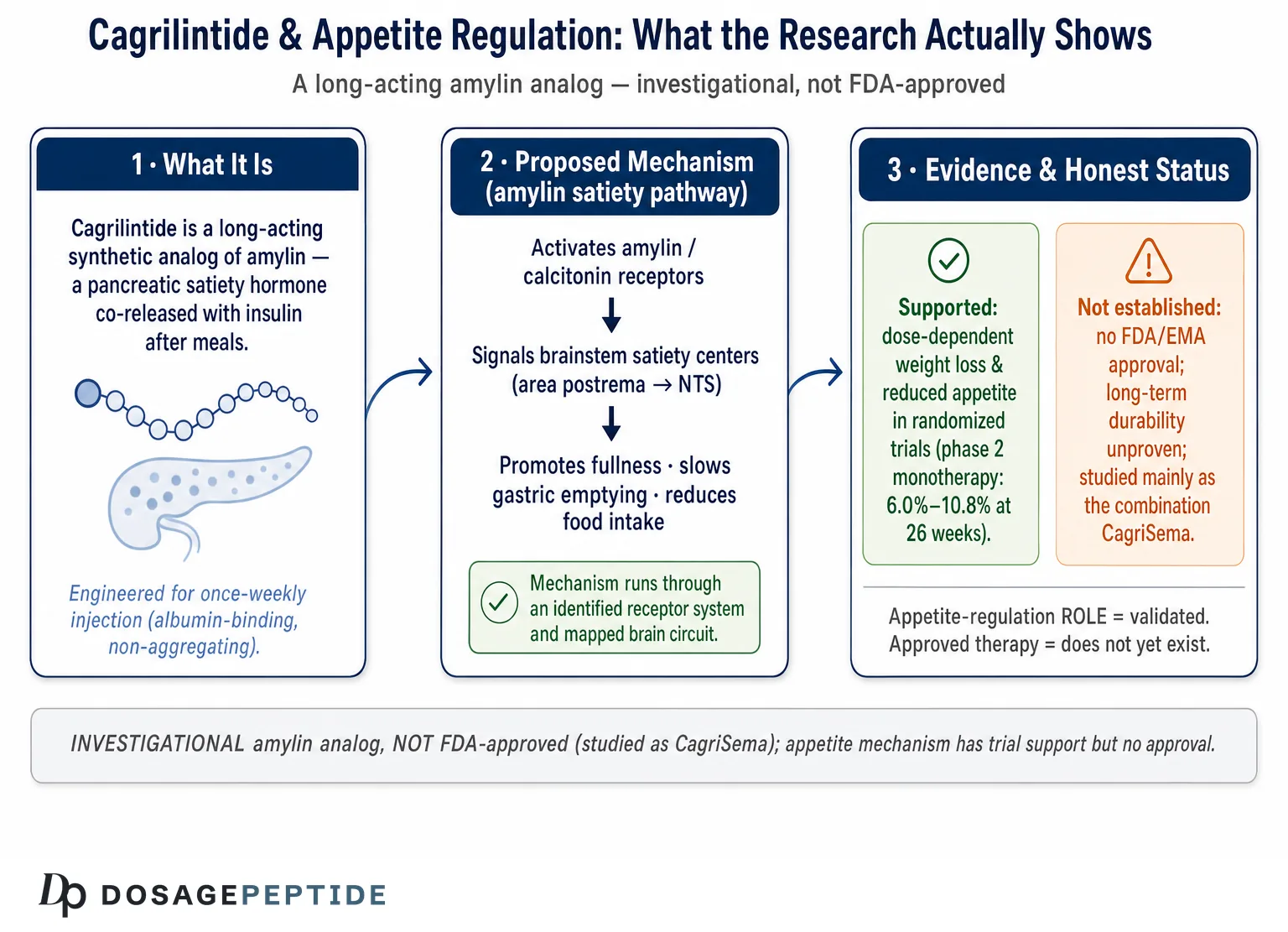
The question in the title is unusually well-posed, because it asks about a role and a mechanism rather than about a finished therapy. That distinction matters. If the question were “Is cagrilintide an approved appetite-suppressing medicine?” the honest answer would be a flat no. But the appetite-regulation question is narrower and, as it happens, far better supported: cagrilintide is a long-acting synthetic analog of amylin, a pancreatic satiety hormone whose role in appetite control is one of the more thoroughly mapped stories in metabolic physiology.1 On that specific point — whether the compound engages the body’s own appetite-regulating circuitry — the research does, in fact, provide substantial validation. Where the honesty is required is in the gap between “engages appetite circuits, produces dose-dependent weight loss in trials” and “is a proven, approved, durable treatment,” which it is not.5
So this article neither dismisses the premise nor inflates it. Unlike many research peptides whose appetite claims rest on rodent data and marketing copy, cagrilintide has been through a randomized, placebo-controlled and active-controlled phase 2 dose-finding trial in more than 700 people, a phase 1b combination study, a phase 2 diabetes trial, and a 68-week phase 3 program.5678 That is a genuine clinical evidence base, and it consistently points to a real, mechanism-consistent effect on appetite, satiety, and body weight. At the same time, cagrilintide is not FDA-approved for any indication; its most advanced development is as one half of a fixed-dose combination called CagriSema, paired with the GLP-1 analog semaglutide; and even that combination produced a phase 3 result that, while large in absolute terms, fell short of the market’s expectations and reopened questions about how much cagrilintide itself adds.9
The piece is written for researchers and scientifically literate readers who want an accurate map: what amylin biology actually is, how cagrilintide reproduces and extends it, what the human trials genuinely show about appetite and weight, where the combination story complicates the picture, how it compares with other appetite-acting agents, and what its regulatory status really is. Throughout, the guiding principle is calibration — crediting the strong mechanistic and trial support for an appetite-regulating role while refusing to let that slide into the unsupported claim that cagrilintide is an established therapy for obesity or any disease.
What Cagrilintide Is and Where It Came From
Cagrilintide (development codes AM833 and NNC0174-0833) is a long-acting, acylated synthetic analog of human amylin, engineered by Novo Nordisk for once-weekly subcutaneous administration.10 Native amylin is a 37-amino-acid peptide hormone with two properties that make it awkward as a drug: it is prone to self-aggregation into insoluble amyloid fibrils, and it has a very short circulating half-life. Cagrilintide was designed to solve both problems at once. Its sequence is modified to resist aggregation, and it carries a lipid side chain (a fatty-acid acylation) that binds reversibly to albumin in the bloodstream, dramatically prolonging its residence time so that a single weekly injection maintains sustained receptor engagement.10 This is the same albumin-binding strategy that gives semaglutide its once-weekly profile, which is part of why the two molecules were natural partners for a combination product.
The intellectual lineage runs back to pramlintide, the first amylin analog to reach the clinic. Pramlintide is a synthetic human-amylin analog with amino-acid substitutions (proline residues at positions 25, 28, and 29) that prevent fibril formation; it was approved in the United States in 2005 as a mealtime adjunct to insulin in type 1 and type 2 diabetes.4 Pramlintide validated the core idea that an amylin analog could safely reproduce amylin’s actions in humans — suppressing glucagon, slowing gastric emptying, and reducing food intake — and it produced modest but real weight loss (on the order of 1–2 kg) as a side effect of its glucose work.4 But pramlintide’s short half-life demanded injection with every meal, which capped its practicality as a weight-management tool. Cagrilintide can be read as the answer to a straightforward development question: what happens if you take amylin’s appetite biology, make it non-aggregating and long-acting enough for weekly dosing, and optimize it for body weight rather than mealtime glucose?3
It helps to keep three levels of this story distinct, because popular writing tends to collapse them. There is the native hormone (amylin/IAPP, co-secreted with insulin from pancreatic beta cells after meals); there is the proof-of-concept analog (pramlintide, short-acting, approved for diabetes); and there is the engineered long-acting analog (cagrilintide, investigational, built for weekly dosing and weight management). Each step preserves the underlying appetite biology while changing the pharmacology. When someone says “amylin controls appetite, therefore cagrilintide controls appetite,” the inference is actually reasonable here — unlike many peptide claims — precisely because cagrilintide was designed to retain that mechanism. The honest caveats live not in the mechanism but in the magnitude, durability, and regulatory status of the effect.
One more framing point deserves emphasis at the outset. The compound most people can actually buy or read about online as a “research chemical” is not a licensed medicine and is not the quality-controlled material used in Novo Nordisk’s trials. The clinical evidence discussed below was generated with pharmaceutical-grade cagrilintide under strict protocols; it does not automatically transfer to unregulated material of uncertain purity, and nothing here should be read as endorsing non-clinical human use. For orientation within the broader compound landscape, the site’s dosage index catalogs how amylin-class and incretin-class research compounds are typically distinguished.
Amylin: The Native Hormone Cagrilintide Was Built to Mimic
To judge whether cagrilintide has a legitimate appetite-regulating role, the starting point is the hormone it copies. Amylin, also called islet amyloid polypeptide (IAPP), is a 37-amino-acid peptide co-secreted with insulin from pancreatic beta cells in response to nutrient intake.1 Because it is released alongside insulin in roughly fixed proportion, amylin functions as a postprandial satiety and glucose-handling signal: as a meal is absorbed, amylin rises and helps tell the brain and gut that food has arrived and that intake can taper.2
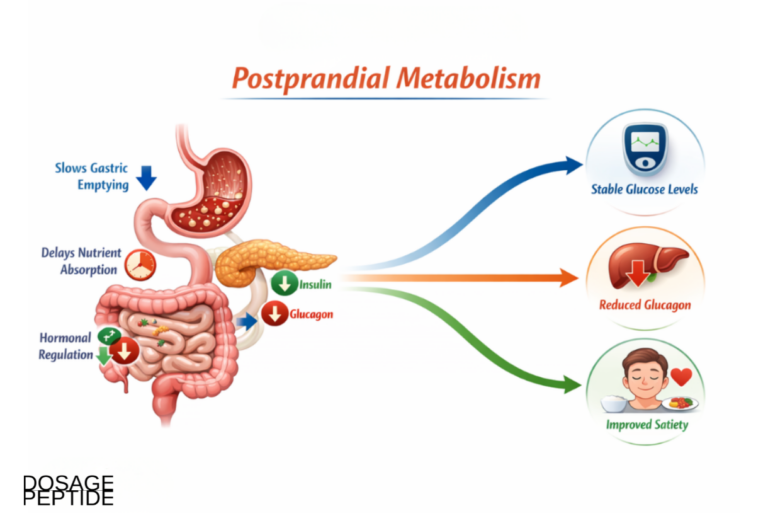
Amylin’s physiological actions cluster into three complementary effects, all of which bear on appetite and energy balance. First, it slows gastric emptying, so nutrients leave the stomach more gradually, blunting the post-meal glucose spike and prolonging the sense of fullness. Second, it suppresses inappropriate post-meal glucagon secretion, which limits the liver’s glucose output. Third, and most relevant here, it acts centrally to promote satiation — the process that brings a meal to an end — and to reduce subsequent food intake.12 In careful human and animal studies, amylin and its analogs reduce meal size and total caloric intake rather than simply making food unpalatable, which is the signature of a true satiety signal.4
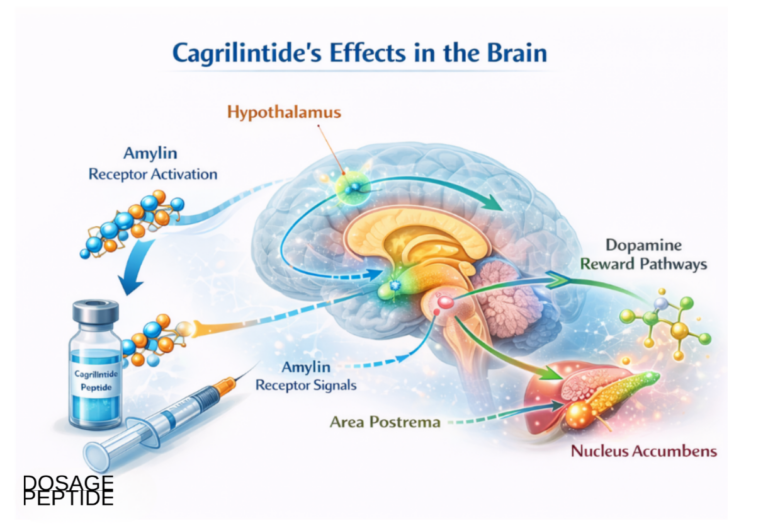
The central action has a well-defined anatomical home. Amylin’s primary appetite-relevant target is the area postrema, a small structure in the brainstem that sits outside the blood–brain barrier and is therefore directly accessible to circulating hormones.1 From the area postrema, satiety signals are relayed to the nucleus tractus solitarius and onward to hypothalamic and mesolimbic regions that govern both the homeostatic drive to eat and the hedonic, reward-related dimension of appetite.2 This dual reach — into both the “how hungry am I” system and the “how rewarding is this food” system — is one reason amylin analogs are attractive for weight management: they act on more than raw hunger.10
It is worth pausing on why amylin, specifically, is such a credible appetite target rather than just one more hormone in the crowded gut–brain field. Amylin is co-released with insulin in fixed proportion, which makes it a faithful real-time reporter of nutrient absorption rather than a slow or indirect signal; its principal central target sits outside the blood–brain barrier, so circulating analog can reach it without needing to cross into protected brain tissue; and its effect is on satiation and meal termination, the physiological lever most relevant to how much a person eats at a sitting.12 These are not incidental facts. They are precisely the properties a drug designer would want in an appetite-regulating hormone, and they are why the amylin pathway has drawn serious pharmaceutical investment rather than remaining a physiological curiosity. The native system also has a built-in safety logic: because amylin normally rises and falls with meals, chronically activating its receptor with a long-acting analog is, in effect, an exaggeration of an existing physiological signal rather than the introduction of a foreign one — part of why the class has been reasonably tolerable in trials.
At the molecular level, the amylin receptor is not a single protein but a family. The core is the calcitonin receptor (a class B G-protein-coupled receptor), which acquires amylin selectivity when it associates with one of three receptor activity-modifying proteins (RAMP1, RAMP2, or RAMP3), generating the AMY1, AMY2, and AMY3 receptor subtypes.1 This RAMP-dependent architecture matters for drug design because different analogs can engage the subtypes with different profiles, and it explains why some newer molecules are described as “selective” amylin agonists while cagrilintide is characterized as a non-selective amylin-receptor and calcitonin-receptor agonist.23 The pharmacological point for a reader assessing the title question is that amylin’s appetite effects run through a genuine, identified receptor system with a mapped central circuit — not a vague or hypothesized pathway. That is the foundation on which cagrilintide’s appetite claim legitimately rests.
How Cagrilintide Engages Appetite Circuits
Cagrilintide reproduces amylin’s core pharmacology and, because it is long-acting, sustains it continuously rather than in mealtime pulses. As a non-selective agonist at the amylin and calcitonin receptors, it activates the same area-postrema and nucleus-tractus-solitarius satiety relay that native amylin uses, driving reductions in food intake and body weight in preclinical models and in humans.310 The pharmacodynamic fingerprint seen in trials — reduced appetite ratings, earlier satiation, lower energy intake, and dose-dependent weight loss — is exactly what amylin biology predicts, which is a meaningful form of mechanistic validation: the observed clinical effect matches the proposed mechanism rather than contradicting it.5
Several features distinguish cagrilintide’s engagement of appetite circuits from that of the native hormone and from short-acting pramlintide. The table below summarizes the pharmacodynamic actions most relevant to appetite regulation.
| Action | How it affects appetite / energy balance | Evidence context |
|---|---|---|
| Central satiety signaling (area postrema → NTS → hypothalamus) | Promotes satiation, reduces meal size and total intake | Amylin physiology; reproduced by analogs12 |
| Action on hedonic / reward circuits | May reduce food reward and cravings, not just hunger | Amylin engages mesolimbic regions10 |
| Slowed gastric emptying | Prolongs fullness, blunts post-meal glucose rise | Core amylin action1 |
| Glucagon suppression (postprandial) | Improves glucose handling; indirect metabolic benefit | Core amylin action; relevant in T2D trial7 |
| Long half-life (albumin binding) | Continuous once-weekly signaling vs mealtime pulses | Acylation design of cagrilintide10 |
| Dose-dependent weight loss | 6.0%–10.8% at 26 weeks across 0.3–4.5 mg | Phase 2 monotherapy trial5 |
There is also a mechanistically interesting rationale for pairing cagrilintide with a GLP-1 agonist that goes beyond simply stacking two appetite drugs. Amylin and GLP-1 act through largely distinct receptors and partly distinct brain circuits, so their satiety effects can be additive or complementary rather than redundant.8 More provocatively, preclinical work has suggested that amylin signaling can restore leptin sensitivity, potentially counteracting the leptin resistance that undermines many weight-loss efforts — a proposed synergy that helped motivate the CagriSema program, though its clinical significance in humans remains an open question rather than a settled fact.3 For readers comparing this satiety-based approach with the incretin mechanism, the site’s explainer on how tirzepatide works lays out the GLP-1/GIP side of the appetite-regulation story.
The honest mechanistic summary is therefore strong but bounded. Cagrilintide has a clearly identified receptor system, a mapped central appetite circuit, and a pharmacodynamic profile in humans that matches its proposed mechanism. That is a far more validated appetite story than most research peptides can claim. What the mechanism cannot tell you is how large, durable, or clinically meaningful the effect is in real populations over years — questions only trials and long-term data can answer, and to those we now turn.
The Phase 2 Monotherapy Evidence: Cagrilintide Alone
The single most important study for the title question is the phase 2 dose-finding trial of cagrilintide monotherapy, published in The Lancet in 2021 by Lau and colleagues.5 It is the clearest look at what cagrilintide does to appetite and weight on its own, without a GLP-1 partner confounding the picture. The design was rigorous: a multicentre, randomized, double-blind, placebo-controlled and active-controlled trial enrolling 706 participants with overweight or obesity (and without type 2 diabetes) across 57 sites in ten countries. Participants received once-weekly subcutaneous cagrilintide at 0.3, 0.6, 1.2, 2.4, or 4.5 mg; once-daily liraglutide 3.0 mg (an approved GLP-1 weight-management drug) as an active comparator; or placebo, over a 26-week treatment period that included up to 6 weeks of dose escalation, all on a background of diet and exercise counseling.5
The results were consistent and dose-dependent. Every cagrilintide dose produced greater weight loss than placebo, with mean reductions ranging from 6.0% at the lowest dose to 10.8% at 4.5 mg, versus roughly 3.0% for placebo.5 Crucially for an appetite claim, the highest cagrilintide dose also numerically outperformed the active comparator: cagrilintide 4.5 mg produced about 10.8% weight loss (approximately 11.5 kg) compared with about 9.0% (approximately 9.6 kg) for liraglutide 3.0 mg, a statistically significant difference.5 Waist circumference, a marker of visceral fat, fell in parallel. This is the crux of the validation: an amylin analog, acting on satiety circuits, matched or beat an established GLP-1 appetite drug over six months.
Several honest qualifications keep this in proportion. The trial was 26 weeks — a medium-term study, not a demonstration of durability. It enrolled people without diabetes, so its findings do not automatically extend to diabetic populations, whose weight response to these agents tends to be blunted. The comparator, liraglutide, is itself a first-generation weight drug now superseded in potency by semaglutide and tirzepatide, so “beat liraglutide” is a real but modest bar. And gastrointestinal side effects — nausea in particular — were common, occurring in roughly 20% to 47% of cagrilintide-treated participants depending on dose, versus about 18% on placebo.5 Still, within those bounds, the phase 2 monotherapy trial is exactly the kind of evidence a rigorous reader should want: a large, well-controlled human study showing that cagrilintide, on its own, regulates appetite strongly enough to drive clinically meaningful, dose-dependent weight loss.
It is also worth being precise about what “appetite regulation” means in a trial like this, because the phrase can be read too loosely. The phase 2 study did not merely report that people weighed less; the weight loss was accompanied by the expected downstream signatures of genuine appetite suppression — reduced energy intake and the class-typical gastrointestinal effects that track with slowed gastric emptying and central satiety signaling.5 In other words, the compound did not produce weight loss through some unrelated route such as malabsorption or increased energy expenditure; it produced it by making participants eat less, which is exactly what an amylin mechanism predicts. That coherence between the proposed mechanism and the observed clinical and side-effect profile is a stronger form of validation than the weight number alone, because it links the outcome to the biology rather than leaving the two merely correlated. A skeptic can still ask how durable and how large the effect is — those are fair questions — but the claim that cagrilintide acts on appetite is about as well supported as such claims get for an investigational peptide.
An accompanying commentary in the same issue of The Lancet underscored both the promise and the caution, noting that a long-acting amylin analog represented a genuinely novel mechanism for weight reduction while emphasizing that longer and larger trials would be needed to establish durability and safety.11 That balance — real novelty, incomplete proof — remains the fair reading years later.
The Combination Story: CagriSema and Why It Complicates the Picture
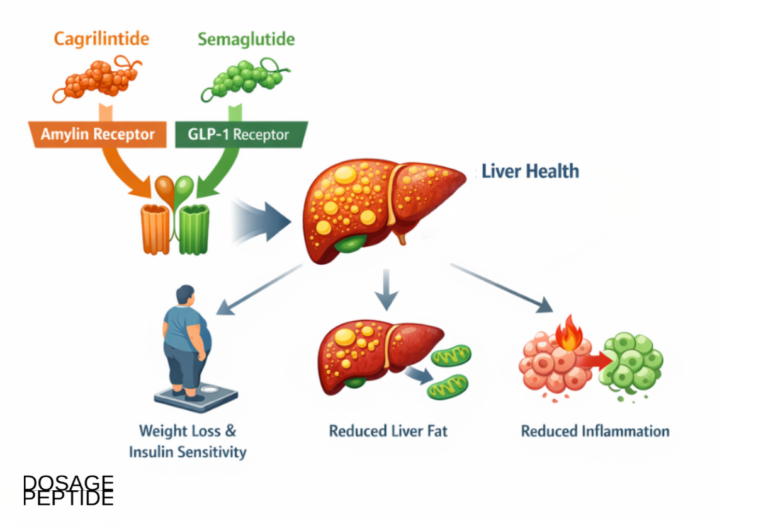
In practice, cagrilintide’s clinical future has been pursued mainly in combination with semaglutide, as the fixed-dose product CagriSema (cagrilintide 2.4 mg plus semaglutide 2.4 mg, once weekly). This makes the combination trials central to understanding the compound — but it also complicates any attempt to isolate cagrilintide’s own appetite-regulating contribution, because most of the headline data blend two mechanisms.
The foundation was a phase 1b trial by Enebo and colleagues, published in The Lancet in 2021, which tested multiple ascending doses of cagrilintide added to semaglutide 2.4 mg in people with overweight or obesity.6 Its primary purpose was safety and pharmacokinetics, and it delivered on both: co-administration was well tolerated with an acceptable safety profile and no unexpected pharmacokinetic interaction. It also produced a striking efficacy signal, with mean weight reductions at 20 weeks reaching roughly 15.7% to 17.1% at the higher cagrilintide doses added to semaglutide.6 Those numbers generated considerable excitement, because they suggested the combination might push weight loss into a range previously associated with bariatric surgery.
Next came a phase 2 trial in type 2 diabetes, published by Frias and colleagues in The Lancet in 2023, a 32-week study comparing coadministered cagrilintide 2.4 mg plus semaglutide 2.4 mg against each agent alone.7 The combination produced significantly greater weight loss and improved glucose control (HbA1c) than either component by itself, supporting the additive-mechanism rationale in a diabetic population where weight responses are typically harder to achieve.7 For readers interested in the metabolic-disease dimension specifically, the site examines related questions in its pieces on cagrilintide and diabetes prevention and on cagrilintide safety in chronic kidney disease.
The decisive test was the phase 3 REDEFINE 1 trial, a 68-week, double-blind, placebo- and active-controlled study of once-weekly CagriSema versus its individual components and placebo in 3,417 adults with obesity or overweight (with a weight-related complication) and without type 2 diabetes, published in the New England Journal of Medicine in 2025.8 On the trial-product estimand (which estimates the effect assuming full adherence), CagriSema achieved a mean weight loss of 22.7%, with 40.4% of participants losing at least 25% of body weight and 23.1% losing at least 30%.8 On the treatment-policy estimand (the effect regardless of adherence), the reduction was 20.4%.9 By any historical standard for a pharmacological weight-loss agent, these are large numbers.
And yet REDEFINE 1 is also a cautionary tale about hype. Novo Nordisk and many analysts had anticipated weight loss approaching or exceeding 25%, and when the December 2024 topline landed at 22.7% (trial-product) and 20.4% (treatment-policy), the company’s share price fell sharply — by more than 20% in a single session — despite the trial meeting its primary endpoint.9 The market’s disappointment is not, in itself, a scientific verdict; a 20%-plus weight loss is clinically substantial. But it is a useful corrective against the earlier phase 1b exuberance, and it feeds directly into the harder question this article must confront: how much of CagriSema’s effect actually comes from cagrilintide’s appetite mechanism, as opposed to from semaglutide?
The phase 3 program did not stop at a single population. A companion pivotal trial, REDEFINE 2, extended the CagriSema evaluation to adults living with both obesity or overweight and type 2 diabetes — a group that is clinically important precisely because its weight response to appetite-acting drugs is typically blunted relative to people without diabetes, so it is a harder test of any satiety-based mechanism.13 Published in the New England Journal of Medicine in 2025 alongside REDEFINE 1, it found that once-weekly cagrilintide–semaglutide produced significantly greater weight loss than placebo in this diabetic population, with the magnitude — as the diabetes literature would predict — more modest than the 20%-plus seen in the non-diabetic REDEFINE 1 cohort.13 The honest reading of the two trials together is that the combination’s appetite effect is real and reproducible across populations, but that its size is context-dependent rather than fixed, and that a diabetic metabolism imposes a ceiling on any amylin-plus-incretin approach just as it does on the incretin drugs alone. For a fuller treatment of why diabetic weight responses differ, the site’s discussion of incretin therapy in type 2 diabetes lays out the relevant physiology.
Isolating Cagrilintide’s Own Contribution
Because REDEFINE 1 included monotherapy arms, it offers the cleanest available answer to that question — and the answer is genuinely instructive, in a way that tempers rather than inflates cagrilintide’s standing. On the treatment-policy estimand, the four arms produced the following approximate weight reductions at 68 weeks: CagriSema 20.4%, semaglutide 2.4 mg alone 14.9%, cagrilintide 2.4 mg alone 11.5%, and placebo 3.0%.9
| REDEFINE 1 arm (68 weeks, treatment-policy estimand) | Mean weight loss | What it tells us |
|---|---|---|
| Placebo + lifestyle | ~3.0%9 | Background lifestyle effect |
| Cagrilintide 2.4 mg alone | ~11.5%9 | Amylin appetite mechanism, isolated |
| Semaglutide 2.4 mg alone | ~14.9%9 | GLP-1 appetite mechanism, isolated |
| CagriSema (both, 2.4/2.4 mg) | ~20.4%9 | Combination; additive but not fully so |
Three honest conclusions follow. First, cagrilintide monotherapy at 2.4 mg produced a real, substantial 11.5% weight loss over 68 weeks — on its own, a clinically meaningful appetite-driven effect that firmly validates the compound’s role in appetite regulation. This is not a marginal or hypothetical signal; it is a large, placebo-controlled phase 3 result. Second, over this longer horizon and in this population, cagrilintide alone was somewhat less potent than semaglutide alone (11.5% vs 14.9%), which reframes the phase 2 story where cagrilintide 4.5 mg had beaten liraglutide; against the more potent semaglutide at the 2.4 mg dose, amylin agonism did not lead. Third, the combination (20.4%) exceeded either component but by less than a simple sum of the two would predict (11.5% + 14.9% would be 26.4% if perfectly additive), indicating partial, overlapping rather than fully independent mechanisms.9
This is exactly the kind of nuance that separates honest analysis from marketing. The appetite-regulation role is validated — cagrilintide alone drives double-digit weight loss through amylin satiety signaling. But the compound is not a miracle standalone agent, its incremental value on top of a potent GLP-1 drug is real but sub-additive, and the disappointment around REDEFINE 1 stemmed precisely from the hope that the two mechanisms would be more independent than they turned out to be. A researcher can hold both truths at once: cagrilintide meaningfully regulates appetite, and it is not obviously superior to, or fully additive with, the incretin agents that dominate the field.
How Cagrilintide Compares With Other Appetite-Regulating Agents
Placing cagrilintide beside other agents that act on appetite clarifies where its amylin mechanism sits in a crowded field. The comparison is not a ranking — head-to-head data are limited — but a map of mechanisms and evidence levels.
| Agent / class | Primary appetite mechanism | Evidence & status |
|---|---|---|
| Cagrilintide (long-acting amylin analog) | Amylin/calcitonin receptor agonism; area-postrema satiety, slowed gastric emptying, hedonic effects | Phase 2 monotherapy (10.8% at 26 wk) and phase 3 as CagriSema; investigational, not approved58 |
| Pramlintide (short-acting amylin analog) | Same amylin mechanism; mealtime dosing | FDA-approved 2005 for diabetes; modest weight loss (~1–2 kg)4 |
| Semaglutide (GLP-1 agonist) | GLP-1 receptor; hypothalamic/brainstem appetite suppression, slowed gastric emptying | Approved for obesity; ~15% weight loss in trials9 |
| Tirzepatide (GIP/GLP-1 co-agonist) | Dual incretin appetite suppression | Approved for T2D and obesity; ~20%+ in trials |
| Eloralintide (selective amylin agonist) | Selective amylin-receptor agonism | Phase 2 (48-week) reported; investigational12 |
| CagriSema (amylin + GLP-1) | Combined amylin and GLP-1 satiety signaling | Phase 3 REDEFINE (20.4%–22.7%); investigational, under regulatory review89 |
A few patterns stand out. Amylin agonism is a validated appetite mechanism — pramlintide proved it in humans two decades ago, and cagrilintide has scaled it up into clinically substantial weight loss.45 The incretin agents (semaglutide, tirzepatide) currently set the potency benchmark, and amylin agents are being positioned largely as partners or alternatives rather than clear front-runners. The emergence of newer selective amylin agonists such as eloralintide, and of amylin/GLP-1 unimolecular co-agonists such as amycretin, signals that the amylin appetite pathway is now a major axis of obesity drug development in its own right, not a footnote.12 Cagrilintide is best understood as the most clinically advanced dedicated long-acting amylin analog to date — a genuine proof that the mechanism works at scale, even as the field races to refine it.
For readers tracing the broader arc of this drug class, the site’s overview of retatrutide and multi-receptor agonism situates amylin agents within the wider evolution of appetite-targeting peptide therapeutics.
Dosing and Titration in a Research Context
Because cagrilintide is investigational and not approved, there is no established therapeutic dose for human use; what exists is the dosing scaffold used in its clinical trials, which is informative purely as a description of how the compound has been studied — not as guidance for use. The pattern across the program is consistent and worth understanding for that reason.
Cagrilintide was administered once weekly by subcutaneous injection, reflecting its long, albumin-mediated half-life.10 Trials used gradual dose escalation rather than starting at the target dose, because — as with GLP-1 agonists — slow titration is the principal strategy for limiting the nausea and other gastrointestinal effects that accompany rapid up-dosing. In the phase 2 monotherapy trial, doses spanned 0.3 mg to 4.5 mg weekly, with an escalation period of up to six weeks before participants reached their assigned maintenance dose.5 In the CagriSema program, the fixed target was cagrilintide 2.4 mg paired with semaglutide 2.4 mg, again reached through stepwise titration over several weeks.8
The general principles visible in the trial design — once-weekly administration, mandatory gradual escalation, a defined maintenance dose, and dose-dependent both efficacy and side effects — are the clinically meaningful takeaways, and they mirror the handling logic of the incretin class. As a lyophilized peptide in research settings, cagrilintide follows the same reconstitution and handling conventions as other injectable research peptides; the site’s peptide reconstitution guide explains the underlying sterile-technique and concentration arithmetic in general educational terms. It bears repeating that none of this constitutes a recommendation for human use of a compound that no regulator has approved, and that unregulated “research” material carries purity and sterility risks entirely separate from the molecule’s intrinsic pharmacology.
Safety and Tolerability
Across its trial program, cagrilintide’s safety profile has been broadly consistent with what the amylin and incretin classes lead one to expect: dominated by gastrointestinal effects, generally mild to moderate, and largely manageable with titration — but characterized over months, not years, and in trial populations rather than the general public.
Gastrointestinal adverse events are the headline. In the phase 2 monotherapy trial, nausea was the most common event, reported in roughly 20% to 47% of cagrilintide participants across the dose range, compared with about 18% on placebo, alongside vomiting, constipation, and diarrhea at lower frequencies.5 These effects were generally dose-related, transient, and most pronounced during escalation — the same pattern that makes slow titration the standard mitigation. In the phase 1b and phase 3 combination studies, the overall tolerability of CagriSema was described as acceptable and consistent with the GLP-1 class, again with gastrointestinal symptoms predominating.68
Several considerations temper any reassurance:
- Duration. The longest pivotal exposure is 68 weeks. Obesity is a chronic condition typically requiring years of treatment; the very-long-term safety of cagrilintide is simply not yet characterized.
- Population. Trial participants were selected and monitored. Effects in unmonitored real-world use, in older or medically complex people, or in those with conditions such as advanced kidney disease may differ — a reason the site addresses cagrilintide in chronic kidney disease separately.
- Combination confounding. Much of the safety data comes from CagriSema, where cagrilintide’s individual contribution to any adverse event can be hard to separate from semaglutide’s.
- Amylin-specific questions. Because native amylin aggregates into amyloid, engineered analogs are designed to avoid fibril formation; cagrilintide is built to be non-aggregating, but long-term immunogenicity and injection-site reactions remain standard peptide-drug concerns to monitor.3
- Unregulated material. Any safety profile established in trials applies to pharmaceutical-grade compound; it does not transfer to research-chemical material of unknown purity, endotoxin content, or identity.
The reasonable reading is that cagrilintide has shown an acceptable, class-typical short-to-medium-term safety profile in controlled trials, with gastrointestinal tolerability as the main practical limitation, and that this is genuinely encouraging without being a guarantee of long-term safety in the broad populations who would ultimately use an obesity drug.
Durability, Weight Regain, and the Limits of the Appetite Model
Even granting a validated appetite mechanism and strong trial weight loss, an honest appraisal has to confront the limits that apply to every appetite-suppressing weight drug — limits that cagrilintide shares and that the appetite model itself helps explain.
The first is durability. Agents that produce weight loss by suppressing appetite tend to work only while they are taken. When GLP-1 agonists are discontinued, substantial weight regain is the norm, because the underlying biology that defends a higher body-weight set-point reasserts itself once the pharmacological satiety signal is withdrawn. There is no reason to expect cagrilintide to be exempt; an amylin-based satiety signal, like a GLP-1 one, is a continuous input, and removing it should be expected to relax the appetite constraint it imposes. The trials to date, running to 68 weeks, do not establish what happens over many years or after discontinuation, and this is one of the most important open questions for the entire class, cagrilintide included.11
The second is the sub-additivity already seen in REDEFINE 1. If amylin and GLP-1 appetite pathways were fully independent, combining them should approach the sum of their individual effects; instead the combination delivered meaningfully less than that sum, implying overlapping downstream circuitry.9 This is scientifically interesting — it suggests a shared satiety bottleneck — but it also caps how far stacking appetite mechanisms can go, and it is part of why the field is now exploring co-agonists and entirely different axes rather than simply adding more satiety signals.
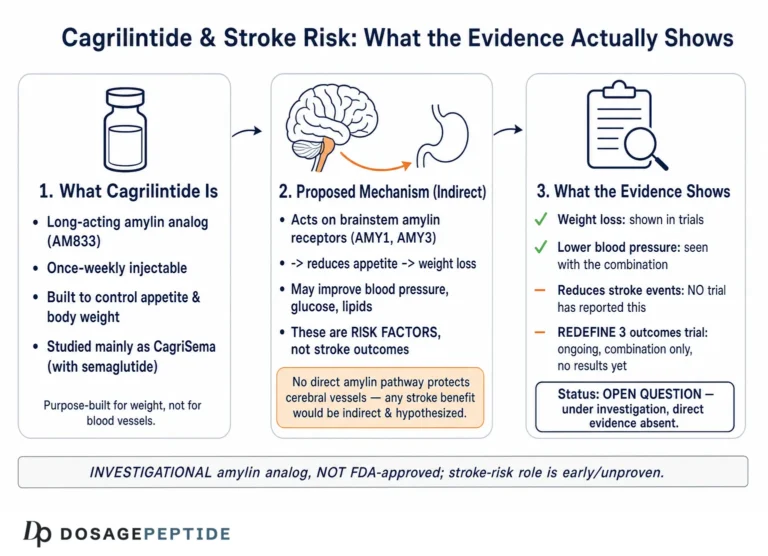
The third is the gap between weight loss and hard clinical outcomes. Weight reduction is a surrogate; what ultimately matters for an obesity therapy is whether it improves cardiovascular events, diabetes incidence, mortality, and quality of life over the long run. Those outcome data are still maturing for CagriSema and are essentially absent for cagrilintide monotherapy. Questions such as whether the compound’s effects translate into reduced stroke risk remain genuinely open and should not be assumed from weight loss alone.
Finally, the appetite model has an inherent ceiling: it works by making people eat less, which means tolerability, adherence, and the body’s counter-regulatory responses (increased hunger signaling, reduced energy expenditure with weight loss) all push back. Cagrilintide is a powerful, mechanism-validated way to lower the appetite set-point, but it operates inside these same constraints that limit every drug in the category. Recognizing that is not skepticism about the mechanism — the mechanism is real — it is realism about what any appetite-regulating agent can deliver.
Regulatory Status
The regulatory picture is straightforward but frequently misstated, so precision matters.
Cagrilintide is not approved as a drug for any indication by the U.S. Food and Drug Administration, the European Medicines Agency, or any comparable regulator. It is an investigational compound. Its appetite-regulating and weight-loss effects are supported by peer-reviewed phase 2 and phase 3 data, but supportive trial data are not the same as marketing authorization, and no approved product containing cagrilintide as a standalone agent exists.510
The most advanced regulatory pathway is for CagriSema, the fixed-dose cagrilintide/semaglutide combination, which completed its pivotal REDEFINE phase 3 program and has been the subject of regulatory filings for obesity. As of this writing, CagriSema’s approval status is pending regulatory decisions; a positive phase 3 result initiates, but does not equal, approval. Even if CagriSema is ultimately approved, that authorization would be for the specific combination product at studied doses, not a general endorsement of cagrilintide for any use.89
The approved precedent in the amylin class is pramlintide, not cagrilintide. Pramlintide’s 2005 approval was for glycemic control as a mealtime adjunct to insulin in diabetes, with weight loss as a secondary effect — a narrower indication than obesity and a different molecule.4 It establishes that amylin analogs can be approvable and reasonably safe, but it does not confer any regulatory status on cagrilintide.
A recurring source of confusion deserves explicit correction: the existence of impressive trial numbers, or of a compound’s availability from “research” suppliers, is routinely misrepresented online as though it implied legitimacy or approval. It does not. Cagrilintide’s genuinely strong appetite-regulation evidence is a scientific finding about a mechanism; it says nothing about the safety, purity, or legality of unregulated material, and it does not authorize human use outside a clinical trial. For any legitimate exploration of cagrilintide, the appropriate route is participation in or conduct of properly authorized research under regulatory oversight. Readers wanting to define the surrounding terminology precisely can consult the site’s peptide glossary.
The regulatory synthesis, then, mirrors the scientific one: the appetite-regulation role is well supported by real trials, while cagrilintide as an approved therapy does not yet exist — it is an investigational compound whose most likely route to market is as one component of a combination product still awaiting regulatory decisions.
Frequently Asked Questions
Does scientific research support cagrilintide’s role in appetite regulation?
Yes, on the specific question of mechanism and appetite effect, the support is substantial. Cagrilintide is a long-acting analog of amylin, a native satiety hormone that acts on brainstem appetite circuits (the area postrema and nucleus tractus solitarius), slows gastric emptying, and reduces food intake.12 In a randomized phase 2 trial of 706 people, cagrilintide monotherapy produced dose-dependent weight loss of 6.0% to 10.8% over 26 weeks, and in the phase 3 REDEFINE 1 trial cagrilintide 2.4 mg alone produced about 11.5% weight loss over 68 weeks.59 The appetite-regulating role is validated; what is not established is that cagrilintide is an approved or long-term-proven therapy.
Is cagrilintide FDA-approved?
No. Cagrilintide is investigational and not approved by the FDA, EMA, or any comparable regulator for obesity or any other indication.10 Its most advanced development is as part of the fixed-dose combination CagriSema (with semaglutide), which completed phase 3 trials and has been filed for regulatory review but is not, as of this writing, an approved product either. The only approved amylin analog is pramlintide, a different, short-acting molecule approved for diabetes.4
How does cagrilintide differ from semaglutide or tirzepatide?
They act through different receptor systems. Cagrilintide is an amylin-receptor agonist; semaglutide is a GLP-1 receptor agonist; tirzepatide is a dual GIP/GLP-1 agonist. All three suppress appetite and slow gastric emptying, but via distinct pathways, which is why cagrilintide and semaglutide were combined to see whether their effects would add.8 In head-to-head phase 3 data, semaglutide 2.4 mg alone (14.9%) outperformed cagrilintide 2.4 mg alone (11.5%) over 68 weeks, and the combination (20.4%) exceeded either but by less than a simple sum.9
How much weight did cagrilintide produce on its own?
In phase 2 monotherapy, up to 10.8% mean weight loss at the 4.5 mg dose over 26 weeks, exceeding the liraglutide comparator.5 In phase 3 REDEFINE 1, cagrilintide 2.4 mg alone produced about 11.5% over 68 weeks — a real, clinically meaningful, placebo-controlled result that validates the appetite mechanism, though it trailed semaglutide in that trial.9
Why did Novo Nordisk’s stock drop if REDEFINE 1 succeeded?
The trial met its primary endpoint with a large 20.4% to 22.7% weight loss, but the market had expected results approaching or exceeding 25%, so the outcome was read as a disappointment relative to expectations rather than a failure.9 This gap between strong absolute results and unmet expectations is a useful reminder to judge the science on its own terms, not on share-price reactions.
Is the appetite effect durable, or does weight come back?
Durability beyond 68 weeks and after discontinuation has not been established for cagrilintide. Because appetite-suppressing weight drugs generally work only while taken — with substantial weight regain common after stopping GLP-1 agonists — there is no reason to assume cagrilintide would be an exception.11 This is one of the most important open questions for the entire class.
What are the main side effects seen in trials?
Predominantly gastrointestinal: nausea was the most common event, reported in roughly 20% to 47% of cagrilintide-treated participants in the phase 2 trial depending on dose, alongside vomiting, constipation, and diarrhea, generally mild to moderate, dose-related, and most pronounced during dose escalation.5 Slow titration is the standard way to limit them. Long-term safety over years is not yet characterized.
Is cagrilintide the same as CagriSema?
No. Cagrilintide is the single amylin-analog compound. CagriSema is the fixed-dose combination product that pairs cagrilintide 2.4 mg with the GLP-1 agonist semaglutide 2.4 mg in one weekly injection.8 Most late-stage clinical data describe CagriSema, which blends two appetite mechanisms; the phase 2 monotherapy and the REDEFINE 1 monotherapy arm are the clearest windows onto cagrilintide’s effect by itself.
Can I use research-grade cagrilintide for weight loss?
This article does not endorse that, and it would be outside any approved or studied use. Cagrilintide is investigational; material sold as a “research chemical” is not the quality-controlled compound used in trials and carries purity, sterility, and identity risks that are independent of the molecule’s pharmacology. Any legitimate use belongs within authorized clinical research under medical and regulatory oversight.
References
- Hay DL, Chen S, Lutz TA, Parkes DG, Roth JD. Amylin: Pharmacology, Physiology, and Clinical Potential. Pharmacol Rev. 2015;67(3):564-600. PMID: 26071095. https://pubmed.ncbi.nlm.nih.gov/26071095/
- Muhammad T, Pastore SF, Good K, Yu WH, Vincent JB. The role of amylin, a gut–brain axis hormone, in metabolic and neurological disorders. FASEB BioAdv. 2025;7(3):e1480. PMID: 40060942. PMCID: PMC11886606. https://pmc.ncbi.nlm.nih.gov/articles/PMC11886606/
- Dehestani B, Stratford NRS, le Roux CW. Amylin as a Future Obesity Treatment. J Obes Metab Syndr. 2021;30(4):320-325. PMID: 34929674. PMCID: PMC8735818. https://pmc.ncbi.nlm.nih.gov/articles/PMC8735818/
- Ryan G, Briscoe TA, Jobe L. Review of pramlintide as adjunctive therapy in treatment of type 1 and type 2 diabetes. Drug Des Devel Ther. 2009;2:203-214. PMID: 19920907. PMCID: PMC2761191. https://pmc.ncbi.nlm.nih.gov/articles/PMC2761191/
- Lau DCW, Erichsen L, Francisco AM, et al. Once-weekly cagrilintide for weight management in people with overweight and obesity: a multicentre, randomised, double-blind, placebo-controlled and active-controlled, dose-finding phase 2 trial. Lancet. 2021;398(10317):2160-2172. PMID: 34798060. https://pubmed.ncbi.nlm.nih.gov/34798060/
- Enebo LB, Berthelsen KK, Kankam M, et al. Safety, tolerability, pharmacokinetics, and pharmacodynamics of concomitant administration of multiple doses of cagrilintide with semaglutide 2·4 mg for weight management: a randomised, controlled, phase 1b trial. Lancet. 2021;397(10286):1736-1748. PMID: 33894838. https://pubmed.ncbi.nlm.nih.gov/33894838/
- Frias JP, Deenadayalan S, Erichsen L, et al. Efficacy and safety of co-administered once-weekly cagrilintide 2·4 mg with once-weekly semaglutide 2·4 mg in type 2 diabetes: a multicentre, randomised, double-blind, active-controlled, phase 2 trial. Lancet. 2023;402(10403):720-730. PMID: 37364590. https://pubmed.ncbi.nlm.nih.gov/37364590/
- Garvey WT, Blüher M, Contreras C, et al. Coadministered Cagrilintide and Semaglutide in Adults with Overweight or Obesity (REDEFINE 1). N Engl J Med. 2025. DOI: 10.1056/NEJMoa2502081. https://www.nejm.org/doi/full/10.1056/NEJMoa2502081
- Novo Nordisk A/S. CagriSema demonstrates superior weight loss in adults with obesity or overweight in the REDEFINE 1 trial. Company announcement, 20 December 2024. https://www.globenewswire.com/news-release/2024/12/20/3000444/0/en/Novo-Nordisk-A-S-CagriSema-demonstrates-superior-weight-loss-in-adults-with-obesity-or-overweight-in-the-REDEFINE-1-trial.html
- D’Ascanio AM, Mullally JA, Frishman WH. Cagrilintide: A Long-Acting Amylin Analog for the Treatment of Obesity. Cardiol Rev. 2024;32(1):83-90. PMID: 36883831. https://pubmed.ncbi.nlm.nih.gov/36883831/
- Gadde KM, Allison DB. Long-acting amylin analogue for weight reduction. Lancet. 2021;398(10317):2132-2134. PMID: 34798059. https://pubmed.ncbi.nlm.nih.gov/34798059/
- Eloralintide, a selective amylin receptor agonist for the treatment of obesity: a 48-week phase 2, multicentre, double-blind, randomised, placebo-controlled trial. Lancet. 2025. DOI: 10.1016/S0140-6736(25)02155-5. https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(25)02155-5/abstract
- Davies MJ, Blüher M, Christensen SB, et al. Cagrilintide–Semaglutide in Adults with Overweight or Obesity and Type 2 Diabetes (REDEFINE 2). N Engl J Med. 2025;393(7):648-659. PMID: 40544432. DOI: 10.1056/NEJMoa2502082. https://www.nejm.org/doi/full/10.1056/NEJMoa2502082
Educational and research-use disclaimer: This article is provided solely for scientific and educational purposes. Cagrilintide is an investigational compound that is not approved by the FDA, EMA, or any comparable regulator for the treatment, cure, or prevention of obesity, type 2 diabetes, or any other disease. While peer-reviewed phase 2 and phase 3 trials support an appetite-regulating and weight-lowering effect — primarily as the combination product CagriSema, which itself remains under regulatory review — supportive trial data are not marketing authorization, and long-term efficacy and safety are not established. Nothing here is medical advice or a recommendation for human use, and material sold as “research” cagrilintide is not the quality-controlled compound studied in trials. Any legitimate investigation of this compound should occur within properly authorized clinical research under appropriate oversight. Readers should consult qualified professionals and applicable regulations before making any decisions.