Few naming conventions in the peptide research literature cause as much confusion as the relationship between Thymosin Beta-4 and the research-market label “TB-500.” The central research question this reference addresses is deceptively simple: when a study or a research supplier refers to Thymosin Beta-4 (Tβ4) and another refers to TB-500, are they describing the same molecule, a defined fragment of it, or two different things sold under overlapping names? The honest answer — explored in detail below — is that the terms are frequently treated as synonyms, but the underlying chemistry and the regulatory-evidence status behind each name are not identical, and product labeling in the research-chemical space is inconsistent enough that the phrase thymosin beta-4 vs tb-500 cannot be reduced to a single tidy structural fact.
This article separates what is well established in the peer-reviewed literature about the endogenous protein Thymosin Beta-4 from what is claimed about the substance marketed as TB-500. It is written as educational reference material for people trying to read the science accurately — not as guidance for human use. Neither TB-500 nor systemic Thymosin Beta-4 is approved by the U.S. Food and Drug Administration for any indication, and both are prohibited in sport by the World Anti-Doping Agency.
What Is Thymosin Beta-4? Research Context
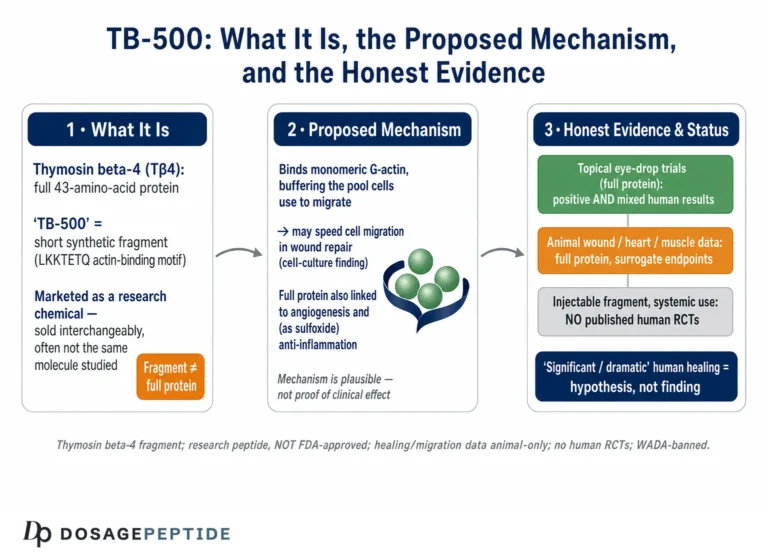
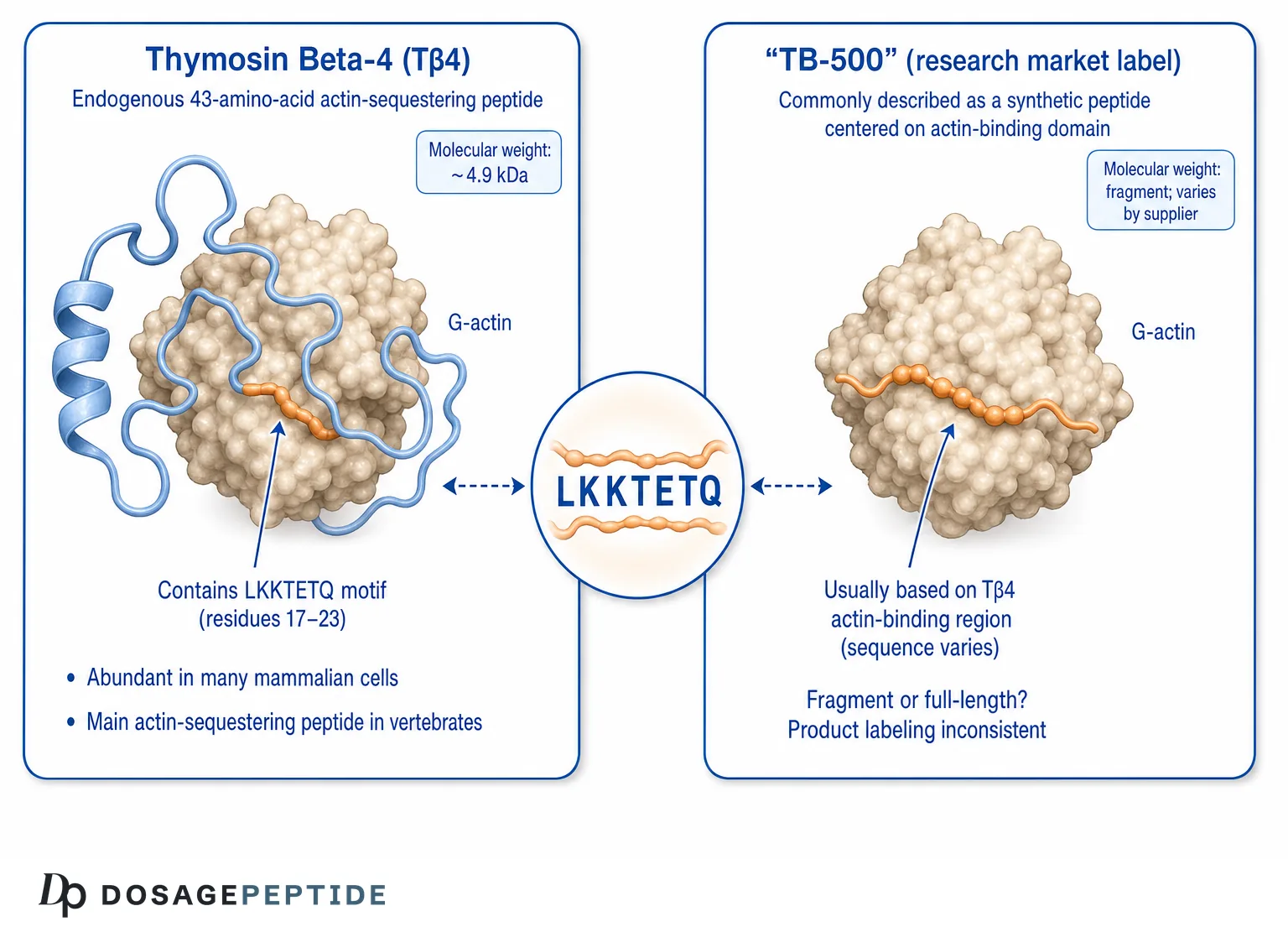
Thymosin Beta-4 is a naturally occurring, highly conserved 43-amino-acid peptide with a molecular weight of approximately 4.9 kDa (roughly 4963 Da for the human sequence).[1] It belongs to the beta-thymosin family and is one of the most abundant intracellular proteins in many mammalian cell types, present at micromolar-to-high-micromolar concentrations in cells such as platelets, macrophages, and neutrophils. Although it was originally isolated from thymus tissue — hence the “thymosin” name — it is not a thymic hormone in the classical sense; it is a cytosolic actin-binding peptide found throughout the body.[2]
The historical naming is worth understanding because it explains much of the modern confusion. Early fractionation of calf thymus in the 1960s and 1970s produced a crude preparation called “thymosin fraction 5,” from which individual peptides were later purified and assigned Greek-letter and numerical designations — thymosin alpha-1, thymosin beta-4, and others. These designations reflected chromatographic behavior (isoelectric point and elution order), not shared biological function. As a result, the beta-thymosins and the alpha-thymosins are structurally and functionally unrelated despite the shared “thymosin” family name. Readers interested in that distinction can compare this material with our overview of thymosin alpha-1 immune-modulation research, which describes a completely different peptide with a completely different mechanism.
From “thymic factor” to actin-binding peptide: a discovery timeline
The scientific understanding of Thymosin Beta-4 shifted substantially over several decades, and that shift explains why older and newer literature can seem to describe different molecules. When beta-thymosins were first purified, they were investigated in the context of immune and thymic biology, reflecting the tissue they were isolated from. It was only later, through biochemical work in the late 1980s and early 1990s, that Thymosin Beta-4 was identified as being the same entity as a previously described actin-sequestering factor — the peptide sometimes called “Fx.”[3] This convergence — recognizing that an intracellular actin regulator and a “thymosin” peptide were one and the same — reframed the molecule from a putative immune factor into a cytoskeletal regulator.
That reframing is important for the disambiguation task. Papers written before this convergence, and papers written after it, can use different conceptual vocabularies for the same peptide. A reader encountering the term in an immunology-flavored older paper and in a cell-biology-flavored newer paper should recognize that the molecule is the same defined 43-residue peptide, even though the framing differs. The research-market “TB-500” terminology emerged later still, largely outside the peer-reviewed tradition, which is why it does not carry the same precise definitional anchor that the biochemistry literature gives to “Thymosin Beta-4.”
The primary established function: actin sequestration
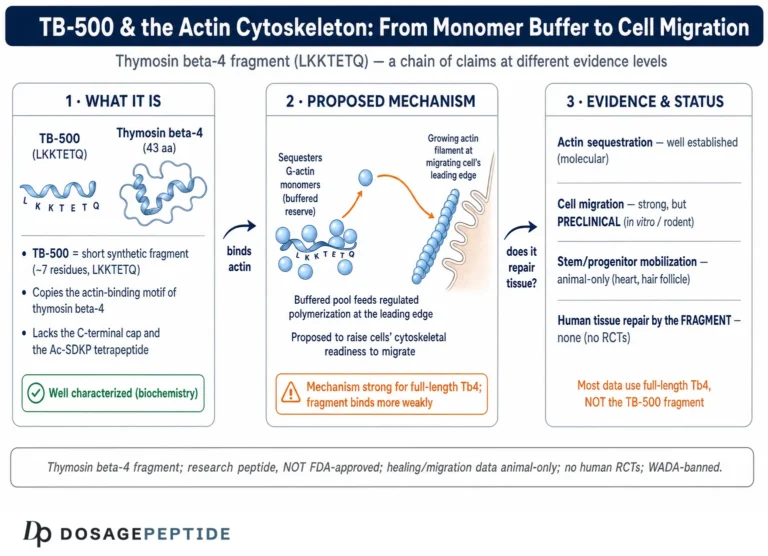
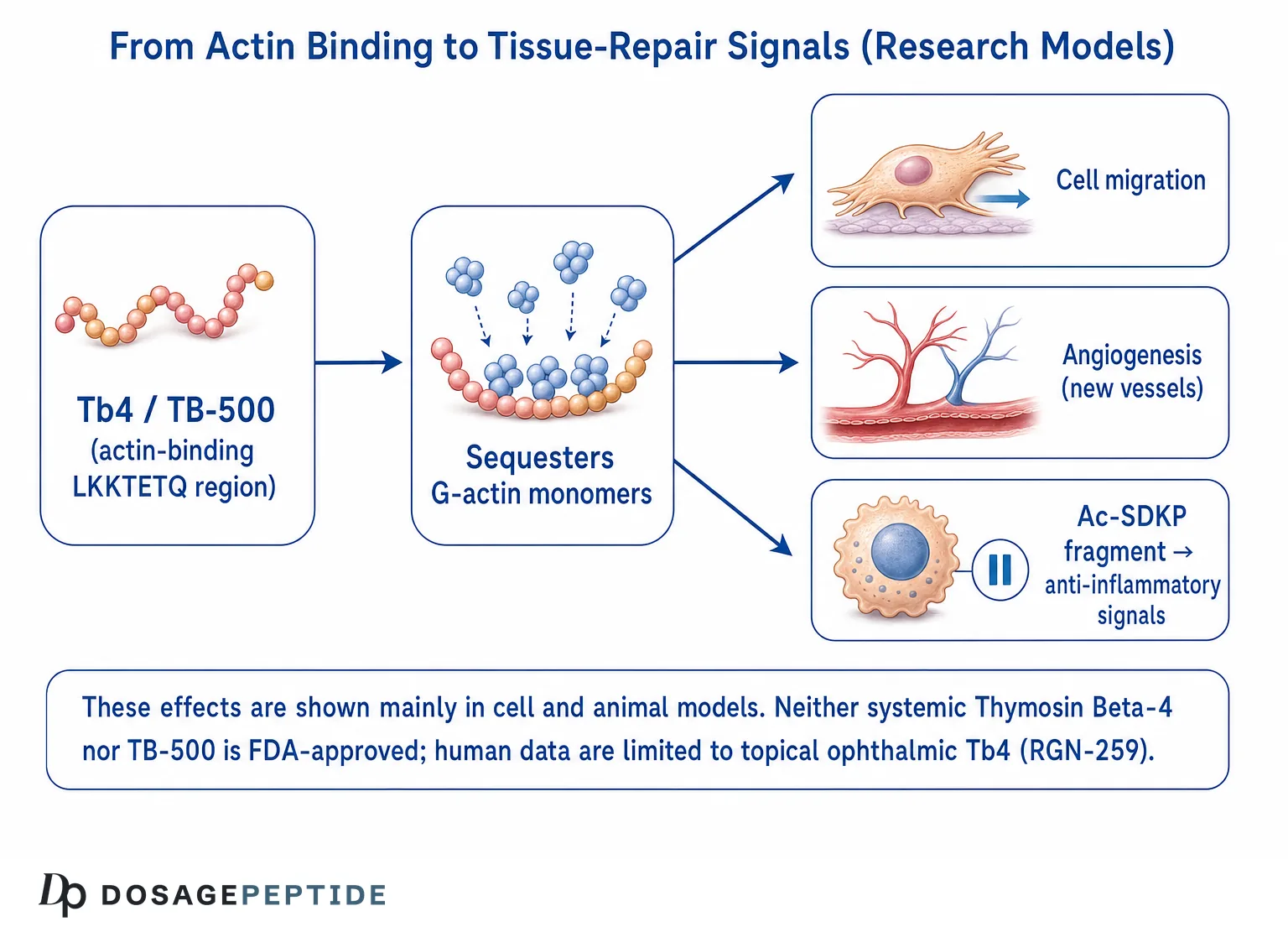
The best-characterized biochemical role of Thymosin Beta-4 is as the principal G-actin (monomeric actin) sequestering peptide in vertebrate cells. It binds monomeric globular actin in an approximately 1:1 stoichiometry and holds it in a form that is not immediately available for polymerization into filaments (F-actin).[3] By buffering the pool of polymerization-ready actin, Tβ4 participates in the dynamic control of the actin cytoskeleton — the scaffolding that governs cell shape, motility, and division. This is not a fringe claim; it is textbook cell biology supported by decades of biochemical and structural work.
Because so many downstream cellular behaviors depend on actin dynamics — cell migration, wound closure, angiogenesis — researchers have hypothesized that manipulating Tβ4 levels could influence tissue-repair processes. That hypothesis is the origin of essentially every therapeutic-sounding claim made about both Tβ4 and TB-500. It is important to hold two ideas at once: the actin-sequestration mechanism is well established, while the leap from that mechanism to reliable tissue-repair outcomes in humans is not.
Is TB-500 the Same as Thymosin Beta-4? The Core Disambiguation
Here is the heart of the is tb-500 thymosin beta 4 question, framed as honestly as the evidence allows. “TB-500” is not a designation that originates in the peer-reviewed biochemistry literature the way “Thymosin Beta-4” does. It is primarily a research-market and sport-doping-context label. What it actually refers to depends heavily on who is using the term:
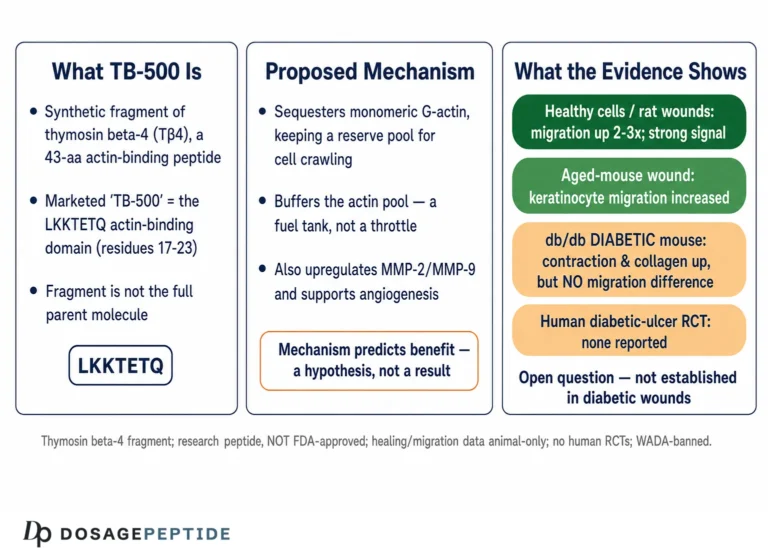
- As commonly described in research-supplier and anti-doping literature, TB-500 is often characterized as a synthetic peptide corresponding to the biologically active actin-binding region of Thymosin Beta-4, frequently associated with the sequence motif centered on LKKTETQ (the actin-binding domain, roughly residues 17–23 of the full protein).[4]
- In practice, however, labeling is inconsistent. Some material sold as “TB-500” is marketed as the full 43-residue Thymosin Beta-4 molecule, while other material is marketed as a shorter fragment. Independent published analyses of what is actually in research-market vials are limited, so a blanket statement that “TB-500 is always the fragment” or “TB-500 is always identical to full Tβ4” would overstate what can be verified.
So the precise answer to tb-500 vs tb4 is: they are closely related and often used interchangeably, but they are not guaranteed to be structurally identical. Thymosin Beta-4 refers to a specific, defined 43-amino-acid endogenous protein. TB-500 is a market/context label that usually refers either to that same protein or to a synthetic fragment built around its actin-binding domain. This nuance matters for anyone reading a study, because a paper studying recombinant full-length Tβ4 is not automatically evidence about a fragment product, and vice versa.
| Attribute | Thymosin Beta-4 (Tβ4, endogenous) | “TB-500” (research-market label) |
|---|---|---|
| Origin of the name | Peer-reviewed biochemistry; isolated from thymus fraction 5 | Research-chemical / anti-doping context; not a formal biochemical designation |
| Defined structure | Specific 43-amino-acid sequence, ~4.9 kDa | Variable; often described as a fragment around the LKKTETQ actin-binding domain, but labeling is inconsistent |
| Actin-binding motif | Contains LKKTETQ (residues ~17–23) | Typically centered on / marketed around this motif |
| Regulatory status | Not FDA-approved systemically; specific ophthalmic formulation (RGN-259) studied in human trials | Not FDA-approved for any indication |
| Sport status | Prohibited by WADA | Prohibited by WADA |
| Human clinical evidence | Limited, formulation-specific (mainly ophthalmic/wound) | Systemic efficacy claims are preclinical/animal |
Why the “fragment” story is plausible but not fully verifiable
The rationale behind a fragment product is biochemically reasonable. Structure–activity studies of Thymosin Beta-4 identified that a short peptide containing the LKKTETQ motif retains actin-binding capacity and can reproduce some of the cell-migration effects attributed to the whole molecule.[4] This gives a scientific basis for the idea that a synthetic peptide focused on the actin-binding domain could be biologically active. What is not well documented in the public literature is a consistent, verified specification of every commercial “TB-500” preparation. Because research-chemical products are not manufactured to pharmaceutical identity standards and are rarely characterized in published third-party assays, the honest position is that the exact structure of any given TB-500 vial cannot be assumed. We describe the mechanistic rationale further in our reference on how TB-500 affects cytoskeletal regulation and stem-cell migration.
The Beta-Thymosin Family: Where Tβ4 Sits
To understand why “Thymosin Beta-4” is a precise term while “TB-500” is a loose one, it helps to see the family Tβ4 belongs to. The beta-thymosins are a group of small, acidic, intrinsically disordered peptides that share the actin-sequestering function. In humans the most abundant is Thymosin Beta-4, but the family also includes Thymosin Beta-10 (Tβ10) and Thymosin Beta-15 (Tβ15), each encoded by distinct genes and each expressed in characteristic tissue and developmental patterns.[15]
These family members are structurally similar — they are roughly 40–44 residues, they are largely unstructured in free solution, and they fold into a more ordered conformation upon binding actin — but they are not identical, and they can differ in expression and in disease associations. Thymosin Beta-15, for instance, has been studied as a marker associated with certain cancers, where its expression correlates with cell motility. This family context matters for the disambiguation question because it underscores that the “thymosin beta” label denotes a defined set of gene products, whereas “TB-500” is a commercial coinage that does not map cleanly onto any single gene product or family member. When a supplier writes “TB-500,” there is no gene, no UniProt entry, and no canonical sequence that the name formally points to — only a conventional association with the actin-binding region of Tβ4.
Intrinsic disorder and why it matters
A structural feature worth appreciating is that beta-thymosins are intrinsically disordered peptides — in free solution they do not adopt a single stable fold. They acquire structure contextually, folding around their binding partner (actin) when they engage it. This “coupled folding and binding” behavior is characteristic of many regulatory peptides and has two consequences for the present discussion. First, it makes short fragments plausibly functional, because activity is tied to a local motif rather than to a globally folded domain. Second, it makes purity and identity harder to infer from simple assays, because a disordered peptide does not present the crisp structural signatures of a folded protein. Both consequences reinforce the earlier caution: fragment products can be biologically active, and their exact identity is hard to confirm without rigorous analytical chemistry.
How Does the Actin-Binding Peptide Work? Mechanisms Studied
The mechanistic research on Thymosin Beta-4 — and by extension the mechanistic hypotheses applied to TB-500 — centers on the actin cytoskeleton and a set of downstream cellular behaviors. This section summarizes the mechanisms that have actually been studied, with attention to which are demonstrated at the molecular/cellular level and which remain hypotheses about tissue-level outcomes.
G-actin sequestration and cytoskeletal buffering
As introduced above, the foundational mechanism is 1:1 binding of monomeric G-actin. Structural studies, including NMR and mutagenesis work, mapped the interaction and showed that the central actin-binding domain is essential for this activity.[5] By maintaining a reservoir of sequestered actin, the peptide contributes to the rapid, reversible remodeling of the cytoskeleton that cells require during migration and shape change. This is the single mechanism that most directly connects the tb-500 mechanism narrative to established biochemistry: if a peptide binds and buffers G-actin, it can in principle influence how readily a cell reorganizes its cytoskeleton to move.
Cell migration and wound-edge dynamics
In cell-culture and animal models, Thymosin Beta-4 has been reported to promote the migration of several cell types relevant to repair, including keratinocytes and endothelial cells, and to accelerate the closure of experimental wounds.[6] The proposed logic is that enhanced actin dynamics facilitate the lamellipodial protrusion and directed movement that cells use to crawl into a wound bed. These findings are consistently described as promising in preclinical models, but they are model findings — petri dishes and rodents — not demonstrations of clinical wound-healing efficacy in humans from systemic dosing.
Angiogenesis
Several studies report that Thymosin Beta-4 can stimulate angiogenesis — the formation of new blood vessels — by promoting endothelial cell migration, adhesion, and tube formation in vitro and by increasing vessel formation in animal assays.[7] Angiogenesis is a plausible contributor to tissue repair because new tissue needs a blood supply. This is one of the most cited mechanistic rationales for the peptide’s repair-associated reputation, and it is also a reason WADA classifies these substances alongside growth factors that modify tissue.
Ac-SDKP: an active N-terminal fragment
An important and often-overlooked piece of the mechanism story is that Thymosin Beta-4 can be enzymatically processed to release Ac-SDKP (N-acetyl-Ser-Asp-Lys-Pro), a tetrapeptide with its own documented biological activities, including anti-fibrotic and pro-angiogenic effects in experimental models.[8] The existence of this bioactive breakdown product complicates simple structure–activity comparisons: some effects attributed to “Tβ4” may be mediated by fragments, and a synthetic actin-binding fragment (as TB-500 is often described) would not necessarily generate the same downstream metabolites as the full-length protein. This is another reason to be cautious about treating thymosin beta 4 fragment products and full-length Tβ4 as interchangeable at the level of biological output.
Other reported cellular effects
- Anti-inflammatory and cell-survival signaling: Some studies report reduced inflammatory markers and anti-apoptotic effects in injured tissue models.[9]
- Stem/progenitor cell recruitment: In cardiac injury models, Tβ4 has been studied for effects on epicardial progenitor activation.[10]
- Corneal and dermal wound models: Repeated reports of accelerated epithelial healing underpin the ophthalmic clinical program discussed below.[11]
Across all of these, the pattern is the same: well-documented molecular and cellular effects, promising animal data, and a large gap before human clinical proof. For a deeper look at the repair-specific literature, see our review of what research says about TB-500 for tissue repair and healing.
Sequence and Molecular Weight: A Structural Comparison
Getting the structural facts right is the anchor of the whole tb-500 vs tb4 discussion. The following reflects what is documented for the endogenous protein, alongside the honest caveats for the market label.
| Property | Thymosin Beta-4 (endogenous protein) | Actin-binding fragment (as often described for TB-500) |
|---|---|---|
| Length | 43 amino acids | Short peptide containing the LKKTETQ motif (exact length varies by product/description) |
| Approx. molecular weight | ~4.9 kDa (~4963 Da) | Substantially smaller if a true fragment; ~full weight if actually full-length Tβ4 |
| Key functional motif | LKKTETQ actin-binding domain (residues ~17–23) | Built around the same motif |
| N-terminal feature | Acetylated; can release Ac-SDKP on processing | Fragment may not reproduce Ac-SDKP generation |
| Verified commercial identity | Defined for research-grade recombinant/synthetic Tβ4 | Not reliably verified across suppliers |
The single most important honesty point in this whole article lives in that table’s last row. The endogenous protein has a defined sequence and mass. A product labeled “TB-500” may match that protein, may be a smaller actin-binding fragment, or may vary between suppliers. The published, verifiable structural fact is about Thymosin Beta-4; the structure of any specific TB-500 vial is a claim on a label, not a fact confirmed in the peer-reviewed record. Our peptide research glossary defines the underlying terms — actin sequestration, angiogenesis, fragment, motif — for readers who want the vocabulary spelled out.
How Do Research Models Use Each One?
One of the clearest ways to separate Tβ4 from TB-500 is to look at how each name actually appears in research settings, because the contexts differ sharply.
Thymosin Beta-4 in formal clinical development: RGN-259
The most credible human-trial evidence for anything in this family comes from a specific, defined ophthalmic formulation of Thymosin Beta-4. RegeneRx Biopharmaceuticals developed a preservative-free Tβ4 eye-drop product, commonly referred to as RGN-259, and (through the joint venture ReGenTree) advanced it into human clinical trials for ocular surface conditions such as dry eye disease and neurotrophic keratopathy.[12] Additional registered trials evaluated the same Tβ4 formulation for dry eye endpoints.[13]
Two points must be stated precisely. First, this is a topical ophthalmic program — eye drops delivering Tβ4 to the ocular surface — not a systemic injectable tissue-repair drug. Second, as of the knowledge reflected here, RGN-259 has been studied in registered human trials but is not FDA-approved; investigational status is not the same as approval, and readers should verify current trial and regulatory status directly on ClinicalTrials.gov and FDA resources, because development programs change over time. The existence of these trials is why it is accurate to say “Tβ4 has been studied in humans in specific formulations” while it would be inaccurate to say “Tβ4 is a proven human wound drug.”
TB-500 in the research-chemical and sport context
By contrast, “TB-500” appears predominantly in two contexts: research-grade peptide supply (labeled for laboratory research, not human use) and anti-doping enforcement. The tissue-repair claims most often attached to TB-500 — tendon, ligament, and muscle recovery — derive from preclinical and animal literature on Thymosin Beta-4 and its actin-binding domain, not from controlled human trials of the TB-500 product itself.[9] Our reference on evidence for TB-500 in tendon and ligament repair walks through exactly what those animal models do and do not show, and the handling parameters used in laboratory research are summarized in the TB-500 5 mg vial research dosage reference. Neither resource is a recommendation for human administration; both are reference material describing how the compound is characterized in research literature.
Actin Sequestration and G-Actin Binding: The Shared Core
If there is one property that genuinely unites Tβ4 and any legitimate TB-500 fragment, it is engagement with actin. This section examines that shared core in more detail, because it is the mechanistic bridge that makes the two names biologically related even when they are not structurally identical.
Why monomeric actin buffering matters
Cells maintain a tightly regulated equilibrium between monomeric G-actin and filamentous F-actin. Rapid assembly and disassembly of actin filaments drive the protrusive edges of migrating cells, the contractile ring in cell division, and the structural remodeling that accompanies tissue repair. Thymosin Beta-4 acts as a buffer in this system: by holding a portion of the G-actin pool in a sequestered state, it helps set how much polymerization-ready actin is available at any moment.[3] When cells receive a migration signal, changes in the balance of actin-binding proteins — including profilin, which competes for the same actin monomers — can rapidly release actin for filament growth at the leading edge.
Fragment activity versus full-length activity
Structure–activity studies established that the LKKTETQ-containing region is central to actin binding, and that peptides retaining this region can retain measurable actin-related and migration-promoting activity.[4] This is the scientific justification for a fragment-based product. However, “retains measurable activity” is not the same as “is functionally equivalent to the whole protein.” The full 43-residue peptide has additional structural context, potential for Ac-SDKP release, and binding characteristics that a short fragment may only partially reproduce. So even in the domain where Tβ4 and TB-500 are most alike — actin engagement — equivalence is an approximation, not a proven identity.
How Tβ4 differs from other actin-binding proteins
Thymosin Beta-4 does not act alone. The actin cytoskeleton is regulated by a whole ensemble of proteins, and understanding where Tβ4 fits clarifies both its mechanism and its limits. The key distinction is between sequestering and severing/capping proteins:
- Profilin also binds G-actin monomers, but rather than simply sequestering them it hands them off to growing filament ends, effectively promoting polymerization at the barbed end. Profilin and Tβ4 compete for overlapping populations of actin monomers, and the balance between them helps determine how much actin is available for assembly.
- Cofilin severs and depolymerizes existing filaments, accelerating turnover of the actin network. It works on F-actin, whereas Tβ4 works on G-actin, so the two act at different points in the cycle.
- Gelsolin caps and severs filaments in a calcium-dependent manner, fragmenting the network. Again, this is a filament-side activity distinct from Tβ4’s monomer buffering.
The upshot is that Tβ4 is one node in a densely interconnected regulatory network. This matters for interpreting claims about TB-500: adding exogenous actin-sequestering peptide does not simply “turn on healing.” It nudges one variable in a homeostatic system that has many compensating players. Cellular systems are buffered against single-variable perturbations, which is one biological reason to be skeptical of the idea that supplementing one actin-binding peptide produces large, predictable tissue-level outcomes.
Neural, Cardiac, and Corneal Repair: What the Injury Models Show
Much of the excitement around Thymosin Beta-4 comes from a set of organ-specific injury models. Reviewing them individually is the fairest way to represent the evidence, because the strength and interpretation differ by organ.
Neurological injury models
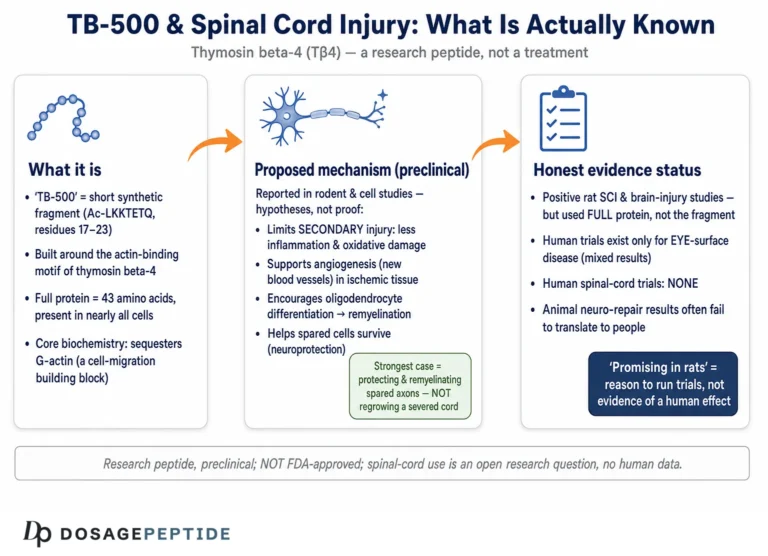
Thymosin Beta-4 has been studied in rodent models of stroke and traumatic brain injury, where investigators reported improvements in functional neurological outcomes and effects on processes such as oligodendrogenesis (the generation of myelin-forming cells) and axonal remodeling.[16] The proposed mechanisms tie back to cell migration and the support of progenitor-cell responses after injury. These are genuinely interesting preclinical findings from established neuroscience groups, and they are consistently described as hypothesis-generating. They are also, without exception, animal studies — there is no controlled human trial demonstrating that systemic Tβ4 or TB-500 improves neurological recovery in people. Reading a mouse stroke paper as evidence for human use is exactly the tier-inflation this reference warns against.
Cardiac injury models
In cardiac research, Thymosin Beta-4 attracted attention after reports that it activated integrin-linked kinase signaling, promoted survival and migration of cardiomyocytes, and could stimulate epicardial progenitor responses in models of cardiac injury.[10] Some of this work generated substantial interest in the regenerative-medicine literature. Subsequent attempts to translate progenitor-activation findings have been more complicated, and the field has debated the reproducibility and interpretation of some regeneration claims. As with the neural work, the honest summary is: mechanistically provocative, preclinically active, and clinically unproven for cardiac repair in humans.
Corneal and ocular surface models
The corneal work is distinct because it is the branch that actually reached human trials. In animal models, topical Tβ4 accelerated corneal epithelial wound closure and reduced ocular surface inflammation.[11] These consistent ocular results, combined with the accessibility and tolerability of eye-drop delivery, are what justified advancing the RGN-259 formulation into registered clinical trials for dry eye and neurotrophic keratopathy. It is not a coincidence that the one branch with human data is the one with a defined formulation, a defined route (topical), and a defined, measurable clinical endpoint (ocular surface healing). That is what disciplined translational development looks like — and it stands in sharp contrast to the systemic, undefined-product, unmeasured-endpoint world of research-market TB-500.
Pharmacokinetics and Delivery Considerations
A frequently overlooked dimension of the thymosin beta-4 vs tb-500 comparison is pharmacokinetics — what happens to the peptide after it enters a biological system. As a small, water-soluble, unstructured peptide, Thymosin Beta-4 is subject to the general vulnerabilities of peptide therapeutics: susceptibility to proteolytic degradation, potential rapid clearance, and limited oral bioavailability. These properties are part of why the successful clinical formulation is a topical eye drop, where the peptide is applied directly to the target surface rather than relying on systemic distribution.
For systemic exposure, the peptide’s susceptibility to enzymatic processing is doubly relevant because, as noted earlier, one processing product (Ac-SDKP) is itself bioactive. This means the pharmacology of full-length Tβ4 in the body may reflect a mixture of intact peptide and active fragments, evolving over time. A synthetic actin-binding fragment marketed as TB-500 would have its own, likely different, degradation profile and would not necessarily generate the same downstream metabolites. From a research-interpretation standpoint, this is another reason that data on one form cannot be assumed to transfer cleanly to the other: even if two preparations share the actin-binding motif, their behavior in a living system — distribution, half-life, metabolite generation — may diverge substantially.
Why route and formulation dominate the outcome
The single most decisive variable in whether any of these peptides “works” in a study is often not the molecule but the delivery. A peptide applied topically to a wound bed, injected locally into a lesion, or infused systemically will produce entirely different exposure at the target tissue. This is why the reading habit of identifying the route and formulation is so important. A large fraction of the confusion in popular discussion comes from collapsing topical ophthalmic Tβ4 results, local-injection animal results, and hypothetical systemic use into a single undifferentiated claim about “TB-500 healing.”
Cell Migration, Angiogenesis, and Tissue-Repair Research Roles
The reputation of both molecules rests on tissue repair. This section lays out the repair-associated research roles in an evidence-tier-honest way, so readers can see exactly how strong each claim is.
| Reported role | Strongest evidence tier | Honest interpretation |
|---|---|---|
| G-actin sequestration | Established biochemistry (in vitro + structural) | Well demonstrated at the molecular level |
| Keratinocyte / endothelial migration | Cell culture + animal models | Consistent preclinical signal; not human-outcome proof |
| Angiogenesis (vessel formation) | In vitro + animal assays | Plausible repair contributor; preclinical |
| Dermal / corneal wound closure | Animal models; ophthalmic human trials for the eye-drop formulation | Human evidence is formulation-specific (ophthalmic), not systemic |
| Tendon / ligament / muscle repair | Animal models only | No controlled human efficacy trials of TB-500 for these uses |
| Cardiac repair / progenitor activation | Animal models | Preclinical; human cardiac benefit not established |
The gradient in that table is the whole story. Move down the rows and the evidence tier weakens from established biochemistry, to cell/animal models, to a narrow slice of human ophthalmic trials, to purely animal-level musculoskeletal data. The popular framing of TB-500 as a general-purpose “healing peptide” compresses this gradient into a single confident claim that the evidence does not support.
Current Evidence Level
This section states the evidence tier for each name as plainly as possible, because it is the most important compliance-critical part of the comparison.
Thymosin Beta-4 (endogenous protein)
- Molecular/biochemical: Strong. Actin sequestration and structure are well established.
- Preclinical (cell/animal): Extensive across wound, cardiac, corneal, and neural injury models.
- Human clinical: Limited and formulation-specific. The most credible human data come from the topical ophthalmic formulation (RGN-259) studied for dry eye and neurotrophic keratopathy.[12] Systemic Tβ4 as a general tissue-repair therapy is not FDA-approved.
TB-500 (research-market label)
- Human clinical efficacy: Absent. There are no adequate, well-controlled human trials establishing that the TB-500 product produces the tissue-repair outcomes attributed to it.
- Preclinical basis: The supporting data are extrapolated from Thymosin Beta-4 / actin-binding-domain animal studies.[9]
- Regulatory: Not FDA-approved for any indication. Sold in the research-chemical channel with laboratory-use labeling.
Put simply: the strongest human evidence in this family attaches to a specific eye-drop formulation of the endogenous protein, not to the systemic “TB-500” product that most fitness-context discussion refers to. Anyone citing TB-500 human tissue-repair efficacy is, in almost all cases, citing animal data by proxy.
Is TB-500 Prohibited in Sport? The WADA Position
Both Thymosin Beta-4 and TB-500 are relevant to anti-doping. The World Anti-Doping Agency (WADA) prohibits a broad class of substances that includes growth factors and peptides affecting muscle, tendon, or vascularization, and TB-500/Thymosin Beta-4 has been treated as a prohibited substance within this framework.[14] Athletes subject to anti-doping rules should treat both names as prohibited and consult the current WADA Prohibited List directly, since the list is updated annually and category wording changes.
This regulatory reality is itself informative about the science: WADA prohibits substances that plausibly modify tissue growth, adhesion, or vascularization. The inclusion of this peptide family reflects the biological plausibility of the actin/angiogenesis mechanisms — not a determination that the substances are proven, safe, or approved therapies. Prohibition in sport and lack of FDA approval coexist without contradiction.
Detection and the analytical context
Anti-doping laboratories have developed mass-spectrometry-based methods to detect Thymosin Beta-4 and related peptides in biological samples, distinguishing exogenous or elevated levels from normal endogenous background. This analytical dimension is relevant to the disambiguation theme because it highlights something the research-chemical market usually ignores: rigorous identification of these peptides requires sophisticated instrumentation, and endogenous Tβ4 is already present in the body. Detecting “a peptide” is not the same as confirming a specific fragment versus full-length identity, and the same analytical rigor that anti-doping science applies is precisely what is absent from most claims about what a given TB-500 vial contains. The contrast underscores a consistent theme of this reference: the endogenous protein is well characterized and measurable, while the market product is neither reliably defined nor independently verified.
Safety, Characterization, and Handling in Research Settings
Because this is reference material rather than usage guidance, this section addresses what the literature and regulatory context say about safety and product characterization — not how a person should administer anything.
What is and isn’t known about safety
Formal human safety data are limited to specific studied formulations. In the ophthalmic trials of the Tβ4 eye drop, topical administration was generally reported as well tolerated for the ocular surface indications studied, but those findings apply to eye drops and cannot be extrapolated to systemic injection of a research-grade product.[13] For systemic TB-500, there is no comparable body of controlled human safety data. The absence of controlled human trials means that both efficacy and safety of systemic use are, from an evidence standpoint, unestablished.
Product identity and purity concerns
Research-chemical peptides are not manufactured to pharmaceutical identity, purity, or sterility standards, and independent published assays of “TB-500” vials are scarce. This is the practical consequence of the labeling ambiguity discussed earlier: a buyer cannot assume that a vial contains the exact molecule, at the stated mass, at high purity, or free of contaminants. In a research context, identity confirmation (e.g., mass spectrometry, HPLC purity) is the kind of characterization that would be required before any conclusion could be drawn — and it is precisely what is usually missing from the market.
This analytical gap compounds every other uncertainty in the chain. If the identity of the material is unconfirmed, then even a perfectly designed study using that material would be studying an undefined input, and its results could not be cleanly attributed to a specific molecule. This is one reason the peer-reviewed literature almost always works with characterized recombinant or synthetic Thymosin Beta-4 of known sequence and purity, rather than with commercial “TB-500” preparations. Anyone attempting to reason from the scientific literature to a research-market product must bridge that gap explicitly, rather than assuming the two are the same input.
Limitations
Honesty about limitations is central to reading this topic correctly. The following constraints apply to essentially every claim in the Tβ4/TB-500 literature.
- Species and model gap: Most tissue-repair evidence comes from rodents and cell culture. Effects in mice do not reliably predict effects in humans, and dosing/exposure in animal models does not translate directly.
- Formulation specificity: Human evidence for Tβ4 is largely limited to a topical ophthalmic product. It is not evidence for systemic injectable use, and it is not evidence about the TB-500 product specifically.
- Structural ambiguity of TB-500: The exact composition of research-market TB-500 is not consistently verified. Studies of full-length Tβ4 are not automatically evidence about a fragment product, and vice versa.
- Bioactive metabolites: The full protein can generate active fragments such as Ac-SDKP; a synthetic actin-binding fragment may not, so downstream effects could differ.
- Publication and interest bias: Much foundational work comes from a relatively small set of investigators and commercial developers; independent replication of key repair outcomes in humans is limited.
- No approved systemic indication: Neither substance is FDA-approved for systemic therapeutic use, so there is no regulatory efficacy/safety determination to rely on.
These limitations do not mean the underlying biology is uninteresting — actin sequestration is real and important. They mean the distance between “interesting mechanism” and “proven human therapy” is large and, for TB-500 specifically, largely uncrossed.
How to Read a Study That Says “Thymosin Beta-4” or “TB-500”
Because the naming is ambiguous, a few practical reading habits help avoid overinterpretation:
- Identify the exact material. Does the paper use recombinant full-length Tβ4, a synthetic fragment, or an unspecified “TB-500”? The conclusions apply only to what was actually tested.
- Identify the model. In vitro, animal, or human? A human ophthalmic trial and a mouse tendon study support very different claims.
- Identify the route and formulation. Topical eye drop, local injection, or systemic administration? Route dramatically changes exposure and relevance.
- Check the endpoint. Is the outcome a molecular readout (actin binding), a cellular readout (migration), or a clinical outcome (healed wound, vision improvement)? The higher the tier, the stronger the evidence.
- Separate mechanism from outcome. A demonstrated mechanism does not guarantee a clinical benefit; the two require separate evidence.
Applying these five checks to the popular claim “TB-500 heals injuries” quickly reveals that it usually rests on animal-model outcomes with an unspecified fragment, extrapolated to human systemic use — a chain with several weak links.
Common Misconceptions About Tβ4 and TB-500
Because this topic is discussed heavily in non-scientific settings, several recurring misconceptions distort the picture. Addressing them directly is part of accurate reference material.
“TB-500 is a proven healing peptide”
This is the most common overstatement. “Proven” implies controlled human efficacy trials with defined endpoints. Those do not exist for the TB-500 product in the tissue-repair uses it is marketed for. The word that fits the evidence is investigational or preclinical, not proven. The demonstrated facts are biochemical (actin binding) and preclinical (animal models); the outcomes claimed for human athletes are extrapolations.
“TB-500 and Thymosin Beta-4 are chemically identical, full stop”
This is a half-truth that runs in both directions. Sometimes a product labeled TB-500 is full-length Tβ4; sometimes it is described as a fragment. Asserting a clean, universal structural identity claims more certainty than the labeling of research-market products supports. The accurate statement is that they are closely related and often used synonymously, with the caveat that composition varies and is not independently verified.
“Because Tβ4 is natural and made by the body, supplementing it is inherently safe”
Endogenous presence does not establish the safety of exogenous administration at non-physiological doses by non-physiological routes. Many molecules the body makes are harmful when introduced in excess or in the wrong place. The safety of systemic supplementation has not been established in controlled human trials, and “natural” is not a pharmacological safety category.
“The eye-drop trials prove the injectable works”
They do not. RGN-259 is a topical ophthalmic formulation studied for ocular surface conditions. Positive or promising ocular results say nothing definitive about systemic injectable use for muscles, tendons, or other tissues. Route, formulation, and target tissue are all different, and evidence does not transfer across those boundaries.
Key Takeaways for Reading This Peptide Family
Pulling the threads together, the essential points a careful reader should retain about thymosin beta-4 vs tb-500 are these:
- Thymosin Beta-4 is a defined molecule; TB-500 is a label. Tβ4 is a specific 43-amino-acid, ~4.9 kDa endogenous actin-sequestering peptide with a UniProt-level identity. TB-500 is a research-market and anti-doping term without a formal canonical sequence.
- The shared core is actin binding. Both are associated with the LKKTETQ actin-binding domain, which is the mechanistic bridge that makes them biologically related.
- Structural equivalence is an approximation, not a verified fact. Product composition varies, and fragment versus full-length forms may differ in metabolite generation and pharmacokinetics.
- Human evidence is narrow and formulation-specific. The credible human data attach to a topical ophthalmic Tβ4 formulation (RGN-259), not to systemic TB-500.
- Neither is FDA-approved, and both are WADA-prohibited. Regulatory status is a hard fact regardless of mechanistic promise.
- Evidence tier is everything. Move from established biochemistry to human clinical outcome and the certainty drops sharply; most exciting repair claims live at the animal-model tier.
For readers building broader context, the mechanistic detail lives in our reference on cytoskeletal regulation and stem-cell migration, and the terminology used throughout is defined in the research glossary.
Frequently Asked Questions
Is TB-500 the same thing as Thymosin Beta-4?
Not exactly. Thymosin Beta-4 is a specific, defined 43-amino-acid endogenous protein. “TB-500” is a research-market label that is often used as a synonym for Tβ4, but is frequently described as a synthetic fragment centered on the actin-binding domain (the LKKTETQ region). Because product labeling varies, the two names are closely related and often used interchangeably, but they are not guaranteed to be structurally identical.
What is the molecular weight of Thymosin Beta-4?
The endogenous human Thymosin Beta-4 protein is 43 amino acids long with a molecular weight of approximately 4.9 kDa (about 4963 Da). A true actin-binding fragment would be substantially smaller. Note that some material sold as “TB-500” is marketed as full-length Tβ4 rather than a fragment, so the stated molecular weight on a research-market label cannot be assumed without independent identity testing.
What is the actin-binding motif in Thymosin Beta-4?
The central actin-binding domain is associated with the sequence motif LKKTETQ, located at roughly residues 17–23 of the full protein. Structure–activity studies show this region is essential for binding monomeric G-actin, which is why fragment-based TB-500 products are typically described as being built around this motif. Retaining the motif preserves some actin-related activity, though not necessarily the full behavior of the intact protein.
Is Thymosin Beta-4 or TB-500 FDA-approved?
No. Neither systemic Thymosin Beta-4 nor TB-500 is FDA-approved for any indication. The most advanced human clinical work is a specific topical ophthalmic formulation of Tβ4 (RGN-259), studied for dry eye disease and neurotrophic keratopathy. Investigational trial status is not the same as approval, and readers should verify current regulatory and trial status directly.
What does TB-500 do mechanistically?
The proposed tb-500 mechanism is based on Thymosin Beta-4 biology: binding and buffering monomeric G-actin, which influences cytoskeletal dynamics and can promote cell migration and angiogenesis in laboratory and animal models. These molecular and cellular effects are documented preclinically. The leap from these mechanisms to reliable tissue-repair outcomes in humans from systemic dosing is not established by controlled trials.
Is there human evidence that TB-500 repairs tendons or muscles?
No adequate, well-controlled human trials establish that TB-500 repairs tendons, ligaments, or muscle. The tissue-repair claims are extrapolated from animal-model studies of Thymosin Beta-4 and its actin-binding domain. In evidence-tier terms, the musculoskeletal repair narrative sits at the preclinical/animal level, which is the weakest tier for predicting human clinical outcomes.
Why do both share the name “thymosin” if they differ from thymosin alpha-1?
The “thymosin” family name is historical, derived from early thymus fractionation (thymosin fraction 5), not from shared function. Beta-thymosins like Tβ4 are actin-binding peptides, while thymosin alpha-1 is an unrelated immune-modulating peptide. The shared prefix reflects chromatographic origin, so it should not be read as implying similar biology.
Are Thymosin Beta-4 and TB-500 banned in sport?
Yes. The World Anti-Doping Agency prohibits this peptide family within its categories covering growth factors and substances affecting muscle, tendon, or vascularization. Athletes under anti-doping rules should treat both Thymosin Beta-4 and TB-500 as prohibited and consult the current WADA Prohibited List, which is updated annually and may change category wording over time.
Can I assume a research vial labeled “TB-500” contains the fragment?
No. Research-chemical products are not made to pharmaceutical identity standards, and independent published assays of TB-500 vials are scarce. A vial may contain a fragment, full-length Tβ4, a different purity, or contaminants. Without independent identity testing (such as mass spectrometry and HPLC), the exact contents of any given TB-500 product cannot be assumed from the label.
References
- Goldstein AL, Hannappel E, Kleinman HK. Thymosin β4: actin-sequestering protein moonlights to repair injured tissues. Trends in Molecular Medicine. 2005.
- Goldstein AL, Hannappel E, Sosne G, Kleinman HK. Thymosin β4: a multi-functional regenerative peptide. Basic properties and clinical applications. Expert Opinion on Biological Therapy. 2012.
- Safer D, Elzinga M, Nachmias VT. Thymosin β4 and Fx, an actin-sequestering peptide, are indistinguishable. Journal of Biological Chemistry. 1991.
- Sosne G, Qiu P, Goldstein AL, Wheater M. Biological activities of thymosin β4 defined by active sites in short peptide sequences. FASEB Journal. 2010 (structure–activity of the actin-binding domain).
- Van Troys M, et al. The actin binding site of thymosin β4 mapped by mutational analysis. EMBO Journal. 1996.
- Malinda KM, Sidhu GS, Mani H, et al. Thymosin β4 accelerates wound healing. Journal of Investigative Dermatology. 1999.
- Grant DS, Rose W, Yaen C, Goldstein A, Martinez J, Kleinman H. Thymosin β4 enhances endothelial cell differentiation and angiogenesis. Angiogenesis. 1999.
- Kumar N, Nakagawa P, Janic B, et al. The anti-inflammatory peptide Ac-SDKP is released from thymosin-β4 by renal meprin-α and prolyl oligopeptidase. American Journal of Physiology-Renal Physiology. 2016.
- Philp D, Kleinman HK. Animal studies with thymosin β4, a multifunctional tissue repair and regeneration peptide. Annals of the New York Academy of Sciences. 2010.
- Bock-Marquette I, Saxena A, White MD, et al. Thymosin β4 activates integrin-linked kinase and promotes cardiac cell migration, survival and cardiac repair. Nature. 2004.
- Sosne G, Szliter EA, Barrett R, et al. Thymosin β4 promotes corneal wound healing and decreases inflammation in vivo following alkali injury. Experimental Eye Research. 2002.
- ClinicalTrials.gov: RGN-259 (thymosin β4) ophthalmic solution for neurotrophic keratopathy (SEER-1 trial).
- ClinicalTrials.gov: RGN-259 (thymosin β4) ophthalmic solution for dry eye syndrome (ARISE-1).
- World Anti-Doping Agency. The Prohibited List (current edition).
- Huff T, Müller CS, Otto AM, et al. β-Thymosins, small acidic peptides with multiple functions. International Journal of Biochemistry & Cell Biology. 2001.
- Morris DC, Chopp M, Zhang L, Zhang ZG. Treatment of neurological injury with thymosin β4. Annals of the New York Academy of Sciences. 2012.
Research-use disclaimer: This article is educational reference material summarizing published research and regulatory context. It is not medical advice, not a therapeutic recommendation, and not instructions for human use. Neither Thymosin Beta-4 nor TB-500 is FDA-approved for systemic therapeutic use, and both are prohibited in sport by WADA. Descriptions of dosing or handling refer to laboratory research settings only. Always verify current clinical-trial and regulatory status through primary sources such as ClinicalTrials.gov, PubMed, and the FDA.