The title of this article asks about “key findings” on retatrutide for managing obesity and metabolic health, and the phrasing deserves a moment of scrutiny before we dive in. It could be read to imply that retatrutide is an established treatment whose place in obesity management is settled — a therapy you might reasonably expect a clinician to prescribe. That is not the situation as of mid-2026. Retatrutide (development code LY3437943) is an investigational triple-hormone-receptor agonist. It is not approved by the U.S. Food and Drug Administration, the European Medicines Agency, or any comparable regulator for obesity, for type 2 diabetes, or for any other indication. It cannot legally be marketed or prescribed as a treatment for those conditions.3
So the honest framing is this: retatrutide has generated some of the most striking metabolic trial data seen in a generation, and that data is genuinely strong and worth reporting accurately. But “strong phase-2 data” and “approved therapy” are different things, and the gap between them is where most of the important caveats live. The largest and longest randomized results are still emerging; the pivotal cardiovascular-outcomes trial that will tell us whether the weight loss translates into fewer heart attacks and strokes is years from reporting; and the durability question — what happens when people stop — is answered mostly by analogy to older drugs rather than by retatrutide’s own long-term record.
This piece is written for researchers and scientifically literate readers who want a clear, sourced map of what retatrutide actually is, how its unusual three-receptor mechanism works, what the human trials have and have not shown, how it compares with the approved incretin drugs, and where it sits on the regulatory timeline. Throughout, the guiding principle is calibration: reporting the impressive numbers exactly as the trials reported them, while never letting the enthusiasm outrun the evidence. Retatrutide is an experimental compound with remarkable early results and a long list of open questions, and both halves of that sentence matter.
What Retatrutide Is: The Triple-Agonist Idea
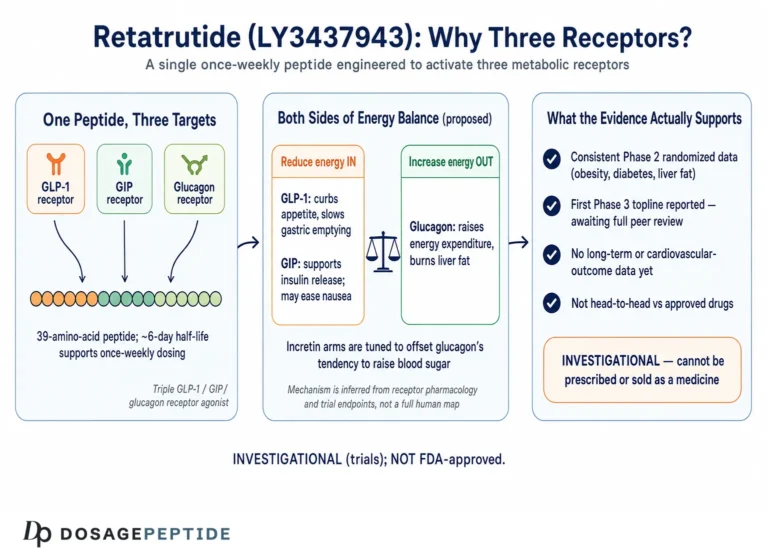
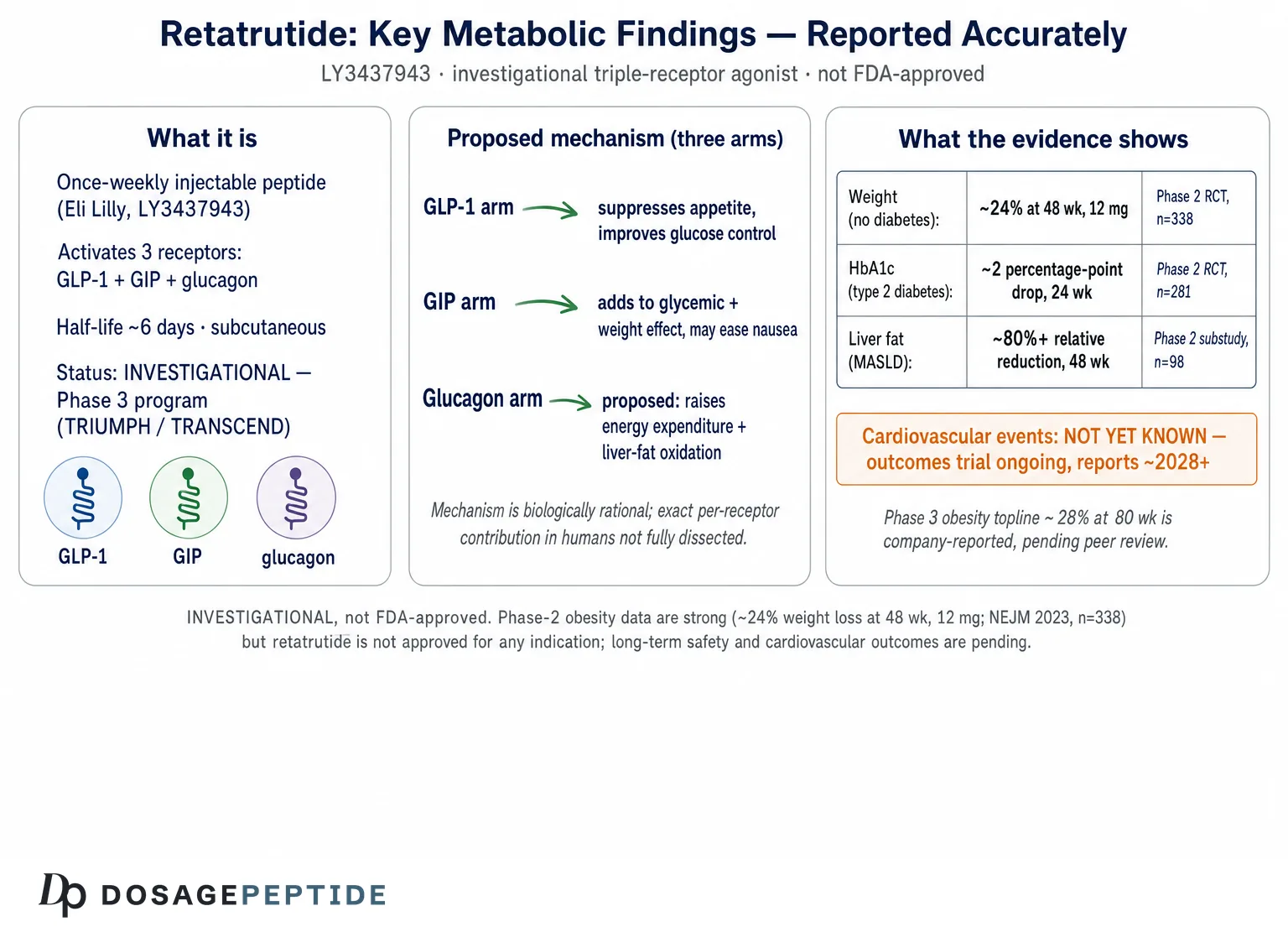
Retatrutide is a synthetic, once-weekly, injectable peptide engineered by Eli Lilly to activate three distinct gut- and pancreas-hormone receptors at the same time: the glucagon-like peptide-1 (GLP-1) receptor, the glucose-dependent insulinotropic polypeptide (GIP) receptor, and the glucagon receptor.1 It is often described in shorthand as a “triple G” or “triagonist,” and it represents the next conceptual step in a lineage that runs from single-hormone GLP-1 drugs (semaglutide) through dual GLP-1/GIP agents (tirzepatide) to this three-receptor molecule.
To understand why a triple agonist is interesting, it helps to see the logic of the progression. GLP-1 receptor agonists reduce appetite and improve glycemic control, and they produce clinically meaningful weight loss. Adding GIP activity, as tirzepatide does, appears to enhance that effect and improve gastrointestinal tolerability in some respects. The third addition — glucagon-receptor agonism — is the conceptually boldest, because glucagon is best known as the hormone that raises blood sugar. Deliberately switching it on in a drug meant to treat diabetes sounds paradoxical. The rationale is that glucagon also increases energy expenditure and drives hepatic fat oxidation, and that its glucose-raising tendency can be more than offset by the powerful glucose-lowering, insulin-sensitizing effects of the GLP-1 and GIP components plus the weight loss itself.1 In other words, the molecule is designed so that the incretin arms dominate glycemic control while the glucagon arm adds a metabolic-rate and liver-fat dimension that the pure incretin drugs lack. Readers who want the fuller conceptual backstory can consult the site’s pillar explainer on what retatrutide is and how the triple-receptor agonist works.
Structurally, retatrutide is a peptide backbone derived from the GIP sequence, modified with a fatty-acid (C20 diacid) side chain that binds albumin and slows clearance, giving the molecule a half-life of roughly six days — long enough to support once-weekly subcutaneous dosing.2 Its receptor-activation profile is deliberately unbalanced: in the discovery work it showed relatively greater GIP-receptor potency alongside more balanced glucagon- and GLP-1-receptor activity, a tuning intended to capture glucagon’s metabolic benefits without ceding glycemic control.1 The compound moved from that preclinical characterization into first-in-human phase 1 studies in 2022, and the discovery-to-proof-of-concept story was published together in a single landmark report.1
It is worth stating plainly what retatrutide is not. It is not a supplement, not a “natural” peptide, and not a compound with a long safety record. It is a purpose-built investigational drug that, as of this writing, exists in the clinic and in Eli Lilly’s phase 3 program — not on pharmacy shelves. Material sold outside regulated clinical channels as “research retatrutide” carries all the purity, dosing, and provenance uncertainties that attach to any unapproved peptide, an issue explored on the site’s page on critical handling protocols for retatrutide research.
A subtle but important point about naming and expectations follows from this. The title’s phrase “managing obesity and metabolic health” describes a clinical activity — something doctors and patients do over years — whereas what actually exists for retatrutide is a set of trial results. Trial results tell us what a drug can do to a group of selected participants under controlled conditions for a fixed period; management describes what happens to real, heterogeneous people over open-ended time. Retatrutide has produced impressive trial results; it has not yet been used to “manage” anyone outside research, because it is not yet a treatment. Holding that distinction firmly is the single most useful habit for reading everything that follows, and it is why this article repeatedly returns to the difference between demonstrated effect and established therapy.
The Mechanism: Three Receptors, One Molecule
The pharmacology of retatrutide is best understood by taking each receptor arm in turn and then seeing how they combine, because the whole point of the molecule is that the three signals are supposed to be complementary rather than redundant.
The GLP-1 arm is the most familiar. GLP-1 receptor agonism enhances glucose-dependent insulin secretion from pancreatic beta cells, suppresses inappropriate glucagon release after meals, slows gastric emptying, and — centrally — acts on hypothalamic and brainstem circuits to reduce appetite and food intake. This appetite suppression is the dominant driver of weight loss in the GLP-1 class, and retatrutide inherits it.1
The GIP arm is more nuanced and, frankly, less completely understood. GIP is an incretin like GLP-1, augmenting insulin secretion after meals, but its role in energy balance has been debated for years. In the context of these multi-agonists, GIP-receptor activity appears to contribute additively to glycemic and weight effects and may improve the nausea profile, possibly through central actions on the area postrema. The tirzepatide experience established that combining GIP with GLP-1 activity yields greater efficacy than GLP-1 alone, and retatrutide carries that GIP component forward.1
The glucagon arm is what makes retatrutide distinctive. In the liver, glucagon-receptor activation stimulates cyclic AMP signaling that promotes fatty-acid oxidation and can increase hepatic glucose output; systemically, glucagon raises resting energy expenditure. The therapeutic bet is twofold. First, that increasing energy expenditure adds a second lever to weight loss beyond appetite suppression — the body burns somewhat more, not just eats less. Second, that direct hepatic fat oxidation drives down liver-fat content in a way that could be especially relevant to metabolic dysfunction-associated steatotic liver disease (MASLD). The risk the design has to manage is glucagon’s glucose-raising tendency; the preclinical and early clinical work indicated that, at the doses studied, the incretin-mediated glucose lowering and the weight loss more than compensated, so net glycemic control improved rather than worsened.1
Preclinically, retatrutide produced weight loss in rodent models that exceeded what could be explained by reduced food intake alone; compared with animals whose calorie intake was matched to the treated group, retatrutide-treated animals lost more, implicating a genuine increase in energy expenditure attributable to the glucagon component.1 That mechanistic signature — appetite suppression plus a metabolic-rate contribution plus direct hepatic fat oxidation — is the biological story that the human trials then had to test.
One detail of the pharmacology deserves emphasis because it is often glossed over in popular accounts. The three receptor activities are not balanced equally. In the discovery characterization, retatrutide showed its greatest potency at the GIP receptor, with more balanced activity at the glucagon and GLP-1 receptors — not the maximal, evenly matched three-receptor activation one might naively assume for a drug marketed on its weight-loss power.1 This balance is deliberate. Overly dominant GLP-1 activity would worsen nausea and could blunt the very energy-expenditure effect the glucagon arm is meant to add, while a meaningful glucagon signal supplies the metabolic-rate and hepatic contributions. The clinical behavior of the molecule therefore reflects a carefully engineered ratio, not simply “three receptors turned on maximally.” It also means that lessons from single-receptor drugs do not transfer cleanly; retatrutide is its own pharmacological entity, and its risk-benefit profile has to be established on its own data rather than inferred from semaglutide or tirzepatide.
It is also worth being precise about where these effects occur. The appetite suppression is largely central, mediated by receptors in hypothalamic and hindbrain circuits that regulate satiety and nausea; the glycemic effects are a mix of central appetite reduction, pancreatic islet actions, and delayed gastric emptying; and the energy-expenditure and hepatic-fat effects are thought to be substantially peripheral, driven by glucagon signaling in the liver and possibly in adipose tissue. This distributed action across the brain, gut, pancreas, and liver is what allows a single weekly injection to move weight, glucose, and liver fat simultaneously — and it is also why the safety monitoring has to be equally broad, watching cardiovascular, hepatic, gastrointestinal, and glycemic parameters at once.
A measured mechanistic summary: retatrutide’s three arms are individually well grounded in incretin and glucagon biology, and the combination is rational rather than speculative. But “rational mechanism” is not the same as “proven clinical benefit,” and the precise contribution of each receptor to the observed human results has not been fully dissected. For the broader question of how these receptor pathways influence metabolic risk, the site’s discussion of how retatrutide influences cardiovascular risk factors covers the downstream effects on blood pressure and lipids.
The Phase 2 Obesity Trial: the Headline Data
The single result that put retatrutide on the map was its phase 2 obesity trial, published in the New England Journal of Medicine in 2023 by Jastreboff and colleagues.3 This is the study most people mean when they cite retatrutide’s weight-loss numbers, so it is worth reporting carefully and completely.
The trial was a randomized, double-blind, placebo-controlled, phase 2 study enrolling 338 adults with obesity (BMI 30 or higher, or 27 or higher with a weight-related complication) but without type 2 diabetes. Participants were randomized to once-weekly subcutaneous retatrutide at maintenance doses of 1, 4, 8, or 12 mg (reached through staged dose escalation), or to placebo, and treated for 48 weeks. The primary endpoint was percentage change in body weight at 24 weeks, with 48-week change as a key secondary endpoint.3
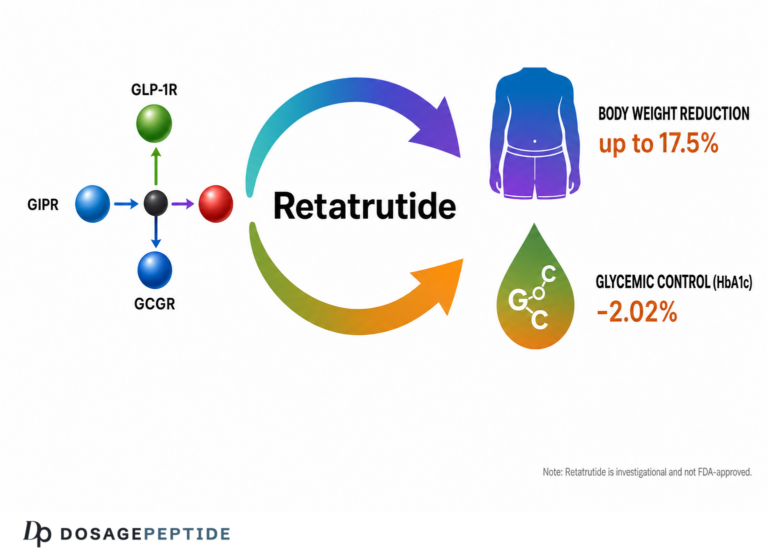
The results were, by the standards of obesity pharmacotherapy, extraordinary. At 48 weeks, the mean weight reduction was approximately 24.2% in the 12 mg group, compared with about 2.1% in the placebo group. The 8 mg group achieved roughly 22%. Weight loss was strongly dose-dependent, and — a point that drew particular attention — the weight-loss curve in the highest-dose groups had not clearly plateaued by 48 weeks, suggesting that the full effect might not yet have been reached.3 Essentially all participants in the higher-dose arms lost at least 5% of body weight, and a substantial proportion of the 12 mg group lost 30% or more — a magnitude approaching what is typically associated with bariatric surgery rather than medication.
| Retatrutide dose (weekly) | Mean weight change at 48 weeks3 |
|---|---|
| Placebo | ≈ −2.1% |
| 1 mg | ≈ −8.7% |
| 4 mg | ≈ −17.1% |
| 8 mg | ≈ −22.8% |
| 12 mg | ≈ −24.2% |
Beyond the scale numbers, the trial reported improvements in a range of cardiometabolic markers: reductions in waist circumference, systolic and diastolic blood pressure, and improvements in lipid measures and glycemic parameters, consistent with the expected downstream benefits of large weight loss.3 These secondary findings are encouraging, but they are exactly that — secondary, surrogate markers measured in a phase 2 study of a few hundred people over less than a year.
The non-plateau observation is worth dwelling on because it shaped expectations for the phase 3 program. In most weight-loss drug trials the curve flattens as the body reaches a new equilibrium, so the endpoint captures close to the maximum effect. Retatrutide’s higher-dose curves were still descending at 48 weeks, which implied either that a longer trial would show even greater loss or that the drug’s effect on the body’s regulated weight set point is unusually strong. The subsequent longer phase 3 data, showing larger figures at 80 weeks, are consistent with the former interpretation.8 This is a genuinely notable pharmacological feature — but it also means the phase 2 endpoint should not be read as the ceiling, and cross-trial comparisons that pit retatrutide’s 48-week number against another drug’s 68- or 72-week number are comparing points at different places on differently shaped curves.
Two further honest qualifications about the obesity data. First, the trial’s remarkable averages conceal individual variability: not everyone responds identically, some participants tolerate the drug poorly and discontinue, and the mean figures are pulled by high responders. Reporting “up to 24%” is accurate for the group average at the top dose but should not be read as a promise for any individual. Second, weight loss of this magnitude raises its own clinical management questions — adequacy of nutrition, preservation of muscle and bone, and the psychological and behavioral dimensions of rapid body change — that a phase 2 efficacy trial is not designed to address and that would need careful attention in any real-world use.
Now the necessary caveats, which do not diminish the result but do define its limits. This was a phase 2 trial: relatively small (338 participants), of moderate duration (48 weeks), and powered to establish dose-response and short-to-medium-term efficacy, not to measure hard outcomes or rare adverse events. It enrolled people with obesity but without diabetes, so its findings do not automatically transfer to other populations. And — the point the title of this article invites — a phase 2 weight-loss result, however dramatic, is a demonstration that the drug can strip fat, not proof that it reduces the diseases obesity causes. Those are separate questions answered by separate, larger, longer trials, which we turn to below.
Glycemic Control: the Phase 2 Type 2 Diabetes Data
Retatrutide’s second major phase 2 readout came in people with type 2 diabetes, published in The Lancet in 2023 by Rosenstock and colleagues.4 Because the glucagon arm raises the theoretical concern of worsening glucose control, this trial was where that worry would either materialize or be laid to rest.
The study randomized 281 adults with type 2 diabetes (HbA1c 7.0–10.5%, on diet and exercise or metformin) to a range of retatrutide doses (0.5, 4, 8, or 12 mg, with different escalation schedules), to placebo, or to the active comparator dulaglutide 1.5 mg (an established GLP-1 receptor agonist). The primary endpoint was change in HbA1c at 24 weeks, with weight and other measures assessed through 36 weeks.4
The glycemic results were robust. At the higher doses, HbA1c fell by approximately 2 percentage points from a baseline near 8.3%, bringing a large share of participants below the 7% threshold that defines adequate control, and the reductions in the higher-dose arms were greater than those achieved with dulaglutide.4 Critically, the feared glucagon-driven deterioration in glycemia did not appear: net glucose control improved, confirming that the incretin arms and the weight loss dominated. Weight reductions were again substantial, reaching roughly 17% at the 12 mg dose by 36 weeks — somewhat less than in the non-diabetic obesity trial, consistent with the general observation that weight loss with incretin drugs tends to be a little smaller in people with diabetes.4
The diabetes trial matters for a reason beyond its own numbers: it was the direct test of the glucagon paradox. Skeptics of glucagon-receptor agonism in a metabolic drug had a legitimate worry — that switching on a glucose-raising hormone would, at minimum, blunt glycemic benefit and, at worst, worsen it in exactly the patients least able to afford it. The trial’s design, with a GLP-1 active comparator and a range of glucagon-inclusive doses, was well suited to expose such a problem if it existed. That the higher retatrutide doses instead outperformed dulaglutide on HbA1c is strong evidence that, within the studied dose range and duration, the engineering worked: the incretin arms and weight loss dominated the glucose equation.4 This does not license complacency — longer exposure, higher doses, or vulnerable subgroups could behave differently — but it converts the glucagon concern from a theoretical objection into a monitored, so-far-manageable parameter.
A later prespecified body-composition substudy in this diabetes population used imaging to show that the weight lost was predominantly fat mass, with reductions in both visceral and subcutaneous fat and a relative preservation of the proportion of lean mass typical of this drug class — though, as with all incretin-based weight loss, some absolute lean mass is lost alongside fat, a point that matters for older and frailer patients.5 Taken together, the diabetes program showed that retatrutide can deliver best-in-class-range glycemic control and large weight loss simultaneously, without the glucagon component sabotaging blood sugar. For context on how this class competes, the site’s overview of tirzepatide and how it works is a useful comparator.
Liver Fat and Metabolic Health Beyond Weight
Perhaps the most mechanistically interesting retatrutide finding — and the one that most directly tests the glucagon-arm hypothesis — concerns the liver. Metabolic dysfunction-associated steatotic liver disease (MASLD, formerly NAFLD) and its inflammatory form (MASH) are downstream consequences of the same metabolic dysfunction that drives obesity and type 2 diabetes, and excess liver fat is a marker of cardiometabolic risk. If glucagon-receptor agonism drives hepatic fat oxidation as the design intends, retatrutide should reduce liver fat especially effectively.
A prespecified substudy of the phase 2 obesity trial, published in Nature Medicine in 2024 by Sanyal and colleagues, tested exactly this.6 It enrolled 98 participants who had at least 10% liver-fat content by MRI-derived proton-density fat fraction (MRI-PDFF) at baseline — a threshold consistent with MASLD — and tracked their liver fat through 48 weeks of retatrutide or placebo.
The reductions were the largest reported for any pharmacological agent to that point. At the 8 mg and 12 mg doses, relative liver-fat content fell by roughly 81% and 82% respectively, versus essentially no change with placebo, and roughly 80–86% of participants in the higher-dose groups achieved normalization of liver fat (below the 5% threshold) by week 48.6 The effect was clearly dose-dependent, with even the 1 mg dose producing a meaningful reduction. These are remarkable numbers, and they lend real support to the idea that the glucagon arm contributes something the pure incretin drugs do not.
| Metabolic domain | Best phase-2 retatrutide signal | Evidence level |
|---|---|---|
| Body weight (no diabetes) | ≈ −24% at 48 weeks, 12 mg3 | Phase 2 RCT, n=338 |
| HbA1c (type 2 diabetes) | ≈ −2 percentage points, 24 weeks4 | Phase 2 RCT, n=281 |
| Liver fat (MASLD) | ≈ 80%+ relative reduction, 48 weeks6 | Phase 2 substudy, n=98 |
| Cardiovascular events | Not yet known | Outcomes trial ongoing10 |
The honest caveats here are important. This was a substudy of fewer than a hundred people, measuring liver fat by imaging rather than histological resolution of MASH by biopsy in a dedicated trial — imaging fat fraction is an excellent surrogate but not identical to biopsy-confirmed disease reversal. Reducing liver fat is a strong signal, but demonstrating that retatrutide improves the fibrosis and long-term liver outcomes that actually matter to patients requires purpose-built MASH trials with histological endpoints, which are a separate undertaking. As with the weight and glucose data, the liver findings are best read as a powerful proof of the mechanistic concept, not as evidence of an approved MASLD therapy — because there is none.
What Phase 3 Has Added So Far
Between 2024 and 2026 retatrutide moved into its large phase 3 program, branded TRIUMPH (obesity) and TRANSCEND (diabetes). As of mid-2026, some of these results have begun to read out, and reporting them requires care to distinguish peer-reviewed publications from company topline announcements, because the two carry very different evidentiary weight.
The first phase 3 diabetes trial to reach peer review, TRANSCEND-T2D-1, was published in The Lancet in 2026.7 This 40-week, randomized, double-blind, placebo-controlled trial in adults with type 2 diabetes inadequately controlled by diet and exercise confirmed and extended the phase 2 signal: retatrutide met its primary HbA1c endpoint and all key secondary endpoints, with mean HbA1c reductions approaching 2 percentage points, a large majority of participants reaching target glycemic thresholds, and dose-dependent weight loss reaching roughly the mid-teens percent at the top dose, with a safety profile consistent with the GLP-1 drug class.7 As a phase 3, peer-reviewed result, this carries more weight than the phase 2 data, though it remains a glycemic-and-weight efficacy trial rather than an outcomes study.
On the obesity side, Eli Lilly announced topline results from the pivotal TRIUMPH-1 obesity trial via press release in May 2026, reporting that in roughly 2,300 adults with obesity or overweight (without type 2 diabetes), retatrutide 12 mg produced a mean weight reduction of about 28% at 80 weeks, with all doses meeting primary and key secondary endpoints.8 This is a striking confirmation of the phase 2 trajectory — and the longer duration appears to have captured more of the weight loss that the earlier trial’s non-plateauing curve had hinted at. But a critical honesty point applies: a company topline press release is not a peer-reviewed publication. It reports summary numbers without the full methods, subgroup analyses, adverse-event tables, and independent scrutiny that peer review provides. Until the complete TRIUMPH-1 data are published and examined, the 28% figure should be treated as a promising but provisional headline, not settled fact.
What none of these trials has yet delivered is the outcome that ultimately determines a weight-loss drug’s medical value: whether it reduces cardiovascular events, kidney disease progression, and mortality. That question is being addressed by a dedicated large-scale cardiovascular and kidney outcomes trial (TRIUMPH-Outcomes) enrolling on the order of ten thousand participants with obesity and established cardiovascular disease, which is not expected to report until the latter part of the decade.10 Until it does, retatrutide’s effect on hard outcomes is genuinely unknown, and no amount of weight-loss or biomarker data can substitute for it. Readers tracking where this fits historically may find the site’s piece on how retatrutide fits into the evolution of peptide therapeutics useful.
Dosing and Escalation in the Research Context
A brief, strictly educational note on how retatrutide has been dosed in trials — with the emphasis that this describes clinical-trial protocols under medical supervision, not a recommendation for use, and that retatrutide is not an approved medicine that anyone should be self-administering.
Across the trials, retatrutide is given as a once-weekly subcutaneous injection, and a defining feature of the protocols is gradual dose escalation. Rather than starting at a maintenance dose, trials began at low doses (for example 2 mg or 4 mg) and stepped up over weeks or months toward maintenance targets of 8 or 12 mg.34 This titration is not incidental; it is the central strategy for managing the gastrointestinal side effects that otherwise limit tolerability. Escalating slowly gives the gut time to adapt, reducing the nausea, vomiting, and diarrhea that peak during dose increases. The escalation schedule itself became an object of study, with different titration speeds compared to find the balance between reaching an effective dose quickly and keeping side effects manageable.4
| Parameter | Retatrutide in clinical trials |
|---|---|
| Route | Subcutaneous injection |
| Frequency | Once weekly2 |
| Half-life | ≈ 6 days (supports weekly dosing)2 |
| Starting dose | Low (e.g. 2–4 mg), then escalated3 |
| Maintenance doses studied | 1, 4, 8, 12 mg (obesity phase 2)3 |
| Escalation rationale | Minimize GI adverse effects4 |
The practical lesson from the dosing data is that retatrutide’s benefits and its tolerability are both dose-dependent, and the escalation schedule is the tool that reconciles them. It also underscores why this is a drug for supervised clinical settings: getting the titration right, monitoring for the safety signals discussed below, and adjusting for individual tolerance are medical judgments, not do-it-yourself calculations. For general background on how injectable peptides are handled and reconstituted in research settings, the site maintains a peptide reconstitution guide, offered purely for educational reference.
Safety and Tolerability
Retatrutide’s safety profile in the trials to date is broadly consistent with the incretin drug class, with a few distinctive wrinkles attributable to its glucagon component and its sheer potency. Reporting it fairly means neither minimizing the side effects nor implying a long-term safety record that does not yet exist.
The dominant adverse effects are gastrointestinal: nausea, vomiting, diarrhea, and constipation, mostly mild to moderate, concentrated during dose escalation, and mitigated by slower titration.34 These are the same tolerability issues that characterize semaglutide and tirzepatide, and they are the main reason a minority of participants discontinue.
Two signals warrant specific attention. First, retatrutide produced a dose-dependent increase in heart rate in the trials, on the order of several beats per minute at higher doses, which tended to peak and then partially attenuate over time.3 Increased heart rate is seen across the incretin class but the magnitude with retatrutide, and its potential relevance in people with cardiovascular disease, is precisely the kind of question the ongoing outcomes trial is designed to address. Second, some participants reported cutaneous sensory symptoms such as skin hyperesthesia or altered sensation, an effect noted in the phase 2 obesity trial that is less familiar from the older drugs and whose mechanism is not fully explained.3
The glucagon arm also created a specific monitoring focus. Because glucagon can raise glucose and because it mobilizes hepatic substrate, the trials watched carefully for deterioration in glycemic control and for changes in liver enzymes and other parameters; in the event, net glycemic control improved and the feared metabolic downsides did not dominate at the studied doses.4 A modest, dose-related increase in heart rate and the transient nature of some effects nonetheless mean that cardiovascular safety cannot be declared settled from efficacy trials alone.
Several structural caveats bound all of this:
- Duration. The longest results are on the order of one to one-and-a-half years. Obesity is a lifelong condition; multi-year safety is not yet characterized.
- Population. Trials enrolled selected participants; effects in the very old, the frail, those with significant organ dysfunction, or during pregnancy are not established.
- Rare events. Phase 2 and even phase 3 efficacy trials are underpowered to detect uncommon serious adverse events; those emerge only from large outcomes trials and post-marketing surveillance — neither of which has completed for retatrutide.
- Unapproved-material risk. Retatrutide obtained outside regulated clinical channels carries additional, non-pharmacological hazards of impurity, mislabeling, and incorrect dosing that have nothing to do with the molecule’s intrinsic profile.
The reasonable reading is that retatrutide has, so far, shown a class-typical and manageable short-to-medium-term safety profile with a couple of distinctive signals (heart rate, skin sensation) that merit ongoing scrutiny — and that its long-term safety remains, by definition, an open question for an investigational drug.
How Retatrutide Compares With Approved Incretin Drugs
Retatrutide does not exist in a vacuum; it is entering a field already occupied by two highly effective, FDA-approved incretin therapies, and the fairest way to gauge it is by comparison. The crucial distinction to keep in mind is that semaglutide and tirzepatide are approved drugs with pivotal trial data and, increasingly, cardiovascular-outcomes evidence, whereas retatrutide is still investigational. So this is a comparison of demonstrated magnitude, not of regulatory standing.
Semaglutide 2.4 mg (a GLP-1 receptor agonist, marketed for obesity as Wegovy) produced mean weight loss of roughly 15% over 68 weeks in its pivotal STEP 1 trial — a landmark result when published.9 Tirzepatide (a dual GIP/GLP-1 agonist, marketed as Zepbound/Mounjaro) raised the bar further, with mean weight loss up to roughly 21% at the highest dose over 72 weeks in SURMOUNT-1.11 Retatrutide’s phase 2 obesity result of about 24% at 48 weeks, and its topline phase 3 figure near 28%, sit at the top of this ascending series — though, again, cross-trial comparisons are inexact because populations, durations, and designs differ, and retatrutide’s figures are not yet fully peer-reviewed at phase 3.38
| Drug | Receptor targets | Peak mean weight loss (pivotal/phase-2) | Status |
|---|---|---|---|
| Semaglutide 2.4 mg | GLP-1 | ≈ 15% / 68 wk9 | FDA-approved (obesity) |
| Tirzepatide | GIP + GLP-1 | ≈ 21% / 72 wk11 | FDA-approved (obesity) |
| Retatrutide | GIP + GLP-1 + glucagon | ≈ 24% / 48 wk (phase 2)3 | Investigational |
The pattern — more receptor targets, more weight loss — is real and striking, but it must be paired with a durability caveat that applies to the entire class. When people stop these drugs, weight tends to return. The STEP 1 extension showed that participants regained roughly two-thirds of their lost weight in the year after semaglutide was withdrawn, and cardiometabolic improvements reverted correspondingly.12 There is no reason to expect retatrutide to be different: these are treatments for a chronic condition that work while taken, not cures that reset the body’s set point. Any honest account of retatrutide’s promise has to sit alongside this reality of weight regain after discontinuation. For a fuller picture of the approved competitor’s evidence base, see the site’s summary of how effective tirzepatide is according to recent clinical studies.
There is a further, easily overlooked dimension to comparing these drugs: tolerability and the proportion of people who can actually stay on an effective dose. Raw efficacy figures describe those who completed the trial at the assigned dose; they do not by themselves tell you how many started but could not tolerate escalation. Because retatrutide is the most potent of the three and shares the class’s gastrointestinal profile plus its own heart-rate and skin-sensation signals, the real-world question of how many people can comfortably reach and maintain the 8–12 mg doses that produce the headline numbers is not fully answered by phase 2 data. A drug that produces 28% loss in those who tolerate it but that a meaningful fraction cannot tolerate has a different practical profile from one whose average is lower but more uniformly achievable. The full phase 3 dataset, with its complete discontinuation and adverse-event tables, is what will let that comparison be made fairly.
The other half of the comparison is outcomes evidence. Semaglutide has demonstrated cardiovascular benefit in dedicated outcomes trials in relevant populations; tirzepatide’s outcomes program is maturing. Retatrutide has no completed outcomes trial at all. So even though retatrutide leads on the weight-loss scale, it currently trails both approved drugs on the more important measure of proven benefit for the diseases these drugs are ultimately meant to prevent.
Regulatory Status and What Remains Unknown
Precision about regulatory status matters, because the impressive trial data can create a false impression that retatrutide is available or nearly so.
Not approved, anywhere, for any indication. As of mid-2026 retatrutide has not received marketing authorization from the FDA, the EMA, or any comparable major regulator for obesity, type 2 diabetes, MASLD, or anything else. It is an investigational drug in Eli Lilly’s phase 3 development program.3 It cannot be legally prescribed or sold as an approved treatment, and material marketed as “research retatrutide” through non-clinical channels is unapproved and of unverified quality.
What approval will require. The path to approval runs through the completion of the phase 3 program — the full TRIUMPH obesity trials and TRANSCEND diabetes trials — with peer-reviewed publication of complete efficacy and safety data, followed by regulatory review.78 Even a favorable review of the efficacy trials would yield an approval for weight management and/or glycemic control based on those endpoints; it would not, by itself, establish cardiovascular or mortality benefit.
The outcomes gap. The most consequential unknown is whether retatrutide’s dramatic effects on weight, glucose, and liver fat translate into fewer heart attacks, strokes, kidney failures, and deaths. That is the province of the large cardiovascular and kidney outcomes trial now underway, which is not expected to report until roughly 2028 or later.10 Until then, claims that retatrutide “prevents” cardiovascular disease or “treats” its downstream consequences run ahead of the evidence. It reduces the risk factors; whether it reduces the events is not yet demonstrated.
Other open questions include long-term (multi-year) safety, durability of effect and management of weight regain, effects in populations excluded from the trials, the histological (not just imaging) impact on MASH, and head-to-head comparisons against tirzepatide and semaglutide under identical conditions. None of these is a reason for pessimism; all of them are reasons for calibrated language.
It is worth naming why this patience is not mere bureaucratic caution. The history of metabolic medicine includes drugs that improved surrogate markers impressively and then failed, or actively harmed, on hard outcomes — agents that lowered glucose or changed lipids yet did not reduce, or even increased, cardiovascular events. That history is precisely why regulators and thoughtful clinicians insist on outcomes trials rather than accepting weight-loss and biomarker data as sufficient. Retatrutide’s surrogate results are far stronger than most, and the analogy to already-successful incretin drugs is reassuring, but analogy is not proof. The discipline of waiting for TRIUMPH-Outcomes is the same discipline that has, in the past, caught problems that looked invisible in shorter efficacy studies.10
The regulatory synthesis is straightforward: retatrutide is a genuinely promising investigational compound with some of the strongest metabolic phase-2 data ever reported, moving through a large phase-3 program, but it is not an approved therapy and its most important long-term questions are unanswered. The correct posture toward it is serious scientific interest tempered by the discipline of waiting for the evidence that approval — and real clinical confidence — requires.
Frequently Asked Questions
Is retatrutide FDA-approved for obesity or diabetes?
No. As of mid-2026, retatrutide is an investigational drug that has not been approved by the FDA, the EMA, or any comparable regulator for obesity, type 2 diabetes, MASLD, or any other condition. It is in Eli Lilly’s phase 3 clinical program.3 It cannot legally be prescribed or marketed as an approved treatment, and any product sold as “research retatrutide” outside regulated clinical trials is unapproved and of unverified quality.
How much weight did people lose with retatrutide in the trials?
In the phase 2 obesity trial (338 adults without diabetes), mean weight loss at 48 weeks was about 24% at the 12 mg dose versus roughly 2% with placebo, and the weight-loss curve had not fully plateaued.3 Topline results from the larger phase 3 TRIUMPH-1 trial, announced by the manufacturer in 2026, reported about 28% mean weight loss at 80 weeks — though those are company-reported topline figures pending full peer-reviewed publication.8
What makes retatrutide different from semaglutide and tirzepatide?
Semaglutide activates one receptor (GLP-1) and tirzepatide activates two (GIP and GLP-1). Retatrutide activates three — adding glucagon-receptor agonism.1 The glucagon component is intended to increase energy expenditure and drive hepatic fat oxidation, which may explain both retatrutide’s numerically larger weight-loss figures and its striking liver-fat reductions. The trade-off is that retatrutide, unlike the other two, is not yet approved and lacks completed cardiovascular-outcomes data.
Doesn’t adding glucagon raise blood sugar? Why use it in a diabetes drug?
Glucagon does tend to raise glucose, which is why a glucagon-receptor agonist in a diabetes drug sounds paradoxical. The design bet is that the powerful glucose-lowering effects of the GLP-1 and GIP arms, plus the weight loss itself, more than offset glucagon’s glucose-raising tendency. In the phase 2 diabetes trial that is exactly what happened: net HbA1c control improved markedly and exceeded that of the GLP-1 comparator, with no glucagon-driven deterioration at the doses studied.4
What did retatrutide do to liver fat?
In a prespecified substudy of participants with fatty liver (at least 10% liver fat by MRI), the higher retatrutide doses reduced relative liver-fat content by roughly 80% or more over 48 weeks, and roughly 80–86% of higher-dose participants achieved normalization of liver fat.6 These are among the largest pharmacological liver-fat reductions reported. Importantly, this measured liver fat by imaging, not biopsy-confirmed reversal of liver disease, so it demonstrates the mechanism strongly but is not the same as proving improvement in long-term liver outcomes.
Does retatrutide reduce heart attacks and strokes?
That is not yet known. Retatrutide improves cardiovascular risk factors such as weight, blood pressure, glucose, and lipids, but whether it reduces actual cardiovascular events is being tested in a large dedicated outcomes trial that is not expected to report until later in the decade.10 Until those results are in, it is inaccurate to say retatrutide prevents cardiovascular disease.
What are the main side effects?
The most common are gastrointestinal — nausea, vomiting, diarrhea, constipation — mostly mild to moderate and concentrated during dose escalation, which is why trials titrate the dose up slowly.34 Retatrutide also produced a dose-dependent increase in heart rate and, in some participants, unusual skin sensory symptoms.3 Because the trials are relatively short, long-term and rare adverse effects are not yet characterized.
If people stop taking it, do they keep the weight off?
Almost certainly not, based on the whole drug class. With semaglutide, participants regained roughly two-thirds of lost weight within a year of stopping, and cardiometabolic gains reverted.12 There is no evidence that retatrutide differs; these drugs treat a chronic condition and work while taken rather than resetting the body permanently. Durability and management of weight regain remain open questions for retatrutide specifically.
Can I buy retatrutide to use for weight loss?
Retatrutide is not an approved medicine and is not available by prescription for weight loss. Products sold online as “research” retatrutide are unapproved, unregulated, and of unknown purity and dose, carrying risks entirely separate from the molecule’s studied profile. The compound should be used only within properly authorized clinical research under medical supervision.
References
- Coskun T, Urva S, Roell WC, et al. LY3437943, a novel triple glucagon, GIP, and GLP-1 receptor agonist for glycemic control and weight loss: from discovery to clinical proof of concept. Cell Metab. 2022;34(9):1234-1247.e9. PMID: 35985340. https://pubmed.ncbi.nlm.nih.gov/35985340/
- Urva S, Coskun T, Loh MT, et al. LY3437943, a novel triple GIP, GLP-1, and glucagon receptor agonist in people with type 2 diabetes: a phase 1b, multicentre, double-blind, placebo-controlled, randomised, multiple-ascending dose trial. Lancet. 2022;400(10366):1869-1881. PMID: 36354040. https://pubmed.ncbi.nlm.nih.gov/36354040/
- Jastreboff AM, Kaplan LM, Frías JP, et al. Triple–Hormone-Receptor Agonist Retatrutide for Obesity — A Phase 2 Trial. N Engl J Med. 2023;389(6):514-526. PMID: 37366315. https://pubmed.ncbi.nlm.nih.gov/37366315/
- Rosenstock J, Frias J, Jastreboff AM, et al. Retatrutide, a GIP, GLP-1 and glucagon receptor agonist, for people with type 2 diabetes: a randomised, double-blind, placebo and active-controlled, parallel-group, phase 2 trial conducted in the USA. Lancet. 2023;402(10401):529-544. PMID: 37385280. https://pubmed.ncbi.nlm.nih.gov/37385280/
- Coskun T, Wu Q, Schloot NC, et al. Effects of retatrutide on body composition in people with type 2 diabetes: a substudy of a phase 2, double-blind, parallel-group, placebo-controlled, randomised trial. Lancet Diabetes Endocrinol. 2025;13(8):674-684. PMID: 40609566. https://pubmed.ncbi.nlm.nih.gov/40609566/
- Sanyal AJ, Kaplan LM, Frias JP, et al. Triple hormone receptor agonist retatrutide for metabolic dysfunction-associated steatotic liver disease: a randomized phase 2a trial. Nat Med. 2024;30(7):2037-2048. PMID: 38858523. https://pubmed.ncbi.nlm.nih.gov/38858523/
- Efficacy and safety of retatrutide, a GIP, GLP-1, and glucagon receptor agonist, in people with type 2 diabetes and inadequate glycaemic control with diet and exercise (TRANSCEND-T2D-1): a double-blind, randomised, phase 3 trial. Lancet. 2026. PMID: 42250575. https://pubmed.ncbi.nlm.nih.gov/42250575/
- Eli Lilly and Company. Lilly’s triple agonist, retatrutide, delivered powerful weight loss in pivotal Phase 3 obesity trial (TRIUMPH-1 topline results press release). 2026. https://www.prnewswire.com/news-releases/lillys-triple-agonist-retatrutide-delivered-powerful-weight-loss-in-pivotal-phase-3-obesity-trial-302778859.html
- Wilding JPH, Batterham RL, Calanna S, et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity (STEP 1). N Engl J Med. 2021;384(11):989-1002. PMID: 33567185. https://pubmed.ncbi.nlm.nih.gov/33567185/
- Eli Lilly and Company (ClinicalTrials.gov). The Effect of Retatrutide Once Weekly on Cardiovascular Outcomes and Kidney Outcomes in Adults Living With Obesity (TRIUMPH-Outcomes). NCT06383390. https://clinicaltrials.gov/study/NCT06383390
- Jastreboff AM, Aronne LJ, Ahmad NN, et al. Tirzepatide Once Weekly for the Treatment of Obesity (SURMOUNT-1). N Engl J Med. 2022;387(3):205-216. PMID: 35658024. https://pubmed.ncbi.nlm.nih.gov/35658024/
- Wilding JPH, Batterham RL, Davies M, et al. Weight regain and cardiometabolic effects after withdrawal of semaglutide: The STEP 1 trial extension. Diabetes Obes Metab. 2022;24(8):1553-1564. PMID: 35441470. https://pubmed.ncbi.nlm.nih.gov/35441470/
Educational and research-use disclaimer: This article is provided solely for scientific and educational purposes. Retatrutide (LY3437943) is an investigational compound that is not approved by the FDA, EMA, or any comparable regulator for the treatment, cure, or prevention of obesity, type 2 diabetes, metabolic dysfunction-associated steatotic liver disease, cardiovascular disease, or any other condition. Its long-term safety and its effect on cardiovascular and mortality outcomes have not been established. Nothing here is medical advice or a recommendation for human use, and material sold outside regulated clinical trials as “research retatrutide” is unapproved and of unverified quality. Any legitimate investigation of this compound should occur within properly authorized clinical research under appropriate medical and regulatory oversight. Readers should consult qualified healthcare professionals and applicable regulations before making any decisions.