The question sounds simple, but it hides a trap worth naming before we go any further. To ask what research says about orforglipron’s long-term effects on weight loss presumes that a body of long-term evidence exists. As of mid-2026 it largely does not — at least not in the sense a cardiologist or a longevity researcher would mean by “long term.” Orforglipron is a genuinely new kind of drug: the first oral, small-molecule (non-peptide) glucagon-like peptide-1 (GLP-1) receptor agonist to reach the market, approved by the U.S. Food and Drug Administration on April 1, 2026 under the brand name Foundayo for chronic weight management.1 That approval rests on a phase 3 program whose flagship weight-loss trials ran for 72 weeks — roughly sixteen months.23 Sixteen months is a substantial trial, but obesity is a chronic, relapsing condition that people live with for decades, and the evidence base does not yet stretch to the multi-year horizon where questions of durability, weight regain, and hard cardiovascular outcomes are actually answered.
So this article does something slightly different from the usual “how much weight will I lose” explainer. It takes the phrase “long-term effects” seriously and asks two separate questions. First, within the timeframe that has actually been studied — up to 72 weeks in the pivotal trials, plus a 52-week maintenance study — what does the research genuinely show about the magnitude and quality of weight loss? Second, and just as important, what remains unknown beyond that window: how durable is the effect over years, what happens on discontinuation, and whether weight loss translates into the outcomes that matter, such as reduced heart attacks, strokes, and mortality. The honest answer to the first is “clinically meaningful weight loss, now confirmed in large randomized trials.” The honest answer to the second is “we do not yet know, and the trials designed to tell us are still running.”4
This piece is written for researchers, clinicians, and educated readers who want the distinction between demonstrated fact and reasonable expectation kept clean throughout. We will cover what orforglipron is and why its non-peptide chemistry matters, the mechanism through which it acts, the full weight-loss evidence chain from phase 2 to phase 3, a close reading of the pivotal ATTAIN-1 trial, an explicit accounting of what “long term” can and cannot mean with the current data, the maintenance-and-regain question, how the drug compares with injectable incretins, its broader cardiometabolic effects, its safety profile, and its regulatory status. The guiding principle is restraint: orforglipron is an effective and now-approved weight-management medicine over the studied intervals, but the specific claim embedded in this article’s title — that we know its long-term effects — is one the evidence only partly supports.
What Orforglipron Is and Why Its Chemistry Is a Departure
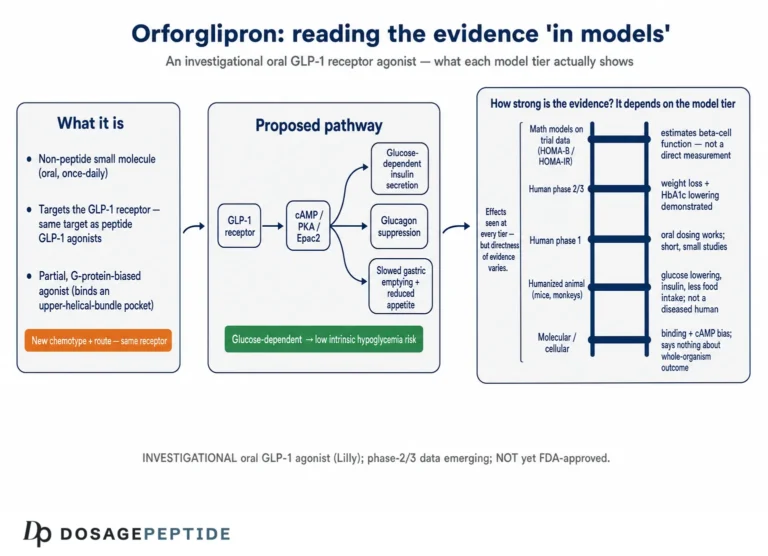
Orforglipron (development code LY3502970; brand name Foundayo) is a once-daily oral small-molecule agonist of the GLP-1 receptor, developed by Eli Lilly.15 To appreciate why it attracted so much attention, it helps to place it against the incretin therapies that came before it. Semaglutide and tirzepatide are peptides — chains of amino acids that structurally resemble the natural gut hormones they mimic. Peptides are exquisitely potent but chemically fragile: they are digested by proteases in the gut, which is why the injectable versions bypass the digestive tract entirely, and why the one approved oral peptide, oral semaglutide, must be taken on an empty stomach with a small sip of water, followed by a 30-minute fast, and even then achieves relatively low and variable absorption.6
Orforglipron is not a peptide at all. It is a fully synthetic small molecule built from aromatic and heteroaromatic ring systems, containing no peptide bonds whatsoever.67 That single structural fact cascades into a set of practical advantages. Because there are no peptide bonds, there is nothing for digestive proteases such as dipeptidyl peptidase-4 (DPP-4) or neutral endopeptidases to cleave, so the molecule survives the gut and is absorbed as an ordinary orally bioavailable drug.6 Its pharmacokinetics are correspondingly drug-like: a long elimination half-life reported in the range of roughly 25 to 68 hours supports once-daily dosing, and — crucially for adherence — it can be taken at any time of day without regard to food or water, the feature Lilly emphasized in its approval announcement.16 Early-phase pharmacology also suggested comparatively low interindividual variability in exposure, a desirable property for a chronically dosed medicine.6
The clinical development history is unusually well documented for a drug this new. Phase 1a and phase 1b studies in healthy volunteers and in people with type 2 diabetes established the safety, tolerability, and pharmacokinetic profile and defined the need for gradual dose escalation to manage gastrointestinal side effects.89 Phase 2 trials — one in obesity and one in type 2 diabetes, both published in 2023 — delivered the first efficacy signals.1011 A large phase 3 program (the ATTAIN trials for obesity and the ACHIEVE trials for diabetes) followed, and it is that program that underpins the 2026 approval.2312 For readers tracking how this molecule fits into the broader incretin story, the site’s explainer on incretin pathways provides useful background on the biology all these agents exploit.
A practical feature that follows directly from the tolerability profile is the dosing schedule. Orforglipron is not started at its effective dose; it is titrated upward over a period of weeks through a defined escalation sequence, precisely because the gastrointestinal effects that dominate its side-effect profile are worst when the receptor is engaged abruptly at full strength. The trials used stepwise escalation to the assigned maintenance dose (6, 12, or 36 mg in the obesity program), and the labeled use follows the same logic: begin low, increase gradually, and hold at the lowest dose that delivers the desired effect at acceptable tolerability. This is standard for the incretin class, but it matters for the long-term discussion because it means the full effect of any given dose is not seen immediately, and because titration is the main lever a clinician has for keeping a patient on therapy through the uncomfortable first weeks — the period when discontinuations cluster.
It is worth being precise about what “small molecule” buys and what it does not. The convenience gains are real and consequential: an oral pill that does not require injections, refrigeration in the same way, or fasting windows removes several of the practical barriers that limit incretin uptake. What the chemistry does not automatically confer is equivalent efficacy. As we will see, the magnitude of weight loss with orforglipron in obesity, while clinically meaningful, has generally trailed the injectable dual and triple agonists. Convenience and potency are separate axes, and orforglipron’s pitch is that it may deliver “most” of the effect in a far more accessible package — a genuinely important proposition for population-scale treatment, but not the same as claiming best-in-class weight loss.
How It Works: Mechanism and Why the Molecule Matters
The GLP-1 receptor is a class B G-protein-coupled receptor expressed in the pancreas, gut, and brain. Its natural ligand, GLP-1, is an incretin hormone released from intestinal cells after eating; it stimulates glucose-dependent insulin secretion, suppresses glucagon, slows gastric emptying, and acts on hypothalamic and brainstem circuits to reduce appetite and food intake. Peptide agonists like semaglutide engage the receptor much as the native hormone does, docking into the large extracellular orthosteric pocket that evolved to bind a peptide.7
Orforglipron cannot bind that way — it is far too small to occupy a pocket built for a 30-residue peptide. Structural work on this class, including a cryo-electron-microscopy study of the receptor bound to LY3502970, showed that the small molecule engages a more compact, largely hydrophobic region within the receptor’s transmembrane and extracellular-domain interface, stabilizing an active receptor conformation through a distinct binding mode.7 A later pharmacology study characterized orforglipron as a high-affinity, selective GLP-1 receptor ligand (with an inhibition constant on the order of 1 nM) and reported that relatively low receptor occupancy was sufficient to produce a full biological response, while its downstream signaling profile differed in detail from that of the peptide agonists.6 In diet-induced-obesity animal models, orally administered orforglipron produced weight loss comparable to subcutaneously injected semaglutide, providing the preclinical rationale that carried the molecule into human trials.6
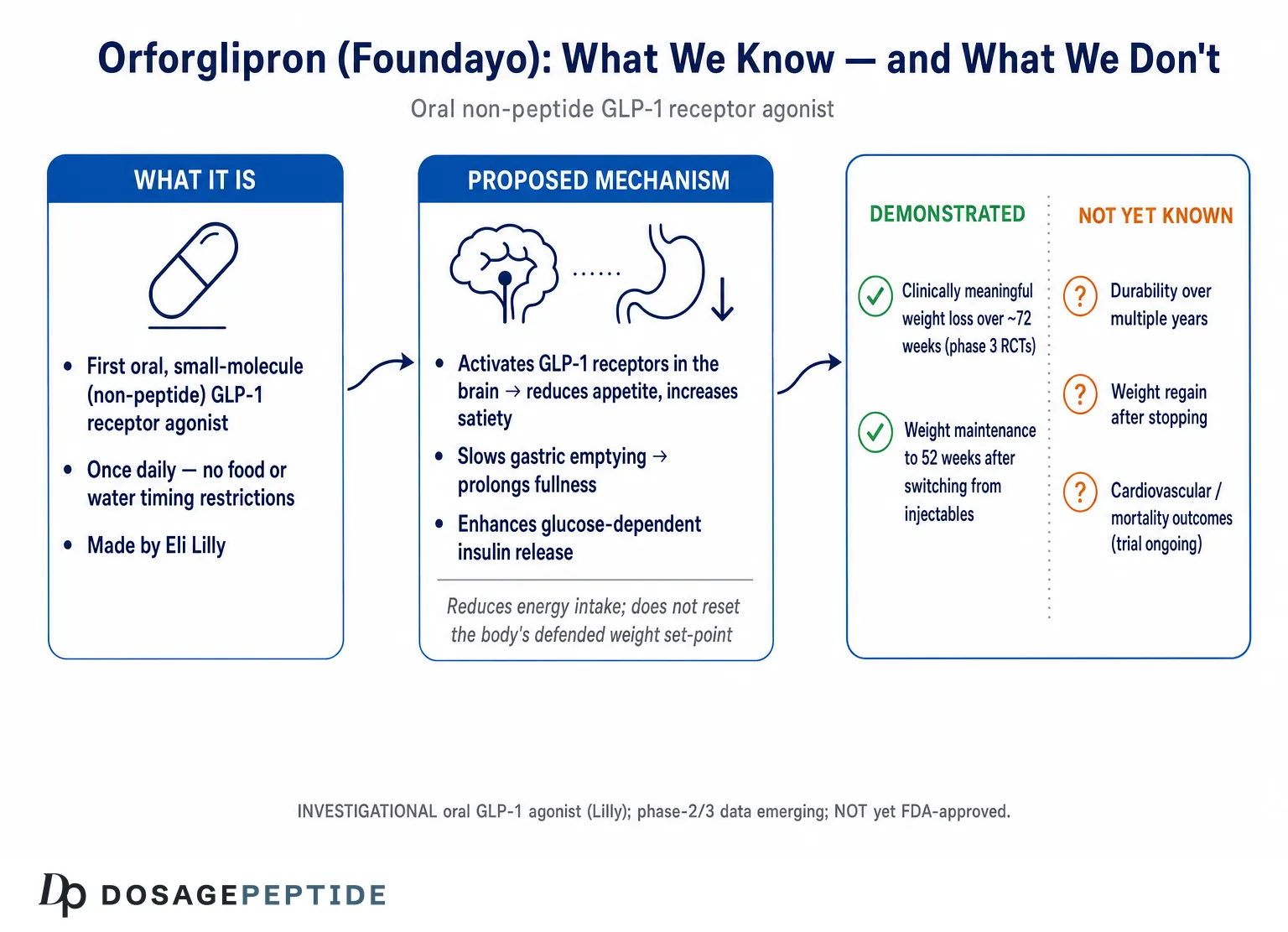
The physiological consequences of that receptor engagement are what actually drive weight loss, and they are worth spelling out because they explain both the benefits and the side-effect pattern. By activating GLP-1 receptors on appetite-regulating neurons, orforglipron reduces hunger and increases satiety, so people eat less without the same white-knuckle effort that undermines diet-alone approaches. By slowing gastric emptying, it prolongs the sense of fullness after a meal — the same mechanism responsible for the nausea and early satiety that dominate the side-effect profile. And by enhancing glucose-dependent insulin secretion and suppressing glucagon, it improves glycemic control, which is why the same molecule is being developed for type 2 diabetes.11
A subtler mechanistic point concerns how the receptor is activated, not merely whether it is. G-protein-coupled receptors can signal through several downstream pathways — classically the G-protein/cyclic-AMP cascade that drives the therapeutic insulin and satiety effects, but also β-arrestin-mediated pathways that promote receptor internalization and, over time, can contribute to desensitization. Because orforglipron engages the receptor through a binding mode distinct from that of the native peptide, its balance of these signaling arms differs in detail from semaglutide’s, and pharmacology work has noted that a relatively low fraction of receptors needs to be occupied to elicit a full functional response.6 The clinical significance of these signaling differences is not yet fully resolved, and it would be an overreach to claim they confer a proven advantage. But the distinction is worth understanding, because much of the marketing enthusiasm for “biased” small-molecule agonists rests on the hope that a favorable signaling profile might improve tolerability or durability — a hypothesis the long-term trials, not the receptor pharmacology, will ultimately have to confirm or refute.
One mechanistic nuance deserves emphasis because it bears on the long-term question. GLP-1 receptor agonism reduces body weight predominantly by reducing energy intake, not by directly and durably resetting the body’s defended weight “set point.” The physiology that defends against weight loss — falling energy expenditure, rising hunger signals — is powerful and does not simply switch off. This is the mechanistic reason weight tends to be regained when incretin therapy stops, a pattern documented repeatedly across the drug class, and a reason to expect (though not yet to have proven for orforglipron specifically) that continued dosing is required to sustain the effect. Readers interested in how the parent hormone family influences downstream metabolism can explore the site’s discussion of GLP-1 pathways in lipid metabolism.
The Weight-Loss Evidence Base: From Phase 2 to Phase 3
The most honest way to gauge orforglipron’s weight-loss effect is to walk up the evidence ladder chronologically, because each rung tested a longer duration and a larger population, and the story is one of a signal that held up as the trials grew.
The phase 2 obesity trial, published in the New England Journal of Medicine in 2023 by Wharton and colleagues, was a 36-week, randomized, double-blind, placebo-controlled dose-ranging study in adults with obesity, or overweight with a weight-related condition, and without diabetes.10 At 36 weeks, mean weight reduction reached up to about 14.7% at the higher doses, versus roughly 2.3% with placebo — a magnitude that immediately drew comparison with injectable agents.10 In parallel, the phase 2 type 2 diabetes trial published in The Lancet by Frías and colleagues showed HbA1c reductions of up to about 2.1% (roughly 1.7% placebo-adjusted) and weight reductions up to about 10.1 kg at 26 weeks, outperforming both placebo and the injectable comparator dulaglutide on those measures.11 These were encouraging but short studies in modest numbers of participants; they justified a phase 3 program rather than settling anything.
The phase 3 program then delivered three large, distinct weight-relevant trials, summarized below. It is this convergence — different populations, consistent direction, adequate size, and 72-week follow-up on the obesity trials — that constitutes the real evidentiary weight behind the drug.
| Trial | Population & duration | Key weight / glycemic result (highest dose) |
|---|---|---|
| Phase 2 obesity (Wharton 2023) | Obesity/overweight, no diabetes; 36 weeks10 | Up to ~14.7% weight loss vs ~2.3% placebo |
| Phase 2 T2D (Frías 2023) | Type 2 diabetes; 26 weeks11 | HbA1c up to −2.1%; weight up to −10.1 kg |
| ATTAIN-1 (2025) | Obesity/overweight, no diabetes; 72 weeks; n=31272 | −12.4% (36 mg) vs −0.9% placebo |
| ATTAIN-2 (2025) | Obesity + type 2 diabetes; 72 weeks; n=161312 | −10.5% weight; HbA1c −1.8% |
| ACHIEVE-1 (2025) | Early T2D monotherapy; 40 weeks; n=55913 | HbA1c −1.5%; weight −7.9% (36 mg) |
Two observations follow from this table. First, the weight-loss effect is consistent and dose-dependent across populations, and it is larger in people without diabetes (ATTAIN-1, −12.4%) than in people with diabetes (ATTAIN-2, −10.5%; ACHIEVE-1, −7.9%) — a pattern seen with every incretin therapy, because diabetes blunts the weight response. Second, and central to this article’s theme, the longest of these trials ran 72 weeks. That is the outer edge of the controlled evidence for weight loss. Everything said about “long-term” effects beyond roughly a year and a half is extrapolation, not demonstration — a point we return to deliberately.
Reading ATTAIN-1 Closely: The Pivotal Obesity Trial
Because ATTAIN-1 is the single most important weight-loss study — the largest, the longest, and the one in the population for which the drug was approved — it repays careful reading rather than a one-line headline.2 It was a phase 3, multinational, randomized, double-blind, placebo-controlled trial that enrolled 3,127 adults with obesity, or overweight with a weight-related complication, and without type 2 diabetes. Participants were assigned to orforglipron 6 mg, 12 mg, or 36 mg, or placebo, once daily for 72 weeks, all as an adjunct to a reduced-calorie diet and increased physical activity.
On the primary endpoint, the 36 mg dose produced a mean weight reduction of 12.4% versus 0.9% with placebo, with the 6 mg and 12 mg doses producing intermediate, dose-ordered reductions.2 The categorical responder analyses arguably matter more for clinical meaning than the average: at the top dose, 59.6% of participants lost at least 10% of body weight and 39.6% lost at least 15%.4 Those thresholds are the ones associated in the broader obesity literature with improvements in blood pressure, glycemia, and other risk factors, so crossing them is what makes the loss clinically consequential rather than merely cosmetic.
Several details deserve honest emphasis. The weight-loss trajectory in ATTAIN-1 had not clearly reached a plateau by week 72; the curve was still gently descending at the end of the trial, which suggests the asymptotic maximum was not captured within the study window and leaves genuinely open the question of what additional loss (or stabilization) longer dosing would produce.2 This cuts both ways for the “long-term” framing: it hints that effects could deepen with time, but it also means the trial did not observe the steady-state that long-term management actually depends on. Beyond weight, orforglipron improved a panel of cardiometabolic risk factors — non-HDL cholesterol, systolic blood pressure, and triglycerides — and reduced high-sensitivity C-reactive protein, a marker of inflammation, by roughly half at the highest dose.4 On the safety side, the profile was consistent with the GLP-1 class: predominantly mild-to-moderate gastrointestinal adverse events (nausea, diarrhea, constipation, vomiting), concentrated during the dose-escalation phase, with treatment discontinuation for adverse events higher on active drug than placebo and driven mainly by those gastrointestinal effects.2
One methodological point is worth surfacing because it explains apparent discrepancies between headline numbers. Modern obesity trials report results under more than one “estimand” — different rules for handling participants who stop the drug or the trial. The efficacy estimand estimates the effect if participants had stayed on treatment as intended and tends to give the larger number (the 12.4% figure), while a treatment-regimen estimand reflects the effect regardless of adherence and is typically somewhat smaller. Neither is “the truth” and the other a spin; they answer different questions, and honest reading requires knowing which is being quoted. For a long-term-management perspective, the treatment-regimen view — what happens on average including the people who cannot tolerate the drug — is arguably the more realistic guide to population-level benefit, and it is systematically lower than the efficacy-estimand headline.
The measured conclusion from ATTAIN-1 is that orforglipron produces clinically meaningful, dose-dependent weight loss over 72 weeks with a class-typical, manageable side-effect profile. That is a strong result and fully supports the drug’s approval for weight management. It is not, however, evidence about years-long use, and the still-descending curve is a reminder that even the mean 12.4% figure is a 72-week snapshot rather than a final destination.
What “Long-Term” Actually Means Here — and the Limits of the Data
This section is the heart of the article, because it is where the title’s premise must be examined rather than assumed. When clinicians, regulators, and patients talk about the “long-term effects” of a chronic-disease therapy, they generally mean at least three things, and orforglipron’s evidence base addresses them very unevenly.
Durability of weight loss over years. The controlled weight-loss data extend to 72 weeks. There is, as of mid-2026, no published multi-year randomized weight-loss trial of orforglipron. By comparison, the injectable incretins accumulated 2-year (and, for the class, longer) data before their long-term durability could be discussed with confidence. For orforglipron, the honest statement is that durability beyond ~72 weeks is expected by analogy to the class but not yet demonstrated for this molecule.
Effect on hard clinical outcomes. Weight loss is a surrogate. What ultimately justifies chronic therapy in a cardiovascular-risk population is a reduction in events — heart attacks, strokes, cardiovascular death, kidney decline. The dedicated cardiovascular-outcomes trial for orforglipron, ATTAIN-Outcomes (NCT07241390), is an event-driven study in people with established atherosclerotic cardiovascular disease and/or chronic kidney disease, and it was still recruiting in 2026.14 Until it reports, any claim that orforglipron improves long-term survival or cardiovascular outcomes is unproven for this drug specifically, however plausible it is given class data from other GLP-1 agents.
Long-term safety. The 72-week trials did not surface unexpected safety signals beyond the known class effects, and the program tracked liver enzymes, heart rate, gallbladder events, and other class-relevant parameters. But rare or slow-to-emerge effects are, by definition, harder to detect in trials of this length, and post-marketing surveillance after the April 2026 approval will be the real source of long-term safety knowledge.1
The table below lays out this “known vs not-yet-known” distinction explicitly, because collapsing it is the single most common way that writing about orforglipron overstates the evidence.
| Question about long-term effects | Status of the evidence (mid-2026) |
|---|---|
| Weight loss over ~72 weeks | Demonstrated in large phase 3 RCTs212 |
| Weight maintenance after switching from injectables (52 wk) | Demonstrated in ATTAIN-MAINTAIN15 |
| Durability over multiple years | Not yet studied; expected by class analogy only |
| Weight regain after stopping | Not yet published for orforglipron; regain typical of the class |
| Cardiovascular / mortality outcomes | Trial (ATTAIN-Outcomes) ongoing; no results yet14 |
| Rare / long-latency safety events | To be defined by post-marketing surveillance |
It is worth being concrete about what a genuine multi-year answer would require, because it clarifies why the current data cannot supply one. A convincing long-term durability study would need to follow a large cohort on continuous orforglipron for at least two to four years, with prespecified weight trajectories, retention and adherence tracking, and ideally a maintained placebo or comparator arm — a demanding design, since long placebo exposure in people with a treatable disease raises ethical and retention problems. It would also need to capture the physiology that fights weight loss: the adaptive fall in resting energy expenditure and the rise in orexigenic (hunger-promoting) signaling that together defend the body’s prior weight. Because orforglipron acts by suppressing appetite rather than by dismantling that defense, the realistic long-term expectation is that continued dosing holds weight at a new lower plateau rather than driving indefinite further loss — but “realistic expectation” is exactly the phrase that signals inference rather than data. Until a multi-year trial reports, the field is reasoning from mechanism and from the behavior of related drugs, not from direct observation of orforglipron over that horizon.
None of this diminishes what has been shown. It simply keeps the ledger honest: orforglipron is an effective weight-loss drug over the intervals studied, and a promising candidate for long-term management, but the specific long-term claims most people care about — years of sustained loss, fewer cardiovascular events, a fully characterized safety tail — are pending, not settled. For a parallel discussion of how the field wrestles with exactly this durability question in a longer-studied agent, the analysis of whether semaglutide offers a sustainable long-term solution is directly relevant.
Weight Maintenance, Discontinuation, and the Regain Question
If the long-term concern is whether weight stays off, two related sub-questions arise: can orforglipron hold weight that was lost by another means, and what happens when a person stops taking it? The evidence speaks clearly to the first and only indirectly to the second.
On maintenance, the phase 3b ATTAIN-MAINTAIN trial provides the most pertinent data. In this randomized, double-blind study, participants who had first lost weight on maximally tolerated doses of injectable semaglutide or tirzepatide were switched to oral orforglipron (or placebo) and followed for 52 weeks.15 Orforglipron met its primary and key secondary endpoints: those who switched from semaglutide, for example, maintained their prior weight loss with only a small average change (on the order of 0.9 kg), whereas the placebo group regained substantially.15 This is genuinely useful evidence for a “step-down” strategy — using a convenient daily pill to hold gains achieved with a more potent injectable — and it directly addresses one long-term-management scenario.
On discontinuation, the picture must be drawn more carefully to avoid overstating. There is not, as of this writing, a published dedicated orforglipron withdrawal trial analogous to the randomized-withdrawal studies conducted for semaglutide and tirzepatide. What we can say is grounded in mechanism and class behavior rather than orforglipron-specific data: because GLP-1 receptor agonists suppress appetite while they are present but do not permanently reset the body’s weight-regulatory physiology, weight is generally regained after the drug is stopped, and the randomized-withdrawal literature for the injectable agents shows substantial regain within a year of discontinuation. It is reasonable to expect orforglipron to behave similarly, but that expectation is an inference from the class, and readers should treat any confident numerical claim about orforglipron-specific regain with skepticism until such a trial is published.
The practical implication, consistent with how obesity medicine now frames these agents, is that orforglipron is best understood as a treatment for a chronic condition — taken continuously, like an antihypertensive — rather than a time-limited “course” after which the problem is cured. This framing is itself a long-term consideration: it means the relevant long-term data are not just about efficacy but about the feasibility, cost, and tolerability of indefinite daily dosing, and about adherence, where the oral, restriction-free format may prove to be orforglipron’s most durable advantage over injectables.
Orforglipron Versus Injectable Incretins: An Honest Comparison
Any realistic assessment of orforglipron’s place in weight management has to compare it with the injectable agents that set the current benchmark, and this is a place where honesty requires resisting hype in both directions. Orforglipron is neither the weak sibling nor the conqueror of the incretin field; it occupies a specific and defensible niche defined by the trade-off between magnitude of effect and accessibility.
On the magnitude of weight loss, the injectable dual and triple agonists remain ahead. In their own pivotal obesity trials, injectable semaglutide produced roughly 15% mean weight loss, tirzepatide (a dual GIP/GLP-1 agonist) reached roughly 20–22%, and retatrutide (a triple GIP/GLP-1/glucagon agonist still in development) reported up to roughly 24% in phase 2. Orforglipron’s 12.4% in ATTAIN-1 places it below all three — broadly in the neighborhood of, though somewhat under, injectable semaglutide, and clearly behind the dual and triple agonists.2 These comparisons are across separate trials with different populations and must not be read as head-to-head results, but the ordering is consistent enough to be meaningful. For context on the higher end of that spectrum, see the site’s overview of how effective tirzepatide is in recent studies and its pillar explainer on the retatrutide triple receptor agonist.
On everything else, orforglipron has the advantage. It is a pill, not an injection. It has no food or water timing restrictions, unlike oral semaglutide. It is a synthetic small molecule that can be manufactured at large scale without the biologics infrastructure peptides require — a point with real implications for global supply and cost, and arguably orforglipron’s most important long-term societal effect, since the binding constraint on incretin therapy has often been access rather than efficacy. The comparison below frames the trade-off.
| Attribute | Orforglipron (oral) | Injectable incretins (semaglutide / tirzepatide) |
|---|---|---|
| Molecule type | Non-peptide small molecule | Peptide |
| Route | Oral, once daily | Subcutaneous injection, weekly |
| Food/water restrictions | None1 | None for injectables; strict for oral semaglutide |
| Peak trial weight loss (obesity) | ~12.4% at 72 wk2 | ~15% (sema) to ~20–22% (tirz) |
| Manufacturing / scalability | Chemical synthesis; highly scalable | Biologic peptide synthesis |
| Long-term CV outcome data | Pending (ATTAIN-Outcomes)14 | Positive outcome trials exist for the class |
There is also a cost-and-access dimension that is easy to overlook but may prove to be the most consequential long-term effect of all — not on any individual’s weight, but on how many people can be treated. Peptide biologics are expensive and supply-constrained to manufacture, which has repeatedly produced shortages of the injectable incretins and priced them out of reach for large populations, particularly outside wealthy health systems. A small molecule made by conventional chemical synthesis sidesteps much of that constraint, and Lilly has positioned orforglipron explicitly as a scalable, potentially lower-cost oral option. If that promise holds, the drug’s largest contribution to long-term weight-loss outcomes at the population level could come less from per-patient efficacy and more from the sheer number of patients who can actually start and stay on an effective therapy. That is a plausible and important hypothesis, but it remains a hypothesis about pricing and supply that the coming years, not the clinical trials, will settle.
The synthesis is that orforglipron is likely to matter less because it beats the injectables on the scale and more because it lowers the barrier to entry: a convenient, scalable oral option that delivers a clinically meaningful fraction of injectable efficacy could expand access far beyond the current treated population. Whether that access advantage also translates into better long-term real-world outcomes — through improved adherence and persistence — is a hypothesis that only years of post-marketing data can test.
Metabolic and Cardiometabolic Effects Beyond the Scale
Weight is the headline, but the trials measured a broader set of metabolic effects that are arguably more important for long-term health, since they map onto the pathways through which obesity actually harms the body. Here the evidence is real for the studied intervals, and again distinct from the not-yet-tested outcome question.
In the type 2 diabetes program, orforglipron demonstrated substantial glycemic benefit. In ACHIEVE-1, a 40-week monotherapy trial in 559 adults with early type 2 diabetes inadequately controlled on diet and exercise, HbA1c fell by roughly 1.3% to 1.6% across doses versus about 0.1% with placebo, and more than 65% of participants on the highest dose reached an HbA1c of 6.5% or below, with no episodes of severe hypoglycemia.13 ATTAIN-2, in people with both obesity and type 2 diabetes, paired a 10.5% weight reduction with an HbA1c drop of about 1.8%.12 The glucose-dependent nature of GLP-1-mediated insulin secretion is what keeps the hypoglycemia risk low when the drug is used without insulin or sulfonylureas — a meaningful safety feature for chronic use.
Beyond glucose, the ATTAIN-1 obesity trial reported favorable movement in a cluster of cardiovascular risk factors: reductions in non-HDL cholesterol, systolic blood pressure, and triglycerides, alongside a roughly 50% reduction in high-sensitivity C-reactive protein, and this pattern of cardiometabolic improvement was consistent across the phase 3 program.4 These are the kinds of intermediate changes that, in other drug classes, have often (though not always) predicted eventual outcome benefits.
The essential caveat repeats here because it is easy to lose: improvements in blood pressure, lipids, inflammation, and HbA1c are surrogate markers. They make a reduction in cardiovascular events plausible, and they are genuine benefits in their own right, but they are not the same as a demonstrated reduction in heart attacks, strokes, or death. That demonstration awaits ATTAIN-Outcomes.14 A reader wanting to understand why the field treats lipid effects as mechanistically important but not automatically outcome-defining will find the discussion of GLP-1 regulation of lipid metabolism a useful companion.
Safety, Tolerability, and Open Questions
Across the phase 3 program, orforglipron’s safety profile was reported as consistent with the established GLP-1 receptor agonist class, which is both reassuring (the class is well characterized) and a reminder that the drug inherits the class’s known issues.213
The dominant adverse events were gastrointestinal — nausea, diarrhea, vomiting, constipation, and dyspepsia — and they were predominantly mild to moderate, most common during the dose-escalation period, and the leading reason for treatment discontinuation on active drug.213 This is precisely why the drug is titrated upward gradually rather than started at the top dose; the escalation schedule is a tolerability tool, not merely a formality. Serious hypoglycemia was rare and, in the diabetes trials, essentially absent in the absence of concomitant insulin or sulfonylureas, reflecting the glucose-dependent mechanism.13
Several considerations temper any “clean-so-far” reading and constitute the honest open questions:
- Trial duration. A favorable 72-week profile does not characterize years of continuous exposure. Class-relevant concerns that require long observation — such as gallbladder disease, pancreatitis signals, and the theoretical thyroid C-cell tumor concern that carries a class boxed warning for GLP-1 agents — are best assessed through extended surveillance rather than a 16-month trial.1
- Muscle and bone. As with all agents that produce large weight loss, a fraction of the loss is lean mass, and the long-term implications for muscle and bone in older or frail patients remain an active area of investigation across the entire incretin class, orforglipron included.
- Population breadth. The pivotal trials studied defined populations; behavior in pregnancy, in advanced organ dysfunction, and in the very elderly is less characterized and warrants caution.
- Real-world adherence. Daily oral dosing trades the burden of weekly injection for the discipline of a daily pill; whether that improves or, in some patients, worsens persistence is an empirical question for post-marketing study.
The balanced reading is that orforglipron has not thrown up unexpected safety signals in trials of up to 72 weeks and behaves like a typical, manageable GLP-1 agent, while the definitive long-term safety statement can only come from the post-approval period now under way. Researchers cataloging the compound alongside related metabolic agents can consult the site’s central dosages index and its peptide-science glossary for terminology and comparative framing.
Regulatory Status and What Comes Next
Precision matters here because the regulatory picture changed materially in 2026 and is easy to misstate. On April 1, 2026, the FDA approved orforglipron under the brand name Foundayo for chronic weight management — specifically, for use with a reduced-calorie diet and increased physical activity in adults with obesity, or overweight with at least one weight-related comorbid condition.1 This made orforglipron the first oral small-molecule GLP-1 receptor agonist approved for weight loss, and Lilly emphasized that it can be taken at any time of day without food or water restrictions.1
Two clarifications keep this accurate. First, the approval is for weight management; as of mid-2026, orforglipron was not yet approved for type 2 diabetes, though Lilly indicated it would file for that indication on the strength of the ACHIEVE program, so the diabetes use remained investigational at the time of writing.113 Second, an FDA approval based on 72-week trials authorizes use; it does not retroactively create the multi-year efficacy and outcome data discussed above. Approval and long-term evidence are different things, and the presence of the former should not be mistaken for the latter.
Looking forward, the evidence gaps this article has flagged are, encouragingly, being addressed by active research. The ATTAIN-Outcomes cardiovascular trial will, when it reports, tell us whether the surrogate improvements translate into fewer events.14 Ongoing and planned studies extend the program into adolescents, into specific comorbid populations, and into head-to-head and combination designs. The comprehensive reviews now appearing in the literature provide a consolidated map of where the molecule stands.5 For the specific question of long-term effects on weight loss, the trajectory is clear: the answer will get more complete over the next several years, and the responsible posture today is to state confidently what the 72-week trials showed while explicitly marking the multi-year horizon as still under investigation.
Frequently Asked Questions
How much weight does orforglipron cause people to lose?
In the pivotal 72-week ATTAIN-1 obesity trial, the 36 mg dose produced a mean weight reduction of 12.4% versus 0.9% with placebo, with 59.6% of participants losing at least 10% of body weight and 39.6% losing at least 15%.24 Weight loss was somewhat lower in people with type 2 diabetes (about 10.5% in ATTAIN-2) — a pattern seen with every incretin therapy.12 These figures are averages over the studied period, not guaranteed individual results.
Do we actually know orforglipron’s long-term (multi-year) effects?
Not yet, and this is the honest crux. The longest controlled weight-loss trials ran 72 weeks, and a separate maintenance study ran 52 weeks after switching from injectables.215 There is no published multi-year randomized weight-loss trial of orforglipron, and its cardiovascular-outcomes trial (ATTAIN-Outcomes) was still recruiting in 2026.14 Durability over years is expected by analogy to the GLP-1 class but has not been demonstrated for this specific drug.
Is orforglipron FDA-approved?
Yes, for weight management. The FDA approved it on April 1, 2026 under the brand name Foundayo for chronic weight management in adults with obesity, or overweight with a weight-related condition, alongside diet and exercise.1 It was not yet approved for type 2 diabetes as of mid-2026, though a filing for that use was anticipated.13
Will the weight come back if someone stops taking it?
Most likely, based on how the entire GLP-1 class behaves. These drugs reduce appetite while present but do not permanently reset the body’s weight-regulatory physiology, so weight is generally regained after stopping in the injectable agents’ withdrawal trials. A dedicated orforglipron-specific withdrawal trial has not been published, so precise regain figures for this drug are not yet established; the expectation of regain is an inference from the class. Obesity medicine now treats these agents as long-term therapies rather than short courses.
How does orforglipron compare with injectable Ozempic, Wegovy, or Zepbound?
On peak weight loss, the injectables lead: injectable semaglutide reaches about 15% and tirzepatide about 20–22% in their own trials, versus 12.4% for orforglipron in ATTAIN-1 — comparisons across separate trials, so not head-to-head.2 Orforglipron’s advantages are convenience (a daily pill with no food or water restrictions) and manufacturing scalability, which could meaningfully expand access.1
Why is it called a “non-peptide” GLP-1 agonist, and why does that matter?
Unlike semaglutide and tirzepatide, which are peptides (amino-acid chains), orforglipron is a fully synthetic small molecule with no peptide bonds.6 That means digestive proteases cannot break it down, so it can be taken as an ordinary oral pill with drug-like pharmacokinetics and a long half-life, and it can be manufactured by chemical synthesis rather than biologic peptide production.67
Does orforglipron do anything beyond weight loss?
Yes, over the studied intervals. It lowers HbA1c substantially in type 2 diabetes (about 1.3–1.8% across trials) and improves cardiovascular risk factors including non-HDL cholesterol, systolic blood pressure, triglycerides, and C-reactive protein.413 These are beneficial surrogate changes, but a reduction in actual cardiovascular events has not yet been demonstrated and awaits the ATTAIN-Outcomes trial.14
What are the main side effects?
Predominantly gastrointestinal — nausea, diarrhea, vomiting, constipation, and dyspepsia — mostly mild to moderate and concentrated during the gradual dose-escalation phase, which is why the drug is titrated up slowly.213 These were the leading reason for discontinuation on active drug. Serious hypoglycemia was rare because the insulin effect is glucose-dependent.
Is orforglipron a peptide sold for research use?
No. Orforglipron is an approved pharmaceutical medicine (Foundayo), not a research peptide, and this article is educational rather than a sourcing or usage guide. It should be used only as prescribed by a qualified clinician; nothing here is medical advice.1
References
- Eli Lilly and Company. FDA approves Lilly’s Foundayo (orforglipron), the only GLP-1 pill for weight loss that can be taken any time of day without food or water restrictions. Press release, April 1, 2026. https://www.prnewswire.com/news-releases/fda-approves-lillys-foundayo-orforglipron-…
- Wharton S, Aronne LJ, et al. Orforglipron, an Oral Small-Molecule GLP-1 Receptor Agonist for Obesity Treatment (ATTAIN-1). N Engl J Med. 2025. DOI 10.1056/NEJMoa2511774. https://www.nejm.org/doi/full/10.1056/NEJMoa2511774
- Eli Lilly and Company. Lilly’s oral GLP-1, orforglipron, demonstrated meaningful weight loss and cardiometabolic improvements in complete ATTAIN-1 results published in NEJM. 2025. https://lilly.gcs-web.com/news-releases/news-release-details/lillys-oral-glp-1-orforglipron-demonstrated-meaningful-weight
- American College of Cardiology. ATTAIN-1: Oral Orforglipron Significantly Reduces Weight, Cardiometabolic Risk. Journal Scan, 2025. https://www.acc.org/Latest-in-Cardiology/Journal-Scans/2025/09/24/16/48/ATTAIN-1
- Orforglipron: A Comprehensive Review of an Oral Small-Molecule GLP-1 Receptor Agonist for Obesity and Type 2 Diabetes. Int J Mol Sci. 2026. PMCID PMC12898445. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12898445/
- Sloop KW, et al. The pharmacological basis for nonpeptide agonism of the GLP-1 receptor by orforglipron. Sci Transl Med. 2024. PMID 39693407. DOI 10.1126/scitranslmed.adp5765. https://www.science.org/doi/10.1126/scitranslmed.adp5765
- Kawai T, et al. Structural basis for GLP-1 receptor activation by LY3502970, an orally active nonpeptide agonist. Proc Natl Acad Sci USA. 2020;117(47):29959-29967. PMCID PMC7703558. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7703558/
- Pratt E, et al. Orforglipron (LY3502970), a novel, oral non-peptide GLP-1 receptor agonist: a Phase 1a, blinded, placebo-controlled, randomized, single- and multiple-ascending-dose study in healthy participants. Diabetes Obes Metab. 2023. PMID 37344954. https://pubmed.ncbi.nlm.nih.gov/37344954/
- Orforglipron (LY3502970), a novel, oral non-peptide GLP-1 receptor agonist: a Phase 1b, multicentre, blinded, placebo-controlled, randomized, multiple-ascending-dose study in people with type 2 diabetes. Diabetes Obes Metab. 2023. PMID 37264711. https://pubmed.ncbi.nlm.nih.gov/37264711/
- Wharton S, Blevins T, Connery L, et al. Daily Oral GLP-1 Receptor Agonist Orforglipron for Adults with Obesity (Phase 2). N Engl J Med. 2023;389(10):877-888. PMID 37351564. DOI 10.1056/NEJMoa2302392. https://pubmed.ncbi.nlm.nih.gov/37351564/
- Frías JP, et al. Efficacy and safety of oral orforglipron in patients with type 2 diabetes: a multicentre, randomised, dose-response, phase 2 study. Lancet. 2023;402(10400):472-483. PMID 37369232. DOI 10.1016/S0140-6736(23)01302-8. https://pubmed.ncbi.nlm.nih.gov/37369232/
- Horn DB, et al. Orforglipron, an oral small-molecule GLP-1 receptor agonist, for the treatment of obesity in people with type 2 diabetes (ATTAIN-2): a phase 3, double-blind, randomised, multicentre, placebo-controlled trial. Lancet. 2025. DOI 10.1016/S0140-6736(25)02165-8. https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(25)02165-8/abstract
- Rosenstock J, et al. Orforglipron, an Oral Small-Molecule GLP-1 Receptor Agonist, in Early Type 2 Diabetes (ACHIEVE-1). N Engl J Med. 2025. DOI 10.1056/NEJMoa2505669. https://www.nejm.org/doi/full/10.1056/NEJMoa2505669
- ClinicalTrials.gov. A Study of Orforglipron (LY3502970) on Cardiovascular Outcomes in Adults With Atherosclerotic Cardiovascular Disease and/or Chronic Kidney Disease (ATTAIN-Outcomes). NCT07241390. https://clinicaltrials.gov/study/NCT07241390
- Orforglipron for maintenance of body weight reduction: the double-blind, randomized phase 3b ATTAIN-MAINTAIN trial. Nat Med. 2026. DOI 10.1038/s41591-026-04386-7. https://www.nature.com/articles/s41591-026-04386-7
Educational and research-use disclaimer: This article is provided solely for scientific and educational purposes and is not medical advice. Orforglipron (brand name Foundayo) was approved by the U.S. FDA on April 1, 2026 for chronic weight management in adults with obesity or overweight with a weight-related condition; as of mid-2026 it was not approved for type 2 diabetes, and its long-term (multi-year) durability and cardiovascular-outcome effects had not yet been established, with the relevant trials ongoing. Weight-loss figures cited are trial averages over defined periods and do not predict individual results. Orforglipron should be used only under the supervision of a qualified healthcare professional and in accordance with its approved labeling. Readers should consult a clinician before making any treatment decisions.