GHK-Cu — the copper(II) complex of the tripeptide glycyl-L-histidyl-L-lysine — is one of the most thoroughly studied small peptides in skin and wound-repair biology, with a research trail stretching back to its isolation from human plasma in 1973. It functions as both a copper-delivery vehicle and a signaling molecule that nudges connective tissue toward regeneration, remodeling collagen, quieting inflammation, and shifting gene expression toward younger, more reparative patterns. This guide walks through what GHK-Cu actually is, how it works at the molecular level, what the human and preclinical evidence honestly supports, and how it is handled — with a clear distinction between well-validated topical cosmetic use and the far less established injectable applications.
What Is GHK-Cu?
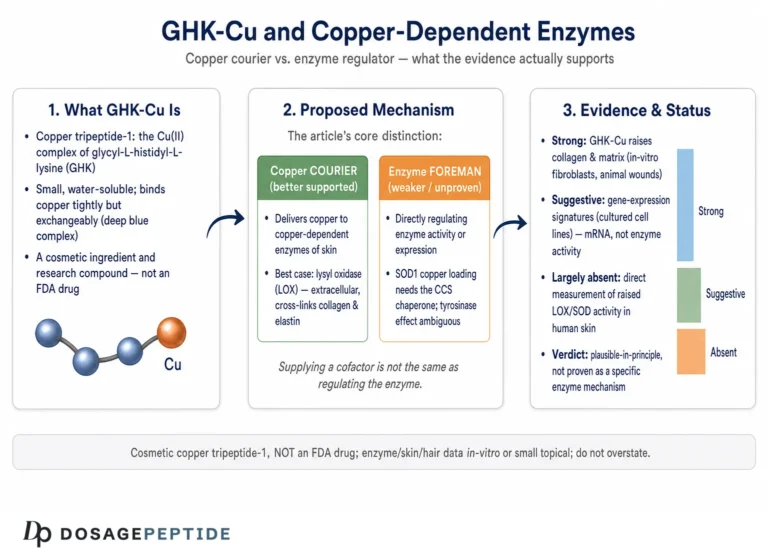
GHK-Cu is a naturally occurring complex formed when the tripeptide glycyl-L-histidyl-L-lysine (GHK) binds a copper(II) ion. The peptide itself is a chain of just three amino acids — glycine, histidine, and lysine — but the histidine imidazole and terminal amine groups create a near-perfect coordination geometry for copper, so GHK captures Cu2+ with an affinity comparable to that of albumin, the body’s main copper-transport protein.[1] In cosmetic labeling it appears under the International Nomenclature of Cosmetic Ingredients (INCI) name Copper Tripeptide-1; in pharmaceutical contexts it has been called prezatide copper acetate.
GHK is not a foreign or synthetic molecule. It is present in human plasma, saliva, and urine, and it was first identified in 1973 by biochemist Loren Pickart, who observed that a factor in human albumin caused aged liver tissue to synthesize proteins in the manner of younger tissue. That factor turned out to be the GHK tripeptide with its strong copper-binding activity.[1] A recurring theme in the literature is that GHK levels decline with age: plasma GHK is roughly 200 ng/mL (about 10−7 M) at age 20 and falls to approximately 80 ng/mL by age 60.[1] This decline coincides with the period in which the body’s capacity to repair skin, remodel connective tissue, and control inflammation begins to falter — a correlation that has driven much of the interest in restoring GHK-Cu externally.
Why Does the Copper Matter?
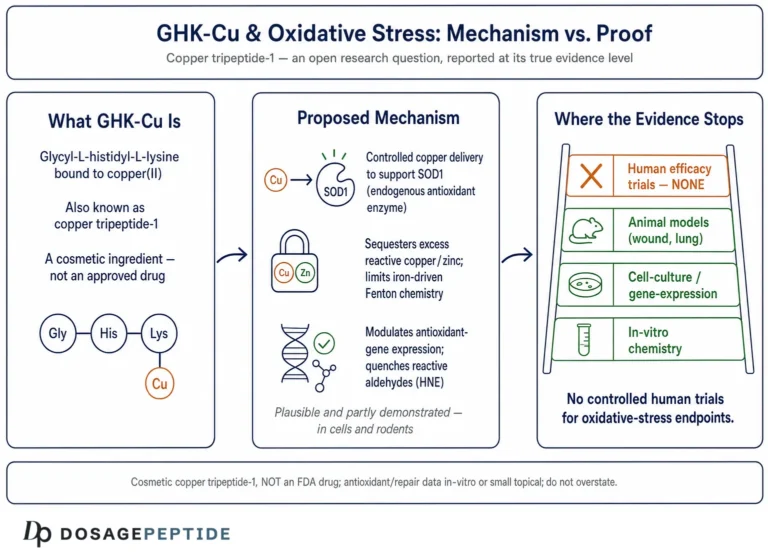
The copper in GHK-Cu is not incidental — it is central to the molecule’s biology. Copper is an essential trace metal and a cofactor for several “cuproenzymes” that skin and connective tissue depend on. The most important for repair is lysyl oxidase, the enzyme that cross-links collagen and elastin fibers to give tissue its tensile strength; without adequate copper, newly synthesized collagen cannot be properly stabilized.[2] Copper also participates in superoxide dismutase (SOD1), a frontline antioxidant enzyme. GHK acts as a copper chaperone, ferrying the ion in a bound, controlled form so it can be delivered where needed without generating the free-radical damage that loose, unbound copper can cause. In other words, the peptide gives the body a way to deliver a reactive metal safely, at the nanomolar concentrations where it signals rather than harms.
Because so many of GHK-Cu’s effects depend on copper delivery and copper-driven signaling, the copper-bound complex is generally more biologically active than the bare peptide. This is a key point of confusion for newcomers: GHK and GHK-Cu are related but not interchangeable, a distinction explored in more detail later in this guide. For readers who want to understand the practical numbers behind reconstituting and diluting research material, our peptide reconstitution guide and dosage calculator cover the concentration math referenced throughout this article.
How Was GHK-Cu Discovered?
The discovery of GHK-Cu is a story of scientific serendipity that continues to shape how the molecule is understood. In the early 1970s, Loren Pickart was studying why aged human liver tissue lost its capacity to synthesize proteins. He noticed that when old liver tissue was incubated with albumin from young donors (aged 20–25), it began synthesizing proteins like younger tissue — but albumin from older donors (aged 50–70) did not produce the same effect. This suggested that some factor present in young plasma, and diminished in older plasma, carried a “youth” signal for tissue function.[1]
Isolating and characterizing that factor revealed it to be the small tripeptide glycyl-L-histidyl-L-lysine, present at higher concentration in younger plasma. Crucially, later work established that GHK’s biological potency was tied to its copper-binding capacity — the peptide and copper together, as GHK-Cu, drove the reparative activity. This early framing of GHK-Cu as a marker and mediator of tissue-repair capacity that declines with age has proven durable: five decades of subsequent research have repeatedly returned to the same core theme of a copper-carrying, pro-regenerative signal that the body makes less of over time.
Where Is GHK Found in the Body?
GHK is an endogenous molecule, meaning the body produces it naturally. It circulates in plasma, and it also appears in saliva and urine.[1] One proposed source is the breakdown of larger proteins: during tissue injury and remodeling, proteolytic cleavage of matrix proteins such as collagen and SPARC (a matricellular protein) is thought to liberate GHK sequences locally at the site of damage. This is an elegant model — injury itself generates the very signal that helps orchestrate repair, releasing GHK where and when it is needed. It also helps explain why GHK-Cu has such coherent wound-healing biology: it is not an external drug imposing a foreign action, but a naturally released signal being supplied in greater quantity.
What Does GHK-Cu Look Like?
In solution, GHK-Cu is visibly blue — a direct consequence of the copper(II) coordination complex, which absorbs light in the red-orange part of the spectrum. This blue tint is a normal, expected property, not a sign of contamination or degradation. The complex has a molecular weight of roughly 403 daltons (the tripeptide itself is about 340 Da, with the copper ion adding the remainder). Its small size is one reason it is studied for topical delivery: at only three amino acids, it is far smaller than most bioactive peptides and can more plausibly interact with skin. A summary of its core physical identity appears in the properties table below.
What Are the Physical and Chemical Properties of GHK-Cu?
Understanding GHK-Cu’s basic identity helps distinguish legitimate research material from mislabeled products and clarifies how it is handled in the laboratory and in cosmetic formulation. The table below consolidates the peptide’s key attributes.
| Property | Detail |
|---|---|
| Common names / aliases | GHK-Cu, copper tripeptide-1 (INCI), prezatide copper acetate |
| Amino acid sequence | Glycyl-L-histidyl-L-lysine (Gly-His-Lys) complexed with Cu2+ |
| Molecular weight | ~403 Da (peptide ~340 Da + copper ion) |
| Year discovered | 1973, by Loren Pickart (isolated from human plasma) |
| Natural plasma levels | ~200 ng/mL at age 20 → ~80 ng/mL by age 60 |
| Solution appearance | Blue (from the copper(II) complex) |
| Primary studied route | Topical (serums, creams, gels) |
| Typical solvent | Distilled/sterile water, sometimes with glycerin, hyaluronic acid, or buffer (pH ~6–7) |
| Storage | Cool, dark, airtight; protect from light and heat |
How Is Concentration Expressed?
Cosmetic and research contexts often express GHK-Cu strength as a percentage (% w/v) or in mg/mL, and the two are easy to convert. The rule is simple: % w/v = (mg/mL) ÷ 10. So a solution at 10 mg/mL equals 1.0%, and 1 mg/mL equals 0.1%. If a 50 mg quantity is reconstituted in 10 mL of solvent, that yields 5 mg/mL, or a 0.5% w/v solution. These conversions matter because published cosmetic trials typically used low single-digit percentages, and understanding the math prevents both under- and over-concentration. Our dosage calculator automates these conversions, and the peptide glossary defines the reconstitution terminology used here.
How Does GHK-Cu Work? Mechanism of Action
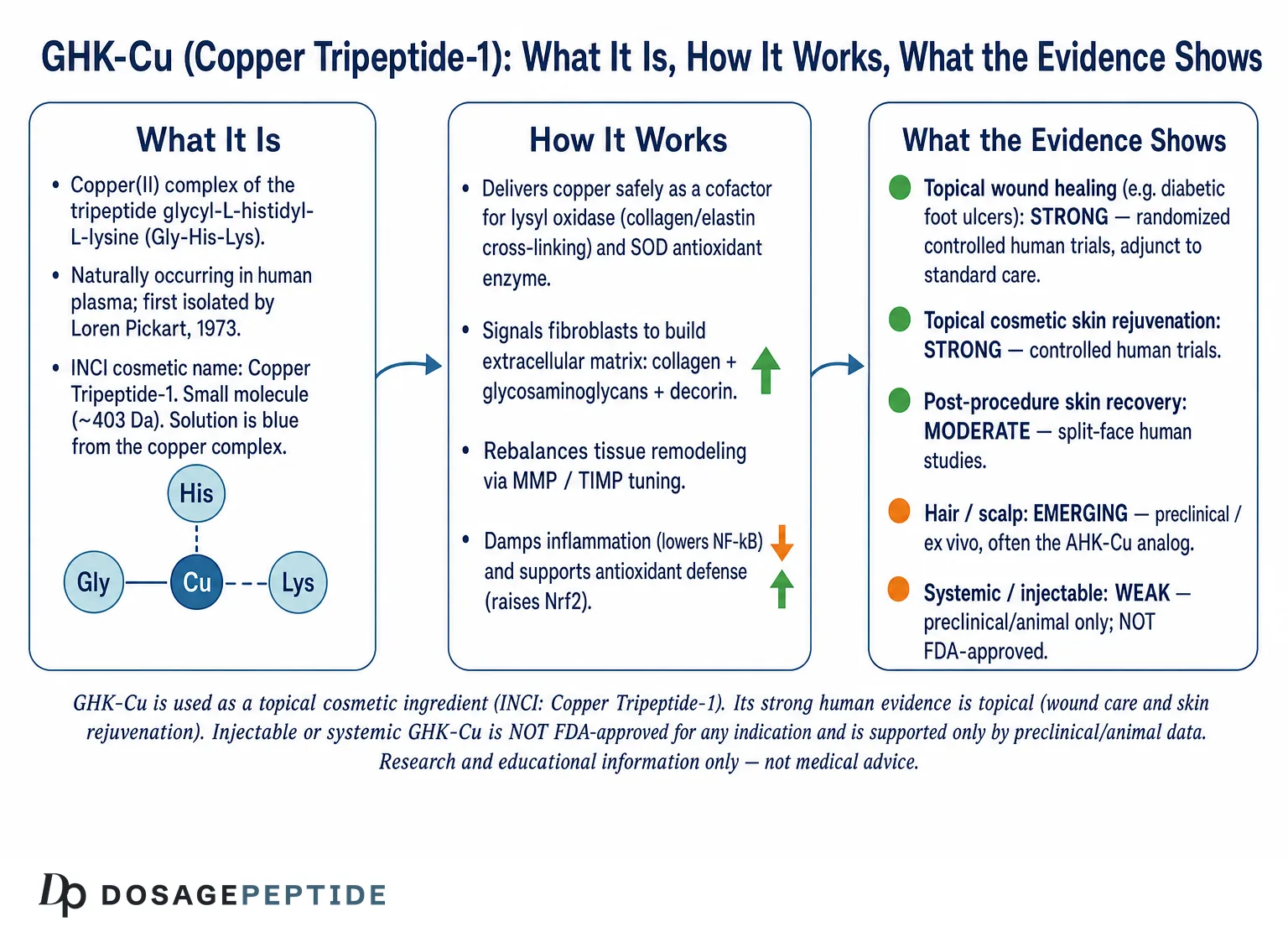
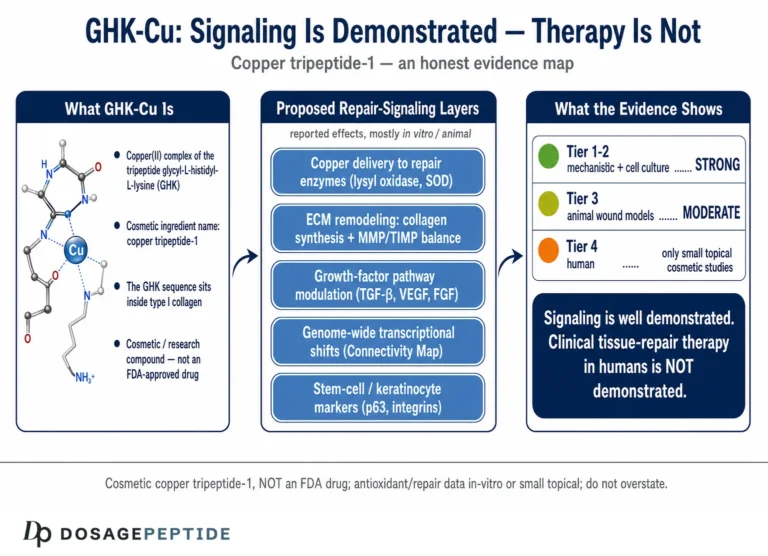
GHK-Cu does not act through a single receptor or pathway. Instead, the accumulated research describes a molecule that works on several fronts at once — delivering copper, stimulating new matrix, rebalancing tissue remodeling, damping inflammation and oxidative stress, and, most strikingly, altering the expression of a large fraction of human genes. The sections below unpack each of these mechanisms as they appear in the peer-reviewed literature.
Copper Delivery and Cuproenzyme Support
The foundational mechanism is copper transport. By binding Cu2+ tightly and delivering it in a controlled form, GHK-Cu supplies the metal cofactor that lysyl oxidase needs to cross-link collagen and elastin, and that SOD needs for antioxidant defense.[2] This is why GHK-Cu is often described as a “pro-repair signal” rather than a simple growth factor: it does not merely stimulate cells, it also ensures the raw material for durable, cross-linked tissue is available. The bound form matters here — free copper is pro-oxidant and can drive damaging Fenton chemistry, whereas peptide-chelated copper is delivered in a form the tissue can use safely.
Stimulating New Extracellular Matrix
Some of the earliest and most reproducible findings concern GHK-Cu’s ability to stimulate synthesis of the extracellular matrix (ECM). In a landmark 1988 study, Maquart, Pickart, and colleagues showed that GHK-Cu stimulated collagen synthesis in cultured fibroblasts at concentrations as low as 10−12 M, with a peak effect near 10−9 M, and independent of changes in cell number — meaning the cells were producing more collagen per cell, not simply proliferating.[1] The extraordinarily low effective concentrations are worth pausing on: at 10−12 M, GHK-Cu is acting at picomolar levels, far below where a nutrient or bulk building block would register. This is the hallmark of a signaling molecule — it instructs cells rather than feeding them, which is consistent with the idea that GHK-Cu is an endogenous regulatory peptide rather than merely a copper supplement.
Later work extended this to the wider matrix. GHK-Cu increases production of glycosaminoglycans such as dermatan sulfate and chondroitin sulfate, and it upregulates decorin, a small proteoglycan that organizes collagen fibrils into orderly, mechanically sound bundles.[3] Decorin is especially important: rather than simply adding more collagen, it governs how collagen fibrils are spaced and bundled, which determines whether tissue heals as smooth, functional dermis or as disorganized scar. By upregulating decorin alongside collagen, GHK-Cu supports the architecture of repair, not just its raw quantity. Glycosaminoglycans, meanwhile, bind large amounts of water and give the dermis its plumpness and resilience, so their increase contributes directly to the improvements in skin density and firmness seen in cosmetic trials. The net result is not just more collagen, but better-structured, better-hydrated connective tissue.
GHK-Cu also influences the cells that build and maintain the matrix. It has been described as promoting the differentiation and activity of fibroblasts, and it supports angiogenesis — the formation of new blood vessels — which is essential for delivering oxygen and nutrients to healing tissue.[3] In wound settings, it is also chemotactic, attracting the immune and repair cells that clear debris and coordinate rebuilding. This combination — matrix synthesis, vascular support, and cell recruitment — is why GHK-Cu is characterized as a comprehensive pro-repair signal rather than a single-pathway agent.
Rebalancing Tissue Remodeling: MMPs and TIMPs
Healthy tissue repair is a two-way process: old, damaged matrix must be cleared while new matrix is laid down. That balance is governed by matrix metalloproteinases (MMPs), which break down matrix, and their counterweights, the tissue inhibitors of metalloproteinases (TIMPs). GHK-Cu modulates this system — influencing MMP-2 and TIMP levels — to favor constructive remodeling rather than uncontrolled degradation.[1] This dual capacity is what makes the peptide interesting: rather than simply switching matrix breakdown on or off, GHK-Cu appears to tune the system toward whatever the tissue needs. In a photoaged or chronically wounded context, where excess, poorly regulated MMP activity chews up healthy matrix, that means restraining degradation; in a stagnant wound that needs debris cleared, it means enabling controlled turnover.
The practical implication is that GHK-Cu appears to steer wounds and aging skin toward organized turnover instead of either matrix breakdown (as in chronic wounds and photoaging) or excessive, disorganized deposition (as in fibrosis and scarring). This anti-scarring, pro-remodeling character distinguishes GHK-Cu from cruder growth-factor approaches: the goal is not maximal tissue deposition but well-organized, functional tissue. It is also consistent with reports that GHK-Cu supports remodeling of existing scar tissue toward a more normal architecture, though this remains an area where cell-model and animal data outpace controlled human trials.
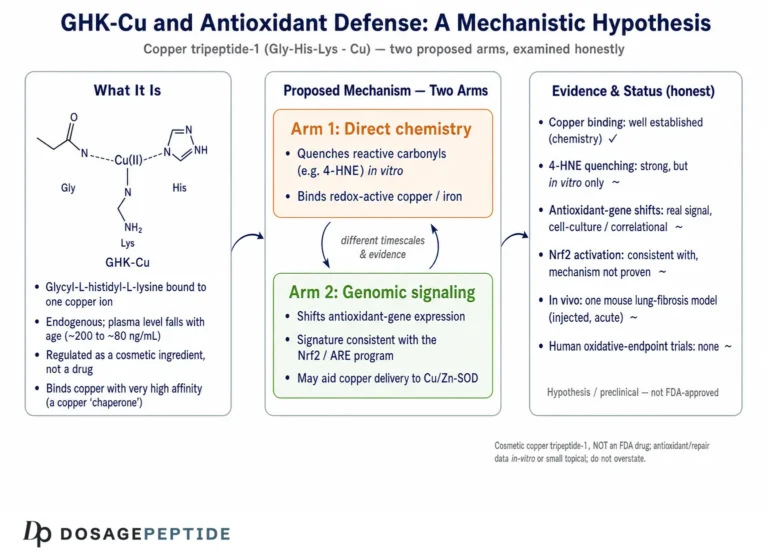
Antioxidant and Anti-Inflammatory Signaling
GHK-Cu also acts on inflammation and oxidative stress, two drivers of both impaired healing and skin aging. In dermal fibroblasts, it can reduce the output of inflammatory mediators, and in a rigorous 2022 lung model, GHK-Cu attenuated cigarette-smoke-induced emphysema by reducing NF-κB activation, lowering inflammatory cytokines including IL-1β and TNF-α, and raising the antioxidant regulator Nrf2.[2] These two named pathways are central to why the finding matters. NF-κB is a master switch for inflammatory gene expression; turning it down calms the cascade at its source rather than merely mopping up downstream mediators. Nrf2, conversely, is the master regulator of the cell’s endogenous antioxidant response, controlling the genes that produce protective enzymes; raising Nrf2 activity means the tissue defends itself more effectively against oxidative damage.
While that study is in lung tissue rather than skin, it illustrates a coherent anti-inflammatory, antioxidant signature that recurs across GHK-Cu research: it tempers inflammatory signaling without broad immunosuppression, and it supports the body’s own antioxidant machinery rather than acting purely as a sacrificial radical scavenger. This distinction is meaningful for skin biology, because chronic low-grade inflammation and cumulative oxidative stress from ultraviolet light are two of the principal engines of skin aging. A molecule that both quiets NF-κB-driven inflammation and boosts Nrf2-driven antioxidant defense is, in principle, addressing aging at a mechanistic level rather than cosmetically masking it — though, again, the skin-specific human confirmation of these particular pathways remains thinner than the wound and cosmetic outcome data.
Gene Expression: Resetting Tissue Toward Repair
Perhaps the most remarkable mechanistic finding is GHK’s breadth of action on gene expression. Using data from the Broad Institute’s Connectivity Map — a large reference database that catalogs how thousands of compounds alter gene-expression patterns in human cells — researchers found that GHK shifts the expression of a strikingly large share of human genes, on the order of ~30% of the genome up or down by more than 50%, broadly in a direction associated with tissue repair and a younger cellular profile.[4] That figure is dramatic and deserves careful interpretation: it does not mean GHK “controls” a third of the genome, but rather that its downstream signaling ripples widely, resetting many interlocking programs toward repair. It is precisely the kind of broad, network-level effect one would expect from a molecule that coordinates something as complex as tissue regeneration.
A collaborative study across several universities showed a concrete example: GHK could reverse gene-expression signatures characteristic of chronic obstructive pulmonary disease (COPD), turning down genes tied to inflammation and turning up genes involved in tissue remodeling and repair.[1] Other analyses have connected GHK to gene programs relevant to DNA repair, antioxidant defense, and the ubiquitin-proteasome system that clears damaged proteins.[4] This gene-modulating capacity is a plausible unifying explanation for why a single small peptide shows effects across so many tissue types: it is not doing one thing, but nudging many reparative programs at once. The important caveat is that a gene-expression signature is a molecular observation, not a clinical outcome — it tells us what a molecule might do, and points research in productive directions, without proving benefit in living people.
Synergy With Hyaluronic Acid
GHK-Cu is frequently combined with hyaluronic acid (HA) in commercial formulations, and there is a mechanistic rationale beyond marketing. In skin models, GHK-Cu paired with HA can synergistically increase multiple collagen types (I, IV, and VII), supporting both the dermal matrix and the dermal-epidermal junction. HA also provides humectant hydration and barrier support, complementing GHK-Cu’s matrix-building action. This is why many well-designed serums list both ingredients — and why blends that combine GHK-Cu with other reparative peptides, such as the components discussed in our KLOW 80 mg vial dosage protocol, are of interest for research.
What Does the Evidence Actually Show?
Honesty about evidence level is essential with GHK-Cu, because the peptide is genuinely well-characterized in some areas and only preliminary in others. The strongest human data supports topical use for wound healing and cosmetic skin rejuvenation. Hair applications rest largely on analogs and preclinical models. And systemic or injectable uses — despite enthusiastic online claims — are the least validated and are not approved by regulators. The sections below grade each application by the quality of evidence behind it.
Chronic Wound Healing (Strongest Human Evidence)
The most robust clinical evidence for GHK-Cu is in chronic wounds, particularly diabetic foot ulcers — a notoriously difficult-to-heal condition where impaired circulation, neuropathy, and dysregulated inflammation combine to stall the normal repair cascade. In a multicenter, randomized, controlled clinical trial, a topical GHK-Cu preparation used adjunctively to standard care produced faster healing than placebo, with the rate of healing significantly quicker (p<0.01).[1] Supporting studies with 2% GHK-Cu gel have reported markedly faster wound closure versus vehicle control. The importance of this evidence lies in its design: randomized, controlled, and multicenter trials are the gold standard for separating a genuine treatment effect from placebo response and natural healing, and it is precisely this level of rigor that elevates GHK-Cu’s wound-care claims above the anecdotal.
The mechanistic picture aligns tightly with the clinical outcome, which is part of why this evidence is persuasive. GHK-Cu is chemotactic for the monocytes, macrophages, and mast cells that orchestrate the healing cascade, drawing these coordinating cells into the wound. It stimulates angiogenesis, restoring the blood supply that chronic wounds so often lack. And it drives the collagen and glycosaminoglycan synthesis needed to rebuild the wound bed, while its MMP/TIMP modulation helps clear the excess proteolytic activity that keeps chronic wounds stuck in a destructive loop.[3] When a molecule’s cell-level actions predict its clinical results, confidence in the finding grows. Importantly, clinical wound care with GHK-Cu should occur under professional supervision, as chronic ulcers require comprehensive management — debridement, infection control, offloading of pressure, and glycemic control — of which any topical agent is only one component.
Cosmetic Skin Rejuvenation (Strong Human Evidence)
Topical GHK-Cu has meaningful human data in cosmetic dermatology. The most-cited trial is a 12-week, randomized study of a GHK-Cu facial cream in women with photoaged skin, in which twice-daily application increased skin density and thickness, reduced fine lines and wrinkle depth, improved skin laxity and clarity, and reduced mottled pigmentation.[5] What makes this study valuable is the breadth of endpoints improved simultaneously: firmness and density reflect deep dermal matrix changes, while clarity and pigmentation reflect surface renewal — together suggesting that GHK-Cu acts at multiple layers of the skin rather than producing a single superficial effect.
A companion study of a GHK-Cu eye cream reported improvements in periorbital lines and skin density that compared favorably to both placebo and a vitamin K comparator — a meaningful benchmark, since the delicate periorbital area is where photoaging shows early and where many ingredients underperform. These findings are consistent with GHK-Cu’s ECM-building mechanism: over weeks of consistent use, the collagen and glycosaminoglycan stimulation that shows up in cell culture appears to translate into measurable improvements in skin firmness and texture.[1] The consistency between mechanism (matrix synthesis in the dish) and outcome (firmer, denser skin in trials) is exactly the kind of concordance that lends credibility to a cosmetic ingredient, in contrast to the many actives whose marketing claims outrun their controlled evidence. It is worth noting that cosmetic trials are typically smaller and shorter than pharmaceutical studies, so while the GHK-Cu cosmetic data is genuine and encouraging, it sits a notch below the level of a large drug-registration trial.
Post-Procedure Skin Recovery (Human Evidence)
GHK-Cu has been studied as an aid to recovery after aesthetic procedures. Randomized split-face designs — in which one side of a patient’s face receives the active and the other a control, eliminating between-subject variability — have examined copper tripeptide complexes applied after ablative procedures such as CO2 laser resurfacing, with reports of improved healing and cosmetic appearance.[5] The rationale mirrors the wound-healing evidence: after a controlled injury like laser resurfacing, a pro-repair, anti-inflammatory signal can plausibly support faster, cleaner recovery. As with all post-procedure care, this should be guided by the treating clinician.
Hair and Scalp (Emerging, Preclinical)
Hair is where enthusiasm most often outruns evidence. The relevant data is largely preclinical and frequently involves the related analog AHK-Cu rather than GHK-Cu itself. In a 2007 study, AHK-Cu at 10−12 to 10−9 M stimulated proliferation of dermal papilla cells and elongated human hair follicles ex vivo.[5] Dermal papilla cells sit at the base of the follicle and act as its command center, directing the hair-growth cycle, so a molecule that boosts their proliferation is mechanistically plausible as a hair-support agent. A 2018 study reported that GHK-Cu increased follicle size and proliferation markers (PCNA staining) in ex vivo human follicle tissue versus vehicle.[1]
These are encouraging mechanistic signals, but the crucial limitation is the phrase “ex vivo” — the work was done on isolated follicles or cells outside the body, where a compound can be applied directly to the target tissue at controlled concentrations. Real scalps are a far harsher test: the ingredient must penetrate skin, reach the follicle at an effective concentration, and outperform placebo across many people. Human clinical trials powered for hair-density endpoints are lacking, which is the decisive gap. Copper peptides should therefore be regarded as a possible adjunct for scalp health, not a substitute for therapies with robust randomized evidence such as minoxidil and finasteride. Anyone experiencing meaningful hair loss is better served by starting with the proven standards and treating copper peptides as an optional add-on. For related blend research framed in the same educational manner, see our GHK-Cu 50 mg vial dosage protocol.
Systemic and Injectable Use (Least Validated, Not Approved)
This is the most important caveat in the entire GHK-Cu picture. The strong evidence base for GHK-Cu is topical. Injectable or systemic administration of GHK-Cu is not approved by the FDA for any indication, and the human evidence for such routes is minimal to nonexistent. Much of the excitement about systemic anti-aging, organ-repair, or lung-protective effects derives from cell-culture experiments, gene-expression analyses, and animal models — valuable for hypothesis generation, but not the same as demonstrated safety and efficacy in people. Any discussion of injectable GHK-Cu, including single-vial research material like the products described in our GHK-Cu 50 mg vial dosage protocol and GHK-Cu 100 mg vial dosage protocol, belongs strictly in a research and educational frame — not clinical practice. Copper homeostasis is tightly regulated in the body, and introducing copper-peptide complexes systemically raises questions about copper balance that topical, localized use largely sidesteps.
| Application | Evidence level | Route | Interpretation |
|---|---|---|---|
| Chronic wound healing | Strong (RCT, human) | Topical gel | Adjunct to standard care, clinician-supervised |
| Cosmetic rejuvenation | Strong (controlled human trials) | Topical cream/serum | Established cosmetic benefit with consistent use |
| Post-procedure recovery | Moderate (split-face human) | Topical | Supports healing after resurfacing procedures |
| Hair/scalp | Emerging (preclinical, analogs) | Topical | Possible adjunct; not proven vs. standard care |
| Systemic / injectable | Weak (preclinical only) | Injection | Not FDA-approved; research/educational only |
What Is the Difference Between GHK and GHK-Cu?
A common source of confusion is the relationship between the bare peptide and the copper complex. GHK is the tripeptide alone — glycyl-L-histidyl-L-lysine, three amino acids with no metal. GHK-Cu is that same peptide with a copper(II) ion bound to it. Because GHK has such a high natural affinity for copper, the two forms interconvert readily in biological fluids, and in the body GHK will readily pick up available copper to form the complex.[1]
For most of the effects that matter — collagen synthesis, lysyl oxidase activation, cuproenzyme support, wound healing — the copper is required or the effect is substantially stronger with it, because so much of GHK’s biology is really copper-delivery biology. That said, gene-expression studies suggest the bare peptide also carries signaling information of its own. The practical takeaway: when research or a cosmetic formulation refers to the reparative, matrix-building actions people associate with “copper peptides,” it is generally the copper-bound GHK-Cu complex that is doing the work.
How Does GHK-Cu Compare to Other Skin and Hair Actives?
GHK-Cu does not exist in a vacuum. Understanding where it sits relative to retinoids, minoxidil, and its own analog AHK-Cu clarifies when it is the right tool and when it is better used as a complement. The table below summarizes the landscape; the key theme is that GHK-Cu is strongest for skin repair and rejuvenation, and works best alongside — not in place of — proven standards for photoaging and hair loss.
| Active | Primary action | Evidence strength | Best suited for |
|---|---|---|---|
| GHK-Cu (copper tripeptide-1) | Collagen/GAG synthesis, MMP/TIMP balance, copper delivery, anti-inflammatory | Strong for topical wound care & cosmetics | Skin rejuvenation, wound care, post-procedure |
| AHK-Cu (analog) | Dermal papilla activation, follicle support | Preclinical / ex vivo | Hair & scalp cosmetics (adjunct) |
| Retinoids (tretinoin/retinol) | Accelerate turnover, collagen I/III synthesis | Strong (especially Rx tretinoin) | Photoaging, deep wrinkles |
| Minoxidil | Vasodilation, prolongs anagen phase | Robust RCT evidence | Pattern hair loss (proven) |
When Is GHK-Cu the Right Choice Versus an Alternative?
Because GHK-Cu, retinoids, and minoxidil have different strengths, the practical question is rarely “which single ingredient is best” but “which tool fits the problem.” For someone whose primary concern is skin firmness, texture, thin or crepey skin, and post-procedure or wound recovery, GHK-Cu is a strong, well-supported choice, and its gentle, anti-inflammatory profile makes it suitable even for sensitive skin that cannot tolerate retinoids. For deep wrinkles and established photoaging, prescription tretinoin remains the most evidence-backed option, and GHK-Cu is best used as a complementary agent that adds matrix support and calms the irritation retinoids often cause. For pattern hair loss, minoxidil and finasteride have the randomized-trial track record; copper peptides are, at most, an adjunct.
The recurring theme is that GHK-Cu is a collaborator, not a rival, to these standards. Its multi-pathway, pro-repair, anti-inflammatory character means it tends to complement rather than duplicate the more aggressive, single-mechanism actives — adding barrier and matrix support that helps skin tolerate and benefit from the proven workhorses. This is why so many thoughtfully designed regimens pair GHK-Cu with a retinoid or with hyaluronic acid rather than treating it as a standalone miracle.
Can GHK-Cu Be Combined With Retinoids and Vitamin C?
Yes, though pacing matters more than incompatibility. There is no strong evidence of a chemical clash that would render GHK-Cu inert when used with retinoids or vitamin C, but combining several potent actives at once can irritate skin. A common approach is to stagger applications — for example, GHK-Cu on alternate nights from a retinoid, or vitamin C in the morning and GHK-Cu in the evening — which reduces irritation while letting the user observe each active’s effect. Pairing GHK-Cu with hyaluronic acid supports hydration and barrier function, and daily broad-spectrum SPF remains non-negotiable when using any collagen-oriented regimen, since ultraviolet exposure directly degrades the matrix these ingredients are meant to build.
How Is GHK-Cu Handled? Formulation, Stability, and Storage
GHK-Cu is relatively forgiving to handle compared to larger, more fragile peptides, but it still benefits from sensible storage. The blue copper complex is sensitive to light and heat over time, so material should be kept cool, dark, and airtight. In finished cosmetic formulations, GHK-Cu is typically dissolved in water, often alongside glycerin, hyaluronic acid, or a mild buffer to hold pH in the roughly 6–7 range where the complex is stable. When working from lyophilized (freeze-dried) material, the standard practice is reconstitution in sterile or bacteriostatic water; the concentration math (% w/v = mg/mL ÷ 10) then determines the working strength. Our reconstitution guide details these steps for research handling.
What Should a Buyer or Formulator Check?
Quality control separates credible material from mislabeled or degraded product. A practical checklist:
- Verify identity and purity by requesting a Certificate of Analysis (COA) with identity tests such as HPLC and mass spectrometry.
- Confirm the label — on cosmetics, look for the INCI name “Copper Tripeptide-1” rather than vague “copper peptide” language.
- Match the vehicle to the goal — a serum or cream with hyaluronic acid suits drier skin, while a lighter serum suits oily skin or scalp use.
- Mind the concentration using the % w/v conversion, and patch-test before broad application.
- Check color and stability — a blue tint is normal; store cool, dark, and airtight, and discard material that has changed markedly in appearance.
- Stack thoughtfully — separate strong actives by time of day if skin is sensitive, and always use daily SPF.
- Track results — monthly photos under consistent lighting, with a log of any irritation and visible improvements.
How Is Topical GHK-Cu Typically Used?
For the topical, cosmetic applications where the evidence is strongest, using GHK-Cu well is more about consistency and sensible layering than about chasing high concentrations. Because the peptide works by signaling fibroblasts over time to rebuild matrix, its benefits accrue over weeks and months, not days. Understanding a reasonable routine helps set realistic expectations.
What Concentration and Frequency Are Reasonable?
Published cosmetic trials that demonstrated benefit used modest concentrations, generally in the low single-digit percentage range, applied consistently over 12 weeks.[5] This is a useful anchor: it means a well-formulated serum at around 1–2% copper tripeptide-1, used once or twice daily, is broadly in line with what produced measurable results in studies. Higher is not reliably better, and very high concentrations may increase the risk of irritation without a proportional gain in benefit. The sensible pattern is to start low, apply consistently, and give the regimen the full multi-week window that the underlying biology requires.
How Should GHK-Cu Be Layered in a Routine?
GHK-Cu is generally applied to clean skin, before heavier occlusive creams, so it can reach the skin surface unimpeded. A practical sequence is cleanser, then GHK-Cu serum, then moisturizer, with sunscreen as the final morning step. Because copper peptides and direct-acid vitamin C formulations can theoretically interfere with each other when layered simultaneously, many users separate them — vitamin C in the morning, GHK-Cu in the evening — which sidesteps the question entirely while preserving both actives’ benefits. The same time-separation logic applies to retinoids, which are potent enough on their own that pairing them with GHK-Cu on alternate nights is often gentler than stacking them nightly.
How Long Until Results Appear?
Realistic timelines matter for both satisfaction and honest expectation. Since the trials that measured firmness, density, and fine-line improvements ran for about 12 weeks, that is a reasonable minimum window before judging whether GHK-Cu is helping.[5] Some users notice improved texture and hydration sooner, but the deeper matrix changes — the ones responsible for firmness and density — take time because collagen remodeling is inherently slow. Tracking with monthly photos under consistent lighting is the most reliable way to see genuine change, which is easy to miss day to day. If no benefit is apparent after a consistent three-month trial, it is reasonable to reassess the product or approach.
Is GHK-Cu Safe? Risks and Tolerability
Topical GHK-Cu has a generally favorable tolerability record across cosmetic and clinical studies. Because the peptide binds copper tightly, it limits the free-copper reactivity that would otherwise be a concern, delivering the metal in a controlled form rather than as loose, pro-oxidant ions.[1] Still, no active is universally tolerated. The most common issues with topical use are localized: mild irritation, redness, or contact sensitivity in a minority of users, which is why patch-testing before first full use is prudent and irritation should prompt discontinuation.
Several safety points deserve emphasis. First, concentration discipline matters — higher is not automatically better, and the cosmetic trials that showed benefit used modest single-digit percentages. Second, chronic wound care should be clinician-supervised, since ulcers require comprehensive management that goes far beyond any single topical agent. Third, and most consequentially, the injectable and systemic routes are not FDA-approved and carry an evidence gap: the reassuring safety data applies to topical, localized use, and cannot simply be transferred to injection. Anyone considering GHK-Cu should also account for individual factors — pregnancy, breastfeeding, known copper-metabolism disorders such as Wilson’s disease, and interactions with other actives — and consult a qualified healthcare professional. Nothing in this article is medical advice.
What About Copper Overload?
A reasonable question is whether repeated GHK-Cu use could cause copper accumulation. For topical cosmetic use, the delivered copper quantities are small and localized, and the peptide-bound form limits systemic uptake, so copper overload is not a recognized concern at cosmetic concentrations. The calculus is different for hypothetical systemic dosing, where the body’s tightly regulated copper homeostasis becomes directly relevant — another reason the injectable route remains poorly justified outside controlled research. People with disorders of copper metabolism should be especially cautious and seek professional guidance before using any copper-containing product.
What Is the Broader Research Context for GHK-Cu?
Beyond skin and wounds, GHK-Cu appears throughout an expanding preclinical literature that hints at broader regenerative and protective roles — while remaining, importantly, preclinical. Investigators have reported GHK-Cu effects on nerve tissue regeneration and angiogenesis, on gene-expression programs relevant to nervous-system function and cognitive decline, and, as noted, on lung tissue in emphysema and COPD models where it reduced oxidative stress and inflammatory signaling.[2] The gene-expression work — showing GHK can shift a large fraction of the genome toward a more youthful, reparative pattern — provides a coherent thread connecting these disparate observations.[4]
The honest framing is that this breadth is scientifically fascinating and worth continued study, but it is not a license to extrapolate to human systemic therapy. A gene-expression signature reversed in a dish, or emphysema attenuated in a rodent, is a starting point for research, not proof of a treatment. The gap between a promising preclinical signal and a validated human therapy is where the majority of candidate compounds fail — often because effects that look robust in isolated cells or animal models do not survive the complexity, dosing constraints, and safety requirements of human physiology. GHK-Cu’s translated, human-validated value therefore remains anchored where the controlled trials are: topical wound healing and cosmetic skin rejuvenation.
This is also why the distinction between topical and systemic use is not pedantry but the central practical fact about GHK-Cu. The rich preclinical literature on nerve regeneration, cognition, and lung protection describes what the molecule can do to cells and tissues under experimental conditions. It does not establish that injecting or systemically dosing GHK-Cu in a human is safe, effective, or wise — and no regulator has concluded that it is. Readers encountering enthusiastic claims about GHK-Cu as a systemic anti-aging or organ-repair therapy should recognize those claims as extrapolations from mechanism, not conclusions from human trials. For readers exploring the wider peptide landscape, our peptide glossary provides definitions and context for the terminology used across this and related research areas, and the GHK-Cu 100 mg vial dosage protocol page frames larger research quantities within that same educational context.
The Bottom Line on GHK-Cu
GHK-Cu is a credible, well-studied skin-repair signal with a rare combination of deep mechanistic understanding and real human data. It delivers copper safely, stimulates collagen and glycosaminoglycan synthesis, rebalances matrix remodeling through the MMP/TIMP system, damps inflammation and oxidative stress, and shifts gene expression toward repair. The strongest, most trustworthy evidence sits in topical wound care and cosmetic rejuvenation; post-procedure recovery has moderate support; hair applications are promising but preliminary; and systemic or injectable use remains unapproved and poorly validated. Used as intended — topically, at sensible concentrations, with quality-verified material, and as an adjunct rather than a replacement for proven therapies — GHK-Cu is one of the better-supported peptides in the regenerative-skincare toolkit. As always, treat this as research and educational information, not medical advice, and consult a qualified professional before acting on it.
Frequently Asked Questions
What is GHK-Cu?
GHK-Cu is the copper(II) complex of the tripeptide glycyl-L-histidyl-L-lysine, a molecule that naturally occurs in human plasma, saliva, and urine and declines with age. It acts as a copper carrier and pro-repair signal, boosting collagen and glycosaminoglycan synthesis, balancing matrix-remodeling enzymes, and tempering inflammation. It was first isolated by Loren Pickart in 1973.
How does GHK-Cu help the skin?
GHK-Cu stimulates fibroblasts to produce more collagen and glycosaminoglycans, upregulates decorin to organize collagen fibrils, and balances MMPs and TIMPs so tissue turns over in a constructive way. In controlled human trials, twice-daily topical use over 12 weeks improved skin density, firmness, clarity, and fine-line depth, consistent with its matrix-building mechanism.
Does GHK-Cu regrow hair?
The evidence for hair is preliminary and largely preclinical, often using the related AHK-Cu analog. Ex vivo studies show follicle elongation and dermal papilla cell proliferation, but human trials powered for hair-density outcomes are lacking. Copper peptides are best considered an adjunct for scalp health, not a proven replacement for minoxidil or finasteride.
Is GHK-Cu safe?
Topical GHK-Cu is generally well-tolerated in cosmetic and clinical studies, and its tight copper binding limits free-copper reactivity. The most common issues are mild local irritation or sensitivity, so patch-testing first is wise. Injectable and systemic use is not FDA-approved and carries an evidence gap; chronic wound care should be clinician-supervised. This is not medical advice.
What is the difference between GHK and GHK-Cu?
GHK is the bare tripeptide of three amino acids, while GHK-Cu is that peptide bound to a copper(II) ion. Because GHK has a high affinity for copper, the two interconvert readily in the body. Most of the reparative effects — collagen synthesis, lysyl oxidase activation, wound healing — require copper or are substantially stronger with the copper complex.
Is injectable GHK-Cu approved?
No. The FDA has not approved GHK-Cu for injectable or systemic use in any indication. The strong human evidence for GHK-Cu is topical — wound care and cosmetics. Claims about systemic anti-aging or organ-repair effects derive from cell-culture and animal studies, which are hypothesis-generating, not proof of safety or efficacy in people. Injectable use should be treated as research only.
Can GHK-Cu be combined with retinoids or vitamin C?
Yes, but pace the actives to avoid irritation. There is no strong evidence of chemical incompatibility, but layering several potent ingredients can stress the skin. Staggering applications — alternating nights, or morning versus evening — reduces irritation while letting you observe each active’s effect. Pairing with hyaluronic acid supports hydration, and daily SPF is essential.
Why is GHK-Cu solution blue?
The blue color comes directly from the copper(II) coordination complex, which absorbs light in the red-orange range and transmits blue. This tint is a normal, expected property of properly formed GHK-Cu, not a sign of contamination. A marked change away from the characteristic blue can, however, indicate degradation, which is why cool, dark, airtight storage is recommended.
References
- Pickart L, Margolina A. Regenerative and Protective Actions of the GHK-Cu Peptide. GHK Peptide as a Natural Modulator of Multiple Cellular Pathways in Skin Regeneration. Biomed Res Int / PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC4508379/
- Glycyl-L-histidyl-L-lysine-Cu2+ attenuates cigarette smoke-induced pulmonary emphysema and inflammation by reducing oxidative stress pathway. Front Mol Biosci / PMC. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9354777/
- Simeon A, et al. Expression of Glycosaminoglycans and Small Proteoglycans in Wounds: Modulation by the Tripeptide-Copper Complex Glycyl-L-Histidyl-L-Lysine-Cu2+. J Invest Dermatol. https://www.sciencedirect.com/science/article/pii/S0022202X1541067X
- Pickart L, Vasquez-Soltero JM, Margolina A. GHK and DNA: Resetting the Human Genome to Health. Biomed Res Int / PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC4180391/
- Copper Tripeptide GHK-Cu and Regenerative Aesthetics. PRIME Journal. https://www.prime-journal.com/copper-tripeptide-ghk-cu-and-regenerative-aesthetics/