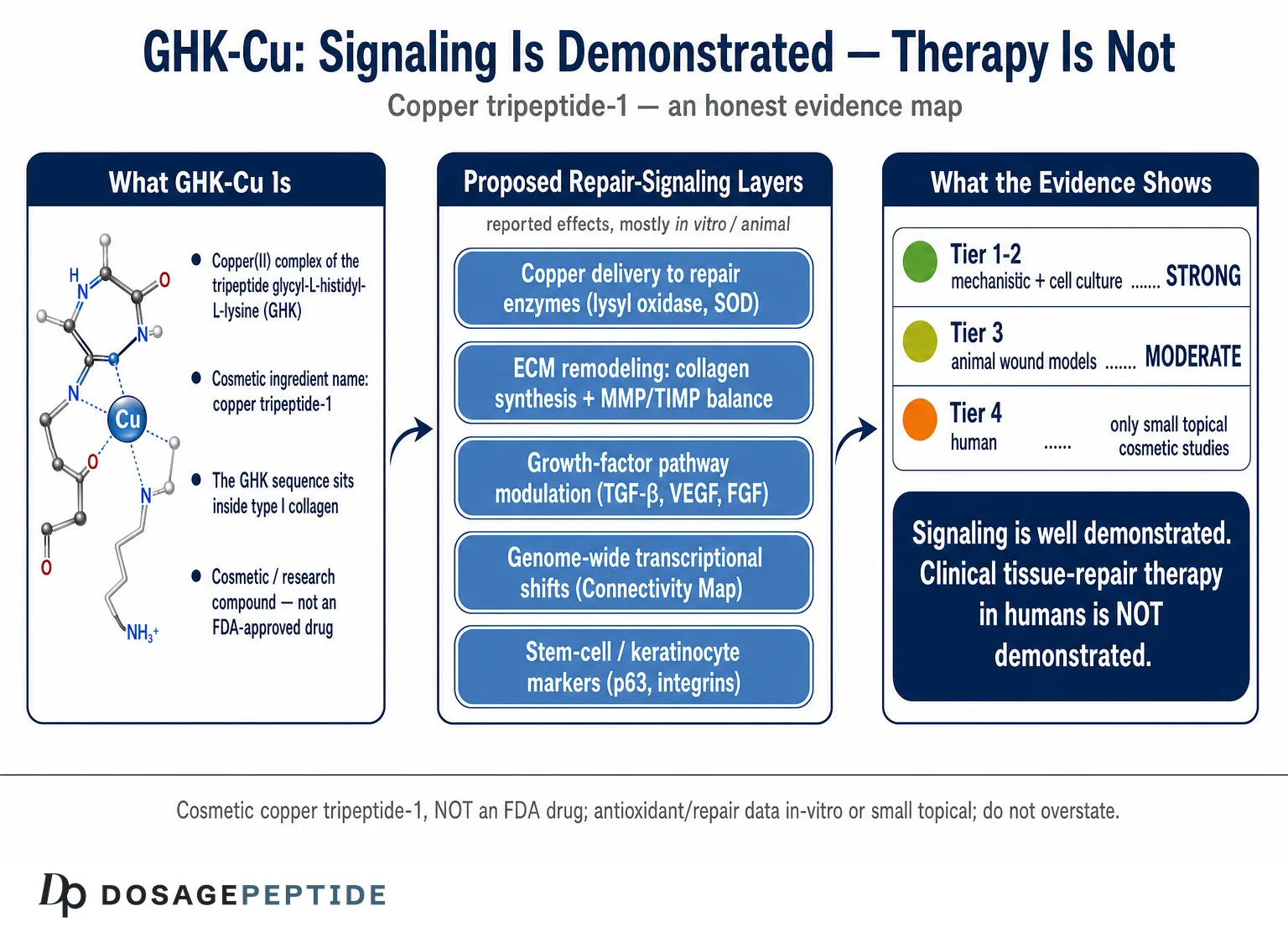
The verb in this question — whether the evidence “demonstrates” GHK-Cu’s role in tissue repair signaling — deserves scrutiny before we accept it. “Demonstrates” is a strong word. In pharmacology it usually implies a proven, reproducible, clinically meaningful effect. For GHK-Cu, the honest picture is more layered than that single word allows. At the level of molecular and cellular signaling — what genes it switches on, what matrix proteins fibroblasts make in a dish, what happens in a rodent wound — the evidence is genuinely substantial and, in places, quite elegant. At the level of demonstrated therapeutic tissue repair in humans, the evidence thins out dramatically and consists mostly of small cosmetic topical studies. Both statements are true at once, and separating them is the whole task of this article.
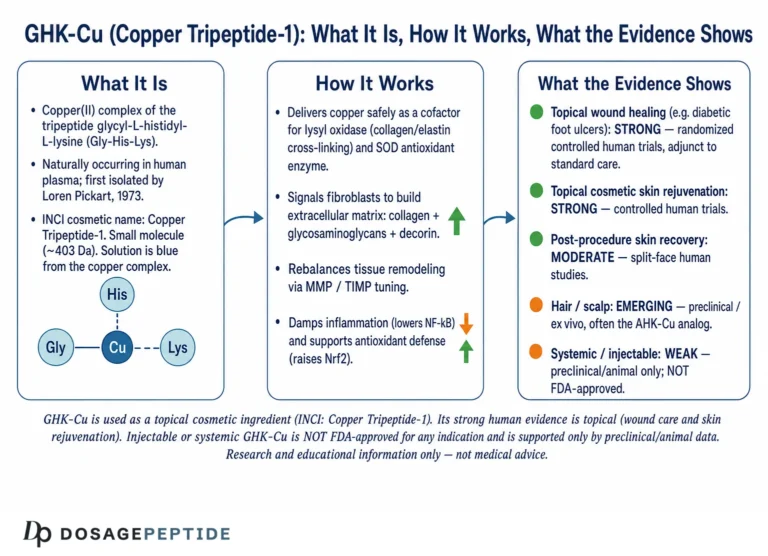
It matters to say at the outset what GHK-Cu actually is in regulatory terms. GHK-Cu is the copper(II) complex of the human tripeptide glycyl-L-histidyl-L-lysine; in cosmetic ingredient nomenclature it is listed as copper tripeptide-1. It is a cosmetic and research compound, not an FDA-approved drug for any disease.1 Much of the tissue-repair literature that circulates online is in vitro (cell culture), ex vivo, or animal work; the human data are dominated by topical facial creams evaluated for cosmetic endpoints such as wrinkle depth and skin firmness, not by controlled trials in patients with wounds, organ injury, or fibrosis. Anyone reading a confident claim that GHK-Cu “repairs tissue” should immediately ask three questions: which tissue, by what route, and at what level of evidence?
This piece is written for researchers and scientifically literate readers who want an honest map of the signaling story. We will define what “tissue repair signaling” means, then walk through the peptide’s proposed signaling layers one at a time — copper delivery, extracellular-matrix remodeling, growth-factor and receptor signaling, genome-wide transcriptional reprogramming, and stem-cell effects — grading the evidence for each. We then step back to ask whether that signaling translates into demonstrated repair, compare GHK-Cu with other repair-associated peptides, and close with the limitations and regulatory reality. The guiding principle throughout is restraint: rich mechanistic signaling data do not, by themselves, prove clinical efficacy, and this article will not pretend otherwise.
What GHK-Cu Is: From a Plasma Tripeptide to a Copper Complex
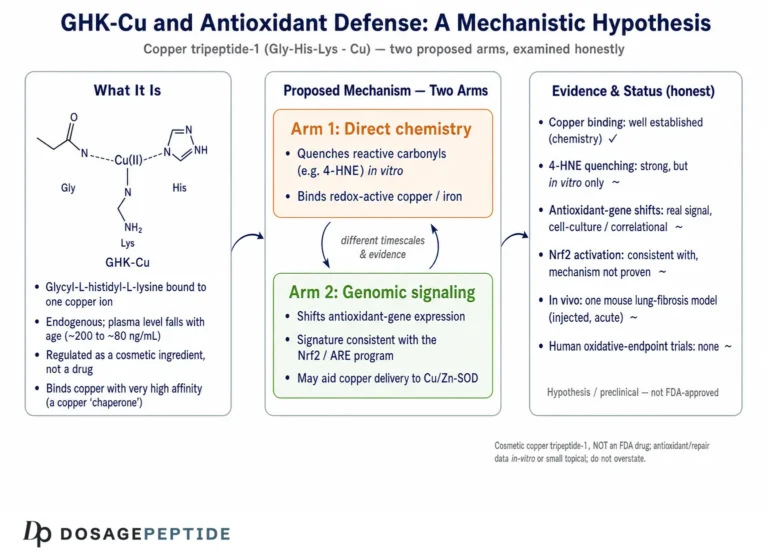
GHK (glycyl-L-histidyl-L-lysine) is a small, naturally occurring tripeptide first isolated from human plasma in 1973 by Loren Pickart, who noticed that a factor in the plasma of younger donors caused aged human liver tissue to synthesize proteins in a more youthful pattern.2 The active molecule turned out to be this three-amino-acid sequence, and — crucially — its biological behavior is inseparable from copper. GHK binds copper(II) ions with high affinity, and the resulting complex, GHK-Cu, is the form thought to carry most of the peptide’s regenerative signaling.3 The histidine and terminal amine of the tripeptide form a coordination geometry that is well suited to holding a single copper ion at the kind of concentrations found in tissue, which is why the molecule is often described not merely as a peptide but as a physiological copper chaperone.
One of the most frequently cited facts about GHK is that its plasma concentration declines with age — reported at roughly 200 ng/mL around age 20 and falling to about 80 ng/mL by age 60.4 This decline is repeatedly invoked to argue that supplementing GHK-Cu could restore a “youthful” repair signal. It is a reasonable hypothesis and a genuinely interesting correlation, but it is worth flagging early that a decline in a circulating molecule with age does not establish that adding it back reverses aging or repairs tissue. Correlation of an endogenous level with youth is a starting point for research, not a demonstration of therapeutic effect.
A detail that gives the signaling hypothesis unusual credibility is where the GHK sequence appears in the body. The glycyl-histidyl-lysine triplet is embedded in the sequence of the alpha-2(I) chain of type I collagen.5 This has led to an appealing model: when tissue is injured and proteases begin breaking down the collagen-rich matrix, GHK-containing fragments could be liberated locally, bind copper, and act as an in situ signal that repair is needed — a kind of molecular alarm released by the very matrix that has been damaged. This is a mechanistically satisfying idea supported by the peptide’s presence in collagen, though the precise degree to which endogenous GHK is generated this way in human wounds remains incompletely quantified.
For clarity, it helps to keep three things distinct. There is the free tripeptide GHK; there is the copper complex GHK-Cu that dominates the functional literature; and there is the cosmetic ingredient copper tripeptide-1 as formulated in creams and serums. These are chemically related but not interchangeable in how they have been studied: much of the mechanistic signaling work uses defined GHK-Cu in culture, while the human evidence overwhelmingly involves topical cosmetic formulations at low concentrations. Blurring these categories is one of the most common ways the evidence gets overstated. Readers wanting the cosmetic-endpoint side of the story in depth can consult the companion article on what GHK-Cu does for skin health, wrinkle reduction, and collagen synthesis; the present article stays focused on the repair-signaling mechanisms beneath those endpoints.
Defining “Tissue Repair Signaling” — and How to Grade the Evidence
Before praising or discounting GHK-Cu, we should be precise about what tissue repair actually requires, because “repair” is not one event but an orchestrated program. Classical wound healing proceeds through overlapping phases: hemostasis, inflammation, proliferation, and remodeling. Each phase is governed by signaling — cytokines and growth factors recruiting and activating cells, cells depositing and then reorganizing extracellular matrix, blood vessels sprouting to supply the new tissue, and finally a maturation phase in which matrix is remodeled and excess cellularity resolves.6 A molecule with a genuine “role in tissue repair signaling” would be expected to touch several of these nodes: attract and activate fibroblasts, promote matrix synthesis and controlled matrix turnover, support angiogenesis, and modulate inflammation.
The remarkable thing about GHK-Cu is that it has reported signaling activity at nearly all of these nodes. That breadth is precisely why the compound is fascinating — and also why it invites overstatement, because a molecule that appears to do everything in a dish can be marketed as a panacea. To keep ourselves honest, it helps to hold an explicit evidence hierarchy in mind as we proceed:
- Tier 1 — Mechanistic/biochemical: binding constants, copper coordination, effects on isolated enzymes. Strong here means the chemistry is real; it does not mean anything happens in a living tissue.
- Tier 2 — Cell culture (in vitro): effects on fibroblasts, keratinocytes, endothelial cells, and gene expression. Informative about plausible pathways, but cell culture routinely over-predicts clinical effect.
- Tier 3 — Animal (in vivo): rodent and rabbit wound and tissue models. Closer to reality, but small, often not blinded, and species-limited.
- Tier 4 — Human: for GHK-Cu, this is almost entirely small topical cosmetic studies with surrogate endpoints, not controlled therapeutic trials.
The thesis of this article can be stated in terms of that hierarchy: GHK-Cu’s tissue-repair-signaling evidence is strong at Tiers 1 and 2, moderate at Tier 3, and weak-to-absent at Tier 4 for most repair indications. The signaling story is well demonstrated; the clinical repair story is not. Keeping this scaffold in view prevents the very common error of citing a gene-expression result as though it were a cure.
Signaling Layer One: Copper Delivery as the Message
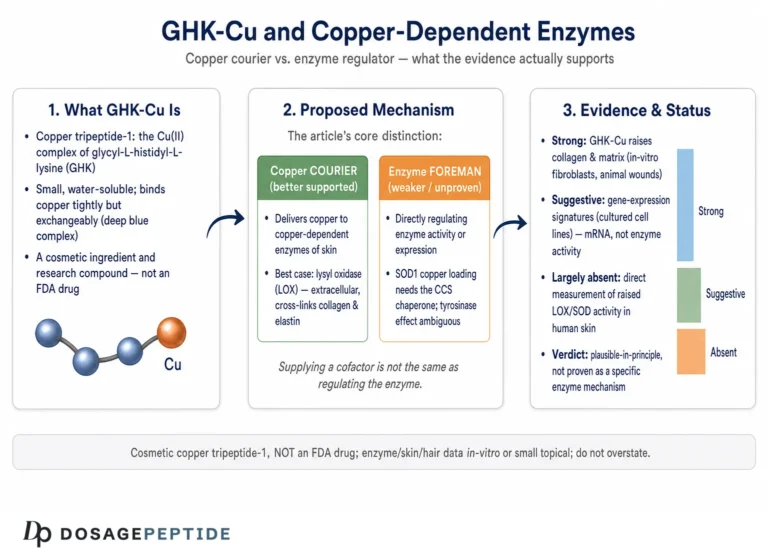
The first and arguably most fundamental signaling role of GHK-Cu concerns copper itself. Copper is not an incidental passenger on this peptide; for many of the molecule’s effects, the copper appears to be the point. Copper is an essential cofactor for enzymes central to tissue repair, most notably lysyl oxidase — the enzyme that cross-links collagen and elastin fibers to give repaired tissue its tensile strength — and copper/zinc superoxide dismutase, a key antioxidant defense.7 Copper ions also participate in the signaling that drives angiogenesis, the sprouting of new blood vessels essential to supplying a healing wound. GHK acts as a small, diffusible shuttle that can deliver copper to cells in a controlled, bioavailable form and buffer it against the toxicity that free copper ions would otherwise cause.
This copper-chaperone framing is important for honesty in both directions. On one hand, it grounds several of GHK-Cu’s effects in well-established inorganic biochemistry: copper genuinely is required for cross-linking and antioxidant enzymes, so a controlled copper source plausibly supports repair machinery.7 On the other hand, it complicates any claim that GHK the peptide is doing something uniquely peptidergic. A revealing example comes from matrix-metalloproteinase studies discussed below, in which certain effects on fibroblasts were reproduced by copper ions but not by the copper-free tripeptide — suggesting that for some endpoints the metal, not the peptide sequence, is the active principle.8 A scientifically careful reader should therefore treat “GHK-Cu signaling” as, in part, “targeted copper delivery,” and should be skeptical of marketing that attributes near-magical specificity to the three amino acids alone.
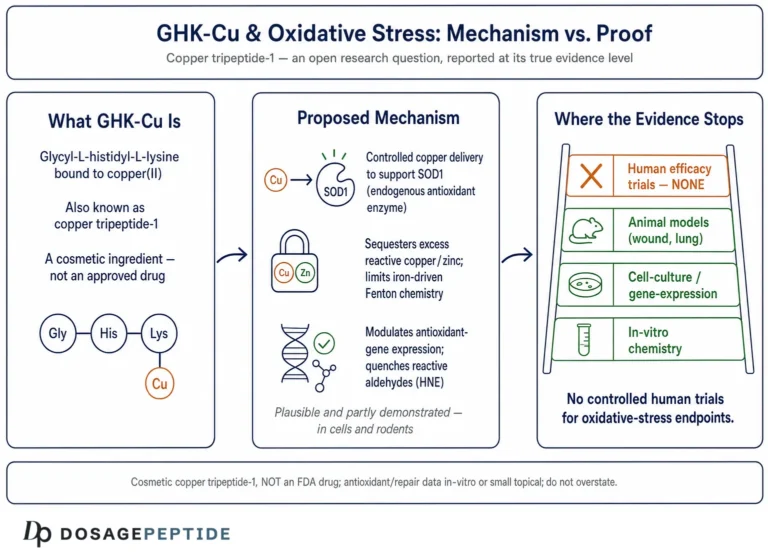
A second facet of copper-linked signaling is redox control, and it cuts in a direction that is easy to get backwards. Copper is a redox-active metal: free, unbuffered copper ions can catalyze the generation of damaging reactive oxygen species through Fenton-type chemistry, yet copper is simultaneously the essential cofactor of copper/zinc superoxide dismutase, one of the cell’s primary antioxidant enzymes. GHK-Cu has been discussed as contributing to antioxidant and anti-oxidative-stress signaling — for example by supporting antioxidant enzyme function and by chelating and controlling the availability of pro-oxidant metals such as iron and unbound copper — which is directly relevant to repair because oxidative stress impairs healing and drives the chronic inflammation seen in non-healing wounds.12 The honest reading is that the peptide’s ability to hold copper in a controlled coordination environment is plausibly what converts a potentially toxic metal into a repair-supportive one. This is an appealing mechanistic story, but it is largely built on biochemical and cell-level reasoning rather than on demonstrations that GHK-Cu reduces oxidative tissue damage in humans.
The angiogenic dimension of copper signaling connects GHK-Cu to the broader repair literature. Because new vessels are indispensable to rebuilding perfused tissue, a copper-delivering peptide that supports endothelial activity fits naturally into the repair narrative. This is the same conceptual territory explored for combination formulations; readers interested in the vascular side can see the discussion of evidence supporting KLOW peptides in angiogenesis and tissue repair, which situates copper-peptide angiogenic signaling among related research compounds. The honest caveat, again, is that angiogenic activity in cell and animal models is a signaling observation, not proof of improved healing outcomes in patients.
Signaling Layer Two: Extracellular-Matrix Remodeling
If copper delivery is the foundation, extracellular-matrix (ECM) remodeling is the layer where GHK-Cu’s signaling reputation was built. The seminal finding dates to 1988, when Maquart, Pickart, and colleagues reported that GHK-Cu stimulated collagen synthesis in cultured human fibroblasts, with the effect beginning at femtomolar-to-picomolar concentrations and peaking around 1 nanomolar — and, importantly, occurring without an increase in cell number, indicating a genuine stimulation of synthesis per cell rather than simply more cells.5 That concentration profile is striking: activity in the picomolar-to-nanomolar range is the hallmark of a signaling molecule engaging a specific pathway, not a bulk nutritional effect.
Subsequent work extended the picture well beyond collagen. GHK-Cu was shown to modulate the synthesis of glycosaminoglycans and the small proteoglycans of the matrix — including dermatan sulfate, chondroitin sulfate, and notably decorin, a proteoglycan that helps organize collagen fibrils and regulates their diameter during healing.9 This matters because functional repair is not just about making more collagen; it is about making the right matrix architecture. A molecule that coordinately influences collagen, elastin precursors, and organizing proteoglycans is signaling toward structured tissue, not a disorganized scar.
The most sophisticated aspect of the ECM story is that GHK-Cu appears to promote controlled matrix turnover, not just deposition. It has been reported to stimulate matrix metalloproteinase-2 (MMP-2) expression in fibroblast cultures — and in that particular study the effect was reproduced by copper ions but not by copper-free GHK, a caveat already noted above.8 In parallel, GHK-Cu has been described as modulating both metalloproteinases and their tissue inhibitors (TIMPs), which is exactly the balance the remodeling phase of healing requires.1 Remodeling is a demolition-and-rebuild process: old or provisional matrix must be degraded in a regulated way even as new matrix is laid down. A signaling molecule that touches both sides of the MMP/TIMP equation is, at least in principle, well suited to the maturation phase of repair.
The clearest way to summarize the ECM signaling evidence is a table, with explicit evidence tiers so nothing is oversold.
| ECM signaling effect | Reported action of GHK-Cu | Evidence tier |
|---|---|---|
| Type I collagen synthesis | Stimulated in fibroblasts, peak ~1 nM, no change in cell number5 | Tier 2 (in vitro) |
| Glycosaminoglycans / proteoglycans | Modulates dermatan sulfate, chondroitin sulfate, decorin9 | Tier 2 (in vitro) |
| MMP-2 (matrix turnover) | Increased in fibroblast media; reproduced by Cu ions, not GHK alone8 | Tier 2 (in vitro) |
| MMP / TIMP balance | Reported modulation of proteases and their inhibitors1 | Tier 1–2 (review-level) |
| Connective-tissue accumulation | Increased ECM in rat experimental wounds in vivo10 | Tier 3 (animal) |
The pattern in the table is the essence of the honest verdict: the ECM signaling evidence is real, coherent, and mechanistically sensible — but it lives almost entirely in cell culture and rodent wounds. It demonstrates that GHK-Cu can signal ECM cells to remodel matrix; it does not, on its own, demonstrate that applying GHK-Cu heals a human wound better than standard care.
Signaling Layer Three: Growth-Factor and Receptor Signaling
Matrix cells do not act in isolation; they respond to and secrete growth factors, and this is the third signaling layer where GHK-Cu has documented activity. Two threads are worth separating carefully because the popular literature tends to merge them into a single overconfident claim.
The first thread is fibroblast recruitment and activation. GHK-Cu has been characterized as a chemoattractant and mitogen for fibroblasts — that is, it can draw fibroblasts toward a signal and support their proliferation and activity, both essential in the proliferative phase of healing.1 A particularly relevant experiment examined normal and irradiated fibroblasts: copper tripeptide influenced their growth and their expression of growth factors, with implications for tissue that has been damaged by radiation and lost regenerative capacity.11 This is one of the more clinically evocative signaling findings, because it points at restoring function to compromised cells rather than merely boosting already-healthy ones — though it remains a cell-culture result.
The second thread involves specific growth-factor pathways. GHK-Cu has been associated in the literature with signaling relevant to transforming growth factor-beta (TGF-β), vascular endothelial growth factor (VEGF), and fibroblast growth factor activity, and with transactivation of receptor tyrosine kinase pathways that drive migration and proliferation.1 These are the canonical growth-factor axes of repair: TGF-β orchestrates fibroblast activation and matrix production, VEGF drives angiogenesis, and FGF supports proliferation. The honest framing here is that GHK-Cu appears to nudge several of these systems in a pro-repair direction in model systems. What the evidence does not support is the frequent marketing shorthand that GHK-Cu is a growth factor or that it reliably reproduces the effects of recombinant growth-factor therapeutics; it is a small copper-binding peptide that modulates these pathways in culture, which is a much more modest — if still interesting — claim.
It is worth pausing on why breadth across growth-factor pathways is a double-edged observation. On one hand, tissue repair genuinely is multi-pathway, so a molecule that touches several nodes is theoretically attractive. On the other hand, a molecule reported to influence TGF-β, VEGF, FGF, MMPs, antioxidant enzymes, and dozens of gene categories starts to strain credulity as a specific pharmacological agent, and the risk of publication and reporting bias — where positive signaling results are emphasized and null results go unpublished — grows accordingly. The correct scientific posture is to accept that GHK-Cu is a promiscuous modulator with genuine effects on repair signaling, while remaining alert that promiscuity plus small studies is exactly the recipe that produces impressive-looking but poorly-reproducible literatures. For a mechanistic contrast with another widely discussed repair peptide, the pillar overview of what BPC-157 is and how the healing peptide is explained illustrates how differently two “repair” compounds are proposed to work.
Signaling Layer Four: Genome-Wide Transcriptional Reprogramming
The most headline-grabbing — and most frequently exaggerated — signaling evidence for GHK-Cu comes from genome-wide gene-expression analysis. Using the Broad Institute’s Connectivity Map, a database that catalogs how cultured human cells change their gene expression in response to thousands of compounds, Pickart and colleagues reported that GHK altered the expression of a very large fraction of the human genome, with estimates in their analyses that the peptide changed a majority of assayed genes at various thresholds and shifted more than four thousand genes in a direction the authors interpreted as pro-repair and anti-inflammatory.17 These changes were mapped onto functional categories including matrix remodeling, growth-factor signaling, antioxidant defense, DNA repair, and the ubiquitin-proteasome protein-cleansing system.1
Taken at face value, this is an extraordinary breadth of transcriptional signaling, and it is the source of claims that GHK-Cu “resets” cells toward a younger, more regenerative state. There is a real and interesting result underneath these claims. But three sobering caveats are essential for honesty. First, the Connectivity Map measures gene-expression changes in specific cultured cancer cell lines exposed to a compound; a large number of altered transcripts is a signature of a broadly active molecule, not proof that any of those changes produces beneficial tissue repair in a living human. Second, “affecting a gene’s expression” includes both increases and decreases and does not tell us whether the net physiological effect is helpful, neutral, or harmful in a given tissue. Third, much of the interpretive work — grouping genes into “tissue repair” or “anti-cancer” categories — comes from a small number of authors closely associated with the compound, so independent replication and interpretation carry particular weight and are, at present, limited.
Two specific strands from this genomic work deserve mention because they recur in repair discussions. GHK has been reported to induce expression of numerous DNA-repair genes and of caspase and growth-regulatory genes in a pattern the authors interpreted as anti-cancer.13 Separately, the gene data have been used to argue for suppression of nuclear factor-kappa B (NF-κB) signaling, a master regulator of inflammation, which would fit the anti-inflammatory phase of repair.1 These are legitimate, published observations. They are also, categorically, transcriptional signaling data in cell systems — hypothesis-generating for tissue repair, not demonstrations of it. Presenting a Connectivity Map heat map as evidence that GHK-Cu treats disease is one of the most common overreaches in the popular literature, and it should be resisted.
One additional strand of the genomic story is worth drawing out because it connects to a distinct repair mechanism: protein quality control. The gene data have been used to argue that GHK activates the ubiquitin-proteasome system, the cellular machinery that tags and degrades damaged or misfolded proteins.1 In the context of repair and aging, a functioning proteasome matters because the accumulation of damaged proteins is a hallmark of senescent, poorly-regenerating tissue, and clearing that debris is part of restoring cellular function. If GHK-Cu genuinely upregulates this cleansing pathway, it would fit the broader “reset toward a younger phenotype” narrative. Yet the same caution applies with full force: this is a transcriptional inference from cell-line data, and demonstrating that GHK-Cu measurably improves proteostasis in living human tissue — let alone that doing so repairs an organ — is a completely different and unmet evidentiary burden.
The fair summary of the genomic layer is that GHK-Cu is, unusually, a small molecule with genome-scale transcriptional footprints pointing broadly toward repair-associated programs. That is a genuine and remarkable signaling observation. It is not, and should never be represented as, clinical proof.
Signaling Layer Five: Stem-Cell and Keratinocyte Effects
Repair ultimately depends on the cells that regenerate tissue, and a further body of work examines GHK-Cu’s effects on progenitor and basal cells. In a three-dimensional skin-equivalent model, copper-GHK at micromolar concentrations increased the expression of epidermal stem-cell-associated markers, including integrins and p63, in basal keratinocytes — findings the authors interpreted as promoting the “stemness” and survival of basal skin stem cells.14 Because p63 is a putative marker of epidermal stem cells and integrins mediate the attachment and proliferative competence of the basal layer, this points to a signaling role in maintaining the regenerative reservoir of the epidermis rather than only stimulating mature fibroblasts.
Related work has explored the stem-cell-recovering effects of the copper-free peptide as well, adding nuance to the copper-versus-peptide question raised earlier and suggesting that at least some progenitor effects may not require the metal.15 The broader theme — that GHK-Cu may act on stem and progenitor populations — connects directly to one of the compound’s most-searched applications; the dedicated discussion of how GHK-Cu affects hair-follicle stem cells and hair growth examines that particular progenitor niche in detail. For the purposes of tissue repair signaling, the takeaway is that GHK-Cu’s reported reach extends from the matrix and growth-factor levels down to the progenitor cells that must ultimately execute regeneration — again, largely in culture and model systems.
It bears repeating, because stem-cell language is especially prone to hype, that increasing a stem-cell marker in a skin-equivalent model is a signaling result, not evidence that GHK-Cu regenerates organs or reverses aging. The distance between “raised p63 in basal keratinocytes in vitro” and “regenerates tissue in patients” is vast, and it is precisely the distance this article is trying to keep visible.
From Signaling to Actual Repair: The In Vivo and Human Evidence
All of the layers above concern signaling — what GHK-Cu does to molecules, cells, and gene expression. The decisive question for the title is whether that signaling produces demonstrated repair in living tissue. Here the evidence weakens by tier, and candor is essential.
The strongest whole-tissue evidence is animal wound work. In a classic study, GHK-Cu increased connective-tissue accumulation in rat experimental wounds in vivo, showing that the culture-level ECM signaling can translate into more matrix in a real wound bed in a rodent.10 Additional animal and biomaterial studies — for example incorporating GHK into collagen scaffolds for diabetic-type wound models — have reported accelerated closure and improved tissue quality, reinforcing that the signaling is capable of producing tissue-level effects in controlled animal settings.16 These are meaningful Tier 3 results. They are also small, mostly unblinded, and confined to specific models and species.
A point often raised in favor of GHK-Cu is that its reported repair signaling is not confined to skin. Review-level summaries describe GHK-associated improvements in tissue repair across skin, lung connective tissue, bone, liver, and the stomach lining in various experimental settings.13 This breadth is consistent with the collagen-liberation model introduced earlier: because the GHK sequence sits within type I collagen, any collagen-rich tissue that is injured could in principle release the signal locally, which would explain why effects appear across multiple organs rather than being skin-specific. It is a coherent unifying idea. But it is important not to let breadth substitute for depth: reports of activity in many tissues, each at the preclinical level, do not add up to demonstrated efficacy in any one of them. Five weak signals are not one strong one. The multi-tissue pattern strengthens the case that GHK-Cu is a general repair-signaling molecule; it does not establish that it is a treatment for lung, bone, liver, or gastric disease, none of which it is approved to treat.
The human evidence is where expectations must drop sharply. The bulk of it comes from cosmetic dermatology. In a widely cited 12-week facial study, a GHK-Cu-containing cream applied twice daily to women with photoaged skin improved measures such as skin firmness, clarity, fine lines, density, and thickness, and stimulated dermal changes consistent with the signaling story.1 Small comparative studies have reported that GHK-Cu facial cream increased collagen in photoaged skin, in some cases performing comparably to or better than vitamin C or retinoic acid in the volunteers studied.1 These are real human data and they are consistent with the mechanistic layers — but they are cosmetic-endpoint studies, typically small, industry-associated, and focused on the appearance of aging skin rather than on healing a wound, repairing an organ, or reversing fibrosis.
What is largely absent is exactly what the word “demonstrates” in the title would require for therapeutic repair: large, randomized, blinded, controlled human trials showing that GHK-Cu improves clinically important repair outcomes — wound closure rates in chronic wounds, functional recovery after injury, organ-function endpoints in fibrosis. Applications such as chronic non-healing wounds remain investigational and hypothesis-driven; the companion analysis of whether GHK-Cu could improve outcomes in chronic non-healing wounds examines that specific gap and reaches a similarly cautious conclusion. Until such trials exist, the accurate statement is that GHK-Cu’s tissue-repair signaling is well demonstrated, while its tissue-repair efficacy in humans is demonstrated only in the narrow, surrogate-endpoint domain of topical cosmetic skin improvement.
How GHK-Cu Compares With Other Repair-Associated Compounds
Placing GHK-Cu beside other molecules discussed for tissue repair clarifies both its distinctive mechanism and its evidentiary standing. The comparison is not a competition — these agents act through different pathways and few have strong human repair data — but it shows what kind of signaling GHK-Cu represents and how mature the evidence is.
| Compound | Proposed repair-signaling mechanism | Highest evidence tier for repair |
|---|---|---|
| GHK-Cu (copper tripeptide-1) | Copper delivery to repair enzymes; ECM synthesis and MMP/TIMP remodeling; growth-factor and genome-wide modulation | Human topical cosmetic studies; animal wound models; not FDA-approved as a drug1 |
| Recombinant PDGF (becaplermin) | Direct platelet-derived growth-factor receptor activation | FDA-approved topical gel for diabetic foot ulcers (a genuine regulated therapeutic) |
| BPC-157 | Proposed angiogenic and cytoprotective signaling; upregulation of growth-factor receptors | Preclinical/animal predominant; no FDA approval |
| TB-500 / thymosin β4 | Actin regulation, cell migration, angiogenesis | Preclinical predominant; limited human data |
| Recombinant growth factors (e.g., FGF, EGF products) | Direct receptor agonism | Some approved regionally for wounds; strong receptor pharmacology |
Two lessons emerge. First, GHK-Cu is mechanistically distinctive: unlike the direct receptor agonists, it works indirectly and diffusely — delivering copper and broadly modulating matrix, growth-factor, and transcriptional programs rather than flipping a single receptor switch. That breadth is its signature and its interpretive challenge. Second, on the evidence axis, GHK-Cu sits alongside compounds like BPC-157 and TB-500 in being rich in preclinical signaling data but thin in controlled human therapeutic trials, and well behind approved agents such as becaplermin that cleared regulatory efficacy bars. It is genuinely better-evidenced than many research peptides at the mechanistic and cosmetic-clinical levels, and genuinely far from an approved tissue-repair drug. Both halves of that sentence are true.
Research Handling, Formulation, and Route — Why They Change the Signaling Story
A point too often ignored in signaling discussions is that route and formulation may determine whether any of this molecular activity reaches the intended tissue. GHK-Cu is a small hydrophilic peptide-metal complex, and its delivery is non-trivial. Topically, penetration through intact stratum corneum is limited, which is why microneedle and enhanced-delivery approaches have been investigated to get copper peptides into the dermis; the cosmetic human data reflect whatever fraction actually penetrated.1 This is a crucial honesty point: a compound with impressive signaling in a dish may deliver only a small, variable dose to living tissue depending entirely on the vehicle.
GHK-Cu is most often encountered in research as a blue lyophilized powder (the color reflects the bound copper). Standard research-peptide handling — reconstitution with sterile or bacteriostatic water, gentle swirling rather than shaking to avoid shearing the peptide, cool and dark storage, and avoidance of repeated freeze-thaw cycles — applies as it does across the class, and general reconstitution mathematics are covered in the site’s peptide reconstitution guide. It must be stated plainly that describing laboratory handling is not an endorsement of human use: GHK-Cu is a cosmetic and research compound, and injectable or systemic administration for tissue repair is not an approved therapeutic use and carries the added risks of any non-approved parenteral product, including sterility, purity, and dosing uncertainties.
The formulation caveat feeds back into evidence interpretation. Because the human evidence base is topical and cosmetic, it tells us relatively little about what systemic or injected GHK-Cu would do — a route for which controlled human repair data are essentially nonexistent. Extrapolating from a cream that modestly improved skin firmness to an injection that repairs internal tissue is precisely the kind of leap that the evidence hierarchy forbids. Signaling activity is necessary but nowhere near sufficient to justify such extrapolation.
Limitations, Biases, and the Honest Bottom Line
Pulling the analysis together, several limitations bear directly on how much weight the phrase “demonstrates a role in tissue repair signaling” can carry.
The evidence is tier-stratified and top-heavy in vitro. The great majority of GHK-Cu’s repair data are cell-culture and gene-expression studies, with a smaller animal literature and a human literature confined to cosmetic topical endpoints. This is a signaling literature far more than an outcomes literature. Cell-culture and rodent results routinely fail to translate to human therapeutic benefit, and there is no reason to assume GHK-Cu is exempt.
Copper versus peptide. For some endpoints, the biological effect tracks with copper ions rather than the tripeptide sequence, most explicitly in the MMP-2 fibroblast work.8 This blurs the claim that a specific “GHK signaling” is responsible and cautions against attributing precise pharmacological specificity to the peptide alone.
Source concentration and reproducibility. A large share of the mechanistic interpretation, particularly the genome-wide claims, originates from a small group of closely associated authors. This does not make the findings wrong, but genuinely independent replication is limited, and extraordinary claims (a peptide affecting a majority of the genome) warrant extraordinary corroboration that is not yet abundant.17
Endpoint surrogacy. Even the human cosmetic studies rely on surrogate and appearance-based endpoints — firmness, wrinkle depth, measured density — rather than hard repair outcomes. Improvement in the appearance of photoaged skin is a legitimate cosmetic result but is not the same as demonstrated healing of injured or diseased tissue.1
Publication and commercial bias. GHK-Cu is a commercially valuable cosmetic ingredient. The incentive structure favors publishing and amplifying positive signaling results, and much of the online literature is marketing rather than science. Readers should weight peer-reviewed primary sources far above vendor summaries.
Dose, timing, and biphasic behavior. A subtler limitation concerns how much and how the signaling translates to dose. The collagen-synthesis data show activity peaking at low nanomolar concentrations, which implies that more is not necessarily better and that higher exposures could produce different or blunted responses — a biphasic pattern common among signaling peptides.5 Because the human cosmetic studies used specific topical formulations at particular concentrations, and because delivery to living dermis is variable, there is genuine uncertainty about what tissue concentration is actually achieved and whether it sits in the favorable part of the dose-response curve. Marketing that implies a simple “more peptide equals more repair” relationship is not supported by the concentration data and may be actively misleading.
The honest bottom line is a genuinely nuanced one, and it refuses both easy narratives. GHK-Cu is not snake oil: it has a coherent, multi-layered, biochemically plausible signaling profile spanning copper delivery, ECM remodeling, growth-factor modulation, genome-wide transcriptional shifts, and stem-cell markers, with supporting animal wound data and small positive human cosmetic studies. But GHK-Cu is also not a proven tissue-repair therapeutic: it is copper tripeptide-1, a cosmetic and research compound, unapproved as a drug, whose therapeutic repair efficacy in humans remains undemonstrated outside the narrow domain of topical skin cosmetics. The evidence demonstrates a rich role in tissue-repair signaling; it does not yet demonstrate tissue-repair therapy. Holding both of those truths simultaneously is the mark of reading this literature correctly. For readers tracking how this evidence base evolves, the site’s research blog follows new peptide literature as it is published, and defined terms used above are collected in the peptide glossary.
Frequently Asked Questions
Does the evidence prove GHK-Cu repairs tissue?
It proves that GHK-Cu is active in tissue-repair signaling — it stimulates collagen and proteoglycan synthesis in fibroblasts, modulates matrix-remodeling enzymes, influences growth-factor pathways, and shifts a large number of genes toward repair-associated programs in cell studies.1517 It does not prove clinical tissue-repair efficacy in humans. The human evidence is largely small topical cosmetic studies with surrogate endpoints, plus animal wound models; there are no large controlled trials demonstrating that GHK-Cu heals wounds or repairs organs in patients.
Is GHK-Cu an FDA-approved drug?
No. GHK-Cu is copper tripeptide-1, used as a cosmetic ingredient and a research compound. It is not approved by the FDA (or comparable regulators) as a drug for the treatment of wounds, aging, fibrosis, or any other disease. Cosmetic use of copper peptides is regulated differently from drug approval and does not require demonstrated therapeutic efficacy.
Is the copper or the peptide doing the work?
Probably both, depending on the endpoint. Copper is an essential cofactor for repair enzymes such as lysyl oxidase and superoxide dismutase, and for at least one documented effect — stimulation of MMP-2 in fibroblasts — the activity was reproduced by copper ions but not by the copper-free tripeptide.78 For other effects, the peptide sequence appears to contribute. This is why GHK-Cu is best understood partly as a targeted copper-delivery system rather than as a purely peptidergic signal.
What is the single strongest piece of mechanistic evidence?
The classic finding that GHK-Cu stimulates collagen synthesis in human fibroblasts at picomolar-to-nanomolar concentrations, peaking near 1 nM and occurring without any increase in cell number.5 That concentration profile is characteristic of a specific signaling molecule rather than a bulk nutrient effect, and it has been extended by later work on proteoglycans and matrix remodeling.9
What does the “thousands of genes” claim actually mean?
Connectivity Map analyses reported that GHK changed the expression of a very large fraction of assayed human genes, with more than four thousand shifted in a repair- and anti-inflammation-associated direction.17 This is a real result, but it measures transcription in specific cultured cell lines. A broad transcriptional footprint indicates a broadly active molecule; it does not demonstrate that those gene changes produce beneficial repair in living human tissue, and independent replication remains limited.
Is there any human evidence at all?
Yes, but it is narrow. The main human data are small topical facial-cream studies in photoaged skin reporting improved firmness, density, and reduced wrinkles, with some comparisons to vitamin C and retinoic acid.1 These are cosmetic-endpoint studies, often small and industry-associated. There are no large randomized controlled trials demonstrating GHK-Cu efficacy for wound healing, organ repair, or fibrosis.
How does GHK-Cu compare with growth-factor drugs like becaplermin?
Becaplermin is recombinant PDGF, an approved topical therapeutic that directly activates a growth-factor receptor and cleared regulatory efficacy standards for diabetic foot ulcers. GHK-Cu acts indirectly and diffusely — delivering copper and modulating many pathways — and is not an approved drug. GHK-Cu is richer in mechanistic breadth but far behind in demonstrated clinical repair efficacy.
Does injecting GHK-Cu repair internal tissue?
There is no controlled human evidence to support that. The human data are topical and cosmetic; systemic or injected use for tissue repair is not an approved therapeutic application and has not been validated in controlled human trials. Extrapolating from a cream that modestly improved skin appearance to an injection that repairs internal tissue is not justified by the current evidence, and non-approved injectable use carries additional sterility, purity, and dosing risks.
How is GHK-Cu handled in a research setting?
It is typically supplied as a blue lyophilized powder (the color from bound copper), reconstituted with sterile or bacteriostatic water using gentle technique, stored cool and dark, and protected from freeze-thaw cycles — standard research-peptide practice.1 Handling quality preserves the molecule’s activity but has no bearing on the unresolved question of clinical repair efficacy, and such handling notes are not a recommendation for human use.
References
- Pickart L, Margolina A. Regenerative and protective actions of the GHK-Cu peptide in the light of the new gene data. Int J Mol Sci. 2018;19(7):1987. PMID: 29986520; PMCID: PMC6073405. https://pubmed.ncbi.nlm.nih.gov/29986520/
- Pickart L, Thaler MM. Tripeptide in human serum which prolongs survival of normal liver cells and stimulates growth in neoplastic liver. Nat New Biol. 1973;243(124):85-87. PMID: 4349963. https://pubmed.ncbi.nlm.nih.gov/4349963/
- Pickart L. The human tri-peptide GHK and tissue remodeling. J Biomater Sci Polym Ed. 2008;19(8):969-988. PMID: 18644225. https://pubmed.ncbi.nlm.nih.gov/18644225/
- Pickart L, Vasquez-Soltero JM, Margolina A. GHK peptide as a natural modulator of multiple cellular pathways in skin regeneration. Biomed Res Int. 2015;2015:648108. PMID: 26236730; PMCID: PMC4508379. https://pmc.ncbi.nlm.nih.gov/articles/PMC4508379/
- Maquart FX, Pickart L, Laurent M, Gillery P, Monboisse JC, Borel JP. Stimulation of collagen synthesis in fibroblast cultures by the tripeptide-copper complex glycyl-L-histidyl-L-lysine-Cu2+. FEBS Lett. 1988;238(2):343-346. PMID: 3169264. https://febs.onlinelibrary.wiley.com/doi/abs/10.1016/0014-5793(88)80509-X
- Gonzalez ACdO, Costa TF, Andrade ZdA, Medrado ARAP. Wound healing — a literature review. An Bras Dermatol. 2016;91(5):614-620. PMCID: PMC5087220. https://pmc.ncbi.nlm.nih.gov/articles/PMC5087220/
- Kornblatt AP, Nicoletti VG, Travaglia A. The neglected role of copper ions in wound healing. J Inorg Biochem. 2016;161:1-8. PMID: 27153355. https://pubmed.ncbi.nlm.nih.gov/27153355/
- Siméon A, Emonard H, Hornebeck W, Maquart FX. The tripeptide-copper complex glycyl-L-histidyl-L-lysine-Cu2+ stimulates matrix metalloproteinase-2 expression by fibroblast cultures. Life Sci. 2000;67(18):2257-2265. PMID: 11045606. https://pubmed.ncbi.nlm.nih.gov/11045606/
- Siméon A, Wegrowski Y, Bontemps Y, Maquart FX. Expression of glycosaminoglycans and small proteoglycans in wounds: modulation by the tripeptide-copper complex glycyl-L-histidyl-L-lysine-Cu2+. J Invest Dermatol. 2000;115(6):962-968. PMID: 11121143. https://www.sciencedirect.com/science/article/pii/S0022202X1541067X
- Maquart FX, Bellon G, Chaqour B, et al. In vivo stimulation of connective tissue accumulation by the tripeptide-copper complex glycyl-L-histidyl-L-lysine-Cu2+ in rat experimental wounds. J Clin Invest. 1993;92(5):2368-2376. PMID: 8227354; PMCID: PMC288419. https://pmc.ncbi.nlm.nih.gov/articles/PMC288419/
- Pollard JD, Quan S, Kang T, Koch RJ. Effects of copper tripeptide on the growth and expression of growth factors by normal and irradiated fibroblasts. Arch Facial Plast Surg. 2005;7(1):27-31. PMID: 15655171. https://pubmed.ncbi.nlm.nih.gov/15655171/
- Pickart L, Vasquez-Soltero JM, Margolina A. The human tripeptide GHK-Cu in prevention of oxidative stress and degenerative conditions of aging: implications for cognitive health. Oxid Med Cell Longev. 2012;2012:324832. PMID: 22666519; PMCID: PMC3359723. https://pmc.ncbi.nlm.nih.gov/articles/PMC3359723/
- Pickart L, Vasquez-Soltero JM, Margolina A. GHK, the human skin remodeling peptide, induces anti-cancer expression of numerous caspase, growth regulatory, and DNA repair genes. J Anal Oncol. 2014;3(2):79-91. https://www.neoplasiaresearch.com/index.php/jao/article/view/217
- Kang YA, Choi HR, Na JI, et al. Copper-GHK increases integrin expression and p63 positivity by keratinocytes. Arch Dermatol Res. 2009;301(4):301-306. PMID: 19319546. https://pubmed.ncbi.nlm.nih.gov/19319546/
- Choi HR, Kang YA, Ryoo SJ, et al. Stem cell recovering effect of copper-free GHK in skin. J Pept Sci. 2012;18(11):685-690. PMID: 23019153. https://pubmed.ncbi.nlm.nih.gov/23019153/
- Arul V, Kartha R, Jayakumar R. A therapeutic approach for diabetic wound healing using biotinylated GHK incorporated collagen matrices. Life Sci. 2007;80(4):275-284. PMID: 17049948. https://pubmed.ncbi.nlm.nih.gov/17049948/
- Pickart L, Vasquez-Soltero JM, Margolina A. GHK and DNA: resetting the human genome to health. Biomed Res Int. 2014;2014:151479. PMID: 25302294; PMCID: PMC4180391. https://pmc.ncbi.nlm.nih.gov/articles/PMC4180391/
Educational and research-use disclaimer: This article is provided solely for scientific and educational purposes. GHK-Cu (copper tripeptide-1) is a cosmetic and research compound and is not approved by the FDA, EMA, or any comparable regulator for the treatment, cure, or prevention of wounds, aging, fibrosis, or any other disease. The tissue-repair-signaling evidence described here is predominantly derived from in vitro, gene-expression, and animal studies, with human data limited largely to small topical cosmetic evaluations using surrogate endpoints; clinical tissue-repair efficacy in humans has not been demonstrated. Nothing here is medical advice or a recommendation for human use, and non-approved injectable or systemic use carries additional sterility, purity, and dosing risks. Any legitimate investigation of this compound should occur within properly authorized preclinical or clinical research under appropriate oversight. Readers should consult qualified professionals and applicable regulations before making any decisions.