GHRP-2 (growth hormone-releasing peptide-2, also written as pralmorelin) is one of the earliest synthetic growth hormone secretagogues — a small peptide engineered to make the pituitary gland release its own stored growth hormone. The central research question this article addresses is deceptively simple: what is GHRP-2, how does it actually work at the receptor level, and what does the human evidence genuinely establish versus what remains preclinical or purely diagnostic? Because the GHRP-2 peptide sits at the crossroads of a fascinating scientific story — a synthetic molecule that predicted the existence of a natural hormone no one had yet found — separating the well-documented pharmacology from the marketing folklore matters more here than almost anywhere else in peptide science.
This is a research and educational reference. GHRP-2 is not an FDA-approved therapeutic drug in the United States. Nothing below is a protocol, a recommendation for human use, or a claim that GHRP-2 treats, cures, or prevents any condition. It is an attempt to describe, honestly and with real citations, what the published literature says.
What Is GHRP-2? A Working Definition
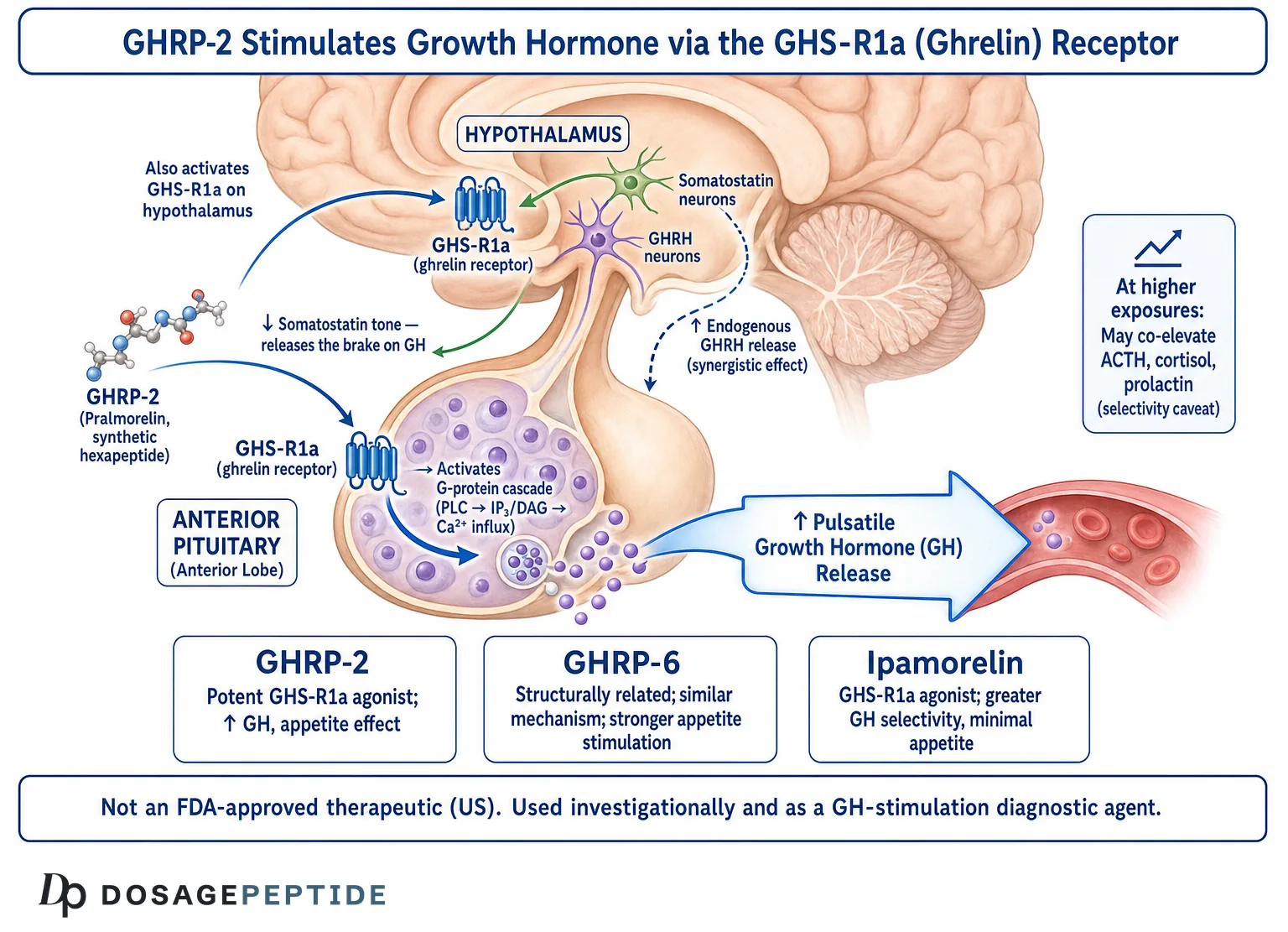
GHRP-2 is a synthetic hexapeptide — a chain of six amino acids — whose sequence is D-Ala-D-2-Nal-Ala-Trp-D-Phe-Lys-NH2. It belongs to a class of molecules called growth hormone secretagogues (GHSs): compounds that provoke the release of growth hormone (GH) without being growth hormone themselves. In pharmacological terms it is best described as a ghrelin mimetic or ghrelin-receptor agonist, because it binds and activates the same receptor that the stomach hormone ghrelin uses — the growth hormone secretagogue receptor type 1a (GHS-R1a).[1]
Three properties define GHRP-2 and separate it from other GH-modulating strategies:
- It is a secretagogue, not a hormone. It does not replace or supplement GH. It signals the somatotroph cells of the anterior pituitary to secrete GH that is already synthesized and stored.
- It works through the ghrelin/GHS-R1a pathway, a mechanism entirely distinct from growth hormone-releasing hormone (GHRH) and its synthetic analogs.
- It amplifies the body’s pulsatile GH rhythm rather than flooding the system with a flat, continuous signal — at least in the short-term endocrine studies that make up most of the human data.
The compound was developed in the laboratory of Cyril Y. Bowers, whose decades of work on GH-releasing peptides created the entire field. Understanding GHRP-2 without understanding Bowers’ pharmacology is like reading the last chapter of a book first. For readers who want the practical companion pages, the compound-specific reference material lives on the GHRP-2 5 mg vial dosage protocol reference and the corresponding GHRP-2 10 mg vial reference; this article is the conceptual foundation beneath them.
What GHRP-2 Is Not
Clearing up common confusions early prevents most of the misinformation that surrounds this compound:
- It is not recombinant human growth hormone (somatropin). HGH is the 191-amino-acid hormone itself; GHRP-2 is a six-amino-acid trigger.
- It is not a GHRH analog. Sermorelin, CJC-1295, and tesamorelin mimic GHRH and act on the GHRH receptor. GHRP-2 acts on a different receptor entirely. The distinction is explored in depth on the reference comparing CJC-1295 with and without DAC.
- It is not an anabolic steroid, an androgen, or a SARM. It has no direct action on androgen or estrogen receptors.
- It is not, in the United States, an approved medicine. Its status is investigational and, in certain countries, diagnostic — not therapeutic.
Research Context: Where GHRP-2 Came From
The GHRP story begins in the 1970s and 1980s with Cyril Bowers and colleagues, who noticed that certain enkephalin-derived peptides could release growth hormone from pituitary tissue through a mechanism that did not fit GHRH. Enkephalins are opioid peptides, and the earliest GH-releasing peptides were structurally related to met-enkephalin — yet the GH-releasing effect was not blocked by opioid antagonists, which told the investigators they had stumbled onto an entirely separate signaling system.[2]
In 1984 the Bowers group published the defining early work on GHRP-6, a hexapeptide that acted directly on the pituitary to release GH with striking specificity.[3] GHRP-6 became the prototype. GHRP-2 followed as a second-generation analog, engineered to be more potent on a molar basis and to release GH more efficiently. Over the following decade Bowers and collaborators mapped the pharmacology of these peptides in remarkable detail, showing across species that they released GH through a receptor that was neither the GHRH receptor nor any opioid receptor — a receptor whose natural ligand was, at the time, completely unknown.[4]
The “Orphan Receptor” Problem
By the mid-1990s the GHRPs presented endocrinology with a genuine puzzle. They clearly worked. They released GH powerfully and synergized with GHRH in a way no other agent did. But there was no known natural molecule that used their receptor. This is what pharmacologists call an orphan receptor — a receptor with no identified endogenous ligand. The existence of a receptor implies the existence of something the body makes to activate it. The GHRPs were, in effect, a synthetic key that fit a lock nobody could find the natural key for.
In 1996 the lock itself was cloned. Howard and colleagues at Merck identified the growth hormone secretagogue receptor, GHS-R, expressed in the pituitary and hypothalamus, and showed that the GHRPs and the non-peptide secretagogue MK-677 acted through it.[1] The natural key remained missing for three more years — a gap that turns out to be central to the GHRP-2 story and is discussed in its own section below.
Mechanisms Studied: How GHRP-2 Works at the GHS-R1a Receptor
The GHRP-2 mechanism is now understood in considerable molecular detail, and it is genuinely elegant. GHRP-2 binds the ghrelin receptor GHS-R1a, a G-protein-coupled receptor (GPCR) of the class A family. Activation triggers a signaling cascade that ends in growth hormone release from the somatotrophs of the anterior pituitary.
The Signaling Cascade Step by Step
- Receptor binding. GHRP-2 occupies the orthosteric binding pocket of GHS-R1a on both pituitary somatotrophs and hypothalamic neurons.
- G-protein coupling. GHS-R1a couples primarily to Gq/11, activating phospholipase C (PLC).
- Second messengers. PLC generates inositol trisphosphate (IP3) and diacylglycerol (DAG), which mobilize intracellular calcium and activate protein kinase C.
- Calcium influx and GH exocytosis. The rise in intracellular calcium drives the fusion of GH-containing secretory vesicles with the cell membrane, releasing growth hormone into the circulation.
Critically, GHRP-2 does not act at the pituitary alone. Its full effect requires an intact hypothalamus, because it works through two complementary central actions as well as its direct pituitary action.
The Dual Central Mechanism
Bowers’ work — later confirmed once ghrelin was discovered — established that GHRPs release GH through more than one node:
- Direct pituitary stimulation. GHS-R1a on somatotrophs directly evokes GH release.
- Stimulation of hypothalamic GHRH neurons. GHRP-2 appears to increase the release of endogenous GHRH, so part of its effect is actually mediated through the GHRH pathway.
- Functional antagonism of somatostatin. Somatostatin is the brake on GH release. GHRPs blunt somatostatin’s inhibitory tone, effectively releasing the brake at the same time they press the accelerator.
This three-part mechanism explains the single most reproducible finding in the entire GHRP literature: the synergy with GHRH. When GHRP and GHRH are given together, the GH released is far greater than the sum of each given alone. Bowers, Reynolds, Thorner and colleagues documented this synergy in normal men as early as 1990, and it has been replicated many times since.[5] Two different receptors, two different mechanisms, one amplified output — this is why combination approaches pairing a GHRP-type secretagogue with a GHRH analog attract so much research interest.
The Structure Behind the Function
GHRP-2’s six-amino-acid sequence is not arbitrary; it is the product of deliberate structure-activity optimization by the Bowers group and their collaborators. Two features of the design are worth understanding because they explain the molecule’s behavior:
- D-amino acids confer stability. The sequence includes D-configuration amino acids (D-Ala, D-2-Nal, D-Phe) rather than the L-forms that make up natural proteins. Peptidase enzymes in blood and tissue are evolved to cleave L-amino-acid bonds; the D-substitutions make GHRP-2 substantially more resistant to enzymatic degradation than a natural peptide of the same length would be. This is why a six-amino-acid molecule can survive long enough to produce a measurable GH pulse.
- Aromatic bulk drives receptor affinity. The 2-naphthylalanine (2-Nal) and phenylalanine residues provide the aromatic, hydrophobic bulk that fits the GHS-R1a binding pocket. The refinement from GHRP-6 to GHRP-2 essentially tuned these residues for greater potency.
This is an underappreciated point: GHRP-2 is a rationally engineered molecule, and its every property — potency, half-life, receptor selectivity — traces back to specific chemical choices made to solve specific problems.
Constitutive Activity of GHS-R1a
One further mechanistic subtlety distinguishes the ghrelin-receptor system. GHS-R1a exhibits unusually high constitutive activity — it signals to a degree even in the absence of any ligand. This basal tone is thought to contribute to the setting of GH pulse amplitude and possibly to appetite regulation. GHRP-2, as a full agonist, drives the receptor above this baseline, but the existence of constitutive activity is part of why the ghrelin/GHS-R1a axis behaves as a rheostat on GH output rather than a simple on/off switch. It is one more reason the effects of a ghrelin mimetic like GHRP-2 are best understood as modulating an existing rhythm rather than imposing a new one.
Why “Pulsatile” Matters
Growth hormone is not secreted continuously. In healthy physiology it is released in discrete bursts, or pulses, mostly during slow-wave sleep, with near-undetectable levels between pulses. This pulsatility is biologically important: many downstream effects of GH depend on the pattern of exposure, not just the total amount. A key theoretical appeal of secretagogues like GHRP-2 is that they amplify existing pulses and preserve the negative-feedback loops that switch GH off — because the pituitary still ultimately controls the output. This stands in contrast to injecting recombinant GH, which imposes an external, non-pulsatile profile and suppresses the body’s own axis. It is important to frame this as a mechanistic rationale observed in short pharmacology studies, not a demonstrated long-term clinical advantage.
How Does GHRP-2 Differ From a GHRH Analog?
This is the single most useful distinction for anyone trying to understand where GHRP-2 fits, and it is worth a dedicated section because the two classes are constantly conflated. Both raise GH. They do so through completely different doors.
| Feature | GHRP-2 (a GHRP / ghrelin mimetic) | GHRH analogs (sermorelin, CJC-1295, tesamorelin) |
|---|---|---|
| Receptor | GHS-R1a (ghrelin receptor) | GHRH receptor (GHRH-R) |
| Natural ligand mimicked | Ghrelin | Growth hormone-releasing hormone |
| Primary action on somatostatin | Functionally opposes somatostatin tone | Does not directly oppose somatostatin |
| Effect on appetite | Can stimulate appetite (ghrelin pathway) | Minimal direct appetite effect |
| Synergy | Strongly synergistic with GHRH analogs | Strongly synergistic with GHRPs |
| Other pituitary hormones | Can co-elevate ACTH/cortisol and prolactin at higher doses | Comparatively GH-selective |
The practical upshot: GHRP-2 and a GHRH analog are complementary, not interchangeable. Each removes a different constraint on GH release. This is precisely why research and anecdote so often pair a GHRP-class peptide with a GHRH-class peptide — a logic examined for the GHRH side on the CJC-1295 DAC versus no-DAC reference. For a glossary of every term in this table, the peptide research glossary defines GHS-R1a, somatostatin, GHRH, pulsatility and the rest.
The Ghrelin Connection: A Synthetic Peptide That Predicted a Natural Hormone
This is the part of the GHRP-2 story that belongs in textbooks. For fifteen years, the GHRPs worked through a receptor whose natural ligand was unknown. The synthetic peptide came first; the hormone it imitated was discovered afterward, precisely because researchers went looking for the endogenous molecule that must exist to justify the orphan receptor.
In 1999 Kojima, Kangawa and colleagues isolated that molecule from the stomach and named it ghrelin — a growth-hormone-releasing acylated peptide.[6] Ghrelin turned out to be the natural ligand of GHS-R1a, the very receptor the GHRPs had been activating all along. Bowers later summarized this beautifully in a paper whose title says it all: an unnatural growth hormone-releasing peptide begat the discovery of natural ghrelin.[7]
Why This History Is More Than Trivia
The ghrelin connection is not just a good story; it explains GHRP-2’s entire pharmacological profile:
- The appetite effect. Ghrelin is the body’s principal hunger hormone. Because GHRP-2 mimics ghrelin, it can stimulate appetite — a property studied specifically as a potential aid in wasting conditions, and one that clearly separates GHRP-2 from GH-selective secretagogues.
- Effects beyond GH. Ghrelin receptors are found in the gut, pancreas, cardiovascular system and brain. GHRP-2’s activity at GHS-R1a therefore predicts a range of non-GH effects seen in animal and early human studies.
- The physiological plausibility. Because GHRP-2 works through a real, endogenous signaling system rather than an artificial one, its short-term endocrine effects are consistent and reproducible — which is exactly why it became useful as a diagnostic tool.
The broader neuroendocrine control of GH — the interplay of GHRH, somatostatin and ghrelin/GHS-R1a — has been reviewed comprehensively and provides the physiological backdrop for everything GHRP-2 does.[8]
A Subtle but Important Caveat: Acylation
There is a chemical wrinkle that makes the GHRP-2/ghrelin relationship even more interesting. Natural ghrelin is only active at GHS-R1a when it carries a specific fatty-acid modification — an octanoyl (C8) group attached to its third amino acid by the enzyme ghrelin O-acyltransferase (GOAT). Unacylated ghrelin, which circulates in larger amounts, does not activate GHS-R1a in the same way. GHRP-2 needs no such modification; as a synthetic full agonist it activates the receptor directly. This means GHRP-2 bypasses a whole layer of endogenous regulation — the acylation step that the body uses to control how much active ghrelin is available — which is part of why a synthetic secretagogue can produce a more reliable, dose-controllable GH pulse than the natural system’s fluctuating acyl-ghrelin levels would.
What GHRP-2 Taught Endocrinology
It is worth stepping back to appreciate the scientific legacy. GHRP-2 and its siblings did something rare in pharmacology: a class of synthetic drugs revealed the existence of an entire, previously unknown hormonal system. Before the GHRPs, textbooks described GH regulation as a two-hormone system — GHRH pushing and somatostatin restraining. The GHRPs forced the recognition of a third arm, the ghrelin/GHS-R1a axis, which links GH regulation to energy balance, appetite and the gut. That conceptual expansion — from a two-factor to a three-factor model of GH control — is arguably GHRP-2’s most durable contribution, independent of any therapeutic question. Comprehensive reviews of ghrelin biology trace this lineage directly back to the GH-releasing peptides.[12]
GHRP-2 as a Diagnostic GH-Stimulation Agent
Here the evidence tier becomes concrete and, importantly, honest. GHRP-2’s most clearly established human application is not as a therapy at all — it is as a diagnostic provocative agent for growth hormone deficiency.
Diagnosing GH deficiency requires a stimulation test: because random GH levels are usually near zero between pulses, clinicians administer an agent that provokes a GH surge and then measure whether the pituitary can mount an adequate response. Traditional agents include insulin-induced hypoglycemia (the classic but unpleasant and risky gold standard), arginine, glucagon and GHRH. Because GHRP-2 is a potent, rapid and relatively well-tolerated GH secretagogue, it was investigated as a stimulation agent — often combined with GHRH to exploit the synergy described earlier.
Regulatory Status: Precision Matters
This is where careful framing is essential, because the regulatory status differs sharply by country:
- In Japan, GHRP-2 (pralmorelin) has been approved and marketed specifically as a diagnostic agent for adult and pediatric growth hormone deficiency — a single-injection GH-stimulation test. Diagnostic studies supporting this application have been published in the endocrinology literature.[9]
- In the United States, GHRP-2 is not an FDA-approved drug for any indication — not therapeutic and not diagnostic. Its status here is investigational / research-chemical.
The distinction between “approved as a diagnostic test in one country” and “approved as a treatment” is enormous and routinely blurred in marketing copy. A diagnostic agent is given once (or occasionally) to measure pituitary function. That is a completely different regulatory and evidentiary category from a chronic therapeutic intended to change a health outcome over months or years. GHRP-2 has genuine, published support for the former in specific jurisdictions. It does not have equivalent long-term outcome-trial support for the latter anywhere.
Why GHRP-2 Makes a Good Diagnostic Probe
Several of the very properties described earlier make GHRP-2 well suited to a stimulation test, and understanding this reinforces the mechanism:
- Speed. The GH response is fast, allowing a short test window rather than the prolonged sampling some other agents require.
- Potency and reliability. A robust, reproducible GH surge in subjects with intact pituitary reserve makes the test discriminating — a blunted response points toward pituitary or hypothalamic insufficiency.
- Tolerability relative to insulin tolerance testing. The insulin-hypoglycemia gold standard is effective but carries real risk and discomfort; a peptide secretagogue avoids deliberate hypoglycemia.
- Compatibility with GHRH. Because of the synergy, a GHRH + GHRP-2 combined test amplifies the signal and improves the separation between deficient and sufficient responses.
In a stimulation test, the logic is diagnostic rather than therapeutic: a single provocation, a peak GH measurement, and an interpretation against an established cut-off. Nothing about this diagnostic validity implies that repeated, chronic administration produces a beneficial clinical outcome — a leap that marketing frequently makes and that the evidence does not license.
The Cortisol, Prolactin, and ACTH Co-Elevation Question
One of the most important and least-discussed features of GHRP-2 — and a genuine differentiator from newer, more selective secretagogues — is its effect on pituitary hormones other than GH. This is not a fringe concern; it is well documented in the pharmacology literature and directly relevant to how the compound is understood.
GHRPs, including GHRP-2, can stimulate the release of adrenocorticotropic hormone (ACTH) and consequently cortisol, and can also raise prolactin, particularly at higher doses. This activity on the corticotroph and lactotroph axes reflects the distribution and signaling of GHS-R1a beyond the pure GH pathway and has been characterized in reviews of GHRP pharmacology.[2]
Why Co-Elevation Matters Scientifically
- It defines selectivity. The degree to which a secretagogue raises only GH, versus also nudging ACTH/cortisol and prolactin, is a central axis on which these compounds are compared. GHRP-2 is potent but comparatively less selective than the next-generation peptides designed specifically to avoid this.
- It shapes the research interpretation. Any study of GHRP-2 must account for the possibility that observed effects reflect not just GH but concurrent shifts in cortisol and prolactin.
- It is the reason ipamorelin was developed. The search for a secretagogue with the GH-releasing power of the GHRPs but without the ACTH/cortisol and prolactin baggage led directly to the design of more selective molecules — the subject of the next section.
Framed honestly, this is a case where a compound’s breadth of action is simultaneously an interesting pharmacological feature and a limitation for anyone seeking a clean, GH-only signal.
GHRP-2 vs GHRP-6 vs Ipamorelin: How Do the Secretagogues Compare?
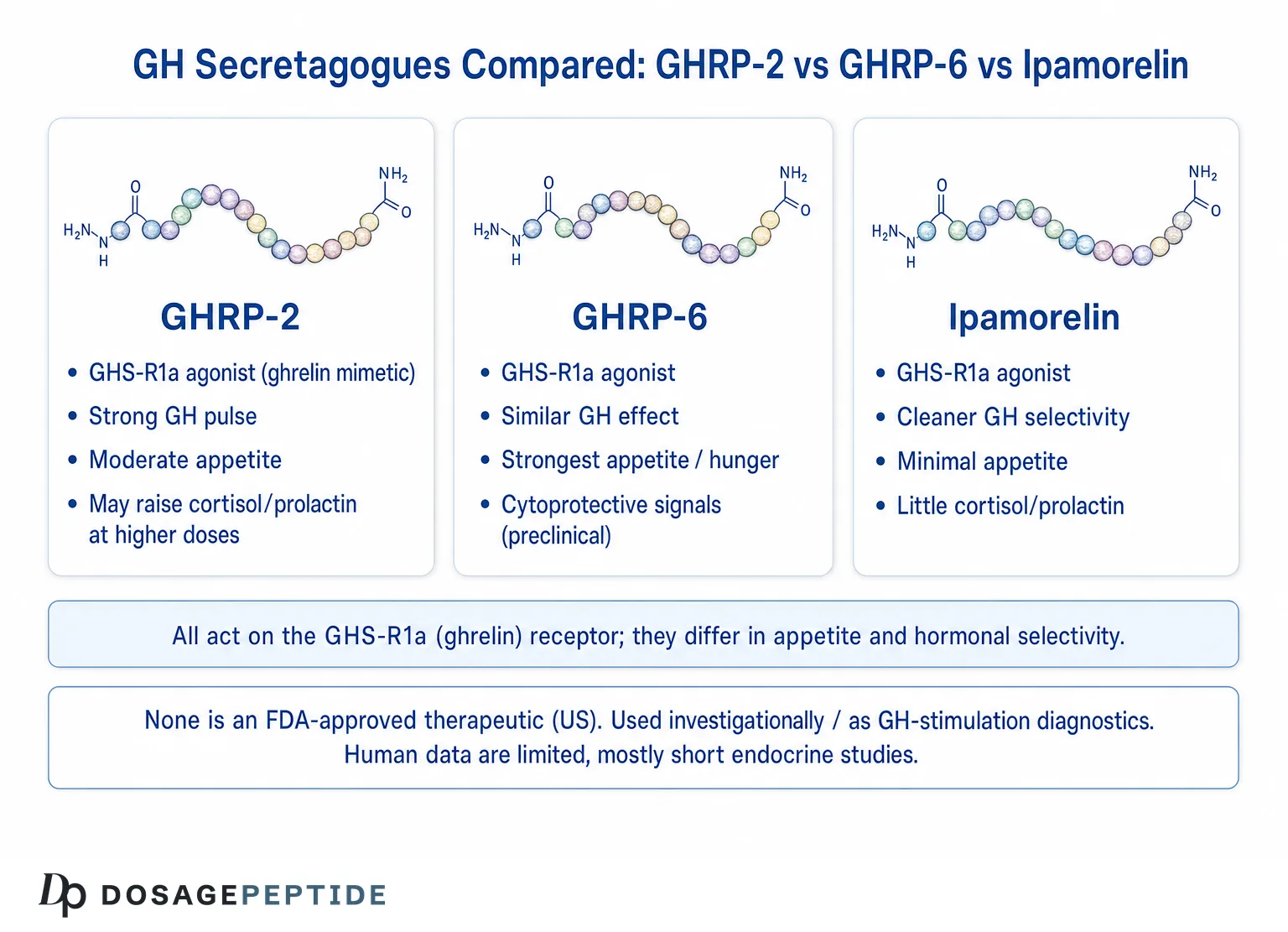
The GHRP-2 vs ipamorelin comparison is probably the most-searched question about this compound, and it deserves a rigorous, non-hyped answer. All three peptides are ghrelin-receptor agonists that release GH through GHS-R1a. They differ in potency, appetite effect, and — most importantly — hormonal selectivity.
| Property | GHRP-6 | GHRP-2 | Ipamorelin |
|---|---|---|---|
| Class | First-gen GHRP | Second-gen GHRP | Selective GHS-R1a agonist |
| Receptor | GHS-R1a | GHS-R1a | GHS-R1a |
| Relative GH potency | Lower | Higher than GHRP-6 | Comparable GH release, high selectivity |
| Appetite / ghrelin-like hunger | Pronounced | Moderate | Minimal |
| ACTH / cortisol effect | Present | Present, dose-dependent | Negligible in studies |
| Prolactin effect | Present | Present at higher doses | Negligible in studies |
| Defining trait | The original prototype | Potency | Selectivity |
The Ipamorelin Difference
Ipamorelin was introduced in 1998 by Raun and colleagues as, in their words, the first selective GH secretagogue — a peptide that released GH with a potency comparable to the GHRPs but without the accompanying rise in ACTH and cortisol that characterizes GHRP-6 and GHRP-2.[10] This selectivity is the entire reason ipamorelin exists and the single most important distinction in the whole comparison. Where GHRP-2 offers potency at the cost of a broader hormonal footprint, ipamorelin trades a slice of the ghrelin-like breadth for a cleaner, GH-focused signal.
Neither is “better” in the abstract — they answer different research questions. If the appetite-stimulating, ghrelin-mimetic breadth is the point of interest, GHRP-2 is the more representative ghrelin mimetic. If a GH-selective probe with minimal cortisol/prolactin confounding is wanted, ipamorelin is the reason the selective class was created. The mechanism of that selectivity is examined directly on the reference explaining how ipamorelin achieves targeted GH secretion without off-target hormonal activation, and the broader ipamorelin overview lives on the what-is-ipamorelin mechanism reference.
GHRP-6 in One Line
GHRP-6 is the historical prototype — the molecule that opened the field — but it is the least potent of the three and produces the most pronounced hunger response, which is why GHRP-2 and later ipamorelin were developed as refinements. In the arc from GHRP-6 to GHRP-2 to ipamorelin, one can read the field’s evolving priorities: first proof of concept, then potency, then selectivity.
Current Evidence Level: What the Human Data Actually Show
This section is the honest heart of the article. It is easy to find breathless claims about GHRP-2; it is harder to state precisely what the peer-reviewed human evidence does and does not establish. Here is that accounting, organized by evidence tier.
What Is Well Established (Short-Term Endocrine Pharmacology)
- GHRP-2 acutely releases growth hormone in humans. This is robust, reproducible, and dose-related. It is the foundation of its diagnostic use.[5]
- It synergizes with GHRH. Co-administration produces GH release greater than either agent alone — one of the most replicated findings in the field.[5]
- It acts through GHS-R1a / the ghrelin pathway. Confirmed by receptor cloning and the subsequent identification of ghrelin.[1]
- It functions as a diagnostic GH-stimulation agent, approved as such for GH-deficiency testing in Japan.[9]
- It can co-elevate ACTH, cortisol and prolactin, distinguishing it from selective secretagogues.[2]
What Is Investigational or Early-Stage
- Appetite stimulation and use in wasting conditions. Studied on the strength of the ghrelin-mimetic mechanism, but not established as an approved therapy.
- Effects in older adults on the GH/IGF-1 axis. Short-term studies show the axis can be stimulated, but this is a long way from demonstrated functional or clinical benefit. The broader lesson from the oral secretagogue MK-677, which raised IGF-1 durably yet did not translate into unambiguous functional gains in key trials, is a cautionary reference point for the whole class.
- Pediatric short-stature exploration. Early studies examined GHRP-2 delivery in children, but these were small and mechanistic rather than definitive outcome trials.
What Is Preclinical or Animal-Only
- Cardiovascular, gastrointestinal and neuroprotective effects attributed to ghrelin-receptor signaling come largely from animal and in-vitro work and should not be described as human clinical findings.
- Body-composition and “anti-aging” claims circulating in non-scientific sources are not supported by long-term human outcome trials for GHRP-2 specifically.
The Evidence-Tier Summary Table
| Claim | Evidence tier | Honest status |
|---|---|---|
| Acute GH release in humans | Human pharmacology | Well established |
| Synergy with GHRH | Human pharmacology | Well established, replicated |
| Diagnostic GH-stimulation testing | Approved (Japan) | Established for diagnosis, not therapy |
| ACTH/cortisol/prolactin co-elevation | Human pharmacology | Documented |
| Appetite stimulation | Mechanism + early human | Investigational |
| Long-term body-composition benefit | — | Not established in outcome trials |
| “Anti-aging” / longevity | Marketing | Not supported |
| Cardio/neuro/GI protection | Preclinical/animal | Not demonstrated in humans for GHRP-2 |
Bottom line: GHRP-2 is exceptionally well characterized as a short-term endocrine pharmacology agent and a diagnostic tool. It is not supported by the kind of long-term, randomized, outcome-based clinical trials that would justify therapeutic claims — and in the United States it is not an approved medicine at all.
What Happens Downstream? The GH/IGF-1 Axis
Understanding GHRP-2 fully means following the signal past the pituitary. Releasing growth hormone is only the first step in a cascade, and the downstream biology is where both the theoretical appeal and the interpretive difficulty of secretagogues live.
When GH enters the circulation, a major fraction of its effects are mediated by insulin-like growth factor 1 (IGF-1), produced mainly by the liver in response to GH. IGF-1 is the more stable, longer-lived signal, and it is what many downstream tissues actually respond to. This creates a two-tier system: GH is the pulsatile, short-lived messenger; IGF-1 is the slower, integrated readout. It also creates a feedback loop — IGF-1 and GH both feed back on the hypothalamus and pituitary to restrain further GH release, principally by promoting somatostatin tone.
Why the Feedback Loop Is Central to the GHRP-2 Rationale
This feedback architecture is exactly why secretagogue proponents argue the approach is more “physiological” than exogenous GH. Because GHRP-2 works by asking the pituitary to release GH, the downstream rise in IGF-1 can still feed back and modulate the system. In principle this preserves a natural ceiling that injected recombinant GH bypasses. It is essential, however, to label this correctly: this is a mechanistic argument supported by short-term endocrine data, not a demonstrated long-term safety or efficacy advantage. The feedback loop that theoretically protects against runaway GH also means the body may adapt to chronic secretagogue exposure in ways that short studies cannot capture — a genuine open question rather than a settled reassurance.
The IGF-1 Surrogate Trap
A recurring error in how GHRP-2 is discussed deserves explicit naming. Studies of secretagogues frequently report that GH and IGF-1 levels rose. Readers — and marketers — then treat a rise in IGF-1 as if it were the benefit itself. It is not. IGF-1 is a surrogate marker: a laboratory value that stands in for a hoped-for outcome. Whether raising IGF-1 with a secretagogue produces the outcomes people actually care about — changes in body composition, physical function, recovery, healthspan — is a separate question that requires long-term outcome trials GHRP-2 does not have. The broader secretagogue field offers a sobering precedent: the orally active GHS ibutamoren (MK-677) durably raised IGF-1 in trials, yet did not reliably convert that biochemical change into the functional benefits investigators hoped for. Elevated IGF-1 is a promise, not a proof.
Pharmacokinetics and Physical Properties Studied
Understanding why GHRP-2 is administered the way it is in research settings requires a few pharmacokinetic facts, all framed here as reference material about the molecule rather than instructions.
Half-Life and Route
GHRP-2 is a small peptide and, like most peptides, is not orally bioavailable in any efficient way because it is degraded in the gastrointestinal tract — which is why parenteral (typically subcutaneous) administration dominates the research literature, and why intranasal delivery was explored in some early studies. Its plasma half-life is short, on the order of tens of minutes, consistent with its role as a pulse-amplifying secretagogue rather than a long-acting agent. The GH response it evokes is rapid, typically peaking within roughly 15–30 minutes of administration in stimulation studies — the very property that makes it convenient as a diagnostic provocative agent.
Stability and Handling in Research Settings
As reference information for laboratory handling (not a use instruction): lyophilized peptides of this class are generally stored cold and protected from light and moisture, reconstituted with bacteriostatic or sterile water for research purposes, and kept refrigerated once in solution because peptides in aqueous solution degrade over time. Compound-specific reconstitution and concentration reference figures — again, as research documentation — are laid out on the GHRP-2 5 mg vial reference page. None of this should be read as a recommendation to administer GHRP-2 to a person.
The short half-life also shapes how the compound behaves conceptually. A pulse-amplifying secretagogue with a brief window of action is, by design, a transient nudge to the system rather than a sustained override — which is consistent with the diagnostic use case, where a single sharp provocation is exactly what a stimulation test needs. It is precisely because the effect is short and self-limiting that the pituitary’s own feedback machinery remains in charge, and it is that feature, more than any other, that supporters cite when they describe secretagogues as working “with” rather than “over” the endocrine axis. Whether that theoretical elegance translates into any durable real-world benefit remains, as this article has stressed throughout, an open and unproven question.
Limitations: What the Research Does Not Establish
A responsible reference article is defined as much by what it refuses to claim as by what it asserts. The limitations of the GHRP-2 evidence base are substantial and must be stated plainly.
Limitations of the Evidence
- Short study durations. The overwhelming majority of human GHRP-2 data come from acute or short-term endocrine studies — single injections, stimulation tests, days-to-weeks pharmacology. Long-term data measuring hard clinical outcomes are essentially absent.
- Surrogate endpoints, not outcomes. Studies typically measure GH and IGF-1 levels — surrogate markers — rather than function, morbidity, or quality of life. A rise in a hormone level is not the same as a demonstrated benefit.
- Small sample sizes. Many foundational studies involved small numbers of subjects, appropriate for mechanistic pharmacology but insufficient for efficacy or safety conclusions.
- The selectivity confound. Because GHRP-2 can raise cortisol and prolactin, isolating the effects of GH from concurrent hormonal shifts is genuinely difficult.
- Publication and translation gaps. Some of the diagnostic and clinical work exists in non-English literature or specific national contexts, complicating a complete synthesis.
Safety Data Limitations
Because GHRP-2 is not an FDA-approved therapeutic, there is no large, rigorously monitored, long-term safety database of the kind that supports approved drugs. Theoretical and mechanistically predicted concerns — for example, the consequences of chronically stimulating the GH/IGF-1 axis, or the metabolic implications of ghrelin-pathway activation and appetite stimulation — have not been resolved by long-term human trials. The gray-market nature of research-chemical GHRP-2 adds a further, non-pharmacological hazard: purity, identity and sterility of material sold outside a regulated pharmaceutical supply chain cannot be assumed.
Why These Limitations Matter for Interpretation
Taken together, the limitations mean GHRP-2 should be understood as a scientifically important and well-characterized research compound — genuinely valuable for what it taught endocrinology about the ghrelin/GHS-R1a system, and genuinely useful as a diagnostic probe — but not as a validated therapy. Any source presenting it as a proven treatment for aging, body composition, injury recovery, or disease is overstating an evidence base that simply does not extend that far.
How to Read the GHRP-2 Literature Responsibly
Because so much online material about GHRP-2 mixes real pharmacology with aspirational claims, a few reading habits help separate signal from noise:
- Check the endpoint. Did the study measure a hormone level (surrogate) or an actual functional or clinical outcome? A rise in GH or IGF-1 is a mechanism confirmation, not proof of benefit.
- Check the duration. Acute or multi-day studies establish pharmacology; they say nothing about what months of exposure would do.
- Check the population. Findings in GH-deficient patients, in older adults, and in healthy young subjects are not interchangeable, and effects seen in one group may not transfer to another.
- Check the species. A great deal of the most exciting GHRP/ghrelin literature — cardiovascular, neuroprotective, metabolic — is animal or in-vitro work that has not been reproduced in controlled human trials for GHRP-2.
- Check for the confounders. Given GHRP-2’s cortisol and prolactin activity, ask whether a reported effect could reflect those hormones rather than GH.
Applied consistently, these five questions dissolve most of the overreach. They also reveal what is genuinely solid: GHRP-2 is a potent, mechanistically elegant, historically pivotal ghrelin mimetic and GH secretagogue, well established as a short-term endocrine and diagnostic tool, and unproven as a long-term therapy. Holding both halves of that sentence at once is what an honest reference demands. Readers moving from concept to the compound-specific reference figures can continue on the GHRP-2 10 mg vial reference, while the glossary anchors any unfamiliar term used above.
How Does GHRP-2 Fit Into the Broader Secretagogue Landscape?
To place GHRP-2 in context, it helps to see the full map of strategies for influencing the GH axis, each with a different mechanism and a different evidence tier.
| Strategy | Example agents | Mechanism | Note on status |
|---|---|---|---|
| GH replacement | Somatropin (recombinant HGH) | The hormone itself | FDA-approved for specific deficiencies |
| GHRH analogs | Sermorelin, CJC-1295, tesamorelin | GHRH receptor | Tesamorelin FDA-approved for a specific indication; others vary |
| Peptide GHS / GHRPs | GHRP-6, GHRP-2, ipamorelin, hexarelin | GHS-R1a (ghrelin receptor) | Research/diagnostic; not FDA-approved therapeutics in the US |
| Non-peptide GHS | MK-677 (ibutamoren) | GHS-R1a, orally active | Investigational; not FDA-approved |
GHRP-2 sits firmly in the peptide-GHS row: a ghrelin-receptor agonist, potent, historically pivotal, diagnostically useful, and therapeutically unproven in long-term trials. The GHRH-analog row is a complementary mechanism, which is why the two rows are so often discussed together; the CJC-1295 reference and the ipamorelin reference cover the two most-discussed neighbors of GHRP-2.
Where Hexarelin and MK-677 Fit
Two more members of the family round out the map. Hexarelin is another synthetic hexapeptide GHRP, structurally close to the others and notably potent, but it is associated with relatively rapid tachyphylaxis (a diminishing response with repeated dosing) and, like GHRP-2, is not GH-selective. MK-677 (ibutamoren) is not a peptide at all but a small-molecule, orally active GHS-R1a agonist — the practical advantage being that it survives the gut and can be taken by mouth, with a longer duration of action than the injectable peptides. Placing GHRP-2 against these neighbors sharpens its identity: it is the potent, injectable, non-selective, second-generation peptide that most faithfully reproduces the ghrelin signal, sitting historically between the GHRP-6 prototype and the selectivity-optimized ipamorelin.
Common Misconceptions About GHRP-2
Because GHRP-2 lives largely in the research-chemical and online-forum ecosystem rather than the regulated pharmaceutical one, it accumulates misconceptions at a rate few compounds match. Correcting them is part of an honest reference.
“GHRP-2 is basically HGH but safer”
False on both halves. GHRP-2 is not growth hormone and does not deliver GH; it asks the pituitary to release its own. And “safer” is an unearned claim — the absence of long-term controlled safety data means safety is unknown, not established. Working through the body’s own machinery is a plausible mechanistic argument, but plausibility is not the same as a demonstrated safety profile.
“More GHRP-2 means proportionally more growth hormone”
Also false. The GH response to secretagogues is saturable: beyond a certain point, additional GHRP-2 does not produce proportionally more GH because the pituitary’s releasable pool and the receptor system are finite, and somatostatin feedback increasingly opposes release. Pushing higher tends to recruit the off-target effects — the cortisol and prolactin elevation — faster than it recruits additional GH. This dose-response ceiling is a central pharmacological fact, not a minor caveat.
“It’s a proven anti-aging peptide”
Unsupported. There is no long-term, randomized, outcome-based human trial demonstrating that GHRP-2 slows aging or produces durable benefit in healthy people. The GH/IGF-1 axis declines with age, and secretagogues can transiently raise it, but restoring a biomarker toward youthful levels has never been shown to equal restored youthful function — and some GH-axis interventions carry theoretical risks that make the anti-aging framing particularly premature.
“Because it’s a peptide, it’s natural and gentle”
A category error. “Peptide” describes chemical structure, not safety or gentleness. GHRP-2 is a rationally engineered synthetic molecule with deliberate non-natural D-amino acids specifically to resist the body’s own breakdown machinery. It is potent enough to serve as a clinical provocative agent. Structure says nothing about risk.
Every one of these misconceptions shares a root: treating a well-characterized short-term pharmacological effect as if it were a validated long-term therapeutic outcome. That single confusion accounts for most of the overstatement surrounding GHRP-2, and keeping the two categories distinct is the most useful habit a reader can carry away from this article.
Frequently Asked Questions
What is GHRP-2 in simple terms?
GHRP-2 is a synthetic six-amino-acid peptide that signals the pituitary gland to release its own stored growth hormone. It is a growth hormone secretagogue that works by mimicking the natural hormone ghrelin at the GHS-R1a receptor. It is not growth hormone itself and not a GHRH analog. In the United States it is a research compound, not an FDA-approved medicine, though it is approved as a diagnostic GH-stimulation agent in some countries such as Japan.
What is the GHRP-2 mechanism of action?
GHRP-2 binds the ghrelin receptor GHS-R1a on pituitary and hypothalamic cells. This activates a G-protein-coupled signaling cascade that raises intracellular calcium and triggers growth hormone release. It works through three complementary actions: direct pituitary stimulation, promotion of endogenous GHRH release, and functional opposition to somatostatin, the hormone that normally brakes GH secretion. This dual central mechanism is why it synergizes so strongly with GHRH analogs.
Is GHRP-2 FDA-approved?
No. GHRP-2 is not an FDA-approved therapeutic or diagnostic drug in the United States. Its US status is investigational / research-chemical. In Japan it has been approved specifically as a diagnostic agent (pralmorelin) for growth hormone deficiency testing, which is a different and narrower category than therapeutic approval. No jurisdiction has approved it based on long-term outcome trials for the anti-aging or body-composition uses often marketed online.
What is the difference between GHRP-2 and ipamorelin?
Both are ghrelin-receptor (GHS-R1a) agonists that release growth hormone. The key difference is selectivity. GHRP-2 is potent but can also raise ACTH, cortisol and prolactin, and can stimulate appetite. Ipamorelin was specifically designed as a selective GH secretagogue that releases GH with minimal effect on cortisol and prolactin. GHRP-2 is the more representative ghrelin mimetic; ipamorelin is the cleaner, GH-focused option.
Why does GHRP-2 stimulate appetite?
Because GHRP-2 mimics ghrelin, and ghrelin is the body’s primary hunger-signaling hormone. Activating the GHS-R1a receptor produces ghrelin-like effects beyond growth hormone release, including increased appetite. This property has been studied for potential relevance to wasting conditions, and it clearly distinguishes GHRP-2 from selective secretagogues like ipamorelin that produce minimal hunger response.
How is GHRP-2 related to ghrelin?
Remarkably, GHRP-2 was discovered before ghrelin existed as a known molecule. Synthetic GH-releasing peptides worked through a receptor whose natural ligand was unknown for years. That search led to the 1999 discovery of ghrelin, the natural hormone that activates the same GHS-R1a receptor GHRP-2 uses. In effect, the synthetic peptide predicted and prompted the discovery of a natural hormone.
Does GHRP-2 raise cortisol?
It can, particularly at higher doses. GHRP-2 is not fully selective for growth hormone; it can co-elevate ACTH and therefore cortisol, as well as prolactin. This broader hormonal footprint is well documented in the pharmacology literature and is one of the main scientific reasons more selective secretagogues were subsequently developed. It is also a reason research interpretation of GHRP-2 effects must account for these concurrent hormonal changes.
Is GHRP-2 the same as GHRP-6?
No, but they are close relatives. GHRP-6 is the first-generation prototype; GHRP-2 is a more potent second-generation analog. Both are hexapeptide ghrelin-receptor agonists. GHRP-6 tends to produce a stronger hunger response, while GHRP-2 is generally more potent for GH release on a molar basis. Both can affect cortisol and prolactin, unlike the later selective secretagogue ipamorelin.
What evidence supports GHRP-2 in humans?
The strongest human evidence is short-term endocrine pharmacology: GHRP-2 reliably and rapidly releases growth hormone, synergizes with GHRH, and works well enough as a GH-stimulation test to be an approved diagnostic agent in Japan. What is missing is long-term, randomized, outcome-based clinical trial evidence for therapeutic uses. Claims about anti-aging or lasting body-composition benefits are not supported by that tier of evidence.
References
- Howard AD, Feighner SD, Cully DF, et al. A receptor in pituitary and hypothalamus that functions in growth hormone release. Science. 1996;273(5277):974–977.
- Ghigo E, Arvat E, Muccioli G, Camanni F. Growth hormone-releasing peptides. Eur J Endocrinol. 1997;136(5):445–460.
- Bowers CY, Momany FA, Reynolds GA, Hong A. On the in vitro and in vivo activity of a new synthetic hexapeptide that acts on the pituitary to specifically release growth hormone. Endocrinology. 1984;114(5):1537–1545.
- Bowers CY. Growth hormone-releasing peptide (GHRP). Cell Mol Life Sci. 1998;54(12):1316–1329.
- Bowers CY, Reynolds GA, Durham D, Barrera CM, Pezzoli SS, Thorner MO. Growth hormone (GH)-releasing peptide stimulates GH release in normal men and acts synergistically with GH-releasing hormone. J Clin Endocrinol Metab. 1990;70(4):975–982.
- Kojima M, Hosoda H, Date Y, Nakazato M, Matsuo H, Kangawa K. Ghrelin is a growth-hormone-releasing acylated peptide from stomach. Nature. 1999;402(6656):656–660.
- Bowers CY. Unnatural growth hormone-releasing peptide begets natural ghrelin. J Clin Endocrinol Metab. 2001;86(4):1464–1469.
- Müller EE, Locatelli V, Cocchi D. Neuroendocrine control of growth hormone secretion. Physiol Rev. 1999;79(2):511–607.
- Chihara K, Shimatsu A, Hizuka N, Tanaka T, Seino Y, Kato Y. A simple diagnostic test using GH-releasing peptide-2 in adult GH deficiency. Eur J Endocrinol. 2007;157(1):19–27.
- Raun K, Hansen BS, Johansen NL, et al. Ipamorelin, the first selective growth hormone secretagogue. Eur J Endocrinol. 1998;139(5):552–561.
- Pihoker C, Badger TM, Reynolds GA, Bowers CY. Treatment effects of intranasal growth hormone releasing peptide-2 in children with short stature. J Endocrinol. 1997;155(1):79–86.
- Kojima M, Kangawa K. Ghrelin: structure and function. Physiol Rev. 2005;85(2):495–522.
- Korbonits M, Goldstone AP, Gueorguiev M, Grossman AB. Ghrelin—a hormone with multiple functions. Front Neuroendocrinol. 2004;25(1):27–68.
Research-use disclaimer: This article is an educational and research reference only. GHRP-2 is not an FDA-approved therapeutic in the United States. Nothing here is medical advice, a treatment recommendation, or a human-use protocol. All handling and dosing descriptions refer strictly to laboratory research contexts. Consult qualified professionals and applicable regulations before any research use.