The question — which studies demonstrate ipamorelin’s precision in targeting the GHSR-1a receptor — is unusual among peptide questions because the honest answer is not “none.” There genuinely is a foundational, peer-reviewed study that established ipamorelin as a remarkably clean growth hormone secretagogue, and it is one of the more elegant pieces of pharmacology in the whole growth-hormone-releasing-peptide (GHRP) literature.1 So this article does not have to debunk a fabricated premise. What it has to do instead is something subtler: define exactly what kind of “precision” the data actually demonstrate, distinguish that from the kind of precision the word tends to imply in marketing copy, and keep a firm line between a well-characterized receptor-pharmacology profile and any claim of proven clinical usefulness.
That distinction matters because “precision in targeting the GHSR-1a receptor” can mean two quite different things. It can mean that ipamorelin binds the growth hormone secretagogue receptor type 1a and little else — a statement about receptor-subtype specificity. Or it can mean that ipamorelin, acting through that receptor, produces a selective endocrine output: a pulse of growth hormone without the parallel surges of adrenocorticotropic hormone (ACTH), cortisol, and prolactin that older GHRPs provoke. The primary literature demonstrates the second kind of precision convincingly and the first kind only loosely. Ipamorelin is not the only molecule that hits GHSR-1a — ghrelin, GHRP-6, GHRP-2, hexarelin, MK-677, anamorelin, and relamorelin all do. What made ipamorelin notable in 1998 was that its downstream hormonal fingerprint was unusually confined to the somatotroph axis.1
And there is a second line that has to stay bright throughout. Demonstrating that a compound engages a receptor precisely, in rats and in isolated pituitary cells, is a statement about mechanism. It is not a statement that the compound treats, improves, or prevents any human condition. Ipamorelin has never been approved by the U.S. Food and Drug Administration, the European Medicines Agency, or any comparable regulator for any indication. Its most rigorous human test — a randomized controlled trial in postoperative ileus — did not meet its primary endpoint in the overall population.8 So the receptor precision is real; the therapeutic payoff is unproven. This piece is written for researchers and educated readers who want both halves of that truth stated plainly, without the mechanism doing rhetorical work the clinical data cannot support.
What Ipamorelin Is and What “Selectivity” Originally Meant
Ipamorelin is a synthetic pentapeptide with the sequence Aib-His-D-2-Nal-D-Phe-Lys-NH2 (2-aminoisobutyric acid, histidine, D-2-naphthylalanine, D-phenylalanine, lysine, C-terminally amidated). It was developed in the late 1990s by researchers at Novo Nordisk in Denmark and described in the paper that gave it its enduring reputation: Raun and colleagues, “Ipamorelin, the first selective growth hormone secretagogue,” published in the European Journal of Endocrinology in 1998.1 The title is a specific claim, and it is worth unpacking the word “selective” carefully, because it has been stretched well past its original meaning in the intervening decades.
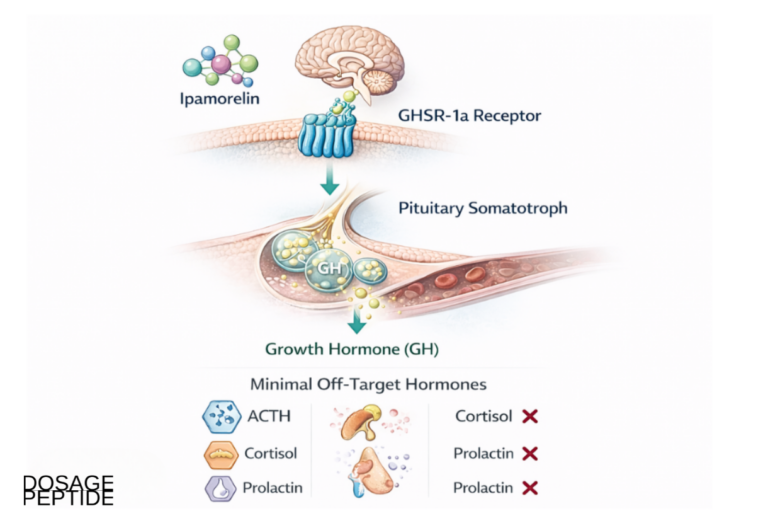
In the 1998 paper, selectivity referred to the hormonal output. The GHRPs that preceded ipamorelin — principally GHRP-6 and GHRP-2 — were potent GH releasers, but they did not act on the somatotroph axis alone. They also stimulated the release of ACTH and, downstream of ACTH, cortisol, and to varying degrees prolactin. That off-target endocrine activity was a nuisance for anyone who wanted a compound that pushed GH cleanly, and it complicated the interpretation of experiments because any observed effect might be mediated by the incidental cortisol or prolactin rather than by GH itself. Raun and colleagues screened for a molecule that would retain the high GH-releasing potency of the GHRP class while shedding the ACTH and cortisol response, and ipamorelin was the result. In their hands, ipamorelin released GH with a potency and efficacy comparable to GHRP-6, yet did not raise ACTH or cortisol to levels significantly different from those seen after growth-hormone-releasing hormone (GHRH) alone — and GHRH is the physiological, exquisitely GH-specific stimulus.1 None of the secretagogues tested, ipamorelin included, meaningfully moved follicle-stimulating hormone, luteinizing hormone, prolactin, or thyroid-stimulating hormone.
So the honest gloss on “the first selective growth hormone secretagogue” is this: ipamorelin was the first GHRP-class peptide whose endocrine effect was as confined to the GH axis as GHRH’s own. That is a genuine and reproducible pharmacological achievement. It is not, however, the same as saying ipamorelin is uniquely specific for the GHSR-1a receptor at the level of binding, and it is emphatically not a statement about clinical benefit. Keeping those three ideas — clean endocrine output, receptor binding specificity, and clinical usefulness — separate is the single most useful habit for reading the ipamorelin literature without being misled.
For readers who want the surrounding vocabulary — secretagogue, somatotroph, pulsatile secretion, GHRH versus GHRP — defined in one place, the site’s peptide glossary collects these terms; and for a sense of where ipamorelin sits among the broader family of GH-axis research compounds, the central dosage index catalogs how these molecules are typically distinguished by mechanism.
The GHSR-1a Receptor: Structure, Signaling, and Why It Is the Right Target
To evaluate any claim about “precision in targeting GHSR-1a,” one has to understand what GHSR-1a is. The growth hormone secretagogue receptor type 1a is a class A (rhodopsin-like) G-protein-coupled receptor. It was cloned in 1996 by Howard and colleagues at Merck, who isolated it from human and porcine pituitary and hypothalamus by capitalizing on the observation that synthetic GH secretagogues signal through the phospholipase C pathway.2 The cloned receptor was a roughly 366-amino-acid, seven-transmembrane protein that was strikingly conserved across species. At the time it was an orphan receptor: its synthetic ligands (the GHRPs and non-peptide secretagogues) were known, but its endogenous ligand was not. That gap was closed in 1999, when Kojima and colleagues purified the natural ligand from rat stomach and named it ghrelin — a 28-amino-acid peptide bearing an unusual n-octanoyl modification on its third serine that is essential for receptor activation.3 The receptor and its ligand together define the ghrelin–GHSR-1a system.
The gene gives rise to two transcripts. GHSR-1a is the full-length, functional, seven-transmembrane receptor that couples to G proteins and signals. GHSR-1b is a truncated splice variant of five transmembrane domains that does not bind the known ligands or signal on its own, though it may modulate 1a. When the ipamorelin literature refers to “the receptor,” it means 1a.
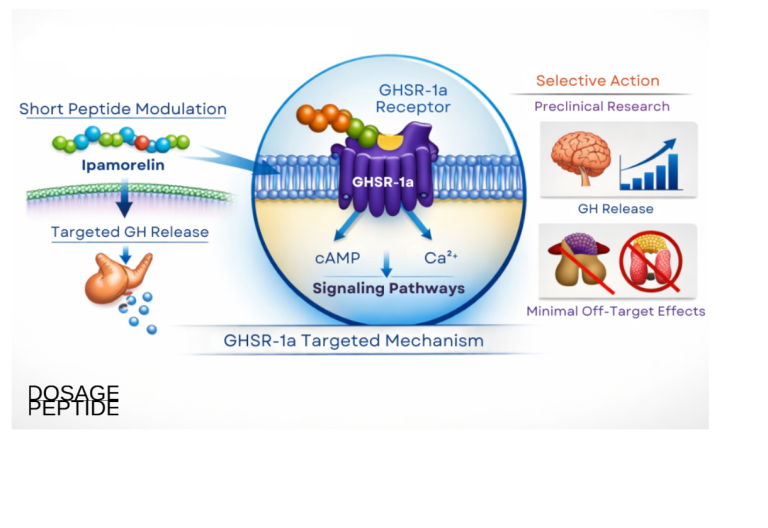
Mechanistically, GHSR-1a couples predominantly to Gq/11. Ligand binding activates phospholipase C-β, which cleaves membrane phosphatidylinositol into inositol trisphosphate (IP3) and diacylglycerol; IP3 mobilizes calcium from intracellular stores and diacylglycerol activates protein kinase C.4 In pituitary somatotrophs, the resulting rise in intracellular calcium triggers exocytosis of stored growth hormone. The receptor is not limited to Gq: depending on cell type it can recruit Gi/o, G12/13, and β-arrestin, and it engages ERK1/2 and other downstream cascades, which is why ghrelin biology extends well beyond GH into appetite, gastrointestinal motility, glucose handling, and reward.4
One property of GHSR-1a is especially relevant to any discussion of “precision.” The receptor exhibits an unusually high level of constitutive activity — that is, it signals even in the absence of ligand, at roughly half of its maximal ghrelin-stimulated output.5 This basal tone has real physiological consequences: a point mutation that selectively abolishes GHSR-1a constitutive activity has been linked to a familial short-stature syndrome, implying that the ligand-independent signaling of the receptor contributes to normal GH secretion and growth.5 For a synthetic agonist such as ipamorelin, this means the receptor it “targets” is not a silent switch waiting to be flipped but a tonically active system that agonists push above an already-elevated baseline. It is an important nuance whenever one models what a secretagogue actually does at the receptor.
It is worth pausing on how this receptor sits inside a larger control loop, because that architecture is what a secretagogue is exploiting. Growth hormone secretion is governed by two opposing hypothalamic inputs — GHRH, which stimulates the somatotroph, and somatostatin, which restrains it — overlaid on the ghrelin–GHSR-1a system, which amplifies GH release and interacts with both. IGF-1, generated in the liver in response to GH, feeds back negatively on the hypothalamus and pituitary to keep the whole system in check. A GHSR-1a agonist such as ipamorelin enters this loop at the ghrelin node: it does not simply inject hormone but nudges an already-regulated oscillator, which is why its effect manifests as a discrete GH pulse that the feedback machinery can still damp. That is the mechanistic basis for the oft-repeated claim that secretagogues are “more physiological” than recombinant GH. The claim is biologically reasonable, but it is a statement about the shape of the hormone curve, not a demonstration that the pulsatile approach yields better clinical outcomes — a distinction that the human evidence, discussed below, does not resolve in ipamorelin’s favor.
The reason GHSR-1a is the right target for a GH secretagogue is that its expression in the pituitary and hypothalamus places it precisely at the control node for GH release, and its activation produces GH secretion that respects the body’s pulsatile architecture and negative-feedback loops. This is the conceptual advantage secretagogues are always said to have over exogenous recombinant GH: rather than flooding the system with hormone, they coax the pituitary to release its own GH in pulses, in principle preserving feedback regulation.12 Whether that theoretical advantage translates into safer or more effective outcomes in humans is a separate, largely unsettled question — and it is one that GHRH analogs such as sermorelin raise in parallel, as discussed in the context of sermorelin and the aging GH axis.
The Foundational Study: Raun et al. 1998
If a single study “demonstrates ipamorelin’s precision” at GHSR-1a, it is Raun 1998, and it deserves to be described in enough detail that a reader can judge exactly what it did and did not show.1
The work combined several experimental layers. In vitro, ipamorelin’s ability to release GH was tested in primary cultures of rat pituitary cells, where it produced a concentration-dependent GH release with an efficacy comparable to GHRP-6 and a potency in the low-nanomolar range. Critically, the investigators also examined receptor pharmacology: ipamorelin’s GH-releasing action was blocked by a GH secretagogue receptor antagonist and was consistent with action at the same receptor as the other GHRPs, anchoring the effect to the GHS-R rather than to some nonspecific mechanism.1 In vivo, in anesthetized and conscious rats and in swine, ipamorelin released GH dose-dependently and with a magnitude on par with the reference GHRPs.
The pivotal experiments, though, were the ones that measured the other pituitary hormones. Here ipamorelin separated itself from the pack. Where GHRP-6 and GHRP-2 raised ACTH and cortisol, ipamorelin did not elevate them beyond what GHRH itself produced — and it maintained this clean profile across a wide dose range, reportedly even at doses far above those needed for GH release.1 This is the empirical core of the “selectivity” claim: a dissociation, within the same molecule and the same GHRP receptor family, between the desired GH signal and the unwanted corticotroph signal. The authors framed ipamorelin as possessing a GHRH-like selectivity while retaining GHRP-like potency, which is precisely why the title called it “the first selective growth hormone secretagogue.”
What the study demonstrated, then, is functional selectivity of endocrine output, mediated through the GH secretagogue receptor, in animal and cell models. What it did not attempt — and what no study should be read as having shown — is any human therapeutic effect, any body-composition or performance outcome, or a formal binding-affinity comparison establishing that ipamorelin discriminates GHSR-1a from GHSR-1a-related targets more sharply than its cousins do. The precision on display is precision of response, elegantly documented, in a preclinical setting.
What the Selectivity Data Actually Show
Because the selectivity finding is the heart of the matter, it helps to lay the hormonal comparison out explicitly. The table below summarizes the qualitative pattern that emerges from the Raun work and the broader GHRP literature: several molecules act at the same GHSR-1a receptor to release GH, but they differ sharply in how much collateral ACTH, cortisol, and prolactin they drag along.1
| Stimulus | GH release | ACTH / cortisol | Prolactin | Interpretation |
|---|---|---|---|---|
| GHRH (physiological) | Strong, GH-specific | Negligible | Negligible | The selectivity benchmark |
| Ipamorelin (GHSR-1a agonist) | Strong, GHRP-like | Not raised above GHRH baseline1 | No significant change | “GHRH-like” selectivity, GHRP-like potency |
| GHRP-6 (GHSR-1a agonist) | Strong | Elevated | Mild | Potent but less selective |
| GHRP-2 (GHSR-1a agonist) | Strong | Elevated | Mild | Potent but less selective |
| Hexarelin (GHSR-1a agonist) | Strong | Elevated | Mild | Potent, notable cortisol effect |
Two honest caveats belong alongside this table. First, the numbers behind the qualitative pattern come predominantly from animal and isolated-cell studies; the exact magnitudes vary by species, dose, and assay, and the frequently quoted precise percentages (“2.3% cortisol change with ipamorelin versus 47% with GHRP-6” and similar) circulate widely in secondary and commercial sources without always tracing cleanly to a single primary measurement. The direction and robustness of the dissociation are well supported; treat specific decimal figures with appropriate skepticism unless you can source them to the primary paper.
Second, “does not raise cortisol” is a statement about a normal, intact neuroendocrine system in healthy animals. It is not a guarantee of endocrine inertness in every human context, at every dose, over long-term repeated exposure — conditions that have simply not been studied. The selectivity is real and reproducible within the settings tested; extrapolating it to open-ended human use is an assumption, not a finding.
Receptor Binding Versus Functional Selectivity: Untangling the “Precision” Claim
This is the section where the article’s central distinction earns its keep, because the word “precision” in the question quietly blends two ideas that the data keep separate.
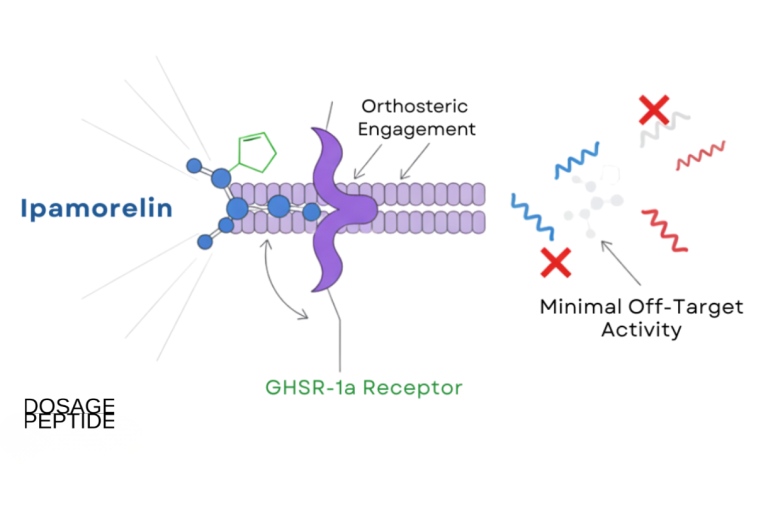
The first idea is receptor-subtype selectivity: the notion that ipamorelin binds GHSR-1a and essentially nothing else. On this point the honest answer is that ipamorelin is a GHSR-1a agonist like the rest of its class, and there is no strong evidence that it is dramatically more receptor-discriminating at the binding level than GHRP-6 or GHRP-2. All of these peptides converge on the same receptor; the GH-releasing effect of ipamorelin was shown to be antagonized by a GH secretagogue receptor blocker, confirming shared receptor mediation rather than a private target.1 So “precision” in the sense of “hits one receptor, ignores its relatives” is not the property the studies establish.
The second idea is functional or endocrine selectivity: the notion that ipamorelin, acting through GHSR-1a, produces an output confined to GH. This is the property the studies genuinely demonstrate, and it is the one that matters for the compound’s reputation.1 How can two peptides act on the same receptor and yet produce different hormonal fingerprints? Several mechanisms are plausible and not mutually exclusive: differences in where in the brain and pituitary each peptide effectively reaches (pharmacokinetics and distribution), differences in the degree to which each engages hypothalamic circuits that feed the corticotropin axis versus the somatotroph directly, and the possibility of biased agonism, in which structurally distinct ligands at the same GPCR stabilize different receptor conformations and thereby favor different downstream pathways.4 Biased agonism at GHSR-1a is an active research area, and functionally selective ghrelin-receptor ligands have been described that dissociate, for example, GH-related from dopamine-related signaling. Whether ipamorelin’s clean corticotroph profile reflects true signaling bias, a distribution effect, or both has not been definitively resolved — which is itself a useful reminder that even the best-supported ipamorelin story still contains open mechanistic questions.
The practical takeaway is that the accurate way to describe ipamorelin’s demonstrated “precision” is: a GHSR-1a agonist that produces an unusually GH-specific endocrine response. That phrasing credits the compound for exactly what the data support — a clean output — without overclaiming a receptor-level uniqueness that the data do not establish. Marketing language that describes ipamorelin as “highly selective for the GHSR-1a receptor” is technically defensible only if the reader understands “selective” to mean the endocrine result, not exclusive receptor occupancy.
Preclinical Evidence Beyond Selectivity: Bone, Body Weight, and GH Pulsatility
Selectivity is the headline, but ipamorelin’s preclinical file contains additional functional studies that clarify what its GHSR-1a agonism produces at the whole-animal level — all in rodents, and all consistent with the compound behaving as a bona fide GH secretagogue.
Johansen and colleagues, in 1999, gave ipamorelin subcutaneously three times daily for fifteen days to adult female rats across a range of doses and measured longitudinal bone growth, body weight, and GH release.6 Ipamorelin dose-dependently increased longitudinal bone growth rate and body weight, confirming that its GH-releasing action translated into a downstream anabolic, growth-related readout in vivo. A companion line of work by Svensson and colleagues in 2000 asked whether the GH secretagogues ipamorelin and GHRP-6 could increase bone mineral content in young adult female rats delivered continuously via osmotic minipump over twelve weeks.7 Both peptides increased body weight and total tibial and vertebral bone mineral content relative to vehicle — but with an important nuance the authors were careful to state: when bone mineral content was corrected for the accompanying increase in body weight, the effect on density disappeared.7 In other words, the peptides grew bigger animals with proportionally more bone, rather than selectively increasing bone density. That is exactly the kind of measured, deflationary detail that separates a primary study from its downstream summaries, which often quote “increased bone mineral content” without the correction.
These studies matter for the precision question in a specific way. They confirm that ipamorelin’s GHSR-1a agonism is coupled to real physiological consequences — GH pulses, growth, weight gain — and not merely to a hormone spike in a test tube. But they are rodent studies with morphometric endpoints, and none of them tested a clinical outcome. They are the right evidence for the statement “ipamorelin releases GH and produces GH-typical effects in rats,” and the wrong evidence for any statement about human body composition, athletic performance, anti-aging, or disease treatment. The gap between the two is the gap between a mechanism and a medicine.
Human Evidence: The Postoperative Ileus Program
Here is where the honest arc of the ipamorelin story bends. A compound with a beautiful preclinical selectivity profile eventually has to be tested in people to matter clinically, and ipamorelin was — not for bodybuilding or anti-aging, but for a specific gastrointestinal indication that follows naturally from ghrelin-receptor biology.
Because GHSR-1a activation stimulates gastrointestinal motility (ghrelin is a prokinetic hormone), ghrelin mimetics were logical candidates for postoperative ileus, the temporary shutdown of gut motility that follows abdominal surgery. Ipamorelin was advanced into this indication. The most rigorous published human study is the proof-of-concept trial by Beck and colleagues, reported in the International Journal of Colorectal Disease in 2014: a multicenter, randomized, double-blind, placebo-controlled study in which adults undergoing small or large bowel resection received intravenous ipamorelin (0.03 mg/kg) or placebo twice daily for up to seven days or until discharge.8
The result is the part that matters, and it must be stated without softening: the trial did not meet its primary efficacy endpoint in the overall study population. Any suggestion of benefit on the speed of bowel-function recovery was confined to a subgroup (patients undergoing open procedures) in post-hoc-flavored analysis, not the pre-specified primary comparison across all patients.8 The compound was reasonably well tolerated — consistent with its clean preclinical profile — but tolerability is not efficacy. The development program for this indication did not proceed to a successful phase 3 approval, and ipamorelin has no approved use anywhere as a result.
There is a broader lesson embedded in this outcome that applies well beyond ipamorelin. The postoperative-ileus program was a rational bet: ghrelin is a genuine prokinetic, GHSR-1a activation demonstrably stimulates gut motility in animals, and a clean, selective agonist looked like an ideal way to test the idea in humans. The bet still did not pay off at the primary endpoint. This is the ordinary fate of mechanistically attractive compounds — the graveyard of drug development is full of molecules that engaged their target beautifully and failed to move the clinical needle, because human physiology is redundant, compensatory, and far messier than a receptor-binding assay. Ipamorelin’s selectivity was never the problem; the problem was that engaging the receptor, however precisely, was not sufficient to produce a robust clinical benefit in the one indication where it was seriously tested. Anyone reasoning from “it hits the receptor cleanly” to “it must work” is skipping exactly the step that trials exist to test.
It is worth being precise about what this human evidence does and does not tell us about the precision question. It confirms that ipamorelin can be given to humans and engages ghrelin-receptor biology enough to be a plausible prokinetic candidate — a real-world echo of its GHSR-1a agonism. It does not demonstrate clinical efficacy, and it certainly does not validate any of the physique, longevity, or wellness uses for which the peptide is informally marketed, none of which have been tested in controlled human trials at all. The single most rigorous thing anyone did with ipamorelin in humans returned a negative primary result. That fact should anchor every discussion of the compound’s clinical value.
How Ipamorelin Compares to Other GHSR-1a Ligands
Placing ipamorelin beside the other molecules that act on GHSR-1a clarifies both its distinctive virtue (endocrine cleanliness) and its shared limitation (a thin or negative clinical record for the uses people care about). The comparison also illustrates a sobering pattern: even ghrelin-receptor agonists that were developed much further than ipamorelin have struggled to convert receptor engagement into approved therapies.
| Compound | Type | Endocrine selectivity vs. ACTH/cortisol | Furthest clinical development |
|---|---|---|---|
| Ghrelin (endogenous) | Native acylated peptide | Broad (appetite, GI, GH, metabolic) | Investigational tool; not a marketed drug3 |
| Ipamorelin | Synthetic pentapeptide | High — GH without ACTH/cortisol rise1 | Phase 2 postoperative ileus, primary endpoint not met8 |
| GHRP-6 / GHRP-2 | Synthetic peptides | Lower — raise ACTH/cortisol | Research/diagnostic use; not approved therapeutics |
| Hexarelin | Synthetic peptide | Lower — notable cortisol effect | Investigational; not approved |
| MK-677 (ibutamoren) | Oral non-peptide agonist | Moderate; sustained GH/IGF-1 rise | Multiple trials (e.g., frailty); not FDA-approved |
| Anamorelin | Oral non-peptide agonist | Moderate | Phase 3 in cancer cachexia (ROMANA): raised lean mass, not grip strength; EMA rejected10 |
| Relamorelin | Synthetic peptide analog | Prokinetic-focused | Phase 2b diabetic gastroparesis: reduced composite symptoms, accelerated emptying (vomiting drop not significant vs. placebo)9 |
The pattern is instructive. Ipamorelin’s claim to fame — the cleanest endocrine output in the class — is real and is its genuine differentiator.1 But note where the clinical action actually happened. The GHSR-1a agonists that advanced furthest did so in gastrointestinal and cachexia indications that exploit ghrelin biology, not in the GH-for-body-composition space where ipamorelin is popularly promoted. Anamorelin reached phase 3 in cancer cachexia and reliably increased lean body mass, yet failed to improve handgrip strength — the functional endpoint regulators wanted — and was rejected by the EMA.10 Relamorelin showed real symptomatic benefit in diabetic gastroparesis in phase 2.9 Against that backdrop, ipamorelin looks like an elegant early tool compound whose selectivity made it scientifically interesting but which was never carried to a successful clinical finish for any use. Researchers comparing the GH-axis peptides for their metabolic versus prokinetic profiles will find the broader family cross-referenced through the dosage catalog, and those tracing how growth-hormone-releasing compounds are being reconsidered for muscle-related endpoints may find the adjacent discussion of GH-fragment approaches to muscle wasting a useful contrast in evidence standards.
Research Models and Methodology
Understanding how ipamorelin’s precision was measured clarifies what the evidence can and cannot support. The methodology falls into three tiers, and the strength of a claim depends heavily on which tier produced it.
In vitro and cellular pharmacology. The bedrock selectivity work used primary rat pituitary cell cultures to measure GH release as a function of ipamorelin concentration, alongside receptor-antagonist experiments to confirm that the effect was GHS-R-mediated.1 This is the appropriate model for establishing potency, efficacy, and receptor dependence, and it is where the “acts through GHSR-1a” claim is best grounded. Complementary receptor-signaling studies — the Gq/PLC/calcium cascade, constitutive activity, and biased-agonism work — come from heterologous receptor-expression systems and neuronal preparations that dissect the GHSR-1a pathway in mechanistic detail.45
Rodent and large-animal in vivo studies. The selectivity of endocrine output (GH up, ACTH/cortisol flat) was demonstrated in living rats and swine by measuring multiple pituitary hormones after dosing.1 The functional consequences — longitudinal bone growth, body-weight gain, bone mineral content — came from multi-week dosing studies in rats with morphometric and densitometric endpoints.67 These models are well suited to characterizing a secretagogue’s GH-axis effects but are not disease models and do not speak to human outcomes.
Human trials. The clinical methodology that exists is essentially the postoperative ileus program: randomized, double-blind, placebo-controlled, intravenous dosing with gastrointestinal-recovery endpoints.8 There is, to the available literature, no controlled human trial of ipamorelin for GH deficiency, body composition, athletic recovery, sleep, or anti-aging — the uses for which it is most often informally promoted. That absence is not a minor footnote; it is the defining limitation of the human evidence base.
The methodological bottom line is that ipamorelin’s receptor and endocrine precision is supported by strong, appropriate preclinical models, while its clinical value rests on a single indication that failed its primary endpoint. Any statement that reaches beyond “selective GH secretagogue in animals with a negative ileus trial in humans” is extrapolation. For readers who work with the compound as a research material, the arithmetic of reconstitution and concentration is covered in the peptide reconstitution guide and the associated dosage calculator, both framed for educational reference rather than human-use guidance.
Dosing in a Research Context and Handling
Because ipamorelin is encountered almost entirely as a lyophilized (freeze-dried) powder in sealed vials, a brief, strictly educational note on laboratory handling is warranted — with the emphasis that this describes standard research-peptide practice, not a usage recommendation, and that ipamorelin is not an approved therapeutic for any indication in humans.
Lyophilized peptides are generally reconstituted with sterile or bacteriostatic water for laboratory purposes. The diluent is directed slowly against the inner wall of the vial rather than sprayed onto the powder, and the vial is swirled gently rather than shaken, because vigorous agitation can shear peptide bonds and denature the material. The volume of diluent simply sets the concentration: a fixed mass of peptide dissolved in a larger volume yields a lower concentration per unit volume, which is the arithmetic behind any reconstitution chart. Ipamorelin’s short plasma half-life — on the order of roughly two hours — is the pharmacokinetic reason the compound produces a discrete GH pulse rather than a sustained elevation, and it is why research protocols that use it typically model transient exposure rather than steady-state levels.
Standard stability and storage considerations that recur across the research-peptide literature are summarized below.
| Parameter | Typical research-context practice |
|---|---|
| Lyophilized storage | Cool, dark conditions; long-term stability favored by freezing |
| After reconstitution | Refrigerated; used within a limited window |
| Light and heat | Minimize exposure; both degrade peptides |
| Agitation | Swirl gently; avoid shaking or foaming |
| Freeze–thaw | Repeated cycles degrade peptides; avoid |
| Reconstitution fluid | Bacteriostatic water for multi-use practice; aseptic technique |
It bears repeating that meticulous handling changes nothing about the evidence question. A perfectly reconstituted, high-purity vial of ipamorelin is still a compound whose only rigorous human trial missed its primary endpoint and which has no approved indication. Good technique preserves whatever biological activity the molecule has; it does not create clinical efficacy where none has been demonstrated. Handling parameters and unit math for this class of material are cataloged for educational reference through the site’s central dosages index.
Safety and Tolerability
Ipamorelin’s safety story is genuinely one of its more favorable features, but it has to be stated with the same care as everything else — because “well tolerated in the trials that were run” is not the same as “safe for open-ended human use.”
The compound’s defining pharmacological virtue — not raising ACTH, cortisol, or prolactin — is itself a safety-relevant property, because it means ipamorelin avoids the cortisol elevation that makes less-selective GHRPs less attractive.1 In the human postoperative ileus trial, intravenous ipamorelin was reasonably well tolerated, consistent with a clean acute profile.8 Several important caveats temper this picture, and they compound one another:
- Narrow evidence base. Human tolerability was characterized mainly in a surgical population over days of intravenous dosing, not in healthy people using subcutaneous injections over weeks or months. Route, duration, and population all differ from typical informal use.
- GH-axis effects are not free of consequence. Any effective GH secretagogue raises GH and, secondarily, IGF-1. Sustained elevation of the GH/IGF-1 axis carries theoretical concerns — insulin resistance and impaired glucose tolerance, fluid retention, joint discomfort, and the long-debated question of IGF-1 and cell proliferation — that are well documented for GH therapy generally and are not neutralized by ipamorelin’s corticotroph selectivity.12 Long-term human safety of repeated ipamorelin dosing has simply not been established.
- Product quality. Material sold outside regulated channels as “research chemical” varies in purity; impurities, endotoxin, and mislabeling are real hazards independent of the molecule’s intrinsic pharmacology.
- Prohibited in sport. Ipamorelin is explicitly named on the World Anti-Doping Agency Prohibited List under class S2 (growth hormone secretagogues and their mimetics), prohibited at all times, in and out of competition.11 For any tested athlete this is a definitive regulatory hazard regardless of pharmacology.
The reasonable reading is that ipamorelin has not thrown up major short-term safety signals in the limited settings studied, and that its selectivity spares it some GHRP-related concerns. But a clean short-term profile in a small surgical trial provides no assurance about repeated long-term administration to healthy people, and it provides no evidence of benefit. Absence of demonstrated harm and absence of demonstrated efficacy can coexist, and for ipamorelin’s popular uses they do.
Regulatory Status
Ipamorelin’s regulatory position is unambiguous and worth stating without hedging, because it is frequently blurred in promotional writing.
No therapeutic approval, anywhere. Ipamorelin is not approved as a drug for any indication by the FDA, the EMA, or any comparable major regulator. It was investigated for postoperative ileus and did not clear the efficacy bar needed to advance to approval.8 There is no approved indication of any kind that could be extended to GH deficiency, body composition, recovery, sleep, or anti-aging.
Not a dietary supplement. Ipamorelin is a synthetic drug candidate, not a lawful dietary-supplement ingredient. In the United States, the FDA has repeatedly acted against the marketing of injectable research peptides for human use, and ipamorelin falls squarely outside the supplement framework. Material sold as “for research use only” is exactly that — a laboratory reagent, not a product cleared for human administration.
Prohibited in sport. As noted, WADA lists ipamorelin by name among prohibited growth hormone secretagogues and mimetics in class S2, banned at all times.11 Athletes subject to anti-doping testing should treat any use as an anti-doping rule violation.
The regulatory synthesis is straightforward: ipamorelin is an investigational compound with a well-characterized preclinical pharmacology, no approved therapeutic use, a negative pivotal human trial in its one seriously pursued indication, and an explicit prohibition in sport. Any legitimate exploration of the molecule belongs within properly authorized preclinical or clinical research under appropriate oversight — not informal human use justified by an elegant selectivity profile.
Putting the Precision Question in Perspective
So, which studies demonstrate ipamorelin’s precision in targeting the GHSR-1a receptor? The honest, specific answer is that Raun et al. 1998 demonstrated, convincingly and reproducibly in cell and animal models, that ipamorelin is a GHSR-1a agonist whose endocrine output is unusually confined to growth hormone — releasing GH with GHRP-like potency while sparing ACTH, cortisol, and prolactin in a manner previously seen only with GHRH.1 That finding is buttressed by receptor-pharmacology work establishing the GHSR-1a signaling machinery it acts on234 and by rodent studies showing the GH-typical downstream consequences of that agonism.67
But precision, properly understood, is precision of endocrine response, not of exclusive receptor occupancy, and it is a preclinical property. It does not license the leap to clinical benefit. The one rigorous human trial missed its primary endpoint,8 the compound is approved nowhere, and the uses for which it is popularly marketed have never been tested in controlled human studies. Ipamorelin is a beautiful example of what a selective tool compound looks like and a cautionary example of how far a clean mechanism can be from a proven medicine. Both statements are true at once, and honest communication about the peptide requires holding them together. Readers who want to keep the terminology straight can consult the glossary, and those following how the peptide evidence base evolves can track new literature through the site’s ongoing coverage.
Frequently Asked Questions
Does ipamorelin really target the GHSR-1a receptor selectively?
It targets the growth hormone secretagogue receptor type 1a (the ghrelin receptor), as the other GHRP-class peptides do, and its GH-releasing effect is blocked by a GHS-R antagonist, confirming it acts through that receptor.1 The “selectivity” that made ipamorelin famous, however, is not exclusive receptor binding — it is the selectivity of its output: it releases growth hormone without meaningfully raising ACTH, cortisol, or prolactin, unlike GHRP-6 and GHRP-2. So the accurate description is a GHSR-1a agonist with an unusually GH-specific endocrine response, not a molecule that binds a unique receptor.
Which single study best demonstrates ipamorelin’s precision?
Raun and colleagues, “Ipamorelin, the first selective growth hormone secretagogue,” European Journal of Endocrinology 1998.1 It combined pituitary-cell pharmacology, receptor-antagonist experiments, and in vivo hormone measurements in rats and swine to show GHRP-like GH potency with GHRH-like endocrine cleanliness. It is a preclinical study; it does not demonstrate any human clinical effect.
Is ipamorelin FDA-approved for anything?
No. Ipamorelin is not approved by the FDA, the EMA, or any comparable regulator for any indication. It was investigated for postoperative ileus in a randomized controlled trial that did not meet its primary endpoint, and development did not lead to approval.8 It is not a lawful dietary supplement and is sold, when sold at all, as a research-use-only reagent.
Has ipamorelin been tested in humans at all?
Yes, but narrowly. The most rigorous human study is a multicenter, randomized, double-blind, placebo-controlled trial of intravenous ipamorelin for postoperative ileus after bowel resection.8 It was reasonably well tolerated but did not meet its primary efficacy endpoint in the overall population. There are no controlled human trials of ipamorelin for GH deficiency, body composition, recovery, sleep, or anti-aging — the uses for which it is most often informally promoted.
Why does ipamorelin raise GH but not cortisol when GHRP-6 raises both?
Both act on GHSR-1a, so the difference is not a different receptor. It likely reflects some combination of how each peptide distributes and reaches the relevant hypothalamic and pituitary circuits and, potentially, biased agonism — the phenomenon in which different ligands at the same G-protein-coupled receptor stabilize different conformations and favor different downstream pathways.4 The exact explanation for ipamorelin’s clean corticotroph profile has not been definitively resolved, which is a reminder that even its best-supported property still contains open mechanistic questions.
What does ipamorelin actually do to the body in animal studies?
In rats, multi-week dosing dose-dependently increased longitudinal bone growth and body weight,6 and both ipamorelin and GHRP-6 increased bone mineral content — though when corrected for the accompanying body-weight gain, the effect on bone density itself disappeared.7 These are GH-typical effects in rodents; none of them establish human outcomes.
How does ipamorelin compare with anamorelin or relamorelin?
All three are ghrelin-receptor (GHSR-1a) agonists, but the other two were developed further clinically. Anamorelin reached phase 3 in cancer cachexia and reliably increased lean body mass but failed to improve handgrip strength and was rejected by the EMA.10 Relamorelin showed symptomatic benefit in diabetic gastroparesis in phase 2.9 Ipamorelin’s distinction is its endocrine cleanliness, but its clinical record is thinner, resting on a single negative ileus trial.
Is ipamorelin allowed in competitive sport?
No. Ipamorelin is named on the World Anti-Doping Agency Prohibited List under class S2 (peptide hormones, growth factors, related substances, and mimetics — specifically growth hormone secretagogues), prohibited at all times, both in and out of competition.11 Use by a tested athlete constitutes an anti-doping rule violation.
How is ipamorelin handled in a research setting?
As a lyophilized powder, it is reconstituted with sterile or bacteriostatic water using gentle technique (swirl, do not shake), stored cool and dark, and protected from freeze–thaw cycles — standard research-peptide practice. Its short plasma half-life underlies the discrete GH pulse it produces. Handling quality preserves activity but has no bearing on the compound’s lack of approved clinical use.
References
- Raun K, Hansen BS, Johansen NL, et al. Ipamorelin, the first selective growth hormone secretagogue. Eur J Endocrinol. 1998;139(5):552-561. PMID: 9849822. https://pubmed.ncbi.nlm.nih.gov/9849822/
- Howard AD, Feighner SD, Cully DF, et al. A receptor in pituitary and hypothalamus that functions in growth hormone release. Science. 1996;273(5277):974-977. PMID: 8688086. https://pubmed.ncbi.nlm.nih.gov/8688086/
- Kojima M, Hosoda H, Date Y, Nakazato M, Matsuo H, Kangawa K. Ghrelin is a growth-hormone-releasing acylated peptide from stomach. Nature. 1999;402(6762):656-660. PMID: 10604470. https://pubmed.ncbi.nlm.nih.gov/10604470/
- Yin Y, Li Y, Zhang W. The growth hormone secretagogue receptor: its intracellular signaling and regulation. Int J Mol Sci. 2014;15(3):4837-4855. PMID: 24651458; PMCID: PMC3975427. https://pmc.ncbi.nlm.nih.gov/articles/PMC3975427/
- Mear Y, Enjalbert A, Thirion S. GHS-R1a constitutive activity and its physiological relevance. Front Neurosci. 2013;7:87. PMID: 23754971; PMCID: PMC3665924. https://pmc.ncbi.nlm.nih.gov/articles/PMC3665924/
- Johansen PB, Nowak J, Skjaerbaek C, et al. Ipamorelin, a new growth-hormone-releasing peptide, induces longitudinal bone growth in rats. Growth Horm IGF Res. 1999;9(2):106-113. PMID: 10373343. https://pubmed.ncbi.nlm.nih.gov/10373343/
- Svensson J, Lall S, Dickson SL, et al. The GH secretagogues ipamorelin and GH-releasing peptide-6 increase bone mineral content in adult female rats. J Endocrinol. 2000;165(3):569-577. PMID: 10828840. https://pubmed.ncbi.nlm.nih.gov/10828840/
- Beck DE, Sweeney WB, McCarter MD; Ipamorelin 201 Study Group. Prospective, randomized, controlled, proof-of-concept study of the ghrelin mimetic ipamorelin for the management of postoperative ileus in bowel resection patients. Int J Colorectal Dis. 2014;29(12):1527-1534. PMID: 25331030. https://pubmed.ncbi.nlm.nih.gov/25331030/
- Camilleri M, McCallum RW, Tack J, et al. Efficacy and safety of relamorelin in diabetics with symptoms of gastroparesis: a randomized, placebo-controlled study. Gastroenterology. 2017;153(5):1240-1250. PMID: 28760384. https://pubmed.ncbi.nlm.nih.gov/28760384/
- Temel JS, Abernethy AP, Currow DC, et al. Anamorelin in patients with non-small-cell lung cancer and cachexia (ROMANA 1 and ROMANA 2): results from two randomised, double-blind, phase 3 trials. Lancet Oncol. 2016;17(4):519-531. PMID: 26906526. https://pubmed.ncbi.nlm.nih.gov/26906526/
- World Anti-Doping Agency. Prohibited List — S2. Peptide Hormones, Growth Factors, Related Substances and Mimetics (growth hormone secretagogues, including ipamorelin). https://www.wada-ama.org/en/prohibited-list
- Sinha DK, Balasubramanian A, Tatem AJ, et al. Beyond the androgen receptor: the role of growth hormone secretagogues in the modern management of body composition in hypogonadal males. Transl Androl Urol. 2020;9(Suppl 2):S149-S159. PMCID: PMC7108996. https://pmc.ncbi.nlm.nih.gov/articles/PMC7108996/
Educational and research-use disclaimer: This article is provided solely for scientific and educational purposes. Ipamorelin is an investigational growth hormone secretagogue that is not approved by the FDA, EMA, or any comparable regulator for the treatment, cure, or prevention of any disease, and it is not a lawful dietary supplement. Its receptor selectivity is established preclinically; no clinical benefit for growth hormone deficiency, body composition, recovery, or any wellness use has been demonstrated in controlled human trials, and its one rigorous human trial (postoperative ileus) did not meet its primary endpoint. Ipamorelin is prohibited in sport by WADA. Nothing here is medical advice or a recommendation for human use. Any legitimate investigation of this compound should occur within properly authorized preclinical or clinical research under appropriate oversight. Readers should consult qualified professionals and applicable regulations before making any decisions.