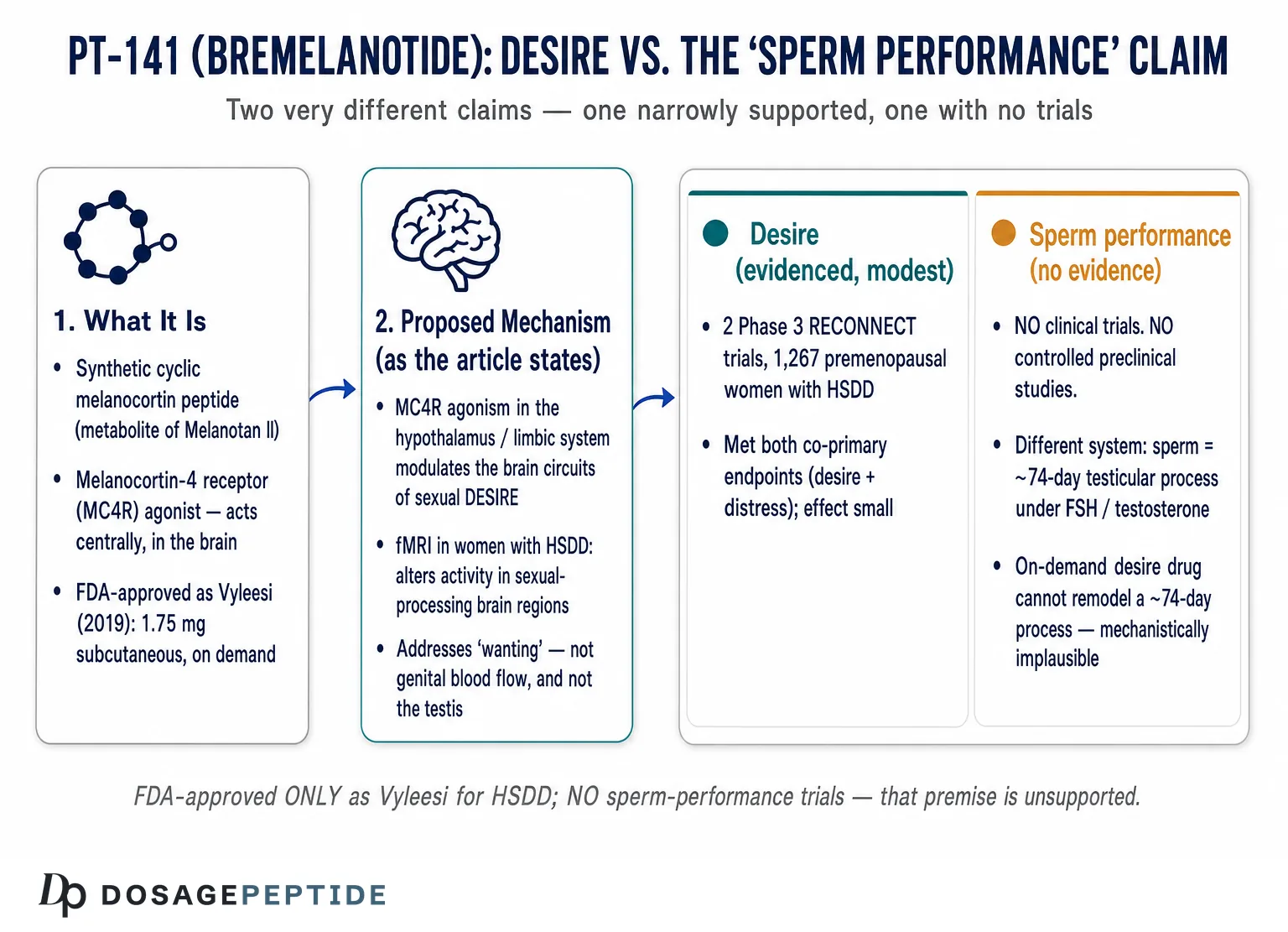
The title of this article yokes together two very different claims, and pulling them apart is the first honest thing a reader deserves. One half — that PT-141 (bremelanotide) “supports enhancing sexual desire” — rests on a genuine, if narrow, foundation: bremelanotide is an FDA-approved drug, sold as Vyleesi, for one specific condition in one specific population, and its approval was earned through two large randomized Phase 3 trials.1 The other half — that it supports “sperm performance” — has no such foundation at all. There are no clinical trials of bremelanotide for sperm count, sperm motility, sperm morphology, or any other measure of male fertility. That premise is not weakly supported or preliminarily supported; it is unsupported, and this piece will treat it as an open question to be examined rather than a finding to be endorsed.
The pairing is worth dwelling on because it is exactly the kind of blend — one real claim, one invented one — that circulates in the informal peptide literature, where a molecule’s legitimate approval is used to lend borrowed credibility to uses it was never tested for. PT-141 acts in the brain to influence the subjective experience of sexual desire. Spermatogenesis — the manufacture of sperm in the testes — is a downstream endocrine and cellular process governed by the hypothalamic-pituitary-gonadal axis, follicle-stimulating hormone, testosterone within the seminiferous tubules, and Sertoli-cell support. These are largely separate biological problems, and a drug engineered to modulate the first should not be assumed to touch the second.3
This article is written for researchers and informed readers who want an accurate map of what bremelanotide is, what it demonstrably does, and where the evidence simply runs out. We will cover the compound’s origin and structure, its melanocortin mechanism, the condition it is actually approved to treat, the pivotal trial data, its abandoned erectile-dysfunction chapter, the complete absence of sperm-performance evidence, how it compares with other agents, dosing in a research context, safety, and regulatory status. The guiding principle throughout is restraint: bremelanotide is approved for one indication, in premenopausal women, and nothing here should be read as suggesting it improves fertility, sperm quality, or any male reproductive outcome.
What PT-141 (Bremelanotide) Is and Where It Came From
Bremelanotide is a synthetic cyclic heptapeptide and a member of the melanocortin family. Its lineage is important because it explains both what the molecule does and why some of the claims attached to it are misplaced. Bremelanotide is the major active metabolite of Melanotan II, an earlier synthetic analogue of α-melanocyte-stimulating hormone (α-MSH) developed at the University of Arizona in tanning and sexual-function research.3 Where α-MSH is a linear peptide that the body rapidly degrades, the melanocortin analogues were engineered to be cyclic and more stable, and bremelanotide is the deacetylated, deamidated product that retains melanocortin-receptor activity while lacking the C-terminal amide of its parent.
The compound was advanced clinically by Palatin Technologies under the research code PT-141, and later co-developed with AMAG Pharmaceuticals for the female-sexual-desire indication.3 The scientific rationale was distinctive. Most drugs marketed for sexual problems — the phosphodiesterase type 5 (PDE5) inhibitors such as sildenafil and tadalafil — act peripherally on the vasculature to improve genital blood flow. Bremelanotide was pursued on a different premise entirely: that sexual desire and arousal have a central, brain-based component mediated by melanocortin signaling, and that an agonist reaching melanocortin receptors in the central nervous system could influence desire itself rather than merely the plumbing of erection.3
It is useful to keep three related molecules distinct, because popular writing routinely blurs them. The first is α-MSH, the endogenous melanocortin peptide with roles in pigmentation, energy balance, inflammation, and sexual behavior. The second is Melanotan II, a synthetic superagonist analogue developed primarily for its pigmentary (tanning) effects, which also produced unexpected erections in early human volunteers — the observation that launched the whole sexual-function program. The third is bremelanotide (PT-141), the metabolite refined and formulated as an approved drug. Each successive molecule narrows and redirects the biology: from a broad endogenous signal, to a tanning-focused superagonist, to a purpose-built agent for sexual desire. When someone reasons from “melanocortins do many things” to “therefore bremelanotide does all of them,” they are collapsing these distinct molecules and their distinct evidence bases back together.
Readers exploring the broader melanocortin family often encounter bremelanotide alongside its structural cousin; the site’s discussion of how Melanotan II influences erectile performance mechanistically traces the shared receptor biology from which PT-141 was derived, while the parallel question of whether Melanotan II could play a role in hypoactive sexual desire disorder shows how the same pathway was probed from the female-desire side.
The Melanocortin Mechanism — Desire in the Brain, Not Blood Flow in the Genitals
The defining feature of bremelanotide, and the thing that separates it from every erectile-dysfunction pill, is that it works centrally. Bremelanotide is a non-selective agonist at melanocortin receptors, with meaningful activity at the melanocortin-4 receptor (MC4R) and, to varying degrees, at MC1R, MC3R, and others.3 The receptor most relevant to sexual desire is MC4R, which is expressed heavily in the hypothalamus and limbic system — brain regions that integrate motivation, reward, and sexual response.
In the prevailing model, agonism at MC4R in the medial preoptic area and adjacent hypothalamic nuclei modulates the neural circuitry that generates sexual desire, with downstream effects on dopaminergic signaling in reward pathways.3 This is a fundamentally different target from the PDE5 inhibitors, which act on the nitric-oxide/cyclic-GMP pathway in penile or clitoral vascular smooth muscle to facilitate engorgement. Bremelanotide, in the language often used to describe it, addresses the “wanting” rather than the “plumbing” — the appetitive, motivational dimension of sexuality rather than the peripheral hemodynamics of the sexual response.
The strongest human mechanistic evidence for this central action comes from a randomized, double-blind, placebo-controlled crossover functional-MRI study published in the Journal of Clinical Investigation in 2022. In 31 premenopausal women with HSDD, a single 1.75 mg subcutaneous dose of bremelanotide significantly increased self-reported sexual desire for up to 24 hours compared with placebo, and altered activity in brain regions involved in sexual processing — enhancing activity in the cerebellum and supplementary motor area and deactivating the secondary somatosensory cortex in response to erotic visual stimuli, among other changes.6 This is direct neuroimaging evidence that the drug acts on brain circuits, not on the genitals, consistent with the melanocortin hypothesis it was built on.
Now consider what this mechanism does not obviously do. Spermatogenesis is governed by the hypothalamic-pituitary-gonadal axis: gonadotropin-releasing hormone drives pituitary secretion of luteinizing hormone and follicle-stimulating hormone, which in turn stimulate testicular testosterone production and Sertoli-cell support of developing germ cells. MC4R does participate in the central regulation of reproduction — recent work shows that melanocortin signaling through MC4R in kisspeptin neurons helps control fertility, particularly in females — but this is a slow, tonic, neuroendocrine role in the upstream control of the reproductive axis, not an acute switch that a single on-demand injection flips to improve the quality of sperm already being made.11 There is a large conceptual gap between “MC4R has a role in the neural control of the reproductive axis” and “bremelanotide, dosed on demand for desire, improves sperm performance.” The former is established biology; the latter is a claim no one has tested.
The honest mechanistic summary is that bremelanotide has a coherent, neuroimaging-supported story for how it influences the subjective experience of sexual desire through central MC4R agonism, and essentially no data-supported story for how it would improve sperm production or quality. The pathways are different, the timescales are different, and the target tissues are different.
It is worth being explicit about the timescale point because it is where the mechanism most decisively separates from any sperm claim. Bremelanotide is dosed on demand and acts within minutes to hours; its pharmacodynamic window — the interval during which self-reported desire rises — is measured in hours, and the fMRI study documented enhanced desire persisting up to 24 hours after a single dose before returning to baseline.6 Spermatogenesis operates on a completely different clock. The full maturation of a spermatozoon from spermatogonial stem cell to ejaculate takes on the order of two-and-a-half months, and meaningful changes in semen parameters typically require sustained interventions maintained across at least one full cycle. A drug whose effect fades within a day cannot, by any plausible pharmacology, remodel a ten-week manufacturing process. Even if one hypothesized some indirect testicular action, the dosing schedule bremelanotide was built around — brief, intermittent, no more than eight times a month — is the opposite of what a spermatogenic intervention would require.
There is also a receptor-distribution consideration. The melanocortin receptors most implicated in bremelanotide’s sexual effect (MC4R) and pigmentary effect (MC1R) are concentrated in the central nervous system and the skin, respectively, not in the seminiferous epithelium where sperm are made. The testis is under the control of gonadotropins and androgen receptors, a signaling system bremelanotide does not directly engage. This is why the compound’s well-documented effects — on desire, on flushing, on pigmentation, on blood pressure — map cleanly onto its known receptor targets, while a sperm effect would require an action on a system it has no established route into.
Understanding HSDD — The One Condition PT-141 Is Actually Approved to Treat
To judge what bremelanotide does and does not do, it helps to be precise about the single condition for which it is approved: acquired, generalized hypoactive sexual desire disorder (HSDD) in premenopausal women.9 Every word of that indication is load-bearing.
Hypoactive sexual desire disorder is characterized by a persistent or recurrent deficiency or absence of sexual desire or fantasy that causes marked personal distress or interpersonal difficulty, and that is not better explained by another medical or psychiatric condition, relationship problem, or the effects of a medication or substance. The distress criterion is essential: low desire alone is not a disorder; it becomes HSDD only when it troubles the person experiencing it.
Acquired means the low desire developed after a period of normal function, rather than being lifelong. Generalized means it occurs across situations and partners rather than being specific to one context. These qualifiers matter because the RECONNECT trials that supported approval enrolled women meeting exactly these criteria, and the label restricts the approved use to them.9 Bremelanotide is not approved for postmenopausal women, is not approved for men, and is not approved to enhance sexual performance in people without HSDD.
HSDD sits within a broader landscape of sexual concerns that are frequently conflated. Desire (the motivation to engage), arousal (the physiological and subjective response once engaged), and orgasm are distinct phases, and dysfunction in one need not accompany dysfunction in another. Bremelanotide targets the desire end of that spectrum. It is also worth distinguishing HSDD from the many reversible causes of low desire — depression, relationship distress, medication side effects (notably from SSRIs), thyroid disease, pain conditions — that should be evaluated before any drug is considered. The site’s discussion of whether PT-141 can scientifically improve fatigue and libido dysregulation in chronic illnesses illustrates how easily the boundaries between a discrete disorder and a symptom of something else can blur, and why the approved indication is deliberately narrow.
The therapeutic goal in HSDD is measured in desire and distress, using validated instruments such as the Female Sexual Function Index (FSFI) desire domain and the Female Sexual Distress Scale, along with counts of satisfying sexual events. Success is defined by improvement in wanting and reduction in distress — not by any measure of fertility, hormone levels, or reproductive output. This is the axis of outcome the drug was designed and tested to move, and it is worth holding in mind whenever a claim about sperm or fertility is attached to it.
The history of HSDD as a diagnosis also explains why the evidence bar for bremelanotide was set where it was. Female sexual desire has long been difficult to medicalize precisely because it is multifactorial — shaped by relationship context, life stress, hormonal status, mental health, and culture as much as by neurochemistry. Regulators responded to that complexity by demanding that any drug demonstrate improvement on both a desire measure and a distress measure in adequately powered, placebo-controlled trials, and by insisting the population be carefully phenotyped to exclude women whose low desire was better explained by depression, medication, or relationship factors. The RECONNECT program was built to those specifications. That rigor is a strength of the desire evidence — and, by the same token, a reminder of how far outside its validated boundaries a sperm-performance claim sits, since no comparable phenotyping, endpoint, or trial exists for any male reproductive outcome.
What the Evidence Actually Shows: The RECONNECT Phase 3 Trials
Before the pivotal program, an earlier proof-of-concept study had already hinted that bremelanotide could influence the subjective sexual response in premenopausal women with sexual arousal disorder, providing part of the rationale for pursuing a female indication.5 The pivotal evidence for bremelanotide, however, lives in the RECONNECT program — two identically designed, randomized, double-blind, placebo-controlled Phase 3 trials (registered as NCT02333071 and NCT02338960) whose primary results were published together by Kingsberg and colleagues in Obstetrics & Gynecology in 2019.1 Understanding these trials in detail is the fairest way to gauge what the drug can actually do.
Across the two studies, 1,267 premenopausal women with acquired, generalized HSDD were randomized to self-administer either bremelanotide 1.75 mg or placebo subcutaneously, on demand, using an autoinjector, over a 24-week core treatment period.1 The co-primary endpoints were the change in the FSFI desire-domain score and the change in a distress item (Item 13 of the Female Sexual Distress Scale–Desire/Arousal/Orgasm) measuring distress related to low desire. Both trials met both co-primary endpoints: bremelanotide produced statistically significant improvements in desire and statistically significant reductions in distress compared with placebo (P < 0.001 for the integrated analyses).1
The honest and important part of the story is the magnitude of those statistically significant effects. On the FSFI desire domain, the placebo-subtracted improvement was modest — on the order of about 0.3 points on that subscale.1 The number of satisfying sexual events, a more concrete behavioral measure, did not improve significantly more with drug than with placebo in the way one might hope. In other words, the trials demonstrated a real, reproducible, statistically robust effect on the subjective desire and distress endpoints, while the practical size of that effect was small and the behavioral-event endpoint was unimpressive. Both facts are true simultaneously, and responsible communication states both.
| Aspect | What the RECONNECT program showed |
|---|---|
| Design | Two identical randomized, double-blind, placebo-controlled Phase 3 trials1 |
| Population | 1,267 premenopausal women with acquired, generalized HSDD1 |
| Intervention | Bremelanotide 1.75 mg subcutaneous, on demand, over 24 weeks1 |
| Co-primary endpoints | Change in FSFI desire domain; change in desire-related distress item1 |
| Result | Both endpoints met (P < 0.001 integrated); statistically significant1 |
| Effect size | Modest (desire domain ~0.3 points placebo-subtracted); small clinical magnitude1 |
| Satisfying sexual events | No robust separation from placebo on this behavioral count1 |
| Open-label extension | Long-term data supported durability and tolerability over ~52 weeks2 |
A 52-week open-label extension and integrated long-term analysis supported the durability of the effect and provided reassurance on tolerability, though a high proportion of participants discontinued over time — a common feature of on-demand sexual-medicine trials that reflects both side effects and the modest magnitude of benefit.2 Prespecified and integrated subgroup analyses later examined consistency of effect across age, baseline severity, and other factors, broadly supporting the primary conclusions.7
The crucial point for this article is the scope of the entire evidence base: it concerns sexual desire and distress in premenopausal women. Not one endpoint in the RECONNECT program measured anything to do with male reproduction, sperm, or fertility. The trials tell us bremelanotide can produce a small but statistically real improvement in how much desire premenopausal women with HSDD report, and how distressed they are by its absence. They tell us nothing whatsoever about sperm performance.
The Erectile-Dysfunction Chapter and Why It Was Abandoned
Because the title gestures toward male sexual outcomes, it is worth tracing the one male indication bremelanotide was seriously investigated for — erectile dysfunction — and why that program did not reach approval. This history is instructive precisely because it is the closest the compound ever came to a male-performance claim, and even that fell short.
The earliest human sexual-function work with PT-141 used an intranasal formulation. In a double-blind, placebo-controlled study published in the International Journal of Impotence Research in 2004, Diamond and colleagues evaluated intranasal PT-141 in healthy men and in men with mild-to-moderate erectile dysfunction, using RigiScan monitoring of penile rigidity.4 The drug produced statistically significant erectile responses compared with placebo at higher doses, with onset of erection within roughly 30 minutes — a genuine pharmacodynamic effect distinct from the vascular mechanism of PDE5 inhibitors. Flushing and nausea were the most common adverse events.
Development then shifted away from the intranasal route and away from erectile dysfunction as the lead indication. The reasons were pharmacological and safety-driven: intranasal absorption was variable, producing inconsistent blood levels, and the melanocortin agonism carried a signal of transient increases in blood pressure that was harder to manage with an unpredictable absorption profile.4 The program was reformulated to subcutaneous, on-demand dosing, and — importantly — the sponsor ultimately pursued the female HSDD indication to approval rather than a male erectile-dysfunction indication. Bremelanotide is therefore not FDA-approved for erectile dysfunction; the male ED work remains an early-phase chapter that established central-mechanism proof of concept but did not become an approved product.
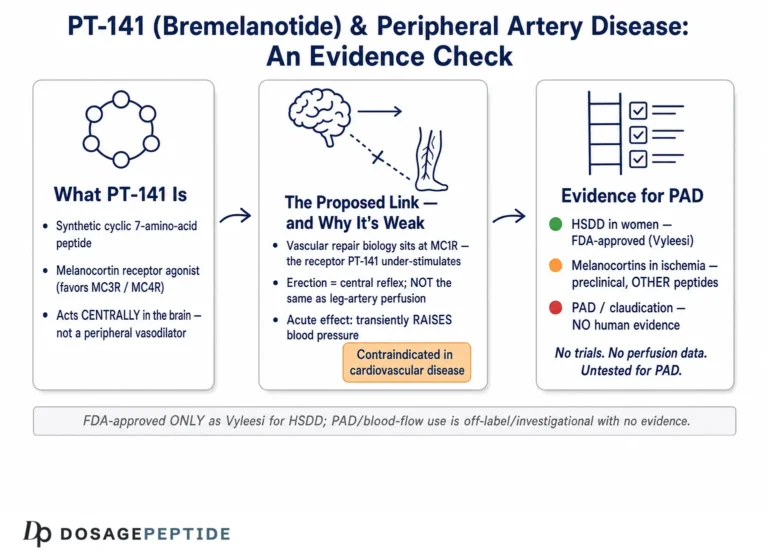
This matters for the sperm-performance question in a specific way. Even the male sexual outcome bremelanotide was directly tested for — erection, a matter of central arousal and, indirectly, penile hemodynamics — did not carry the compound to a male approval. Erection and spermatogenesis are entirely separate physiological processes: a man can have normal erectile function and severely impaired sperm production, or vice versa. The erectile-dysfunction data, such as they are, concern the mechanics of arousal and provide no bridge whatsoever to sperm count, motility, or morphology. Readers interested in the vascular dimension of the compound’s effects can review the separate question of whether PT-141 can enhance blood flow in peripheral artery disease, which is itself an exploratory, non-approved research direction rather than an established use.
The “Sperm Performance” Premise: Examining a Claim With No Trials
This section is the heart of the honesty directive, and the honest answer is unambiguous: there are no clinical trials — and no controlled preclinical studies — demonstrating that bremelanotide improves sperm count, motility, morphology, DNA integrity, or any other measure of sperm performance. A search of the primary literature returns no human fertility trials, no semen-analysis endpoints, and no animal spermatogenesis models using bremelanotide as an intervention to enhance sperm. The premise embedded in the title is, at the level of evidence, empty.
It is worth explaining why the premise is not merely unproven but mechanistically implausible as usually stated. Sperm performance is a product of the testis: FSH acting on Sertoli cells, intratesticular testosterone maintaining the spermatogenic environment, and a roughly 74-day cycle of germ-cell maturation. Improving sperm quality generally requires sustained changes to that hormonal milieu over months, or the correction of a specific pathology (varicocele, oxidative stress, hormonal deficiency, genetic factors). Bremelanotide is a short-acting, on-demand melanocortin agonist that produces transient central effects lasting hours; it is not dosed, and was never designed, to remodel testicular function over a spermatogenic cycle.3
There is a further, subtler point about melanocortin biology and the testis that must be handled carefully so it is not misread as support. MC4R does play a role in the central neuroendocrine control of reproduction — work in animal models shows that POMC/melanocortin signaling through MC4R in kisspeptin neurons contributes to fertility regulation, predominantly on the female side, and Mc4r-knockout mice display reproductive abnormalities.11 Intriguingly, the Mc4r gene has even been implicated in experimentally induced testicular teratoma development in certain mouse strains, a finding about tumor susceptibility rather than sperm enhancement.12 None of this constitutes evidence that a melanocortin agonist improves sperm performance. If anything, it illustrates that MC4R’s reproductive roles are complex, largely upstream and central, sometimes female-predominant, and in some contexts pathological — a far cry from a clean, beneficial effect on sperm that a fertility claim would require.
The correct scientific posture here is the one the exemplar of good peptide writing models: where a compound has not been studied for an outcome, the answer is not “weak evidence” or “emerging evidence” but no evidence, combined with attention to whether the mechanism even makes the hypothesis plausible. For bremelanotide and sperm performance, the evidence level is zero and the mechanistic case is weak. Anyone encountering a confident claim that PT-141 “boosts sperm” or “enhances male fertility” is reading marketing or extrapolation, not data. The compound’s genuine, approved effect is on the subjective desire of premenopausal women with HSDD; the leap from there to male sperm output crosses species of physiology with nothing on the far side.
It helps to name the specific reasoning error that produces the sperm claim, because it recurs across the informal literature. The error is a chain of loose associations: bremelanotide affects “sexual function,” sexual function is related to “reproduction,” reproduction involves “sperm,” therefore bremelanotide must affect sperm. Every link in that chain is a category slide. “Sexual function” in the bremelanotide evidence base means the subjective desire of women; “reproduction” is a separate biological domain; and “sperm” is a specific cellular output of the male testis measured by count, motility, and morphology. Sliding from one to the next feels intuitive because everyday language lumps all of sexuality together, but the biology does not. A man can have robust sexual desire and azoospermia (no sperm at all); a man can have normal semen parameters and profound loss of desire. The two are dissociable, which is exactly why a desire drug cannot be assumed to touch sperm.
A useful discipline, whenever a sexual-health compound is credited with a fertility benefit, is to ask which measurable endpoint is being claimed and which study measured it. For bremelanotide the honest audit is short: the endpoints measured were desire, distress, and satisfying sexual events (in women), plus erectile response (in the early male ED work) — and none of these is a sperm parameter. No study of bremelanotide has ever reported a sperm count, a motility percentage, a morphology assessment, or a fertilization or pregnancy outcome. When the list of measured endpoints contains nothing about sperm, a sperm claim has no data to stand on.
How PT-141 Compares With Other Sexual-Health Agents
Placing bremelanotide beside the agents it is often mentioned alongside clarifies both what it is and what it is not. The instructive contrast is mechanism and approved scope, not a head-to-head efficacy race.
| Agent / class | Primary mechanism | Approved use / evidence scope |
|---|---|---|
| Bremelanotide (PT-141) | Central melanocortin (MC4R) agonist; acts on brain desire circuits3 | FDA-approved (Vyleesi, 2019) for acquired, generalized HSDD in premenopausal women only19 |
| Flibanserin (Addyi) | Serotonin 5-HT1A agonist / 5-HT2A antagonist; daily oral, central | FDA-approved for HSDD in premenopausal women; daily dosing, alcohol cautions |
| Sildenafil / tadalafil (PDE5 inhibitors) | Peripheral vasodilation via NO/cGMP; genital blood flow | Approved for erectile dysfunction in men; do not primarily address desire |
| Testosterone (in men) | Androgen replacement; supports libido and spermatogenesis milieu | Approved for hypogonadism; exogenous testosterone can suppress sperm production |
| Melanotan II | Non-selective melanocortin agonist (parent of bremelanotide) | Not approved for any use; sold illicitly; safety concerns |
| Bremelanotide for sperm performance | Central desire agonist; not a spermatogenic agent | No trials of any kind; no approved or evidenced fertility use |
Two lessons emerge. First, the agents that genuinely act on male fertility do so through the hormonal axis and over sustained periods — and one of them, exogenous testosterone, famously impairs sperm production by suppressing gonadotropins, a reminder that “improving sexual function” and “improving sperm” can even move in opposite directions. Second, within the desire-focused category, bremelanotide occupies a specific niche: an on-demand, central, non-hormonal option for a narrowly defined female population, distinct from daily flibanserin and from the peripheral PDE5 inhibitors. None of these comparators is a sperm-performance drug, and bremelanotide is the furthest of all from that role.
The comparison also underscores why the melanocortin approach was considered novel enough to pursue. By targeting desire centrally rather than arousal peripherally, bremelanotide addressed a gap the PDE5 inhibitors never filled — the problem of wanting, not just the problem of physical response. That genuine novelty is part of what makes the misattributed sperm claim so out of place: the compound’s real distinction lies entirely on the desire axis.
Dosing in a Research and Clinical Context
Because bremelanotide is an approved drug with a defined label, its dosing is better characterized than that of most research peptides — and stating it accurately is itself a corrective against off-label extrapolation. The following reflects the approved regimen and general research-handling considerations; it is descriptive, not a recommendation for any unapproved use, and certainly not for any male or fertility application, for which no dosing has ever been established.
| Parameter | Approved / characterized value (Vyleesi label) |
|---|---|
| Approved dose | 1.75 mg subcutaneous, single autoinjector9 |
| Route | Subcutaneous (abdomen or thigh); on demand9 |
| Timing | At least 45 minutes before anticipated sexual activity9 |
| Maximum frequency | No more than one dose per 24 hours; no more than 8 doses per month9 |
| Discontinuation rule | Stop after 8 weeks if no improvement9 |
| Population | Premenopausal women with acquired, generalized HSDD only9 |
Several features of this regimen are worth reading closely. The dose is fixed, not titrated. It is explicitly on-demand rather than daily, reflecting the drug’s acute, hours-long window of effect — which is precisely why it is ill-suited to any goal, like spermatogenesis, that would require sustained hormonal change over months. The monthly cap (no more than eight doses) exists partly because of the cumulative blood-pressure and pigmentation considerations discussed below. And the eight-week stopping rule institutionalizes honesty about the modest effect size: if a woman has not benefited within roughly eight weeks, the label directs discontinuation rather than dose escalation.9
In a research context, bremelanotide obtained as a lyophilized powder is reconstituted with sterile or bacteriostatic water using standard gentle technique — directing the diluent against the vial wall, swirling rather than shaking, and storing the reconstituted solution refrigerated and protected from light. General reconstitution arithmetic and syringe-math principles that apply across research peptides are covered in the site’s peptide reconstitution guide. It bears emphasizing that meticulous handling of a research vial changes nothing about the evidence question: a perfectly prepared solution of bremelanotide is still a compound with zero sperm-performance data and an approval limited to one female indication.
Safety, Tolerability, and the Blood-Pressure Question
Bremelanotide’s safety profile is reasonably well characterized for its approved use, and it is dominated by a few predictable, mechanism-linked effects. The most common adverse events in the RECONNECT trials were nausea, flushing, and headache, each occurring in a substantial minority of treated women; nausea in particular was frequent, sometimes severe, and a common reason for discontinuation.1 Injection-site reactions also occurred. These effects follow directly from broad melanocortin agonism, which influences nausea pathways, cutaneous vasodilation (flushing), and pigmentation.
Two safety issues deserve specific attention. The first is blood pressure. Melanocortin agonism produces transient increases in blood pressure and reductions in heart rate. A dedicated ambulatory blood-pressure-monitoring study by White and colleagues quantified this: at the 1.75 mg dose, the mean maximum increase in systolic blood pressure was about 3 mmHg relative to placebo in the hours after dosing, with the peak elevations typically lasting less than 15 minutes and resolving within 12 hours.8 These transient elevations are modest in healthy normotensive individuals but are the reason the label contraindicates use in people with uncontrolled hypertension or known cardiovascular disease, and the reason dosing is capped and separated by at least 24 hours.9
The second is hyperpigmentation. Because bremelanotide engages MC1R on melanocytes, focal hyperpigmentation of the skin, face, and gums can occur, more commonly with repeated dosing and in individuals with darker skin. This is a direct extension of the same melanocortin biology that made Melanotan II a tanning agent.9 Additionally, post-marketing pharmacovigilance summarized in the NIH LiverTox resource notes that bremelanotide can cause mild, usually transient serum aminotransferase elevations and has been associated with rare instances of clinically apparent liver injury, though a firm causal relationship remains uncertain.10
Several caveats bound this safety picture. The data derive overwhelmingly from premenopausal women dosed on demand for HSDD; they do not license conclusions about safety in men, in older or medically complex patients, or under the frequent or continuous dosing that a hypothetical fertility application would imply. Product obtained outside regulated channels as a “research chemical” carries additional, sourcing-related risks — variable purity, endotoxin, mislabeling — that are independent of the molecule’s intrinsic pharmacology. And a tolerable short-term profile in the studied population is not evidence of benefit for any unstudied use: absence of major harm and absence of demonstrated efficacy for sperm performance coexist here, exactly as they should when a use has never been tested.
Regulatory Status
The regulatory picture is where precision most clearly separates fact from marketing. On June 21, 2019, the U.S. Food and Drug Administration approved bremelanotide injection under the brand name Vyleesi for the treatment of acquired, generalized hypoactive sexual desire disorder in premenopausal women.9 That approval — the second ever for female HSDD, after flibanserin in 2015, and the first on-demand option — is the entirety of bremelanotide’s approved therapeutic footprint.
No male indication, and no fertility indication, anywhere. Bremelanotide is not approved for erectile dysfunction, for male sexual dysfunction of any kind, for infertility, or for improving sperm parameters, by the FDA or any comparable regulator. Its erectile-dysfunction development was an early chapter that did not proceed to approval, and no sperm-performance program has ever existed.4 There is, correspondingly, no approved indication that could be stretched to cover male fertility.
Label restrictions reflect the evidence. The Vyleesi prescribing information limits use to premenopausal women, contraindicates it in people with uncontrolled hypertension or established cardiovascular disease, cautions about nausea and hyperpigmentation, and advises discontinuation after eight weeks without benefit.9 These boundaries are not incidental; they are the regulatory expression of exactly what the trials did and did not show.
A recurring source of public confusion deserves explicit correction. The fact that bremelanotide is “FDA-approved” is frequently deployed as though it validated every use the molecule is marketed for. It does not. FDA approval is indication-specific: it certifies that, for one defined condition in one defined population, the benefits were shown to outweigh the risks in adequate and well-controlled trials. It says nothing about safety or efficacy for any other use. An approval for female HSDD provides no support — none — for a male sperm-performance claim, which occupies an entirely separate regulatory and evidentiary universe. Conflating “approved for HSDD in women” with “works for sperm in men” is among the most common errors in the informal literature around this compound.
Limitations and the Evidence Gap
Pulling the threads together, the limitations that bear on the title’s twin claims are asymmetric, and naming them plainly is the point.
On the desire claim. Bremelanotide’s effect on sexual desire in premenopausal women with HSDD is real, reproducible, and statistically robust — but modest in magnitude, accompanied by frequent nausea, limited to a narrow population, and unimpressive on the more concrete measure of satisfying sexual events.1 The honest framing is “a genuine but small effect on subjective desire and distress in one female population,” not “a powerful libido enhancer.”
On the sperm claim. Here the limitation is total. There is no human trial, no controlled animal study, and no mechanistic rationale of any strength connecting bremelanotide to improved sperm performance. The claim is not under-evidenced; it is un-evidenced, and it runs against the compound’s pharmacology — an acute, central, on-demand desire agonist rather than a sustained modulator of testicular function.3
Mechanistic mismatch. Desire and spermatogenesis are governed by different systems on different timescales. MC4R’s documented reproductive roles are largely central, upstream, and in some models female-predominant or even pathological — not a demonstrated route to better sperm.1112
Population and sourcing. Efficacy and safety data come from premenopausal women; extrapolation to men, to fertility patients, or to frequent dosing is unsupported. And because non-prescription material varies in purity and provenance, even informal observations about it are unreliable.
The responsible synthesis is that bremelanotide is a legitimate, approved, if modestly effective, drug for a specific female sexual-desire disorder — and that everything in the title beyond that, particularly the sperm-performance premise, is unsupported by evidence. Readers who want to ground the terminology used here can consult the site’s peptide glossary, and can situate bremelanotide among related compounds via the central dosages index, which catalogs peptides for educational reference rather than as guidance for human use.
Frequently Asked Questions
Is PT-141 (bremelanotide) FDA-approved, and for what?
Yes, but narrowly. Bremelanotide is FDA-approved as Vyleesi, since June 2019, for acquired, generalized hypoactive sexual desire disorder (HSDD) in premenopausal women.9 It is not approved for postmenopausal women, for men, for erectile dysfunction, or for enhancing sexual performance in people without HSDD. The approval is indication-specific and does not extend to any male or fertility use.
Does bremelanotide improve sperm performance or male fertility?
There is no evidence that it does. No clinical trials, and no controlled preclinical studies, have tested bremelanotide for sperm count, motility, morphology, or any fertility outcome. Its mechanism — acute, central melanocortin agonism affecting the subjective experience of desire — is not directed at the testicular processes that govern sperm production, which unfold over roughly 74 days under hormonal control.3 The sperm-performance premise is unsupported and mechanistically implausible as usually stated.
How does PT-141 work, and how is that different from Viagra?
PT-141 is a melanocortin-4 receptor agonist that acts centrally, in the hypothalamus and limbic system, on the brain circuits that generate sexual desire; functional-MRI work in women with HSDD shows it alters activity and connectivity in sexual-processing regions.6 PDE5 inhibitors such as sildenafil (Viagra) act peripherally on genital blood vessels to facilitate the physical response. PT-141 addresses “wanting”; PDE5 inhibitors address blood flow. They are fundamentally different mechanisms.
How large is the effect on sexual desire in women?
Statistically significant but clinically modest. In the two Phase 3 RECONNECT trials (1,267 premenopausal women), bremelanotide 1.75 mg improved the FSFI desire-domain score by roughly 0.3 points more than placebo and reduced desire-related distress, meeting both co-primary endpoints (P < 0.001 integrated), while the count of satisfying sexual events did not separate robustly from placebo.1 The effect is real and reproducible but small.
Was PT-141 ever studied for erectile dysfunction in men?
Yes, in early development. An intranasal formulation produced statistically significant erectile responses versus placebo in men with mild-to-moderate ED, with onset around 30 minutes.4 But development shifted away from the intranasal route because of variable absorption and blood-pressure concerns, and the compound was ultimately approved for female HSDD, not male ED. Erection and sperm production are separate processes, so even this ED work says nothing about sperm performance.
What are the main side effects and safety concerns?
The most common are nausea (sometimes severe and a frequent reason for stopping), flushing, and headache.1 Bremelanotide causes transient increases in blood pressure and reductions in heart rate — on the order of a 3 mmHg systolic rise at the approved dose, usually lasting under 15 minutes — so it is contraindicated in uncontrolled hypertension and cardiovascular disease.89 Focal hyperpigmentation can occur with repeated use, and rare liver-enzyme elevations have been reported.10
Why do some sources claim a melanocortin drug should help male fertility?
That reasoning over-extends real biology. MC4R does participate in the central neuroendocrine control of reproduction, and melanocortin signaling in kisspeptin neurons influences fertility — but predominantly in females and as a slow, upstream regulatory role, not as an acute enhancer of sperm quality.11 Some melanocortin effects on the testis are even pathological in animal models.12 None of this supports a claim that on-demand bremelanotide improves sperm performance.
Is PT-141 sold as a research chemical the same as prescription Vyleesi?
Not necessarily. Prescription Vyleesi is a regulated product with defined purity and a fixed 1.75 mg autoinjector dose. Material sold informally as “PT-141” research chemical varies in purity and provenance and is not quality-assured, introducing risks of impurities, endotoxin, and mislabeling that are independent of the molecule’s pharmacology. Handling quality does not create efficacy for any unapproved use.
Could bremelanotide ever be developed for a fertility indication?
It cannot be ruled out in principle, but it would require an entirely new research program — controlled animal spermatogenesis models with semen endpoints, followed by human fertility trials — starting from no data and against a mechanism pointed at acute central desire rather than sustained testicular function. Given that even the compound’s directly tested male outcome (erection) did not reach approval, a repurposing toward sperm performance is, realistically, speculative and untested.
References
- Kingsberg SA, Clayton AH, Portman D, et al. Bremelanotide for the Treatment of Hypoactive Sexual Desire Disorder: Two Randomized Phase 3 Trials. Obstet Gynecol. 2019;134(5):899-908. PMID: 31599840. https://pubmed.ncbi.nlm.nih.gov/31599840/
- Simon JA, Kingsberg SA, Portman D, et al. Long-Term Safety and Efficacy of Bremelanotide for Hypoactive Sexual Desire Disorder. Obstet Gynecol. 2019;134(5):909-917. PMCID: PMC6819023. https://pmc.ncbi.nlm.nih.gov/articles/PMC6819023/
- Molinoff PB, Shadiack AM, Earle D, Diamond LE, Quon CY. PT-141: a melanocortin agonist for the treatment of sexual dysfunction. Ann N Y Acad Sci. 2003;994:96-102. PMID: 12851303. https://pubmed.ncbi.nlm.nih.gov/12851303/
- Diamond LE, Earle DC, Rosen RC, Willett MS, Molinoff PB. Double-blind, placebo-controlled evaluation of the safety, pharmacokinetic properties and pharmacodynamic effects of intranasal PT-141, a melanocortin receptor agonist, in healthy males and patients with mild-to-moderate erectile dysfunction. Int J Impot Res. 2004;16(1):51-59. PMID: 14963471. https://pubmed.ncbi.nlm.nih.gov/14963471/
- Diamond LE, Earle DC, Heiman JR, Rosen RC, Perelman MA, Harning R. An effect on the subjective sexual response in premenopausal women with sexual arousal disorder by bremelanotide (PT-141), a melanocortin receptor agonist. J Sex Med. 2006;3(4):628-638. PMID: 16839319. https://pubmed.ncbi.nlm.nih.gov/16839319/
- Thurston L, Hunjan T, Mills EG, et al. Melanocortin 4 receptor agonism enhances sexual brain processing in women with hypoactive sexual desire disorder. J Clin Invest. 2022;132(19):e152341. PMID: 36189794. https://pubmed.ncbi.nlm.nih.gov/36189794/
- Simon JA, Kingsberg SA, Portman D, Jordan R, Lucas J, Sadiq A, Krop J, Clayton AH. Prespecified and Integrated Subgroup Analyses from the RECONNECT Phase 3 Studies of Bremelanotide. J Womens Health (Larchmt). 2022;31(3):391-400. PMID: 35230162. https://pubmed.ncbi.nlm.nih.gov/35230162/
- White WB, Myers MG, Jordan R, Lucas J. Usefulness of ambulatory blood pressure monitoring to assess the melanocortin receptor agonist bremelanotide. J Hypertens. 2017;35(4):761-768. PMID: 27977473. https://pubmed.ncbi.nlm.nih.gov/27977473/
- VYLEESI (bremelanotide injection), for subcutaneous use. Full Prescribing Information. AMAG/Palatin; U.S. FDA, initial approval 2019. https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/210557s000lbl.pdf
- Bremelanotide. In: LiverTox: Clinical and Research Information on Drug-Induced Liver Injury. Bethesda (MD): National Institute of Diabetes and Digestive and Kidney Diseases. NBK573221. https://www.ncbi.nlm.nih.gov/books/NBK573221/
- Talbi R, Stincic TL, Ferrari K, et al. POMC neurons control fertility through differential signaling of MC4R in kisspeptin neurons. eLife. 2025. PMCID: PMC12270483. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12270483/
- Seki S, Ohura K, Miyazaki T, Naser AA, Takabayashi S, Tsutsumi E, Tokumoto T. The Mc4r gene is responsible for the development of experimentally induced testicular teratomas. Sci Rep. 2023;13(1):6756. PMID: 37127675. PMCID: PMC10151343. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10151343/
Educational and research-use disclaimer: This article is provided solely for scientific and educational purposes. PT-141 (bremelanotide) is FDA-approved (as Vyleesi) only for the treatment of acquired, generalized hypoactive sexual desire disorder in premenopausal women; it is not approved for use in men, for erectile dysfunction, or for any fertility or sperm-performance indication, and no clinical evidence supports its use to enhance sperm count, motility, or quality. Nothing here is medical advice or a recommendation for human use. Any legitimate investigation of this compound outside its approved indication should occur within properly authorized clinical research under appropriate oversight. Readers should consult qualified healthcare professionals and applicable regulations before making any decisions.