The question of “biomarker responses” associated with the Grow-H peptide blend carries a quiet assumption that is worth surfacing before we examine any data: it presumes that there is a characterized biomarker signature for Grow-H — a reproducible set of measurable changes in blood or tissue that the blend reliably produces. That assumption does not survive contact with the evidence. Grow-H is not a studied clinical entity. It is a commercial research-only pairing of two peptides — CJC-1295 without DAC (the modified growth-hormone-releasing factor fragment, Mod GRF 1–29) and ipamorelin — sold as a lyophilized powder for laboratory use. No clinical trial has ever administered this specific combination to humans and measured its biomarker output. So the honest version of the question is not “what biomarkers does Grow-H move?” but rather “what biomarkers would a competent researcher measure to test whether this GHRH-analog-plus-ghrelin-mimetic pairing does anything, and what do we actually know — from the individual components and from GH-axis physiology — about how those markers might respond?”
That reframing matters because the phrase “biomarker response” is doing a lot of marketing work in the peptide space. It sounds rigorous and quantitative, which lends borrowed credibility to compounds that have never been formally tested as sold. A biomarker is only meaningful when it has been measured, under controlled conditions, against a comparator, with attention to assay reliability and timing. Growth-hormone biology is a notoriously difficult place to do this well, because the hormone itself is secreted in pulses, its half-life is minutes, and its principal downstream marker — insulin-like growth factor 1 (IGF-1) — is measured by assays that disagree with one another substantially.9 A confident claim about “Grow-H biomarker responses” therefore has to clear a high bar that, at present, no one has cleared.
This article is written for researchers and educated readers who want an honest map rather than a sales sheet. We will define what Grow-H actually contains and how the two components are supposed to work together; specify the candidate biomarkers a real study would track (GH pulse characteristics, IGF-1, IGFBP-3, and metabolic markers such as glucose and insulin sensitivity); examine what the human data on the individual ingredients suggest those markers might do; confront the critical and widely ignored distinction between the long-acting CJC-1295-with-DAC that was actually studied in humans and the no-DAC fragment that Grow-H contains; work through why GH-axis biomarkers are so hard to measure reliably; and lay out the evidence gap, the regulatory status, and the handling context. Throughout, the guiding principle is restraint: Grow-H is not an approved therapy for anything, and nothing here should be read as suggesting it treats, prevents, or cures any condition, or that any biomarker change — even if real — translates into a clinical benefit.
What Grow-H Actually Is
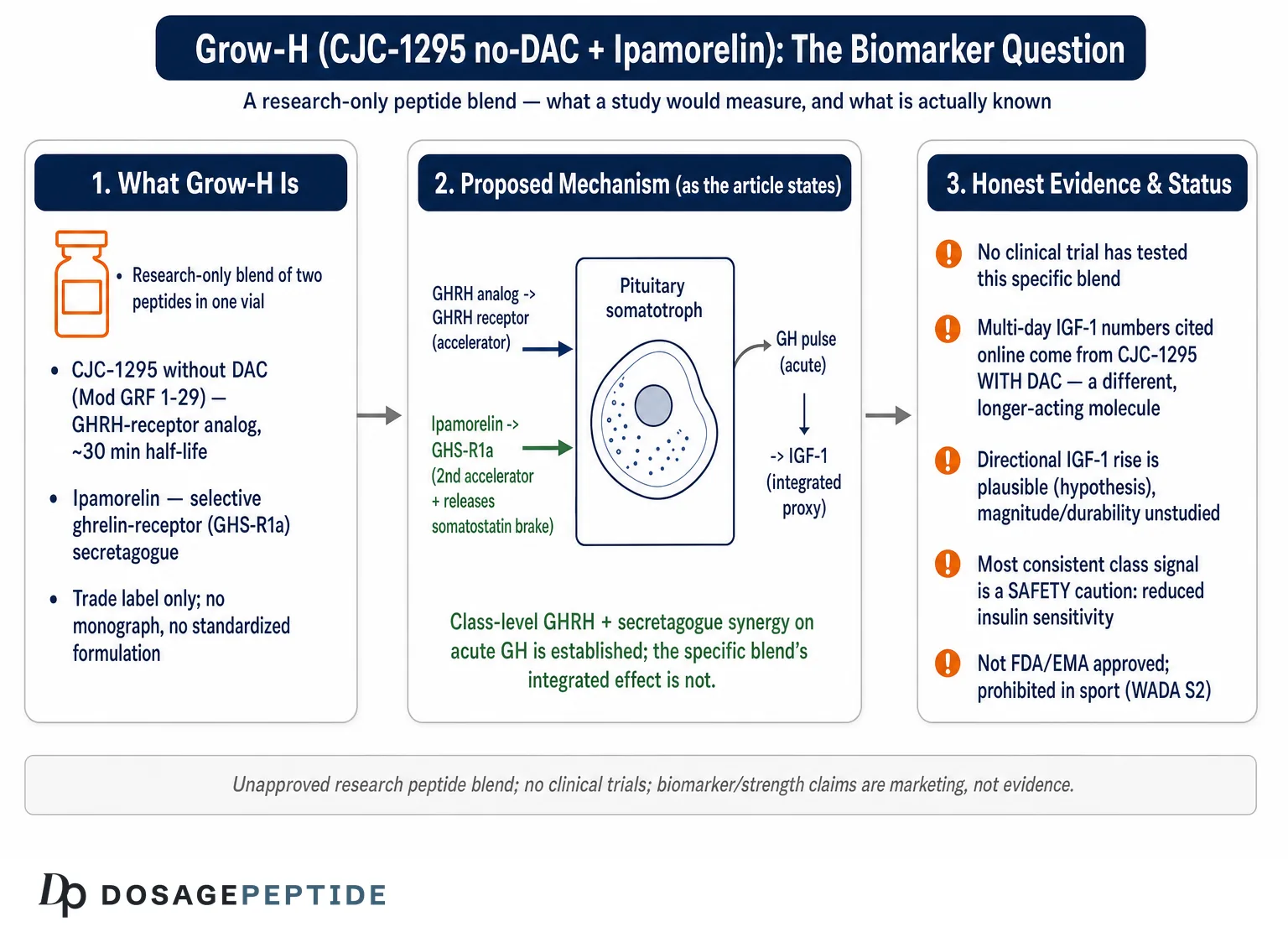
Grow-H, as sold by research-chemical vendors, is a two-peptide blend, most commonly supplied as a 10 mg vial containing 5 mg of CJC-1295 without DAC and 5 mg of ipamorelin. The name is a trade label, not a pharmacological designation; there is no monograph, no standardized formulation, and no regulatory identity behind it. Understanding the biomarker question requires understanding each half of the pairing, because they act on different receptors and, in principle, contribute differently to any measurable output.
CJC-1295 without DAC is the more confusingly named of the two. The label “CJC-1295” is frequently used loosely. In the peer-reviewed literature, CJC-1295 refers specifically to a growth-hormone-releasing hormone (GHRH) analog engineered with a drug-affinity complex (DAC) — a maleimidopropionic acid group that lets the peptide bind covalently to circulating albumin, extending its half-life to roughly six to eight days.1 The “without DAC” version sold in blends like Grow-H is a different molecule pharmacokinetically: it is the tetrasubstituted GHRH(1–29) fragment, often called Modified GRF 1–29 or CJC-1295 no-DAC, which carries the same stabilizing amino-acid substitutions that resist enzymatic degradation but lacks the albumin-binding complex. Without the DAC, its circulating half-life is on the order of about 30 minutes rather than days. This distinction is not pedantic; as we will see, it is the single most important reason why the human IGF-1 data usually cited for “CJC-1295” cannot be transferred wholesale to the compound in Grow-H.
Mechanistically, the no-DAC fragment binds the GHRH receptor on pituitary somatotrophs, reproducing the physiological signal that the hypothalamus normally sends to stimulate growth-hormone synthesis and release. It is a short, sharp GHRH-like pulse-promoter rather than a long-acting one. For readers interested in the closely related native-mimicking GHRH analog, the site’s discussion of sermorelin’s role in stimulating natural growth hormone covers the same receptor family and the same underlying logic of amplifying the body’s own secretory machinery rather than supplying exogenous hormone.
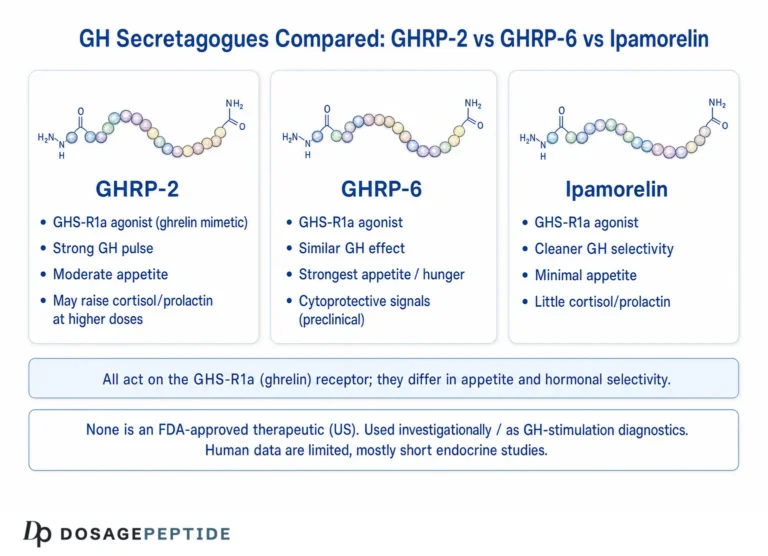
Ipamorelin is the second component and comes from an entirely different pharmacological lineage. It is a synthetic pentapeptide (Aib-His-D-2-Nal-D-Phe-Lys-NH2) and was described by Raun and colleagues in 1998 as “the first selective growth hormone secretagogue.”3 It acts not on the GHRH receptor but on the growth-hormone secretagogue receptor (GHS-R1a) — the same receptor targeted by the endogenous hormone ghrelin, which Kojima and colleagues identified in 1999 as a growth-hormone-releasing acylated peptide from the stomach.5 Ipamorelin’s defining feature is its selectivity: in the original characterization it released GH with potency comparable to earlier GH-releasing peptides but, unlike them, did not meaningfully elevate adrenocorticotropic hormone (ACTH), cortisol, or prolactin even at doses more than 200-fold above its GH-releasing threshold.3 That clean profile is why it is favored over older secretagogues such as GHRP-6 and GHRP-2 in research pairings, and the site’s account of the studies demonstrating ipamorelin’s precision in targeting the GHS-R1a receptor details that selectivity in depth.
The rationale for combining the two is not arbitrary. A GHRH analog and a ghrelin-receptor agonist act through separate, complementary pathways on the same target cells, and the pharmacology literature has long held that combined GHRH-plus-GHRP administration produces a larger GH response than either agent alone. We will examine that synergy and its actual evidential standing shortly. For now, the essential point is that Grow-H is a hypothesis in a vial: a plausible pairing assembled from two reasonably characterized peptides, sold under a name that implies a settled identity it does not possess. Whatever biomarker story exists must be built from the components and from GH-axis physiology, because the blend itself has never been formally studied. Readers wanting the companion discussion of whether this same blend delivers functional outcomes can see the sibling analysis of whether clinical insights show the Grow-H blend truly boosts strength and repair, which tackles the downstream performance claims that lie beyond the biomarker question addressed here.
What “Biomarker Response” Means for a Growth-Hormone-Axis Compound
Before asking whether Grow-H moves biomarkers, we need to be precise about which biomarkers are even relevant and what each one actually tells us. In the context of a GHRH-analog-plus-secretagogue blend, “biomarker” is not one thing; it is a layered hierarchy of measurements, each with different reliability, timing, and interpretive weight.
The most proximal biomarker is growth hormone itself. GH is the direct output of the pituitary somatotrophs that both components are meant to stimulate. But GH is a treacherous biomarker. It is secreted in discrete pulses, chiefly at night, with very low concentrations between pulses and a plasma half-life measured in minutes. A single random GH measurement is nearly uninterpretable, because a “normal” person can have an undetectable GH level ten minutes after a large pulse. To characterize a GH response properly, researchers must sample blood frequently — every 10 to 20 minutes over many hours — and then compute derived parameters: peak (maximum) GH, trough (interpulse) GH, mean GH over the sampling window, area under the curve, and pulse frequency and amplitude. This is exactly the methodology that Ionescu and Frohman used to show that a long-acting GHRH analog raised mean and trough GH while preserving the pulsatile pattern rather than flattening it into a continuous elevation.2 The practical implication is that any honest “GH biomarker response” for Grow-H would require this kind of intensive sampling protocol, which no published study of the blend has performed.
The most useful and most commonly cited biomarker is IGF-1 (insulin-like growth factor 1). GH acts largely by inducing hepatic and peripheral production of IGF-1, which mediates many of GH’s anabolic and metabolic effects. Because IGF-1 has a much longer half-life than GH and does not pulse the way GH does, it provides a stable, integrated readout of GH secretory activity over roughly the preceding day — a time-averaged proxy for “how much GH signaling has been occurring.” This stability is why IGF-1 is the workhorse biomarker in GH-axis pharmacology and why the CJC-1295-with-DAC trials reported IGF-1 as their headline endpoint.1 It is also why any claim about a peptide “raising IGF-1” deserves scrutiny about magnitude, duration, assay, and comparator.
A closely related marker is IGFBP-3 (insulin-like growth factor binding protein 3), the principal carrier protein for circulating IGF-1. IGFBP-3 is itself GH-dependent and, measured together with IGF-1, provides a more complete picture of GH-axis activity than either alone; the combination is regarded as superior to a single analyte for evaluating GH status.8 A rigorous Grow-H biomarker study would report IGFBP-3 alongside IGF-1, and ideally the IGF-1/IGFBP-3 molar ratio, which reflects free (bioavailable) IGF-1.
Beyond the GH–IGF-1 axis proper sit the metabolic and safety biomarkers that matter for interpreting whether stimulating GH does anything benign or otherwise. Chief among these is glucose metabolism: GH is a counter-regulatory, diabetogenic hormone that tends to reduce insulin sensitivity, so fasting glucose, fasting insulin, and derived indices such as HOMA-IR are essential biomarkers in any GH-secretagogue evaluation. The review literature on growth-hormone secretagogues flags precisely this concern — a signal toward decreased insulin sensitivity and increased blood glucose — as one of the few consistent findings across the class.6 Additional markers a thorough study might track include cortisol and prolactin (to confirm the selectivity ipamorelin is prized for), and, over longer horizons, lipid parameters and body-composition surrogates.
The key conceptual point is that these biomarkers are not interchangeable and do not carry equal weight. A change in GH is proximal but noisy; a change in IGF-1 is more stable but slower and assay-dependent; a change in a metabolic marker speaks to safety as much as efficacy. When a vendor asserts that Grow-H produces “biomarker responses,” the honest questions are: which marker, measured how, changed by how much, for how long, relative to what, and does that change mean anything for health? For a compound that has never been studied as sold, all of those questions currently return the same answer — unknown.
The Mechanistic Rationale: Why Pair a GHRH Analog With a Ghrelin Mimetic?
The strongest part of the Grow-H story is its mechanistic logic, and it is worth giving that logic a fair hearing before returning to the evidence gap. The pairing of a GHRH analog with a GH-releasing peptide is not a modern invention of the research-chemical market; it rests on genuinely foundational endocrinology.
The two peptides engage the somatotroph through distinct, cooperating mechanisms. The GHRH analog (the no-DAC CJC-1295 fragment) binds the GHRH receptor, a G-protein-coupled receptor that raises intracellular cyclic AMP and drives both the synthesis and the release of stored GH. Ipamorelin, acting at GHS-R1a, works through a different second-messenger route (phospholipase C and intracellular calcium mobilization) and, critically, also appears to suppress somatostatin — the hypothalamic hormone that normally brakes GH release.5 So one component pushes the accelerator (GHRH drive) while the other both pushes a second accelerator and releases the brake (ghrelin-receptor stimulation plus somatostatin withdrawal). Because these are separate levers, their combined effect on GH secretion can exceed the sum of the individual effects.
This synergy is not speculative in the general case. Bowers and colleagues demonstrated in 1990 that a GH-releasing peptide stimulated GH release in normal men and acted synergistically with GHRH, producing GH peaks substantially larger than either agent alone.4 That classic finding — replicated in various forms across the GHRP literature — is the pharmacological foundation for every GHRH-plus-secretagogue pairing sold today, Grow-H included. The observation that endogenous GHRH is required for the full GH response to a GHRP, and that the two classes are merely additive in isolated pituitary cells but strongly synergistic in the intact animal, points to a mechanism that depends on the coordinated state of the whole hypothalamic-pituitary unit rather than on a single receptor.4
Here is where honesty has to intrude on an attractive narrative, though. The synergy demonstrated by Bowers and successors was shown for specific GHRH and GHRP molecules, at specific doses, with GH (not IGF-1, and not any downstream biomarker) as the readout, in acute experimental settings. It establishes that pairing the two classes can amplify an acute GH pulse. It does not establish that the particular combination in Grow-H, at whatever doses a given user reconstitutes, produces a defined, reproducible, and durable change in IGF-1 or any other integrated biomarker — still less that such a change confers benefit. The leap from “GHRH and GHRP synergize on acute GH release” to “Grow-H reliably shifts a person’s biomarker profile in a meaningful way” skips over dose, duration, tolerance, formulation, and the entire question of whether transient GH pulses translate into sustained IGF-1 elevation. The mechanism makes the hypothesis plausible. It does not make the biomarker claim proven. For a broader view of how ipamorelin sits among alternative secretagogues used in these pairings, the site’s comparison of how research compares ipamorelin with other growth-hormone peptides is a useful adjunct.
The DAC Problem: Why the Human IGF-1 Data Do Not Transfer
If there is one section of this article that most separates an honest analysis from a marketing summary, it is this one. The confident IGF-1 numbers that circulate under the heading “CJC-1295” come almost entirely from studies of CJC-1295 with DAC — a molecule that Grow-H does not contain.
Consider the flagship human study. Teichman and colleagues conducted two randomized, double-blind, placebo-controlled ascending-dose trials of CJC-1295 (the DAC version) in healthy adults. A single subcutaneous injection produced dose-dependent increases in mean plasma GH of roughly 2- to 10-fold sustained for six days or more, and increases in mean IGF-1 of about 1.5- to 3-fold sustained for nine to eleven days; with multiple doses, mean IGF-1 remained above baseline for up to 28 days, and the estimated half-life of the compound was 5.8 to 8.1 days.1 Ionescu and Frohman then showed, again with the DAC version, that this continuous GHRH-receptor stimulation raised trough and mean GH and increased IGF-1 by roughly 45% while preserving pulsatile GH secretion.2
Every one of those striking, durable IGF-1 effects depends on the drug-affinity complex. The DAC is what tethers the peptide to albumin and keeps it circulating for days, producing the sustained receptor stimulation that drives IGF-1 up and holds it there. Grow-H contains CJC-1295 without DAC — the Mod GRF 1–29 fragment with a half-life of roughly half an hour. That short-acting fragment delivers a brief GHRH pulse and is cleared quickly. It has not been the subject of a comparable published, controlled human trial reporting multi-day IGF-1 elevation, and there is no pharmacological reason to expect a 30-minute-half-life peptide to reproduce the multi-week IGF-1 kinetics of a 6-to-8-day-half-life peptide. The two are related in sequence and receptor target but are pharmacokinetically different animals.
This is why so much online material about “CJC-1295 IGF-1 responses” is quietly misleading when applied to blends. It imports the impressive DAC-version numbers and attaches them to the no-DAC fragment that products actually contain, as if the half-life difference were a footnote rather than the whole mechanism behind those numbers. An honest biomarker analysis of Grow-H must set the Teichman and Ionescu–Frohman IGF-1 figures aside as evidence about a different molecule, useful for understanding what sustained GHRH-receptor stimulation can do in principle, but not as a prediction of what the no-DAC fragment in Grow-H will do to a person’s IGF-1. The table below makes the contrast explicit.
| Property | CJC-1295 with DAC (studied) | CJC-1295 no-DAC / Mod GRF 1–29 (in Grow-H) |
|---|---|---|
| Albumin binding | Yes (drug-affinity complex) | No |
| Approximate half-life | ~6–8 days1 | ~30 minutes |
| Human IGF-1 data | 1.5–3× rise sustained days–weeks1 | No comparable controlled human trial |
| GH pattern | Elevated mean/trough GH, pulsatility preserved2 | Brief acute GH pulse; integrated effect unstudied |
| Intended research role | Long-acting sustained GHRH drive | Short, physiologic-style GHRH pulse |
None of this means the no-DAC fragment does nothing. A short GHRH pulse can certainly release GH acutely, and paired with ipamorelin it may produce a larger acute GH pulse than either alone, consistent with the synergy literature.4 The point is narrower and more important: the durable, multi-day IGF-1 biomarker signature that people cite as the reason to expect a “Grow-H biomarker response” belongs to a molecule Grow-H does not contain, and cannot be assumed for the one it does.
IGF-1 as the Central Biomarker: What We Can and Cannot Say
Given that IGF-1 is the biomarker most likely to be invoked for Grow-H, it deserves its own careful accounting. What can we responsibly say about how IGF-1 might respond to a no-DAC GHRH fragment plus ipamorelin?
First, the directional plausibility is real. Both components stimulate GH release, and GH drives IGF-1 production; secretagogues as a class have been shown to raise IGF-1 to varying degrees. The Sigalos and Pastuszak review of GH secretagogues notes that these agents can increase fat-free mass and produce measurable endocrine effects, while emphasizing that few long-term, rigorously controlled studies exist and that safety and efficacy across populations remain under-characterized.6 A related review of secretagogues in body-composition management similarly treats IGF-1 elevation as a mechanistically expected but incompletely quantified consequence of this class.7 So a modest IGF-1 rise from a GHRH-plus-secretagogue pairing is biologically reasonable to hypothesize.
Second, the magnitude and durability are genuinely uncertain for the no-DAC blend. Whether a series of short GH pulses from a 30-minute-half-life fragment plus a selective secretagogue is sufficient to shift the time-averaged IGF-1 concentration — and by how much, and for how long — has not been established in a controlled human study of this combination. The integrated IGF-1 response to pulsatile versus sustained GH stimulation is not a solved question, and it is precisely the kind of thing that the DAC-versus-no-DAC distinction makes non-trivial. It is entirely possible that the no-DAC blend produces a smaller and more transient IGF-1 movement than the DAC-version numbers would suggest, or that tolerance and receptor desensitization blunt the response over repeated exposure. We do not know, because the study has not been done.
Third, even a documented IGF-1 rise would be a biomarker change, not a health outcome. This is the interpretive trap that catches most peptide discussions. IGF-1 is a proxy. An increase in a proxy is not evidence of benefit unless it has been linked, in the relevant population and context, to an outcome that matters — and higher IGF-1 is not unambiguously good. IGF-1 sits in the middle of a complicated risk landscape; both low and high IGF-1 have been associated in epidemiology with adverse outcomes, and elevating a mitogenic growth factor is not a free action. The correct posture toward a hypothetical Grow-H IGF-1 signal is therefore doubly cautious: uncertain that it occurs at a meaningful magnitude, and unclear that it would be beneficial if it did.
The tesamorelin literature offers a useful, sobering comparison here. Tesamorelin is an approved GHRH analog whose IGF-1-raising effect has been characterized in rigorous trials, and the pathways linking its receptor stimulation to sustained IGF-1 elevation are relatively well mapped, as the site’s discussion of the molecular pathways linking tesamorelin stimulation to sustained IGF-1 elevation describes. The instructive point is the contrast: tesamorelin’s IGF-1 biomarker behavior is known because it was studied in controlled trials with defined dosing and endpoints. Grow-H’s is not, and no amount of mechanistic analogy can substitute for that missing evidence.
Secondary and Safety Biomarkers: Glucose, Insulin Sensitivity, Cortisol, Prolactin
An analysis that stopped at IGF-1 would miss half the reason to measure biomarkers in the first place. Biomarkers are not only efficacy signals; they are safety instruments, and for a GH-axis compound the metabolic panel is where the most consistent class-level signal actually lives.
Growth hormone is counter-regulatory to insulin. Elevating GH secretion tends, over time, to reduce insulin sensitivity and raise blood glucose — a well-established property of the hormone that carries directly to agents that stimulate it. This is arguably the most reproducible biomarker signal in the secretagogue literature: the Sigalos and Pastuszak review explicitly flags concern for increases in blood glucose owing to decreases in insulin sensitivity as a recurring finding across GH secretagogues, even as it notes these agents are generally well tolerated in the short studies available.6 In other words, if one had to bet on which biomarker Grow-H is most likely to move in a consistent direction, a modest adverse shift in glucose handling is a more defensible prediction than a dramatic IGF-1 gain. That asymmetry — the most reliable biomarker response may be a safety signal rather than a benefit — is exactly the sort of thing marketing framings omit. A responsible research protocol would therefore track fasting glucose, fasting insulin, and HOMA-IR as core endpoints, not afterthoughts.
The second cluster of safety biomarkers concerns the selectivity that makes ipamorelin attractive. Older GH-releasing peptides raised ACTH, cortisol, and prolactin along with GH; ipamorelin’s original characterization emphasized that it did not meaningfully elevate these hormones even at very high doses.3 A rigorous Grow-H study would measure cortisol and prolactin specifically to confirm that the blend inherits ipamorelin’s clean profile in practice and at the doses used. This is not merely box-checking: prolactin and cortisol elevations would signal off-target stimulation with its own clinical implications, and the assumption that the blend behaves as cleanly as the isolated pentapeptide is exactly the kind of thing that should be verified rather than presumed.
A third consideration is that ipamorelin acts on the ghrelin receptor, and ghrelin is not solely a GH secretagogue — it is an orexigenic (appetite-stimulating) and metabolically active hormone.5 Depending on dose and exposure, ghrelin-receptor stimulation can influence appetite and, potentially, downstream metabolic markers independent of the GH axis. This means a full biomarker picture for Grow-H is not confined to the GH–IGF-1 pathway; it spans glucose regulation, appetite-related signaling, and the classic pituitary safety hormones. The table below summarizes the candidate biomarkers a competent study would track and the current state of evidence for each in the context of this specific blend.
| Candidate biomarker | What it indexes | Evidence status for the Grow-H blend |
|---|---|---|
| GH (peak/trough/mean, pulse amplitude) | Direct pituitary output; proximal target of both peptides | Acute GH release plausible from synergy data on the classes;4 no blend-specific frequent-sampling study |
| IGF-1 | Integrated GH signaling over ~1 day; workhorse efficacy proxy | Directionally plausible; magnitude/durability unstudied for no-DAC blend; DAC-version data do not transfer1 |
| IGFBP-3 | GH-dependent IGF-1 carrier; refines GH-status estimate | Would be expected to move with IGF-1; not measured for the blend8 |
| Fasting glucose / insulin / HOMA-IR | Insulin sensitivity; key safety signal for GH stimulation | Class-level concern for reduced insulin sensitivity;6 unquantified for blend |
| Cortisol / prolactin | Off-target pituitary stimulation (selectivity check) | Ipamorelin selective in isolation;3 blend-level confirmation absent |
Why Growth-Hormone Biomarkers Are So Hard to Measure Reliably
Even setting aside the absence of Grow-H-specific trials, there is a deeper reason to distrust confident biomarker claims in this space: GH-axis biomarkers are genuinely difficult to measure and compare, and the difficulty is systematic, not incidental. A researcher who understands these measurement problems reads “raises IGF-1 by X%” very differently from a consumer who does not.
The first problem is GH pulsatility and half-life, already noted. Because GH is secreted in bursts and cleared in minutes, any GH measurement is a snapshot of a rapidly moving target. Two blood draws minutes apart can differ enormously. This is why serious GH pharmacology uses frequent-sampling protocols and derived parameters rather than single measurements, and why any “GH response” asserted for Grow-H without such a protocol should be treated as anecdote.2
The second problem is IGF-1 assay discordance, and it is worse than most people assume. IGF-1 is measured by immunoassays that are not standardized across platforms, and the disagreement between them is substantial. A 2023 comparison of IGF-1 measured on four different analytical platforms found wide variation between methods, with poor overall agreement and systematic differences that grew larger at higher IGF-1 values — precisely the range where a supposed treatment effect would be claimed.9 This means the same blood sample can yield materially different IGF-1 numbers depending on which lab and which analyzer processed it. A claimed “IGF-1 increase” that is not anchored to a single, consistent, well-characterized assay, ideally traceable to the WHO international standard, is scientifically soft.
The third problem is the absence of a shared reference framework. Recognizing these issues, the endocrine field has issued formal consensus guidance on standardizing and evaluating GH and IGF-1 assays — establishing common standards, reporting practices, and validation expectations precisely because uncontrolled assay variability had been undermining comparability across studies and clinics.8 The existence of such a consensus is itself a tell: if measuring IGF-1 reliably were easy, no one would need to convene experts to standardize it. Against that backdrop, a research-chemical blend with no defined dose, no controlled trial, and no specified assay is about as far from a reliable biomarker readout as one can get.
These measurement realities compound the evidence gap rather than sitting beside it. Even if someone reconstituted Grow-H, injected it, and measured their IGF-1 before and after, the result would be confounded by assay choice, sampling timing, diurnal and nutritional variation, and the absence of a placebo comparator or blinding. An uncontrolled n-of-1 measurement on a non-standardized assay is not a biomarker response in any rigorous sense; it is a number that feels like evidence. Distinguishing the two is the core competence this section is meant to build. For readers who want the underlying vocabulary of these axis measurements, the site’s peptide research glossary defines the relevant terms in one place.
Direct Evidence for the Grow-H Blend: The Gap
This section is deliberately short, because the honest answer is short. There is no published clinical trial, and no controlled preclinical study, that administered the Grow-H combination — CJC-1295 without DAC plus ipamorelin at defined doses — and characterized its biomarker responses. A search of the literature returns no such combination study measuring GH pulse parameters, IGF-1, IGFBP-3, or metabolic markers for this specific pairing sold under this name or any equivalent.
What exists instead is a scaffold of adjacent evidence from which the blend’s behavior is inferred: human data on CJC-1295 with DAC (a different, longer-acting molecule);12 the original characterization of ipamorelin’s GH-releasing potency and selectivity, largely in animal and in vitro systems;3 the classical demonstration that GHRH and GHRP classes synergize on acute GH release in humans;4 and review-level summaries of GH secretagogues as a class that stress how thin the long-term controlled evidence remains.67 Each piece is real and relevant. None of them is a study of Grow-H, and stacking them together does not manufacture one. The synergy data tell us the acute GH pulse may be amplified; they do not tell us the integrated IGF-1 response, the durability, the dose–response, the safety-marker profile, or the reproducibility of the specific blend.
It is worth being explicit about what a genuine biomarker study of Grow-H would require, because the contrast with what exists is stark. It would need defined, verified doses of each component; a controlled design with placebo and, ideally, arms testing each peptide alone versus the combination (to demonstrate that the synergy actually manifests in this pairing); frequent GH sampling to capture pulse parameters; IGF-1 and IGFBP-3 measured on a single standardized, WHO-traceable assay at defined time points; metabolic and pituitary safety markers; and a duration long enough to detect tolerance or desensitization. Until something resembling that is done, every statement about “Grow-H biomarker responses” is a hypothesis dressed in the vocabulary of data. The correct scientific description of the current state is not “weak evidence” but “no direct evidence,” supported by a plausible mechanism and by transferable-with-caveats data on the components.
Interpreting Vendor Biomarker Claims Critically
Because the honest evidence base is an empty set at the level of the blend, the marketplace fills the vacuum with mechanism-flavored assertions. Learning to parse those claims is a practical skill, so it is worth walking through the common patterns and why each falls short of what it implies.
“Clinically studied ingredients.” This phrasing is technically defensible and practically misleading. CJC-1295 (with DAC) and ipamorelin have indeed been studied; the blend has not, and the no-DAC fragment is not the studied CJC-1295. “Studied ingredients” is not “studied product,” and the difference is where all the uncertainty lives — dose, combination, formulation, and pharmacokinetics.
“Raises IGF-1 by [large percentage].” When a specific IGF-1 figure appears, it almost always traces back to the DAC-version human trials.1 As established above, those numbers belong to a molecule with a multi-day half-life and cannot be attributed to the 30-minute no-DAC fragment in the blend. A percentage borrowed from the wrong molecule is not a biomarker response; it is a citation error with a decimal point.
“Synergistic GH release.” This one has a real basis in the Bowers synergy literature,4 but it describes acute GH pulses in controlled experiments with defined molecules and doses, not a durable, integrated biomarker shift from an arbitrarily dosed research blend. The word “synergistic” is doing legitimate mechanistic work and illegitimate rhetorical work simultaneously.
“Optimizes” or “restores” the GH axis. These are outcome claims wearing biomarker clothing. “Optimize” presupposes a defined target state and evidence that the compound moves people toward it; neither exists here. This is the language of wellness marketing, not endocrinology.
The through-line is that each claim takes a real, narrow piece of science and stretches it across a gap it cannot span — from a different molecule, or an acute experiment, or an isolated ingredient, to a durable, beneficial, reproducible effect of the specific product. Recognizing the stretch is the whole game. A useful habit is to ask, for any biomarker claim: is this about the blend, at a defined dose, in a controlled comparison, measured properly, with a magnitude and duration attached? For Grow-H, the answer to at least one of those questions is always no.
Handling and Research Context
Because Grow-H is encountered as a lyophilized (freeze-dried) two-peptide powder, a brief, strictly educational note on laboratory handling is warranted — with the emphasis that this is standard research-peptide practice, not a usage recommendation, and that Grow-H is not an approved therapeutic and its biomarker effects are unestablished.
Lyophilized peptides are generally reconstituted with sterile or bacteriostatic water for laboratory purposes. The diluent is directed slowly against the inside wall of the vial rather than sprayed onto the powder, and the vial is swirled gently rather than shaken, because vigorous agitation can shear peptide bonds and denature the material. The chosen diluent volume simply sets the concentration: a fixed mass of peptide in a larger volume yields a lower concentration per unit volume, the arithmetic underlying any reconstitution chart. General walkthroughs of this process appear on the site’s peptide reconstitution guide, and the broader dosage index catalogs how these compounds are organized for educational reference.
Two handling considerations are specific to a blend like this. First, because Grow-H combines two peptides in one vial, their relative amounts are fixed by the manufacturer; a researcher cannot independently vary the GHRH-analog and secretagogue doses without a separate single-component preparation. This constrains exactly the kind of component-versus-combination comparison that a real biomarker study would require. Second, blends purchased through research-chemical channels carry the usual and serious quality caveats: purity, correct identity of each component, absence of the DAC where “no-DAC” is claimed, endotoxin, and accurate labeling are all real variables that vary by source and that no amount of careful reconstitution can fix. From a biomarker standpoint, product-quality uncertainty is itself a confounder: an unexpected biomarker reading could reflect an impurity, a mislabeled component, or a DAC-containing peptide sold as no-DAC, rather than the intended pharmacology.
The overarching point is that meticulous handling preserves whatever activity the molecules possess but creates no evidence. A perfectly reconstituted, high-purity vial of Grow-H is still a compound with no controlled biomarker data. Good technique keeps the experiment clean; it does not tell you what the experiment would show, because the experiment has not been run.
Regulatory Status and Prohibition in Sport
The regulatory picture reinforces, from a different direction, how far Grow-H sits from established medicine — and it has direct implications for anyone who imagines biomarker monitoring as part of a sanctioned protocol.
No therapeutic approval. Neither Grow-H as a blend nor its individual components (CJC-1295 in either form, ipamorelin) is approved by the U.S. Food and Drug Administration, the European Medicines Agency, or comparable regulators as a drug for any indication. The blend is sold explicitly for laboratory research use only, not for human consumption. There is no approved use to which any biomarker claim could attach.
U.S. compounding review. Both components were examined by the FDA’s Pharmacy Compounding Advisory Committee in 2024 as part of the review of peptide substances nominated for the Section 503A bulk drug substances list. Ipamorelin was among the substances reviewed in October 2024, with the FDA recommending against inclusion and the committee voting against adding it to the 503A bulks list.10 CJC-1295 and its DAC-modified variants were assessed at the subsequent December 2024 meeting within the same framework of continued regulatory caution about compounded peptide products.11 The clear signal is that, in the United States, these peptides do not have a settled, sanctioned place even within the compounding pathway — the venue where clinician-supervised biomarker monitoring might otherwise occur.
Prohibition in sport. This is unambiguous and consequential. The World Anti-Doping Agency’s Prohibited List places GHRH and its analogues (explicitly including CJC-1295) and growth-hormone secretagogues and their mimetics (explicitly including ipamorelin) under section S2, prohibited at all times.12 Both halves of Grow-H are therefore banned substances for any athlete subject to anti-doping rules, and recent list language extends the prohibition to substances with similar chemical structure or biological effect, closing analog loopholes.12 For an athlete, the most predictable “biomarker” consequence of Grow-H is not a favorable IGF-1 shift but a positive doping test and a rule violation — a point that anti-doping science actually does measure and enforce, in contrast to the unmeasured benefit claims.
The regulatory synthesis is straightforward. Grow-H occupies the unregulated research-chemical margin: no approved therapeutic identity, no sanctioned compounding pathway, and outright prohibition in sport. Any legitimate investigation of its biomarker effects belongs in formal preclinical and clinical research under proper oversight, not in informal self-experimentation whose results — for all the measurement reasons above — would be uninterpretable anyway.
Frequently Asked Questions
Does Grow-H reliably raise IGF-1?
There is no controlled human study of the Grow-H blend measuring IGF-1, so the honest answer is that we do not know its magnitude or durability. A directional rise is mechanistically plausible because both components stimulate GH, which drives IGF-1.6 But the impressive multi-day IGF-1 increases often cited come from studies of CJC-1295 with DAC, a longer-acting molecule that Grow-H does not contain;1 those numbers cannot be transferred to the ~30-minute-half-life no-DAC fragment in the blend. Any specific percentage attached to Grow-H’s IGF-1 effect should be treated as borrowed from the wrong molecule until a study of the actual blend exists.
What is the difference between CJC-1295 with and without DAC, and why does it matter for biomarkers?
The DAC (drug-affinity complex) tethers the peptide to albumin, extending its half-life to roughly six to eight days and producing sustained GH and IGF-1 elevation for days to weeks.1 The no-DAC version in Grow-H (Modified GRF 1–29) lacks that complex and is cleared in about half an hour, delivering a brief GHRH pulse instead. Because the durable IGF-1 biomarker signature depends entirely on the DAC-driven long half-life, the human IGF-1 data for “CJC-1295” describe a different molecule and do not predict the no-DAC blend’s biomarker behavior.
Which biomarkers would a proper study of Grow-H actually measure?
At minimum: GH via frequent sampling (peak, trough, mean, pulse amplitude); IGF-1 and IGFBP-3 on a single standardized, WHO-traceable assay;8 and metabolic safety markers — fasting glucose, insulin, and HOMA-IR — because GH stimulation tends to reduce insulin sensitivity.6 Cortisol and prolactin would confirm that the blend preserves ipamorelin’s selectivity.3 A single random IGF-1 draw is not an adequate biomarker readout for a GH-axis compound.
Is the GHRH-plus-secretagogue synergy real?
Yes, in the general sense. Bowers and colleagues showed in 1990 that a GH-releasing peptide and GHRH act synergistically on acute GH release in normal men, producing larger GH peaks than either alone.4 This is the mechanistic rationale for pairing the two classes. However, that synergy was demonstrated for specific molecules and doses using acute GH as the readout; it does not establish a durable, integrated IGF-1 or downstream biomarker response for the Grow-H blend specifically.
Could a measured IGF-1 increase mean Grow-H is “working”?
Not on its own. IGF-1 is a proxy, and a change in a proxy is not a health outcome unless it has been linked to a meaningful endpoint in the relevant context. Higher IGF-1 is not unambiguously beneficial — it is a mitogenic growth factor with a complex risk profile. A biomarker moving is a starting point for investigation, not proof of benefit, and treating it as an outcome is one of the most common errors in this field.
Why can’t I just measure my own IGF-1 before and after?
An uncontrolled n-of-1 measurement is confounded by several things at once: IGF-1 assays disagree substantially across platforms, with differences that grow at higher values;9 there is no placebo or blinding; and diurnal, nutritional, and sampling-timing variation adds noise. The result is a number that feels like evidence but cannot distinguish a true drug effect from assay drift or normal fluctuation. Reliable biomarker readouts require standardized assays and controlled designs.8
Has the Grow-H blend itself ever been studied in a trial?
No. There is no published clinical or controlled preclinical study of CJC-1295 no-DAC plus ipamorelin at defined doses characterizing its biomarker responses. The available evidence is adjacent — DAC-version CJC-1295 human data,12 ipamorelin’s isolated characterization,3 class-level synergy,4 and secretagogue reviews67 — none of which is a study of the blend as sold.
Is Grow-H legal or approved, and is it allowed in sport?
It is not approved as a drug by the FDA, EMA, or comparable regulators, and is sold for research use only. Both components were reviewed and not recommended for the FDA’s 503A compounding bulks list in 2024.1011 Both are prohibited at all times in sport under WADA’s section S2 (GHRH analogues and GH secretagogues), so use by any tested athlete is an anti-doping rule violation.12
What is the single most reliable biomarker signal to expect?
Paradoxically, the most defensible prediction is a safety signal rather than a benefit: because GH stimulation tends to reduce insulin sensitivity, a modest adverse shift in glucose handling is the class-level effect flagged most consistently in the secretagogue literature.6 That the most reproducible expected biomarker response is a metabolic caution — not a dramatic IGF-1 gain — captures the honest state of knowledge about this blend.
References
- Teichman SL, Neale A, Lawrence B, Gagnon C, Castaigne JP, Frohman LA. Prolonged stimulation of growth hormone (GH) and insulin-like growth factor I secretion by CJC-1295, a long-acting analog of GH-releasing hormone, in healthy adults. J Clin Endocrinol Metab. 2006;91(3):799-805. PMID: 16352683. https://pubmed.ncbi.nlm.nih.gov/16352683/
- Ionescu M, Frohman LA. Pulsatile secretion of growth hormone (GH) persists during continuous stimulation by CJC-1295, a long-acting GH-releasing hormone analog. J Clin Endocrinol Metab. 2006;91(12):4792-4797. PMID: 17018654. https://pubmed.ncbi.nlm.nih.gov/17018654/
- Raun K, Hansen BS, Johansen NL, Thøgersen H, Madsen K, Ankersen M, Andersen PH. Ipamorelin, the first selective growth hormone secretagogue. Eur J Endocrinol. 1998;139(5):552-561. PMID: 9849822. https://pubmed.ncbi.nlm.nih.gov/9849822/
- Bowers CY, Reynolds GA, Durham D, Barrera CM, Pezzoli SS, Thorner MO. Growth hormone (GH)-releasing peptide stimulates GH release in normal men and acts synergistically with GH-releasing hormone. J Clin Endocrinol Metab. 1990;70(4):975-982. PMID: 2108187. https://pubmed.ncbi.nlm.nih.gov/2108187/
- Kojima M, Hosoda H, Date Y, Nakazato M, Matsuo H, Kangawa K. Ghrelin is a growth-hormone-releasing acylated peptide from stomach. Nature. 1999;402(6762):656-660. PMID: 10604470. https://pubmed.ncbi.nlm.nih.gov/10604470/
- Sigalos JT, Pastuszak AW. The safety and efficacy of growth hormone secretagogues. Sex Med Rev. 2018;6(1):45-53. PMID: 28400207. https://pubmed.ncbi.nlm.nih.gov/28400207/
- Sinha DK, Balasubramanian A, Tatem AJ, Rivera-Mirabal J, Yu J, Kovac J, Pastuszak AW, Lipshultz LI. Beyond the androgen receptor: the role of growth hormone secretagogues in the modern management of body composition in hypogonadal males. Transl Androl Urol. 2020;9(Suppl 2):S149-S159. PMID: 32257855. PMCID: PMC7108996. https://pubmed.ncbi.nlm.nih.gov/32257855/
- Clemmons DR. Consensus statement on the standardization and evaluation of growth hormone and insulin-like growth factor assays. Clin Chem. 2011;57(4):555-559. PMID: 21285256. https://pubmed.ncbi.nlm.nih.gov/21285256/
- Lee JKY, Cradic K, Singh RJ, Jones J, Li J. Discordance of insulin-like growth factor-1 results and interpretation on four different platforms. Clin Chim Acta. 2023;539:130-133. PMID: 36528048. https://pubmed.ncbi.nlm.nih.gov/36528048/
- U.S. Food and Drug Administration. October 29, 2024: Meeting of the Pharmacy Compounding Advisory Committee — review of ipamorelin and other bulk drug substances nominated for the Section 503A bulk drug substances list (committee voted against inclusion). https://www.fda.gov/advisory-committees/advisory-committee-calendar/october-29-2024-meeting-pharmacy-compounding-advisory-committee-10292024
- U.S. Food and Drug Administration. December 4, 2024: Meeting of the Pharmacy Compounding Advisory Committee — review of CJC-1295 and CJC-1295 DAC related bulk drug substances for the Section 503A bulk drug substances list. https://www.fda.gov/advisory-committees/advisory-committee-calendar/december-4-2024-meeting-pharmacy-compounding-advisory-committee-12042024
- World Anti-Doping Agency. The Prohibited List — Section S2: Peptide Hormones, Growth Factors, Related Substances and Mimetics (GHRH analogues including CJC-1295; GH secretagogues including ipamorelin). https://www.wada-ama.org/en/prohibited-list
Educational and research-use disclaimer: This article is provided solely for scientific and educational purposes. Grow-H is a research-only peptide blend (CJC-1295 without DAC plus ipamorelin) and is not approved by the FDA, EMA, or any comparable regulator for the treatment, cure, or prevention of any disease, nor for human consumption. No controlled study has characterized the biomarker responses of this specific blend, and no biomarker change — even if real — has been shown to confer a clinical benefit. Both components are prohibited in sport at all times by WADA. Nothing here is medical advice or a recommendation for human use. Any legitimate investigation of this compound should occur within properly authorized preclinical or clinical research under appropriate oversight. Readers should consult qualified professionals and applicable regulations before making any decisions.