Few molecules in modern metabolic medicine have been studied as intensively, or as publicly, as semaglutide. Approved by the U.S. Food and Drug Administration as Ozempic for type 2 diabetes in 2017 and as Wegovy for chronic weight management in 2021, semaglutide is a glucagon-like peptide-1 (GLP-1) receptor agonist whose clinical development produced one of the largest and most consistent bodies of randomized evidence in the history of obesity pharmacotherapy.1 For an educational audience trying to understand how a drug earns the label “long-term obesity treatment,” semaglutide is an unusually instructive case study: its trial program was explicitly designed to answer that question over 68 to 104 weeks, with pre-specified endpoints, withdrawal designs, and a dedicated cardiovascular outcomes study.
This article examines the question in the title directly: what did the semaglutide trials actually demonstrate about its role in long-term obesity management, and how confident should a careful reader be in each claim? The short answer is that the evidence is genuinely strong and comes from large, well-controlled, peer-reviewed phase 3 trials, but that “strong” is not the same as “unlimited.” The trials show durable weight reduction while treatment continues, meaningful improvements in cardiometabolic risk factors, and a reduction in major cardiovascular events in a high-risk population, alongside a consistent gastrointestinal side-effect profile and rapid weight regain after discontinuation.1,3,5,6
Throughout, the aim is to be measured. Semaglutide is a legitimately approved medicine, not a fringe “bioregulator” with thin evidence; the challenge here is the opposite of hype-checking an obscure compound. The task is to represent a large evidence base accurately, distinguish what the trials proved from what they did not, and keep every number anchored to a primary source. This is an educational overview for people who study peptide science and read the clinical literature. It is not medical advice, a treatment protocol, or a recommendation to obtain or self-administer any substance.
What Semaglutide Is and Where It Came From
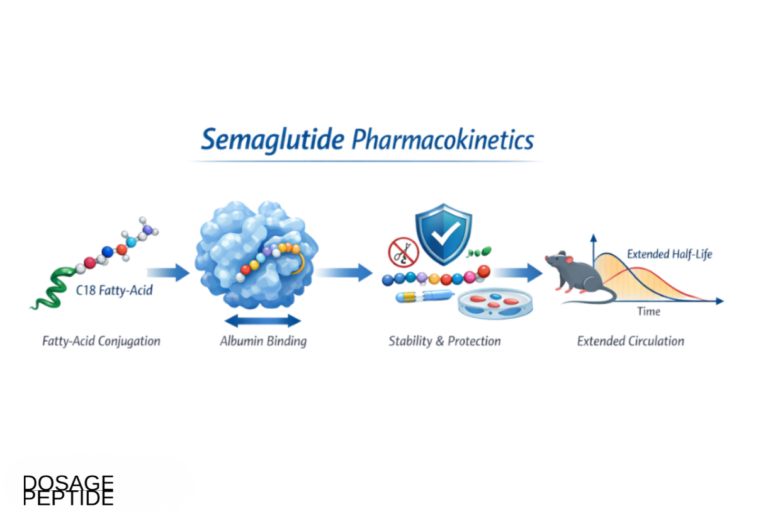
Semaglutide is a synthetic analogue of human glucagon-like peptide-1, an incretin hormone released by intestinal L-cells after eating. Native GLP-1 has two problems as a drug: it is degraded within roughly one to two minutes by the enzyme dipeptidyl peptidase-4 (DPP-4), and it is cleared quickly by the kidneys.12 Any therapeutic GLP-1 receptor agonist therefore has to solve the half-life problem. Semaglutide does so through three deliberate structural modifications to the native peptide backbone: substitution of the position-8 alanine with 2-aminoisobutyric acid (Aib) to block DPP-4 cleavage, a lysine substitution at position 34, and, most importantly, attachment of a C18 fatty di-acid chain via a short linker at position 26.12
That fatty-acid “acylation” allows semaglutide to bind reversibly and tightly to circulating albumin. Because albumin is abundant and long-lived in plasma, the bound drug is protected from enzymatic degradation and renal filtration, and it is released slowly. The net result is a terminal half-life of approximately one week, which is what makes once-weekly subcutaneous dosing feasible.12 This is the same molecular logic used in the earlier, shorter-acting analogue liraglutide (once-daily), refined to extend the dosing interval sevenfold. Understanding this design detail matters because it explains several downstream clinical realities: the slow titration schedule, the delayed onset of full effect, and the persistence of drug in the body for weeks after the last dose.
Semaglutide was developed by Novo Nordisk and first reached the market as a diabetes therapy. The subcutaneous formulation was approved by the FDA as Ozempic (up to 1.0 mg, later 2.0 mg, once weekly) for glycemic control in type 2 diabetes in December 2017, and an oral formulation (Rybelsus) followed in 2019.9 The pivotal insight for obesity was that the appetite-suppressing effects observed in diabetes trials scaled with dose. This prompted a dedicated development program at a higher dose, 2.4 mg once weekly, marketed as Wegovy and approved specifically for chronic weight management in June 2021.9 The 2.4 mg dose is the version that anchors essentially all of the long-term obesity evidence discussed below; when this article refers to the “obesity dose,” it means semaglutide 2.4 mg once weekly.
It is worth being precise about terminology. Semaglutide is a peptide drug, but it is not one of the loosely evidenced “bioregulator” or “research peptide” compounds that circulate in unregulated markets with minimal human data. It is a fully characterized, patent-protected, pharmacopoeia-grade active pharmaceutical ingredient with a defined molecular formula (C187H291N45O59) and a mature regulatory dossier. That distinction is important for any reader accustomed to the caveat “rigorous independent evidence is scarce”: for semaglutide, the opposite is true, and the analytical job is to weigh a large, high-quality evidence base rather than to compensate for its absence. Readers who want the compound-specific handling details can consult the site’s semaglutide 10 mg vial reference page for the physicochemical and reconstitution specifics discussed later in this article.
Molecular Mechanism: How Semaglutide Acts on GLP-1 Biology
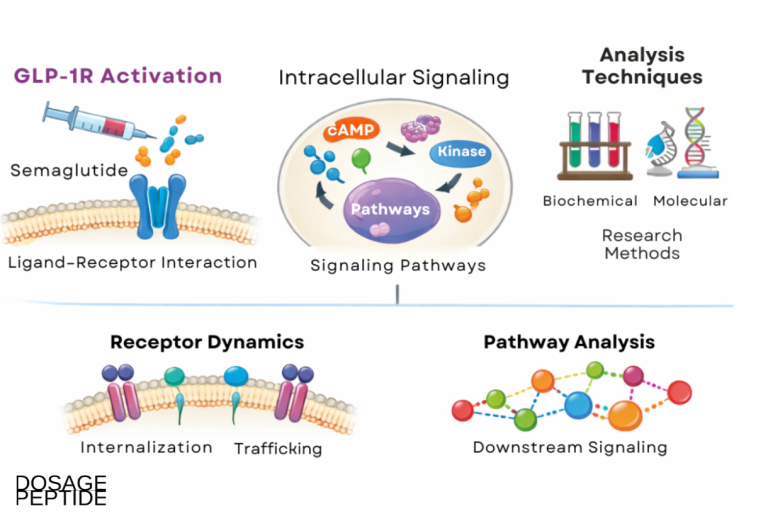
The GLP-1 receptor is a class B G-protein-coupled receptor expressed in the pancreas, gastrointestinal tract, heart, kidney, and, critically for weight regulation, the central nervous system. When semaglutide binds and activates this receptor, it triggers Gs-protein coupling, adenylate cyclase activation, and a rise in intracellular cyclic AMP, which sets off the cascade of downstream effects.11 For metabolic and weight outcomes, four of these effects matter most.
First, semaglutide enhances glucose-dependent insulin secretion from pancreatic beta cells. The “glucose-dependent” qualifier is important: insulin release is amplified only when blood glucose is elevated, which is why GLP-1 receptor agonists carry a relatively low intrinsic risk of hypoglycemia compared with insulin or sulfonylureas. Second, it suppresses glucagon secretion from pancreatic alpha cells under hyperglycemic conditions, reducing hepatic glucose output. These two pancreatic actions underlie semaglutide’s glucose-lowering efficacy in type 2 diabetes and explain why the diabetes and obesity programs are biologically linked.11
Third, semaglutide slows gastric emptying, particularly early in treatment. Delayed gastric emptying increases the sensation of fullness after meals and blunts post-prandial glucose spikes. This effect appears to attenuate somewhat over time (a phenomenon called tachyphylaxis), but it contributes to both the early satiety patients report and, plausibly, to the gastrointestinal side effects that dominate the tolerability profile.11
Fourth, and most central to the obesity indication, semaglutide acts on appetite-regulating circuits in the brain. GLP-1 receptors are expressed in the hypothalamic arcuate nucleus and in the brainstem. Preclinical and mechanistic work indicates that semaglutide stimulates anorexigenic pro-opiomelanocortin/cocaine- and amphetamine-regulated transcript (POMC/CART) neurons while inhibiting orexigenic neuropeptide Y/agouti-related peptide (NPY/AgRP) neurons.11 The functional consequence, documented in controlled feeding studies, is reduced hunger, reduced food cravings, altered food preference, and lower overall energy intake. Because the molecule is large and does not freely cross the blood-brain barrier everywhere, much of this central action is thought to occur at circumventricular organs and other regions with a permeable barrier, from which signals propagate to deeper appetite centers.
Mechanistically, then, semaglutide produces weight loss primarily by reducing caloric intake rather than by substantially increasing energy expenditure. This is a meaningful distinction. It means the drug works “downstream” of the willpower narrative that has historically framed obesity: it changes the biological hunger signal itself. It also frames a limitation that recurs throughout the trial data. Because the effect depends on continuous receptor activation, appetite and body weight tend to return toward baseline once drug exposure falls, a point the withdrawal trials make with uncomfortable clarity.3,5 The table below summarizes the principal mechanistic actions and where each is thought to be clinically relevant.
| Action | Site | Primary clinical relevance |
|---|---|---|
| Glucose-dependent insulin secretion | Pancreatic beta cells | Glycemic control; low hypoglycemia risk |
| Glucagon suppression | Pancreatic alpha cells | Reduced hepatic glucose output |
| Delayed gastric emptying | Stomach / GI tract | Early satiety; post-prandial glucose; GI side effects |
| Appetite suppression | Hypothalamus, brainstem | Reduced energy intake; weight loss |
The STEP Program: What the Pivotal Weight-Management Trials Showed
The evidence that semaglutide works as a long-term obesity treatment comes primarily from the Semaglutide Treatment Effect in People with obesity (STEP) program, a coordinated series of phase 3 randomized, double-blind, placebo-controlled trials. Each STEP trial addressed a different population or question, but they shared a common backbone: semaglutide 2.4 mg once weekly (titrated over 16 weeks) versus placebo, both combined with lifestyle counseling, over 68 weeks in most cases.
STEP 1, published by Wilding and colleagues in the New England Journal of Medicine in 2021, is the anchor trial. It enrolled 1,961 adults with a body mass index (BMI) of at least 30, or at least 27 with a weight-related comorbidity, and without diabetes. Over 68 weeks, participants assigned to semaglutide lost a mean of −14.9% of body weight versus −2.4% for placebo, an estimated treatment difference of roughly 12.4 percentage points.1 The proportion achieving at least 5% weight loss, a standard regulatory threshold for clinically meaningful response, was 86.4% on semaglutide versus 31.5% on placebo. Notably, 69.1% reached at least 10% and 50.5% reached at least 15%, categories rarely achieved with previous anti-obesity drugs.1
STEP 2, reported by Davies and colleagues in The Lancet, extended the question to the harder population of adults who also have type 2 diabetes, a group that typically loses less weight on any intervention. Among 1,210 participants, semaglutide 2.4 mg produced a mean weight change of approximately −9.6% versus −3.4% for placebo at 68 weeks, with a superior effect over the lower 1.0 mg diabetes dose as well.2 The smaller absolute effect in diabetes is a consistent and important finding: it demonstrates that the drug’s benefit is real across populations but is genuinely blunted by coexisting type 2 diabetes.
STEP 5, reported by Garvey and colleagues in Nature Medicine, is arguably the single most important trial for the “long-term” question because it ran for 104 weeks (two years). The mean weight change from baseline to week 104 was −15.2% with semaglutide versus −2.6% with placebo, an estimated difference of −12.6 percentage points, and 77.1% of the semaglutide group achieved at least 5% loss versus 34.4% on placebo.4 Crucially, the weight-loss curve plateaued rather than reversing, indicating that on continued treatment the effect is durable across two years rather than being a transient first-year phenomenon.
The STEP program also reached into adolescents. STEP TEENS (Weghuber and colleagues, NEJM 2022) studied adolescents aged 12 to 17 with obesity and reported a mean BMI reduction of about 16.1% with semaglutide versus a 0.6% increase with placebo, supporting a pediatric indication.10 Taken together, the STEP results are strikingly consistent: across adults without diabetes, adults with diabetes, a two-year horizon, and adolescents, semaglutide 2.4 mg reliably produces double-digit percentage weight loss that is several fold greater than placebo plus lifestyle intervention. The table below assembles the headline figures.
| Trial | Population | Duration | Mean weight change (sema vs placebo) |
|---|---|---|---|
| STEP 11 | Adults, no diabetes | 68 wk | −14.9% vs −2.4% |
| STEP 22 | Adults with type 2 diabetes | 68 wk | ≈−9.6% vs −3.4% |
| STEP 43 | Adults, maintenance design | 68 wk | −17.4% (continued) vs regain on switch |
| STEP 54 | Adults, no diabetes | 104 wk | −15.2% vs −2.6% |
| STEP TEENS10 | Adolescents 12–17 | 68 wk | −16.1% BMI vs +0.6% BMI |
One honest caveat applies to all of these: the trials combined semaglutide with structured lifestyle counseling, and the placebo groups received the same counseling. The reported treatment differences therefore represent the drug effect on top of lifestyle support, which is the correct comparison, but it also means these numbers describe a supervised trial context rather than unmonitored real-world use, where adherence and titration are less controlled.
Long-Term Maintenance and Weight Regain: STEP 4 and the STEP 1 Extension
A drug can produce large short-term weight loss and still fail the “long-term treatment” test if the benefit evaporates. Two studies were designed specifically to interrogate durability and dependence on continued dosing, and their results are among the most clinically consequential in the entire program.
STEP 4 (Rubino and colleagues, JAMA 2021) used a randomized withdrawal design. All participants first took semaglutide during a 20-week run-in and titrated to 2.4 mg, losing on average about 10.6% of body weight. At week 20, they were randomized either to continue semaglutide or to switch to placebo, with follow-up to week 68. The contrast was stark. Those who continued semaglutide lost an additional increment of weight, reaching an estimated total reduction of −17.4% from the original baseline, whereas those switched to placebo regained weight steadily, ending roughly 5% above their week-20 nadir (a net change of about +6.9% from randomization).3 Cardiometabolic improvements, including blood pressure and lipids, similarly reversed toward baseline in the placebo-switch group.
The STEP 1 trial extension (Wilding and colleagues, Diabetes, Obesity and Metabolism 2022) reinforced the same message from a different angle. It followed participants for one year after all treatment (both semaglutide and placebo) was stopped at week 68. On average, participants who had been on semaglutide regained about two-thirds of their lost weight within that year, and cardiometabolic variables that had improved during treatment likewise drifted back toward pre-treatment values.5
The interpretation is unambiguous and worth stating plainly: semaglutide’s benefit is contingent on continued administration. This is not a flaw unique to semaglutide; it mirrors the behavior of medications for hypertension, dyslipidemia, and diabetes, none of which are expected to work after they are stopped. The scientific framing that emerged from these trials is that obesity is a chronic, relapsing condition and that pharmacotherapy manages it rather than curing it. That framing is central to how the field now interprets “long-term obesity treatment,” and it is a direct product of the STEP 4 and extension data rather than an assumption imposed on them.3,5
For an educational reader, the practical takeaway is conceptual rather than prescriptive. The withdrawal data mean that any claim that semaglutide “cures” obesity is unsupported; the drug demonstrably manages a physiological drive that reasserts itself once receptor activation ends. It also means that trial results describing 15% to 17% weight loss should be mentally paired with the phrase “while treatment continues.” The durability shown in STEP 5 out to two years is genuine, but it is durability on drug, not durability after stopping. This distinction is the single most important nuance in the entire body of evidence, and it is one the trials were carefully designed to expose rather than to obscure.
It also raises questions that the pivotal trials did not fully answer. How much of the regained weight can be prevented with lower maintenance doses, intermittent dosing, or intensified lifestyle support after discontinuation? What is the optimal long-term strategy for someone who cannot tolerate or afford indefinite treatment? These remain active research questions, and the honest position is that the maintenance strategy beyond continuous full-dose therapy is not yet settled by high-quality evidence.
Beyond Weight: The SELECT Cardiovascular Outcomes Trial
Weight loss is a surrogate. What clinicians and regulators ultimately want to know is whether it translates into fewer hard clinical events. The Semaglutide Effects on Cardiovascular Outcomes in People with Overweight or Obesity (SELECT) trial, reported by Lincoff and colleagues in the New England Journal of Medicine in 2023, was designed to answer exactly that question and is the most important non-weight trial in the semaglutide obesity literature.6
SELECT was large and long: 17,604 adults aged 45 or older with overweight or obesity (BMI at least 27) and established cardiovascular disease, but without diabetes, randomized to semaglutide 2.4 mg once weekly or placebo and followed for a mean of about 40 months. The primary composite endpoint of major adverse cardiovascular events (MACE), defined as cardiovascular death, non-fatal myocardial infarction, or non-fatal stroke, occurred in 6.5% of the semaglutide group versus 8.0% of the placebo group, a 20% relative risk reduction (hazard ratio 0.80, 95% confidence interval 0.72–0.90).6 This was a statistically robust result in a population selected for high baseline risk.
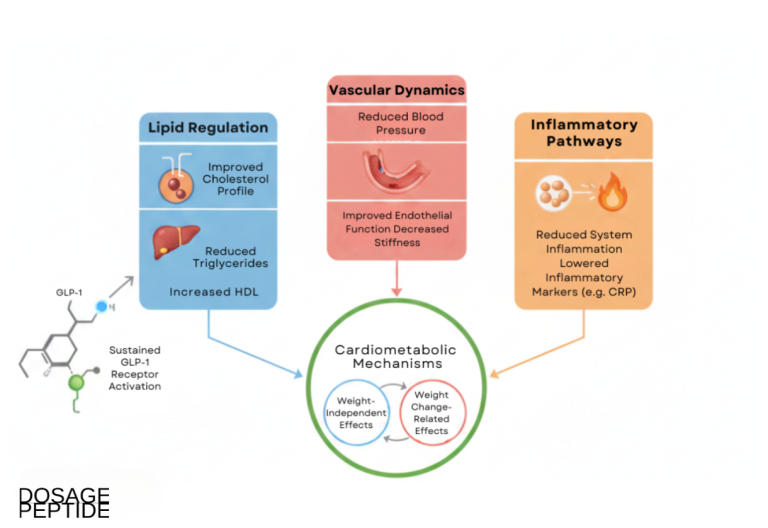
Several features of SELECT deserve careful, non-inflated interpretation. First, the trial enrolled a secondary-prevention population, meaning everyone already had cardiovascular disease; the 20% relative reduction therefore applies to high-risk patients and should not be extrapolated to healthy individuals with a lower baseline event rate, in whom the absolute benefit would be smaller. Second, the mechanism of benefit is not fully attributable to weight loss alone. A pre-specified analysis found that an estimated one-third of the MACE benefit was statistically mediated by reduction in waist circumference, implying that roughly two-thirds operated through other or unmeasured pathways such as improvements in blood pressure, inflammation, lipids, or direct vascular effects.6 The drug’s cardiovascular value, in other words, is real but mechanistically incompletely explained.
SELECT was the direct basis for the FDA’s March 2024 label expansion, which added an indication for reducing the risk of cardiovascular death, non-fatal myocardial infarction, and non-fatal stroke in adults with established cardiovascular disease and either obesity or overweight.9 That regulatory milestone is significant because it marked one of the first times an anti-obesity medication demonstrated a hard cardiovascular outcome benefit in a dedicated trial, moving the conversation beyond weight and cardiometabolic surrogates to clinical event reduction.
Still, the appropriate stance is measured. SELECT does not show that semaglutide prevents heart attacks in the general population, that it should be used purely for cardiovascular protection independent of weight, or that its benefit is entirely explained by any single pathway. It shows that in a specific, high-risk, non-diabetic population with overweight or obesity and existing cardiovascular disease, adding semaglutide over roughly three years reduced the composite of cardiovascular death, myocardial infarction, and stroke by a fifth on a relative basis, with a smaller absolute-risk difference of about 1.5 percentage points.6 That is a genuine and important finding, and it is also a bounded one. Subsequent secondary analyses have explored kidney outcomes, heart-failure subgroups, and adiposity measures, extending the picture without overturning the core result.
How Semaglutide Compares With Related Compounds
Semaglutide does not exist in isolation. It sits within a rapidly expanding class of incretin-based therapies, and understanding its place requires comparing it to both its predecessors and its newer competitors. These comparisons are educational context, not endorsements of any product.
Versus liraglutide. Liraglutide (Saxenda at 3.0 mg for obesity) is the earlier, shorter-acting GLP-1 receptor agonist requiring daily injection. In the head-to-head STEP 8 trial, once-weekly semaglutide 2.4 mg produced substantially greater weight loss than daily liraglutide 3.0 mg, roughly 15.8% versus 6.4% over 68 weeks.13 The comparison illustrates how the longer half-life, higher dose ceiling, and once-weekly convenience of semaglutide translated into a clinically meaningful efficacy advantage within the same drug class.
Versus tirzepatide. The most clinically relevant comparison today is with tirzepatide (Mounjaro/Zepbound), a “twincretin” that activates both the GLP-1 receptor and the glucose-dependent insulinotropic polypeptide (GIP) receptor. The head-to-head SURMOUNT-5 trial (Aronne and colleagues, NEJM 2025) randomized 751 adults with obesity but without diabetes to tirzepatide or semaglutide 2.4 mg for 72 weeks. Tirzepatide produced greater mean weight loss, approximately −20.2% versus −13.7%, and a higher proportion of participants reached the deepest weight-loss categories.8 Both drugs shared the same predominantly gastrointestinal side-effect profile. The honest summary is that current head-to-head evidence favors tirzepatide for magnitude of weight loss, while semaglutide retains the larger and longer cardiovascular outcomes dataset from SELECT.
Versus combination and next-generation agents. The field is moving quickly toward multi-receptor and combination approaches. Cagrilintide, a long-acting amylin analogue, has been co-formulated with semaglutide (the investigational combination often called CagriSema) with the aim of amplifying weight loss beyond either agent alone. Triple agonists such as retatrutide (targeting GLP-1, GIP, and glucagon receptors) are in advanced trials and have reported still-larger weight reductions in phase 2 data, though with less mature long-term and outcome evidence. Educational reference pages for several of these related molecules exist on this site, including tirzepatide, cagrilintide, the cagrilintide-semaglutide blend, and retatrutide.
The comparative landscape is summarized below. The central lesson is that semaglutide is best understood not as the endpoint of obesity pharmacology but as the molecule that proved the category, established the trial templates, and generated the first hard-outcome data, even as newer agents post larger weight-loss numbers.
| Compound | Target(s) | Dosing | Representative weight loss | Evidence maturity |
|---|---|---|---|---|
| Liraglutide 3.0 mg | GLP-1 | Daily | ≈6–8% | Approved; mature |
| Semaglutide 2.4 mg | GLP-1 | Weekly | ≈15% | Approved; very mature + CV outcomes |
| Tirzepatide | GLP-1 + GIP | Weekly | ≈20% | Approved; maturing |
| Retatrutide | GLP-1 + GIP + glucagon | Weekly | ≈24% (phase 2) | Investigational |
Research Models and Trial Methodology
Part of what makes the semaglutide evidence persuasive is not just the results but the rigor of the methods that produced them. For readers who evaluate evidence quality rather than just headline numbers, the design features of the STEP and SELECT programs are worth examining directly.
The pivotal trials were randomized, double-blind, and placebo-controlled, the strongest design for causal inference in clinical research. Randomization balances known and unknown confounders across groups; blinding of both participants and investigators guards against expectation effects, which are substantial in weight-loss research where behavior is easily influenced by knowledge of treatment assignment. Several trials, notably STEP 2, used a double-dummy design so that participants receiving different injection schedules could not infer their assignment from the injection pattern.2
The trials also used pre-specified co-primary endpoints, typically the percentage change in body weight and the proportion achieving at least 5% loss, defined before the data were unblinded. Pre-specification matters because it prevents the selective reporting of whichever outcome happened to look best. Statistical analysis relied on estimands, a framework that explicitly defines how to handle events such as treatment discontinuation and rescue medication. The STEP program reported both a “treatment policy” estimand (the effect regardless of adherence, closer to real-world conditions) and a “trial product” estimand (the effect if treatment is taken as intended). Reporting both is a mark of methodological care, and the two can differ meaningfully, with the treatment-policy estimate generally more conservative.
Sample sizes were large and adequately powered. STEP 1 enrolled nearly 2,000 participants; SELECT enrolled more than 17,000 and accrued events over roughly three years.1,6 Large samples narrow confidence intervals and allow detection of both efficacy and less common adverse events. The trials were also multinational and multi-site, improving generalizability across health systems and populations, though enrollment still skewed toward certain demographics, a limitation noted below.
The preclinical and early-phase foundation deserves brief mention as well. Before the phase 3 STEP trials, semaglutide’s appetite effects were characterized in controlled human feeding studies measuring ad libitum energy intake, appetite ratings, and gastric emptying, and its pharmacokinetics were established in dose-ranging studies. Animal models, including rodent obesity models, were used to map the central mechanism onto specific hypothalamic neuronal populations.11 This layered evidence, from molecular pharmacology through mechanistic human physiology to large outcome trials, is what distinguishes semaglutide’s dossier from that of compounds supported only by anecdote or small uncontrolled series.
One methodological limitation applies across the program and should be stated honestly: the pivotal trials were sponsored by the manufacturer, and the manufacturer was involved in trial design, data analysis, and manuscript preparation. This is standard for pharmaceutical development and does not by itself invalidate results, particularly for trials published in high-scrutiny journals with independent data-monitoring committees and, for SELECT, an independently adjudicated endpoint. But it is a real consideration in the hierarchy of evidence, and the field’s confidence rests substantially on the consistency of results across many trials, the transparency of the estimand reporting, and the emergence of independent real-world and comparative data, rather than on any single sponsored study.
Safety and Tolerability
No honest account of semaglutide’s role in obesity treatment is complete without its safety profile, which is well characterized precisely because the trials were large and long. The dominant theme is that the drug is generally tolerable but that gastrointestinal side effects are common, and a minority of participants discontinue because of them.
Gastrointestinal events are by far the most frequent adverse effects. In STEP 1, nausea was reported by 44.2% of the semaglutide group versus 16.1% on placebo, with diarrhea (29.7% vs 15.9%), vomiting (24.8% vs 6.8%), and constipation also elevated.1 These events were predominantly mild to moderate, appeared mostly during the 16-week dose-escalation phase, and typically attenuated over time.7 This temporal pattern is why the titration schedule is deliberately slow: starting at 0.25 mg and stepping up over four months is a tolerability strategy, not merely a pharmacokinetic one. Discontinuation attributable to gastrointestinal events was roughly 4.5% in STEP 1, a non-trivial but minority figure.1,7
Gallbladder-related disorders, particularly cholelithiasis (gallstones), were more frequent with semaglutide (about 2.6% vs 1.2% in STEP 1). This is thought to relate substantially to the rate of weight loss itself, a known trigger for gallstone formation, rather than to a unique drug toxicity.1 Acute pancreatitis has been a theoretical concern for the entire GLP-1 class; in the large trials, adjudicated pancreatitis events were uncommon and not clearly increased versus placebo, but the label advises discontinuation if pancreatitis is suspected.9
The most-discussed regulatory warning is the boxed warning for thyroid C-cell tumors. Rodent studies showed dose- and duration-dependent thyroid C-cell (medullary) tumors with GLP-1 receptor agonists. Whether this translates to humans is unknown; human relevance has not been established, and rodents have far higher thyroid C-cell GLP-1 receptor expression. Nonetheless, the FDA label contraindicates semaglutide in people with a personal or family history of medullary thyroid carcinoma or multiple endocrine neoplasia syndrome type 2.9 This is a precautionary contraindication grounded in animal data, and it is appropriate to describe it as such rather than as a demonstrated human hazard.
Other considerations documented in the label and trials include a modest increase in heart rate, the potential for injection-site reactions, rare hypersensitivity, and caution around diabetic retinopathy in some diabetic populations. In SELECT, adverse events leading to permanent discontinuation, driven largely by gastrointestinal disorders, occurred in about 10.0% of the semaglutide group versus 2.0% on placebo, a higher discontinuation rate than in the shorter STEP trials and a reminder that tolerability over multi-year exposure in an older, sicker population differs from tolerability in a 68-week efficacy trial.6 The table summarizes the principal safety signals.
| Signal | Frequency / nature | Interpretation |
|---|---|---|
| Nausea, vomiting, diarrhea | Common; mostly mild-moderate, titration-phase | Main tolerability limiter; attenuates over time |
| Cholelithiasis | Modestly increased | Largely linked to rapid weight loss |
| Acute pancreatitis | Uncommon; not clearly increased in trials | Class caution; discontinue if suspected |
| Thyroid C-cell tumors | Rodent finding; boxed warning | Human relevance unknown; precautionary contraindication |
| Heart rate increase | Small mean rise | Class effect; generally not clinically limiting |
Handling and Reconstitution in a Research Context
Commercial semaglutide (Ozempic, Wegovy, Rybelsus) is supplied as a ready-to-use pen or tablet with defined stability and does not require any preparation by the end user. In laboratory and research settings, however, semaglutide is often encountered as a lyophilized (freeze-dried) powder that must be reconstituted before it can be measured or used, and understanding the physicochemical handling is part of understanding the molecule. The material below is descriptive educational chemistry, not a use protocol, and it applies to research-grade handling rather than to any approved therapeutic product.
As a peptide, semaglutide is sensitive to heat, light, agitation, and repeated freeze-thaw cycles, all of which can promote aggregation or degradation and compromise the integrity of the molecule. Lyophilized peptide is the most stable form and is typically stored frozen (commonly around −20 °C) and protected from light until reconstitution. Reconstitution is generally performed with bacteriostatic water, which contains a small percentage of benzyl alcohol as a preservative and is preferred over plain sterile water when a solution will be accessed more than once, because the preservative limits microbial growth over the in-use period.
The mechanics of reconstitution follow standard peptide practice: the diluent is introduced slowly down the inner wall of the vial rather than injected directly onto the powder, and the vial is swirled gently rather than shaken, because vigorous agitation and foaming can denature peptides. After reconstitution, a solution is typically refrigerated at 2–8 °C and used within a defined window (commonly cited as around 28 days for a bacteriostatic-preserved peptide solution), with any change in clarity, the appearance of particulates, or discoloration taken as a signal to discard the material. These handling principles are generic to injectable peptides and are covered in more detail on the site’s semaglutide reference page and its broader dosage and reconstitution index.
Concentration arithmetic is where reconstitution becomes quantitatively relevant. The concentration of a reconstituted solution is simply the mass of peptide in the vial divided by the volume of diluent added. For example, a 10 mg vial reconstituted with 3.0 mL of bacteriostatic water yields approximately 3.33 mg/mL; on a U-100 insulin syringe, where 100 “units” correspond to 1.0 mL, one unit then corresponds to about 0.033 mg. Changing the diluent volume changes the concentration and therefore the volume that would contain any given mass. This is elementary dimensional analysis, but it is also the step where measurement errors most commonly arise in any injectable-peptide context, which is why calculators and worked examples are emphasized in educational materials.
It bears repeating that none of this constitutes a directive to prepare or administer semaglutide. The physicochemistry of peptide reconstitution is legitimately part of understanding how the molecule is studied and stored, and it is included here for that educational purpose. Any actual therapeutic use of semaglutide involves an approved, pre-formulated product under professional medical supervision, not a self-reconstituted preparation. Research-grade material is not manufactured, tested, or labeled to the standards required for human use, and treating it as interchangeable with an approved medicine would be a serious category error.
Limitations and the Human-Evidence Gap
Even with an unusually strong evidence base, semaglutide’s trial program has real limitations, and identifying them is part of reading the literature honestly rather than promotionally.
The most important limitation, already emphasized, is dependence on continued treatment. The withdrawal data show that weight and cardiometabolic benefits largely reverse after discontinuation, which means the trials demonstrate durable management on therapy rather than lasting change after therapy.3,5 The optimal long-term strategy, whether indefinite full-dose treatment, dose reduction, or structured off-drug maintenance, is not resolved by high-quality evidence, and this is a genuine gap rather than a settled question.
Second, generalizability is constrained by who was studied. Trial populations, while multinational, were not fully representative of the global population living with obesity; enrollment skewed toward certain age ranges, and long-term data beyond two to three years in unselected real-world populations are still accumulating. Real-world adherence, titration quality, and persistence differ markedly from the supervised trial setting, and observational data suggest a meaningful proportion of people discontinue within the first year, which erodes the average benefit seen in trials.
Third, the durability horizon is finite. STEP 5 provides two-year data and SELECT provides roughly three-year outcome data, which is excellent by pharmacotherapy standards, but obesity is a lifelong condition and definitive multi-decade safety and efficacy data do not yet exist. Rare long-latency adverse effects, by definition, are hard to exclude even with tens of thousands of patient-years of exposure.
Fourth, several mechanistic and outcome questions remain open. The SELECT mediation analysis showed that most of the cardiovascular benefit was not statistically explained by waist-circumference change, meaning the causal pathway is only partly understood.6 The effects of semaglutide on lean mass versus fat mass, on bone, and on outcomes in specific subpopulations (older adults, those with heart failure with preserved ejection fraction, chronic kidney disease) are being addressed in ongoing and secondary analyses but are not fully mature.
Finally, it is worth distinguishing this compound sharply from the “human-evidence gap” caveat that applies to many research peptides. For a poorly studied bioregulator, the honest statement is that rigorous independent human data barely exist. For semaglutide, the situation is inverted: the human evidence is abundant, high quality, and largely consistent, and the residual gaps are the refined, second-order questions that follow a mature evidence base, such as optimal maintenance strategy, very-long-term safety, and full mechanistic attribution. Conflating these two very different evidential situations would misrepresent both. The appropriate posture toward semaglutide is confidence in the demonstrated effects paired with clear-eyed acknowledgment of the specific questions still unanswered.
Regulatory Status
Semaglutide’s regulatory history is one of the clearest markers of how thoroughly it has been evaluated, and it maps directly onto the trial evidence discussed above. Each approval was tied to specific pivotal data rather than granted on general promise.
In the United States, the FDA approved subcutaneous semaglutide as Ozempic for type 2 diabetes glycemic control in December 2017, and the oral formulation Rybelsus in 2019.9 The higher-dose obesity formulation, Wegovy (semaglutide 2.4 mg once weekly), was approved for chronic weight management in June 2021, in adults with a BMI of at least 30, or at least 27 with a weight-related comorbidity, on the basis of the STEP program.9 In December 2022, the indication was extended to adolescents aged 12 and older following STEP TEENS.10 In March 2024, on the strength of SELECT, the FDA added the cardiovascular risk-reduction indication for adults with established cardiovascular disease and overweight or obesity, and more recently an oral 25 mg formulation for weight management advanced through the OASIS program.6,9
In Europe, the European Medicines Agency granted marketing authorization for Wegovy for weight management, mirroring the US indications and BMI thresholds, and semaglutide is authorized across numerous other jurisdictions worldwide. The consistency of approvals across independent regulators, each conducting its own review of the same underlying trial data, is itself a form of corroboration: multiple agencies with different standards reached concordant conclusions about efficacy and acceptable risk.
An important regulatory nuance concerns compounded and research-grade semaglutide. During periods of shortage, some pharmacies in the US compounded semaglutide, and separately, “research chemical” vendors have marketed semaglutide powder not intended for human use. These products are not FDA-approved, are not manufactured to the same quality standards as the branded product, and have been the subject of explicit regulatory warnings about potency, purity, and safety. Nothing in the trial evidence discussed in this article transfers to unapproved compounded or research-grade material; the STEP and SELECT results were generated with a specific, quality-controlled formulation. This distinction is not a technicality. The demonstrated benefit-risk profile belongs to the studied product under medical supervision, not to any peptide labeled “semaglutide.”
The regulatory arc also illustrates how “long-term obesity treatment” became an accepted framing. Regulators did not merely approve a drug that causes weight loss; they progressively endorsed indications reflecting chronic management (adults, then adolescents, then cardiovascular risk reduction), each grounded in a trial designed to answer a durability or outcome question. The regulatory record and the trial record are, in this sense, the same story told through two institutions.
Frequently Asked Questions
Is semaglutide FDA-approved for weight loss?
Yes. The high-dose formulation, semaglutide 2.4 mg once weekly (brand name Wegovy), was approved by the FDA for chronic weight management in adults in June 2021, extended to adolescents 12 and older in 2022, and given an additional cardiovascular risk-reduction indication in 2024.9 The lower-dose Ozempic is approved for type 2 diabetes, not weight management, though it contains the same active molecule. Approval was based on the STEP and SELECT trials.
How much weight did people lose in the trials?
In STEP 1, adults without diabetes lost a mean of about 14.9% of body weight over 68 weeks versus 2.4% on placebo, with roughly 86% achieving at least 5% loss.1 STEP 5 extended this to two years with a mean loss of about 15.2%.4 In adults with type 2 diabetes (STEP 2), the effect was smaller, around 9.6%.2 These figures describe supervised trials that paired the drug with lifestyle counseling, so they represent the drug effect on top of that support.
Does the weight come back if you stop taking it?
Largely, yes. In the STEP 1 extension, participants regained about two-thirds of their lost weight in the year after stopping, and cardiometabolic improvements reversed.5 In STEP 4, switching to placebo at week 20 led to steady regain while continuing the drug sustained and deepened the loss.3 This is why the field describes semaglutide as managing a chronic condition rather than curing it. The benefit depends on continued treatment.
Did the trials show heart benefits or just weight loss?
The dedicated SELECT trial showed a 20% relative reduction in major adverse cardiovascular events (cardiovascular death, heart attack, or stroke) over about 40 months in more than 17,000 adults with overweight or obesity and established cardiovascular disease, but without diabetes.6 This is a genuine hard-outcome benefit, but it applies to a high-risk population and should not be generalized to healthy people. Notably, only about a third of the benefit was statistically explained by waist-circumference reduction, so weight loss alone does not fully account for it.
How does semaglutide compare with tirzepatide?
In the head-to-head SURMOUNT-5 trial, tirzepatide produced greater mean weight loss than semaglutide 2.4 mg (about 20.2% versus 13.7% over 72 weeks), with a similar gastrointestinal side-effect profile.8 Tirzepatide activates both GLP-1 and GIP receptors, whereas semaglutide targets GLP-1 alone. Semaglutide, however, has the larger and longer cardiovascular outcomes dataset. Neither is universally “better”; they differ in mechanism, magnitude of weight loss, and depth of outcome evidence.
What are the most common side effects?
Gastrointestinal effects dominate: nausea, diarrhea, vomiting, and constipation, reported far more often than on placebo (for example, nausea in about 44% versus 16% in STEP 1).1 These are usually mild to moderate, most common during the 16-week dose-escalation period, and tend to lessen over time. Gallstones can occur, largely related to rapid weight loss, and the label carries a precautionary boxed warning about thyroid C-cell tumors based on rodent data whose human relevance is unknown.9
Why is semaglutide titrated up slowly?
Dose escalation from 0.25 mg to the 2.4 mg maintenance dose over about 16 weeks is primarily a tolerability strategy. Gastrointestinal side effects are most intense when the dose increases, so gradual escalation gives the body time to adapt and reduces the likelihood of nausea severe enough to cause discontinuation.7 The long, roughly one-week half-life also means the drug accumulates to steady state gradually, which the titration schedule accommodates.
Is research-grade or compounded semaglutide the same as Wegovy?
No. The trial evidence in this article was generated with a specific, quality-controlled, FDA-approved formulation. Compounded semaglutide and “research chemical” powders are not FDA-approved, are not manufactured or tested to the same standards, and have been the subject of regulatory warnings about potency and purity. The demonstrated benefit-risk profile does not transfer to unapproved material, and any therapeutic use should involve an approved product under medical supervision.
References
- Wilding JPH, Batterham RL, Calanna S, et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity (STEP 1). N Engl J Med. 2021;384(11):989–1002. https://www.nejm.org/doi/full/10.1056/NEJMoa2032183
- Davies M, Faerch L, Jeppesen OK, et al. Semaglutide 2·4 mg once a week in adults with overweight or obesity, and type 2 diabetes (STEP 2). Lancet. 2021;397(10278):971–984. https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(21)00213-0/abstract
- Rubino D, Abrahamsson N, Davies M, et al. Effect of Continued Weekly Subcutaneous Semaglutide vs Placebo on Weight Loss Maintenance in Adults With Overweight or Obesity (STEP 4). JAMA. 2021;325(14):1414–1425. https://pmc.ncbi.nlm.nih.gov/articles/PMC7988425/
- Garvey WT, Batterham RL, Bhatta M, et al. Two-year effects of semaglutide in adults with overweight or obesity: the STEP 5 trial. Nat Med. 2022;28(10):2083–2091. https://www.nature.com/articles/s41591-022-02026-4
- Wilding JPH, Batterham RL, Davies M, et al. Weight regain and cardiometabolic effects after withdrawal of semaglutide: The STEP 1 trial extension. Diabetes Obes Metab. 2022;24(8):1553–1564. https://pmc.ncbi.nlm.nih.gov/articles/PMC9542252/
- Lincoff AM, Brown-Frandsen K, Colhoun HM, et al. Semaglutide and Cardiovascular Outcomes in Obesity without Diabetes (SELECT). N Engl J Med. 2023;389(24):2221–2232. https://www.nejm.org/doi/full/10.1056/NEJMoa2307563
- Wharton S, Calanna S, Davies M, et al. Gastrointestinal tolerability of once-weekly semaglutide 2.4 mg in adults with overweight or obesity, and the relationship between gastrointestinal adverse events and weight loss. Diabetes Obes Metab. 2022;24(1):94–105. https://pmc.ncbi.nlm.nih.gov/articles/PMC9293236/
- Aronne LJ, Horn DB, le Roux CW, et al. Tirzepatide versus Semaglutide for Weight Loss in Adults with Obesity (SURMOUNT-5). N Engl J Med. 2025;392(1):26–36. https://www.nejm.org/doi/full/10.1056/NEJMoa2416394
- U.S. Food and Drug Administration. Wegovy (semaglutide) injection, for subcutaneous use: Highlights of Prescribing Information (revised 2024; includes boxed warning for thyroid C-cell tumors, MTC/MEN 2 contraindication, and the March 2024 cardiovascular risk-reduction indication). Reference NDA 215256. https://www.accessdata.fda.gov/drugsatfda_docs/label/2024/215256s015lbl.pdf
- Weghuber D, Barrett T, Barrientos-Perez M, et al. Once-Weekly Semaglutide in Adolescents with Obesity (STEP TEENS). N Engl J Med. 2022;387(24):2245–2257. https://www.nejm.org/doi/full/10.1056/NEJMoa2208601
- Müller TD, Finan B, Bloom SR, et al. Glucagon-like peptide 1 (GLP-1): molecular pharmacology, receptor signaling, and central appetite regulation. Mol Metab. 2019;30:72–130. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6812410/
- Lau J, Bloch P, Schäffer L, et al. Discovery of the Once-Weekly Glucagon-Like Peptide-1 (GLP-1) Analogue Semaglutide. J Med Chem. 2015;58(18):7370–7380. https://pubmed.ncbi.nlm.nih.gov/26308095/
- Rubino DM, Greenway FL, Khalid U, et al. Effect of Weekly Subcutaneous Semaglutide vs Daily Liraglutide on Body Weight in Adults With Overweight or Obesity Without Diabetes (STEP 8): A Randomized Clinical Trial. JAMA. 2022;327(2):138–150. https://jamanetwork.com/journals/jama/fullarticle/2788093
Educational and research-use disclaimer: This article is provided solely for scientific education about the peer-reviewed clinical literature and does not constitute medical advice, diagnosis, treatment guidance, or a recommendation to obtain, prepare, or use any substance. Semaglutide is a prescription medicine; decisions about its use belong to qualified healthcare professionals in the context of an individual patient. Research-grade or compounded material is not approved for human use and is not equivalent to any FDA-approved product. Claims here are limited to what the cited primary trials actually demonstrated, and nothing in this article should be read as asserting that semaglutide cures obesity or any other disease.