Orforglipron has moved, in the space of roughly three years, from an obscure clinical-stage molecule to one of the most closely watched compounds in metabolic medicine. It is an oral, non-peptide, small-molecule agonist of the glucagon-like peptide-1 (GLP-1) receptor, and in April 2026 the United States Food and Drug Administration (FDA) approved it under the brand name Foundayo for chronic weight management in adults with obesity, or overweight with at least one weight-related comorbidity.18 That approval reframed a question researchers had been asking since the first phase 1 data appeared: not simply whether an orally available small molecule could meaningfully activate the GLP-1 pathway, but how effective it is for obesity when judged against the standard of randomized, placebo-controlled evidence.
This article works through that question deliberately. It is written for readers who want to understand the controlled-study evidence base rather than marketing summaries, and it keeps the level of evidence in view at every step. The short answer is that orforglipron produces clinically meaningful, dose-dependent weight reduction in large phase 3 trials, with a magnitude that sits below the most potent injectable agents but well above placebo and broadly in the range of established GLP-1 therapy.25 The longer answer, which occupies most of what follows, is that “effective” is a multidimensional judgment involving effect size, durability, comparators, tolerability, methodology, and how much long-term outcome data still remains to be collected.
Throughout, the framing is educational and research-oriented. Orforglipron is a prescription medication that should only ever be used under qualified medical supervision; nothing here is medical advice, an endorsement, or a protocol for self-experimentation. Where the evidence is strong, this article says so. Where it is thin, emerging, or industry-sponsored, it says that too. For a plain-language primer before diving into the trial data, the companion overview What Is Orforglipron? The Oral GLP-1 Pill Explained is a useful starting point.
What Orforglipron Is and Where It Came From
Orforglipron is a synthetic small molecule, not a peptide. That single structural fact is the origin of nearly everything distinctive about it. Peptide GLP-1 agonists such as semaglutide, liraglutide, and the GLP-1 component of tirzepatide are chains of amino acids that mimic the body’s native incretin hormone. They are large, fragile in the acidic environment of the stomach, and poorly absorbed when swallowed, which is why almost all of them are injected. Orforglipron, by contrast, has a molecular weight of roughly 883 daltons and a conventional drug-like organic structure, which allows it to survive digestion and be absorbed through the gut without the specialized absorption enhancers that oral peptide formulations require.10
The compound was originally discovered by Chugai Pharmaceutical, where it carried the internal designation OWL833. In 2018 Chugai licensed the molecule to Eli Lilly, which advanced it through clinical development under the code LY3502970 and, eventually, the international nonproprietary name orforglipron.10 This lineage matters for interpreting the evidence base: essentially all of the pivotal human data on orforglipron has been generated or sponsored by a single manufacturer, a point returned to in the sections on methodology and limitations.
The strategic appeal of a non-peptide oral GLP-1 agonist is straightforward. Injectable incretin therapies have transformed obesity medicine, but they carry manufacturing constraints, cold-chain logistics, needle-associated hesitancy, and cost pressures. A small molecule can, in principle, be manufactured by standard chemical synthesis at large scale and formulated as an ordinary tablet. Lilly has explicitly positioned orforglipron as a potential “foundational” oral therapy that could broaden access relative to injectables.1 Whether that access advantage translates into better real-world outcomes is an economic and adherence question that controlled efficacy trials were not designed to answer.
It is worth being precise about what orforglipron is not. It is not a so-called “bioregulator” or gray-market research peptide of the kind that populate underground catalogs with little or no rigorous human data. On the contrary, orforglipron is among the most heavily studied metabolic compounds of its generation, supported by multiple large randomized trials published in high-impact journals and by a formal regulatory dossier. The relevant honesty here runs in the opposite direction from most emerging peptides: the challenge is not a shortage of data but the need to keep effect sizes in proportion and to distinguish approved, well-characterized use from the exaggerated claims that inevitably accompany any successful weight-loss agent.
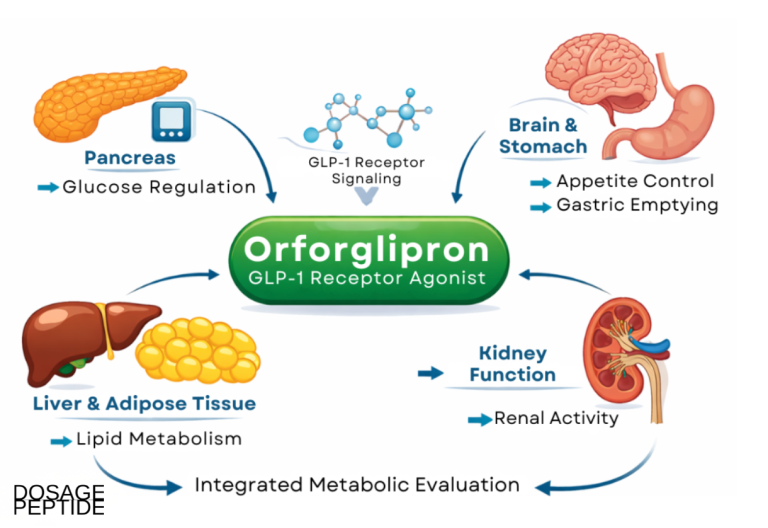
Structurally and pharmacologically, orforglipron belongs to the broader GLP-1 receptor agonist class, so much of the physiology it engages is shared with the injectable peptides. It slows gastric emptying, enhances glucose-dependent insulin secretion, suppresses inappropriate glucagon release, and acts on central appetite circuits to reduce energy intake. Readers who want the underlying receptor biology in more depth may find the general reference What Is a GLP-1? A Complete Guide helpful, and the specifics of how a small molecule differs mechanistically from the peptides are covered in the next section and in How Does Orforglipron Differ From Peptide GLP-1 Agonists?.
Molecular Mechanism: A Non-Peptide, Allosteric GLP-1 Receptor Agonist
The GLP-1 receptor is a class B G-protein-coupled receptor (GPCR). Its native ligand, the GLP-1 peptide, binds primarily at an orthosteric site: the large extracellular domain captures the peptide’s tail, and the amino terminus inserts into the transmembrane core to trigger the conformational change that activates downstream signaling. Because this binding mode depends on an extended peptide making many contacts across a large surface, it has historically been considered difficult for a compact small molecule to reproduce.10
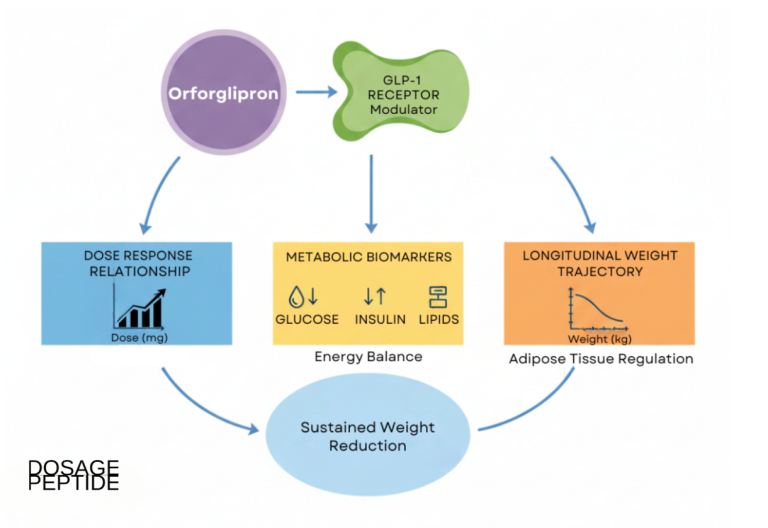
Orforglipron resolves that problem by engaging the receptor differently. Rather than reaching across the full orthosteric interface, it occupies a pocket within the transmembrane helical bundle and stabilizes the active-state conformation of the receptor from within. Structural work using cryogenic electron microscopy (cryo-EM) on GLP-1 receptor complexes has shown how small molecules can sit in a druggable transmembrane sub-pocket distinct from the peptide-binding surface, and orforglipron is understood to bind within this upper helical region and promote coupling to the stimulatory Gs protein.10 The functional consequence is the same second messenger cascade the peptide would trigger: activated Gs raises intracellular cyclic AMP (cAMP), which drives the insulinotropic, appetite-suppressing, and gastric-emptying effects characteristic of the class.
This mechanism is sometimes described as allosteric, meaning the compound acts at a site separate from where the endogenous peptide binds. From a pharmacology standpoint, one interesting feature reported for orforglipron is biased or differential engagement of downstream pathways relative to peptide agonists, with the practical relevance of any such bias still an area of active investigation rather than settled fact. The core point for an efficacy discussion is that a non-peptide can achieve near-peptide-level receptor activation, which is the biological prerequisite for meaningful clinical effect.
The pharmacokinetic profile is where the small-molecule identity becomes clinically decisive. Orforglipron is absorbed as a conventional oral drug and has a plasma half-life on the order of 30 to 40 hours, long enough to support convenient once-daily dosing.4 Critically, and unlike oral semaglutide, its absorption does not depend on the absorption enhancer sodium N-(8-[2-hydroxybenzoyl]amino) caprylate (SNAC), and it does not require the strict fasting-and-water-only administration window that peptide oral formulations impose.110 In the approved product this translates into a pill that can be taken at any time of day, with or without food. That is a genuine differentiator, though it is a convenience and adherence attribute rather than a measure of intrinsic efficacy.
A species-specificity detail is relevant to safety interpretation. Orforglipron is reported to be pharmacologically inactive at the rodent GLP-1 receptor, which complicates the use of standard mouse and rat models for on-target efficacy and, notably, means the compound did not produce the thyroid C-cell findings seen with peptide agonists in rodent carcinogenicity studies.10 That does not remove the class-wide regulatory caution around thyroid tumors, as discussed later, but it is a meaningful mechanistic footnote. The overall takeaway from mechanism is coherent: orforglipron is a bona fide GLP-1 receptor agonist that reaches the same intracellular endpoint as the peptides through a different molecular door, and its drug-like pharmacokinetics are what make oral, unrestricted dosing possible.
The Controlled Evidence Base: What the Trials Actually Showed
Any honest assessment of effectiveness has to begin by describing the evidence, and here orforglipron is unusually well documented for a recently approved metabolic agent. Its clinical program spans a phase 1a single- and multiple-ascending-dose study, a phase 2 randomized controlled trial in obesity, and a suite of large phase 3 trials under the ATTAIN (obesity) and ACHIEVE (type 2 diabetes) program names, several of which have been published in the New England Journal of Medicine, The Lancet, and Nature Medicine.234567 This is a mature, peer-reviewed dataset, not a preprint-and-press-release situation.
The first-in-human phase 1a study, published by Pratt and colleagues in Diabetes, Obesity and Metabolism in 2023, established that orforglipron was orally bioavailable in healthy participants, had a pharmacokinetic profile compatible with once-daily dosing, and produced the expected GLP-1 class effects with a tolerability signal dominated by gastrointestinal events.4 These early studies do not measure obesity efficacy in a clinically meaningful population, but they are the foundation on which dose selection for later trials rested.
The phase 2 obesity trial, published in NEJM in 2023, was the first controlled look at weight outcomes. In adults with obesity, or overweight with a weight-related condition, orforglipron produced mean weight reductions in the range of roughly 8.6 percent to 12.6 percent at 26 weeks and approximately 9.4 percent to 14.7 percent at 36 weeks across the higher dose groups, substantially exceeding placebo.3 The magnitude at that stage was striking enough to justify a large phase 3 commitment, and importantly it was consistent with the class expectation that GLP-1 receptor agonism drives double-digit percentage weight loss over months rather than weeks.
The pivotal evidence, however, comes from phase 3. The table below orients the reader to the main controlled trials most relevant to obesity effectiveness before the following sections examine them in detail. All effect sizes should be read as trial-level averages; individual response varies widely, and the estimand (the statistical rule for handling people who stop treatment) materially changes the reported number, as explained in the methodology section.
| Trial | Population | Design and duration | Headline weight outcome (highest dose) |
|---|---|---|---|
| Phase 2 (NEJM 2023) | Obesity / overweight, no diabetes | Randomized, placebo-controlled, 36 weeks | Up to about 14.7% mean reduction3 |
| ATTAIN-1 | Obesity / overweight, no diabetes (n = 3127) | Randomized, placebo-controlled, 72 weeks | 12.4% (about 27.3 lb) by efficacy estimand2 |
| ATTAIN-2 | Obesity / overweight WITH type 2 diabetes (n = 1613) | Randomized, placebo-controlled, 72 weeks | 10.5% (about 22.9 lb)5 |
| ATTAIN-MAINTAIN | Prior injectable-GLP-1 responders | Randomized, placebo-controlled maintenance | Maintained roughly 75 to 79% of prior loss7 |
Read as a whole, the controlled evidence supports a confident claim: orforglipron reliably produces clinically meaningful weight reduction that is clearly superior to placebo across multiple large, well-conducted randomized trials. It does not support the claim that it is the most powerful weight-loss agent available, nor that its long-term cardiovascular and mortality benefits are established, because the outcome trials needed to prove those endpoints are still maturing. Keeping those two statements in the same frame is the essence of an evidence-cautious reading, and the next sections unpack each pivotal study so the numbers can be interpreted rather than simply repeated.
ATTAIN-1 in Detail: The Pivotal Obesity Trial
ATTAIN-1 is the study most directly relevant to the question in this article’s title, because it tested orforglipron specifically for obesity in people without diabetes, the population in which weight-loss efficacy is cleanest to interpret. It was a randomized, double-blind, placebo-controlled phase 3 trial that enrolled 3,127 adults with obesity, or overweight with a weight-related medical problem, and randomized them to one of three orforglipron doses (6 mg, 12 mg, or 36 mg once daily) or matching placebo, with treatment continuing for 72 weeks.212 The full results were published in the New England Journal of Medicine.2
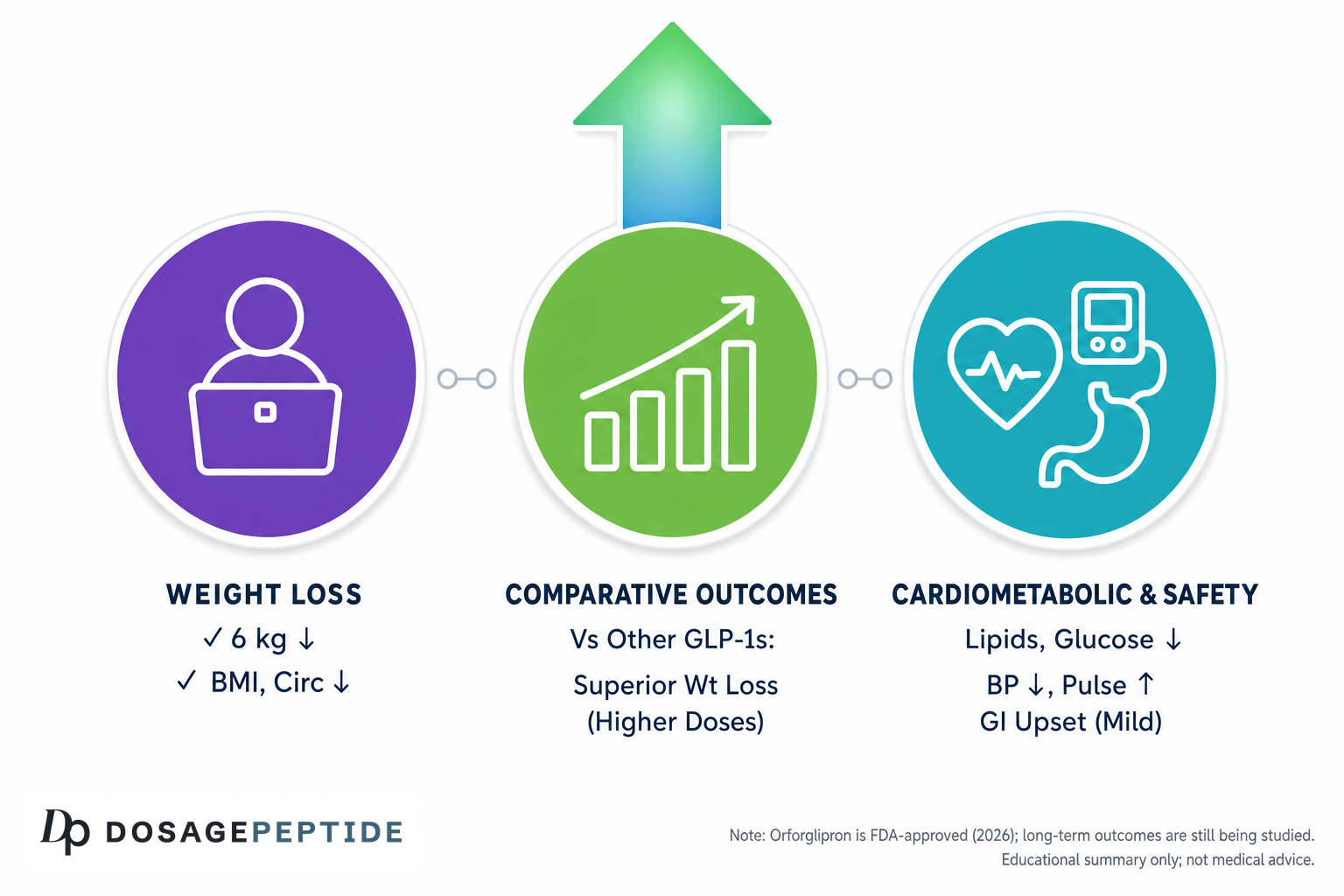
The primary efficacy finding was dose-dependent weight loss. Using the efficacy estimand, which estimates the effect if participants had adhered to treatment, the highest 36 mg dose produced a mean reduction of about 12.4 percent of body weight, corresponding to roughly 27.3 pounds, compared with about 0.9 percent (approximately 2.2 pounds) on placebo.12 Under the more conservative treatment-regimen estimand, which counts everyone as randomized regardless of whether they stopped the drug, the dose groups showed mean reductions in the region of 7.5 percent to 11.2 percent versus roughly 2.1 percent for placebo.2 The gap between those two numbers is not a contradiction; it is a window into how discontinuation affects apparent efficacy, and the honest reporting of both is a sign of a rigorous trial.
Responder analyses reinforced the average. On the highest dose, about 59.6 percent of participants achieved at least a 10 percent reduction in body weight, a categorical threshold widely used because losses in that range are associated with improvements in metabolic risk factors.2 Secondary cardiometabolic endpoints moved in the expected favorable direction as well, with improvements in waist circumference, blood pressure, and lipid measures accompanying the weight change.12 These are surrogate improvements rather than proven reductions in clinical events, a distinction that matters and is revisited under limitations.
The following table summarizes the dose-response relationship from ATTAIN-1 as reported, which is useful both for gauging effect size and for understanding why tolerability, not just efficacy, drives dose selection.
| Group | Mean weight change, efficacy estimand | Participants losing at least 10% |
|---|---|---|
| Placebo | About -0.9% | Low (reference) |
| Orforglipron 6 mg | Intermediate, dose-dependent | Intermediate |
| Orforglipron 12 mg | Intermediate, dose-dependent | Intermediate |
| Orforglipron 36 mg | About -12.4% (about 27.3 lb) | About 59.6%2 |
Two interpretive points deserve emphasis. First, the 72-week duration is a genuine strength; weight-loss agents are frequently over-hyped on short-term data, and a year and a half of controlled follow-up gives a far more trustworthy read on both magnitude and plateau behavior than a three-month study. Second, the clear dose response, with efficacy climbing from 6 mg to 36 mg alongside rising gastrointestinal side-effect and discontinuation rates, is the classic GLP-1 trade-off: more receptor engagement buys more weight loss at the cost of more nausea and more dropouts. That trade-off, rather than any ceiling on the molecule itself, is a large part of why the average effect sits where it does. Readers interested in how these controlled figures bear on durability over longer horizons can consult What Does Research Say About Orforglipron’s Long-Term Effects on Weight Loss?.
Beyond ATTAIN-1: Diabetes, Maintenance, and Head-to-Head Data
Effectiveness is easier to judge when a compound has been tested in several distinct populations and against active comparators rather than placebo alone. Orforglipron’s program is broad enough to allow that triangulation.
ATTAIN-2 extended the obesity question to people who also have type 2 diabetes, a population that historically loses somewhat less weight on GLP-1 therapy than people without diabetes. This 72-week randomized, double-blind, placebo-controlled trial enrolled 1,613 adults with obesity or overweight (body mass index at least 27) plus type 2 diabetes, using the same 6 mg, 12 mg, and 36 mg doses.5 The highest dose lowered body weight by about 10.5 percent (roughly 22.9 pounds) versus about 2.2 percent on placebo, with the three doses producing reductions of approximately 5.5 percent, 7.8 percent, and 10.5 percent.5 Glycemic control improved substantially, with a mean glycated hemoglobin (HbA1c) reduction of about 1.8 percent at the top dose, and between roughly 49.8 percent and 72.8 percent of participants across doses lost at least 5 percent of body weight, compared with about 24.4 percent on placebo.5 The slightly lower weight effect than in ATTAIN-1 is consistent with the well-known pattern in diabetes and does not signal a weaker drug.
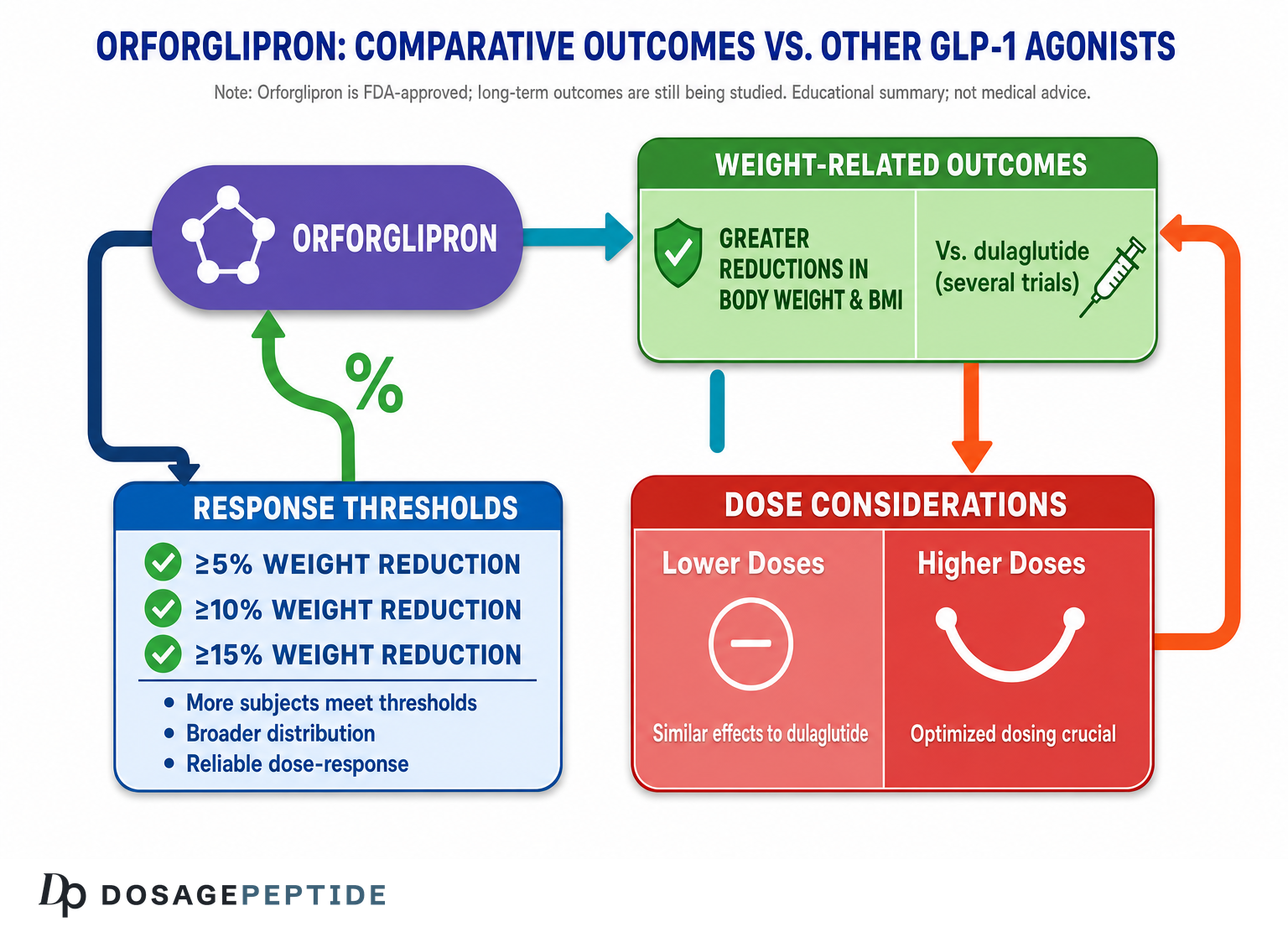
ACHIEVE-3 provided the most informative comparison of all: a head-to-head phase 3 trial against oral semaglutide, the only other approved oral GLP-1 option, in adults with type 2 diabetes. Over 52 weeks, orforglipron 36 mg lowered HbA1c by about 2.2 percent versus about 1.4 percent for oral semaglutide 14 mg, and produced greater weight loss, roughly 9.2 percent (about 19.7 pounds) versus about 5.3 percent (about 11.0 pounds).6 The 12 mg and 36 mg orforglipron doses met both non-inferiority and superiority criteria for HbA1c against the corresponding semaglutide doses.6 This is a strong efficacy signal because it comes from a direct randomized comparison rather than an unreliable cross-trial comparison, though the open-label design and the fact that both drugs are made by different manufacturers with different dose-optimization histories warrant caution.
ATTAIN-MAINTAIN addressed a different but practically vital question: can an oral pill hold onto weight loss that was originally achieved with a more potent injectable? In this phase 3b double-blind, placebo-controlled trial, participants who had lost weight on injectable tirzepatide (cohort 1) or semaglutide (cohort 2) during the SURMOUNT-5 study were switched to once-daily orforglipron or placebo.7 In the tirzepatide cohort, orforglipron maintained a mean 74.7 percent of the prior body-weight reduction versus 49.2 percent on placebo; in the semaglutide cohort, it maintained about 79.3 percent versus 37.6 percent.7 The candid framing used by the investigators was that switching to oral orforglipron preserved most, but not all, of the earlier loss, which is a reasonable summary and a useful counterweight to any impression that an oral agent fully substitutes for a maximally potent injectable.
Taken together, these three trials show orforglipron performing consistently across obesity, diabetes-complicated obesity, and maintenance settings, and beating an active oral comparator on glycemic and weight endpoints. That breadth is a real strength of the effectiveness case. It also sharpens the honest boundary: none of these trials was primarily a cardiovascular outcomes trial, so improved weight and metabolic markers should be read as strong intermediate evidence, not as proof of reduced heart attacks, strokes, or mortality.
How Orforglipron Compares With Related Compounds
Comparison is where a lot of well-meaning coverage goes astray, because the temptation is to line up headline percentages from separate trials as if they were a leaderboard. Cross-trial comparisons are genuinely unreliable: populations, baseline weights, durations, titration schemes, and estimands all differ. With that caveat stated plainly, an approximate landscape is still useful for orientation, provided the numbers are treated as ballpark context rather than precise rankings.
| Compound | Class / mechanism | Route | Approximate peak trial weight loss (context only) |
|---|---|---|---|
| Orforglipron | Non-peptide GLP-1 agonist | Oral, once daily | About 12.4% (ATTAIN-1)2 |
| Oral semaglutide (high dose) | Peptide GLP-1 agonist | Oral, once daily | Roughly mid-teens percent in its own trials10 |
| Injectable semaglutide 2.4 mg | Peptide GLP-1 agonist | Injectable, weekly | Roughly 15% (STEP program)10 |
| Tirzepatide | Dual GIP/GLP-1 agonist | Injectable, weekly | About 20% (SURMOUNT-1)13 |
| Retatrutide (investigational) | Triple GLP-1/GIP/glucagon agonist | Injectable, weekly | About 24% at 48 weeks in phase 214 |
Three fair conclusions emerge from this landscape. First, orforglipron’s weight effect is squarely in the range of established GLP-1 monotherapy and is not out of line with what a single-hormone agonist should achieve. Second, it sits below the dual and triple agonists, which is expected on mechanistic grounds: tirzepatide adds GIP receptor agonism and retatrutide adds both GIP and glucagon receptor engagement, and hitting more incretin pathways generally buys more weight loss.1314 Third, orforglipron’s advantage is not raw potency but form factor: it is the first small-molecule oral agent that delivers GLP-1-class efficacy without injections, cold chain, or restrictive dosing conditions.
Against oral semaglutide specifically, the head-to-head ACHIEVE-3 data give orforglipron a legitimate edge on both HbA1c and weight at the doses studied, which is the single most defensible comparative claim in its file because it rests on randomization rather than cross-study inference.6 Against the injectables, the honest statement is that orforglipron trades some efficacy for oral convenience. For many people that trade is attractive; for someone who needs the largest possible weight reduction, the injectable dual or triple agonists remain more potent. A more detailed side-by-side treatment lives in Orforglipron vs Semaglutide vs Tirzepatide.
One more comparison deserves mention because it is easy to overlook: orforglipron versus placebo-plus-lifestyle. Every trial discussed here delivered lifestyle counseling to all arms, so the drug effect is on top of diet and activity guidance, not instead of it. That is the correct real-world framing, since GLP-1 agonists are adjuncts to, not replacements for, behavioral and dietary change, and interpreting the effect sizes without that context overstates what the pill does on its own.
Research Models and Trial Methodology
Understanding how the orforglipron studies were built is essential to judging how much weight to put on their conclusions. The pivotal trials share a robust methodological backbone, and appreciating that backbone is what separates an informed reading from simply quoting a percentage.
The ATTAIN and ACHIEVE phase 3 trials were randomized and, for the placebo-controlled studies, double-blind, meaning neither participants nor investigators knew who received active drug.257 Randomization balances known and unknown confounders across arms, and blinding guards against the substantial placebo and expectation effects that plague weight-loss research. They were also large and multicenter, with several thousand participants across the obesity program, which improves the precision of effect estimates and the generalizability of tolerability findings. Registration on public trial registries such as ClinicalTrials.gov, for example the ATTAIN-1 record, adds a layer of pre-specification accountability.12
The single most important methodological concept for interpreting the numbers is the estimand. Modern obesity trials report at least two: the efficacy estimand (also called the on-treatment or trial-product estimand), which estimates the effect assuming participants stayed on the drug, and the treatment-regimen estimand (also called treatment-policy or intention-to-treat), which includes everyone as randomized even after they stop. Because a nontrivial fraction of participants discontinue GLP-1 agonists, usually for gastrointestinal intolerance, the efficacy estimand always yields a larger headline number than the treatment-regimen estimand. In ATTAIN-1 the top dose read as roughly 12.4 percent under the efficacy estimand but closer to 11 percent under the treatment-regimen estimand.2 Neither is “the truth”; they answer different questions, and any responsible summary should acknowledge which one it is quoting.
Several other design features shape interpretation. The 72-week duration in the obesity trials is long enough to capture the weight-loss plateau that typically emerges after the first year, which is valuable, but it is still short relative to the lifelong course of obesity. The endpoints are predominantly weight and cardiometabolic surrogates rather than hard outcomes such as myocardial infarction, stroke, or death; demonstrating hard-outcome benefit requires dedicated, longer, and larger cardiovascular outcomes trials that were not the purpose of the registration studies. And the trials embed a forced titration schedule, which optimizes tolerability but also means the reported side-effect rates reflect careful dose escalation rather than abrupt initiation.
Finally, sponsorship is a structural feature that belongs in any methodology discussion. The orforglipron program is overwhelmingly funded and run by its manufacturer. That does not invalidate the results; the trials are peer-reviewed, registered, and published in journals with rigorous standards, and the reporting of both estimands and of discontinuation is a mark of transparency. But industry sponsorship is a known source of potential bias in framing, comparator selection, and publication emphasis, and independent replication and post-marketing surveillance remain important for a fully rounded picture. Discussion of the mechanistic and preclinical models that underpin these human trials, including the rodent-inactivity issue, is expanded in What Evidence Shows Orforglipron Alters Systemic Metabolic Pathways in Models?.
Safety and Tolerability
Efficacy is only half of an effectiveness judgment; a drug that works but cannot be tolerated fails in practice. The controlled data give a clear and, importantly, class-consistent tolerability picture for orforglipron.
The dominant adverse events are gastrointestinal, exactly as expected for a GLP-1 receptor agonist. In ATTAIN-1, nausea was reported by approximately 28.9 percent, 35.9 percent, and 33.7 percent of participants on the 6 mg, 12 mg, and 36 mg doses respectively, versus about 10.4 percent on placebo.2 Constipation (roughly 21.7 to 29.8 percent versus 9.3 percent), diarrhea (roughly 21.0 to 23.1 percent versus 9.6 percent), and vomiting (roughly 13.0 to 24.0 percent versus 3.5 percent) followed the same pattern.2 Crucially, most of these events were mild to moderate, occurred during the dose-escalation phase, and were transient, resolving without permanent discontinuation.2 That temporal signature, front-loaded and self-limiting, is the reason slow titration is built into the dosing schedule.
| Adverse event (ATTAIN-1) | Orforglipron range across doses | Placebo |
|---|---|---|
| Nausea | About 28.9% to 35.9% | About 10.4% |
| Constipation | About 21.7% to 29.8% | About 9.3% |
| Diarrhea | About 21.0% to 23.1% | About 9.6% |
| Vomiting | About 13.0% to 24.0% | About 3.5% |
| Discontinuation for adverse events | About 5.3% to 10.3% | About 2.7% |
2
Discontinuation because of adverse events rose with dose, from about 5.3 percent at 6 mg to about 7.9 percent at 12 mg and about 10.3 percent at 36 mg, compared with about 2.7 percent on placebo, with most dropouts occurring during escalation and driven by gastrointestinal intolerance.2 This dose-dependence is the direct counterpart of the dose-dependent efficacy and is why the “best” dose for a given person is the highest one they can comfortably tolerate rather than automatically the maximum.
Beyond the gastrointestinal profile, a few points stand out from the controlled data. No hepatic safety signal was observed across the phase 3 program, which is reassuring given that some other small molecules in this space encountered liver-enzyme concerns.6 A modest increase in resting heart rate was seen, consistent with the GLP-1 class.6 In the head-to-head ACHIEVE-3 comparison, orforglipron carried somewhat higher rates of gastrointestinal events and adverse-event discontinuations than oral semaglutide, a reminder that its efficacy edge in that trial came with a tolerability cost.6
The approved labeling carries the GLP-1 class safeguards. There is a boxed warning regarding the potential risk of thyroid C-cell tumors, derived from rodent findings with peptide agonists; orforglipron is contraindicated in people with a personal or family history of medullary thyroid carcinoma or multiple endocrine neoplasia syndrome type 2, and it should be discontinued if pregnancy is recognized because of potential fetal harm.89 As noted earlier, orforglipron itself did not produce thyroid tumors in rodents and is not pharmacologically active at the rodent receptor, so the boxed warning is a conservative class-level precaution rather than a compound-specific finding, but it remains part of responsible use.10 Other class considerations, including pancreatitis vigilance and gallbladder events, apply as they do to GLP-1 therapy generally. Overall, the tolerability verdict is that orforglipron is manageable for most people with careful titration, unremarkable within its class, and free of any novel safety alarm in the controlled data collected so far.
Handling, Titration, and Formulation in a Research Context
Because orforglipron is a tablet rather than an injectable peptide, its handling profile is fundamentally different from the reconstituted lyophilized powders that dominate the research-peptide world. There is no vial to reconstitute, no bacteriostatic water to calculate, no cold-chain reconstitution math, and no drawing-up of doses; the compound is a stable, orally administered small molecule formulated as a conventional pill.1 For readers accustomed to the reconstitution workflow of peptide agonists, that alone is a meaningful practical distinction, and it is one of the recurring themes in coverage that frames orforglipron as a simplification of GLP-1 therapy.
The controlled trials used a forced titration approach, and the marketed product follows the same logic with a stepwise escalation to a maintenance dose. The pivotal obesity trials studied 6 mg, 12 mg, and 36 mg once-daily doses, and the therapeutic rationale for titration is entirely tolerability: escalating gradually allows the gastrointestinal system to adapt and dramatically reduces the nausea and vomiting that would otherwise accompany an abrupt start at a high dose.2 The approved product uses a monthly stepwise increase toward a maintenance dose, taken once daily at any time of day with or without food, precisely because the small-molecule pharmacology removes the fasting-and-water constraints that oral peptide formulations impose.19 Exact commercial titration steps are defined in the FDA prescribing information and should be followed only under medical supervision; this article does not reproduce them as a protocol.
It is worth flagging a source of confusion. The dose numbers used in the pivotal trials (6, 12, and 36 mg) are not necessarily identical to the milligram figures a person will see on a commercial titration pack, because formulation and bioavailability decisions can change the milligram-to-effect relationship between a trial tablet and a marketed one. Anyone comparing a trial paper to a pharmacy label should therefore not assume the numbers map one-to-one, and should defer to the official prescribing information for the approved product.9
From a research-context standpoint, the key handling messages are these. First, orforglipron is a pharmaceutical-grade prescription medicine with a defined manufacturing standard, not a compound that should be sourced from unregulated channels; material of unknown identity or purity sold as “orforglipron” carries no assurance of dose accuracy or safety. Second, the once-daily, food-independent oral administration is a genuine adherence advantage that could matter as much as intrinsic potency in real-world effectiveness, because a drug taken consistently outperforms a more potent one taken erratically. Third, because tolerability is titration-dependent, the trajectory of dose escalation is itself part of the intervention rather than an afterthought. For a structured overview of how a representative dosing schedule is laid out for study purposes, see the reference page Orforglipron 6 mg Dosage Protocol, with the caveat that any real-world use belongs strictly under a prescriber’s direction.
None of this should be read as encouragement to obtain or self-administer orforglipron outside a regulated clinical relationship. The point of covering handling is to complete the picture of what makes the compound distinctive, not to provide operational instructions. The convenience of a pill is real, but the medical supervision requirements of a potent metabolic drug are equally real, and the two facts sit together rather than in tension.
Limitations and the Human-Evidence Gap
A measured effectiveness verdict has to state clearly what the controlled evidence does not yet establish. For orforglipron, the gaps are less about the existence of data, which is abundant, and more about the specific endpoints and time horizons that remain open.
The most important limitation is that the pivotal trials measured weight and cardiometabolic surrogates, not hard clinical outcomes. Weight loss of 10 to 12 percent, improved HbA1c, better blood pressure, and improved lipids are all favorable and are reasonably associated with reduced risk, but association is not the same as proof that orforglipron reduces heart attacks, strokes, kidney disease progression, or death. Those endpoints require dedicated cardiovascular and renal outcomes trials with years of follow-up, and until such trials read out, any claim that orforglipron prevents disease events is unsupported by the current evidence.25
Durability beyond the trial windows is a second open question. The obesity trials ran 72 weeks, which is genuinely informative, but obesity is a chronic, relapsing condition, and GLP-1 pharmacology is well known to show substantial weight regain after discontinuation. The ATTAIN-MAINTAIN trial is encouraging in showing that oral orforglipron can preserve most, though not all, of previously achieved loss, yet it also implicitly confirms that continued treatment is required to maintain benefit and that stopping tends to reverse it.7 Multi-year real-world persistence and regain data are still accumulating.
Third, cross-trial comparisons remain unreliable, and this cuts against both over- and under-selling. The tidy leaderboard that ranks orforglipron below tirzepatide and retatrutide is directionally reasonable on mechanistic grounds but should not be treated as precise, because only the ACHIEVE-3 head-to-head against oral semaglutide rests on randomization.6 Everything else is inference across differently designed studies.
Fourth, the population studied, while large, does not cover every group. Long-term safety in older adults, people with significant comorbidities, adolescents, and pregnancy is either limited or, in the case of pregnancy, a contraindication, and the sponsor-driven nature of the program means independent long-horizon surveillance is only beginning. Network meta-analyses attempting to place orforglipron among its peers exist and are useful, but they inherit the limitations of the underlying trials and of indirect comparison.11
Finally, there is the ordinary gap between clinical-trial conditions and real life. Trial participants receive structured lifestyle support, close monitoring, and careful titration; adherence and tolerability in routine practice may differ, and the efficacy-versus-treatment-regimen estimand gap is a preview of how much discontinuation can erode average benefit. None of these limitations undermines the core finding that orforglipron is an effective weight-loss agent by the standard of controlled trials. They simply bound the claim: effective for weight and metabolic surrogates over roughly a year and a half, in the studied populations, with hard-outcome and very-long-term questions still to be answered.
Regulatory Status
Orforglipron’s regulatory position is unusually clear-cut for a compound often discussed alongside experimental peptides. In April 2026 the FDA approved it under the brand name Foundayo for chronic weight management in adults with obesity, or overweight adults with at least one weight-related comorbidity, making it the second oral GLP-1 receptor agonist approved for weight management and the first small-molecule, non-peptide one.18 The approval was notable procedurally as well, being handled under an FDA priority pathway, and it followed a large, published phase 3 program rather than accelerated or surrogate-only evidence.8
The approved indication is specific, and honesty about scope matters here. Orforglipron is authorized as an adjunct to a reduced-calorie diet and increased physical activity for weight management within defined body-mass-index criteria; it is not approved as a general wellness product, a cosmetic slimming aid, or a treatment for conditions outside its label. The prescribing information carries the class boxed warning on thyroid C-cell tumors, the contraindications in medullary thyroid carcinoma and multiple endocrine neoplasia type 2, and the standard pregnancy precautions discussed in the safety section.89 The full, legally controlling details live in the FDA label, which should be regarded as the authoritative source over any secondary summary.9
Beyond the United States, the regulatory picture in mid-2026 is one of active review and rolling submissions rather than universal approval. Lilly has pursued global regulatory filings on the strength of the completed phase 3 program, and European and United Kingdom authorities have the compound under evaluation, with additional diabetes and other indications also progressing through their own regulatory tracks.15 Availability, approved indications, and exact labeling therefore vary by country and continue to evolve, so region-specific verification against the relevant national regulator is essential rather than assuming the US position applies everywhere.
A concluding regulatory nuance is worth stating for an evidence-cautious audience. FDA approval confirms that, in the agency’s judgment, orforglipron’s demonstrated benefits outweigh its risks for the approved use based on the available data; it is a meaningful bar, not a rubber stamp. But approval is a beginning as much as an endpoint. Post-marketing safety surveillance, ongoing outcomes trials, and independent real-world studies will refine the effectiveness and safety profile over the coming years, and it would be premature to treat the current, largely sponsor-generated dataset as the final word. The compound is genuinely approved and genuinely effective for weight reduction by controlled-trial standards; it is also genuinely early in the accumulation of the long-term evidence that ultimately defines a chronic-disease therapy.
Frequently Asked Questions
How much weight did orforglipron produce in controlled obesity studies?
In the pivotal ATTAIN-1 phase 3 trial of adults with obesity and without diabetes, the highest 36 mg dose produced a mean reduction of about 12.4 percent of body weight, roughly 27.3 pounds, over 72 weeks using the efficacy estimand, compared with about 0.9 percent on placebo.2 Using the more conservative treatment-regimen estimand, which counts people who stopped the drug, the top-dose effect was closer to 11 percent.2 About 59.6 percent of participants on the highest dose lost at least 10 percent of body weight.2
Is orforglipron as effective as tirzepatide or retatrutide?
On the available evidence, no. Orforglipron’s roughly 12 percent average weight loss sits below the approximately 20 percent seen with injectable tirzepatide and the roughly 24 percent seen with investigational retatrutide in their own trials.21314 Those agents engage additional incretin pathways (GIP, and for retatrutide also glucagon), which mechanistically explains the larger effect. Orforglipron’s advantage is being an oral pill with GLP-1-class efficacy, not being the most potent option. Cross-trial numbers are approximate, since only direct randomized comparisons are fully reliable.
How does orforglipron compare with oral semaglutide?
In the head-to-head ACHIEVE-3 phase 3 trial in type 2 diabetes, orforglipron 36 mg lowered HbA1c more than oral semaglutide 14 mg (about 2.2 versus 1.4 percent) and produced greater weight loss (about 9.2 versus 5.3 percent), meeting non-inferiority and superiority criteria for glycemic control.6 This is the most reliable comparison in orforglipron’s file because it comes from a single randomized study. The trade-off was somewhat higher gastrointestinal side effects and discontinuations with orforglipron.6
What are the most common side effects?
The dominant adverse events are gastrointestinal and typical of the GLP-1 class: nausea, constipation, diarrhea, and vomiting. In ATTAIN-1, nausea occurred in roughly 29 to 36 percent of orforglipron participants versus about 10 percent on placebo, and most events were mild to moderate, happened during dose escalation, and resolved without stopping treatment.2 Discontinuation for adverse events ranged from about 5.3 percent at the lowest dose to about 10.3 percent at the highest, versus about 2.7 percent on placebo.2
Why can orforglipron be taken orally when most GLP-1 drugs are injected?
Because it is a non-peptide small molecule rather than a peptide. Peptide GLP-1 agonists are large and are degraded in the gut, so they are usually injected, and even oral semaglutide needs an absorption enhancer and strict fasting conditions. Orforglipron is a compact, drug-like molecule (about 883 daltons) that survives digestion, is absorbed as an ordinary tablet, and has a half-life supporting once-daily dosing with or without food.410 It activates the GLP-1 receptor through a transmembrane binding pocket distinct from where the natural peptide binds.10
Is orforglipron FDA approved, and for what?
Yes. The FDA approved orforglipron under the brand name Foundayo in April 2026 for chronic weight management in adults with obesity, or overweight with at least one weight-related comorbidity, as an adjunct to reduced-calorie diet and increased physical activity.18 It is the first small-molecule oral GLP-1 receptor agonist approved for weight management. The label carries a boxed warning on thyroid C-cell tumors and contraindications in medullary thyroid carcinoma and multiple endocrine neoplasia type 2.89
Does the weight loss last after stopping the drug?
The controlled evidence indicates that, like other GLP-1 agonists, benefit depends on continued treatment. The ATTAIN-MAINTAIN trial showed orforglipron preserved most, but not all, of the weight loss previously achieved with injectables (about 75 to 79 percent maintained versus roughly 37 to 49 percent on placebo), which implies that discontinuation tends to be followed by regain.7 Long-term, multi-year durability and real-world persistence data are still accumulating.
Has orforglipron been shown to reduce heart attacks, strokes, or death?
Not yet. The pivotal trials measured weight and cardiometabolic surrogate markers such as HbA1c, blood pressure, and lipids, all of which improved, but they were not designed to prove reductions in hard cardiovascular or mortality outcomes.25 Establishing such benefits requires dedicated, longer, and larger outcomes trials. Until those data are available, claims that orforglipron prevents disease events go beyond what the current controlled evidence supports.
Educational and Research-Only Disclaimer
This article is provided strictly for educational and informational purposes as part of a research-focused resource, and it is not medical advice, a treatment recommendation, or an endorsement of any product or supplier. Orforglipron (Foundayo) is a prescription medication that carries a boxed warning and defined contraindications, and it should be used only under the supervision of a qualified, licensed healthcare professional who can evaluate an individual’s full medical history. Nothing here should be interpreted as encouragement to obtain, compound, or self-administer orforglipron or any related compound outside a regulated clinical setting; material sold as “research grade” outside licensed pharmacies carries no assurance of identity, purity, or safety. Effect sizes summarized above are trial-level averages that do not predict any individual’s response, the evidence base is largely sponsor-generated and still maturing on long-term and hard-outcome endpoints, and no statement here should be read as a claim that orforglipron treats, cures, or prevents any disease. Always consult the current FDA prescribing information and a healthcare provider before making any decision related to this or any medication.
References
- Eli Lilly and Company. “Lilly’s oral GLP-1, orforglipron, delivers weight loss of up to an average of 27.3 lbs in first of two pivotal Phase 3 trials in adults with obesity” (ATTAIN-1 topline). Lilly Investor News. https://investor.lilly.com/news-releases/news-release-details/lillys-oral-glp-1-orforglipron-delivers-weight-loss-average-273
- Orforglipron, an Oral Small-Molecule GLP-1 Receptor Agonist for Obesity Treatment (ATTAIN-1). New England Journal of Medicine, 2026. https://www.nejm.org/doi/full/10.1056/NEJMoa2511774
- Wharton S, et al. Daily Oral GLP-1 Receptor Agonist Orforglipron for Adults with Obesity (Phase 2). New England Journal of Medicine, 2023. https://www.nejm.org/doi/full/10.1056/NEJMoa2302392 (PubMed 37351564)
- Pratt E, et al. Orforglipron (LY3502970), a novel oral non-peptide GLP-1 receptor agonist: a Phase 1a single- and multiple-ascending-dose study. Diabetes, Obesity and Metabolism, 2023. https://dom-pubs.onlinelibrary.wiley.com/doi/10.1111/dom.15184
- Orforglipron for the treatment of obesity in people with type 2 diabetes (ATTAIN-2): a phase 3 randomised, placebo-controlled trial. The Lancet, 2025. https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(25)02165-8/abstract
- Efficacy and safety of once-daily oral orforglipron compared with oral semaglutide in adults with type 2 diabetes (ACHIEVE-3): a non-inferiority, open-label, randomised phase 3 trial. The Lancet, 2026. https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(26)00202-3/abstract
- Orforglipron for maintenance of body weight reduction: the double-blind, randomized phase 3b ATTAIN-MAINTAIN trial. Nature Medicine, 2026. https://www.nature.com/articles/s41591-026-04386-7
- Eli Lilly and Company. “FDA approves Lilly’s Foundayo (orforglipron), the only GLP-1 pill for weight loss that can be taken any time of day without food or water restrictions.” Lilly Investor News, April 2026. https://investor.lilly.com/news-releases/news-release-details/fda-approves-lillys-foundayotm-orforglipron-only-glp-1-pill
- FOUNDAYO (orforglipron) tablets, for oral use – US FDA Prescribing Information, 2026. https://www.accessdata.fda.gov/drugsatfda_docs/label/2026/220934Orig1s000lbl.pdf
- Orforglipron: A Comprehensive Review of an Oral Small-Molecule GLP-1 Receptor Agonist for Obesity and Type 2 Diabetes. Int J Mol Sci / PMC, 2026. https://pmc.ncbi.nlm.nih.gov/articles/PMC12898445/
- Comparative Efficacy and Safety of Different Orforglipron Doses in Patients With Type 2 Diabetes Mellitus and Obesity: A Systematic Review and Network Meta-Analysis. PMC, 2026. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12923295/
- ClinicalTrials.gov. A Study of Orforglipron (LY3502970) in Adult Participants With Obesity or Overweight With Weight-Related Comorbidities (ATTAIN-1), NCT05869903. https://clinicaltrials.gov/study/NCT05869903
- Jastreboff AM, et al. Tirzepatide Once Weekly for the Treatment of Obesity (SURMOUNT-1). New England Journal of Medicine, 2022. https://www.nejm.org/doi/full/10.1056/NEJMoa2206038
- Jastreboff AM, et al. Triple-Hormone-Receptor Agonist Retatrutide for Obesity – A Phase 2 Trial. New England Journal of Medicine, 2023. https://www.nejm.org/doi/full/10.1056/NEJMoa2301972