come largely from observational studies, and while most men do recover spontaneously over time, the timeframe is highly variable and depends on baseline testicular function, drug duration, and age.[6] HCG-based recovery protocols are widely used by fertility specialists and are supported by case series and reviews, but rigorous randomized trials remain scarce. This is a legitimate off-label medical use, guided by a reproductive specialist — not a do-it-yourself endeavor.
How does HCG monotherapy compare with simply replacing testosterone?
For a man with secondary hypogonadism who wants to preserve fertility, HCG monotherapy is a genuine alternative to conventional TRT. Rather than supplying testosterone from outside — which shuts down the testis — HCG stimulates the testis to make its own testosterone, keeping intratesticular androgen high and the testes functional. In appropriately selected men, HCG monotherapy can normalize serum testosterone and relieve hypogonadal symptoms while, unlike exogenous testosterone, maintaining testicular volume and sperm production.
There is also a physiological ceiling worth understanding. HCG supplies only the LH side of the equation; it does not replace FSH. In many men with partial gonadotropin deficiency, enough residual FSH remains that HCG-driven intratesticular testosterone is sufficient to sustain or restart spermatogenesis on its own. But in men with more complete gonadotropin deficiency — particularly congenital cases who never underwent normal puberty — FSH is often required in addition to HCG to achieve meaningful sperm output, which is exactly why fertility-induction regimens layer an FSH preparation on top of HCG rather than relying on HCG alone. HCG monotherapy, in other words, is a reasonable first step and is frequently sufficient for symptom control and testicular maintenance, but it is not guaranteed to maximize fertility in every man.
The trade-offs are real. HCG monotherapy requires frequent subcutaneous or intramuscular injections (often several times weekly), it can raise estradiol because the extra testosterone it generates is aromatized, and it depends on the testis being able to respond — it will not work in primary testicular failure, where the Leydig cells themselves are damaged. It is also more expensive and more complex to monitor than a standard testosterone gel or injection. For men who do not care about fertility and simply want symptom relief, conventional TRT is simpler; for men who prioritize fertility and testicular function, HCG-based approaches (with or without an SERM or FSH) are the fertility-sparing option. This is the essential fork in the road that the comparison below maps out.
HCG versus gonadorelin, enclomiphene, and clomiphene — how do they differ?
HCG is only one of several agents used to raise testosterone while trying to preserve the testis. They differ fundamentally in where on the HPG axis they act, which drives their advantages and limitations. Understanding this map is more useful than memorizing any single drug.
- HCG acts at the very bottom of the axis, directly on the Leydig-cell LHCGR — an LH mimic. It works even when the pituitary is fully suppressed, which is its defining strength.
- Gonadorelin is a GnRH (gonadotropin-releasing hormone) analog that acts at the top, on the pituitary, prompting it to release its own LH and FSH. Because native GnRH signaling is pulsatile, gonadorelin has a very short half-life and physiologically needs pulsatile delivery; continuous exposure paradoxically desensitizes the pituitary. It only works if the pituitary itself is intact.
- Enclomiphene is the trans-isomer of clomiphene, a selective estrogen receptor modulator (SERM). It blocks estrogen’s negative feedback at the hypothalamus and pituitary, so the brain increases its own LH and FSH output. It is oral, and it raises the man’s own gonadotropins rather than substituting for them.
- Clomiphene is the older, mixed-isomer SERM (containing both enclomiphene and the estrogenic zuclomiphene isomer), used off-label for male hypogonadism by the same feedback-blocking mechanism as enclomiphene.
The randomized evidence for the SERMs is worth noting because it directly parallels HCG’s fertility-sparing appeal. In a randomized phase II trial, Wiehle and colleagues showed that enclomiphene citrate raised serum testosterone comparably to a topical testosterone gel while preserving sperm concentration, whereas the testosterone-gel arm showed declining sperm counts.[10] A separate trial in obese hypogonadal men reported the same pattern — enclomiphene restored testosterone while maintaining sperm counts, unlike topical testosterone.[11] Both enclomiphene and HCG, therefore, offer a “restoration rather than replacement” strategy, but by opposite ends of the axis.
| Feature | HCG | Gonadorelin (GnRH analog) | Enclomiphene | Clomiphene |
|---|---|---|---|---|
| Class | Glycoprotein hormone (LH mimic) | GnRH analog / peptide | SERM (trans-isomer) | SERM (mixed isomer) |
| Site of action | Leydig-cell LHCGR (testis) | Pituitary GnRH receptor | Hypothalamus / pituitary (estrogen receptor) | Hypothalamus / pituitary (estrogen receptor) |
| Requires intact pituitary? | No | Yes | Yes | Yes |
| Route | Subcutaneous / intramuscular injection | Injection (needs pulsatile delivery) | Oral | Oral |
| Raises own LH/FSH? | No (substitutes for LH) | Yes (stimulates release) | Yes | Yes |
| Regulatory status (male) | FDA-approved for HH & cryptorchidism; TRT-adjunct is off-label | Off-label for male hypogonadism | Investigational / off-label in US | Off-label in US |
| Fertility-sparing rationale | Maintains intratesticular testosterone directly | Restores full gonadotropin drive | Preserves sperm counts in RCTs | Preserves gonadotropin output |
The regulatory column deserves emphasis: only HCG carries FDA approval for specific male indications, and even that approval does not extend to its most popular current use (TRT adjunct). Gonadorelin, clomiphene, and enclomiphene are all used off-label in this context in the United States. None of this is a ranking — the “best” agent depends entirely on the individual’s diagnosis, fertility goals, and whether the pituitary is functional, which is a determination for a clinician.
What dosing concepts appear in the clinical and research literature?
This section describes dosing only as it is reported in drug labels and published studies. It is a summary of the literature, not guidance for personal use, and the numbers vary widely by indication. Anyone considering HCG should do so under a physician’s supervision; a calculator such as the reconstitution and dosage calculator is an educational tool for understanding how vial concentrations translate to volumes, not a substitute for medical direction.
Several distinct dosing patterns appear across the literature, and they differ by an order of magnitude depending on the goal:
- Hypogonadotropic hypogonadism (label dosing): The Pregnyl label describes regimens such as 500–1000 units three times weekly, and higher-intensity schedules like 4000 units three times weekly for fertility-oriented courses, tapering thereafter.[3]
- TRT-adjunct / testicular preservation (research literature): The intratesticular-testosterone and cohort studies used notably lower doses — Coviello studied 125–500 IU every other day, and Hsieh used 500 IU every other day.[7][8] The Coviello data specifically showed that even these low doses maintained intratesticular testosterone in the normal range.[7]
- Post-androgen fertility recovery (review literature): Recovery protocols in the reviewed literature used higher doses, around 3,000 IU every other day, combined with a SERM or FSH analog, to restart suppressed spermatogenesis.[9]
The pattern that emerges from the literature is that “maintenance” of an already-functioning axis (as in TRT adjunct) uses small, frequent doses, whereas “induction” or “recovery” of a suppressed or immature axis uses larger doses over longer courses. The frequency of dosing — typically every other day or a few times weekly — reflects HCG’s long-but-finite half-life. Again, these figures are the published record; they are not a protocol for any reader to follow, and reconstituted concentration matters as much as the unit dose, which is where handling technique becomes relevant.
Which biomarkers are monitored during HCG therapy?
Whatever the indication, HCG therapy in the clinical literature is guided by laboratory monitoring rather than symptoms alone. The relevant biomarkers map directly onto the physiology discussed above.
Serum testosterone
Total (and sometimes free) testosterone is the first-line marker of whether HCG is driving Leydig-cell output effectively. Because HCG has a long half-life, timing of the blood draw relative to the last injection matters for interpretation. It is worth remembering, though, that serum testosterone is an imperfect proxy for the intratesticular concentration that actually governs fertility — a man can have adequate serum testosterone and still have suboptimal spermatogenesis.
Estradiol
HCG raises testosterone, and a portion of that testosterone is converted to estradiol by the enzyme aromatase. Rising estradiol is expected to some degree and is not automatically harmful, but excessive estradiol can produce gynecomastia and other estrogenic effects, which is why estradiol is monitored and sometimes managed alongside HCG.
Semen parameters
When fertility is the goal, semen analysis — sperm concentration, motility, and morphology — is the true outcome measure. It is the endpoint that matters in fertility-induction and recovery protocols, and it is the parameter Hsieh’s cohort tracked to conclude that HCG preserved spermatogenesis during TRT.[8] Sperm production responds slowly, over the roughly 70-plus-day cycle of spermatogenesis plus transit time, so semen parameters are reassessed over months, not weeks.
Testicular volume and inhibin B
Two markers specific to testicular function are useful in HCG therapy. Testicular volume, assessed by physical examination or ultrasound, is a practical readout of whether the testis is being adequately stimulated — testes shrink under androgen suppression and can regrow when Leydig-cell and Sertoli-cell activity is restored. Inhibin B, a peptide secreted by Sertoli cells, serves as a hormonal proxy for the health of the sperm-producing compartment and, as noted earlier, higher baseline inhibin B predicts better response to gonadotropin therapy. Together with semen analysis, these markers help distinguish a testis that is responding to HCG from one that cannot respond — a critical distinction, because HCG can only work if the testis itself is capable.
Hematocrit and other labs
Because HCG raises testosterone, it can raise hematocrit (red-cell concentration) just as exogenous testosterone can — an effect that must be watched to avoid erythrocytosis. General testosterone-therapy monitoring frameworks, such as the Endocrine Society’s clinical practice guideline on testosterone therapy, emphasize periodic assessment of hematocrit alongside testosterone and, where relevant, prostate-specific antigen in appropriate patients.[12] While that guideline addresses testosterone therapy specifically, the hematologic principle carries over to any intervention that meaningfully raises androgen levels.
What are the side effects and safety considerations?
HCG is generally well tolerated in clinical use, but it is not free of adverse effects, and most of them flow logically from the fact that it raises testosterone and, downstream, estradiol.
Gynecomastia and estrogenic effects
The most characteristic HCG-related concern is gynecomastia — breast tissue development — driven by aromatization of the extra testosterone into estradiol. Estrogen excess of any origin, including peripheral aromatization of androgens, can initiate breast-tissue proliferation, and gynecomastia is a recognized consequence of the estrogen shift.[13] Related estrogenic effects can include fluid retention and mood changes. Risk tends to be higher in men with more adipose tissue (fat is a site of aromatase activity) and when HCG is combined with other androgens.
Androgenic and other effects
Because HCG elevates testosterone, it can produce androgenic effects such as acne, oily skin, and — as noted — a rise in hematocrit. Injection-site reactions (pain, redness), headaches, and mood fluctuations are reported but generally mild and dose-related. In the pediatric cryptorchidism setting, the label specifically warns that HCG-induced androgen secretion may cause precocious puberty, and treatment should stop if signs of precocious puberty appear.[3]
Contraindications and rare risks
HCG is contraindicated in the presence of androgen-dependent malignancy (such as prostate cancer) and precocious puberty, per its labeling.[3] As a protein hormone, it can rarely provoke hypersensitivity reactions. The most familiar HCG-related syndrome — ovarian hyperstimulation — is specific to women undergoing ovulation induction and is not relevant to male use. Overall, the male safety profile in the published literature is favorable, but the combination of androgen elevation, estrogen elevation, and injection-based delivery means HCG is appropriately used with medical oversight and laboratory monitoring rather than casually.
How is HCG reconstituted and handled?
Pharmaceutical HCG is supplied as a lyophilized (freeze-dried) powder that must be reconstituted with a sterile diluent before use, and handling technique affects both potency and safety. The general principles — adding diluent slowly against the vial wall, avoiding vigorous agitation of a protein solution, and respecting cold-chain storage after reconstitution — apply to HCG as they do to other peptide and glycoprotein preparations. A detailed walkthrough of these steps is available in the peptide reconstitution guide, and the arithmetic of converting a vial’s total units into a per-dose volume can be worked through with a dosage calculator.
Two honesty points belong here. First, HCG is a protein and is sensitive to heat and mechanical stress; once reconstituted it generally requires refrigeration and has a limited shelf life, which is why bulk reconstitution and long storage are discouraged. Second — and this is the critical distinction for this site — material sold to laboratories as “research use only” HCG is not the FDA-approved pharmaceutical product studied in the clinical trials cited throughout this article. Research-grade material is not manufactured, tested, or labeled to pharmaceutical standards, its identity and purity are not guaranteed, and it is not intended for human administration. The clinical evidence discussed here applies to approved drug products used under medical supervision, and it cannot be assumed to transfer to unregulated research chemicals.
What are the limitations of the evidence?
An honest review has to be explicit about where the science is strong and where it is thin, because the strength of evidence varies dramatically across HCG’s different uses.
Strong, on-label evidence: HCG’s role in hypogonadotropic hypogonadism — both for raising testosterone and, combined with FSH, for inducing spermatogenesis and fertility — rests on decades of use, FDA approval, and consistent outcome data, with spermatogenesis induced in roughly 80 percent of men in combined-therapy reviews.[4] This is the firmest ground HCG stands on.
Plausible but limited, off-label evidence: The use of HCG to preserve fertility and testicular volume during TRT is mechanistically well-supported (Coviello’s direct intratesticular measurements) and clinically encouraging (Hsieh’s cohort), but the clinical data are observational and small, without randomized controlled confirmation.[7][8] Similarly, post-androgen fertility-recovery protocols rest largely on case series and reviews rather than randomized trials.[6]
Superseded on-label evidence: Cryptorchidism remains on the label but is no longer recommended by urologic guidelines, a reminder that regulatory approval and current best practice can diverge.[5]
Additional limitations cut across all uses: many of the informative studies are small, short in duration, or retrospective; HCG is frequently studied in combination with other agents (FSH, SERMs, aromatase inhibitors), which makes it hard to isolate its independent contribution; and much of the TRT-adjunct practice has outrun the controlled-trial evidence base. None of this means HCG “doesn’t work” — the physiology is sound and the on-label data are genuinely good — but it does mean readers should weight each claim according to the evidence behind it rather than treating all HCG uses as equally proven.
What is the honest bottom line on HCG for testosterone and fertility?
HCG is one of the few tools in male endocrinology that does exactly what its mechanism promises. As an LH mimic acting on the Leydig-cell LHCGR, it raises testosterone from inside the testis, and because intratesticular testosterone — not serum testosterone — is what spermatogenesis requires, HCG can accomplish something exogenous testosterone cannot: raise androgen levels while preserving fertility. For FDA-approved indications, particularly hypogonadotropic hypogonadism and gonadotropin-based fertility induction, the evidence is strong and HCG is a legitimate, guideline-consistent therapy.
For its most popular current use — adjunct to TRT to protect testicular volume and fertility — the rationale is compelling and the early data (Coviello’s intratesticular measurements, Hsieh’s cohort) are supportive, but the clinical evidence is observational and this use remains off-label. It is a reasonable, physician-supervised choice for men who want to keep their fertility options open on testosterone therapy, not a proven mandate. And throughout, the distinction between the approved pharmaceutical product and unregulated “research-grade” material is not a technicality: the clinical evidence applies only to the former.
The genuinely honest summary is this: HCG is well-established where it is approved, promising but not yet definitively proven where it is used off-label alongside TRT, and — like every hormone therapy — appropriate only within a monitored clinical relationship. Readers wanting to go deeper into the specific mechanism and protocols can review the HCG 5000 IU dosage protocol resource for context, while remembering that this article is educational and not a prescription. Those exploring adjacent endocrine and sexual-health compounds may also find the research summaries on sermorelin and growth-hormone secretion and on PT-141 and sexual dysfunction useful for a fuller picture of the field.
Frequently Asked Questions
Is HCG FDA-approved for men?
Yes, for specific indications. The FDA-approved label for chorionic-gonadotropin products such as Pregnyl lists two male uses: prepubertal cryptorchidism not caused by anatomical obstruction, and selected cases of hypogonadotropic hypogonadism due to pituitary deficiency. However, its widely discussed use as an adjunct to testosterone replacement therapy for fertility or testicular-volume preservation is off-label, meaning it is not among the approved indications even though it is used clinically.
Why does testosterone therapy cause infertility, and how does HCG help?
Exogenous testosterone suppresses the pituitary’s LH and FSH output, so the testes stop being stimulated and intratesticular testosterone — which is far higher than blood testosterone and is what sperm production needs — collapses. HCG mimics LH and stimulates the testicular Leydig cells directly, keeping intratesticular testosterone elevated even while the pituitary is suppressed. That is why co-administering HCG can preserve sperm production during testosterone therapy in observational studies.
How is HCG different from LH?
HCG and LH share an identical alpha subunit and act on the same LH/CG receptor, but HCG’s beta subunit carries extra sialic-acid-rich carbohydrate that gives it a much longer half-life. They are also biased agonists: at the same receptor, HCG shows stronger steroidogenic (testosterone-producing) signaling, while LH favors cell-survival pathways. Functionally, HCG behaves like a longer-acting, more steroidogenically potent version of LH.
How does HCG compare to enclomiphene or clomiphene?
They act at opposite ends of the HPG axis. HCG is an injectable LH mimic that stimulates the testis directly and works even if the pituitary is suppressed. Enclomiphene and clomiphene are oral SERMs that block estrogen feedback in the brain, prompting the pituitary to make more of the man’s own LH and FSH — so they require an intact pituitary. Both approaches can raise testosterone while preserving sperm production, but by different mechanisms.
Does HCG cause side effects like gynecomastia?
It can. HCG raises testosterone, and some of that testosterone is converted to estradiol by aromatase. Elevated estradiol can cause gynecomastia (breast tissue development), fluid retention, and mood changes, with higher risk in men who carry more body fat. Other possible effects include acne, a rise in hematocrit, and injection-site reactions. Estradiol and hematocrit are commonly monitored during therapy for this reason.
Is “research-grade” HCG the same as the prescription drug?
No. Material sold as “research use only” is not the FDA-approved pharmaceutical product studied in the clinical trials, is not manufactured or tested to pharmaceutical standards, and is not intended for human use. The clinical evidence discussed in this article applies to approved drug products used under medical supervision and cannot be assumed to apply to unregulated research chemicals. This article is educational and not a prescription.
Can HCG restore fertility after anabolic steroid use?
It is used for this purpose off-label. After stopping the offending androgen, HCG supplies the LH-like stimulus to reactivate dormant Leydig cells, often combined with a SERM or an FSH analog. Review literature describes restoration of spermatogenesis within roughly four months in the reported protocols, though recovery time varies with the drug used and duration of prior exposure, and the evidence is largely from case series rather than randomized trials.
How long does it take to see fertility results with HCG?
Longer than most people expect. Sperm production follows the roughly 70-plus-day cycle of spermatogenesis plus epididymal transit, so semen parameters are reassessed over months, not weeks. In hypogonadotropic hypogonadism, combined HCG-plus-FSH courses often run 12 to 24 months to induce spermatogenesis and achieve pregnancy. This slow timeline is why fertility-oriented HCG therapy is monitored with periodic semen analyses.
References
- Riccetti L, Casarini L, et al. Human luteinizing hormone and chorionic gonadotropin display biased agonism at the LH and LH/CG receptors. Scientific Reports. 2017. https://pmc.ncbi.nlm.nih.gov/articles/PMC5430435/
- Crosnoe LE, Grober E, Ohl D, Kim ED. Exogenous testosterone: a preventable cause of male infertility. Translational Andrology and Urology. https://pmc.ncbi.nlm.nih.gov/articles/PMC4708215/
- Pregnyl (chorionic gonadotropin for injection, USP) — FDA-approved prescribing information. U.S. Food and Drug Administration. https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/017692s028s036s043lbl.pdf
- Gonadotropin treatment for the male hypogonadotropic hypogonadism. PubMed (PMID 32445446). https://pubmed.ncbi.nlm.nih.gov/32445446/
- Kolon TF, et al. Evaluation and treatment of cryptorchidism: AUA guideline. Journal of Urology. 2014. https://www.auajournals.org/doi/10.1016/j.juro.2014.05.005
- Desai A, Yassin M, Cayetano A, Tharakan T, Jayasena CN, Minhas S. Understanding and managing the suppression of spermatogenesis caused by testosterone replacement therapy (TRT) and anabolic-androgenic steroids (AAS). Therapeutic Advances in Urology. 2022. https://pmc.ncbi.nlm.nih.gov/articles/PMC9243576/
- Coviello AD, Matsumoto AM, Bremner WJ, et al. Low-dose human chorionic gonadotropin maintains intratesticular testosterone in normal men with testosterone-induced gonadotropin suppression. Journal of Clinical Endocrinology & Metabolism. 2005;90(5):2595-2602. https://academic.oup.com/jcem/article-abstract/90/5/2595/2836735
- Hsieh TC, Pastuszak AW, Hwang K, Lipshultz LI. Concomitant intramuscular human chorionic gonadotropin preserves spermatogenesis in men undergoing testosterone replacement therapy. Journal of Urology. 2013;189(2):647-650. https://pubmed.ncbi.nlm.nih.gov/23260550/
- Wenker EP, Dupree JM, Langille GM, Kovac J, Ramasamy R, et al. The use of HCG-based combination therapy for recovery of spermatogenesis after testosterone use. The Journal of Sexual Medicine. 2015;12(6):1334-1337. https://academic.oup.com/jsm/article-abstract/12/6/1334/6980062
- Wiehle RD, Fontenot GK, Wike J, et al. Enclomiphene citrate stimulates testosterone production while preventing oligospermia: a randomized phase II clinical trial comparing topical testosterone. Fertility and Sterility. 2014. https://pubmed.ncbi.nlm.nih.gov/25044085/
- Kim ED, McCullough A, Kaminetsky J. Oral enclomiphene citrate raises testosterone and preserves sperm counts in obese hypogonadal men, unlike topical testosterone: restoration instead of replacement. BJU International. 2016. https://bjui-journals.onlinelibrary.wiley.com/doi/10.1111/bju.13337
- Bhasin S, Brito JP, Cunningham GR, et al. Testosterone therapy in men with hypogonadism: an Endocrine Society clinical practice guideline. Journal of Clinical Endocrinology & Metabolism. 2018;103(5):1715-1744. https://academic.oup.com/jcem/article/103/5/1715/4939465
- Gynecomastia: etiology, diagnosis, and treatment. Endotext (NCBI Bookshelf). https://www.ncbi.nlm.nih.gov/books/NBK279105/