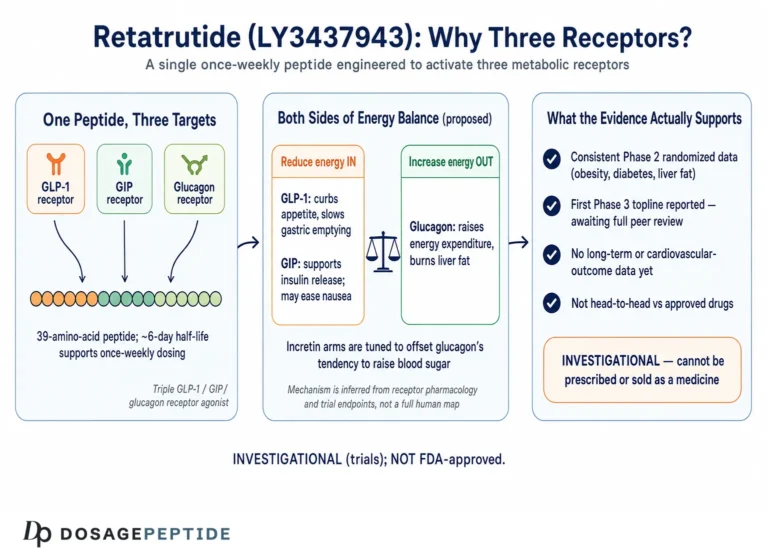
Few investigational molecules have generated as much scientific curiosity in metabolic medicine as retatrutide, a synthetic peptide developed by Eli Lilly under the code name LY3437943. What sets it apart is not simply that it lowers blood glucose or reduces body weight, but that it does so by engaging three separate hormone receptors at once: the glucagon-like peptide-1 receptor (GLP-1R), the glucose-dependent insulinotropic polypeptide receptor (GIPR), and the glucagon receptor (GCGR). Because type 2 diabetes sits at the intersection of impaired insulin secretion, excess body fat, and disordered hepatic glucose handling, a compound that touches all three axes has become one of the most closely watched candidates in the endocrinology pipeline.1
This article examines what the peer-reviewed clinical record actually says about retatrutide in the context of type 2 diabetes management. The honest headline is that the evidence is promising but still maturing. The pivotal glucose-lowering data come from a single Phase 2 randomized trial published in The Lancet in 2023, supplemented by a Phase 3 trial (TRANSCEND-T2D-1) reported in 2026, alongside a broad Phase 3 program (TRIUMPH) whose diabetes-specific readouts are still emerging.1,3,8 Retatrutide is an investigational agent. As of this writing it is not approved by the U.S. Food and Drug Administration (FDA), the European Medicines Agency (EMA), or any other major regulator for the treatment of type 2 diabetes or any other condition.
Everything that follows is written for an educational and research-literacy audience. It describes what investigators measured, in whom, and with what caveats. It does not recommend that anyone use retatrutide, and it does not present the compound as a therapy. Where the underlying data are preclinical, in vitro, or drawn from early-phase human studies, that limitation is stated plainly. Readers interested in how the molecule is characterized in a laboratory setting can also consult the compound-specific reference material such as the Retatrutide 12 mg vial dosage protocol and the broader peptide dosage catalog maintained on this site.
What Retatrutide Is and Where It Came From
Retatrutide is a once-weekly, subcutaneously administered peptide belonging to the incretin-based class of metabolic agents. Structurally, it is a synthetic 39-amino-acid peptide built on a modified glucagon/GIP backbone and engineered with a fatty-acid moiety that binds albumin to extend its circulating half-life to roughly six days, which is what makes weekly dosing feasible.5 It is described in the literature as a “triple hormone receptor agonist” or “triple G” agonist, referring to its simultaneous activity at GLP-1R, GIPR, and GCGR.2
The molecule’s lineage is instructive. The first incretin mimetics targeted the GLP-1 receptor alone; exenatide, liraglutide, dulaglutide, and semaglutide all belong to this single-agonist generation. The next conceptual leap combined GLP-1 with GIP activity in a single molecule, producing tirzepatide, the first dual GIP/GLP-1 receptor agonist to reach the market. Retatrutide extends this trajectory by adding a third arm, glucagon receptor agonism, on the hypothesis that glucagon signaling can be harnessed to increase energy expenditure and mobilize hepatic fat, effects that pure incretin agonists do not deliver.5
Glucagon’s inclusion is counterintuitive at first glance. Endogenous glucagon raises blood glucose by stimulating hepatic glucose output, so a naive reading would suggest that adding glucagon activity to a diabetes drug is self-defeating. The resolution lies in the balance of the three signals. The powerful insulinotropic and glucose-dependent actions of GLP-1 and GIP are designed to counteract and outweigh any hyperglycemic tendency from the glucagon arm, while glucagon’s favorable effects on resting energy expenditure and hepatic lipid handling are retained.5 In preclinical work, this careful receptor balance was tuned deliberately; the foundational pharmacology paper by Coskun and colleagues in Cell Metabolism (2022) characterized the binding ratios and demonstrated in rodent models that the glucagon component augmented fat-mass loss beyond what GLP-1/GIP co-agonism achieved at matched doses.5
It is worth emphasizing the developmental stage this represents. The compound entered human testing only in the early 2020s. The obesity Phase 2 trial (NCT04881760) and the type 2 diabetes Phase 2 trial (NCT04867785) both read out in 2023, and Phase 3 diabetes data began appearing in 2026.1,2,3 By comparison, semaglutide and tirzepatide each accumulated years of large outcome data before and after approval. Retatrutide is, in other words, a compound at the frontier of clinical evidence rather than one with a settled therapeutic profile.
From a research-handling standpoint, retatrutide is typically supplied as a lyophilized (freeze-dried) powder in vials of varying nominal peptide content, which is why the compound-specific literature on this site is organized by vial size, from smaller 6 mg presentations up through 30 mg vials. None of that supply framing implies human use; it reflects how a laboratory reference compound is catalogued. The essential point for this article is that retatrutide is a well-defined, single molecule with a documented mechanism and a small but growing body of controlled clinical data, all of it generated under investigational protocols.
The Molecular Mechanism: Three Receptors, One Peptide
To understand why retatrutide is being studied in type 2 diabetes, it helps to separate what each of its three receptor targets contributes and then consider how they interact. All three receptors are class B G-protein-coupled receptors that signal primarily through the Gs-adenylyl cyclase-cyclic AMP pathway, which is part of why a single peptide can be engineered to engage all of them.6
GLP-1 receptor agonism is the best-characterized arm. Activating GLP-1R on pancreatic beta cells enhances glucose-dependent insulin secretion, meaning insulin release is amplified when blood glucose is elevated but not when it is normal, which limits hypoglycemia risk. GLP-1R activation also suppresses inappropriate glucagon secretion from alpha cells, slows gastric emptying, and acts on hypothalamic circuits to reduce appetite. In the context of diabetes, the glucose-dependent insulinotropic effect is the central glucose-lowering mechanism.1
GIP receptor agonism adds a second incretin signal. GIP is the other major incretin hormone, and GIPR activation on beta cells further potentiates glucose-dependent insulin secretion. GIP biology is more nuanced than GLP-1 biology and its role in adipose tissue and appetite remains an area of active investigation, but in combination with GLP-1 activity it appears to improve both insulin secretion and insulin sensitivity, and it may improve gastrointestinal tolerability relative to GLP-1 activity alone.6
Glucagon receptor agonism is the distinguishing third arm and the one most specific to retatrutide’s design. Glucagon receptors are densely expressed in the liver, where glucagon signaling increases energy expenditure, promotes hepatic fat oxidation, and reduces hepatic steatosis. The preclinical rationale, established by Coskun and colleagues, was that layering controlled glucagon agonism on top of dual incretin action would recruit an energy-expenditure component absent from GLP-1/GIP drugs, producing greater fat loss and pronounced reductions in liver fat.5 The trade-off is that unbalanced glucagon activity could raise glucose or heart rate, which is precisely why the receptor potencies were tuned so that incretin-driven glucose lowering dominates.
Structural studies published in Cell Discovery in 2024 used cryo-electron microscopy to visualize how a single retatrutide molecule adopts distinct conformations to fit into the orthosteric binding pockets of GLP-1R, GIPR, and GCGR, and how it recruits the Gs protein at each.6 These structural insights matter because they explain how one peptide sequence can be a balanced agonist at three receptors that, while related, differ in the shape of their ligand-binding domains. The work also helps rationalize the observed potency ratios: retatrutide is reported to be a relatively more potent agonist at GIPR and GCGR with balanced GLP-1R activity, a profile that shapes both its efficacy and its side-effect signals.5,6
The net physiological hypothesis for type 2 diabetes, then, is multi-pronged. The incretin arms drive glucose-dependent insulin secretion and suppress excess glucagon secretion to lower blood glucose, the appetite-suppressing central effects and glucagon-mediated energy expenditure drive weight and fat loss, and hepatic glucagon action reduces the fatty liver that so often accompanies insulin resistance.4,5 Because obesity, hepatic steatosis, and hyperglycemia are mechanistically intertwined in type 2 diabetes, a molecule that addresses all three simultaneously is attractive in theory. Whether that theoretical elegance translates into durable, safe, real-world benefit is an empirical question that only the clinical trials can answer, and it is to those trials that we now turn.
The Key Clinical Evidence in Type 2 Diabetes
The cornerstone of retatrutide’s diabetes evidence is the Phase 2 trial led by Julio Rosenstock and colleagues, published in The Lancet in 2023 (registered as NCT04867785).1 This was a randomized, double-blind, placebo-controlled and active-controlled, parallel-group study conducted across sites in the United States. It randomized 281 adults with type 2 diabetes (275 in the efficacy analysis) whose glucose was inadequately controlled with diet and exercise or metformin. Participants had a mean age of 56 years, a mean diabetes duration of about eight years, and a mean baseline HbA1c in the high-7% to low-8% range, making this a reasonably representative early-diabetes population.1
Participants were assigned to placebo, to the GLP-1 receptor agonist dulaglutide 1.5 mg as an active comparator, or to one of several retatrutide regimens using different target doses and escalation schedules over a 36-week treatment period. The primary endpoint was the change in HbA1c at 24 weeks, with body weight and other metabolic measures as key secondary endpoints. The design deliberately tested multiple doses and titration speeds to characterize the dose-response relationship.1
The glucose-lowering results were substantial and dose-dependent. Mean HbA1c reductions at 24 weeks are summarized below.
| Group | Mean HbA1c change at 24 weeks |
|---|---|
| Placebo | -0.01% |
| Dulaglutide 1.5 mg (comparator) | -1.41% |
| Retatrutide 0.5 mg | -0.43% |
| Retatrutide 4 mg (no escalation) | -1.30% |
| Retatrutide 4 mg (escalation) | -1.39% |
| Retatrutide 8 mg (fast escalation) | -1.88% |
| Retatrutide 8 mg (slow escalation) | -1.99% |
| Retatrutide 12 mg (escalation) | -2.02% |
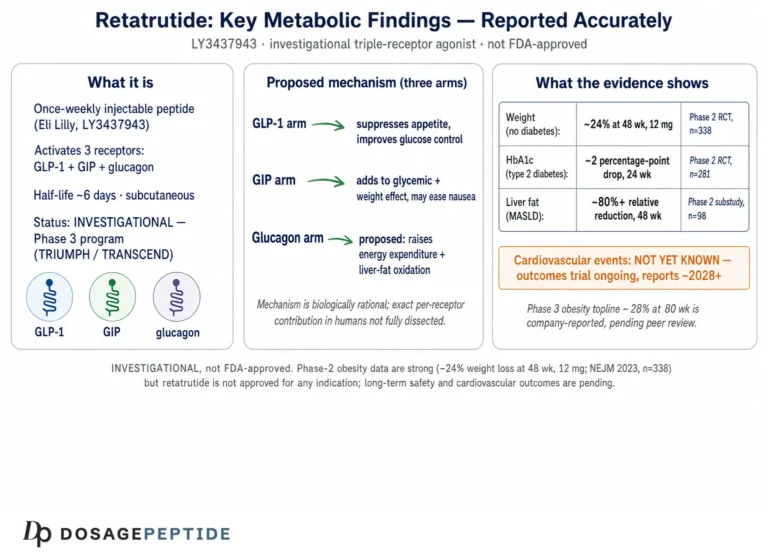
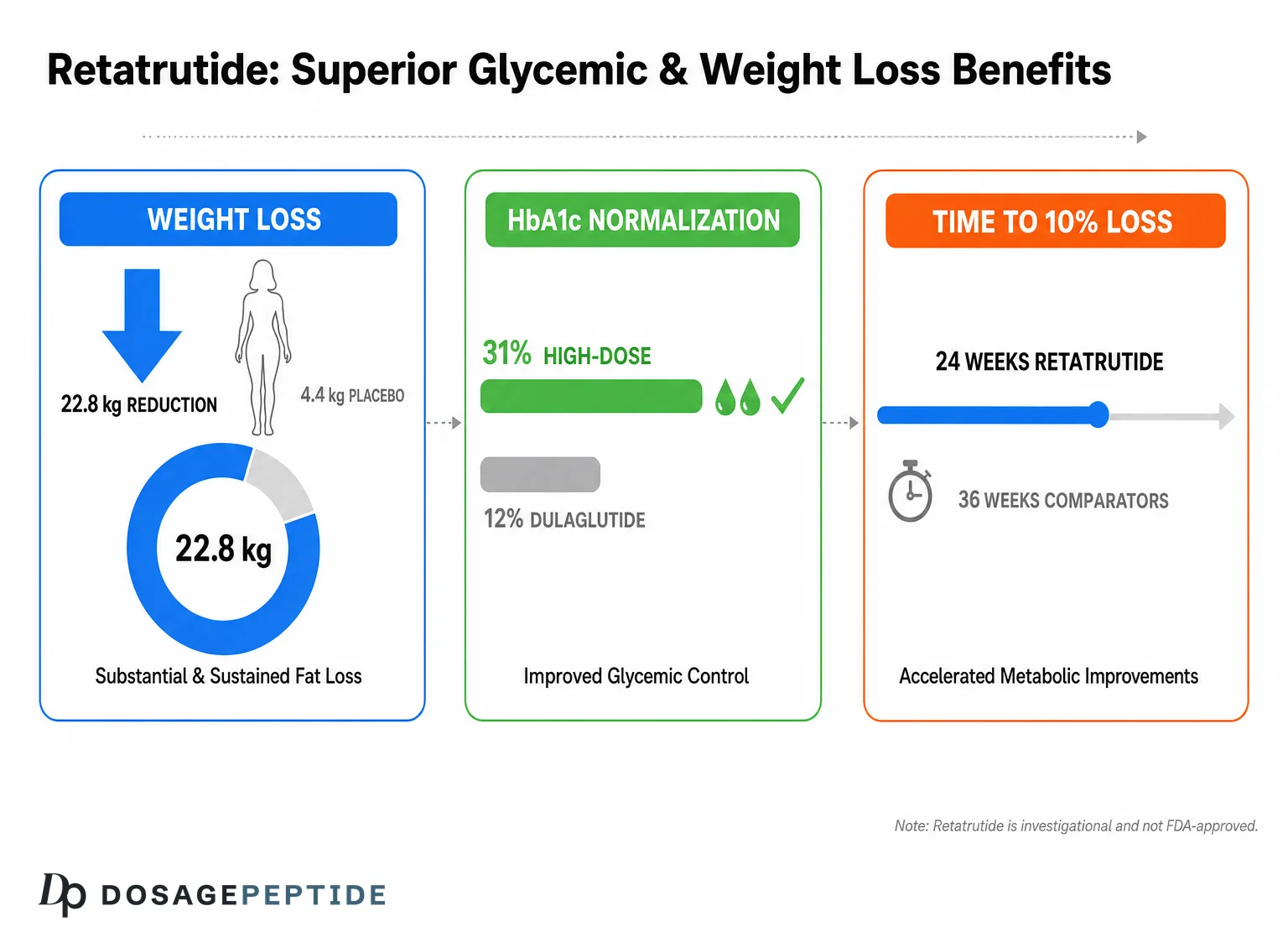
At the higher doses, HbA1c reductions of roughly 1.9% to 2.0% were achieved, and the reductions were statistically significantly greater than placebo in all groups except the lowest 0.5 mg dose.1 Compared with dulaglutide, the 8 mg slow-escalation and 12 mg groups produced significantly greater HbA1c lowering, which is notable given that dulaglutide is itself an established, effective GLP-1 agent. A large proportion of participants on the higher retatrutide doses reached an HbA1c below 6.5%, the threshold sometimes used to define normoglycemia, though this should be read as a within-trial biomarker outcome rather than evidence of disease reversal.1
Weight loss over the 36-week treatment period was also strongly dose-dependent, ranging from about 3.2% at the lowest dose to 16.9% at the 12 mg dose, compared with roughly 3.0% for placebo and 2.0% for dulaglutide.1 The concurrent achievement of large HbA1c and weight reductions is mechanistically coherent, since fat loss improves insulin sensitivity and reinforces glycemic improvement. Investigators also reported favorable movement in blood pressure and lipid measures, consistent with the broader cardiometabolic effects seen in the parallel obesity trial.1,2
A further methodological strength of this trial was its use of multiple escalation schedules at the same target dose, which allowed investigators to separate the influence of how quickly a dose is reached from the influence of the dose itself. The finding that the 8 mg slow-escalation arm achieved slightly greater HbA1c lowering than the 8 mg fast-escalation arm, while both were well tolerated, is a practically useful observation: it suggests that a more gradual approach may not sacrifice efficacy and may improve tolerability, an insight that directly informed the escalation strategies carried forward into the Phase 3 program.1 Nonetheless, these are secondary, exploratory comparisons within a Phase 2 study and were not the trial’s primary hypothesis, so they should be read as hypothesis-generating rather than definitive.
It is essential to frame the evidence level honestly. This was a Phase 2, dose-finding study of modest size (a few hundred participants) and short duration (36 weeks). It was designed to establish proof of concept and inform dose selection, not to demonstrate long-term glycemic durability, cardiovascular or renal outcomes, or safety across years of exposure. HbA1c and weight are validated surrogate endpoints, but they are surrogates; they do not by themselves prove reductions in the complications that matter most to people with diabetes. The Phase 2 signal was strong enough to justify a large Phase 3 program, and it is that program, not this single trial, that will determine retatrutide’s ultimate place, if any, in diabetes care. Readers who want the compound-level reference material can review the Retatrutide 10 mg reconstitution reference for how the molecule is described outside the clinical context.
Phase 3 Signals: TRANSCEND-T2D-1 and the TRIUMPH Program
Since the Phase 2 readout, retatrutide has advanced into an extensive Phase 3 development program. For type 2 diabetes specifically, the most directly relevant published result is the TRANSCEND-T2D-1 trial, reported by Harpreet Bajaj and colleagues in The Lancet in 2026 (NCT06354660).3 This was a Phase 3, randomized, double-blind, placebo-controlled study conducted across 48 sites in the United States, Mexico, and India, enrolling 537 adults with type 2 diabetes inadequately controlled with diet and exercise. The population was somewhat earlier in disease course than the Phase 2 cohort, with a mean diabetes duration of about 2.5 years, a mean baseline HbA1c of 7.9%, and a mean BMI of about 36 kg/m2.3
Participants were randomized to retatrutide 4 mg, 9 mg, or 12 mg, or placebo, once weekly for 40 weeks. The results reinforced the Phase 2 signal. Mean HbA1c reductions were -1.69% at 4 mg, -1.86% at 9 mg, and -1.94% at 12 mg, versus -0.81% with placebo, giving placebo-adjusted treatment differences of roughly 0.9% to 1.1% (all p<0.0001).3 Body-weight reductions were -11.5%, -13.9%, and -15.3% across the three doses versus -2.6% for placebo. In other words, a larger and more rigorously powered Phase 3 trial reproduced the twin findings of meaningful glucose lowering and substantial weight loss first seen in Phase 2.3
| Group (40 weeks) | Mean HbA1c change | Mean weight change |
|---|---|---|
| Placebo | -0.81% | -2.6% |
| Retatrutide 4 mg | -1.69% | -11.5% |
| Retatrutide 9 mg | -1.86% | -13.9% |
| Retatrutide 12 mg | -1.94% | -15.3% |
Beyond TRANSCEND-T2D-1, retatrutide is being evaluated in the broader TRIUMPH registrational program, a suite of Phase 3 trials whose rationale and design were described in a dedicated methodology paper.8 The TRIUMPH trials span general obesity, obesity with type 2 diabetes, obesity with established cardiovascular disease, obstructive sleep apnea, and knee osteoarthritis, reflecting a strategy of testing the compound across multiple obesity-related conditions. Within this program, at least one trial bears directly on diabetes: TRIUMPH-2 studies obesity in adults with type 2 diabetes. Some trials in the wider development program are designed with active comparators rather than placebo, though the specific design of each diabetes-relevant trial should be confirmed against its own registry entry before being relied upon. Publicly reported timelines placed many of these readouts across 2026.8
On the obesity side, which is closely related because most people with type 2 diabetes also carry excess weight, topline Phase 3 results have begun to appear. Reporting on the pivotal general-obesity trial TRIUMPH-1 described average weight reductions of up to roughly 30% at the highest dose, extending the striking Phase 2 obesity results into a larger population.9 These obesity figures are relevant context for diabetes management because weight loss of that magnitude typically drives large improvements in glycemia, but they are weight endpoints, not glucose endpoints, and should not be conflated with proof of diabetes benefit.
Two cautions are important when interpreting this Phase 3 material. First, at the time of writing, much of the diabetes-specific Phase 3 evidence remains partial: TRANSCEND-T2D-1 is published, but several diabetes-relevant TRIUMPH trials had readouts pending or reported only as topline summaries rather than full peer-reviewed manuscripts. Topline press announcements are not equivalent to complete published data with full safety tables and adjudicated endpoints. Second, none of these trials is a cardiovascular or renal outcomes trial of the kind that ultimately defines a diabetes drug’s clinical value; those studies take years and had not reported. The trajectory is clearly positive, but the file is not yet complete.
It is also useful to keep the population differences between the Phase 2 and Phase 3 diabetes cohorts in view when comparing their numbers. The Phase 3 TRANSCEND-T2D-1 participants had a much shorter mean diabetes duration (about 2.5 years versus roughly 8 years in Phase 2) and a lower baseline HbA1c, which tends to compress the absolute reduction achievable because there is simply less elevation to correct. That the Phase 3 trial still delivered placebo-adjusted HbA1c differences above 1% in an earlier, better-controlled population is arguably more impressive than the raw numbers suggest, though it also means the two trials are not directly interchangeable and their results should be read as complementary rather than as a single continuous dataset.1,3
How Retatrutide Compares With Related Compounds
Retatrutide does not exist in a vacuum; it is the newest member of a rapidly evolving class, and its significance is best understood by comparison with the incretin agents that preceded it. The most useful comparators are the GLP-1 receptor agonists semaglutide and dulaglutide, and the dual GIP/GLP-1 receptor agonist tirzepatide.
Against dulaglutide, retatrutide has the advantage of a head-to-head comparison within its own Phase 2 diabetes trial. There, the higher retatrutide doses produced significantly greater HbA1c reductions than dulaglutide 1.5 mg, and dramatically greater weight loss (roughly 17% versus 2%).1 This is a genuine within-trial comparison rather than a cross-study inference, which strengthens it, though dulaglutide 1.5 mg is a mid-range rather than maximal GLP-1 dose.
Against semaglutide and tirzepatide, no head-to-head diabetes trials had been published at the time of writing, so any comparison relies on cross-trial inference, which is methodologically weak because populations, durations, and designs differ. With that caveat, the pattern in the literature is that each additional receptor arm has tended to increase efficacy: single-agonist GLP-1 therapy, then dual GIP/GLP-1 therapy with tirzepatide, then triple agonism with retatrutide, with weight-loss magnitudes broadly increasing along that sequence.2 The compound reference material on this site frames the often-cited contrast as roughly 24% weight loss with retatrutide at 48 weeks in the obesity Phase 2 trial versus about 21% for tirzepatide at 72 weeks in its own program, but such numbers come from separate studies and cannot be treated as a fair head-to-head.2 The sponsor’s own reporting of that Phase 2 obesity trial noted an interim mean weight reduction of up to roughly 17.5% by 24 weeks, before the larger 48-week figure accrued, which underscores that the headline numbers depend heavily on the time point chosen.7
| Feature | GLP-1 agonists (e.g., semaglutide, dulaglutide) | Tirzepatide | Retatrutide |
|---|---|---|---|
| Receptor targets | GLP-1R | GIP/GLP-1R | GIP/GLP-1R/GCGR |
| Class | Single agonist | Dual agonist | Triple agonist |
| Distinct energy-expenditure arm | No | No | Yes (glucagon) |
| Regulatory status (T2D) | Approved | Approved | Investigational, not approved |
| Head-to-head diabetes data vs. retatrutide | Yes (dulaglutide, Phase 2) | No published | – |
The mechanistic distinction that sets retatrutide apart from its predecessors is the glucagon arm and its putative energy-expenditure and hepatic-fat effects. This is supported by the MASLD (metabolic dysfunction-associated steatotic liver disease) Phase 2a data discussed later, in which retatrutide produced very large reductions in liver fat, a signal not typically as pronounced with pure incretin agents.4 For a person with type 2 diabetes and fatty liver, that hepatic effect could in principle be an advantage, but it remains a hypothesis grounded in early-phase data rather than a proven differentiator.
A fair comparative summary is this: retatrutide’s early efficacy signals in both glucose and weight are at least as strong as, and by some measures numerically larger than, the best currently approved incretin therapies. But approved agents like semaglutide and tirzepatide carry something retatrutide entirely lacks, namely regulatory approval, large long-term safety databases, and in some cases dedicated cardiovascular outcome data. Efficacy is only one axis of comparison; the evidence maturity axis strongly favors the established drugs. Anyone weighing the class should treat retatrutide as a promising investigational entrant rather than a proven step-change, and should be skeptical of cross-trial “retatrutide beats X” claims that ignore study-design differences. Compound-level reference pages such as the Retatrutide 20 mg vial reference describe the molecule itself but do not, and cannot, substitute for that missing long-term outcome evidence.
Research Models and Trial Methodology
Understanding retatrutide’s evidence requires understanding how that evidence was generated, because the strength of a conclusion depends on the design that produced it. The retatrutide record spans a familiar translational ladder: in vitro receptor pharmacology, rodent models, and then human trials of increasing size and rigor.
At the in vitro and preclinical level, the foundational work by Coskun and colleagues characterized retatrutide’s activity at cloned human GLP-1, GIP, and glucagon receptors, measuring cyclic AMP signaling to establish the balance of potencies across the three targets.5 This receptor-level work defined what “balanced triple agonism” means quantitatively. It was followed by studies in rodent models of obesity, in which retatrutide produced greater fat-mass reduction than dual agonism and demonstrated the glucagon-driven increase in energy expenditure and reduction in liver fat that motivated the whole program.5 These are essential mechanistic experiments, but they are, by definition, preclinical: results in mice do not establish efficacy or safety in humans, and appetite, metabolism, and cardiovascular physiology differ meaningfully across species. The 2024 Cell Discovery structural study added another preclinical layer, using cryo-electron microscopy to resolve how the peptide engages each receptor at the molecular level.6
At the clinical level, the methodology grows progressively more robust. The Phase 2 diabetes trial used the design features that lend credibility to a glucose-lowering claim: randomization to remove selection bias, double-blinding to prevent placebo and observer effects, a placebo control to isolate drug effect, and, importantly, an active comparator (dulaglutide) to benchmark against an established therapy.1 The inclusion of multiple doses and escalation schedules was a dose-finding feature, letting investigators map the dose-response relationship and identify titration approaches that balance efficacy against gastrointestinal tolerability. HbA1c at 24 weeks was the primary endpoint, a well-validated surrogate that integrates glycemia over roughly three months.1
The Phase 3 TRANSCEND-T2D-1 trial preserved these strengths and added scale and geographic diversity, enrolling 537 participants across three countries, which improves the generalizability of the findings and the precision of the effect estimates.3 Larger sample sizes narrow confidence intervals and allow rarer adverse events to surface. The TRIUMPH program extends the methodology further into disease-specific populations and active-comparator designs.8
Several methodological limitations recur across this literature and deserve explicit mention. Trial durations remain relatively short for a chronic disease: 36 to 48 weeks captures glycemic and weight response but not multi-year durability or the accrual of hard clinical outcomes. Populations in early-phase trials are enriched for participants likely to tolerate and respond to the drug and are not fully representative of the broader diabetes population, which includes people with long-standing disease, advanced complications, renal impairment, and extensive comorbidity. Surrogate endpoints such as HbA1c, body weight, and liver-fat fraction are validated and clinically meaningful, but they are not the same as reductions in myocardial infarction, stroke, kidney failure, or death, which only dedicated long-term outcome trials can demonstrate. And industry sponsorship, while standard and not inherently invalidating, is a factor a careful reader notes when weighing any drug-development program. None of these caveats undercut the positive signal; they simply define the boundary of what the current methodology can legitimately support.
Safety and Tolerability
Any honest appraisal of retatrutide must give safety equal weight to efficacy, because a drug’s risk profile is what ultimately gates its use. The safety picture from the published trials is broadly consistent with the incretin class, with a few signals specific to the glucagon arm that warrant attention.
The dominant adverse events are gastrointestinal: nausea, vomiting, diarrhea, and constipation. In the Phase 2 diabetes trial, gastrointestinal events occurred in roughly 35% of retatrutide-treated participants, were generally mild to moderate in severity, appeared most often during dose escalation, and tended to subside over time.1 This is the same tolerability pattern seen with GLP-1 and GIP/GLP-1 agonists and is the principal reason that gradual dose titration is built into the trial protocols. In the Phase 3 TRANSCEND-T2D-1 trial, gastrointestinal events were again the most frequent adverse events, mostly mild to moderate, and discontinuations due to adverse events were low, in the range of 2% to 5% across retatrutide doses versus 0% for placebo.3
Regarding hypoglycemia, a central safety concern for any glucose-lowering drug, the trials are reassuring on this specific point. No severe hypoglycemia was reported in either the Phase 2 or Phase 3 diabetes trials, consistent with the glucose-dependent mechanism of incretin action, in which insulin is stimulated preferentially when glucose is high.1,3 Hypoglycemia risk would be expected to rise mainly when retatrutide is combined with insulin or sulfonylureas, a combination the early trials largely did not test.
Two signals related to the glucagon and dose-response profile merit specific attention. First, retatrutide produced a dose-dependent increase in heart rate; in the obesity Phase 2 trial, mean heart rate rose by roughly 5 to 7 beats per minute at higher doses, increasing up to about week 24 and then declining thereafter.2 Small increases in heart rate are seen across the incretin class, but the magnitude and its interaction with glucagon-driven physiology are being watched closely, and cardiac arrhythmias were reported at higher frequency than placebo in some analyses, though not classified as serious.2 Second, a cutaneous hyperesthesia or skin-sensitivity signal was noted, reported in about 7% of retatrutide participants versus 1% of placebo participants in the obesity trial; none of these events were severe, serious, or led to discontinuation, but it is an unusual signal not typical of pure incretin agents and appears related to the compound.2
| Safety domain | What the trials reported |
|---|---|
| Gastrointestinal (nausea, vomiting, diarrhea) | Most common; mild-moderate; dose-escalation related; subside over time |
| Severe hypoglycemia | None reported in the diabetes trials |
| Heart rate | Dose-dependent increase (~5-7 bpm at higher doses), later declining |
| Cutaneous hyperesthesia | ~7% vs ~1% placebo (obesity trial); none severe or serious |
| Discontinuation due to adverse events | Low (~2-5%) vs 0% placebo in Phase 3 T2D |
The critical safety caveat is what the current data cannot tell us. The trials to date are too short and too small to characterize rare but serious risks, long-term cardiovascular safety, effects on the pancreas or thyroid C-cells (a labeled concern for the incretin class based on rodent data), or safety in vulnerable subgroups. Dedicated cardiovascular outcome data, which are considered essential for a modern diabetes drug, had not been reported. A study of retatrutide’s effects on renal function in people with overweight or obesity and chronic kidney disease (NCT05936151) speaks to the kind of subgroup work still in progress.10 Until such long-term and subgroup data mature, retatrutide’s safety profile should be described as “reassuring in early trials but not yet fully defined.”
Handling and Reconstitution in a Research Context
Because retatrutide is an investigational compound that laboratories and researchers may encounter as a reference material, a brief note on its physical handling is warranted, framed strictly in a research context and not as any instruction for human use. In clinical trials, retatrutide is administered as a once-weekly subcutaneous injection using pre-specified, pharmacy-prepared formulations under medical supervision; nothing in this section describes or endorses self-administration.
As supplied for laboratory purposes, retatrutide is typically a lyophilized peptide powder, freeze-dried to maximize stability during shipping and storage. Lyophilized peptides of this class are generally stored cold and protected from light and moisture, and the dry powder is comparatively stable. The peptide’s albumin-binding fatty-acid modification, which confers its long circulating half-life in vivo, is a feature of the molecule’s design rather than something that affects benchtop handling.5
Reconstitution, in a research context, refers to dissolving the lyophilized powder in an appropriate sterile diluent, most commonly bacteriostatic or sterile water, to produce a defined-concentration solution for laboratory measurement or in vitro work. Peptides are sensitive molecules: they can be degraded by vigorous agitation, extreme pH, repeated freeze-thaw cycles, and prolonged storage of the reconstituted solution at room temperature. General good practice in peptide handling therefore emphasizes gentle mixing rather than shaking, careful attention to diluent volume so that concentration is accurately known, and cold storage of any reconstituted solution with minimized freeze-thaw cycling. Because the vials are labeled by nominal peptide content, the relationship between vial mass, diluent volume, and resulting concentration is a matter of straightforward dilution arithmetic that the compound-specific reference pages lay out.
This site organizes that reference material by vial size precisely because the reconstitution math changes with the amount of peptide in the vial. Readers seeking the concentration and handling details for specific presentations can consult the 12 mg vial reference, the 6 mg vial reference, or the higher-content 30 mg vial reference, all of which treat the compound as a laboratory material. The essential and non-negotiable framing is that retatrutide is investigational and not approved for human use; handling information exists to support accurate laboratory work, not to facilitate consumption. No reconstitution guide, on this site or anywhere else, converts an unapproved research compound into a medicine.
Limitations and the Human-Evidence Gap
Having surveyed the encouraging efficacy signals, it is important to devote focused attention to the limits of what is actually known, because the gap between “promising Phase 2 and early Phase 3 data” and “proven therapy” is wide and consequential. Overstating retatrutide’s evidentiary standing would be a disservice to readers.
The first and most fundamental limitation is evidence maturity. Retatrutide’s diabetes efficacy rests on one Phase 2 trial and one published Phase 3 trial, supplemented by topline announcements from an ongoing program.1,3,8 By the standards of an approved diabetes drug, this is a thin file. Approved agents accumulate tens of thousands of patient-years of exposure across numerous trials and post-marketing surveillance before their risk-benefit balance is considered settled. Retatrutide is early on that curve.
The second limitation is the surrogate-endpoint problem. Every efficacy claim discussed here rests on surrogate markers: HbA1c, body weight, liver-fat fraction, blood pressure, and lipids. These are validated and clinically meaningful surrogates, and improving them is genuinely valuable, but they are not the outcomes that ultimately define a diabetes therapy’s worth. Whether retatrutide reduces heart attacks, strokes, kidney failure, amputations, or death, and whether its benefits persist over many years, cannot be inferred from HbA1c and weight alone. Only long-term cardiovascular and renal outcome trials can answer those questions, and at the time of writing those definitive outcome data were not available.
Third is the durability and real-world question. Trials of 36 to 48 weeks show what happens over roughly a year in selected, closely monitored participants. They do not show what happens over five or ten years, whether weight and glycemic benefits are maintained after the titration period, what happens on discontinuation (weight regain is common across the class), or how the drug performs in the messy reality of routine care with imperfect adherence and complex comorbidity.
Fourth are unresolved safety uncertainties. The glucagon-related heart-rate increase, the cutaneous hyperesthesia signal, and the class-wide theoretical concerns around pancreatitis and thyroid C-cell effects all require larger and longer datasets to characterize fully.2 Rare serious events, by their nature, are only detectable in large populations followed for a long time.
Fifth, and pervasive across the peptide-education landscape, is the gap between the clinical record and non-clinical claims. A great deal of online content about retatrutide extrapolates well beyond the trial data, presents cross-study comparisons as if they were head-to-head, or blurs the line between an investigational compound and a marketed medicine. The disciplined reading is to anchor every claim to a primary source, to note the evidence level (in vitro, animal, Phase 2, Phase 3) attached to each, and to treat anything beyond that as speculation. Where preclinical or animal data are cited, as with the energy-expenditure and liver-fat mechanisms, those findings are hypothesis-generating for humans, not confirmatory.4,5 The honest bottom line is that retatrutide is one of the most promising metabolic compounds in development, and simultaneously an unapproved agent whose long-term human risk-benefit profile is not yet established. Both statements are true, and holding them together is the essence of an evidence-cautious appraisal.
Regulatory Status
The regulatory status of retatrutide can be stated simply and unambiguously: it is an investigational drug that, as of this writing in 2026, has not been approved by the FDA, the EMA, or any other major regulatory authority for the treatment of type 2 diabetes, obesity, or any other indication.1,8 It is available to humans only through participation in authorized clinical trials conducted under regulatory oversight.
To place this in the regulatory framework: a compound must pass through Phase 1 (safety and pharmacokinetics in small numbers of volunteers), Phase 2 (dose-finding and proof of concept), and Phase 3 (large, confirmatory trials) before a sponsor can submit a marketing application. A regulator then reviews the complete efficacy and safety dossier and, if satisfied, grants approval for specific indications with a defined label. Retatrutide is in the Phase 3 stage of this process.8 Its sponsor, Eli Lilly, has been running the TRIUMPH and TRANSCEND registrational programs precisely to generate the confirmatory evidence a regulatory submission requires, and public reporting has pointed to a potential regulatory filing in the 2026-2027 window, contingent on the trial results.8
Several practical implications follow from this status. Because retatrutide is not approved, it has no regulator-sanctioned dosing, no approved label, no official indication, and no pharmacy-dispensed prescription form. Any material sold outside a clinical trial as “retatrutide” is not an approved medicine, is not subject to the manufacturing and quality controls that govern approved drugs, and cannot be assumed to match the purity, identity, or content of the trial compound. This is a substantial safety consideration entirely separate from the drug’s intrinsic pharmacology. The compound-specific reference pages on this site, including the individual vial pages and the dosage catalog, exist for educational and research-literacy purposes and describe the molecule as characterized in the scientific literature; they do not represent, and cannot substitute for, an approved therapeutic product.
It is also worth distinguishing between the obesity and diabetes regulatory pathways, since a drug can be approved for one indication before another. Retatrutide’s most advanced Phase 3 readouts to date have been on the obesity side, and it is plausible that an obesity indication could precede a diabetes indication if the program proceeds favorably.9 But even an obesity approval, were it to come, would not by itself constitute approval for type 2 diabetes management, which requires its own dedicated evidence and a separate regulatory decision. Until such decisions are made and published, the accurate and responsible characterization of retatrutide for diabetes is: investigational, supported by encouraging but incomplete clinical evidence, and not approved for use.
Frequently Asked Questions
Is retatrutide approved to treat type 2 diabetes?
No. Retatrutide is an investigational triple hormone receptor agonist in Phase 3 development. As of 2026 it has not been approved by the FDA, EMA, or any other major regulator for type 2 diabetes or any other condition. It is available to humans only within authorized clinical trials.1,3,8
How much did retatrutide lower HbA1c in the diabetes trials?
In the Phase 2 diabetes trial, mean HbA1c fell by up to roughly 2.0% at the higher doses over 24 weeks, versus essentially no change with placebo and about 1.4% with the comparator dulaglutide.1 The Phase 3 TRANSCEND-T2D-1 trial reported HbA1c reductions of about 1.7% to 1.9% at 40 weeks versus 0.8% with placebo.3 These are surrogate biomarker outcomes from investigational trials, not proof of long-term disease outcomes.
What makes retatrutide different from tirzepatide and semaglutide?
Semaglutide is a single GLP-1 receptor agonist and tirzepatide is a dual GIP/GLP-1 receptor agonist. Retatrutide adds a third arm, glucagon receptor agonism, which in preclinical models increases energy expenditure and reduces liver fat. This triple mechanism is the defining structural difference.5,6 However, unlike the other two, retatrutide is not approved and lacks long-term outcome data, and no published head-to-head diabetes trials against tirzepatide or semaglutide exist.
What are the most common side effects reported?
Gastrointestinal effects, mainly nausea, vomiting, diarrhea, and constipation, are the most common, typically mild to moderate and most frequent during dose escalation.1,3 Trials also noted a dose-dependent increase in heart rate and a cutaneous hyperesthesia (skin-sensitivity) signal.2 No severe hypoglycemia was reported in the diabetes trials.1,3
Does retatrutide help with fatty liver in people with diabetes?
A Phase 2a trial in metabolic dysfunction-associated steatotic liver disease (MASLD) reported large reductions in liver fat, up to about 82% at higher doses at 24 weeks, with most higher-dose participants achieving liver-fat normalization.4 This is an encouraging early-phase signal relevant to the many people who have both diabetes and fatty liver, but it comes from a small proof-of-concept study and is not an approved use.
Why does a diabetes drug include glucagon activity, which raises blood sugar?
It is counterintuitive, but the receptor potencies are balanced so that the strong glucose-lowering effects of the GLP-1 and GIP arms dominate over glucagon’s hyperglycemic tendency, while glucagon’s beneficial effects on energy expenditure and liver-fat handling are retained.5 The net effect in the trials was robust glucose lowering alongside substantial weight and liver-fat reduction.
When might retatrutide become available?
Timing depends entirely on the ongoing Phase 3 trials and subsequent regulatory review. Public reporting has pointed to a possible regulatory filing in the 2026-2027 window, but approval is never guaranteed and would follow, not precede, complete review of the full safety and efficacy dossier.8 Until then it remains investigational.
Is retatrutide sold online the same as the trial compound?
No assumption of equivalence is warranted. Because retatrutide is not an approved medicine, any material sold outside a clinical trial is not manufactured or quality-controlled under the standards that govern approved drugs, and its identity, purity, and content cannot be assumed to match the compound used in the published trials. This is an important safety consideration independent of the drug’s pharmacology.1
Closing Disclaimer
This article is provided strictly for educational and research-literacy purposes. It summarizes published scientific literature about an investigational compound and is not medical advice, a treatment recommendation, or an endorsement of any use of retatrutide. Retatrutide is not approved by the FDA, EMA, or other major regulators, and nothing here should be interpreted as guidance to obtain, prepare, or use it. Anyone with questions about type 2 diabetes management should consult a qualified, licensed healthcare professional. Statements about efficacy and safety reflect the evidence level of their sources, which range from preclinical and in vitro work to early- and late-phase human trials, and should be read with the limitations described above in mind.
References
- Rosenstock J, Frias J, Jastreboff AM, et al. Retatrutide, a GIP, GLP-1 and glucagon receptor agonist, for people with type 2 diabetes: a randomised, double-blind, placebo and active-controlled, parallel-group, phase 2 trial conducted in the USA. Lancet. 2023. NCT04867785. https://pubmed.ncbi.nlm.nih.gov/37385280/
- Jastreboff AM, Kaplan LM, Frias JP, et al. Triple-Hormone-Receptor Agonist Retatrutide for Obesity – A Phase 2 Trial. New England Journal of Medicine. 2023. NCT04881760. https://www.nejm.org/doi/full/10.1056/NEJMoa2301972
- Bajaj HS, et al. Efficacy and safety of retatrutide in people with type 2 diabetes and inadequate glycaemic control with diet and exercise (TRANSCEND-T2D-1): a double-blind, randomised, phase 3 trial. Lancet. 2026. NCT06354660. https://pubmed.ncbi.nlm.nih.gov/42250575/
- Sanyal AJ, Kaplan LM, Frias JP, et al. Triple hormone receptor agonist retatrutide for metabolic dysfunction-associated steatotic liver disease: a randomized phase 2a trial. Nature Medicine. 2024. https://pmc.ncbi.nlm.nih.gov/articles/PMC11271400/
- Coskun T, Urva S, Roell WC, et al. LY3437943, a novel triple glucagon, GIP, and GLP-1 receptor agonist for glycemic control and weight loss: From discovery to clinical proof of concept. Cell Metabolism. 2022;34(9). https://www.cell.com/cell-metabolism/fulltext/S1550-4131(22)00312-6
- Structural insights into the triple agonism at GLP-1R, GIPR and GCGR manifested by retatrutide. Cell Discovery. 2024. https://www.nature.com/articles/s41421-024-00700-0
- Eli Lilly and Company. Lilly’s phase 2 retatrutide results published in The New England Journal of Medicine show up to 17.5% mean weight reduction at 24 weeks. Investor news release, 2023. investor.lilly.com
- Retatrutide for the treatment of obesity, obstructive sleep apnea and knee osteoarthritis: Rationale and design of the TRIUMPH registrational clinical trials. PubMed, 2025. https://pubmed.ncbi.nlm.nih.gov/41090431/
- Retatrutide Achieves Up to 30.3% Average Weight Loss in Phase 3 TRIUMPH-1 Trial. AJMC, 2026. ajmc.com
- A Study of Retatrutide (LY3437943) on Renal Function in Participants With Overweight or Obesity and Chronic Kidney Disease With or Without Type 2 Diabetes. ClinicalTrials.gov, NCT05936151. https://clinicaltrials.gov/study/NCT05936151