The question in the title carries a quiet assumption worth surfacing before we examine any pharmacology: it presumes that Selank does regulate behavior, and that the interesting task is merely to trace the central-nervous-system wiring by which it does so. That framing is common in the popular literature on this peptide, but it runs ahead of the evidence. Selank is a synthetic heptapeptide developed in Russia as an anxiolytic, and it has a genuinely intriguing set of proposed molecular actions in the brain. What it does not have is the deep, replicated, independent human trial base that would justify speaking of confirmed “behavioral regulation” in the way we can speak of, say, a benzodiazepine or an SSRI. Most of what is known comes from Russian-language studies, small clinical series, and rodent work, much of it from the laboratories that developed the compound.
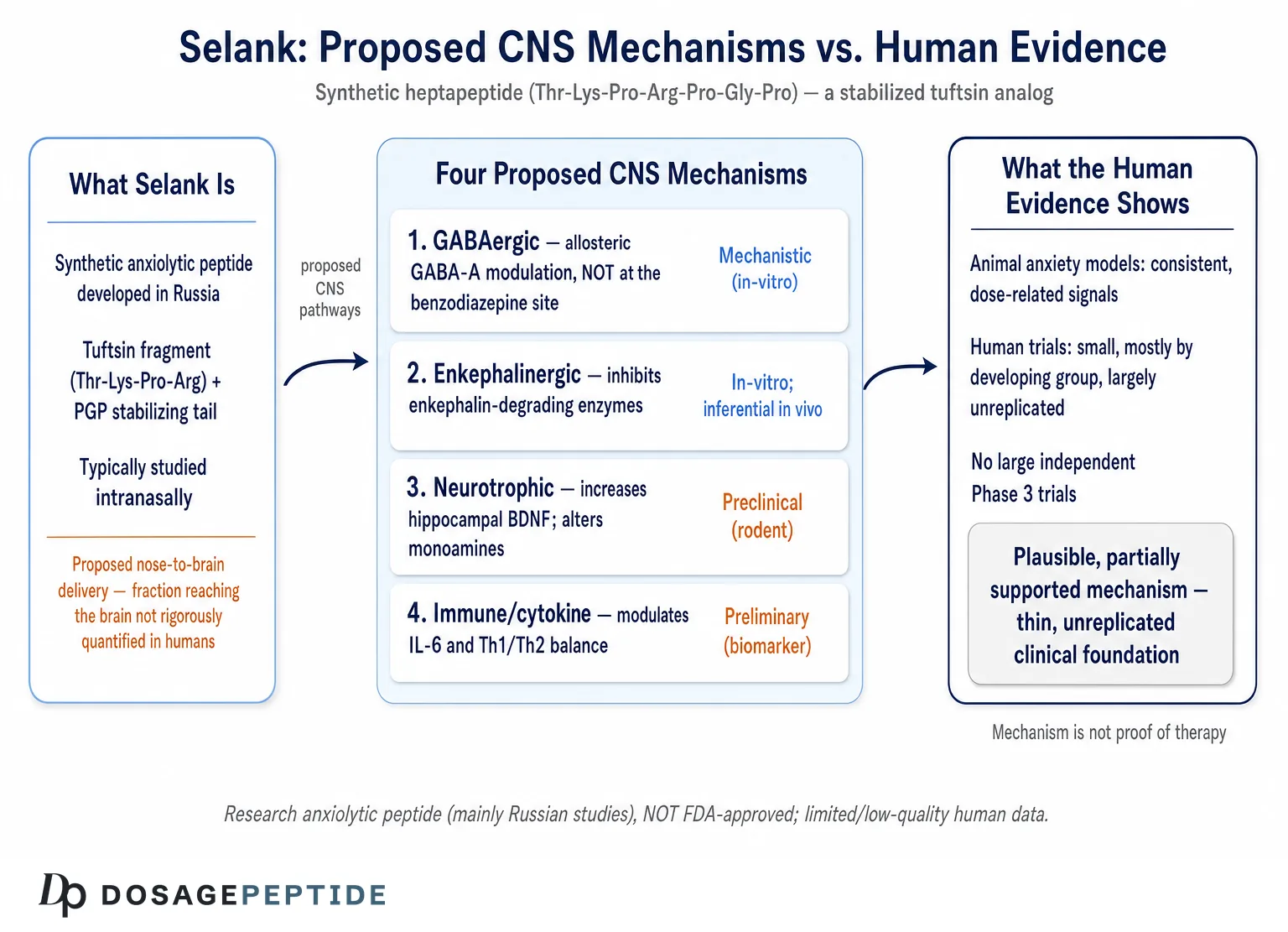
So rather than accept the premise, this article treats it as an open research question with two parts. First, is there a coherent, mechanistically plausible story for how Selank could influence behavior through CNS pathways? The answer here is a qualified yes: there are at least four candidate mechanisms — GABAergic modulation, inhibition of enkephalin breakdown, neurotrophic (BDNF) and monoaminergic effects, and immune-to-brain cytokine signaling — each with some experimental support. Second, is that story confirmed at the level of human behavior by high-quality evidence? Here the answer is a candid no. Selank is not approved by the U.S. Food and Drug Administration or the European Medicines Agency for any indication; it is a prescription anxiolytic only in Russia and a few neighboring jurisdictions, and the clinical trials underpinning that status are small, largely unblinded to Western scrutiny, and rarely replicated outside their country of origin.4
This piece is written for researchers and scientifically literate readers who want an honest map of a compound that is frequently oversold. We will trace Selank’s origin in tuftsin biology, examine each proposed CNS pathway on its own merits, weigh the actual human and animal evidence, discuss how it is handled in a research context, compare it candidly with established anxiolytics, and lay out its ambiguous regulatory position. The governing principle throughout is proportion: describing a mechanism is not the same as proving a therapy, and a plausible pathway in a rat hippocampus is a long way from a validated treatment for a human being.
What Selank Is: From Tuftsin to a Synthetic Heptapeptide
Selank is a synthetic heptapeptide with the amino-acid sequence Thr-Lys-Pro-Arg-Pro-Gly-Pro (threonine–lysine–proline–arginine–proline–glycine–proline). It was developed at the Institute of Molecular Genetics of the Russian Academy of Sciences, the same institution that produced the related nootropic peptide Semax.4 Understanding the molecule requires understanding its parent, tuftsin, because the entire design logic flows from it.
Tuftsin is a naturally occurring tetrapeptide — Thr-Lys-Pro-Arg — that corresponds to residues 289–292 of the heavy chain of immunoglobulin G. It was first described at Tufts University (hence the name) and is classically known as an immunomodulatory peptide that stimulates phagocytosis and other functions of macrophages and neutrophils. Tuftsin, however, is a poor drug candidate on its own: it is rapidly degraded by peptidases in blood and tissue, giving it a half-life measured in minutes. The Russian designers set out to solve that problem by extending the tetrapeptide with a C-terminal tripeptide motif, proline–glycine–proline (Pro-Gly-Pro, or PGP). The full Selank sequence is therefore the tuftsin fragment at the N-terminus fused to a PGP “stabilizing tail.”1
That PGP tail is not arbitrary. Proline-rich sequences resist cleavage by many aminopeptidases and carboxypeptidases, and the PGP motif in particular is thought to shield the biologically active tuftsin core from rapid enzymatic destruction, substantially prolonging the peptide’s functional presence. This is why Selank is often described as a “stabilized tuftsin analog.” The design achieves two things simultaneously: it retains the tuftsin pharmacophore that engages immune and, apparently, neural targets, while extending the window during which the molecule can act. It is a clean example of rational peptide engineering — take a short natural signaling peptide with an interesting activity but a hopeless pharmacokinetic profile, and bolt on a protective sequence to make it druggable.
A useful mental model is to keep three layers distinct. First is the immunological ancestor (tuftsin, an IgG-derived phagocytosis stimulant). Second is the active core (the Thr-Lys-Pro-Arg tuftsin fragment, which carries the biological signal). Third is the engineered drug (Selank, the core plus PGP, built for stability). Popular writing often collapses these layers, attributing to Selank the full immunological reputation of tuftsin and the full neurological ambition of a designed nootropic at once. Holding the layers apart is the single most useful habit for reasoning honestly about what this molecule can and cannot be expected to do. For readers surveying how such research peptides are catalogued and distinguished by their intended targets, the site’s dosage index organizes these compounds for educational reference.
One further point of identity matters for the behavioral question. Because Selank descends from an immune peptide, its CNS effects — if real — may be inseparable from its immune effects. Several of its proposed behavioral mechanisms run through immune signaling molecules such as interleukins and interferons rather than through classical neurotransmitter receptors alone. This makes Selank an interesting probe of the neuroimmune interface, but it also complicates any tidy story of “a peptide that binds a brain receptor and changes behavior.” The reality is messier and more distributed than that, which is part of why the mechanistic picture remains unsettled.
Examining the Premise: What “Regulating Behavior via CNS Pathways” Would Require
Before cataloguing mechanisms, it is worth being precise about what it would actually take to establish that Selank regulates behavior through the central nervous system. This is not pedantry; it is the difference between a marketing claim and a scientific one.
To credibly say a compound “regulates behavior via CNS pathways,” several things need to hold. The molecule must reach the brain in meaningful quantity (a real question for a hydrophilic heptapeptide). It must engage identifiable central targets — receptors, transporters, enzymes, or gene-expression programs — in a dose-dependent, reproducible way. Those molecular engagements must translate into measurable changes in neural activity or neurochemistry. Those neurochemical changes must, in turn, produce reliable, replicable behavioral effects in validated models. And finally, for any claim of therapeutic behavioral regulation in humans, those effects must appear in adequately powered, randomized, double-blind, placebo-controlled trials, ideally replicated by independent groups.
Selank clears the early hurdles more convincingly than the late ones. There is reasonable evidence that it engages central targets and shifts neurochemistry in rodents, and there are behavioral signals in animal anxiety models. The clinical layer is where the evidence thins dramatically: the human trials are small, mostly conducted by the developing institutions, and not replicated in the rigorous, independent, multicenter fashion that Western regulators require. So the honest framing is that Selank has a plausible and partially supported mechanistic account of behavioral regulation, resting on a thin and largely unreplicated clinical foundation.
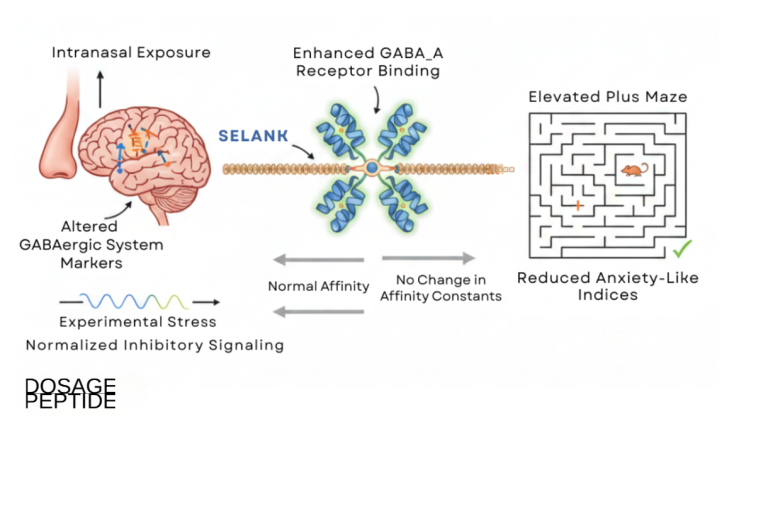
There is also the delivery question, which is easy to overlook. Selank is typically administered intranasally, and the rationale offered is that intranasal delivery may allow some peptide to reach the CNS via olfactory and trigeminal routes while bypassing first-pass metabolism. Intranasal nose-to-brain transport is a real and actively studied phenomenon, but the fraction of an intranasal peptide dose that actually reaches functionally relevant brain concentrations is generally small and highly variable, and it has not been rigorously quantified for Selank in humans. So even the foundational assumption — that enough peptide reaches the brain to act centrally — is more asserted than demonstrated. Keeping that caveat in view prevents the common error of treating an elegant mechanistic diagram as settled physiology.
With those standards stated, we can examine the four proposed CNS pathways in turn, asking of each not only “what is the mechanism?” but “how strong is the evidence, and in what system was it obtained?”
The GABAergic Pathway: Allosteric Modulation Without the Benzodiazepine Site
The most frequently cited mechanism for Selank’s anxiolytic effect is modulation of the GABAergic system — the brain’s principal inhibitory neurotransmitter network. This is an appealing story because anxiety, sedation, and the calming actions of benzodiazepines all run through GABA-A receptors, so a peptide that touched this system would have an obvious route to influencing anxious behavior.
The strongest primary evidence comes from radioligand-receptor binding work by Vyunova and colleagues, who used tritiated GABA to probe how Selank affects GABA binding to isolated brain-cell plasma membranes.2 Their data indicate that Selank acts as a positive allosteric modulator of GABA binding at GABA-A receptors, altering the affinity of the receptor for its native ligand in a concentration-dependent manner, and — importantly — doing so without engaging the classical benzodiazepine binding site.2 In plain terms, the finding suggests Selank does not act like a benzodiazepine at the molecular level; instead of binding the same pocket that diazepam does, it appears to influence the receptor’s interaction with GABA through a distinct allosteric mechanism. This distinction, if it holds, would be mechanistically significant, because it could in principle allow modulation of GABAergic tone without the full pharmacology — and liabilities — of benzodiazepine-site agonism.
A complementary line of evidence examined gene expression rather than binding. Filatova and colleagues studied 84 genes involved in GABAergic neurotransmission in human IMR-32 neuroblastoma cells exposed to GABA, Selank, and olanzapine.3 The result is instructive and, in a way, deflationary for simplistic accounts: Selank alone produced no statistically significant changes in the mRNA levels of the genes studied. Its effects appeared only in combination — when co-applied with GABA, Selank nearly completely suppressed the gene-expression changes that GABA induced on its own, and when co-applied with olanzapine it amplified that drug’s effects.3 The authors concluded that Selank lacks direct effects on GABAergic gene expression but may act as a modulator of GABA-receptor interactions — consistent with the allosteric-modulation picture from the binding studies rather than with any notion that Selank floods or directly activates the system.
The behavioral correlate of this GABAergic story comes from a rat study by Kasian and colleagues, who tested Selank alongside diazepam under unpredictable chronic mild stress.5 They reported that the combination of Selank and diazepam was the most effective at reducing anxiety-like behavior under chronic stress, that Selank alone produced minimal changes in locomotor activity (unlike diazepam, which is sedating), and they interpreted the results as suggesting Selank modulates GABA receptors in a way that might permit lower benzodiazepine doses while preserving the anti-anxiety effect.5 That is a genuinely interesting hypothesis — a benzodiazepine-sparing adjunct — but it is exactly that: a hypothesis generated in rodents, not a demonstrated clinical strategy.
The honest summary of the GABAergic pathway is that it is the best-supported of Selank’s proposed mechanisms and rests on at least one careful binding study and one gene-expression study, but that the picture is one of subtle, context-dependent modulation rather than direct receptor activation. Selank does not appear to be a peptide benzodiazepine. Whether its gentle allosteric nudging of GABA binding is strong enough to produce clinically meaningful anxiolysis in humans is not answered by these mechanistic studies.
The Enkephalin and Endogenous Opioid Pathway
A second, mechanistically distinct pathway concerns the endogenous opioid system — specifically the enkephalins, short opioid peptides that modulate pain, mood, and stress responses. Here the proposed mechanism is not receptor binding but enzyme inhibition: the idea that Selank prolongs the life of enkephalins by slowing the enzymes that degrade them.
The primary evidence is a pair of related studies from the developing group. Zozulya and colleagues reported that Selank dose-dependently inhibited the enzymatic hydrolysis of plasma enkephalin, with a half-maximal inhibitory concentration (IC50) around 15 micromolar, and that this inhibitory capacity exceeded that of standard peptidase inhibitors such as bacitracin and puromycin.6 They further observed that patients with generalized anxiety showed an abnormally shortened enkephalin half-life — consistent with reduced endogenous enzyme inhibition — and proposed that Selank’s anxiolytic activity is due, at least in part, to its ability to inhibit enkephalin breakdown and thereby restore or extend enkephalinergic signaling.6 A companion paper examined both Semax and Selank and confirmed that both heptapeptides inhibit the enkephalin-degrading enzymes of human serum in a dose-dependent way, again more potently than classic inhibitors.7
Mechanistically, this is an attractive and internally consistent story. If anxiety is associated with excessively rapid enkephalin degradation, and Selank slows that degradation, then Selank could raise ambient enkephalin tone and produce a calming, mood-stabilizing effect through the body’s own opioid peptides rather than through exogenous opioid receptor agonism. Crucially, this would be a fundamentally different pharmacology from opioid drugs: rather than flooding opioid receptors with an external agonist (with all the attendant tolerance, dependence, and respiratory risks), Selank would merely extend the signaling life of the peptides the body already makes. This framing is often used to explain why Selank is not thought to carry classical opioid abuse liability.
There is even downstream behavioral support that touches the opioid system. A 2022 study by Konstantinopolsky and colleagues tested Selank in a naloxone-precipitated morphine-withdrawal model in rats and reported that a single dose at an anxiolytic level (0.3 mg/kg) reduced the total morphine-withdrawal index by roughly 40 percent, attenuated specific withdrawal signs such as convulsive reactions and posture disturbances, and raised tactile sensitivity thresholds — effects the authors compared to those of diazepam.8 That finding is consistent with an interaction between Selank and stress-and-opioid circuitry, though it is again a rodent result and does not establish any human application.
The measured reading is that the enkephalin-degradation mechanism is biochemically well demonstrated in vitro — Selank genuinely inhibits these enzymes — but the leap from “inhibits an enzyme in a test tube at micromolar concentrations” to “raises brain enkephalin tone enough to regulate human behavior” requires that sufficient Selank reach the relevant tissue at sufficient concentration, which, as noted, has not been rigorously demonstrated in humans. The enzyme inhibition is real; its behavioral sufficiency is inferred.
BDNF, Monoamines, and Neurotrophic Signaling
A third pathway moves from fast neurotransmission to slower, structural changes in the brain: neurotrophic signaling, and in particular brain-derived neurotrophic factor (BDNF). BDNF supports the survival, growth, and plasticity of neurons and is implicated in mood regulation; reduced BDNF signaling is associated with depression and stress, and many antidepressants raise BDNF over time. A compound that increased BDNF could therefore plausibly influence mood and behavior through neuroplasticity rather than through moment-to-moment receptor activity.
The key study here is by Inozemtseva and colleagues, who administered Selank intranasally to rats and measured BDNF in the hippocampus.9 They reported that Selank increased BDNF mRNA levels three hours after administration and BDNF protein levels twenty-four hours after administration, at doses of 250 and 500 micrograms per kilogram.9 Notably, the pattern suggested Selank stimulates local BDNF expression within hippocampal cells rather than merely increasing its transport from elsewhere — a distinction that matters for interpreting the effect as a genuine local neurotrophic action. This is one of the more mechanistically concrete findings in the Selank literature, because it links a defined dose and route to a measurable, time-resolved change in a mood-relevant neurotrophin.
A related study by Kolik and colleagues extended the BDNF theme into a behavioral-cognitive context, examining Selank in aged rats exposed to chronic ethanol.10 They reported that Selank (0.3 mg/kg daily for seven days) produced a cognitive-stimulating effect in older rats not exposed to ethanol and prevented ethanol-withdrawal-associated memory and attention disturbances, while modulating BDNF content in the hippocampus and frontal cortex.10 The authors interpreted the results as confirming involvement of a BDNF-related neurotrophic mechanism in Selank’s effects on age-related and alcohol-associated cognitive impairment. Again, the framing is careful and the model is specific — but it is a rodent model of alcohol-related cognitive change, not a human cognitive-enhancement trial.
Beyond BDNF, Selank has been reported to influence monoamine neurotransmitters, including effects on serotonin metabolism. Studies in rats have described Selank altering the concentration and turnover of monoamines and inducing serotonin metabolism in certain brain regions, which is often invoked to explain putative mood and anxiety effects and to draw an analogy (a loose one) with serotonergic antidepressants.4 The serotonergic evidence is thinner and less mechanistically pinned down than the BDNF work, and it should be treated as suggestive rather than established.
Taken together, the neurotrophic and monoaminergic pathway offers a plausible route by which Selank could exert slower, plasticity-based influences on mood and cognition, distinct from its faster GABAergic and enkephalinergic actions. It is worth noting how different this is in character from the anxiolytic mechanisms: BDNF effects unfold over hours to days and would predict cumulative rather than acute benefits. Readers interested in how neurotrophic and growth-factor signaling is discussed for other peptides can compare the framing in coverage of BPC-157 and nerve and brain health and of sermorelin and age-related cognitive function, both of which similarly involve plausible mechanisms held to a demanding evidentiary standard.
Immune-to-Brain Crosstalk: Cytokines as Behavioral Modulators
The fourth pathway is the one most tied to Selank’s tuftsin ancestry and the least familiar to those who think of anxiolytics purely in neurotransmitter terms: immune-to-brain signaling. Because Selank derives from an immunomodulatory peptide, several of its proposed behavioral effects run through cytokines — the signaling molecules of the immune system, which are increasingly recognized as powerful modulators of mood and behavior.
The relevant clinical-immunological work comes from Uchakina and colleagues, who studied Selank’s effects on cytokines in patients with anxiety-asthenic disorders.11 They reported that Selank modulated interleukin-6 (IL-6) — a pro-inflammatory cytokine strongly linked to depression and sickness behavior — and shifted the balance of T-helper (Th1/Th2) cytokines, with effects observed in the serum of patients receiving Selank over fourteen days.11 In vitro work described in the same line of research indicated that Selank could suppress IL-6 gene expression in immune cells from patients but not necessarily from healthy controls, and could influence interferon-related signaling.11 The proposed logic is that by damping pro-inflammatory cytokine tone, Selank could relieve the component of anxiety and asthenia (fatigue, weakness) that is driven or sustained by low-grade inflammation.
This mechanism is scientifically fashionable and biologically reasonable — the neuroinflammatory model of depression and anxiety is one of the most active areas in psychiatry, and IL-6 in particular is a well-validated correlate of mood disorder. A peptide that modulates IL-6 and cytokine balance could, in principle, influence behavior through the same immune-to-brain pathways that make people feel low and anxious when they are physically ill. It also fits Selank’s origin: an IgG-derived immune peptide acting on immune signaling is more mechanistically coherent than an immune peptide somehow behaving purely like a neurotransmitter.
The caution is the same as elsewhere, only sharper: the cytokine studies are small, are conducted in specific patient populations by the developing groups, and describe biomarker changes rather than definitively causal links to behavior. Showing that Selank lowers IL-6 in some patients is not the same as showing that this cytokine change causes the anxiety reduction, nor that it does so reliably across populations. The immune pathway is best understood as a genuinely interesting and distinctive feature of Selank’s proposed pharmacology — one that sets it apart from conventional anxiolytics — whose behavioral relevance remains to be established with proper controlled designs.
The following table summarizes the four proposed CNS pathways, the nature of the primary evidence for each, and the system in which that evidence was obtained — a reminder that “mechanism” ranges from careful binding assays to inferential clinical biomarker studies.
| Proposed pathway | Molecular action | Nature and system of primary evidence | Evidence strength |
|---|---|---|---|
| GABAergic | Positive allosteric modulation of GABA-A binding, not at the benzodiazepine site2 | Radioligand binding on brain membranes; gene expression in IMR-32 cells23 | Moderate (mechanistic) |
| Enkephalinergic | Inhibition of enkephalin-degrading enzymes (IC50 ≈15 µM)6 | Enzyme kinetics in human serum; anxiety-patient correlations67 | Moderate in vitro; inferential in vivo |
| Neurotrophic / monoaminergic | Increased hippocampal BDNF expression; altered serotonin metabolism9 | Intranasal dosing in rats; ethanol-cognition rat model910 | Preclinical (rodent) |
| Immune / cytokine | Modulation of IL-6 and Th1/Th2 cytokine balance; interferon signaling11 | Small patient studies and in vitro immune-cell work11 | Preliminary (biomarker) |
What the Human Clinical Evidence Actually Shows
Everything above concerns mechanism. The harder and more important question is whether Selank has been shown to regulate behavior in humans through properly controlled clinical study. Here candor is essential, because this is where the gap between reputation and evidence is widest.
The cornerstone clinical citation is a 2008 study by Zozulia, Neznamov, and colleagues, published in the Russian journal Zhurnal Nevrologii i Psikhiatrii, which evaluated Selank in patients with generalized anxiety disorder (GAD) and neurasthenia.4 In a comparative design, patients received either Selank or medazepam (a benzodiazepine), with outcomes measured on standard instruments — the Hamilton Anxiety Scale, the Zung scale, and Clinical Global Impression — alongside biochemical measures such as serum enkephalin activity. The reported result was that Selank produced anxiolytic activity broadly comparable to medazepam on these scales, with additional anti-asthenic (anti-fatigue) effects and a favorable side-effect profile, and that increases in serum leu-enkephalin half-life correlated with the reduction in anxiety — a finding that ties the clinical effect back to the enkephalin mechanism.4
On its face this is a supportive result, and it is the study most often cited to justify Selank’s status as a registered anxiolytic in Russia. But several limitations must be stated plainly. The trial was small — on the order of a few dozen patients per arm. It compared Selank against an active comparator rather than definitively against placebo in a large, blinded, multicenter design of the sort Western regulators demand. It was conducted by the group associated with the compound’s development, in a single national research context, and it has not, to the best of the available literature, been replicated by fully independent investigators outside Russia. A single small comparative study, however carefully done, cannot bear the weight of a confident claim that a drug “regulates behavior” in the general sense the title implies.
The broader clinical literature reinforces this reading. Additional Russian-language reports describe Selank’s effects on anxiety, asthenia, and associated immune and neurochemical markers, and conference abstracts have described patterns of rapid versus slow clinical response during GAD treatment.11 But the corpus as a whole shares consistent limitations: small samples, concentration within the developing country and its associated laboratories, limited blinding and placebo control by contemporary standards, and near-absence of independent international replication. There are no large-scale, regulator-grade Phase 3 trials of the kind that support FDA- or EMA-approved anxiolytics. This is precisely why Selank is not approved in the United States or the European Union — not because it has failed such trials, but because they have essentially never been done.
It is important to be even-handed here. The absence of large Western trials is not proof that Selank is ineffective; it is proof that its efficacy has not been established to the standard those regulators require. A compound can be genuinely useful and still under-evidenced, particularly when its development occurred largely within one national research system with limited incentive or funding for the enormous, expensive trials Western approval demands. The correct scientific posture is neither dismissal nor endorsement, but calibrated uncertainty: there is a real, if modest, human signal, embedded in a body of evidence too small and too concentrated to support strong conclusions.
Preclinical Behavioral Models and the Translation Problem
Because the human evidence is thin, much of the case for Selank as a behavioral regulator rests on animal work. It is therefore worth understanding what those models can and cannot tell us.
Selank has been examined across a range of rodent behavioral paradigms associated with anxiety, stress, and adaptive behavior. Kozlovskaya and colleagues, in a review of Selank and short peptides of the tuftsin family, described antistress and positive emotional effects in conflict-based models of emotional stress, attributing physiologically significant effects to the peptides’ molecular structures and their degradation fragments.1 The unpredictable-chronic-mild-stress work of Kasian and colleagues, discussed earlier, used elevated-plus-maze measures of anxiety-like behavior and reported meaningful reductions, particularly in combination with diazepam.5 The morphine-withdrawal study demonstrated attenuation of aversive withdrawal signs, a different but related behavioral domain touching stress and dependence circuitry.8 And the ethanol-cognition study linked Selank to preserved memory and attention in a challenge model.10
These are legitimate, published behavioral findings, and collectively they establish that Selank produces detectable, dose-related effects in validated rodent assays of anxiety and stress — effects that align with the proposed GABAergic, enkephalinergic, and neurotrophic mechanisms. That coherence between mechanism and behavior in animals is a genuine strength of the Selank literature relative to some research peptides that have mechanism claims but little behavioral data.
The unavoidable caveat is the translation problem. The history of anxiolytic and antidepressant development is littered with compounds that produced clean, reproducible effects in rodent anxiety models and then failed to translate into human benefit. Rodent models such as the elevated plus maze capture certain conserved features of anxiety-related behavior but are imperfect predictors of clinical efficacy, and effects that look robust in a stressed rat frequently shrink or vanish in a randomized human trial. So while the preclinical behavioral data are supportive and internally consistent, they cannot substitute for the human evidence that is lacking. The animal work makes Selank a reasonable candidate for further study; it does not make it a proven behavioral therapeutic.
The following table places the principal preclinical and clinical evidence side by side, to make the structure of the overall evidence base visible at a glance.
| Study / source | System | Behavioral or clinical domain | Key reported outcome |
|---|---|---|---|
| Zozulia et al. 20084 | Humans (GAD, neurasthenia) | Anxiety, asthenia | Anxiolysis comparable to medazepam; small, single-context trial |
| Uchakina et al. 200811 | Humans (anxiety-asthenic) | Immune/behavioral markers | Modulation of IL-6 and Th1/Th2 balance |
| Kasian et al. 20175 | Rats (chronic mild stress) | Anxiety-like behavior | Selank + diazepam most effective; minimal sedation from Selank |
| Konstantinopolsky et al. 20228 | Rats (morphine withdrawal) | Withdrawal-related distress | ~40% reduction in withdrawal index |
| Kolik et al. 201910 | Aged rats (ethanol) | Memory, attention | Preserved cognition; BDNF modulation |
| Inozemtseva et al. 20089 | Rats (intranasal) | Neurotrophic substrate | Increased hippocampal BDNF mRNA and protein |
Dosing, Formulation, and Routes in a Research Context
Because Selank is encountered by researchers as a lyophilized (freeze-dried) powder and, in its registered Russian form, as an intranasal solution, a brief and strictly educational note on handling is warranted — with the emphasis that this describes standard research-peptide practice and the compound’s studied formulations, not a usage recommendation, and that Selank is not approved for human use outside its specific regional registrations.
The registered Russian anxiolytic product is formulated as a nasal drop solution, and the intranasal route dominates both clinical use and much of the human research, chosen for the nose-to-brain delivery rationale discussed earlier. Preclinical studies have variously used intranasal, intraperitoneal, and intravenous routes; the rodent BDNF and behavioral studies cited above used doses in the range of roughly 0.3 mg/kg (behavioral studies) up to 250–500 µg/kg (the intranasal BDNF study), figures that illustrate how dose and route vary with experimental purpose rather than constituting any human dosing guidance.89
As a lyophilized research peptide, Selank shares the general handling considerations of the class. Reconstitution for laboratory purposes is typically performed with sterile or bacteriostatic water, directed slowly against the vial wall rather than sprayed onto the powder, with gentle swirling rather than shaking, because vigorous agitation can shear peptide bonds. The chosen diluent volume simply sets the working concentration — a fixed mass of peptide in a larger volume yields a lower concentration, the arithmetic behind any reconstitution calculation. General educational walkthroughs of this arithmetic appear in the site’s peptide reconstitution guide and its dosage calculator, both of which present the calculations for illustrative purposes rather than as guidance for human use.
Stability considerations recurring across the research-peptide literature apply to Selank as well: lyophilized material is generally stored cold and dark, favored by freezing for long-term stability; reconstituted solution is refrigerated and used within a limited window; light, heat, repeated freeze-thaw cycles, and vigorous agitation all promote degradation; and aseptic technique matters, with bacteriostatic water preferred for any multi-use context. It bears repeating that meticulous handling changes nothing about the evidence question. A perfectly reconstituted, high-purity vial of Selank is still a compound whose human behavioral efficacy rests on a thin, unreplicated clinical base. Good technique preserves whatever activity the molecule has; it does not create efficacy where the trials to demonstrate it have not been done. Terms encountered in this handling context are defined in the site’s peptide glossary.
Safety, Tolerability, and How Selank Compares With Established Anxiolytics
One area where Selank’s reputation is comparatively favorable is short-term tolerability — but this too must be stated carefully, because “appeared well tolerated in small studies” is not the same as “established as safe,” and the safety database is as limited as the efficacy database.
In the human studies reported, Selank was generally described as well tolerated over the studied durations, without the pronounced sedation, psychomotor impairment, or dependence liability associated with benzodiazepines, and without a clear withdrawal syndrome on discontinuation.4 The mechanistic rationale for this benign profile is coherent: if Selank modulates GABA allosterically without engaging the benzodiazepine site,2 and acts through endogenous enkephalin and neurotrophic systems rather than as a direct receptor agonist, one would predict less of the tolerance-and-dependence pharmacology that plagues benzodiazepines. The rodent data reinforcing minimal locomotor sedation relative to diazepam fit this picture.5
Several caveats temper any reassurance. The safety data come from small, short-duration studies in specific populations; long-term safety is essentially uncharacterized. There are no rigorous data on use in pregnancy, in children, in the elderly with polypharmacy, or in people with significant medical comorbidity. Interactions with other CNS-active drugs — including the very benzodiazepines and antipsychotics with which Selank has been studied in combination — are not well mapped in humans. And because most Selank encountered outside its regional registration is sold as “research chemical” material of variable purity, real-world risks from impurities, endotoxin, or mislabeling are substantial and have nothing to do with the molecule’s intrinsic pharmacology. Intranasal administration also carries its own local-tolerability considerations that differ from systemic routes.
Placed beside established anxiolytics, Selank occupies a distinctive but under-evidenced position. The comparison below is not an endorsement of interchangeability — the evidence bases are wildly asymmetric — but it clarifies where Selank sits mechanistically and evidentially.
| Feature | Selank | Benzodiazepines (e.g. diazepam) | SSRIs |
|---|---|---|---|
| Primary mechanism | Allosteric GABA modulation + enkephalin/BDNF/cytokine effects (proposed)26 | Benzodiazepine-site GABA-A agonism | Serotonin reuptake inhibition |
| Onset | Reported rapid (anxiolytic)4 | Rapid | Delayed (weeks) |
| Sedation | Minimal reported5 | Prominent | Variable |
| Dependence liability | Low (proposed; limited data) | High | Discontinuation effects |
| Evidence base | Small Russian trials + rodent data; not replicated internationally4 | Extensive, decades of RCTs | Extensive, decades of RCTs |
| Regulatory status | Registered in Russia; not FDA/EMA approved | Approved worldwide | Approved worldwide |
The table makes the central asymmetry unmistakable. Selank’s proposed advantages — rapid onset without sedation or dependence — are genuinely appealing on paper, and if they held up they would address real limitations of benzodiazepines. But the rightmost columns of the evidence and regulatory rows tell the honest story: benzodiazepines and SSRIs rest on decades of large, replicated, independently scrutinized trials, while Selank rests on a handful of small studies concentrated in one research tradition. The mechanistic promise is real; the evidentiary parity is not remotely there.
Regulatory Status
Selank’s regulatory position is unusual and frequently misrepresented, so precision matters.
Registered in Russia, not in the West. Selank is registered as a prescription anxiolytic medication in Russia (and has been used in some neighboring jurisdictions), where it is prescribed for anxiety and asthenic conditions on the strength of the domestic clinical program. It is not approved by the U.S. Food and Drug Administration, the European Medicines Agency, or comparable Western regulators for any indication. There is no approved Selank product in the United States or European Union, and it has not undergone the large-scale, independent, regulator-grade trials those agencies require. This regional split is the single most important fact about its status: a genuine registered medicine in one system, an investigational and unapproved substance in another.
U.S. compounding and research-chemical gray zone. In the United States, Selank has moved through the ambiguous territory surrounding pharmacy compounding of peptides. It was among peptide substances that appeared on and were subsequently removed from the interim Category 2 of the FDA’s Section 503A bulk drug substances list, and its nomination for consideration was withdrawn rather than approved.12 Removal from a category is not the same as authorization to compound; a substance must be affirmatively added to the 503A bulks list through formal review and rulemaking before licensed compounding pharmacies may legally use it, and Selank has not cleared that bar.12 In practice, most Selank in circulation in Western markets is sold as a “research chemical” explicitly not for human use, a designation that carries no assurance of purity, identity, or safety.
Implications for the behavioral-regulation claim. The regulatory picture reinforces the evidentiary one. Regulators approve drugs when the totality of controlled evidence establishes that benefits outweigh risks for a defined indication. Selank’s registration in Russia reflects a national judgment based on the domestic program; its absence of Western approval reflects the absence of the large, independent, replicated trials those systems demand. Neither situation licenses a confident universal claim that Selank “regulates behavior” in the way an approved anxiolytic does. For any legitimate exploration of Selank’s behavioral pharmacology, the appropriate path is formal preclinical and clinical research under proper oversight, not off-label or informal human use. Readers tracking how other investigational peptides sit within this regulatory landscape can review the framing applied to compounds such as NAD-based neuroprotection candidates, which face the same demand for controlled human evidence before any therapeutic claim is warranted.
Frequently Asked Questions
Does Selank actually regulate behavior through the brain?
There is a plausible, partially supported mechanistic case that it can, but no confirmation to the standard of an approved drug. Selank has documented effects on GABA binding,2 enkephalin-degrading enzymes,6 hippocampal BDNF,9 and cytokines such as IL-6,11 and it produces anxiety-reducing effects in rodent models.5 But the human evidence is limited to small studies conducted largely by the developing groups, without large independent replication. So the honest answer is that the CNS mechanisms are real and interesting, while the claim of reliable behavioral regulation in humans remains under-evidenced.
How is Selank different from a benzodiazepine like Valium?
At the molecular level, quite different. Radioligand studies indicate Selank acts as a positive allosteric modulator of GABA-A receptors without binding the benzodiazepine site that diazepam uses.2 It also acts through non-GABA pathways (enkephalin, BDNF, cytokines). In rodents it produces anxiolytic effects with minimal sedation, unlike diazepam.5 This profile is often cited to suggest lower dependence and sedation liability, but the human safety database is far too small to confirm those advantages, whereas benzodiazepines rest on decades of trials.
Is Selank approved by the FDA?
No. Selank is a registered prescription anxiolytic in Russia but is not approved by the FDA or EMA for any indication. In the United States it has passed through the ambiguous territory of peptide compounding regulation without being approved for that use, and most Selank sold in Western markets is labeled as a research chemical not for human consumption.12
What is the strongest scientific evidence for Selank?
The most concrete mechanistic findings are the radioligand demonstration of allosteric GABA modulation,2 the biochemical demonstration that Selank inhibits enkephalin-degrading enzymes,6 and the time-resolved increase in hippocampal BDNF after intranasal dosing in rats.9 The main human evidence is a small comparative trial in generalized anxiety disorder and neurasthenia reporting anxiolysis comparable to medazepam.4 None of these individually establishes efficacy at a regulatory standard.
Why is most Selank research from Russia?
Selank was developed at the Institute of Molecular Genetics of the Russian Academy of Sciences, and its clinical development occurred within the Russian medical-research system.4 The compound was registered there, so the studies and the clinical experience are concentrated in Russian-language literature. The near-absence of independent Western trials is a limitation of the evidence base, not proof of ineffectiveness — the expensive, large-scale trials required for FDA or EMA approval have essentially not been undertaken.
How is Selank usually administered in studies?
The registered Russian product is an intranasal solution, and intranasal delivery is favored on the rationale that some peptide may reach the brain via nose-to-brain routes.9 Preclinical studies have also used intraperitoneal and intravenous routes. The actual fraction of an intranasal peptide dose reaching functionally relevant brain concentrations is generally small and has not been rigorously quantified for Selank in humans, which is an important caveat for any central-action claim.
Does Selank have side effects or cause dependence?
In the small studies reported, Selank was generally well tolerated without prominent sedation or a clear withdrawal syndrome,4 and its proposed mechanisms predict low dependence liability. However, long-term safety, use in vulnerable populations, and drug interactions are essentially uncharacterized, and research-chemical material of unverified purity carries additional, unrelated risks. Absence of demonstrated harm in small short-term studies is not the same as established long-term safety.
Can Selank be used to treat anxiety or depression?
It is used as a prescription anxiolytic in Russia, but it is not approved for anxiety, depression, or any other condition in the United States or European Union, and the controlled evidence is insufficient to support a general therapeutic claim.4 Nothing here is medical advice. Anyone considering treatment for anxiety or depression should work with a qualified clinician using therapies supported by robust evidence.
References
- Kozlovskaya MM, Kozlovskii II, Val’dman EA, Seredenin SB. Selank and short peptides of the tuftsin family in the regulation of adaptive behavior in stress. Neurosci Behav Physiol. 2003;33(9):853-860. PMID: 14969422. https://pubmed.ncbi.nlm.nih.gov/14969422/
- Vyunova TV, Andreeva LA, Shevchenko KV, Myasoedov NF. Peptide-based Anxiolytics: The Molecular Aspects of Heptapeptide Selank Biological Activity. Protein Pept Lett. 2018;25(10):914-923. PMID: 30255741. https://pubmed.ncbi.nlm.nih.gov/30255741/
- Filatova E, Kasian A, Kolomin T, et al. GABA, Selank, and Olanzapine Affect the Expression of Genes Involved in GABAergic Neurotransmission in IMR-32 Cells. Front Pharmacol. 2017;8:89. PMID: 28293190. PMCID: PMC5328971. https://pmc.ncbi.nlm.nih.gov/articles/PMC5328971/
- Zozulia AA, Neznamov GG, Siuniakov TS, et al. [Efficacy and possible mechanisms of action of a new peptide anxiolytic selank in the therapy of generalized anxiety disorders and neurasthenia]. Zh Nevrol Psikhiatr Im S S Korsakova. 2008;108(4):38-48. PMID: 18454096. https://pubmed.ncbi.nlm.nih.gov/18454096/
- Kasian A, Kolomin T, Andreeva L, et al. Peptide Selank Enhances the Effect of Diazepam in Reducing Anxiety in Unpredictable Chronic Mild Stress Conditions in Rats. Behav Neurol. 2017;2017:5091027. PMID: 28280289. PMCID: PMC5322660. https://pmc.ncbi.nlm.nih.gov/articles/PMC5322660/
- Zozulya AA, Kost NV, Sokolov OY, et al. The inhibitory effect of Selank on enkephalin-degrading enzymes as a possible mechanism of its anxiolytic activity. Bull Exp Biol Med. 2001;131(4):315-317. PMID: 11550013. https://pubmed.ncbi.nlm.nih.gov/11550013/
- Kost NV, Sokolov OY, Gabaeva MV, et al. Semax and Selank inhibit the enkephalin-degrading enzymes from human serum. Russ J Bioorg Chem (Bioorg Khim). 2001;27(3):180-183. PMID: 11443939. https://pubmed.ncbi.nlm.nih.gov/11443939/
- Konstantinopolsky MA, Chernyakova IV, Kolik LG. Selank, a Peptide Analog of Tuftsin, Attenuates Aversive Signs of Morphine Withdrawal in Rats. Bull Exp Biol Med. 2022;173(5):609-613. PMID: 36322304. https://pubmed.ncbi.nlm.nih.gov/36322304/
- Inozemtseva LS, Karpenko EA, Dolotov OV, et al. Intranasal administration of the peptide Selank regulates BDNF expression in the rat hippocampus in vivo. Dokl Biol Sci. 2008;421:241-243. DOI: 10.1134/S0012496608040066. https://link.springer.com/article/10.1134/S0012496608040066
- Kolik LG, Nadorova AV, Antipova TA, et al. Selank, Peptide Analogue of Tuftsin, Protects Against Ethanol-Induced Memory Impairment by Regulating of BDNF Content in the Hippocampus and Prefrontal Cortex in Rats. Bull Exp Biol Med. 2019;167(5):641-644. PMID: 31625062. https://pubmed.ncbi.nlm.nih.gov/31625062/
- Uchakina ON, Uchakin PN, Miasoedov NF, et al. [Immunomodulatory effects of selank in patients with anxiety-asthenic disorders]. Zh Nevrol Psikhiatr Im S S Korsakova. 2008;108(5):71-75. PMID: 18577961. https://pubmed.ncbi.nlm.nih.gov/18577961/
- U.S. Food and Drug Administration. Certain Bulk Drug Substances for Use in Compounding That May Present Significant Safety Risks (Section 503A interim Category 2 list; Selank acetate among peptide substances removed as of September 27, 2024 following withdrawal of their nominations). https://www.fda.gov/drugs/human-drug-compounding/certain-bulk-drug-substances-use-compounding-may-present-significant-safety-risks
Educational and research-use disclaimer: This article is provided solely for scientific and educational purposes. Selank is not approved by the U.S. Food and Drug Administration, the European Medicines Agency, or comparable Western regulators for the treatment, cure, or prevention of anxiety, depression, or any other disease; it is a registered prescription anxiolytic only in Russia and certain neighboring jurisdictions, on the basis of a small and largely unreplicated clinical evidence base. The central-nervous-system mechanisms described here are drawn substantially from preclinical and Russian-language studies and should be regarded as proposed and partially supported rather than definitively established. Nothing here is medical advice or a recommendation for human use. Any legitimate investigation of Selank should occur within properly authorized preclinical or clinical research under appropriate oversight. Readers should consult qualified professionals and applicable regulations before making any decisions.