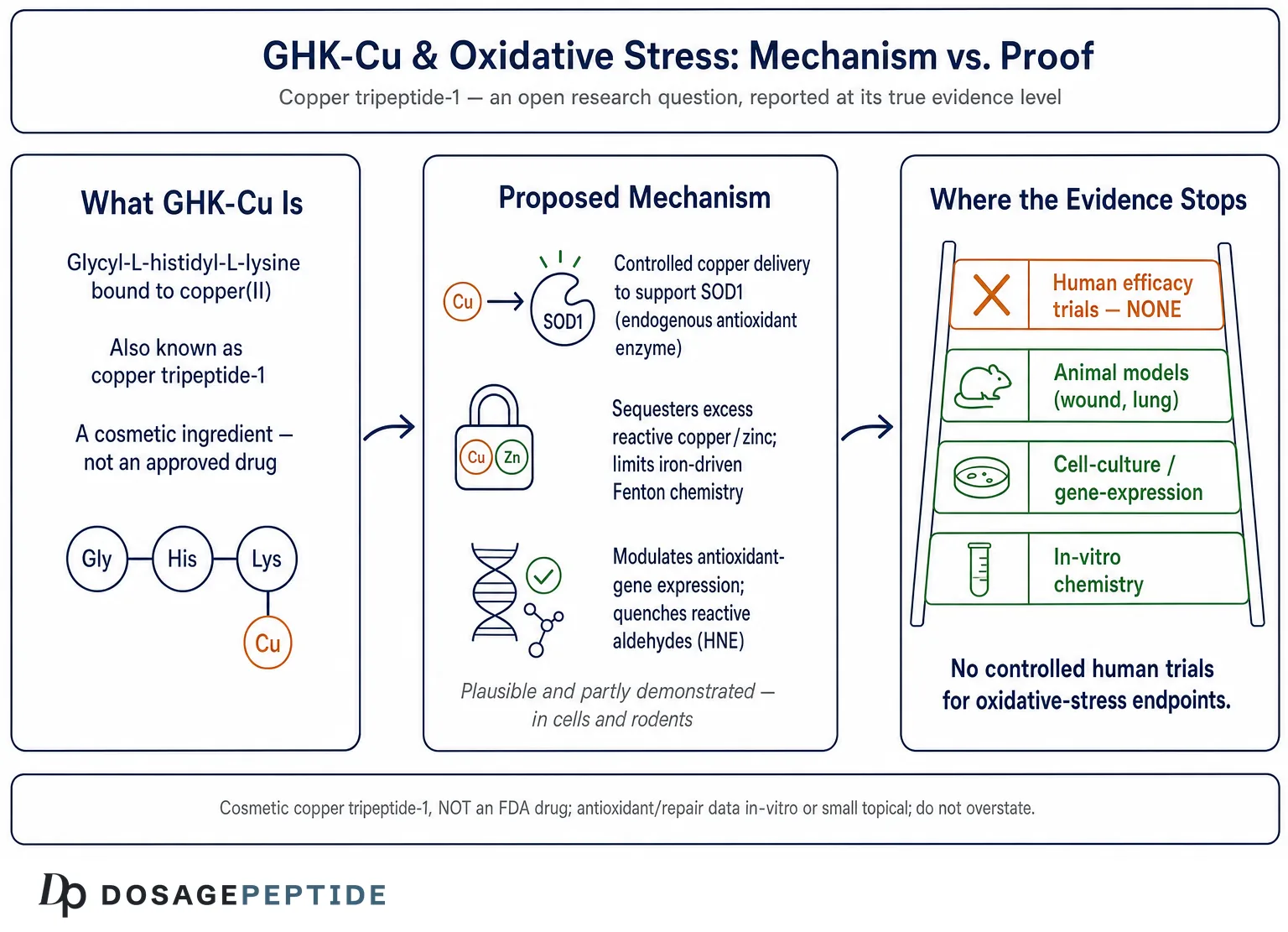
The verb in this article’s title deserves scrutiny before anything else, because it carries more weight than the evidence can bear. To ask what studies “prove” GHK-Cu’s therapeutic potential against oxidative stress is to assume that proof exists — that somewhere in the literature there is a body of controlled human trials establishing that this copper tripeptide treats or prevents an oxidative-stress-driven disease. That assumption does not survive contact with the actual record. GHK-Cu (glycyl-L-histidyl-L-lysine bound to copper(II), known to regulators and formulators as copper tripeptide-1) is a cosmetic ingredient, not an approved drug for any condition.3 Its antioxidant credentials rest almost entirely on in-vitro chemistry, gene-expression profiling, and small animal or topical studies. There is no pivotal randomized controlled trial demonstrating that GHK-Cu reduces clinical oxidative-stress endpoints in humans.
So rather than affirm the premise, this piece treats it as an open research question and reports the evidence at its true level. That is not a hostile posture toward the molecule — GHK-Cu is genuinely interesting, and the mechanistic case that it interacts with oxidative biology is one of the more coherent stories in the peptide field. It is a posture of honesty. The distance between “a plausible, partially demonstrated antioxidant mechanism in cells and rodents” and “a proven therapy against oxidative stress in people” is enormous, and most popular writing about GHK-Cu collapses it. The whole value of a careful review is to hold that distance open and show exactly where the data stop.
What follows is written for researchers and scientifically literate readers who want a candid map: what GHK-Cu is at the level of chemistry, why oxidative stress is a harder target than marketing implies, what the mechanistic and gene-expression studies actually found, how much of that has been confirmed in living tissue versus a cuvette, how it compares with established antioxidant strategies, where the human-evidence gap lies, and what its regulatory status really means. Throughout, the guiding rule is restraint. Nothing here should be read as suggesting GHK-Cu treats, cures, or prevents any disease of oxidative stress; where the evidence is preclinical or cosmetic, it will be labeled as such.
What GHK-Cu Actually Is
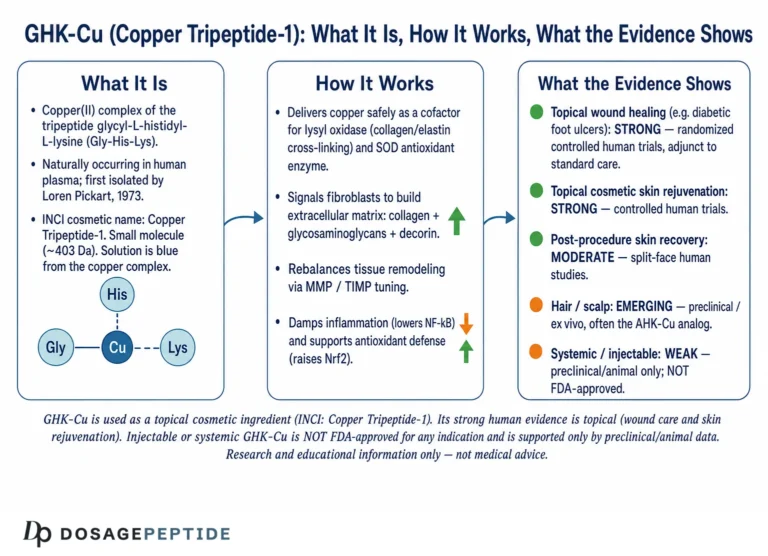
GHK is a tripeptide with the sequence glycyl-L-histidyl-L-lysine. It was first isolated from human plasma in 1973, when it was identified as a serum factor that influenced the behavior of cultured liver cells, and it also occurs in saliva and urine.12 Its defining biochemical feature is a near-perfect geometry for chelating copper(II): the terminal amine, the imidazole nitrogen of histidine, and a deprotonated amide nitrogen form a tight square-planar coordination sphere around the copper ion, with the lysine side chain contributing to stability. The complex that results — GHK-Cu — has the molecular formula C₁₄H₂₂CuN₆O₄ and a naturally high affinity for copper that lets it move the metal into and out of cells and between other copper-binding proteins.1
That copper-carrying property is the entire hinge of the oxidative-stress hypothesis, so it is worth stating precisely. Copper is not incidental to GHK-Cu; it is the business end of the molecule. Free copper ions are dangerous to cells because copper cycles readily between its Cu(II) and Cu(I) oxidation states and can drive Fenton-type chemistry that generates hydroxyl radicals — among the most destructive reactive oxygen species (ROS) in biology. Yet copper is also indispensable, because it is the catalytic cofactor of copper/zinc superoxide dismutase (SOD1), one of the cell’s primary enzymatic defenses against superoxide. The cell therefore never lets copper wander freely; it hands it off through a relay of chaperone proteins. The proposed appeal of GHK-Cu is that it may act as a similarly controlled carrier — delivering copper in a bound, redox-buffered form rather than as a loose, radical-generating ion.19
It is important to separate three things that popular accounts routinely blur. First, there is the peptide GHK on its own, which has some intrinsic chemistry (notably the ability to react with certain toxic aldehydes and to bind metals). Second, there is the copper complex GHK-Cu, whose properties are dominated by the coordinated metal. Third, there is the cosmetic ingredient copper tripeptide-1, a manufactured, formulated version used in topical skincare at low concentrations. When a study reports an effect, it matters enormously which of these three was tested, at what concentration, and in what system. An in-vitro result for the bare peptide reacting with an aldehyde tells you something quite different from a topical serum applied to skin, which in turn tells you nothing definitive about systemic oxidative-stress disease. Keeping these levels distinct is the single most useful discipline for reading the GHK-Cu literature honestly.
Historically, GHK-Cu entered practical use through wound care and cosmetics rather than through the drug-development pipeline. Loren Pickart, who first isolated the peptide, went on to author or co-author much of the mechanistic and review literature that underpins today’s antioxidant claims.135 That concentration of the foundational work in a small number of related authors is not a disqualification — the chemistry is real and independently reproducible — but it is a reason to read the strongest efficacy language with the awareness that much of it originates from advocates of the molecule rather than from a broad, adversarial clinical literature.
One more biological detail sharpens the framing. GHK circulates in human plasma at meaningful levels in youth — on the order of the low hundreds of nanograms per milliliter — and those levels decline substantially with age.1 This age-related fall is the seed of a popular and superficially attractive narrative: that GHK is a “youth signal” whose replacement might restore a more youthful, less oxidatively stressed physiology. The narrative is worth naming precisely because it is seductive and unproven. A correlation between falling GHK and rising oxidative damage across the lifespan does not establish that GHK loss causes the damage, still less that supplementing GHK-Cu reverses it. Countless molecules decline with age; restoring any one of them to youthful levels has rarely turned out to rejuvenate the system. The decline is a legitimate reason to study the peptide; it is not, on its own, evidence of therapeutic benefit, and it should never be presented as such.
Why Oxidative Stress Is a Harder Target Than It Sounds
“Oxidative stress” is one of the most invoked and least disciplined terms in wellness writing, so a working definition matters. Oxidative stress is the imbalance between the production of reactive oxygen and nitrogen species and a cell’s capacity to neutralize them and repair the damage they cause. ROS include superoxide, hydrogen peroxide, and the hydroxyl radical, along with reactive carbonyls and lipid-peroxidation products such as 4-hydroxynonenal (HNE) and acrolein. When these overwhelm the antioxidant defenses — enzymatic ones such as superoxide dismutase, catalase, and glutathione peroxidase, and small-molecule ones such as glutathione and ascorbate — they oxidize lipids, proteins, and DNA, and that damage is implicated in aging, neurodegeneration, fibrosis, chronic inflammation, and many other conditions.1
The crucial nuance, and the reason the antioxidant field has humbled so many promising compounds, is that ROS are not simply toxic waste to be mopped up. They are also signaling molecules. Hydrogen peroxide at low concentrations regulates gene transcription, immune responses, and the adaptive stress pathways (such as Nrf2) that build a cell’s own defenses. Blunt, indiscriminate antioxidant supplementation has repeatedly failed — and in some large trials has caused harm — precisely because flooding the system with radical scavengers can suppress useful signaling as readily as harmful oxidation. This history is why the modern view favors modulating redox biology, ideally by restoring the cell’s own enzymatic defenses, over crudely quenching every radical in sight.
This framing is directly relevant to GHK-Cu, because the more interesting version of its hypothesis is not “GHK-Cu is a radical sponge” but “GHK-Cu may help re-tune the cell’s endogenous antioxidant machinery, in part by managing copper.” That is a subtler and, if true, more valuable mechanism — but it is also harder to prove, because it requires showing durable changes in enzyme activity, gene expression, and damage markers in a living system, not just a favorable reaction in a test tube. As we will see, GHK-Cu has generated encouraging signals at the test-tube and gene-expression levels, and some supportive tissue data, but the leap to demonstrated clinical benefit against an oxidative-stress disease has not been made.
It is also worth being explicit about why the “more antioxidant is always better” intuition is not just unhelpful but actively misleading in this context. The large intervention trials of high-dose antioxidant vitamins — beta-carotene, vitamin E, and vitamin C among them — are among the more instructive failures in modern preventive medicine: several found no benefit for chronic-disease prevention, and a few found that supplementation increased certain risks. The mechanistic explanation is that transient, localized bursts of ROS are how cells sense stress and mount adaptive defenses, including the very antioxidant enzymes that long-term protection depends on. A therapy that suppresses that signaling wholesale can leave a cell less resilient, not more. This is precisely why a compound that claims to work by supporting endogenous defenses and managing reactive metals — as GHK-Cu’s proponents argue — would, if genuinely validated, be more interesting than a brute-force scavenger. But “would be more interesting if validated” is the operative phrase, and it keeps returning us to the same unmet requirement: controlled evidence in humans.
A second reason oxidative stress is a hard target is measurement. Human oxidative-stress studies rely on surrogate markers — malondialdehyde, protein carbonyls, 8-OHdG, F2-isoprostanes — each with its own analytical noise, and none of which is a validated regulatory endpoint for approving a therapy. A compound can nudge a biomarker without changing any outcome a patient would notice. Any honest assessment of GHK-Cu has to keep asking not just “did a marker move?” but “was this a clinically meaningful, reproducible change in a relevant population?” For GHK-Cu, the answer to the second question is, so far, that the studies to establish it have not been done.
The Central Mechanism: Copper Handling, SOD, and Redox-Silent Delivery
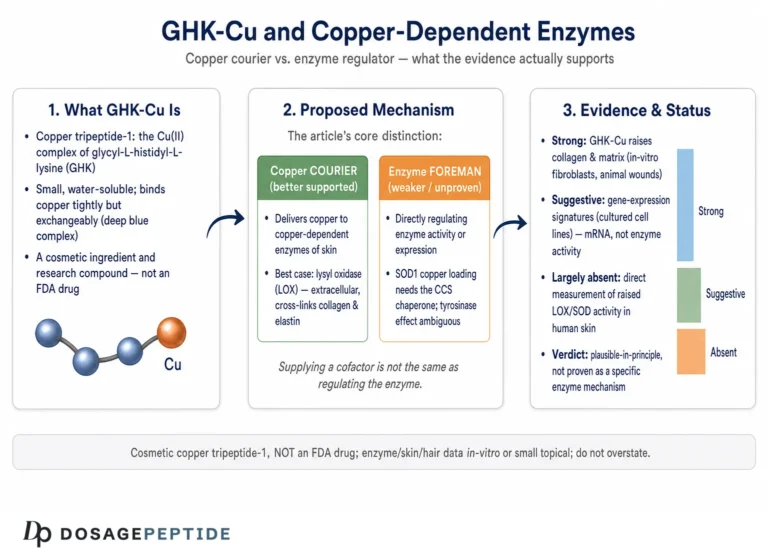
The most coherent mechanistic account of how GHK-Cu might counter oxidative stress runs through copper homeostasis. Copper’s redox versatility is exactly what makes it both essential and dangerous. As a loose ion it can reduce molecular oxygen and hydrogen peroxide to hydroxyl radicals via Fenton and Haber-Weiss chemistry, initiating lipid peroxidation and protein oxidation. As a tightly held cofactor inside SOD1, that same redox versatility is harnessed to dismantle superoxide. The difference between poison and protector is entirely a matter of whether the copper is controlled.19
The proposed value of GHK-Cu is that it may deliver copper in a controlled, redox-buffered state. Because the peptide sequesters the metal in a stable coordination geometry, the hypothesis is that GHK-Cu can shuttle copper to where it is needed — supporting cuproenzymes such as SOD1 — without releasing the free, radical-generating ionic copper that would otherwise contribute to oxidative damage. In this reading, GHK-Cu behaves less like an antioxidant molecule and more like a logistics system for the metal that powers the cell’s own antioxidant enzymes.1 Reviews of the compound frame the downstream consequence as improved copper availability for SOD1 and, potentially, higher SOD activity.2
There is genuine experimental support for the idea that GHK can tame copper’s toxicity, though it comes from a specific and limited context. In a 2024 in-vitro study, GHK prevented copper- and zinc-induced protein aggregation and reduced metal-catalyzed cell death in cultured central nervous system cells, and it could even resolubilize already-aggregated protein.9 That is a clean demonstration that the peptide can bind excess copper and blunt its damaging, ROS-linked effects in a dish. It is also, importantly, a cell-culture result in a neuronal model — not evidence that oral or topical GHK-Cu protects a human brain, and the authors did not claim it was.
A related mechanistic thread concerns iron rather than copper. Some of GHK-Cu’s earliest antioxidant data described inhibition of iron release from ferritin. Because free ferrous iron is itself a potent Fenton catalyst, a molecule that limits its release could indirectly reduce hydroxyl-radical generation and downstream lipid peroxidation. The classic figure cited from this line of work is a roughly 75% reduction in lipid peroxidation in a gastric-tissue preparation attributed to blocked ferritin iron release.1 This is a real and specific finding, but note its nature: it is an ex-vivo biochemical measurement, not a clinical outcome, and it describes an indirect antioxidant effect (starving the Fenton reaction of iron) rather than direct radical scavenging.
The honest mechanistic summary is that GHK-Cu has a plausible, partially-evidenced story built on three legs — controlled copper delivery to support endogenous SOD, sequestration of excess reactive copper and zinc, and limitation of iron-driven Fenton chemistry — each supported by in-vitro or ex-vivo work. What the mechanism does not have is a demonstration that these effects translate into meaningful antioxidant protection in a human being with an oxidative-stress disease. Mechanism and outcome are different currencies, and only the first has been paid out.
What the Gene-Expression Studies Actually Show
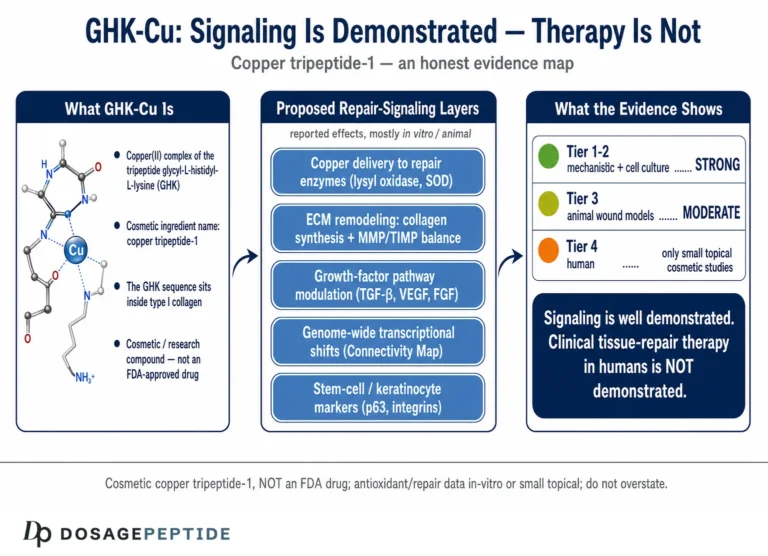
The most-cited pillar of GHK-Cu’s antioxidant reputation is not a scavenging assay at all — it is transcriptomics. Using data from the Broad Institute’s Connectivity Map, which profiles how cultured human cells change their gene expression in response to bioactive compounds, Pickart and colleagues reported that GHK induces a change of 50% or greater in the expression of a large fraction of assessed human genes, and they parsed subsets relevant to antioxidant defense, DNA repair, tissue remodeling, and inflammation.245
Within the antioxidant subset specifically, the 2015 analysis in Cosmetics reported that GHK stimulated a set of genes associated with antioxidant defense while suppressing a smaller number tied to pro-oxidant activity — the authors framed this as GHK potentially resetting the skin’s redox-related gene pattern toward a healthier state.2 Later gene-ontology reviews extended the same Connectivity Map approach to nervous-system and general regenerative pathways, again describing a pattern of up- and down-regulation the authors interpreted as broadly protective.34
This is real, publicly documented data, and it is the strongest single reason to take GHK-Cu’s antioxidant hypothesis seriously. But it must be read for exactly what it is, and several caveats are non-negotiable:
- Gene expression is not function. A change in mRNA level is a signal that a pathway may be engaged; it is not proof that protein was made, that enzyme activity rose, or that a cell was protected from damage. The gap between transcript and phenotype is where a great many promising compounds fail.
- The Connectivity Map is a cultured-cell screen. Its power is in generating hypotheses across many compounds and genes; it was never designed to establish clinical efficacy, and the concentrations and cell lines used may not reflect skin in situ, let alone a diseased human organ.
- Breadth can cut against specificity. A compound that changes a very large share of the transcriptome is exhibiting a broad, pleiotropic signal. That is biologically intriguing, but it also makes it harder to attribute any single benefit to a clean, targeted antioxidant mechanism.
- Author concentration. The dominant gene-expression interpretations come from a closely related group of papers. Independent replication and adversarial reanalysis remain comparatively thin.
So the gene-expression literature legitimately elevates GHK-Cu from “interesting metal chelator” to “compound with a documented, redox-relevant transcriptional footprint.” It does not, and cannot on its own, prove therapeutic potential against oxidative stress. It is hypothesis-generating evidence of high quality within its category and of limited reach outside it. Readers who want to see how the same transcriptional data are invoked for GHK-Cu’s better-known cosmetic role can compare this analysis with the site’s discussion of GHK-Cu for skin health and collagen synthesis, where the collagen-remodeling gene set is the focus rather than the antioxidant one.
Direct Antioxidant Chemistry: Quenching Reactive Carbonyls
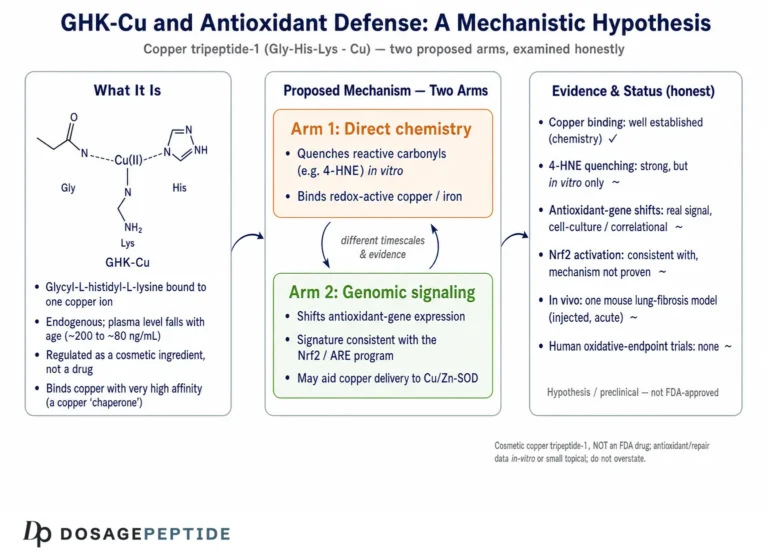
Beyond copper handling and gene expression, GHK has a third, more directly chemical antioxidant credential: it can react with and neutralize certain toxic byproducts of lipid peroxidation. When polyunsaturated fatty acids in membranes are oxidized, they fragment into reactive α,β-unsaturated aldehydes — most notably 4-hydroxy-trans-2-nonenal (HNE) and acrolein — which are highly electrophilic and form damaging adducts with proteins and DNA. These aldehydes are not merely markers of oxidative stress; they propagate it, and HNE in particular is implicated in the pathology of neurodegenerative disease.1
A 2007 mechanistic study in Chemical Research in Toxicology examined this directly, using mass spectrometry, NMR, and computational modeling to show that GHK acts as a quencher of HNE — the histidine imidazole and the lysine amine provide nucleophilic sites that trap the reactive aldehyde, forming stable adducts and removing it from circulation.6 The same study is candid about the effect’s magnitude: GHK was an effective quencher but significantly less potent than carnosine, the reference histidine-containing peptide against which it was compared.6 That comparative honesty is worth emphasizing, because promotional summaries often cite the HNE-quenching result while omitting that GHK underperformed the benchmark compound.
This carbonyl-quenching chemistry is the closest GHK comes to being a “classic” antioxidant — a molecule that directly reacts with and detoxifies a damaging species. It is real, it is mechanistically characterized, and it is measured in a rigorous physicochemical study. But its relevance to whole-organism oxidative stress is bounded by pharmacology: quenching HNE in a reaction vessel requires the peptide to be present at the site of lipid peroxidation, at adequate concentration, at the right time. Whether topically applied or systemically administered GHK-Cu ever reaches such concentrations at a relevant tissue in a living human is unstudied. The chemistry establishes capability; it does not establish delivery or clinical effect.
Taken together, the three mechanistic strands — copper/iron management, transcriptional modulation of antioxidant genes, and direct carbonyl quenching — make GHK-Cu one of the more mechanistically layered candidates in the peptide space. The problem, consistently, is not the plausibility of the mechanisms but the altitude of the evidence: nearly all of it sits at the in-vitro or ex-vivo level, with a thin and largely non-human tier of tissue studies above it.
In-Vivo and Tissue-Level Evidence
Where GHK-Cu’s story moves from the cuvette into living tissue, it does so mainly through wound-healing and organ-fibrosis models in animals, with antioxidant markers measured as secondary endpoints. These studies are genuine and peer-reviewed, but their designs were built around tissue repair, not around oxidative-stress disease as a primary indication.
In diabetic wound-healing work, biotinylated GHK incorporated into collagen matrices accelerated wound closure in diabetic rats, and the treated tissue showed higher levels of the antioxidants glutathione and ascorbic acid along with increased activity of antioxidant enzymes, better epithelialization, and greater collagen synthesis.7 A separate study in rabbits found that topical tripeptide-copper complex, alone or combined with helium-neon laser therapy, improved wound contraction and granulation tissue and raised the activity of antioxidant enzymes in the healing wound.8 These are supportive of the idea that GHK-Cu can shift a local redox environment in a repairing tissue — but they are rodent and rabbit wound models, the antioxidant readouts are secondary, and the delivery is local. They speak to the compound’s tissue-repair biology, which the site examines further in the context of chronic non-healing wounds, more than to systemic antioxidant therapy.
The most mechanistically pointed in-vivo antioxidant evidence comes from the lung. A 2024 study in Redox Biology reported that the GHK-Cu complex attenuated lung inflammation and fibrosis in a mouse model of silicosis by binding peroxiredoxin 6 (PRDX6), an antioxidant enzyme, with the protective effect linked in part to suppression of crystalline-silica-induced oxidative stress in alveolar macrophages.10 This is notable because it identifies a specific molecular target within the antioxidant machinery and ties the benefit to reduced oxidative stress in a defined cell type. Earlier work had also shown that GHK inhibited bleomycin-induced pulmonary fibrosis in mice, acting on the TGF-β1/Smad pathway and epithelial-to-mesenchymal transition, with anti-oxidative and anti-inflammatory effects described as part of the mechanism.11 The site’s companion analysis of GHK-Cu in COPD and pulmonary fibrosis goes deeper into these respiratory models.
Even at its strongest, though, this tier of evidence remains preclinical. The silicosis and bleomycin studies are mouse models of specific occupational and drug-induced lung diseases; the PRDX6 targeting is a promising lead, not an approved indication. No controlled human trial has tested whether GHK-Cu reduces oxidative-stress-driven lung disease, neurodegeneration, or any other systemic condition in people. The consistent pattern — encouraging animal and cell data, no human efficacy trials — is the defining feature of the entire GHK-Cu antioxidant literature.
A useful way to hold all of this together is to map each claim to the highest level of evidence that actually supports it, rather than to the level implied by marketing.
| Antioxidant-related claim | Highest supporting evidence | Level |
|---|---|---|
| Binds and buffers copper, limiting free-ion Fenton chemistry | Coordination chemistry; CNS cell-culture protection19 | In vitro |
| Supports copper availability for SOD1 | Mechanistic reasoning + review synthesis12 | Hypothesis / in vitro |
| Modulates antioxidant-gene expression | Connectivity Map transcriptomics24 | Cultured-cell screen |
| Quenches reactive aldehydes (HNE, acrolein) | MS/NMR/computational study (weaker than carnosine)6 | In vitro chemistry |
| Limits iron-driven lipid peroxidation | Ferritin iron-release inhibition, ~75% in tissue prep1 | Ex vivo |
| Raises tissue antioxidant enzymes/GSH in healing | Diabetic-rat and rabbit wound models78 | Animal (local) |
| Reduces oxidative stress in lung disease | Silicosis + bleomycin mouse models, PRDX6 target1011 | Animal (preclinical) |
| Treats/prevents an oxidative-stress disease in humans | No controlled human efficacy trials | None |
The bottom row is the one to carry away. Every claim above it has some genuine support; the claim that GHK-Cu is a proven human therapy against oxidative stress has none.
How GHK-Cu Compares With Established Antioxidant Strategies
Placing GHK-Cu beside better-characterized antioxidant approaches clarifies both its distinctiveness and the evidentiary distance it still has to travel. The comparison is not a competition — GHK-Cu has never been tested head-to-head against these agents for an oxidative-stress indication — but it shows what different tiers of evidence look like.
| Agent / strategy | Primary antioxidant mechanism | Human evidence level |
|---|---|---|
| N-acetylcysteine | Glutathione precursor; direct radical scavenging | Approved uses (e.g., acetaminophen toxicity); mixed results elsewhere |
| Vitamin C / vitamin E | Direct radical scavenging | Extensive RCTs; largely disappointing for chronic disease prevention |
| Nrf2 activators (e.g., sulforaphane) | Induce endogenous antioxidant genes | Multiple clinical trials; signals but no broad disease approval for this use |
| SOD mimetics | Catalytically dismutate superoxide | Investigational; several clinical programs, none broadly approved |
| Carnosine | Carbonyl quenching, metal chelation | Small human studies; supplement, not approved therapy |
| GHK-Cu | Copper/iron handling, gene modulation, carbonyl quenching | In vitro + animal only; no oxidative-stress efficacy RCTs |
Two lessons emerge. First, GHK-Cu’s conceptual profile actually aligns with the more sophisticated end of the field — it is closer to an Nrf2-style endogenous-defense modulator combined with a metal-handling agent than to a crude radical sponge, and that is arguably the more promising design. Second, and sobering, even the direct-scavenging vitamins with enormous RCT programs have largely failed to prevent chronic oxidative-stress disease, and even the mechanistically elegant Nrf2 activators and SOD mimetics have not converted into broad approvals. A compound like GHK-Cu, sitting at the in-vitro-and-animal stage, is therefore not merely “a few trials away” from proven therapy; it is at the very start of a path on which far better-resourced candidates have stalled.
That comparison also underscores why the copper component is a double-edged design choice. Bundling the antioxidant hypothesis to a redox-active metal is exactly what gives GHK-Cu its distinctive SOD-supporting rationale — and exactly what raises the safety and characterization questions that regulators scrutinize, as discussed below. For a broader orientation on how researchers categorize peptides by mechanism and evidence tier, the site’s peptide glossary is a useful reference point.
Research Models and Methodology
Understanding how GHK-Cu’s antioxidant data were generated clarifies what they can and cannot support. The methodology falls into four tiers, each answering a different and progressively harder question.
Coordination chemistry and cell-free assays. The foundational work characterized GHK-Cu’s copper-binding geometry and its direct reactions — iron-release inhibition from ferritin, aldehyde quenching, metal buffering — using spectroscopy, mass spectrometry, NMR, and computational modeling.16 These methods are ideal for establishing that a molecule can perform a chemical action; they say nothing about whether it does so usefully inside a cell.
Cell-culture studies. The next tier examined GHK or GHK-Cu applied to cultured cells — fibroblasts, keratinocytes, neuronal lines — measuring survival under metal or oxidative challenge, gene expression, and enzyme markers.9 The 2024 CNS protein-aggregation study is a strong example: a clean, mechanistically interpretable result in a defined system.9 The Connectivity Map transcriptomics also live at this tier.24 Cell culture bridges chemistry and biology but strips away pharmacokinetics, tissue barriers, and whole-organism regulation.
Animal models. The in-vivo antioxidant evidence comes from wound-healing models in diabetic rats and rabbits, where antioxidant enzymes and glutathione were secondary endpoints, and from mouse lung-disease models (silicosis, bleomycin fibrosis) where oxidative stress was part of the mechanism.781011 These are the gold standard among the available GHK-Cu antioxidant studies — but they are disease-specific rodent models with local or targeted delivery, not systemic antioxidant-therapy trials, and rodent redox biology does not map cleanly onto human physiology.
Human trials. This tier is essentially empty for oxidative-stress endpoints. GHK-Cu’s human use is overwhelmingly cosmetic — topical serums and creams evaluated, when at all, for skin appearance and tolerability, not for validated oxidative-stress biomarkers or disease outcomes. There is no published randomized, placebo-controlled trial demonstrating that GHK-Cu reduces a clinical oxidative-stress endpoint in humans. The rigorous methodology needed to answer the title’s question — controlled human trials with pre-specified redox biomarkers and clinical outcomes in a relevant population — has not been applied.
The methodological bottom line is that GHK-Cu’s evidence architecture is inverted relative to what “proof of therapeutic potential” requires: it is strongest at the chemical and cellular base, thins to preclinical animal work in the middle, and vanishes at the human-efficacy apex where proof would actually reside.
Safety, Handling, and the Research Context
Because GHK-Cu is most often encountered either as a topical cosmetic or as a lyophilized research powder, a brief, strictly educational note on safety and handling is warranted — with the emphasis that this is not a usage recommendation and that GHK-Cu is not an approved therapeutic for oxidative stress or any other disease.
In topical cosmetic use at the low concentrations typical of skincare, copper tripeptide-1 has a long track record and is generally well tolerated, with adverse effects usually limited to local irritation or, rarely, sensitization. That cosmetic-exposure safety record is reassuring on its own terms but does not transfer to systemic administration. The key safety consideration that distinguishes GHK-Cu from a plain peptide is the copper payload: the entire antioxidant rationale depends on the metal, and copper has a narrow therapeutic window. Delivering copper systemically and repeatedly raises questions about copper accumulation and the very Fenton chemistry the molecule is supposed to prevent — questions that are adequately contained in a controlled cosmetic formulation but are unstudied for high-dose or long-term systemic exposure.
Several caveats follow directly:
- Route matters. Safety established for low-concentration topical application says nothing about injected or high-dose exposure, where copper handling becomes the dominant risk.
- Population matters. Individuals with disorders of copper metabolism (such as Wilson’s disease) or compromised excretion could be uniquely vulnerable to a copper-delivering compound.
- Product quality matters. Material sold outside regulated cosmetic channels as “research chemical” varies in purity, copper stoichiometry, and endotoxin load; these sourcing risks are independent of the molecule’s intrinsic properties.
- Characterization gaps. Regulators have flagged incomplete physicochemical characterization and immunogenicity/impurity concerns for compounded peptides generally, which applies to informally sourced GHK-Cu.
On the handling side, GHK-Cu is typically supplied as a blue lyophilized powder (the color reflects the coordinated copper). In a research context, lyophilized peptides are reconstituted with sterile or bacteriostatic water directed gently against the vial wall and swirled rather than shaken, since vigorous agitation can degrade peptide material; they are stored cool and dark and protected from repeated freeze-thaw cycles. The volume of diluent simply sets the concentration — a fixed mass in a larger volume yields a lower concentration per unit volume, the arithmetic behind any reconstitution chart. General, compound-agnostic walkthroughs of this process appear in the site’s peptide reconstitution guide. It bears repeating that meticulous handling preserves whatever activity the molecule has; it does not create clinical efficacy where none has been demonstrated.
Limitations and the Human-Evidence Gap
Pulling the threads together, the limitations that bear on the title’s question are severe, and they compound one another rather than sitting in isolation.
No human efficacy trials. The single largest limitation is the absence of controlled human studies with oxidative-stress endpoints. Every claim of therapeutic potential against oxidative stress is therefore an extrapolation from cells and animals, not a finding in people.
Evidence concentrated at the wrong altitude. The data are strongest exactly where they prove least — chemistry and cell culture — and weakest where proof would live, in the clinic. A robust in-vitro mechanism is a reason to run trials, not a substitute for them.
Biomarker-versus-outcome problem. Even the supportive animal data mostly move secondary redox markers (glutathione, enzyme activity, ROS levels) rather than demonstrating durable clinical outcomes. The antioxidant field is littered with agents that improved a marker and changed nothing a patient would feel.
Delivery and pharmacokinetics unresolved. The direct antioxidant chemistry (aldehyde quenching, iron sequestration) requires adequate concentrations at the site of oxidative damage. Whether topical or systemic GHK-Cu ever achieves this in a human tissue of interest is unstudied.
Author and replication concentration. Much of the interpretive framework, especially the gene-expression synthesis, originates from a small, related group of publications. Independent, adversarial replication is comparatively limited.
The copper double-bind. The metal that powers the mechanism is also the source of its principal systemic-safety uncertainty, which constrains how aggressively the compound could be dosed even if efficacy were shown.
The human-evidence gap is thus not a narrow crack to be papered over with mechanism talk and rodent extrapolation. It is the whole story of whether GHK-Cu is a proven therapy: it is not, because the studies that would constitute proof have not been done. Responsible communication means resisting the pull of a genuinely elegant mechanism and stating plainly that therapeutic potential against oxidative stress remains a hypothesis. Readers tracking how the wider peptide-and-tissue-repair literature evolves can follow the site’s foundational explainer on the healing peptide BPC-157 for a parallel example of a compound with strong preclinical signals and thin human data.
Regulatory and Cosmetic Status
GHK-Cu’s regulatory picture is frequently misrepresented, so precision matters.
Cosmetic ingredient, not an approved drug. GHK-Cu is used commercially as copper tripeptide-1, a cosmetic ingredient in topical skincare. In that capacity it is regulated under cosmetics frameworks, which govern safety for topical use and labeling — not therapeutic efficacy. It is not approved by the U.S. Food and Drug Administration, the European Medicines Agency, or any comparable regulator as a drug for oxidative stress, aging, neurodegeneration, fibrosis, wound healing, or any other disease. There is, correspondingly, no approved indication of any kind that could be described as “proven” therapy.
Cosmetic clearance is not efficacy. A recurring source of confusion is the assumption that because GHK-Cu is legally sold in skincare, its antioxidant benefits are established. They are not. Cosmetic regulation addresses whether an ingredient is safe for topical use at defined concentrations; it makes no finding that the ingredient reduces oxidative stress or treats any condition. Cosmetic claims are, by design, restricted to appearance rather than physiological or disease outcomes.
Compounding scrutiny. Peptides marketed for systemic use outside the cosmetic lane sit in a contested regulatory space. Copper-containing peptides have drawn attention over incomplete characterization and impurity and immunogenicity concerns, consistent with regulators’ broader caution about compounded peptide products. This underscores that GHK-Cu has no settled, sanctioned place as a systemic therapeutic in the United States.
The regulatory synthesis is straightforward: GHK-Cu is a legitimate, well-established cosmetic ingredient with an interesting antioxidant mechanism and encouraging preclinical data, and it is not an approved therapy for oxidative stress. Any legitimate exploration of the compound as an antioxidant medicine would require formal preclinical and clinical development under regulatory oversight — the very process whose absence is the reason the title’s premise cannot yet be affirmed.
Frequently Asked Questions
Do any studies prove GHK-Cu treats oxidative stress in humans?
No. There are no controlled human efficacy trials demonstrating that GHK-Cu reduces a clinical oxidative-stress endpoint or treats an oxidative-stress-driven disease. The antioxidant evidence is in-vitro (copper and iron handling, aldehyde quenching, gene expression) and preclinical animal work (wound and lung-disease models).1610 “Proof” of human therapeutic potential does not exist; the honest framing is an open research question.
What is the strongest evidence that GHK-Cu does anything against oxidative stress?
The most rigorous single findings are the mechanistic ones: GHK quenches the toxic lipid-peroxidation aldehyde HNE in a mass-spectrometry/NMR study (though less potently than carnosine),6 and GHK prevents copper- and zinc-induced protein aggregation and cell death in cultured CNS cells.9 The most pointed in-vivo lead is a 2024 mouse study in which GHK-Cu bound peroxiredoxin 6 and reduced silica-induced oxidative stress in the lung.10 All are preclinical.
How does GHK-Cu’s copper relate to superoxide dismutase?
Copper is the catalytic cofactor of copper/zinc superoxide dismutase (SOD1), a core antioxidant enzyme. The hypothesis is that GHK-Cu delivers copper in a controlled, redox-buffered form that supports SOD1 function without releasing free, radical-generating copper.12 This is mechanistically plausible and partly supported in cell studies, but it has not been shown to raise SOD activity meaningfully in a human tissue in a controlled trial.
Doesn’t copper itself cause oxidative stress?
Free copper ions can drive Fenton chemistry that generates destructive hydroxyl radicals, which is exactly why cells never let copper roam freely. GHK-Cu’s proposed advantage is that it holds copper in a tight coordination geometry, buffering its reactivity while keeping it bioavailable for enzymes.19 This same dependence on a redox-active metal, however, is the main systemic-safety uncertainty for anything beyond low-concentration topical use.
What do the gene-expression studies actually establish?
Connectivity Map transcriptomic analyses report that GHK changes the expression of a large share of human genes, including a set tied to antioxidant defense.24 This is high-quality hypothesis-generating data from a cultured-cell screen. It shows the compound has a redox-relevant transcriptional footprint; it does not prove that protein was made, that enzyme activity rose, or that any human benefited — gene expression is a signal, not a clinical outcome.
Is GHK-Cu approved by the FDA for anything?
Not as a drug. GHK-Cu is used as the cosmetic ingredient copper tripeptide-1, regulated for topical safety rather than therapeutic efficacy. It is not approved by the FDA, EMA, or comparable regulators to treat, cure, or prevent oxidative stress or any disease. Cosmetic legality is not evidence of antioxidant efficacy.
Is the antioxidant research on GHK-Cu independent?
Partly. The direct chemistry (aldehyde quenching), the CNS metal-toxicity work, and the lung-disease models come from independent groups.6910 However, much of the interpretive framework — especially the gene-expression synthesis and broad antioxidant narrative — originates from a small, closely related set of review papers,235 so the strongest efficacy language should be read with that concentration in mind.
Could GHK-Cu ever become a proven antioxidant therapy?
It cannot be ruled out. The mechanism is coherent and aligns with the more sophisticated end of the antioxidant field (endogenous-defense modulation plus metal handling rather than crude scavenging). But it would require the full research program that is currently missing — pharmacokinetic characterization, validated animal models with functional endpoints, and controlled human trials with pre-specified redox biomarkers — and it would have to clear a bar on which far better-resourced antioxidant candidates have already stalled.
How is GHK-Cu handled in a research setting?
As a blue lyophilized powder (the color comes from the bound copper), it is reconstituted with sterile or bacteriostatic water using gentle technique, stored cool and dark, and protected from freeze-thaw cycles — standard research-peptide practice covered in general reconstitution references. Handling quality preserves activity but has no bearing on the absence of human antioxidant-efficacy data.
References
- Pickart L, Vasquez-Soltero JM, Margolina A. The Human Tripeptide GHK-Cu in Prevention of Oxidative Stress and Degenerative Conditions of Aging: Implications for Cognitive Health. Oxid Med Cell Longev. 2012;2012:324832. PMID: 22666519; PMCID: PMC3359723. https://pmc.ncbi.nlm.nih.gov/articles/PMC3359723/
- Pickart L, Vasquez-Soltero JM, Margolina A. GHK-Cu may Prevent Oxidative Stress in Skin by Regulating Copper and Modifying Expression of Numerous Antioxidant Genes. Cosmetics. 2015;2(3):236-247. doi:10.3390/cosmetics2030236. https://www.mdpi.com/2079-9284/2/3/236
- Pickart L, Margolina A. Regenerative and Protective Actions of the GHK-Cu Peptide in the Light of the New Gene Data. Int J Mol Sci. 2018;19(7):1987. PMID: 29986520; PMCID: PMC6073405. https://pubmed.ncbi.nlm.nih.gov/29986520/
- Pickart L, Vasquez-Soltero JM, Margolina A. The Effect of the Human Peptide GHK on Gene Expression Relevant to Nervous System Function and Cognitive Decline. Brain Sci. 2017;7(2):20. PMID: 28212278; PMCID: PMC5332963. https://pmc.ncbi.nlm.nih.gov/articles/PMC5332963/
- Pickart L, Vasquez-Soltero JM, Margolina A. GHK Peptide as a Natural Modulator of Multiple Cellular Pathways in Skin Regeneration. Biomed Res Int. 2015;2015:648108. PMID: 26236730; PMCID: PMC4508379. https://pmc.ncbi.nlm.nih.gov/articles/PMC4508379/
- Beretta G, Arlandini E, Artali R, Anton JM, Maffei Facino R. Glycyl-histidyl-lysine (GHK) is a quencher of α,β-4-hydroxy-trans-2-nonenal: a comparison with carnosine. Insights into the mechanism of reaction by electrospray ionization mass spectrometry, 1H NMR, and computational techniques. Chem Res Toxicol. 2007;20(9):1309-1314. PMID: 17672515. https://pubmed.ncbi.nlm.nih.gov/17672515/
- Arul V, Kartha R, Jayakumar R. A therapeutic approach for diabetic wound healing using biotinylated GHK incorporated collagen matrices. Life Sci. 2007;80(4):275-284. PMID: 17049946. https://pubmed.ncbi.nlm.nih.gov/17049946/
- Gul NY, Topal A, Cangul IT, Yanik K. The effects of topical tripeptide copper complex and helium-neon laser on wound healing in rabbits. Vet Dermatol. 2008;19(1):7-14. PMID: 18177285. https://pubmed.ncbi.nlm.nih.gov/18177285/
- Min JH, Sarlus H, Harris RA. Glycyl-L-histidyl-L-lysine prevents copper- and zinc-induced protein aggregation and central nervous system cell death in vitro. Metallomics. 2024;16(5):mfae019. PMID: 38599632; PMCID: PMC11135135. https://pmc.ncbi.nlm.nih.gov/articles/PMC11135135/
- Li J, Zhang Q, Deng M, Bian Y, et al. The glycyl-L-histidyl-L-lysine-Cu2+ tripeptide complex attenuates lung inflammation and fibrosis in silicosis by targeting peroxiredoxin 6. Redox Biol. 2024;75:103237. PMID: 38879894. https://www.sciencedirect.com/science/article/pii/S2213231724002155
- Zhou XM, Wang GL, Wang XB, Liu L, Zhang Q, Yin Y, Wang QY, Kang J, Hou G. GHK Peptide Inhibits Bleomycin-Induced Pulmonary Fibrosis in Mice by Suppressing TGFβ1/Smad-Mediated Epithelial-to-Mesenchymal Transition. Front Pharmacol. 2017;8:904. PMID: 29311918; PMCID: PMC5733019. https://pmc.ncbi.nlm.nih.gov/articles/PMC5733019/
- Pickart L, Thaler MM. Tripeptide in human serum which prolongs survival of normal liver cells and stimulates growth in neoplastic liver. Nat New Biol. 1973;243(124):85-87. PMID: 4349963. https://pubmed.ncbi.nlm.nih.gov/4349963/
Educational and research-use disclaimer: This article is provided solely for scientific and educational purposes. GHK-Cu (copper tripeptide-1) is a cosmetic ingredient and is not approved by the FDA, EMA, or any comparable regulator for the treatment, cure, or prevention of oxidative stress or any other disease, and no human clinical efficacy against oxidative-stress endpoints has been demonstrated. The antioxidant evidence described here is in-vitro, ex-vivo, or preclinical animal data. Nothing here is medical advice or a recommendation for human use. Any legitimate investigation of this compound as an antioxidant medicine should occur within properly authorized preclinical or clinical research under appropriate oversight. Readers should consult qualified professionals and applicable regulations before making any decisions.