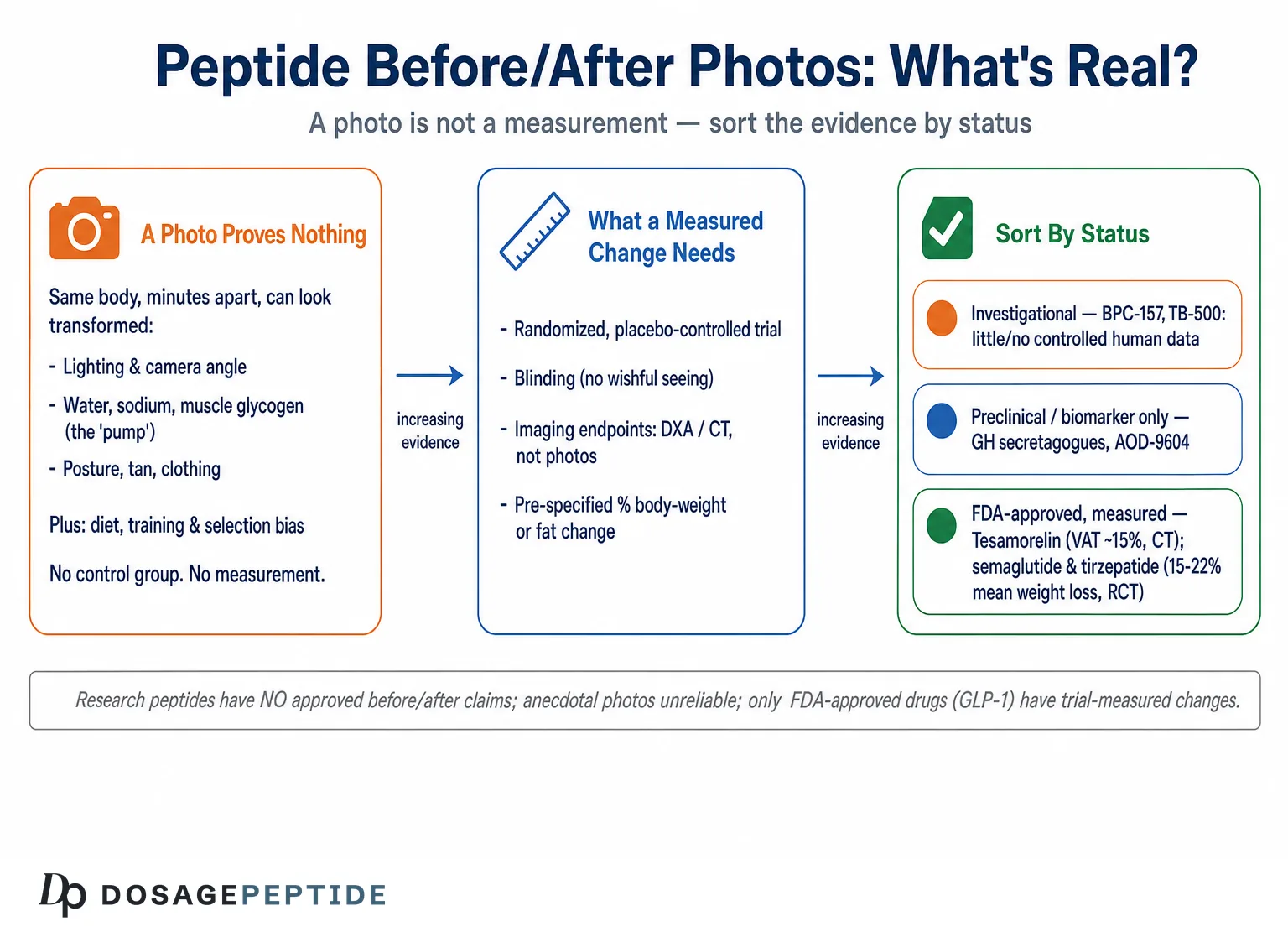
Type any peptide name into a search bar with the words “before and after” and you will be flooded with side-by-side photographs: a slack, dim, slumped “before” on the left and a lit, dry, flexed “after” on the right. The images are persuasive precisely because they are visual — they seem to skip past argument and simply show you the result. But a photograph is not a measurement, and a research peptide is not a proven cosmetic. The honest answer to the question “what results are realistic?” begins with an uncomfortable fact that most of these galleries are built to obscure: for the overwhelming majority of research peptides, there is no approved before/after claim for body composition, skin, hair, or physique, and the anecdotal photographs circulating online are among the least reliable forms of evidence a person can consult.
This article is not an attempt to talk anyone out of curiosity. It is an attempt to give that curiosity a ruler. We will separate three things that popular writing constantly blurs: what a research peptide legally and scientifically is, what a before/after photograph can and cannot demonstrate, and what a genuinely trial-measured body change looks like when a compound has actually been studied. The contrast at the center of the piece is deliberate. On one side sit unapproved research peptides with photographic anecdotes and no controlled human outcome data for the effect being claimed. On the other sit a handful of FDA-approved drugs — the GLP-1 and dual/triple incretin agonists, and the growth-hormone-releasing analog tesamorelin — whose body changes were measured in thousands of people, under blinding, against placebo, with imaging and body-composition endpoints rather than posing.14 Understanding why one kind of evidence is trustworthy and the other is not is the single most useful skill for reading any peptide “transformation.”
The guiding principle throughout is calibration, not cynicism. Some peptides do things; some approved drugs produce large, real, measured changes in the body; and some popular research compounds have almost no human data at all for the outcomes their photos imply. The goal is to tell those cases apart honestly, so that a reader looking at two photographs knows exactly what they are — and are not — entitled to conclude.
What a “Research Peptide” Actually Is — and Why It Has No Before/After Claim
The phrase “research peptide” is doing a great deal of quiet work in every before/after gallery, and it is worth unpacking because it is the legal and scientific root of why those photos cannot mean what they appear to mean. A research peptide, in the sense used across this field, is a compound sold and labeled for laboratory or investigational use only — not an approved medicine, not a dietary supplement with a substantiated structure-function claim, and not a cosmetic with a demonstrated effect on appearance. That labeling is not a technicality or a marketing pose; it reflects the actual regulatory reality that the compound has not cleared the evidentiary bar that would permit any claim that it changes the human body in a specified way.
To earn an approved before/after claim — the kind a pharmaceutical company can print — a compound must generally pass through randomized, controlled, adequately powered human trials with pre-specified endpoints, then survive regulatory review of that evidence. The endpoints are quantitative and defined in advance: percent change in body weight, visceral adipose tissue measured by imaging, lean mass by dual-energy X-ray absorptiometry (DXA), wrinkle depth by validated grading scale, and so on. A photograph is never the primary endpoint, because a photograph cannot be standardized across thousands of participants or blinded to the person taking it. When a compound has passed this process, its “before and after” is a table of numbers with confidence intervals. When it has not, its “before and after” is, at best, a collection of individual anecdotes and, at worst, a marketing artifact.
Most research peptides sit in the second category for the outcomes their photos imply. BPC-157 is the clearest example: despite enormous popularity and confident regenerative marketing, the entire human evidence base consists of a handful of tiny studies, and independent reviews describe it as investigational with minimal human data.911 The U.S. Department of Defense’s Operation Supplement Safety program flatly classifies BPC-157 as an unapproved drug and a prohibited substance found in wellness products — not a compound with an established cosmetic or physique effect.10 None of that means BPC-157 does nothing in a petri dish or a rat; it means there is no approved, trial-measured human before/after for it, and any photo presented as one is an anecdote wearing a lab coat. Readers who want the fuller picture on that specific compound can consult our explainer on what BPC-157 is and what the evidence actually shows.
It is worth pausing on why the “for research use only” label is not merely defensive boilerplate. That designation exists because the compound has not been characterized to pharmaceutical standards for human use: its purity, dosing, pharmacokinetics, long-term safety, and — crucially — its efficacy for any stated outcome have not been established through the process that would license a claim. A vendor can therefore sell the molecule while making no legal representation that it does anything at all to a human body. The before/after photographs then function as a workaround: they imply the efficacy claim the label is legally forbidden to make. Recognizing that structure — a disclaimer that denies efficacy paired with imagery that asserts it — is one of the fastest ways to calibrate how much weight a given gallery deserves.
The upshot of this section is a reframing that should travel with you through the rest of the article. When someone shows you a research-peptide before/after, the correct first question is not “is that transformation real?” but “what kind of evidence is this, and what claim is it entitled to support?” For an unapproved research compound, the answer is almost always: an uncontrolled personal anecdote that cannot, by its nature, separate the peptide from everything else that changed between the two photographs.
The Photography Problem: How Two Photos Can Lie Without a Single Edited Pixel
The most important thing to understand about before/after photographs is that they can be profoundly misleading even when nobody has touched Photoshop, lied about a timeline, or staged anything the person would call “fake.” The deception is built into the medium. A photograph captures a single instant of a body under a specific set of conditions — lighting, hydration, glycogen, posture, muscle contraction, camera angle, lens, and clothing — and every one of those variables can be moved dramatically in minutes without changing an ounce of actual fat or muscle.
Fitness professionals have documented this openly. A widely cited breakdown of “transformation” tricks describes taking a deliberately unflattering “before” — harsh overhead light, relaxed and pushed-out abdomen, ill-fitting clothes, taken after a salty, carbohydrate-heavy meal that maximizes water retention and bloat — then producing the “after” hours or a day later: softer frontal lighting, abdomen braced, a set of push-ups to engorge the muscles with blood (the “pump”), better-fitting clothing, a slight tan, and a confident posture.12 In one documented case a bodybuilder produced a convincing “before” and “after” in a matter of hours, in the wrong order, using nothing but food, water, lighting, and posing.12 No fat was lost. No muscle was built. Yet the two images look like months of transformation.
The physiological levers behind this are worth naming, because they are exactly the ones a peptide anecdote cannot control for:
- Water and sodium. Subcutaneous water shifts blur muscle definition and abdominal lines. A high-sodium, high-carbohydrate day versus a depleted, low-sodium day can change how “lean” a person looks without altering fat mass at all.
- Muscle glycogen and the pump. Skeletal muscle stores glycogen with water; a trained, carb-loaded, recently exercised muscle looks fuller and more vascular than the same muscle depleted and at rest.
- Lighting direction and hardness. Overhead, hard light casts shadows that exaggerate softness and sag; frontal or angled soft light flatters. This alone can manufacture the appearance of an abdominal “six-pack.”
- Posture and contraction. Standing tall, rolling the shoulders back, and bracing the core versus slumping and relaxing changes the visible silhouette instantly.
- Camera angle, distance, and lens. A slightly higher camera, greater distance, and a longer focal length are all slimming; the opposite exaggerates the waist.
- Tan and clothing. Darker skin tone increases visible muscle contrast; fitted or strategically colored clothing changes perceived proportions independent of the body underneath.
Because all of these can be adjusted in a single session, a pair of photographs is essentially unfalsifiable as evidence of a compound’s effect. There is no way, from the images alone, to know whether the difference reflects fat loss, muscle gain, a change in water and glycogen, or simply a better-produced second photo. Research on transformation imagery adds a further wrinkle: these paired “before/after” images are unusually persuasive precisely because they imply not just an ideal outcome but its attainability, which is part of why they drive behavior and emotion more strongly than a single physique photo.13 That persuasive power is a feature for the person selling the peptide and a hazard for the person evaluating it.
Confounders: Everything Else That Changed Between the Two Photos
Suppose the photographs are honest — same lighting, same time of day, same hydration, genuinely months apart, and a real visible change. Even then, an uncontrolled anecdote cannot attribute that change to the peptide, because a person who buys and uses a research peptide almost never changes only the peptide. The decision to try a compound is usually embedded in a broader burst of motivation, and that motivation moves many levers at once.
The classic confounders in any self-reported peptide transformation include:
- Diet. The single most powerful determinant of visible body change. Someone motivated enough to source and inject a peptide is frequently also eating in a caloric deficit or surplus, raising protein, and cutting alcohol — each capable of producing the entire observed effect.
- Training. New or intensified resistance training reliably changes physique and the “pump” that photos capture. Beginners in particular can gain muscle and lose fat simultaneously, producing dramatic photos from training alone.
- Sleep and stress. Improvements here alter cortisol, water retention, and facial appearance in ways that read as “the peptide is working.”
- Concurrent compounds. Peptides are frequently stacked with other peptides, supplements, or, in some cases, anabolic agents — any of which could be responsible for the change.
- Time and regression to the mean. People often start a compound at a low point (post-injury, post-holiday, deconditioned). Simple return to baseline over weeks can masquerade as a treatment effect.
Layered on top of these is the most corrosive statistical problem of all: selection bias. The before/after photos you see are not a random sample of everyone who tried the compound. They are the tiny, self-selected subset who both experienced a favorable change and chose to post it. The people who saw nothing, felt worse, or had a side effect are silently absent. This is survivorship bias in its purest form: the gallery is assembled by filtering for success after the fact, which guarantees an impressive collage no matter how ineffective the compound. Even a completely inert substance would generate a wall of “transformations” given enough users, enough motivation-driven diet-and-training changes, and enough photographic latitude.
This is not a peptide-specific failing; it is why medicine abandoned the anecdote as a basis for efficacy claims more than half a century ago in favor of the randomized controlled trial. A trial fixes each of these confounders deliberately: it randomizes participants so diet, training, and baseline are balanced across groups; it blinds participants and investigators so expectation cannot color the outcome; it includes a placebo group so the effect of “doing something” is subtracted; and it pre-specifies quantitative endpoints so the result cannot be curated after the fact. A before/after photo has none of these protections. It is, structurally, the thing the entire apparatus of clinical trials exists to replace.
There is a subtler cognitive trap worth naming here as well: the placebo response is real and powerful for exactly the things photos capture. Expectation alone can change training intensity, dietary discipline, sleep, posture, and self-perception. A person who believes a peptide is working often trains harder and eats more carefully because they believe it — and then attributes the resulting change to the compound rather than to their own altered behavior. This is not dishonesty; it is how human psychology interacts with self-experimentation. It is also precisely why the placebo arm of a trial is indispensable: it captures all of that behavioral and perceptual lift and subtracts it, leaving only the compound’s specific pharmacological contribution. In an uncontrolled anecdote, the placebo effect and the drug effect are permanently fused, and no amount of sincerity on the user’s part can pull them apart.
A final structural point about anecdotes: they are non-cumulative in a way trials are not. A hundred before/after photos are not a hundred times more convincing than one, because they share the same biases — each is self-selected, uncontrolled, and confounded in the same direction. Stacking biased evidence does not average out the bias; it amplifies the illusion of consensus. Trials, by contrast, are designed to accumulate: independent, controlled studies can be pooled in meta-analyses precisely because each one has already neutralized the confounders that make anecdotes incommensurable. When people say “but thousands of users can’t all be wrong,” they are misunderstanding how bias works. Thousands of users under the same systematic bias can, in fact, all be wrong in the same direction — that is what systematic bias means.
The Contrast Case: What a Trial-Measured Body Change Actually Looks Like
To see how far an anecdote falls short, it helps to look at the opposite extreme — compounds whose body-composition effects have been measured properly — and the clearest modern examples are the incretin-based weight-loss drugs. These are not research peptides in the unapproved sense; the leading agents are FDA-approved medicines whose changes were quantified in large, blinded, placebo-controlled trials. They are the right yardstick precisely because they show what real, defensible before/after evidence looks like.
Consider semaglutide, the GLP-1 receptor agonist. In the STEP 1 trial — a randomized, double-blind, placebo-controlled study of 1,961 adults with overweight or obesity — participants on the 2.4 mg weekly dose lost a mean of 14.9% of body weight over 68 weeks, versus 2.4% on placebo.2 That difference is not a curated photo; it is a mean across nearly two thousand people, with a placebo arm subtracting the effect of the accompanying diet-and-activity program, published in a peer-reviewed journal.2 A DXA substudy went further and measured composition, not just weight, documenting reductions in both fat mass and lean mass with a net increase in the proportion of lean mass to total mass — the kind of granular, imaging-based readout no photograph can provide.2
Tirzepatide, the dual GIP/GLP-1 agonist, pushed the numbers higher. In SURMOUNT-1, a randomized, double-blind, placebo-controlled trial in adults with obesity or overweight, mean weight reductions at 72 weeks were 16.0%, 21.4%, and 22.5% at the 5, 10, and 15 mg doses respectively, versus 2.4% for placebo.1 Nearly all treated participants (89–96%) lost at least 5% of body weight, and roughly a third to 40% at the higher doses lost at least a quarter of their body weight.1 Our overview of how tirzepatide works and a closer look at its measured effects on fat loss and insulin sensitivity walk through the mechanism behind those numbers.
The investigational triple agonist retatrutide (GLP-1/GIP/glucagon) went higher still in phase 2: least-squares mean weight change at 48 weeks reached −24.2% at the 12 mg dose versus −2.1% for placebo, in a randomized, double-blind, placebo-controlled trial.3 It is worth flagging the honesty caveat here — retatrutide is investigational, not FDA-approved, and phase 2 results can shrink in larger phase 3 programs — but even as an investigational agent, its evidence is a different species from an anecdote: pre-registered, blinded, placebo-controlled, and quantitatively reported.3 Our primer on what retatrutide is and how it works covers the receptor pharmacology in detail.
| Feature | Anecdotal peptide “before/after” | Trial-measured body change (GLP-1 class) |
|---|---|---|
| Sample | Self-selected individuals who posted a success | Hundreds to thousands, randomized12 |
| Control group | None | Placebo arm, double-blind12 |
| Outcome measured | A posed photograph | % body weight; fat & lean mass by DXA2 |
| Confounders (diet, training, water) | Uncontrolled and usually unreported | Balanced by randomization; lifestyle standardized1 |
| Pre-specified endpoint | No — result curated after the fact | Yes — registered before enrollment3 |
| Reproducibility | Cannot be reproduced or audited | Replicated across multiple trials & sites13 |
| Typical effect claim | Implied but unquantified | 15–24% mean weight loss, with CIs123 |
The table makes the asymmetry visceral. It is not that trials are “more impressive” than photos; it is that they answer a fundamentally different question. A photo asks “can this compound ever coincide with a good-looking result?” — to which the answer is trivially yes for almost anything. A trial asks “does this compound, on average, cause a measurable change beyond placebo?” That is the only question worth basing an expectation on, and only the second kind of evidence can answer it.
The Scale, the Mirror, and the DXA: Why Body Composition Undermines Photos
Even trial-measured weight loss hides a subtlety that photographs completely miss and that matters enormously for “realistic results”: what is being lost. Body weight is a crude aggregate of fat, muscle, bone, water, and gut contents. Two people can lose the same number of kilograms and look and function very differently depending on the composition of that loss. This is exactly why serious trials measure body composition by DXA rather than relying on the scale — and why a photo, which can be manipulated by water and glycogen alone, is such a poor proxy.
The incretin drugs illustrate the point precisely. Across GLP-1 receptor agonist and co-agonist studies, a meaningful fraction of the weight lost is lean mass, not fat — reviews and analyses put lean-mass loss at roughly 20–40% of total weight lost, depending on the population and how it is measured.68 That is not necessarily pathological: because fat is lost preferentially, the proportion of lean mass to total mass typically rises, and dedicated studies such as SEMALEAN have examined how semaglutide affects fat mass, lean mass, and muscle function together rather than in isolation.27 The clinical field now actively debates how to preserve muscle during rapid weight loss — through resistance training and adequate protein, and in research settings through agents aimed at muscle — precisely because the scale and the mirror cannot see the difference between fat loss and muscle loss.68
For the reader evaluating a peptide before/after, this has two blunt implications. First, a “leaner”-looking after photo tells you nothing about whether the person retained or lost muscle, protected bone, or simply dropped water — distinctions that require imaging, not posing. Second, the compounds that do have measured composition data are, again, the approved and investigational drugs studied with DXA, not the research peptides whose galleries dominate social media. When someone claims a peptide produced “body recomposition” — simultaneous fat loss and muscle gain — ask for the DXA scans and the controlled comparison. In nearly every case for an unapproved research peptide, they do not exist.
It is also worth stating plainly that the mirror is not a neutral instrument for the person looking into it. Motivation, expectation, and the money and effort already invested in a compound bias self-perception toward seeing improvement. This is why blinding exists in trials and why it cannot exist in a personal anecdote. The user who wants the peptide to work is, unavoidably, the least reliable judge of whether it did.
Tesamorelin: A Peptide With a Real, Approved, Measured Body Change
To keep this honest in both directions, it is important to acknowledge that “peptide” and “no approved body-change claim” are not synonyms. At least one peptide-class agent has an FDA-approved indication for changing where fat sits on the body, backed by imaging endpoints in randomized trials — and it is instructive precisely because it shows what a legitimate peptide before/after requires.
Tesamorelin is a synthetic analog of growth-hormone-releasing hormone (GHRH). In a randomized, double-blind, placebo-controlled trial of 412 patients with HIV-associated abdominal fat accumulation, daily subcutaneous tesamorelin reduced visceral adipose tissue (VAT) by about 15% as measured by CT imaging, versus a slight increase on placebo, over 26 weeks.4 On the strength of that and confirmatory data, it is FDA-approved specifically for the reduction of excess abdominal fat in adults with HIV-associated lipodystrophy — and the approved labeling is careful to note that the long-term safety and cardiovascular benefit of that fat reduction have not been established, and that the effect reverses when the drug is stopped.45
Several features of the tesamorelin story are worth extracting as a template for what a trustworthy peptide before/after actually needs:
- A defined population and indication. The claim is not “melts belly fat” in general; it is a reduction in visceral fat in a specific patient group.
- An imaging endpoint. The change was measured by CT-quantified VAT, not by photographs — a number that is reproducible and blinded.4
- A placebo comparison. The 15% reduction is meaningful because placebo did the opposite; the difference is attributable to the drug.4
- Honest limits in the label. The approved indication does not claim general weight loss, cosmetic physique change, or proven downstream health benefit, and it notes reversibility.5
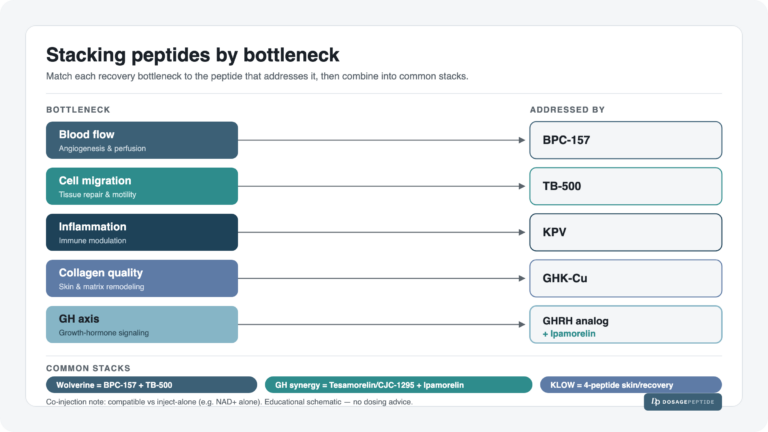
Contrast this with the way growth-hormone-releasing and secretagogue peptides are marketed informally for “fat loss” and “lean gains” in the general population. The moment you move outside the studied indication — a different population, a cosmetic rather than clinical goal, no imaging, no control — the tesamorelin evidence does not transfer, and you are back to anecdote. The lesson is not “peptides never work.” It is that a real before/after claim is narrow, measured, controlled, and honestly bounded — and that almost none of the sweeping physique claims attached to research peptides meet that standard.
Peptide by Peptide: What the Evidence Actually Supports
Generalities only go so far; it helps to walk through the compounds whose before/after galleries are most common and label the evidence for the specific outcome being pictured. The recurring pattern is that mechanistic and preclinical plausibility is often real, while controlled human evidence for the cosmetic or physique claim is thin to nonexistent.
| Compound | Common before/after claim | Best available human evidence for that claim | Honest label |
|---|---|---|---|
| BPC-157 | Healing, recovery, leaner recovery physique | A few tiny studies (single digits to ~16 participants), no large controlled trials911 | Investigational; unapproved drug10 |
| TB-500 / thymosin β4 fragment | Injury recovery, muscle repair | Preclinical/animal signals; no controlled human physique trials | Preclinical; no human outcome data |
| GHK-Cu (topical) | Wrinkle reduction, skin firmness | Small cosmetic-dermatology studies; short-term, mostly industry-linked | Limited cosmetic evidence, not a drug claim |
| AOD-9604 | Fat loss / physique change | Obesity RCTs did not reliably beat placebo; development halted | No convincing human efficacy |
| GH secretagogues (e.g., ipamorelin, CJC-1295) | Fat loss, lean gains, anti-aging | Raise GH/IGF-1 markers; no controlled physique-outcome trials in healthy adults | Biomarker change ≠ proven body change |
| Tesamorelin | Visceral fat reduction | RCTs with CT-measured VAT reduction ~15%4 | FDA-approved, narrow indication5 |
| Tirzepatide / semaglutide | Major weight/fat loss | Large RCTs, 15–22% mean weight loss vs placebo12 | FDA-approved; strongest evidence |
Reading down the table, the gradient is clear. At the bottom sit approved drugs with large, replicated, controlled human outcomes and imaging or composition endpoints. In the middle sits tesamorelin, approved for a narrow, measured indication. At the top sit the classic research peptides, where the strongest honest statement is usually “plausible mechanism, promising preclinical data, little or no controlled human evidence for the pictured effect.” A before/after photo attached to a top-of-table compound is not evidence that it works; it is evidence that a motivated person took two photos.
Two specific corrections are worth making because they recur constantly. First, AOD-9604 — frequently marketed with fat-loss transformations — is a growth-hormone fragment whose own obesity trials failed to reliably separate from placebo, and whose development as a weight-loss drug was abandoned; our review of what the clinical trials indicate about AOD-9604’s fat-burning potential lays out that record. Second, growth-hormone secretagogues that raise IGF-1 on a lab report are often presented as if the biomarker is the physique change. It is not. A rise in a signaling molecule is a mechanistic step, not a demonstrated, controlled change in fat mass or muscle in the people using it. For skin-focused claims around GHK-Cu, our piece on what GHK-Cu does for skin health and collagen similarly separates the small cosmetic studies from the sweeping anti-aging claims.
It is worth stating explicitly what the evidence for these top-of-table research peptides does not show, because the absence is easy to miss under a wall of confident marketing. For BPC-157, TB-500, and the growth-hormone secretagogues, there are no adequately powered, randomized, placebo-controlled human trials demonstrating fat loss, muscle gain, or “recomposition” measured by DXA or any other validated instrument in healthy people. There is no established, characterized human dose that has been shown to produce a specific body change; no published composition endpoints; no long-term human safety dataset; and, for most of these compounds, no independent replication outside a small number of laboratories. That is not a claim that they are inert — preclinical and mechanistic signals are often genuine — but it is a precise statement that the specific cosmetic or physique outcome the photographs imply has not been demonstrated to the standard that would license the claim. When a compound is described as “preclinical” or “investigational” in the table above, that word is doing real work: it means the human before/after has not been generated, only imagined onto a molecule with promising cell-culture and animal data.
How the Body Actually Changes — and How Fast It Realistically Can
Part of what makes before/after photos so misleading is that they compress and exaggerate timelines the body cannot actually follow. Setting compounds aside entirely, it is worth grounding “realistic” in physiology, because the ceilings are far lower than the galleries imply.
Fat loss is bounded by energy balance. A pound of body fat stores roughly 3,500 kcal, so even an aggressive, sustainable daily deficit yields on the order of 0.5–1% of body weight per week before muscle loss and metabolic adaptation become serious problems. The GLP-1 trials, with their large mean losses, achieved them over 68–72 weeks, not weeks — 15–22% body-weight loss is a year-plus of consistent treatment plus lifestyle, not a month.12 Any before/after implying comparable change in a few weeks is describing water, glycogen, and photography, not fat.
Muscle gain is slower and more tightly capped. A well-trained adult may add only a few pounds of true muscle in a year of dedicated resistance training and adequate protein; untrained beginners gain faster initially, which is exactly why beginner “transformations” are so dramatic and so easily misattributed to whatever supplement or peptide happened to be introduced at the same time. No approved peptide, and certainly no research peptide with human data, has been shown to override these ceilings for physique in healthy people.
Skin and hair changes are governed by even longer biological clocks. Dermal collagen remodeling and the hair-growth cycle operate over months; a two-week “before/after” for skin or hair is measuring lighting, grooming, and product film far more than tissue change. When cosmetic ingredients are studied properly, meaningful endpoints are measured over 8–12 weeks or longer with instrumented grading, not selfies. A realistic mental model, then, is this: the faster and more dramatic a before/after appears relative to these biological timelines, the more of the apparent change is being carried by the reversible, manipulable variables — water, glycogen, pump, light, and pose — rather than by any durable remodeling of fat, muscle, skin, or hair.
The table below sets those biological ceilings against the timeframes most before/after galleries imply. The gap between the two columns is, in practice, the space where photographic manipulation and confounders live.
| Change | Realistic biological rate | What a fast “before/after” is usually showing |
|---|---|---|
| Fat loss | ~0.5–1% of body weight/week; 15–22% took 68–72 weeks in trials12 | Water, glycogen depletion, lighting, posing |
| Muscle gain | A few pounds/year in trained adults; faster only in true beginners | The “pump,” tan, contraction, camera angle |
| Skin (collagen) | Remodeling over months; studied at 8–12+ weeks | Grooming, product film, lighting, makeup |
| Hair growth | Follicle cycles over months; ~1 cm/month at most | Styling, lighting, wet-vs-dry, camera resolution |
| Visible “definition” | Requires real fat loss over months | Sodium/water shifts within a single day12 |
Read across any row and the same lesson repeats: the durable, tissue-level change is slow and modest, while the appearance of change can be conjured quickly and cheaply. A gallery that promises the slow column on the timeline of the fast column is, definitionally, selling the manipulable variables as if they were biology.
Red Flags: How to Read Any Peptide “Transformation”
Given all of the above, a practical checklist is more useful than any single verdict. When you encounter a peptide before/after — on a vendor site, a forum, or social media — the following features should sharply lower your confidence that the compound caused the pictured change:
- Different lighting, angle, or posture between the two photos. Hard overhead light and a slumped “before” versus soft frontal light and a braced “after” is the oldest trick in the book.12
- A pump or tan in the after but not the before. Both are minutes-to-hours variables with zero relationship to the compound.
- No stated timeline, or an implausibly short one. Dramatic change in days or a couple of weeks is water and photography, not fat or muscle.1
- No mention of diet, training, or other compounds. If the confounders are invisible, they are almost certainly doing the work.
- A single dramatic example rather than a controlled average. One person’s photo is selection bias; a mean with a placebo comparison is evidence.
- Commercial context. The photo is next to a “buy” button, discount code, or affiliate link. The incentive to curate is total.
- Claims that outrun the compound’s human data. “Builds muscle,” “melts fat,” or “reverses aging” for a compound with no controlled human trials for that outcome is a marketing claim, not a finding.
- Biomarker-as-outcome substitution. “IGF-1 went up” or “collagen increased in vitro” presented as if it were a demonstrated physique or skin change.
The inverse checklist — the features that would raise confidence — describes a clinical trial, not a photo: a control group, blinding, a pre-specified quantitative endpoint, imaging or composition measurement, an adequate sample, and peer-reviewed publication. For any compound where that evidence exists, you will not need the photos; for any compound where it does not, the photos cannot substitute for it. Our peptide research glossary defines many of the endpoint and study-design terms that separate the two, which is useful when a claim leans on technical-sounding language to imply rigor it does not have.
Research Context: Measuring Change Honestly
None of this is an argument that peptides are uninteresting or that measuring their effects is impossible. It is an argument for measuring them the way legitimate research does — and briefly describing that machinery clarifies why anecdote falls so far short. In a properly designed study of a body-composition effect, participants are randomized to compound or placebo; investigators and participants are blinded; the primary endpoint (say, percent change in fat mass by DXA, or VAT by CT) is registered before anyone is dosed; a pre-specified sample size gives the study adequate power to detect a plausible effect; and the analysis is conducted on all randomized participants, not just those who completed or improved.14
Each of these elements neutralizes a failure mode of the anecdote. Randomization balances diet, training, and baseline. Blinding removes expectation and the biased self-perception of the motivated user. The placebo arm subtracts the effect of “doing something” and of the accompanying lifestyle program. Registered endpoints prevent the after-the-fact curation that a photo gallery embodies. Objective measurement replaces the manipulable photograph with a reproducible number. Intention-to-treat analysis prevents the silent disappearance of the people for whom nothing happened. Strip any one of these away and the result becomes less trustworthy; strip all of them away and you have a before/after photo.
This is also why the compounds with the most convincing body-change stories are the ones that went through this machinery: the GLP-1 and dual/triple agonists, and tesamorelin in its narrow indication.1234 Their “before and after” is a dataset, auditable and reproducible, and it is honest about its own limits — including lean-mass loss, reversibility on discontinuation, and unproven long-term outcomes.256 That combination of a measured effect and candid limitations is the signature of real evidence. For readers who want to see how measured, durable weight change is evaluated over time rather than in a snapshot, our discussion of whether semaglutide offers a sustainable long-term solution is a useful companion.
The honest closing frame is therefore not “ignore all before/after images” but “know what class of evidence you are looking at, and hold your conclusions to that class.” For approved drugs studied in trials, realistic expectations are quantifiable and, in the case of the incretins, genuinely large — but bounded, measured, and accompanied by real trade-offs. For unapproved research peptides, the realistic expectation for the pictured cosmetic or physique effect is, in most cases, unknown, because the controlled human evidence needed to answer the question has not been generated. A wall of transformation photos does not change that; it is the appearance of evidence in the absence of the thing itself.
Frequently Asked Questions
Are peptide before/after photos ever trustworthy?
As proof that a compound caused a change, essentially never. A single pair of photos cannot control for diet, training, water, glycogen, lighting, or posing, and it is drawn from a self-selected pool of people who chose to post a success.1213 Even honest, months-apart photos cannot separate the peptide from everything else that changed. Trustworthy before/after evidence comes from randomized, placebo-controlled trials with measured endpoints, not photographs — which is exactly why approved weight-loss drugs report percentages and DXA scans rather than galleries.12
Do any peptides have real, approved before/after evidence for the body?
Yes, a few. Tesamorelin, a GHRH analog, is FDA-approved to reduce excess visceral abdominal fat in HIV-associated lipodystrophy, based on trials that measured a roughly 15% reduction in visceral fat by CT imaging versus placebo.45 The GLP-1 and dual/triple incretin agonists (semaglutide, tirzepatide; investigational retatrutide) have large randomized trials showing 15–24% mean weight loss.123 These are approved or investigational drugs with controlled data — a different category from unapproved research peptides marketed with photos.
Why can two photos look so different in a single day?
Because most of what a physique photo captures is reversible in hours. Water and sodium shifts, muscle glycogen, the post-exercise “pump,” lighting direction, posture, tan, camera angle, and clothing can each dramatically change how lean or muscular a body appears without any change in actual fat or muscle.12 Fitness professionals have demonstrated producing convincing “before” and “after” images hours apart, in the wrong order, using only these levers.12
Does a rise in IGF-1 or collagen prove a peptide is working?
No. A change in a biomarker is a mechanistic step, not a demonstrated outcome. Growth-hormone secretagogues can raise IGF-1, and some peptides increase collagen markers in a dish, but neither is the same as a controlled, measured change in fat, muscle, skin, or hair in the people using them. Substituting a biomarker for the actual body change is one of the most common ways marketing overstates a compound’s effect.
Is BPC-157 proven to transform the body or speed recovery in humans?
No. Despite its popularity, BPC-157’s human evidence base consists of only a few very small studies, and independent reviews describe it as investigational with minimal human data; it is not an approved drug and is treated by U.S. military supplement-safety authorities as an unapproved, prohibited substance found in wellness products.91011 Preclinical signals exist, but there is no controlled human before/after evidence for the physique or recovery claims typically attached to it.
How much of GLP-1 weight loss is fat versus muscle?
Both are lost, but fat preferentially. Across incretin studies, lean mass accounts for roughly 20–40% of total weight lost, while fat makes up the majority, so the proportion of lean mass to total mass usually rises.68 This is why serious trials use DXA rather than the scale, and why preserving muscle with resistance training and adequate protein is an active clinical focus.27 A photograph cannot distinguish fat loss from muscle or water loss at all.
What is a realistic timeline for genuine body change?
Slower than galleries imply. Sustainable fat loss runs roughly 0.5–1% of body weight per week, and the large GLP-1 trial results accrued over 68–72 weeks, not weeks.12 True muscle gain is a few pounds per year for trained adults. Skin and hair changes unfold over months of biological remodeling. Any before/after implying dramatic change in days is showing water, glycogen, and photography rather than durable tissue change.
What should I look for to judge a before/after critically?
Ask for the things a photo cannot fake: a control group, blinding, a pre-specified quantitative endpoint, imaging or body-composition measurement, an adequate sample, and peer-reviewed publication. Red flags include mismatched lighting or posing, a pump or tan only in the “after,” no stated timeline, no mention of diet or training, a single curated example, a nearby purchase link, and claims that outrun the compound’s actual human data.1213 If controlled evidence exists, you will not need the photos; if it does not, the photos cannot replace it.
References
- Jastreboff AM, Aronne LJ, Ahmad NN, et al. Tirzepatide Once Weekly for the Treatment of Obesity (SURMOUNT-1). N Engl J Med. 2022;387(3):205-216. PMID: 35658024. https://www.nejm.org/doi/full/10.1056/NEJMoa2206038
- Wilding JPH, Batterham RL, Calanna S, et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity (STEP 1). N Engl J Med. 2021;384(11):989-1002. PMID: 33567185. https://www.nejm.org/doi/full/10.1056/NEJMoa2032183
- Jastreboff AM, Kaplan LM, Frías JP, et al. Triple–Hormone-Receptor Agonist Retatrutide for Obesity — A Phase 2 Trial. N Engl J Med. 2023;389(6):514-526. PMID: 37366315. https://www.nejm.org/doi/full/10.1056/NEJMoa2301972
- Falutz J, Allas S, Blot K, et al. Metabolic Effects of a Growth Hormone–Releasing Factor in Patients with HIV. N Engl J Med. 2007;357(23):2359-2370. PMID: 18057338. https://www.nejm.org/doi/full/10.1056/NEJMoa072375
- EGRIFTA SV (tesamorelin for injection) U.S. Prescribing Information. Theratechnologies. FDA, 2019. https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/022505s012s013lbl.pdf
- The Influence of GLP-1 Receptor Agonists and Other Incretin Hormone Agonists on Body Composition. Nutrients (review). 2025. PMCID: PMC12733374. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12733374/
- Impact of Semaglutide on fat mass, lean mass and muscle function in patients with obesity: the SEMALEAN study. 2025. PMCID: PMC12673431. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12673431/
- The Potential of SARMs and Antimyostatin Agents in Addressing Lean Body Mass Loss From GLP-1 Agonists: A Literature Review. 2025. PMCID: PMC12311314. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12311314/
- Regeneration or Risk? A Narrative Review of BPC-157 for Musculoskeletal Healing. 2025. PMCID: PMC12446177. https://pmc.ncbi.nlm.nih.gov/articles/PMC12446177/
- Operation Supplement Safety (OPSS), U.S. Department of Defense. BPC-157: A prohibited peptide and an unapproved drug found in health and wellness products. https://www.opss.org/article/bpc-157-prohibited-peptide-and-unapproved-drug-found-health-and-wellness-products
- BPC-157: The peptide with big claims and scant evidence. STAT News (in partnership with Undark). 2026. https://www.statnews.com/2026/02/03/bpc-157-peptide-science-safety-regulatory-questions/
- The Secret Tricks Behind Misleading Images of Fitness Success. Fast Company. https://www.fastcompany.com/3021203/the-secret-tricks-behind-misleading-images-of-fitness-success
- The impact of viewing thinness and fitness transformation images on women’s body dissatisfaction, weight management intentions, and emotions: an ecological momentary assessment study. 2025. PMCID: PMC12436844. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12436844/
Educational and research-use disclaimer: This article is provided solely for scientific and educational purposes. Most research peptides discussed here are not approved by the FDA, EMA, or any comparable regulator for cosmetic, body-composition, or physique changes, and no such before/after efficacy has been demonstrated for them in controlled human studies. Approved medicines referenced (including the incretin agonists and tesamorelin) are indicated only for specific conditions and populations, carry their own risks and limitations, and should be used only under qualified medical supervision. Nothing here is medical advice or a recommendation for human use of any unapproved compound. Readers should consult qualified professionals and applicable regulations before making any decisions.