Ovagen is one of the more obscure members of the so-called “peptide bioregulator” family, a group of very short synthetic peptides associated with the Russian gerontologist Vladimir Khavinson and the St. Petersburg Institute of Bioregulation and Gerontology. On vendor sites it is almost always described as a “liver peptide” said to normalize hepatic and gastrointestinal function. The chemistry behind the marketing name is simpler than the claims: Ovagen is the research-market label for the tripeptide Glu-Asp-Leu (abbreviated EDL), a three-amino-acid molecule that would fit comfortably inside a single turn of a protein. Understanding what this peptide is, and just as importantly what it is not, requires separating a genuinely interesting laboratory hypothesis from a much larger body of confident-sounding but unsupported marketing.
This article is a research-education overview. It walks through where Ovagen came from, the theoretical mechanism its originators proposed, what the peer-reviewed literature actually demonstrates (and the substantial gaps in it), how the compound is positioned relative to related bioregulators, and the practical and regulatory realities that surround it. The honest headline, stated up front, is this: Ovagen is not an approved drug anywhere, the rigorous independent evidence base is thin, and essentially all of the human-relevant claims circulating online extrapolate far beyond what has been demonstrated. Nothing here should be read as an endorsement, a protocol, or a suggestion that Ovagen treats, prevents, or cures liver disease or any other condition.
If you are researching Ovagen because you encountered it in the bioregulator ecosystem, the most useful thing this page can do is give you an accurate map: which claims trace back to real experiments, which are theoretical, and which are simply vendor copy. Throughout, claims are cited to primary sources where they exist, and flagged as unverified where they do not.
One more framing note before the details. The bioregulator category occupies an unusual position in the peptide landscape. Unlike well-studied research peptides that at least have a substantial preclinical literature, and unlike approved peptide drugs that have cleared regulatory review, the bioregulators sit in a space defined by an ambitious theory, a modest and largely single-source experimental record, and an outsized marketing presence. That combination is precisely the situation in which careful readers are most easily misled, because the confident tone of the marketing fills the vacuum left by the thin evidence. Reading Ovagen accurately is therefore as much an exercise in evidence literacy as it is in peptide chemistry.
What Ovagen Is and Where It Comes From
Ovagen is a synthetic tripeptide with the amino-acid sequence glutamic acid–aspartic acid–leucine, conventionally written Glu-Asp-Leu and abbreviated EDL using single-letter codes.1 A tripeptide is exactly what it sounds like: three amino acids joined by two peptide bonds. For scale, a small protein such as insulin has 51 residues; a typical antibody has well over a thousand. EDL sits at the extreme short end of the peptide spectrum, in the category researchers in this field call “short peptides” or “ultrashort peptides,” generally defined as chains of roughly two to seven amino acids.2 That size is central to both the theory behind Ovagen and the skepticism it attracts.
The intellectual lineage is specific and worth stating plainly. The peptide-bioregulator concept was developed largely by Vladimir Khavinson and colleagues at the St. Petersburg Institute of Bioregulation and Gerontology in Russia, building on Cold-War-era work extracting peptide fractions from animal organs.5,6 The original preparations were complex peptide mixtures isolated from specific tissues (thymus, pineal gland, and others). Over time the group proposed that within these extracts, short defined sequences carried the biological signal, and they synthesized a series of di-, tri-, and tetrapeptides intended to reproduce organ-specific effects. Epitalon (Ala-Glu-Asp-Gly), Vesugen (Lys-Glu-Asp), Livagen (Lys-Glu-Asp-Ala), and Ovagen (Glu-Asp-Leu) all belong to this designed family.2,6
It is important to distinguish two different products that share the “Ovagen” name in different markets. In the older Russian consumer-supplement context, “Ovagen” appears as a capsule-format “Cytogen” containing synthesized peptides marketed for liver and digestive support. In the modern research-chemical market, “Ovagen” is sold as a lyophilized powder in vials (commonly labeled 20 mg) representing the isolated EDL tripeptide for laboratory use. This article concerns the EDL tripeptide, because that is the defined chemical entity the scientific literature can actually address. When a claim is based only on the capsule product or on vendor description, that is noted.
Ovagen’s marketed target organ is the liver, with secondary claims around the gastrointestinal tract. In the Khavinson framework, each bioregulator is assigned a “home” tissue: Epitalon to the pineal gland, Cardiogen to the heart, Testagen to the reproductive axis, and so on. This tissue assignment is a theoretical construct rather than a demonstrated pharmacological property for most sequences. For Ovagen specifically, the liver designation appears to derive from the broader family logic and from related liver-peptide work, not from a large body of EDL-in-liver experiments — a nuance that matters when weighing the evidence, and one we return to below.
A striking and under-appreciated fact is that the single most cited peer-reviewed experimental paper on EDL is not about the liver at all. It is a 2017 study in the Bulletin of Experimental Biology and Medicine examining EDL’s protective effect in the kidney, not the liver.1 That mismatch — a “liver peptide” whose best-documented organ effect is renal — is a useful early signal that the marketing narrative and the published record are not tightly aligned. Researchers comparing Ovagen with its sibling compounds can find dosage-format context in our Ovagen 20 mg vial reference and the broader peptide dosage index, both of which frame these compounds strictly as research materials.
The Molecular Mechanism: How a Tripeptide Is Proposed to Work
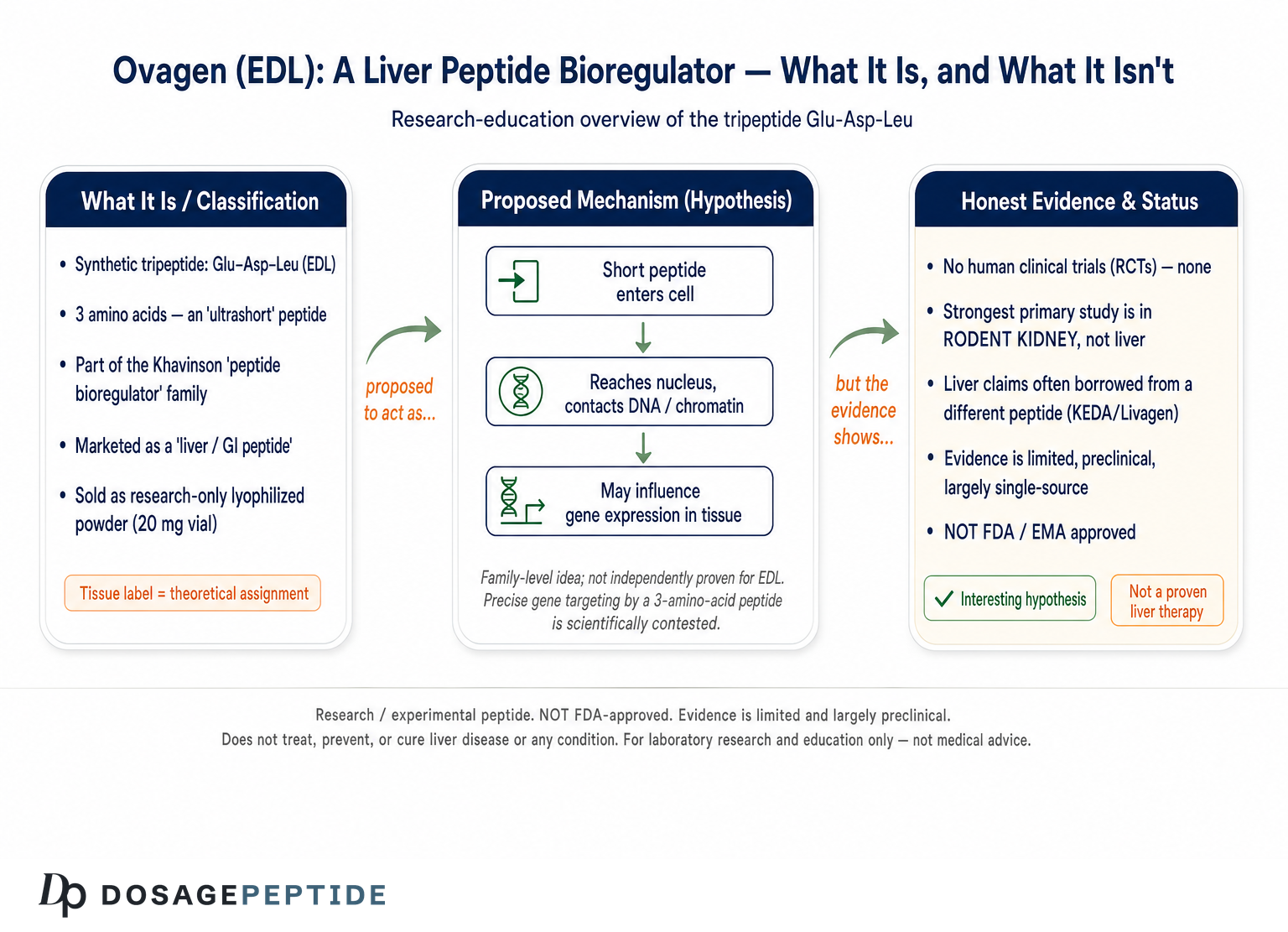
The mechanistic story attached to Ovagen is the same story attached to every Khavinson bioregulator, and it is genuinely interesting as a hypothesis. The core proposal is that short peptides act as endogenous gene-regulatory signals: they are small enough to enter cells, reach the nucleus, contact DNA or chromatin-associated proteins, and thereby influence which genes are transcribed.2,3 In this model, Ovagen would not act like a hormone binding a surface receptor, nor like a small-molecule drug inhibiting an enzyme, but as a kind of molecular tuning signal for gene expression in a specific tissue.
Several strands of laboratory work from the originating group support pieces of this picture in a general sense. Fluorescently labeled short peptides have been reported to penetrate into the nuclei and nucleoli of cultured cells and to associate with histones and with single- and double-stranded DNA.3 The group has published a molecular model in which a short peptide binds in the major or minor groove of DNA at particular sequences, proposing complementarity between specific amino-acid side chains and specific bases.2 They have also reported effects on DNA methylation and chromatin decondensation, framing the peptides as epigenetic modulators that can, for example, reactivate ribosomal genes silenced during cellular aging.4 A 2021 systematic review from the same lineage collates these observations into a unified “peptide regulation of gene expression” framework.2
For Ovagen (EDL) specifically, the tissue-targeting story is sometimes extended with a transport argument: because di- and tripeptides are substrates for the peptide transporters PEPT1 and PEPT2 (SLC15A1/2), which are highly expressed in the intestine, kidney, and liver, EDL could be preferentially taken up by exactly those tissues. This is a plausible-sounding molecular rationale, but readers should treat it with care — in the sources reviewed for this article it appears primarily in secondary and vendor material rather than in a dedicated EDL transport study, so it is best regarded as hypothesis rather than established fact.
| Proposed step | What the theory claims | Evidence status for EDL specifically |
|---|---|---|
| Cell/nuclear entry | Short peptide crosses membranes and reaches the nucleus | Shown for some short peptides as a class; not separately demonstrated for EDL in the reviewed primary literature |
| DNA/chromatin contact | Sequence-specific binding to DNA groove or histones | Modeled and reported for the class; EDL-specific binding data are limited |
| Gene-expression change | Up- or down-regulation of tissue-relevant genes | Reported at the family level; direct EDL liver-gene datasets are scarce |
| Tissue targeting | PEPT1/PEPT2 transport concentrates EDL in liver, gut, kidney | Mechanistically plausible; largely inferential, not directly proven for EDL |
| Functional outcome | Normalized organ function, antioxidant support, tissue repair | Best documented for EDL in a kidney-injury model, not the liver |
It is worth being explicit about the scientific tension here. A three-amino-acid peptide has very little surface area with which to achieve sequence-specific DNA recognition — the kind of specificity that transcription factors accomplish with large, structured DNA-binding domains. Critics of the bioregulator model point out that the proposed “one tripeptide, one gene-regulatory outcome” specificity is difficult to reconcile with basic biophysics, and that many of the supporting studies come from a small number of affiliated laboratories rather than independent replication.2,5 None of this proves the mechanism is wrong, but it explains why mainstream molecular biology has not adopted it and why the appropriate posture is curiosity paired with skepticism.
It also helps to contrast this proposed mechanism with how mainstream biology explains gene regulation. In conventional molecular biology, sequence-specific control of transcription is carried out by proteins — transcription factors — that fold into elaborate three-dimensional domains presenting many contact points to a stretch of DNA, achieving specificity through dozens of coordinated interactions. A tripeptide has neither the size nor the structural complexity to reproduce that. Proponents answer that short peptides need not act as classical transcription factors at all; they might modulate chromatin packaging, methylation status, or the activity of larger regulatory complexes rather than reading a gene directly.4 That is a reasonable reframing, but it also loosens the tidy “one peptide targets one gene” narrative that makes the marketing so appealing, replacing it with something far less specific and far harder to pin to a particular organ outcome.
The practical upshot for anyone evaluating Ovagen is that the mechanism is theoretical and largely generic to the family. When a vendor asserts that “Ovagen switches on liver detoxification genes,” they are describing a hypothesis about how the whole class might work, dressed up as an established fact about this one molecule. The distance between those two statements is the entire subject of the next section.
What the Evidence Actually Shows (An Honest Assessment)
This is the section that matters most, so it is worth stating the conclusion before the details: for Ovagen/EDL, the directly relevant, peer-reviewed, independent human evidence is effectively zero, and even the preclinical animal evidence that exists is thin, largely single-source, and not primarily about the liver. Everything beyond that is extrapolation.
The strongest single piece of primary evidence is the 2017 nephroprotection study by Zamorskii and colleagues, published in the Bulletin of Experimental Biology and Medicine.1 In that work, EDL peptide was tested in rat models of acute kidney injury — gentamicin-induced nephropathy and ischemia/reperfusion injury. The authors reported that EDL administration was associated with prevention of oliguria and retention azotemia, reduced proteinuria and sodium excretion, preservation of antioxidant enzyme activity, suppression of lipid peroxidation, and improved cellular energy supply in the kidney. Taken at face value, this is a coherent preclinical antioxidant/organ-protection signal. But note carefully: it is a rodent study, in the kidney, from a laboratory within the bioregulator research lineage, and it does not establish anything about liver function or about effects in humans.
For the liver claim specifically, the picture is weaker still. Much of the “liver evidence” cited for Ovagen actually belongs to related but different compounds — most notably the tetrapeptide KEDA (Lys-Glu-Asp-Ala, marketed as Livagen) and complex liver-peptide preparations, which have been evaluated in animal models of liver fibrosis and hepatitis and reviewed as putative hepatoprotectors.7 That KEDA work is frequently borrowed to imply that EDL does the same thing. It may or may not; they are not the same molecule, and evidence for one tripeptide/tetrapeptide does not transfer to another. Conflating them is one of the most common errors in Ovagen marketing.
The broader family-level literature — reviews and mechanistic papers on short-peptide gene regulation, epigenetics, and cell differentiation2,3,4,9 — is real and peer-reviewed, but it is exactly that: family-level and mechanistic. It supports the general research program that short peptides can influence gene expression in model systems. It does not demonstrate that Ovagen produces clinically meaningful liver benefits in any organism, and certainly not in people. Reviews of the wider Khavinson program report life-span and biomarker effects for a few specific preparations (notably Thymalin and Epithalamin/Epitalon) in rodents and in some human cohorts,5,6 but those results belong to those compounds, not to EDL.
| Evidence type | Available for Ovagen/EDL? | Notes |
|---|---|---|
| Randomized controlled human trials | None found | No Phase I/II/III trials in registries or the peer-reviewed record |
| Non-randomized human/clinical data | None specific to EDL | Human bioregulator data exist for other compounds, not EDL |
| Animal studies (liver) | Very limited / indirect | Liver-model data mostly concern KEDA and liver-peptide complexes |
| Animal studies (other organs) | Yes — kidney | 2017 rat nephroprotection study is the key primary EDL paper |
| In vitro / mechanistic | Family-level | Short-peptide gene-expression and epigenetic work, not EDL-liver specific |
| Independent replication | Largely absent | Most work traces to affiliated laboratories |
Two additional claims deserve direct comment because they circulate widely. The first is that Ovagen has “anti-aging” or telomere-extending properties. That claim is imported wholesale from Epitalon research and has no EDL-specific basis. The second is that EDL inhibits HIV-1 protease and could affect viral replication. This appears in vendor copy and in secondary summaries, sometimes with a specific inhibition constant. In the sources reviewed here, this is not supported by a solid, EDL-specific, independently reproduced primary study, and it should be treated as unverified at best. Presenting an antiviral capability for a liver “wellness” tripeptide, on that evidentiary basis, is exactly the kind of overreach research readers should learn to spot.
It is worth pausing on why “one respectable rodent paper” is such a low rung on the evidence ladder, because the point generalizes. The history of drug development is littered with compounds that produced clean, encouraging results in animal-injury models and then failed in humans — neuroprotectants that rescued rodent brains but did nothing in stroke trials, antioxidants that looked protective in dishes and neutral or harmful in people. Animal organ-protection signals are a reason to run the next experiment, not a reason to believe the human result is in hand. For Ovagen, the “next experiment” — a proper human trial — has never been run and reported, so the chain of inference simply stops at the rodent kidney.
A further complication specific to this compound is the frequent slippage between the branded capsule “Cytogen” product and the isolated EDL tripeptide. Some of the reassuring-sounding usage history attached to Ovagen refers to the older consumer capsule sold in Russia, which is a different formulation used in a different context. Consumer availability is not evidence of efficacy, and a product having been sold for years tells you nothing about whether it works — only that it has not been conspicuously dangerous enough to be pulled. Folding decades of capsule sales into the EDL research narrative is another way the perceived evidence base gets inflated beyond what the controlled studies support.
The honest bottom line: Ovagen is an interesting laboratory hypothesis with one respectable rodent organ-protection paper (in the kidney), embedded in a larger family research program of mixed independent standing. It is not a demonstrated liver therapy. Anyone stating otherwise is ahead of the data.
How Ovagen Compares With Related Bioregulators
Ovagen is easiest to understand in the context of its siblings, because the entire class shares a design philosophy, a manufacturing origin, and an evidentiary profile. The differences between members are mostly the amino-acid sequence and the assigned target tissue; the similarities — short length, gene-regulation hypothesis, limited independent human data — run deeper than the differences.
The most direct comparison is Livagen, the tetrapeptide KEDA (Lys-Glu-Asp-Ala). Livagen is also positioned as a liver bioregulator, and confusingly it has arguably more published liver-model support than Ovagen does, thanks to the hepatoprotection reviews of the KEDA peptide and liver-peptide complexes.7 If someone’s interest is specifically the “liver bioregulator” concept, Livagen is the compound with the somewhat larger (though still limited and largely single-source) liver-specific literature. Our Livagen 20 mg vial reference covers that compound’s research-context framing in parallel with Ovagen’s.
| Compound | Sequence | Assigned tissue | Relative evidence note |
|---|---|---|---|
| Ovagen | Glu-Asp-Leu (EDL, tripeptide) | Liver / GI | Key primary paper is renal; liver data indirect |
| Livagen | Lys-Glu-Asp-Ala (KEDA, tetrapeptide) | Liver | More liver-model literature, still single-lineage |
| Vesugen | Lys-Glu-Asp (KED, tripeptide) | Vascular | Family-level mechanistic claims |
| Cardiogen | Ala-Glu-Asp-Arg (AEDR, tetrapeptide) | Heart / myocardium | Family-level, limited independent data |
| Testagen | Lys-Glu-Asp-Gly (tetrapeptide) | Reproductive axis | Family-level, limited independent data |
| Epitalon | Ala-Glu-Asp-Gly (AEDG, tetrapeptide) | Pineal / systemic | Largest research base of the group (telomere/aging) |
Several structural observations are worth making. Notice that these sequences are combinatorially close: Glu-Asp appears repeatedly, and single-residue swaps distinguish several “different” compounds. This is by design in the Khavinson model, where each small change is proposed to redirect the peptide to a different gene or tissue. It also means that experimental results for one sequence are frequently — and improperly — generalized to neighbors. A reader who understands that EDL, KED, KEDA, and AEDG are treated by the field as distinct molecules with distinct (and mostly unproven) tissue assignments is already better equipped than most marketing copy.
How does the class compare with mainstream, evidence-backed peptides? The contrast is stark. Regulated peptide drugs — insulin, GLP-1 receptor agonists, and others — have defined receptors, dose-response data, large randomized trials, and regulatory approval. Even among “research peptides” with more traction, such as those studied for tissue repair, the evidence base dwarfs anything available for Ovagen. Placing Ovagen on that spectrum, it sits at the far speculative end: a designed short peptide with an elegant hypothesis and comparatively little to show for it in rigorous, independent, human-relevant testing. Readers exploring the broader family for research context may also find our overviews of related compounds useful, including Prostamax, Testagen, and Cardiogen, each framed strictly for laboratory education.
The comparison also clarifies a marketing tactic to watch for: “stacking.” Because the compounds are cheap to synthesize and share a family story, vendors often promote using several bioregulators together. From an evidence standpoint, combining multiple compounds whose individual effects are unproven does not produce proven combined effects; it multiplies uncertainty. Our peptide-stack reference exists to document how such combinations are discussed in the research-chemical market, not to endorse them.
Research Models and Methodology
Understanding how bioregulator peptides are studied helps explain why the evidence feels simultaneously suggestive and unsatisfying. The methods used are legitimate laboratory techniques; the limitation is in scale, independence, and translation to humans.
The animal work, exemplified by the 2017 EDL nephroprotection study, typically follows a classic organ-injury-and-rescue design.1 Researchers induce a defined injury in rodents — a nephrotoxin like gentamicin, or a surgical ischemia/reperfusion insult — then administer the peptide and measure functional and biochemical endpoints against untreated injured controls. Endpoints include urine output, blood markers of organ function (for kidney, markers of azotemia; for liver studies of related compounds, transaminases and histology), oxidative-stress measures such as lipid-peroxidation products, and antioxidant-enzyme activities. These are reasonable, interpretable readouts. The recurring caveats are small group sizes, short durations, administration routes and doses that may not map onto human exposure, and the concentration of such studies within a small network of affiliated laboratories.
The in vitro and mechanistic work uses cell cultures and molecular-biology assays: fluorescently tagged peptides tracked into nuclei by microscopy; chromatin-structure assessments; DNA-methylation and gene-expression measurements after peptide exposure; and computational or biophysical modeling of peptide–DNA interactions.2,3,4 Some of this is done with human cells, including studies of chromatin decondensation in lymphocytes from elderly donors, which is where much of the “epigenetic rejuvenation” language originates.4 Again, these are real experiments. The gap is between “a short peptide altered chromatin or gene expression in a dish” and “Ovagen improves liver health in a living human,” which spans several validation stages that have not been completed.
| Model tier | Typical methods | What it can and cannot show |
|---|---|---|
| Molecular / biophysical | Peptide–DNA binding models, fluorescence tracking | Can suggest a mechanism; cannot show clinical benefit |
| Cell culture (in vitro) | Gene expression, methylation, chromatin assays | Can show cellular effects; translation is unproven |
| Animal (in vivo) | Injury-rescue designs, biochemical/histologic endpoints | Can show organ effects in rodents; not human proof |
| Human observational | Cohort follow-up (for other bioregulators) | Hypothesis-generating; confounded; not EDL-specific |
| Randomized controlled trials | Blinded, placebo-controlled human trials | The standard for efficacy — absent for Ovagen |
A recurring methodological weakness across the bioregulator literature is the scarcity of independent, adversarial replication. In robust areas of biomedicine, an interesting finding from one group is stress-tested by competing labs with different incentives. For Ovagen and its siblings, most of the supporting literature originates from or is closely tied to the founding institute and its collaborators. That does not make the results false, but it lowers the confidence a careful reader should assign, because publication within a like-minded network is more vulnerable to unrecognized bias, optimistic interpretation, and non-publication of negative results.
Another methodological subtlety concerns endpoints. Many bioregulator studies report changes in intermediate biomarkers — enzyme activities, gene-expression levels, chromatin appearance — rather than hard clinical outcomes. Intermediate markers are useful for probing mechanism, but they are notoriously unreliable as stand-ins for benefit. A marker can move in the “right” direction without any corresponding improvement in how an organ or organism actually functions, and the medical literature contains many cautionary examples where a biomarker improved while patient outcomes did not, or even worsened. When Ovagen material cites a change in a liver-related gene or an antioxidant enzyme, that is a mechanistic observation, not a demonstration that liver function improved in a way that would matter to a living organism.
Sample size and statistical power are worth a mention too. Rodent bioregulator studies typically use small groups, which makes them prone both to false positives (a chance difference reaching significance) and to false negatives (a real effect missed). Small studies also tend to overestimate the magnitude of any true effect, a well-documented phenomenon. None of this is unique to Ovagen — it is a general feature of early preclinical work — but it means the individual numbers reported in these papers should be held loosely, as directional hints rather than precise quantities.
For a research reader, the practical methodological lesson is to always ask three questions of any Ovagen claim: Which exact molecule was tested (EDL, or a relative)? Which organism and model (dish, rat, or human)? And who ran and funded the study? In the great majority of Ovagen claims encountered online, at least one of those answers quietly undermines the confident wording of the claim itself.
Safety and Tolerability: What Is and Is Not Known
Safety is an area where the absence of evidence is frequently misread as evidence of safety. For Ovagen, there is no adequate human safety database — no completed clinical trials, no pharmacovigilance system capturing adverse events, and no regulatory safety review. What can be said honestly is narrow.
On general principles, very short peptides composed of standard amino acids are often expected to have modest acute toxicity, because they are chemically similar to fragments produced during ordinary protein digestion and are subject to rapid enzymatic breakdown by peptidases. The available animal studies of EDL and related bioregulators do not, in the reviewed literature, report dramatic acute toxicity at the doses tested.1,5 That is a weak reassurance, not a strong one: rodent studies at particular doses over short periods cannot characterize the risks that matter for humans, such as rare hypersensitivity reactions, effects of chronic exposure, immunogenicity, drug interactions, or consequences in people with existing liver, kidney, or immune disease.
Several category-level risks deserve emphasis for anyone handling these materials in a research setting:
| Risk domain | Concern | Status |
|---|---|---|
| Product identity/purity | Research-market vials may vary in actual content, purity, and endotoxin load | No standardized oversight; third-party analysis not guaranteed |
| Contamination | Non-sterile powder, bacterial endotoxin, residual synthesis reagents | Real risk with unregulated supply chains |
| Immunogenicity | Even short peptides can, in principle, provoke immune responses | Uncharacterized for EDL in humans |
| Chronic/long-term effects | No long-duration human data | Unknown |
| Special populations | Liver/kidney disease, pregnancy, immune disorders, concomitant drugs | Not studied; unknown |
The contamination and identity concerns are not hypothetical. Because Ovagen is sold as a research chemical outside any pharmaceutical quality system, what is in a given vial is only as reliable as the individual supplier’s (often unverifiable) claims. Independent testing of grey-market peptides across the industry has repeatedly found discrepancies between labeled and actual content. A tripeptide that is theoretically low-risk becomes a genuinely uncertain risk once it is manufactured, filled, and shipped without enforceable standards.
It also bears stating clearly that “natural,” “bioidentical,” or “just a peptide your body already makes” framings do not establish safety. The relevant question is not whether a molecule sounds benign but whether it has been tested, in the relevant population, at the relevant exposure, with systematic adverse-event capture. For Ovagen, it has not. The correct summary is therefore: no serious toxicity is documented in the limited animal work, and simultaneously the human safety profile is fundamentally unknown. Both halves of that sentence are true and neither should be dropped.
A specific caution applies to anyone with actual liver concerns, since that is Ovagen’s marketed target. Impaired liver function alters how the body handles many substances, and someone with liver disease is precisely the person for whom an unstudied, unpurified, unapproved compound carries the greatest uncertainty. It is a genuine irony of the marketing that the population most likely to be drawn to a “liver peptide” is the population for whom the absence of safety data is most consequential. The responsible course for any real liver concern is evaluation and management by a qualified clinician using established, evidence-based options — not experimentation with a research chemical.
Finally, because Ovagen is often discussed alongside injectable-format peptides, note that any parenteral use of a non-sterile, non-approved product introduces infection and injection-site risks entirely separate from the molecule’s intrinsic pharmacology. Those are handling risks, not evidence of therapeutic value, and they weigh against casual experimentation.
Handling and Reconstitution in a Research Context
This section describes how lyophilized research peptides are handled in laboratory settings for completeness and accuracy. It is descriptive, not instructional encouragement: Ovagen is not an approved product for human use, and nothing here should be read as guidance to administer it to anyone.
Research-market Ovagen typically ships as a lyophilized (freeze-dried) white powder in a sealed vial, commonly labeled 20 mg, sometimes with mannitol or another bulking/cryoprotectant excipient. Lyophilized short peptides are generally more stable than solutions, and the dry powder is usually stored cold — refrigerated for short periods and frozen (for example around −20 °C, or colder for long-term storage) to limit hydrolysis and microbial growth — protected from light and moisture. Repeated warming and refreezing is avoided because freeze–thaw cycling can degrade peptides.
In laboratory protocols, reconstitution means dissolving the powder in an appropriate sterile diluent, most often bacteriostatic or sterile water, added slowly down the vial wall rather than forcefully onto the powder, then allowed to dissolve without vigorous shaking. The resulting concentration is simply the mass of peptide divided by the volume of diluent; reconstituted solutions are kept refrigerated and are far less stable than the dry powder, so they are typically used within a limited window. These are standard bench practices for handling any lyophilized peptide and say nothing about whether a given peptide is safe or effective to use.
| Parameter | Typical laboratory handling of lyophilized peptides |
|---|---|
| Physical form | Freeze-dried powder in sealed vial |
| Dry storage | Cold and dark; frozen for longer-term storage; moisture-protected |
| Diluent | Sterile / bacteriostatic water added gently to the vial wall |
| Mixing | Swirl gently; avoid vigorous shaking and foaming |
| Reconstituted storage | Refrigerated; short usable window; avoid freeze–thaw cycles |
| Concentration | Peptide mass ÷ diluent volume |
Two honesty points close this section. First, the existence of neat reconstitution math and tidy storage tables can create a false impression of legitimacy — the same professional-looking numerical presentation surrounds compounds with real evidence and compounds with none, so tidy dosing charts are not a proxy for efficacy. Second, none of these handling details resolve the fundamental identity and purity uncertainty discussed under safety: careful technique with an unverified powder still yields an unverified solution. For a purely research-oriented, format-level reference to how Ovagen vials are described in the market, see our Ovagen vial page, which is presented for laboratory education only.
Limitations and the Human-Evidence Gap
Every preceding section has pointed toward one conclusion, and it deserves a dedicated treatment: the gap between what is claimed for Ovagen and what has been demonstrated in humans is not a small gap to be bridged with a little more research — it is essentially the whole distance. As of this writing, there is no published randomized controlled trial of Ovagen/EDL in humans for any indication, no registered clinical trial establishing efficacy for liver function, and no regulatory body anywhere that has reviewed and approved it as a drug.
Consider what a credible human efficacy claim would require. It would need at least one adequately powered, randomized, placebo-controlled trial in the relevant population — say, people with a defined liver condition — measuring meaningful clinical endpoints (not just a biomarker moving in a dish), with pre-registered outcomes, independent conduct, and ideally replication by a second group. Ovagen has none of these. What it has is a rodent kidney study, a family of mechanistic papers about short peptides in general, borrowed liver data from a chemically distinct sibling, and a large volume of confident marketing that treats all of the above as if it were the missing clinical trial.
The specific ways the evidence falls short are worth enumerating so they can be recognized elsewhere:
| Gap | Why it matters |
|---|---|
| No human trials | Animal and cell effects routinely fail to translate to people |
| Wrong-organ primary data | The strongest EDL study is renal, not hepatic |
| Borrowed evidence | Liver claims lean on KEDA/other peptides, not EDL |
| Single-lineage sourcing | Little independent, adversarial replication |
| Biomarker ≠ benefit | Gene-expression changes are not proven clinical outcomes |
| Publication/selection bias | Negative results in this niche are rarely published |
There is also a subtler limitation: the bioregulator field’s central mechanistic claim — sequence-specific gene regulation by tripeptides — remains outside the biological mainstream and has not been independently validated to the standard that would move it from intriguing hypothesis to accepted mechanism.2,5 When the proposed mechanism is itself unsettled, downstream efficacy claims inherit that uncertainty. A reader is entitled to remain interested in the research program while declining to accept its conclusions as established.
The constructive framing is that Ovagen is a candidate hypothesis, not a validated intervention. Candidate hypotheses are valuable — they motivate careful experiments — but they are precisely the things that should not be marketed to the public as functional health products. Keeping that distinction sharp is the single most protective habit a research reader can develop, and it applies well beyond this one compound.
Regulatory Status
Ovagen’s regulatory position is straightforward and unambiguous: it is not an approved drug. It has no U.S. Food and Drug Administration approval, no European Medicines Agency authorization, and no marketing authorization as a medicine in the jurisdictions relevant to most readers. It is neither a licensed pharmaceutical nor an established dietary-supplement ingredient with a recognized safety history; in practice it is sold as a “research chemical,” “for laboratory research use only,” a label that explicitly signals it is not intended for human consumption or medical use.
The broader regulatory environment for peptides has been unusually active recently, and it is worth situating Ovagen within it. In the United States, the FDA regulates compounding pharmacies under sections 503A and 503B of the Federal Food, Drug, and Cosmetic Act, and maintains lists of bulk drug substances that may or may not be used in compounding.10 In 2023 the agency placed a number of peptides into “Category 2” of the 503A list, a designation reserved for substances judged to raise significant safety concerns, which effectively blocked their use in compounding. In 2026 the FDA announced procedural changes — removing several peptides from Category 2 after nominations were withdrawn and scheduling Pharmacy Compounding Advisory Committee meetings to consider a small number of peptides for the permitted bulks list. Crucially, none of this regulatory churn constitutes drug approval: removal from a compounding-restriction category is a procedural step, not an FDA finding of safety and efficacy, and it does not create an approved product.
| Jurisdiction / framework | Ovagen status |
|---|---|
| FDA approved drug (NDA/BLA) | No — not approved |
| EMA authorized medicine | No |
| Recognized dietary supplement ingredient | No established status |
| 503A/503B compounding bulks list | Not an approved compounding substance |
| Typical market label | “Research use only” / research chemical |
The practical significance of “research use only” status is often underestimated. It means the product falls outside the quality, labeling, and safety obligations that apply to medicines and, in many respects, to supplements. There is no guarantee that the vial contains what the label says, in the amount stated, at any particular purity, free of contaminants. There is no approved indication, which is why legitimate educational material — including this article — cannot and does not tell you that Ovagen treats anything. And marketing that presents a research chemical as a solution for liver health is making claims the regulatory system has specifically not endorsed.
Regulatory status can also differ by country and can change over time, so the specifics above should be read as a snapshot rather than permanent fact. What is very unlikely to change quickly is the core reality: absent completed clinical trials and a formal approval process, Ovagen will remain an experimental, non-approved compound. That status is the appropriate frame for every other statement on this page.
Frequently Asked Questions
What is Ovagen in simple terms?
Ovagen is the research-market name for a synthetic tripeptide, Glu-Asp-Leu (EDL), one of the short “peptide bioregulators” associated with the Khavinson research program in Russia.1,2 It is marketed as a “liver peptide,” but that label reflects a theoretical tissue assignment and marketing convention more than a proven, liver-specific clinical effect. It is not an approved medicine and is sold for laboratory research only.
Does Ovagen actually improve liver health?
There is no reliable evidence that Ovagen improves liver health in humans. No randomized controlled human trials exist for this compound, and its strongest single primary study is actually a rodent kidney-protection experiment, not a liver study.1 Much of the “liver evidence” attributed to Ovagen belongs to a different peptide, KEDA/Livagen.7 Claims that it treats or protects the liver are unsupported.
How is Ovagen supposed to work?
The proposed mechanism is that very short peptides can enter cells, reach the nucleus, contact DNA or chromatin, and influence gene expression in a tissue-specific way.2,3,4 This is a genuine research hypothesis supported by family-level laboratory data, but it is not independently established as a mechanism for Ovagen specifically, and the idea that a three-amino-acid peptide achieves precise gene targeting is scientifically contested.
Is Ovagen FDA approved or legal to use?
Ovagen is not FDA approved and has no approval from other major regulators.10 It is typically sold as a “research use only” chemical, which is not intended for human consumption. Recent FDA activity around peptide compounding lists is procedural and does not represent approval of Ovagen or a finding that it is safe and effective.
How does Ovagen differ from Livagen?
They are different molecules. Ovagen is the tripeptide EDL (Glu-Asp-Leu); Livagen is the tetrapeptide KEDA (Lys-Glu-Asp-Ala).1,7 Both are marketed as liver bioregulators, but Livagen has somewhat more liver-model literature, though still limited and largely from the same research lineage. Evidence for one does not transfer to the other.
Is Ovagen safe?
Its safety in humans is unknown. There are no completed human safety trials, no pharmacovigilance data, and no regulatory safety review. Limited animal studies do not report dramatic acute toxicity at tested doses,1 but that does not establish human safety, and research-market products carry additional risks of impurity, contamination, and mislabeling because they are made outside pharmaceutical quality systems.
Can Ovagen treat HIV or slow aging?
No. The occasional claims that EDL inhibits HIV protease or produces anti-aging/telomere effects are not supported by solid, EDL-specific, independently reproduced evidence; the anti-aging language is largely borrowed from research on a different peptide, Epitalon. These claims should be treated as unverified marketing rather than established science.
Why do research sites list dosages if it is not approved?
Dosage and reconstitution references describe how the compound is handled and discussed in the research-chemical market; they are educational and format-oriented, not medical instructions or endorsements. Tidy dosing charts do not imply that a compound is proven safe or effective. Ovagen remains experimental, and our references frame it strictly for laboratory education.
Educational and Research-Only Disclaimer
This article is provided for educational and informational purposes only and describes a compound that is experimental, not approved by the FDA or other major regulators, and sold for laboratory research use only. Nothing here is medical advice, and nothing here should be interpreted as a claim that Ovagen (EDL) diagnoses, treats, cures, prevents, or improves any disease or health condition, including any liver or gastrointestinal condition. The evidence base for Ovagen is limited, largely preclinical, and in important respects indirect; human clinical evidence is absent. Do not use Ovagen or any research chemical on yourself or others. If you have questions about liver health or any medical concern, consult a qualified, licensed healthcare professional. References below point to the primary and regulatory sources cited throughout; readers are encouraged to consult them directly and to interpret all claims with appropriate scientific caution.
References
- Zamorskii II, Shchudrova TS, Lin’kova NS, Nichik TE, Khavinson VKh. Nephroprotective Effect of EDL Peptide at Acute Injury of Kidneys of Different Genesis. Bulletin of Experimental Biology and Medicine. 2017;163(4):389–393. PMID: 28744634. https://pubmed.ncbi.nlm.nih.gov/28744634/
- Khavinson VKh, Popovich IG, Linkova NS, Mironova ES, Ilina AR. Peptide Regulation of Gene Expression: A Systematic Review. Molecules. 2021;26(22):7053. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8619776/
- Khavinson V, Diomede F, Mironova E, Linkova N, Trofimova S, Trubiani O, Caputi S, Sinjari B. AEDG Peptide (Epitalon) Stimulates Gene Expression and Protein Synthesis during Neurogenesis: Possible Epigenetic Mechanism. Molecules. 2020;25(3):609. https://www.mdpi.com/1420-3049/25/3/609
- Ashapkin VV, Linkova NS, Khavinson VKh, Vanyushin BF. Epigenetic Mechanisms of Peptidergic Regulation of Gene Expression during Aging of Human Cells. Biochemistry (Moscow). 2015;80(3):310–322.
- Anisimov VN, Khavinson VKh. Peptide bioregulation of aging: results and prospects. Biogerontology. 2010;11(2):139–149.
- Khavinson VKh. Peptide bioregulators: a new class of geroprotectors. Results of experimental studies. Advances in Gerontology. 2013. PMID: 23734519. https://pubmed.ncbi.nlm.nih.gov/23734519/
- Kuznik BI, Khavinson VKh, Linkova NS, et al. The influence of polypeptide liver complex and tetrapeptide KEDA (Livagen) on physiological function in norm and age-related pathology. Advances in Gerontology. 2020;33(1):159–164.
- Khavinson VKh, Lin’kova NS, et al. Short Peptides Regulate Gene Expression. Bulletin of Experimental Biology and Medicine. 2016;162(2):288–292. doi:10.1007/s10517-016-3596-7.
- Khavinson VKh, Linkova NS, et al. Peptide Regulation of Cell Differentiation. Stem Cell Reviews and Reports. 2020. PMID: 31808038. https://pubmed.ncbi.nlm.nih.gov/31808038/
- U.S. Food and Drug Administration. Bulk Drug Substances Used in Compounding Under Section 503A of the FD&C Act. https://www.fda.gov/drugs/human-drug-compounding/bulk-drug-substances-used-compounding-under-section-503a-fdc-act