The headline question deserves an honest answer before we go any further: AOD-9604 has not been shown to deliver clinically backed fat loss in humans. The phrasing “clinically backed fat loss without affecting lean muscle” is a marketing claim that has circulated widely across wellness clinics and peptide vendors, but it does not survive contact with the actual clinical record. When AOD-9604 was carried into an adequately powered, randomized, placebo-controlled human obesity trial, it failed to produce statistically significant weight loss versus placebo, and its pharmaceutical development was terminated in 2007.8 That is the single most important fact anyone researching this compound should carry with them.
None of this means AOD-9604 is uninteresting. It has a genuinely elegant scientific origin story, a plausible and partially validated mechanism in animal models, and an unusually clean short-term safety signal in the human data that does exist.8 The gap is not between “dangerous” and “safe” — it is between “biologically plausible in mice” and “proven to work in people.” Understanding exactly where that gap sits is the whole point of a careful, evidence-first read of this molecule, and it is far more useful to a researcher than another round of recycled fat-loss promises.
This article walks through what AOD-9604 actually is, the mechanism its developers proposed and how much of it was demonstrated, the human and animal evidence graded honestly by strength, how it compares to related compounds, the laboratory models used to study it, its safety and tolerability record, handling considerations in a research setting, the specific reasons the human-efficacy case remains unproven, and its current regulatory status. Every substantive claim is tied to a primary source in the reference list. Where the evidence is thin — and for AOD-9604 it frequently is — this article says so plainly rather than filling the void with confident-sounding conjecture.
What AOD-9604 Is and Where It Came From
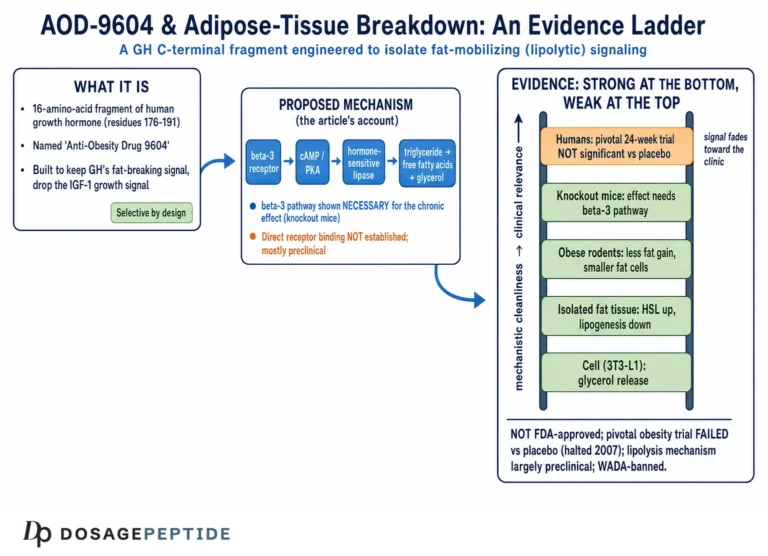
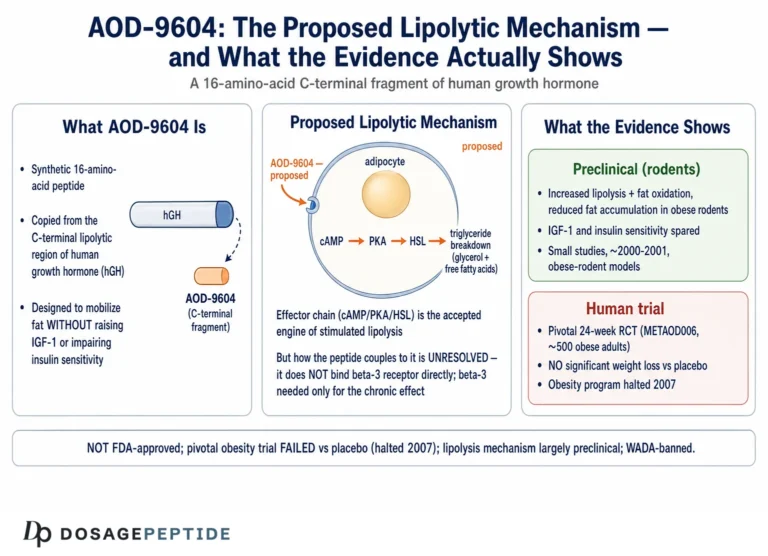
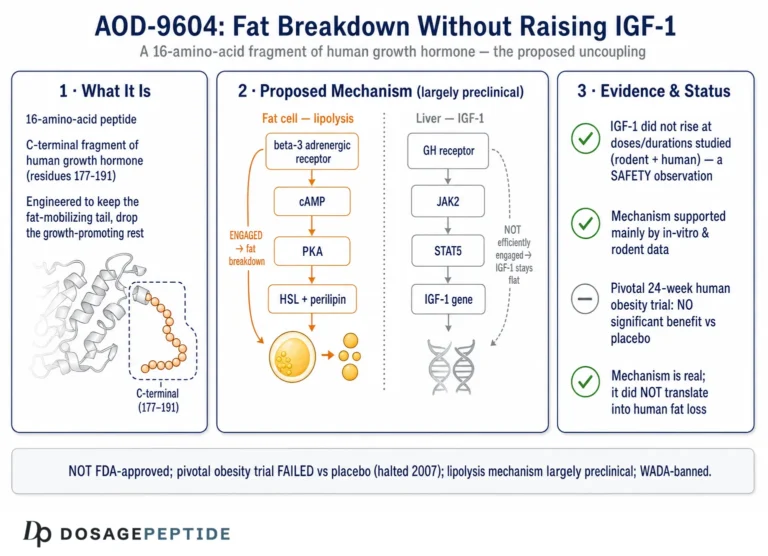
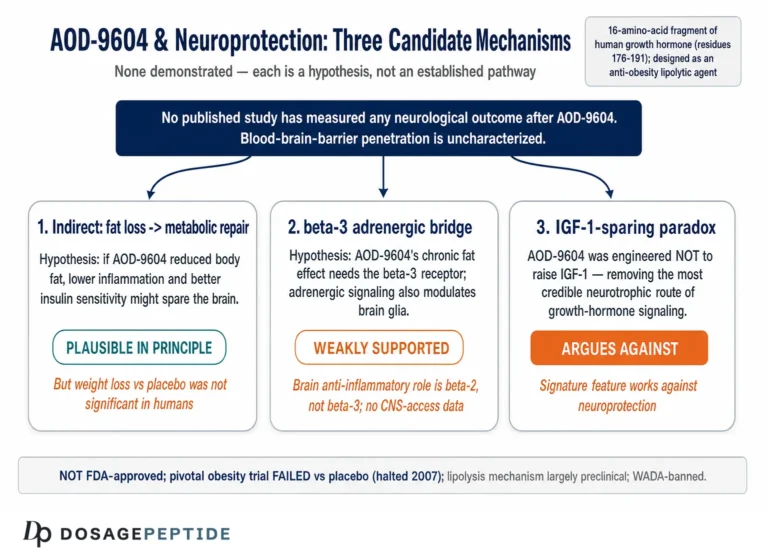
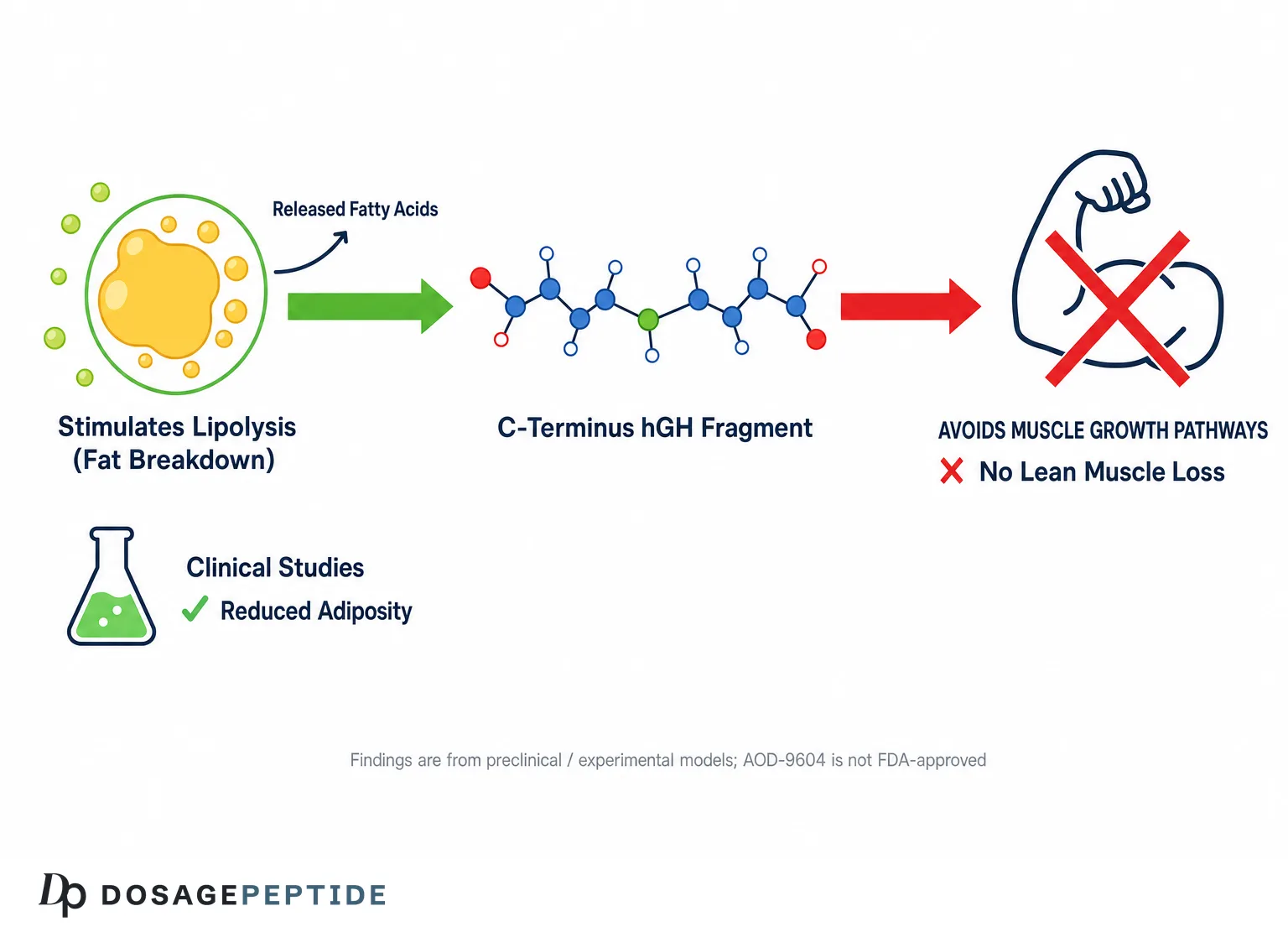
AOD-9604 is a synthetic peptide fragment derived from the C-terminal region of human growth hormone (hGH). Its name is an abbreviation of “Anti-Obesity Drug,” reflecting the therapeutic ambition under which it was created rather than any demonstrated effect. Structurally it corresponds to amino acid residues 176 through 191 of the hGH molecule — a 16-residue (hexadecapeptide) sequence — with one deliberate modification: a tyrosine residue is added at the N-terminus in place of, or ahead of, the native phenylalanine, a change introduced to improve the stability of the peptide.1 The published sequence is H-Tyr-Leu-Arg-Ile-Val-Gln-Cys-Arg-Ser-Val-Glu-Gly-Ser-Cys-Gly-Phe-OH, and the two cysteine residues form a disulfide bridge that helps the fragment retain a conformation resembling the corresponding loop within intact growth hormone.1
The compound emerged from research led by Professor Frank Ng and colleagues at Monash University in Australia during the 1990s, and was subsequently developed commercially by Metabolic Pharmaceuticals Ltd.14 The founding scientific idea was that the fat-metabolizing (lipolytic) activity of growth hormone might be separable from its growth-promoting and glucose-disrupting activities. Full-length hGH is a potent metabolic hormone, but using it to reduce body fat is problematic: it raises insulin-like growth factor 1 (IGF-1), can promote tissue growth, and tends to impair insulin sensitivity and glucose tolerance. The hypothesis behind AOD-9604 was that a small, defined region near the C-terminus of the molecule carried the lipolytic signal on its own, and that isolating this fragment could produce fat loss while leaving the growth-promoting and diabetogenic effects of the parent hormone behind.14
That is a legitimately clever premise, and it is worth appreciating on its own terms. Growth hormone’s C-terminal domain had been implicated in lipid metabolism in earlier structure-function work, and the Monash group set out to map and then reproduce that activity in a stand-alone peptide. AOD-9604 was not the only fragment they studied — a closely related analogue designated AOD9401 was characterized in parallel, particularly in rat models — and the broader research program is best understood as an attempt to define the smallest peptide domain that retained hGH’s lipolytic character.4
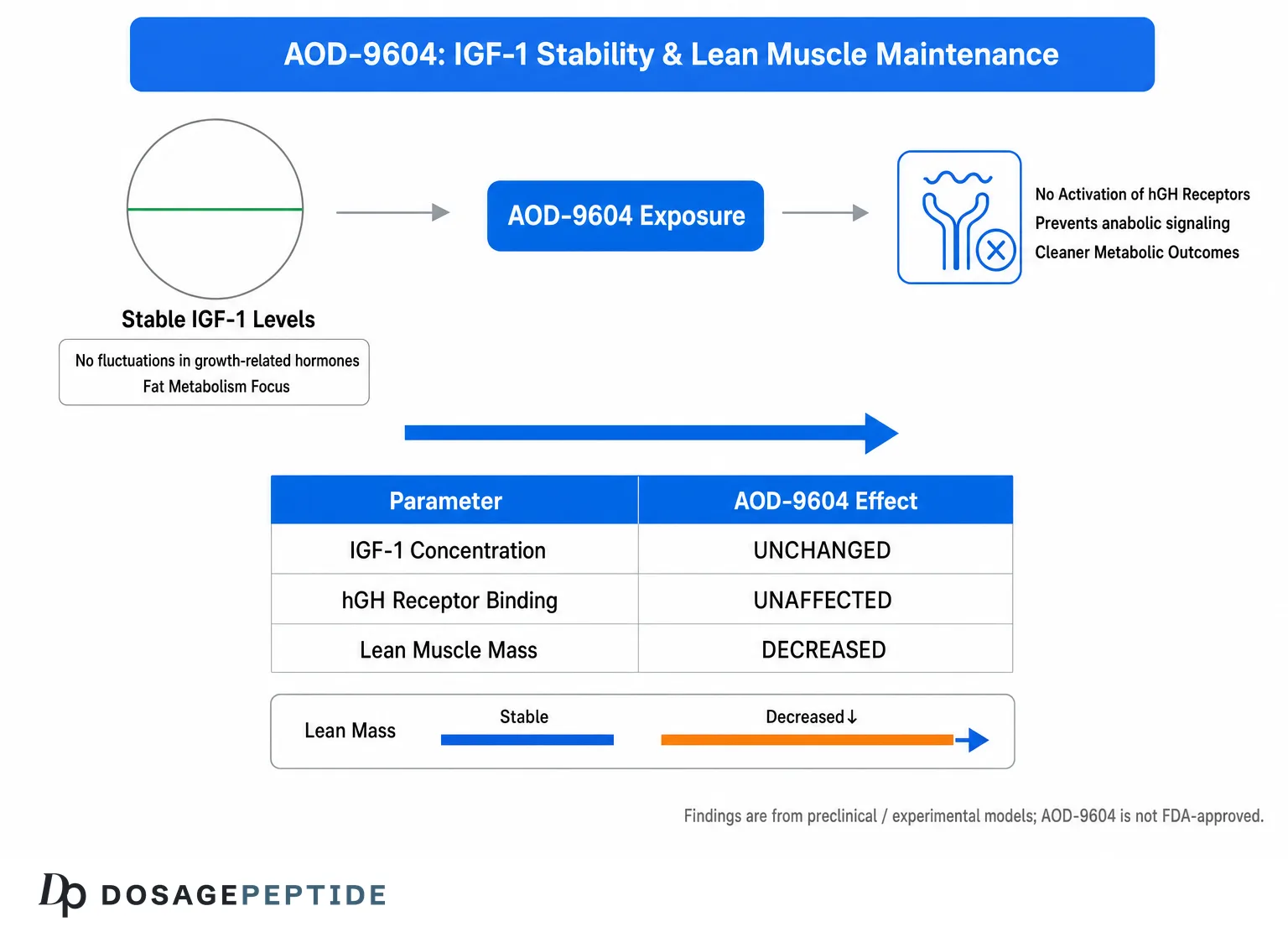
It is important not to overstate what the name and origin imply. AOD-9604 being “derived from growth hormone” does not make it growth hormone, and it does not confer growth hormone’s proven clinical effects. In fact the entire design goal was to strip away most of what growth hormone does. Crucially, AOD-9604 does not bind the growth hormone receptor and does not raise circulating IGF-1 in the models where it has been tested, which is central both to its proposed safety advantage and to the reason it cannot be assumed to share hGH’s body-composition effects.13 On the site, AOD-9604 appears in several research-oriented dosing references, including the AOD-9604 (2mg vial) dosage protocol and the AOD-9604 (5mg vial) dosage protocol, which are framed strictly as laboratory-handling references rather than treatment guidance.
To summarize the identity of the compound: AOD-9604 is a stabilized 16-amino-acid fragment of the C-terminus of human growth hormone, engineered in the 1990s at Monash University and developed by Metabolic Pharmaceuticals with the explicit goal of producing a fat-directed agent that avoids growth hormone’s growth-promoting and glucose-disrupting effects. Whether it achieves the fat-loss half of that ambition in humans is exactly the question the rest of this article examines.
The Proposed Molecular Mechanism of Action
The mechanistic story most often told about AOD-9604 has two halves: it is said to stimulate lipolysis (the breakdown of stored triglycerides into free fatty acids) and to inhibit lipogenesis (the conversion of energy substrates into new fat), while doing neither through the growth hormone receptor nor through elevation of IGF-1.13 Understanding how much of this is demonstrated versus inferred is essential, because the popular retelling frequently presents plausible biochemistry as if it were established human physiology.
The lipolytic side of the mechanism was investigated most directly in mouse work by Heffernan and colleagues. In obese mice, both hGH and AOD-9604 increased fat oxidation, reduced body-weight gain, and stimulated lipid metabolism.2 The pivotal mechanistic experiment used beta-3 adrenergic receptor (β3-AR) knockout mice: when AOD-9604 was administered to animals lacking the β3-AR, the metabolic changes seen in normal (wild-type) animals largely failed to appear.3 This is the strongest single piece of evidence that AOD-9604’s effect in mice depends on β3-adrenergic signaling — a pathway that, when activated, raises intracellular cyclic AMP, activates hormone-sensitive lipase, and drives triglyceride breakdown in fat cells. The knockout result matters because it moves beyond correlation toward a causal, pathway-specific explanation, at least within the mouse system.3
A frequently repeated claim in clinic and vendor write-ups is that AOD-9604 “binds the β3-adrenergic receptor” as an agonist. This is an over-specification of what the primary literature shows. The knockout experiments demonstrate that the β3-AR is required for the effect; they do not establish that AOD-9604 is a direct orthosteric agonist at that receptor in the way a small-molecule β3-agonist would be. The mechanistic literature more cautiously describes AOD-9604 as acting through, or upregulating signaling associated with, the β3-adrenergic pathway.3 This distinction is not pedantic: “requires a receptor” and “is a classical agonist of that receptor” are different pharmacological statements, and confidently asserting the latter goes beyond the data.
The anti-lipogenic half of the mechanism — the idea that AOD-9604 blocks the conversion of substrates into stored fat — is supported by animal and cell-based observations of reduced fat accumulation and smaller adipocytes after treatment, particularly in the Zucker rat work on the related fragment AOD9401, where adipocyte diameter fell from roughly 110 to 80 micrometers over a chronic treatment course.4 Whether AOD-9604 meaningfully suppresses lipogenesis in humans at tolerated exposures is not established.
The most consequential and best-supported mechanistic point is what AOD-9604 does not do. Across the animal studies, AOD-9604 did not interact with the growth hormone receptor, did not raise IGF-1, and — unlike full-length hGH — did not induce the insulin resistance and glucose intolerance associated with chronic growth hormone exposure.134 This “clean” metabolic profile is genuinely the compound’s most distinctive and reproducible feature. It is the basis for the appealing narrative that AOD-9604 could burn fat “like growth hormone” without growth hormone’s downsides.
But this is precisely where the mechanistic story is most often misused. Demonstrating that a compound lacks growth hormone’s harmful effects is not the same as demonstrating that it possesses growth hormone’s fat-loss efficacy in people. The absence of IGF-1 elevation is real and well documented; the presence of clinically meaningful human fat loss is not. A mechanism can be biologically coherent, receptor-dependent in a knockout model, and still fail to translate into a measurable clinical outcome — which, as the next section shows, is exactly what happened.
The Key Human Evidence — and Why It Does Not Support the Headline
This is the section the title of this article is really about, so it will be blunt. The claim that AOD-9604 produces “clinically backed fat loss” is not supported by the pivotal human trial. When the compound was tested in an adequately powered, randomized, double-blind, placebo-controlled study, it did not beat placebo on weight, and development was discontinued.8 Any content that presents human fat-loss efficacy as established is either unaware of, or omitting, this outcome.
The clinical program is usually summarized in two stages. An earlier, smaller phase in obese adults — a randomized, double-blind, placebo-controlled study with daily subcutaneous dosing over roughly 12 weeks across doses from about 0.25 mg to 1 mg — was reported to show a modest separation from placebo, on the order of a couple of kilograms of additional weight loss at the higher doses. These early figures (frequently quoted as roughly 2.6 kg on the top dose versus about 0.8 kg on placebo, or an average difference of a little under 2 kg) are the origin of essentially every “AOD-9604 causes fat loss” statement in circulation.8 They were encouraging enough to justify a larger confirmatory trial, which is exactly how drug development is supposed to work.
The larger confirmatory study is where the narrative collapses. A subsequent phase IIb trial enrolled several hundred obese participants (commonly cited as 536 subjects) in a randomized, double-blind, placebo-controlled design over 24 weeks, testing doses up to about 1 mg/day. It did not reproduce the earlier signal: AOD-9604 did not produce statistically significant weight loss versus placebo at the primary endpoint, and Metabolic Pharmaceuticals halted development of the compound for obesity in 2007.8 In evidentiary terms, a small promising study followed by a larger rigorous study that fails to confirm it is the classic pattern of an unproven intervention — the larger, better-powered result is the one that should dominate any honest assessment.
Two further caveats deepen the problem. First, the definitive negative trial’s full results were not published as a standalone peer-reviewed clinical paper; the failure is documented through company disclosures and secondary review rather than a primary efficacy publication in a major journal.8 That is a real limitation on the human record — the positive early numbers are better preserved in the literature than the negative confirmatory ones, which can create a misleading impression for anyone reading selectively. Second, even the early “positive” numbers describe modest weight change over a few months in a small sample; they never demonstrated the specific claim of preferential fat loss with lean-mass sparing at a level that would meet a modern efficacy standard.
The “without affecting lean muscle” portion of the headline deserves its own scrutiny. The mechanistic rationale — that a fat-directed, β3-dependent lipolytic signal that does not raise IGF-1 would act on adipose tissue rather than muscle — is reasonable, and body-composition measures were part of the research program.13 But “lean-mass sparing” is only a meaningful clinical claim if there is meaningful fat loss to spare muscle from, and the pivotal trial did not establish meaningful fat loss in the first place. You cannot credibly claim a favorable partition of a weight change that did not reach statistical significance.
It is also worth naming the cognitive trap that keeps the “clinically backed” claim alive. The early, smaller, more optimistic numbers are easy to quote and emotionally satisfying, while the larger negative result is harder to find and less quotable, so the weaker evidence circulates more freely than the stronger evidence. A disciplined reader does the opposite of what the marketing does: weight the single best-designed, best-powered study most heavily and treat a promising pilot that a rigorous confirmatory trial failed to reproduce as a hypothesis that was tested and not supported, rather than as a benefit that merely awaits rediscovery. Applied to AOD-9604, that discipline points to one conclusion.
The honest bottom line on human evidence is therefore straightforward. The best-supported human finding for AOD-9604 is a short-term safety and tolerability signal, not an efficacy signal.8 On the efficacy question that the title poses, the strongest and most rigorous human data point in the opposite direction: no significant weight-loss benefit over placebo. AOD-9604 should be described as a research compound with an unproven human fat-loss effect — full stop.
Preclinical and Animal Research
If the human efficacy record is weak, the animal and cell-based record is where AOD-9604’s scientific interest actually lives — provided it is not oversold as if mouse results were human results. The preclinical work is genuinely the foundation of the whole story, and it is reasonably coherent within its own domain.
The earliest defining studies characterized the synthetic lipolytic domain itself. Ng and colleagues published metabolic studies of AOD-9604 establishing that this small C-terminal fragment reproduced lipolytic activity associated with growth hormone while lacking hGH-receptor interaction — the proof of concept that a stand-alone peptide could carry the lipolytic signal.1 In parallel, the related fragment AOD9401 was studied in obese Zucker fatty rats, where chronic treatment reduced body-weight gain and shrank adipocytes, and — importantly — did not induce the insulin resistance or glucose intolerance that chronic hGH would.4 These rat data are the origin of the “fat effects without the glucose penalty” framing.
The mouse studies by Heffernan and colleagues built the mechanistic and body-composition case. Chronic treatment of obese mice with either hGH or AOD-9604 increased fat oxidation and reduced weight gain, and the β3-AR knockout experiments showed the effect depended on intact β3-adrenergic signaling.23 A separate strand of work examined oral administration of a synthetic hGH fragment and its effects on lipid metabolism, exploring whether the molecule could act after oral dosing — relevant because oral bioavailability of peptides is normally poor, and a fat-loss agent that survived the gut would have been commercially attractive.5
Beyond obesity, a smaller preclinical literature examined AOD-9604 in cartilage and joint contexts. A 2015 rabbit osteoarthritis study reported that intra-articular AOD-9604, alone and especially in combination with hyaluronic acid, was associated with greater cartilage regeneration than saline control.7 This is frequently invoked to support “joint health” marketing, but it is a single small-animal study in a specific injury model, and no human randomized trial of AOD-9604 for osteoarthritis has been published. It should be treated as an early hypothesis-generating result, not as evidence of a joint benefit in people.
| Study / model | System | Principal finding | What it does not show |
|---|---|---|---|
| Ng et al. (2000)1 | Synthetic domain / metabolic characterization | AOD-9604 reproduces lipolytic activity without hGH-receptor binding | No human efficacy |
| Ng et al. (2000), AOD94014 | Zucker fatty rats | Reduced weight gain, smaller adipocytes, no glucose intolerance | Different analogue; rodent only |
| Heffernan et al. (2001)2 | Obese mice | Increased fat oxidation, reduced weight gain | Rodent dose/exposure, not human |
| Heffernan et al. (2001), knockout3 | β3-AR knockout mice | Effect requires β3-adrenergic signaling | Does not prove direct β3 agonism |
| Kwon & Park (2015)7 | Rabbit osteoarthritis | Cartilage regeneration vs saline, better with HA | Single small-animal study; no human trial |
The correct way to read this body of work is that AOD-9604 has a real, internally consistent preclinical rationale: it does something to fat metabolism in rodents through a β3-dependent pathway, without the growth and glucose liabilities of hGH. The error to avoid is treating that rodent coherence as if it settled the human question. Many compounds with clean, mechanistically satisfying animal data — including in obesity specifically — have failed in human trials, and AOD-9604 is one of them.8 Preclinical strength is a reason to run human trials, not a substitute for their results.
How AOD-9604 Compares With Related Compounds
AOD-9604 is frequently discussed alongside a cluster of other peptides, and the comparisons are often muddled. Setting them out clearly helps a researcher understand what is actually being compared, and it repeatedly reinforces the central point that mechanistic difference does not equal proven human benefit.
The most direct comparison is to HGH Fragment 176-191, sometimes just called “the frag.” This is the same underlying 176-191 region of growth hormone; AOD-9604 is essentially a stabilized, tyrosine-modified version of that fragment developed for pharmaceutical use.1 In practice the two are close chemical relatives with the same proposed lipolytic rationale, and the human-efficacy evidence for the unmodified fragment is, if anything, even thinner than for AOD-9604. Presenting them as fundamentally different mechanisms is inaccurate; the honest framing is that they are variants of the same idea, and neither has demonstrated clinically meaningful human fat loss.
The comparison to full-length human growth hormone is the one that defines AOD-9604’s identity. hGH is a proven, potent metabolic hormone with well-characterized effects on body composition, but it raises IGF-1, can promote tissue growth, and impairs glucose handling with chronic use. AOD-9604 was engineered specifically to shed those properties, and the animal data support that it does — no hGH-receptor binding, no IGF-1 elevation, no glucose intolerance.134 The trade-off, made explicit by the clinical failure, is that in shedding growth hormone’s liabilities the fragment also appears to have shed the reliable efficacy: hGH works and carries risk, whereas AOD-9604 is well tolerated but did not demonstrate the benefit.8
A comparison researchers increasingly ask about is to GLP-1 and GIP/GLP-1 receptor agonists such as semaglutide and tirzepatide. This comparison is stark and worth stating plainly: those agents have large, replicated, randomized phase III trials showing double-digit percentage weight loss and are approved regulatory-grade obesity medicines. AOD-9604 has a failed confirmatory obesity trial and no approval.8 They are not in the same evidentiary universe, and any content implying AOD-9604 is a comparable “fat-loss peptide” to the incretin agonists is deeply misleading about the level of evidence.
Finally, AOD-9604 is often combined with growth-hormone secretagogues such as CJC-1295 and Ipamorelin in blended research preparations — the site catalogs one such combination in its AOD-9604 + CJC-1295 + Ipamorelin blend dosage reference. The logic offered for such blends is that the secretagogues raise endogenous growth hormone pulses while AOD-9604 supplies an ostensibly fat-directed signal. It is worth being explicit that no controlled human trial has evaluated this specific combination for body composition; the pairing is a theoretical construct, not an evidence-based protocol, and combining agents also compounds the uncertainty around each of them. Broader context on how such combinations are catalogued for research purposes is available through the site’s peptide stacks reference and general dosages index.
| Compound | Relationship to AOD-9604 | Human efficacy evidence |
|---|---|---|
| HGH Fragment 176-191 | Unmodified parent fragment; same region | Very limited; no robust human fat-loss data |
| Full-length hGH | Source molecule AOD-9604 is derived from | Proven metabolic effects, but with IGF-1/glucose liabilities |
| Semaglutide / tirzepatide (GLP-1 class) | Unrelated mechanism (incretin) | Large phase III trials; approved obesity drugs |
| CJC-1295 / Ipamorelin (secretagogues) | Often blended with AOD-9604 in research prep | No controlled human trial of the combination for fat loss |
Research Models and Methodology
Because AOD-9604’s story is so dependent on the difference between animal and human results, it helps to understand the actual methods used to study it — both to appreciate what the positive findings mean and to see why they did not carry over to people.
The foundational in vitro and cellular work looked at adipocyte lipid metabolism: measuring lipolysis (release of glycerol and free fatty acids) and lipogenesis (incorporation of labeled substrate into stored lipid) in fat-cell preparations exposed to the peptide. These assays are the front line for a proposed lipolytic agent because they can isolate a direct effect on fat cells from whole-body confounders. They established that the synthetic domain had measurable activity on lipid handling in the dish.1
The in vivo rodent models were the workhorses of efficacy characterization. Two genetic obesity models featured prominently: obese mice and Zucker fatty rats, the latter a widely used model of genetic obesity and insulin resistance.24 Chronic dosing protocols (typically days to a few weeks) allowed researchers to measure changes in body-weight gain, fat oxidation, adipocyte size, and glucose parameters. The great methodological strength of this program was the use of the β3-adrenergic receptor knockout mouse as a mechanistic scalpel: by removing a single receptor and showing the effect disappeared, the researchers converted an association into pathway-level evidence, which is a genuinely rigorous design choice.3
There are, however, methodological limits baked into these models that directly explain the translational failure. Genetic-obesity rodents are not miniature humans with diet-related obesity; their physiology, receptor densities, and metabolic set points differ, and the β3-adrenergic pathway in particular is notoriously species-divergent — β3-agonists have a long history of impressive rodent thermogenic and lipolytic effects that shrink or vanish in humans. A mechanism that runs through the β3-AR is therefore a priori at elevated risk of failing to translate, which is a useful lens for interpreting AOD-9604’s trajectory. Short study durations, small group sizes, and supraphysiologic dosing relative to body size further widen the gap between the rodent signal and a human outcome.
On the human side, the methodology that matters is the trial design, and here the program was actually reasonably sound — which is part of why the negative result is credible. The obesity studies were randomized, double-blind, and placebo-controlled, the appropriate design for a weight-loss claim, and the confirmatory study was large enough (hundreds of participants over 24 weeks) to detect a clinically relevant effect if one existed.8 The fact that a well-designed, adequately powered trial returned a null result is not a methodological weakness to explain away; it is the strongest kind of evidence that the earlier small-study signal was not real or not reproducible at scale.
A methodological point specific to reading the literature: publication asymmetry. The positive early-phase and mechanistic findings are well represented in peer-reviewed journals, while the definitive negative confirmatory trial was disclosed largely through the company rather than a full primary publication.8 A researcher searching databases will therefore find disproportionately more “it works” than “it did not,” and must actively correct for that imbalance rather than mistaking the density of positive citations for weight of evidence. This is a textbook illustration of why counting supportive references is a poor substitute for weighing the single best-designed study.
Safety and Tolerability
Safety is the one domain where AOD-9604 arguably comes off well in the human data, and it deserves fair credit — with the constant caveat that “well tolerated” is not “effective,” and short-term tolerability is not long-term safety.
The most relevant human safety document is a published study of the safety and tolerability of the hexadecapeptide AOD-9604 in humans, which reported that the peptide was well tolerated across the doses studied, without evidence of the adverse metabolic effects that chronic growth hormone would raise — notably no signal of IGF-1 elevation or impaired glucose tolerance attributable to the compound.8 Across the obesity trials, reported side effects were generally mild and non-specific: headache, occasional mild edema, and fatigue were the kinds of events noted, consistent with a compound that did not produce dramatic physiological perturbation.8 The absence of IGF-1 elevation is mechanistically expected given that AOD-9604 does not engage the growth hormone receptor, and it is one of the more consistently reproduced findings in the whole dossier.13
On the strength of these data, a private (industry-sponsored) expert panel concluded AOD-9604 was “Generally Recognized As Safe” (GRAS) for use as a food ingredient at doses up to about 1 mg/day.6 This is genuinely part of the record and should be reported — but it must be framed accurately, because it is routinely misrepresented. A self-affirmed or panel-affirmed GRAS conclusion is a food-additive safety determination made by parties other than a regulator; it is not an FDA drug approval, it does not speak to efficacy at all, and it does not apply to injectable use for weight loss.6 Citing GRAS status to imply that AOD-9604 is an approved or validated fat-loss treatment is a category error.
The honest limits of the safety picture are as important as its strengths. First, the human safety data are short-term. The trials ran on the order of weeks to a few months; there is no long-term human safety database for AOD-9604, and nothing meaningful is known about effects over years of use.8 Second, safety was characterized under controlled trial conditions with pharmaceutical-grade material at defined doses — conditions that do not describe unregulated research-chemical products, where identity, purity, sterility, and actual peptide content can vary widely and introduce risks entirely separate from the molecule’s own pharmacology. Third, “no signal” in modestly sized trials is not the same as “no risk”; rare adverse events and interactions can only be excluded by large, long exposures that AOD-9604 never accumulated because development stopped.
There is also a sport-integrity dimension worth flagging for completeness: AOD-9604 is prohibited in sport by the World Anti-Doping Agency and is tested for in competition, so its presence in an athlete’s sample can trigger an anti-doping violation regardless of the efficacy debate.9 That is a regulatory and eligibility fact, not a safety claim, but it is part of responsibly understanding the compound. The overall safety verdict: reassuring but shallow — a clean short-term tolerability signal that says nothing about efficacy and cannot substitute for long-term data or for the quality controls of a regulated product.
Handling and Reconstitution in a Research Context
Because AOD-9604 is encountered almost entirely as a lyophilized (freeze-dried) research peptide rather than a finished pharmaceutical, handling questions arise in laboratory settings. This section describes general peptide-handling practice for context only; it is not clinical guidance, and nothing here should be read as instruction for human use, which is neither approved nor supported by the evidence.
Lyophilized peptides are typically supplied as a small amount of white powder in a sealed vial and are reconstituted with a sterile diluent before any laboratory use. Bacteriostatic water (water containing a low concentration of benzyl alcohol, which suppresses microbial growth) is the diluent most commonly referenced for multi-use research vials, while plain sterile water is sometimes used for single-use contexts. Reconstitution is generally done by directing the diluent slowly down the inner wall of the vial rather than injecting it forcefully onto the powder, because peptides can be sensitive to shear and foaming; the vial is then left to dissolve, with gentle swirling rather than vigorous shaking.1
The relationship between the amount of diluent added and the resulting concentration is simple arithmetic, and it is the part researchers most often get wrong. The concentration equals the peptide mass in the vial divided by the volume of diluent added. The table below illustrates this for the common AOD-9604 vial sizes; note it describes concentration math only and implies nothing about an appropriate human dose, of which there is none established.
| Vial content | Diluent added | Resulting concentration | Volume containing 300 mcg |
|---|---|---|---|
| 2 mg | 2.0 mL | 1.0 mg/mL (1000 mcg/mL) | 0.30 mL |
| 2 mg | 1.0 mL | 2.0 mg/mL (2000 mcg/mL) | 0.15 mL |
| 5 mg | 2.5 mL | 2.0 mg/mL (2000 mcg/mL) | 0.15 mL |
| 5 mg | 5.0 mL | 1.0 mg/mL (1000 mcg/mL) | 0.30 mL |
Stability and storage are the other practical considerations. As a dry powder, AOD-9604 is generally stored frozen or refrigerated and protected from light and moisture; once reconstituted, aqueous peptide solutions are far less stable and are typically kept refrigerated and used within a limited window, because hydrolysis and other degradation pathways accelerate in solution. The internal disulfide bond and the general fragility of small peptides mean that repeated freeze-thaw cycles, heat, and vigorous agitation are all avoided in careful handling.1 Site references such as the AOD-9604 (5mg vial) dosage protocol and the AOD-9604 (2mg vial) protocol present this kind of reconstitution and concentration math in a structured research-reference format.
One overriding caveat must accompany any handling discussion: a compound obtained as an unregulated research chemical carries no guarantee of identity, purity, sterility, or actual peptide content. The clean safety signal discussed earlier was generated with pharmaceutical-grade material under trial conditions; it does not transfer to research-chemical products of unknown provenance. Handling technique cannot compensate for an unverified starting material, and the risks introduced by contamination or misidentification are entirely separate from — and can dwarf — the intrinsic pharmacology of the peptide itself.
Limitations and the Human-Evidence Gap
Pulling the threads together, the defining feature of AOD-9604 is a wide and well-documented gap between mechanistic plausibility and demonstrated human benefit. Being explicit about the specific limitations is the most useful thing a research-education resource can do, because it inoculates the reader against the confident overstatement that dominates commercial coverage.
The first and largest limitation is the failed confirmatory trial. The pivotal, adequately powered, randomized, placebo-controlled obesity study did not show statistically significant weight loss versus placebo, and development was terminated.8 This is not a minor gap or a matter of “more research needed” around a positive core; it is a direct negative result on the exact question — human fat loss — that the compound is marketed for. Every downstream claim inherits this failure.
The second limitation is translational risk baked into the mechanism. The lipolytic effect in animals depended on the β3-adrenergic receptor, a pathway with a well-earned reputation for producing striking rodent effects that fail to reproduce in humans.3 A mechanism running through β3-AR is exactly the kind that should have prompted caution about translation, and the clinical outcome is consistent with that caution.
The third limitation is publication asymmetry and citation inflation. The positive early and mechanistic data are more visible in the literature than the definitive negative trial, which was largely company-disclosed.8 This makes it easy to assemble an impressive-looking list of supportive citations while omitting the one study that actually answers the efficacy question. Readers should weigh the single best-designed study more heavily than the count of favorable references — an approach that reverses the impression most commercial write-ups cultivate.
The fourth limitation concerns the specific “lean-mass sparing” claim. It is mechanistically reasonable but clinically unsubstantiated, because a favorable fat-versus-lean partition is only meaningful in the presence of real fat loss, which was not established.8 The claim rests on rodent body-composition data and mechanistic inference, not on a demonstrated human body-composition benefit.
The fifth limitation is the absence of long-term human data of any kind — efficacy or safety. Because development stopped in 2007, there is no extended human experience with AOD-9604, no long-term safety database, and no evidence about durability of any effect.8 The “well tolerated” conclusion is bounded by weeks-to-months of exposure.
Finally, there is the product-quality gap: the human data were generated with controlled pharmaceutical material, whereas real-world availability is dominated by unregulated research chemicals of uncertain identity and purity, so even the modest, honestly-characterized findings may not describe what an individual actually obtains. Taken together, these limitations do not make AOD-9604 a scientific dead end worth ignoring, but they do make it categorically wrong to describe it as a “clinically backed” fat-loss agent. The accurate description is a mechanistically interesting, well-tolerated, human-unproven research peptide.
Regulatory Status
The regulatory picture for AOD-9604 is unambiguous and directly contradicts any impression that it is an accepted therapy. It is not an approved drug in any major jurisdiction. The U.S. Food and Drug Administration has not approved AOD-9604 for weight loss or for any other indication, and no equivalent approval exists from other major regulators.68 Its pharmaceutical development for obesity ended in 2007 after the confirmatory trial failure, so it never advanced to an approval application on efficacy grounds.8
The most commonly misrepresented regulatory element is the GRAS (“Generally Recognized As Safe”) designation. A privately convened expert panel concluded that AOD-9604 could be considered GRAS as a food ingredient at doses up to roughly 1 mg/day.6 It is essential to understand what this is and is not. GRAS is a food-safety pathway; a self-determined or panel-affirmed GRAS conclusion is reached by industry-selected experts rather than granted by the FDA as a drug approval, it addresses ingestion safety rather than therapeutic efficacy, and it explicitly does not authorize injectable drug use or make any efficacy claim.6 Marketing that leans on “GRAS status” to suggest regulatory endorsement of a fat-loss treatment is misusing the term.
In the compounding arena, AOD-9604 has been the subject of FDA review of substances nominated for use in pharmacy compounding. The trajectory here reflects regulatory caution rather than acceptance: peptides of this type have faced FDA scrutiny over their suitability and safety for compounding, and AOD-9604 has not emerged as an approved compounding substance available for lawful clinical use.6 The practical upshot is that legitimate, regulator-sanctioned clinical access to AOD-9604 does not exist in the way it does for approved obesity medicines.
In sport, the regulatory status is clear and consequential: AOD-9604 is included on the World Anti-Doping Agency Prohibited List and is tested for, including in competition.9 An athlete subject to anti-doping rules who uses AOD-9604 risks an anti-doping rule violation irrespective of whether the compound “works,” and this prohibition has been in place despite — not because of — its limited demonstrated efficacy.
Putting the regulatory facts alongside the efficacy record produces a coherent and cautionary picture. A compound that failed its pivotal human trial, was discontinued by its developer, holds only a food-ingredient safety opinion rather than drug approval, is not an accepted compounding substance, and is banned in sport, is by any reasonable standard an experimental research compound — not a validated therapeutic. That is the frame every reader should retain: AOD-9604 is legitimate to study and discuss, but it is neither approved nor clinically proven, and it must never be represented as a treatment for obesity or any disease.
Frequently Asked Questions
Does AOD-9604 actually cause fat loss in humans?
Not in the sense the marketing implies. A small early-phase trial suggested a modest weight difference versus placebo, but the larger, adequately powered, randomized, placebo-controlled confirmatory trial did not show statistically significant weight loss over placebo, and development was terminated in 2007.8 The honest summary is that human fat-loss efficacy was not demonstrated. AOD-9604 should be regarded as a research compound with an unproven effect, not a clinically backed fat-loss agent.
Is AOD-9604 FDA-approved?
No. The FDA has not approved AOD-9604 for weight loss or any other use.68 A private expert panel issued a food-ingredient GRAS (“Generally Recognized As Safe”) opinion at low oral doses, but that is a food-safety determination — not a drug approval, and it makes no efficacy claim and does not authorize injectable use.6
Why does it supposedly spare lean muscle?
The rationale is mechanistic: AOD-9604 is proposed to act on fat cells through a β3-adrenergic-dependent lipolytic pathway without raising IGF-1 or engaging the growth hormone receptor, which would in theory direct its action toward fat rather than muscle.13 But “lean-mass sparing” is only a meaningful clinical claim if there is real fat loss to begin with, and the pivotal human trial did not establish significant fat loss.8 So the muscle-sparing claim rests on animal data and inference, not on demonstrated human body-composition benefit.
How is AOD-9604 different from HGH Fragment 176-191?
They are close chemical relatives, not fundamentally different mechanisms. AOD-9604 is essentially a stabilized, tyrosine-modified version of the same 176-191 region of growth hormone.1 Both share the identical lipolytic rationale, and neither has demonstrated clinically meaningful human fat loss. Content presenting them as unrelated or as one being clearly superior in humans is overstating what the evidence supports.
Is AOD-9604 the same kind of thing as semaglutide or tirzepatide?
No, and the comparison is misleading. GLP-1 and GIP/GLP-1 agonists like semaglutide and tirzepatide have large, replicated phase III trials showing substantial weight loss and are approved obesity medicines. AOD-9604 has a failed confirmatory obesity trial and no approval.8 They are not comparable in mechanism or, more importantly, in level of evidence.
Is AOD-9604 safe?
Short-term human data suggest it was well tolerated at the doses studied, with mostly mild, non-specific side effects and no signal of IGF-1 elevation or glucose intolerance.8 However, those data are short-term and were generated with pharmaceutical-grade material under trial conditions. There is no long-term human safety database, and unregulated research-chemical products carry additional risks of impurity, contamination, or misidentification that are separate from the molecule itself. “Well tolerated short-term” is not the same as “proven safe long-term,” and it says nothing about efficacy.
Is AOD-9604 banned in sport?
Yes. AOD-9604 is on the World Anti-Doping Agency Prohibited List and is tested for, including in competition, so its use can result in an anti-doping rule violation for athletes subject to those rules — independent of the efficacy question.9
Why was development stopped if it looked promising early?
This is a textbook example of why confirmatory trials exist. A small early study can produce an encouraging but ultimately spurious or non-reproducible signal; the larger, better-designed trial is run precisely to test whether that signal is real. For AOD-9604 the larger trial did not confirm the benefit, so the responsible interpretation is that the early signal did not hold up, and the developer discontinued the program in 2007.8
References
- Ng FM, Sun J, Sharma L, Libinaka R, Jiang WJ, Gianello R. Metabolic studies of a synthetic lipolytic domain (AOD9604) of human growth hormone. Horm Res. 2000;53(6):274-278. doi:10.1159/000053183.
- Heffernan MA, Thorburn AW, Fam B, et al. Increase of fat oxidation and weight loss in obese mice caused by chronic treatment with human growth hormone or a modified C-terminal fragment. Int J Obes Relat Metab Disord. 2001;25(10):1442-1449. PMID: 11673763.
- Heffernan M, Summers RJ, Thorburn A, et al. The effects of human GH and its lipolytic fragment (AOD9604) on lipid metabolism following chronic treatment in obese mice and beta3-AR knock-out mice. Endocrinology. 2001;142(12):5182-5189. doi:10.1210/endo.142.12.8522.
- Ng FM, Jiang WJ, Gianello R, et al. Molecular and cellular actions of a structural domain of human growth hormone (AOD9401) on lipid metabolism in Zucker fatty rats. J Mol Endocrinol. 2000;25(3):287-298. PMID: 11116208.
- Heffernan MA, Jiang WJ, Thorburn AW, Ng FM. Effects of oral administration of a synthetic fragment of human growth hormone on lipid metabolism. Am J Physiol Endocrinol Metab. 2000;279(3):E501-E507. doi:10.1152/ajpendo.2000.279.3.E501.
- Moré MI, Freitas U, Rutenberg D. Safety and metabolism of AOD9604, a novel nutraceutical ingredient for improved metabolic health. J Endocrinol Metab. 2014;4(3):64-77. doi:10.14740/jem213w. (Industry-sponsored safety/GRAS assessment; food-ingredient scope, not a drug-approval document.)
- Kwon DR, Park GY. Effect of intra-articular injection of AOD9604 with or without hyaluronic acid in a rabbit osteoarthritis model. Ann Clin Lab Sci. 2015;45(4):426-432.
- Stier H, Vos E, Kenley D. Safety and tolerability of the hexadecapeptide AOD9604 in humans. J Endocrinol Metab. 2013;3(1-2):7-15. (Human tolerability data; also summarizes the obesity clinical program outcome and 2007 discontinuation.)
- World Anti-Doping Agency. The Prohibited List (AOD-9604 listed as a prohibited substance/growth-hormone fragment). World Anti-Doping Agency; current edition.
Educational and research-only disclaimer: This article is provided strictly for scientific education and research-context reference. It is not medical advice, and nothing in it should be read as a recommendation to obtain, administer, or use AOD-9604 in humans. AOD-9604 is not approved by the FDA or other major regulators for any indication, it did not demonstrate significant fat loss versus placebo in its pivotal human trial, and its development was discontinued in 2007. It does not treat, cure, or prevent any disease, and any body-composition or “fat-loss” benefit in humans remains unproven. Handling and concentration information is included only to describe general laboratory practice and does not constitute dosing guidance for human use. Anyone considering questions about weight, metabolism, or health should consult a qualified, licensed healthcare professional and rely on approved, evidence-based options.