The question in the title carries a promise inside it. To ask whether “clinical insights” show that the Grow-H blend “truly boosts strength and repair” is to presuppose that there is a body of clinical evidence to consult, and that the only remaining task is to weigh it. That framing does not survive contact with the actual literature. Grow-H is not a studied therapeutic. It is a commercial pairing of two research peptides — CJC-1295 without DAC (a growth-hormone-releasing hormone analog, often labeled modified GRF 1-29) and ipamorelin (a selective growth-hormone-releasing peptide) — sold as a lyophilized powder for laboratory use.12 There has never been a clinical trial of the Grow-H blend. There is no published human study of this specific two-peptide combination measuring strength, muscle mass, tendon healing, wound closure, or any recovery endpoint. So the honest version of the title is not a yes-or-no question about proven benefit; it is an open research question about a plausible mechanism that has not been tested in the form it is marketed.
That distinction matters because the marketing language around Grow-H leans heavily on a chain of inference that sounds airtight and is in fact a series of hopeful hand-offs. The reasoning goes: growth hormone builds muscle and aids healing; CJC-1295 and ipamorelin raise growth hormone; therefore Grow-H boosts strength and repair. Each link in that chain is either weaker than it sounds or contested by direct human data. Growth hormone’s effect on muscle strength in healthy adults is, at best, small and largely attributable to fluid retention rather than contractile tissue.56 Growth hormone stimulates collagen synthesis in tendon and muscle connective tissue but does not increase myofibrillar (contractile) protein synthesis in controlled human work.7 And the leap from “these peptides raise GH” to “this raises functional strength” skips over the entire question of whether the resulting GH pulses translate into anything a person or an animal could measure as performance.
This article is written for researchers and scientifically literate readers who want an accurate map of what is known, what is merely plausible, and what is simply untested about Grow-H. We will define exactly what is in the vial, trace the mechanism of each component honestly, examine the real evidence for the individual peptides, confront the total absence of trials on the blend itself, look at what growth hormone actually does for muscle and repair in humans, compare Grow-H with agents that have genuinely been studied, and cover research-context dosing, safety, handling, and regulatory status. The guiding posture throughout is restraint. Grow-H is not an approved therapy for any condition, and nothing here should be read as a claim that it treats, cures, or prevents disease, or that it has been shown to build strength or accelerate healing in humans.
What Grow-H Actually Is: Two Peptides in One Vial
Grow-H is not a single molecule with a defined pharmacology of its own. It is a fixed-ratio co-formulation, most commonly sold as a 10 mg vial containing 5 mg of CJC-1295 (no DAC) and 5 mg of ipamorelin.12 Understanding the blend therefore means understanding its two ingredients separately and then the logic of combining them. They belong to two different, complementary classes of growth-hormone secretagogue.
CJC-1295 (no DAC) is a growth-hormone-releasing hormone (GHRH) analog. Native GHRH is a 44-amino-acid hypothalamic peptide, and its biological activity resides in the first 29 residues — the fragment known as GRF(1-29) or sermorelin. CJC-1295 without DAC is a modified version of that 1-29 fragment carrying a small set of amino-acid substitutions (the “modified GRF 1-29” changes) that resist enzymatic degradation and slightly extend its otherwise very short half-life. It binds the GHRH receptor on pituitary somatotrophs and stimulates them to synthesize and release growth hormone in a pattern that preserves the body’s natural pulsatility.1 This is the “no DAC” version, and the distinction is important. The original CJC-1295 molecule studied by Teichman and colleagues carried a Drug Affinity Complex (DAC) — a maleimide group that binds covalently to circulating albumin, extending the half-life to roughly 6–8 days and producing a sustained, non-pulsatile elevation of GH and IGF-1 for weeks after a single dose.1 The no-DAC version in Grow-H has a half-life measured in roughly half an hour, which is precisely why it is paired with a second peptide and dosed frequently in research protocols rather than weekly.
Ipamorelin is a growth-hormone-releasing peptide (GHRP) and a selective agonist of the growth-hormone secretagogue receptor (GHS-R1a) — the same receptor that the stomach hormone ghrelin activates.23 It is a synthetic pentapeptide (Aib-His-D-2-Nal-D-Phe-Lys-NH2) that was described in 1998 as the first selective GH secretagogue: it stimulates GH release with potency comparable to the older GHRP-6, but, unlike GHRP-6 and GHRP-2, it does not meaningfully raise ACTH, cortisol, or prolactin even at doses far above the effective dose for GH release.2 That selectivity — a clean GH signal without the stress-hormone spillover — is the property that made ipamorelin attractive as a research tool and the reason it is favored over cruder GHRPs in blends like this one.
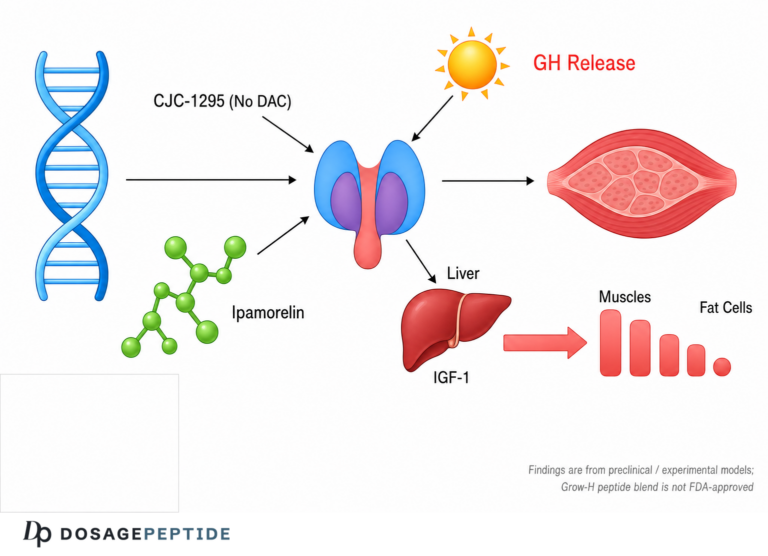
The rationale for putting the two together is genuine pharmacology, not marketing invention. GHRH analogs and GHRPs act through separate receptors and separate intracellular pathways, and when given together they produce a GH release that is larger than the simple sum of each alone — a synergistic rather than merely additive response.4 The GHRH analog (CJC-1295) primes the somatotroph and raises the amplitude of the GH pulse; the GHRP (ipamorelin) amplifies that pulse through the ghrelin-receptor pathway and simultaneously suppresses somatostatin, the brake that normally shuts GH secretion down.4 The combination is a well-established experimental strategy for maximizing endogenous GH output while keeping the secretion pulsatile, and it is this documented synergy that Grow-H is built to exploit.
What deserves emphasis, and is easy to lose in the enthusiasm for the synergy, is that “produces more GH than either alone” is a statement about a biomarker, not about strength or repair. The combination reliably raises a hormone. Whether that hormone elevation, delivered this way, produces the downstream physical outcomes the product name implies is a completely separate question — and it is the question the evidence does not answer. Readers new to this vocabulary of secretagogues, analogs, and pulsatility may find the site’s peptide glossary useful for keeping the terms straight before going further.
The Mechanism: How CJC-1295 and Ipamorelin Raise Growth Hormone

To evaluate any claim about Grow-H fairly, it helps to trace the mechanism carefully, because the mechanism is genuinely well characterized up to a certain point — and then abruptly stops being characterized at exactly the point where the strength-and-repair claims begin.
Growth hormone secretion from the anterior pituitary is governed by a push-pull system. Two hypothalamic signals drive it up: GHRH, which acts on the GHRH receptor to stimulate synthesis and release, and ghrelin, the endogenous ligand of the GHS-R1a receptor, discovered in 1999 as a growth-hormone-releasing acylated peptide from the stomach.3 One signal holds it down: somatostatin, which suppresses release. The pulsatile pattern of GH in healthy physiology — sharp bursts, especially during deep sleep, against a low baseline — emerges from the interplay of these three signals. That pulsatility is not incidental; the tissues downstream of GH respond differently to pulsatile versus continuous exposure, which is part of why continuous, flat GH elevation (as with the DAC version or with exogenous recombinant GH) is biologically different from amplified pulses.
CJC-1295 (no DAC) plugs into the GHRH arm. By resisting the dipeptidyl-peptidase degradation that destroys native GHRH within minutes, it provides a somewhat more durable GHRH-receptor signal, priming the somatotrophs so that when a pulse fires, more GH is available to release.1 Ipamorelin plugs into the ghrelin arm. By activating GHS-R1a, it both triggers GH release directly and antagonizes the somatostatin brake, so the pulse it evokes is larger and less opposed.23 Give both at once and you have primed the pump (GHRH side) and released the brake while pressing the accelerator (GHRP side). The result, documented across the GHRH-plus-GHRP literature, is a GH pulse substantially greater than either agent produces on its own.4
The GH released then acts in two ways. Some of its effects are direct, mediated by GH receptors on target tissues including fat (where it is lipolytic) and, to a lesser and more debated degree, muscle. Most of its anabolic reputation, however, is indirect and runs through insulin-like growth factor 1 (IGF-1), produced chiefly in the liver in response to GH and acting on the PI3K/Akt/mTOR pathway that governs protein synthesis. This is the pathway that the whole “strength and repair” narrative depends on: GH raises IGF-1, IGF-1 drives anabolic signaling, anabolic signaling builds tissue. And the GHRH-plus-GHRP combination does raise IGF-1 with repeated dosing.14
Here is where honesty requires a hard stop. Everything above is a mechanism for raising a hormone axis. It is not, by itself, evidence that raising that axis with these peptides produces measurable gains in muscle strength, contractile muscle mass, or tissue healing in a living organism. The gap between “IGF-1 goes up” and “the subject is stronger or heals faster” is enormous, and it is precisely the gap that clinical research exists to fill. In the case of Grow-H, that research has not been done. And as the next sections show, when researchers have filled a similar gap for growth hormone itself, the answer has frequently been disappointing: the hormone rises, body water rises, and functional strength does not reliably follow.56 The mechanism is real; its translation into the promised outcomes is the unproven part. For a sense of how these secretagogue mechanisms sit within the broader family of growth-hormone-axis peptides, the related discussion of sermorelin, the parent GHRH(1-29) fragment, illustrates how much of this class shares the same mechanistic story and the same evidentiary caution.
From a GH Pulse to “Strength and Repair”: The Chain of Inference
It is worth making the chain of inference explicit, link by link, because seeing it laid out is the clearest way to understand why confident claims about Grow-H are premature.
Link 1: Grow-H raises GH pulses. This is the best-supported link. The synergy of GHRH analog plus GHRP is real and reproducible in the literature on the two classes.4 Reasonable confidence.
Link 2: Higher GH pulses raise IGF-1. Also well supported; repeated secretagogue dosing raises circulating IGF-1.1 Reasonable confidence.
Link 3: Higher IGF-1 increases contractile muscle protein and strength. This is where the chain frays. In healthy adults, growth hormone administration — a more direct and forceful intervention than a secretagogue — increases lean body mass on the scale but does so substantially through fluid retention, and controlled trials do not show a reliable increase in muscle strength or exercise performance attributable to new contractile tissue.56 Weak and partly contradicted.
Link 4: Higher GH/IGF-1 accelerates tissue repair. Partly true in a specific and limited sense — GH stimulates collagen synthesis in tendon and muscle connective tissue — but the same controlled work shows no effect on the contractile machinery, so “repair” here means connective-tissue matrix turnover, not muscle rebuilding.7 Narrow and easily overstated.
Link 5: What is true for exogenous GH is true for Grow-H’s amplified endogenous pulses. Untested. No one has run the trial. Even if links 1–4 held perfectly, this final extrapolation from “recombinant GH” to “this specific peptide blend, at research doses, in this population” is an assumption, not a finding.
The overall integrity of a chain is set by its weakest link, and this chain has two weak links (3 and 4) and one entirely missing one (5). That is the honest structure of the case for Grow-H boosting strength and repair: a solid mechanistic beginning, a contested middle, and an untested end. Anyone who presents the conclusion as established is treating the strong early links as if they carried the whole chain.
What the Evidence Actually Shows for the Individual Components
Because the blend has no studies of its own, the fairest thing we can do is examine what is genuinely known about each ingredient. The evidence is real but narrow, and almost none of it addresses strength or repair endpoints.
CJC-1295. The pivotal human pharmacology comes from Teichman and colleagues, who studied the DAC-bearing version in healthy adults across two randomized, placebo-controlled, double-blind ascending-dose trials.1 A single subcutaneous injection produced dose-dependent increases in mean plasma GH of 2- to 10-fold lasting six days or more, and increases in IGF-1 of 1.5- to 3-fold lasting nine to eleven days; with multiple doses, IGF-1 stayed above baseline for up to 28 days, and no serious adverse reactions were reported.1 This is genuinely important data — but note carefully what it measures and what it does not. It measures hormone concentrations. It does not measure muscle strength, muscle cross-sectional area, tendon healing, wound closure, body composition by DXA, or physical function. It establishes that CJC-1295 does what a GHRH analog is supposed to do to the hormone axis; it says nothing about downstream physical outcomes. It also studied the DAC version, whose pharmacokinetics differ dramatically from the no-DAC version in Grow-H.
Ipamorelin. The foundational work is Raun and colleagues’ 1998 characterization in rats and swine, which established ipamorelin as a potent, selective GH secretagogue — releasing GH comparably to GHRP-6 but without the ACTH and cortisol release that limits the older GHRPs.2 Subsequent preclinical work explored ipamorelin’s effects on bone and, in some models, on GH-dependent growth parameters. This is solid preclinical pharmacology. But again: it is largely animal work, it centers on the selectivity and potency of GH release, and it does not constitute human trials demonstrating strength gains or accelerated tissue repair. Ipamorelin has never been approved for any therapeutic indication, and its clinical development for one candidate use (postoperative ileus, exploiting the ghrelin-receptor effect on gut motility) did not result in an approved product.
The combination. The GHRH-plus-GHRP synergy is documented at the level of GH secretion.4 Reviews of GH secretagogues in the context of body composition note that such combinations can shift lean and fat mass in some settings, but they consistently emphasize that the human data specific to these secretagogue peptides for muscle and functional outcomes are limited and that much of the enthusiasm outruns the evidence.4 The specific pairing sold as Grow-H — CJC-1295 no-DAC 5 mg with ipamorelin 5 mg — has no dedicated clinical literature at all.
| Component | Class / receptor | Best human/preclinical evidence | What it does NOT show |
|---|---|---|---|
| CJC-1295 (no DAC) | GHRH analog / GHRH receptor | DAC version: dose-dependent GH and IGF-1 elevation in healthy adults1 | No strength, muscle-mass, or repair endpoints; no-DAC form less studied |
| Ipamorelin | GHRP / GHS-R1a (ghrelin receptor) | Selective, potent GH release without ACTH/cortisol spike (rats, swine)2 | No approved indication; no human strength/repair trials |
| Grow-H blend | GHRH analog + GHRP combination | Mechanistic synergy of the two classes on GH output4 | No trials of this blend for any endpoint |
The table makes the pattern unmistakable. Each ingredient has real pharmacology anchored to a small number of solid studies, every one of which stops at the hormone-secretion level. The strength-and-repair story lives entirely in the empty right-hand column.
The Missing Piece: No Trials of the Blend for Strength or Repair
This section is short because the honest answer is short. A search of the primary literature returns no randomized controlled trial, no controlled preclinical study, and no case series in which the Grow-H blend — or even the generic CJC-1295-no-DAC-plus-ipamorelin combination — was administered and strength, power, muscle mass, tendon or ligament healing, fracture repair, wound closure, or recovery from exercise was measured as an outcome. Not weak evidence; not mixed evidence; no evidence of that specific kind.
It is worth being precise about what this absence does and does not mean. It does not mean the blend is inert — it clearly raises GH and IGF-1, which are real biological effects. It does not mean the blend is dangerous — the short-term tolerability of the components in the studies that exist has been reasonable. What it means is narrower and more important: the specific claim embedded in the product’s name and in the title of this article — that it “truly boosts strength and repair” — has never been tested in the form in which the product is sold. Every confident assertion to that effect that a reader encounters online is an inference dressed as a finding, usually built by borrowing the reputation of growth hormone and stapling it to a compound that merely raises growth hormone.
There is also a subtler problem that a rigorous researcher would flag. Even the studies that do exist for the components mostly measured biomarkers over days to weeks, not functional outcomes over the months it would take for strength or connective-tissue remodeling to manifest and be measured against placebo. Strength is not a hormone concentration; it is a trainable, slowly changing property of the neuromuscular system, and demonstrating that any intervention improves it requires controlled resistance-training designs with objective strength testing, adequate duration, and blinding. None of that exists for Grow-H. The correct scientific posture toward the title’s question is therefore not skepticism for its own sake but calibrated agnosticism: the mechanism is plausible, the outcome is untested, and plausibility is not proof. For readers who want to see how a comparably GH-adjacent fragment has been examined against a genuine muscle endpoint — and found wanting — the analysis of whether AOD-9604 can aid recovery from muscle wasting is a useful companion piece in the same honest key.
What Growth Hormone Itself Does — and Doesn’t Do — for Muscle and Repair
Since the entire case for Grow-H rests on growth hormone being an effective builder of strength and an accelerator of repair, the most illuminating evidence is not about the peptides at all: it is about GH itself, which has been studied far more rigorously than any secretagogue. If GH — delivered directly, at pharmacological doses — does not reliably build functional strength in healthy people, then a peptide blend whose only job is to raise endogenous GH has a serious problem at the root of its rationale.
The most important human dataset is the randomized, placebo-controlled trial by Meinhardt and colleagues in 96 recreationally trained athletes. Eight weeks of growth hormone, alone or with testosterone, significantly reduced fat mass and increased lean body mass — but the increase in lean mass was largely water, and GH did not significantly improve muscle strength, power, or maximal aerobic capacity. The one performance measure that moved was sprint capacity, and even that finding was of uncertain durability and did not extend to strength.6 In other words, in the population most likely to benefit, GH changed the number on the scale without changing what the muscles could do.
The systematic review by Liu and colleagues in the healthy elderly reaches a convergent conclusion from a different population. Across the randomized trials of GH in older adults, the hormone produced small changes in body composition — a modest rise in lean mass, a modest fall in fat mass — but these were accompanied by high rates of adverse effects (joint swelling and pain, carpal tunnel syndrome, gynecomastia, and a trend toward new-onset diabetes or impaired glucose tolerance), and the review concluded that GH cannot be recommended as an anti-aging or functional therapy.5 Once again, the body-composition change was real but did not translate into a compelling functional benefit, and it came at a genuine safety cost.
The mechanistic reason for this disappointing pattern is beautifully clarified by Doessing and colleagues, who gave recombinant GH to healthy young people for 14 days and directly measured protein synthesis in tendon and muscle. GH markedly increased collagen synthesis in both tendon and the connective-tissue compartment of skeletal muscle — but it did not increase myofibrillar protein synthesis, the making of the actual contractile machinery.7 This single finding reorganizes the whole conversation. It tells us that GH’s effect on the musculotendinous system is real but is concentrated in the extracellular matrix — the collagen scaffold — rather than in the force-generating muscle fibers. That explains why GH can plausibly influence connective-tissue “repair” and tendon matrix turnover while failing to increase strength: it is building scaffolding, not engines.
| Growth-hormone effect | What controlled human data show | Relevance to “strength & repair” |
|---|---|---|
| Lean body mass (scale) | Increases, but substantially via fluid retention56 | Misleading proxy; not new contractile tissue |
| Muscle strength / power | No reliable improvement in healthy adults6 | Undercuts the core “strength” claim |
| Myofibrillar (contractile) protein synthesis | Not increased by 14 days of GH7 | No boost to force-generating machinery |
| Tendon / muscle collagen synthesis | Increased7 | Plausible connective-tissue “repair” effect only |
| Fat mass | Modest decrease56 | Real but unrelated to strength |
| Adverse effects | Edema, arthralgia, carpal tunnel, glucose intolerance5 | Nontrivial safety cost even short-term |
The synthesis is sobering for the Grow-H thesis. The best human evidence on growth hormone — the very outcome Grow-H is designed to elevate — shows that even direct, forceful GH administration produces cosmetic body-composition shifts and connective-tissue collagen turnover without delivering the functional strength gains the product name promises. A secretagogue blend that raises GH more gently and more briefly than injected recombinant GH is not positioned to do better than the hormone itself; if anything, it is positioned to do less. This does not prove Grow-H is useless for connective-tissue repair — the collagen-synthesis finding leaves a narrow, plausible door open there — but it strongly cautions against the strength claim and reframes “repair” as a matrix-remodeling hypothesis rather than a muscle-rebuilding fact.
How Grow-H Compares With Agents Actually Studied for Its Claims
A useful way to locate Grow-H on the evidence landscape is to set it beside compounds that have genuinely been taken into human trials for the outcomes Grow-H is marketed toward. The contrast is not a competition — Grow-H has never entered the arena — but it shows what an evidence-backed candidate looks like and how far the blend sits from that standard.
The most instructive comparator is tesamorelin, because it is a GHRH analog in the same mechanistic family as CJC-1295 and it is the only GH-secretagogue-class molecule with full FDA approval. Tesamorelin was studied in a 26-week randomized, double-blind, placebo-controlled trial of 412 patients with HIV-associated abdominal fat accumulation, where it reduced visceral adipose tissue by roughly 15–18% with an acceptable safety profile.8 That is what a GHRH-analog success story looks like: a large, rigorous, prospectively powered trial with a defined endpoint (visceral fat) that the drug actually moved. Note two things. First, the demonstrated benefit is metabolic (fat reduction), not strength or muscle repair. Second, achieving approval required exactly the kind of trial that Grow-H has never had. Tesamorelin shows both that this receptor pathway can yield a genuine, approvable clinical effect and that the effect proven so far is not the one Grow-H is sold for.
The recombinant growth hormone literature, discussed above, is the second comparator: heavily studied, and largely negative for functional strength in the non-deficient.56 A third useful contrast, for the “repair” half of the claim, is a compound like BPC-157, whose tissue-repair story rests almost entirely on rodent models and which, despite far more preclinical healing data than Grow-H, still lacks the controlled human trials needed to substantiate repair claims — a reminder that even compounds with a richer preclinical repair literature remain unproven in people. Readers exploring that comparison can consult the overview of what BPC-157 is and how its healing claims are framed.
| Agent | Mechanism | Highest level of evidence | Approved use? |
|---|---|---|---|
| Tesamorelin | GHRH analog | Phase 3 RCT, n=412, visceral-fat reduction8 | Yes — HIV lipodystrophy (FDA) |
| Recombinant GH | Direct GH receptor agonist | Multiple RCTs; body composition changes, no reliable strength gain56 | Yes — GH deficiency, specific wasting states |
| Sermorelin (GHRH 1-29) | GHRH analog (parent of modified GRF) | Historical diagnostic/pediatric use; brand withdrawn 2008 | Formerly (Geref); withdrawn |
| BPC-157 | Body-protection compound (repair) | Rodent models only; no controlled human trials | No |
| Grow-H (CJC-1295 + ipamorelin) | GHRH analog + GHRP combination | No trials of the blend for any endpoint | No |
The lesson embedded in this comparison is twofold. The GH-secretagogue pathway is capable of producing a real, approvable clinical effect — tesamorelin proves it — but that proven effect is fat reduction, achieved only through a large controlled trial, and it is not strength or muscle repair. And even growth hormone itself, the most direct possible intervention on this axis, has repeatedly failed to convert body-composition change into functional strength. Grow-H inherits the plausibility of this pathway and none of its proof. It sits at the bottom of the evidence hierarchy: a mechanistically reasonable combination with zero outcome data for the claims attached to it.
Dosing in a Research Context
Because Grow-H is sold for laboratory research and is not an approved therapeutic, there is no established, validated human dose, and nothing in this section should be read as a usage recommendation. What follows is a description of how the blend is typically presented and how reconstitution arithmetic works, offered for educational completeness and because dosing errors are a common source of confusion.
The pharmacology of the two components explains the frequent-dosing logic seen in research protocols. Because CJC-1295 without DAC has a short half-life — on the order of roughly 30 minutes, unlike the multi-day DAC version — its effect on GH is brief and must be re-triggered, which is precisely why it is combined with ipamorelin and dosed in a pulsatile fashion rather than weekly.1 This is a deliberate design choice: the no-DAC blend aims to amplify natural pulses at chosen times rather than flood the system with a flat, continuous GH elevation the way the DAC version or exogenous recombinant GH would. The distinction is not trivia; sustained non-pulsatile GH exposure is more strongly associated with the adverse-effect profile (edema, insulin resistance) seen in the GH literature, so the pulsatile rationale is partly a safety argument — though, again, one that has not been validated in controlled trials of this blend.
Reconstitution is where most practical error occurs, and the math is worth stating plainly. A 10 mg vial (5 mg CJC-1295 + 5 mg ipamorelin) reconstituted with a given volume of bacteriostatic water yields a concentration set entirely by that volume: the same peptide mass dissolved in a larger volume produces a lower concentration per unit volume. If 2 mL of diluent is added to the 10 mg vial, the solution contains 5 mg/mL of total peptide (2.5 mg/mL of each component); drawing 0.1 mL then contains 0.5 mg of total peptide. This is the arithmetic underlying any reconstitution chart, and it is where slips of a decimal place cause order-of-magnitude errors. Researchers documenting these calculations can work through the general method on the peptide reconstitution guide and check their figures with the reconstitution and dosage calculator, both of which present the concentration-and-volume relationship in worked form.
What no calculator can supply is an evidence-based dose for a strength or repair outcome, because no trial has established one. Any number circulating in forums or vendor literature for “muscle” or “recovery” dosing is an extrapolation from GH-secretion pharmacology or from anecdote, not a validated therapeutic dose. That gap — precise reconstitution arithmetic sitting atop a total absence of validated outcome dosing — is itself a fair summary of the compound’s status. The broader catalog of how these growth-hormone-axis peptides are organized for reference can be found through the site’s central dosages index.
Safety and Tolerability
The safety picture for Grow-H must be assembled from its components, because the blend itself has not been formally studied, and it should be read with the standing caveat that short-term tolerability in a small number of studies is not the same as established safety for repeated or long-term use.
In the CJC-1295 human pharmacology work, no serious adverse reactions were reported over the studied durations, and injection-site reactions were the most common complaint.1 Ipamorelin’s defining safety feature is its selectivity: unlike older GHRPs, it releases GH without meaningfully raising cortisol, ACTH, or prolactin, which removes one class of concern.2 Those are genuinely reassuring features as far as they go. But the relevant safety questions for a compound that chronically elevates the GH/IGF-1 axis are not answered by short pharmacology studies, and the growth-hormone literature supplies the cautions that the secretagogue literature has not yet had the trials to address:
- Fluid retention and joint symptoms. Elevated GH characteristically causes edema, arthralgia, and carpal-tunnel-type symptoms; these were prominent adverse effects in the GH trials in older adults.5 A secretagogue that raises GH can be expected to carry a version of this risk.
- Glucose and insulin sensitivity. GH is a counter-regulatory, insulin-antagonizing hormone; chronic elevation can impair glucose tolerance and push toward insulin resistance, a trend seen in the elderly GH review.5 This is the single most important metabolic caution for any GH-raising intervention.
- IGF-1 and theoretical proliferation risk. IGF-1 is mitogenic, and sustained elevation raises theoretical concerns relevant to occult malignancy; this is a reason approved GH-axis therapies are used under monitoring and contraindicated in active cancer.
- Cardiovascular context. The one death in a CJC-1295-DAC trial was a cardiovascular event that the attending physician attributed to pre-existing coronary disease and considered unrelated to treatment, and no subsequent studies have linked CJC-1295 to cardiac events — but the episode is a reminder that these compounds have been given to medically complex populations and that safety cannot be assumed across contexts.9
- Product-quality risk. Material sold as “research chemical” varies in purity, sterility, and accuracy of labeling. Endotoxin, impurities, and mis-dosed vials are real hazards independent of the molecules’ intrinsic pharmacology.
- Anti-doping prohibition. Growth-hormone secretagogues, including GHRH analogs and GHRPs, are prohibited in sport by the World Anti-Doping Agency at all times; for any competitive athlete this is a categorical hazard regardless of pharmacology.10
The balanced reading is that the components have not produced alarming short-term safety signals in the limited studies available, and ipamorelin’s selectivity is a real advantage over older GHRPs. But “no alarming signal in short studies” is a low bar, and the predictable consequences of chronically raising the GH/IGF-1 axis — fluid retention, glucose intolerance, and the theoretical IGF-1 concerns — have simply not been characterized for this blend over meaningful durations. Absence of demonstrated harm and absence of demonstrated benefit coexist here, which is exactly the situation that should counsel caution rather than confidence.
Handling and Reconstitution in a Research Setting
Grow-H is supplied as a lyophilized (freeze-dried) powder, a form chosen for stability during shipping and storage. A brief, strictly educational note on laboratory handling is warranted, with the emphasis that this is standard research-peptide practice and not a recommendation for human use.
Lyophilized peptides are reconstituted with sterile or bacteriostatic water for laboratory purposes. The diluent is directed slowly against the inner wall of the vial rather than sprayed onto the powder, and the vial is swirled gently rather than shaken, because vigorous agitation can shear peptide bonds and cause foaming that denatures material. Both peptides in the blend are relatively robust as lyophilized powders but sensitive once in solution, so post-reconstitution handling is where activity is most easily lost.
| Parameter | Typical research-context practice |
|---|---|
| Lyophilized storage | Cool and dark; long-term stability favored by freezing |
| After reconstitution | Refrigerated (2–8 °C); used within a limited window |
| Diluent | Bacteriostatic water for multi-draw practice; sterile water for single use |
| Light and heat | Minimize exposure; both degrade peptides in solution |
| Agitation | Swirl gently; never shake or foam |
| Freeze-thaw | Repeated cycles degrade peptides; avoid re-freezing reconstituted solution |
| Sterility | Aseptic technique throughout |
It bears repeating that meticulous handling changes nothing about the evidence question. A perfectly reconstituted, high-purity vial of Grow-H is still a blend with zero outcome trials for strength or repair. Good technique preserves whatever biological activity the peptides have; it does not manufacture efficacy where none has been demonstrated. The distinction between doing the chemistry carefully and knowing whether the compound works is the whole of the matter, and the two are independent.
Regulatory Status
The regulatory picture for Grow-H is straightforward once its components are examined, and it is frequently misrepresented in marketing, so precision matters.
No therapeutic approval. Neither CJC-1295 nor ipamorelin is approved by the U.S. Food and Drug Administration, the European Medicines Agency, or any comparable regulator for any condition, and the Grow-H blend has no approval anywhere. The DAC version of CJC-1295 reached Phase 2 for HIV-associated lipodystrophy under ConjuChem but development was discontinued; ipamorelin’s clinical development did not yield an approved product.9 There is, correspondingly, no approved indication of any kind — certainly none for strength or repair.
U.S. compounding status. The regulatory trajectory of these peptides in the United States has been turbulent and is a clear signal of official caution. In September 2023 the FDA placed both CJC-1295 and ipamorelin into “Category 2” of its bulk-drug-substances review — the category for substances that may present significant safety risks — citing concerns including immunogenicity, aggregation, sterility, and insufficient clinical evidence.11 The agency subsequently removed them from that specific category in 2024 after the nominators withdrew their nominations — a procedural withdrawal, not a safety clearance — and they were never added to the approved list; the Pharmacy Compounding Advisory Committee process has not sanctioned their inclusion, leaving them in regulatory limbo rather than approval.11 The relevant point for a reader is that U.S. regulators have expressed documented concern about exactly these substances and have not endorsed their use.
Sermorelin as a cautionary parallel. Even the parent GHRH(1-29) fragment, sermorelin, which was once an FDA-approved product (Geref, for diagnostic use and pediatric GH deficiency), had its brand withdrawn in 2008, and all sermorelin available today is compounded rather than FDA-approved as a finished drug. If the well-characterized parent molecule no longer carries approval, the modified analog in Grow-H — which has never had it — certainly does not.
Anti-doping. Growth-hormone-releasing factors and their analogs, and GH secretagogues generally, are on the World Anti-Doping Agency’s Prohibited List under the peptide-hormones and growth-factors category, banned in and out of competition.10 Any athlete subject to WADA-compliant testing should assume that use of Grow-H constitutes an anti-doping rule violation.
A recurring source of confusion deserves explicit correction: the fact that a compound is sold openly as a “research peptide” is not a regulatory endorsement of any kind. “For research use only” is a commercial and legal framing that specifically disclaims human use; it is the opposite of an approval. Conflating easy availability with legitimacy — “if I can buy it, it must be established” — is one of the most common errors in this space, and it is precisely the gap that the honest reading of Grow-H is meant to close. The regulatory synthesis is clean: Grow-H is an unapproved combination of two unapproved research peptides, viewed with documented caution by U.S. regulators, banned in sport, and carrying no sanctioned therapeutic use for any indication, let alone the strength and repair its name implies.
Frequently Asked Questions
Does the Grow-H blend actually boost strength and repair?
There is no clinical evidence that it does. Grow-H (CJC-1295 no-DAC plus ipamorelin) reliably raises growth hormone and IGF-1, but no controlled trial of this blend has ever measured strength, muscle mass, or tissue repair.124 The claim rests on inference from growth hormone’s reputation, and that reputation is itself qualified: controlled trials show that even direct GH administration does not reliably increase muscle strength in healthy adults and that its lean-mass effect is largely fluid retention.56 The honest answer is that this is an untested hypothesis, not a demonstrated effect.
What exactly is in Grow-H?
Grow-H is most commonly a 10 mg vial containing 5 mg of CJC-1295 without DAC (a GHRH analog, also called modified GRF 1-29) and 5 mg of ipamorelin (a selective growth-hormone-releasing peptide that acts on the ghrelin receptor).12 The two are combined because a GHRH analog and a GHRP act through different receptors and together produce a larger GH pulse than either alone.4
How is CJC-1295 “no DAC” different from CJC-1295 with DAC?
The DAC (Drug Affinity Complex) version binds to albumin and has a half-life of roughly 6–8 days, producing sustained, non-pulsatile GH and IGF-1 elevation for weeks.1 The no-DAC version in Grow-H has a half-life of about 30 minutes and is used to amplify natural GH pulses briefly, which is why it is paired with ipamorelin and dosed frequently rather than weekly. They are pharmacokinetically very different molecules despite the shared name.
Has this specific blend been studied in humans?
No. There is no published clinical trial or controlled preclinical study of the Grow-H blend, or of the generic CJC-1295-no-DAC-plus-ipamorelin combination, measuring any strength, muscle, or repair endpoint. The evidence that exists concerns the individual components and stops at the level of GH and IGF-1 secretion.12
Does growth hormone build muscle and heal tissue?
Less than its reputation suggests. In controlled human work, GH increases collagen synthesis in tendon and muscle connective tissue but does not increase myofibrillar (contractile) protein synthesis, and it does not reliably improve muscle strength in healthy adults.67 So GH may plausibly influence connective-tissue matrix “repair,” but the evidence does not support it as a builder of functional strength — a crucial distinction for evaluating any GH-raising compound.
Is Grow-H approved or legal?
It is not approved as a drug by the FDA, EMA, or any comparable regulator for any condition. Both components were flagged by the FDA in 2023 as bulk substances that may present significant safety risks, and neither has been sanctioned for compounding.11 Growth-hormone secretagogues are also prohibited in sport by WADA.10 It is sold “for research use only,” which is a disclaimer of human use, not an endorsement.
Is Grow-H safe?
Its short-term tolerability in the limited studies of the individual components has been reasonable, and ipamorelin’s selectivity avoids the cortisol and prolactin spikes of older GHRPs.2 But chronically raising the GH/IGF-1 axis carries predictable concerns — fluid retention, joint symptoms, impaired glucose tolerance, and theoretical IGF-1-related proliferation risk — that have not been characterized for this blend over meaningful durations.5 Short-term tolerability is not the same as established long-term safety.
How does Grow-H compare with tesamorelin?
Tesamorelin is a GHRH analog in the same family that is FDA-approved, but only after a large Phase 3 trial and only for reducing visceral fat in HIV-associated lipodystrophy — not for strength or muscle repair.8 The comparison shows both that this receptor pathway can produce a genuine, approvable effect and that the proven effect is metabolic, achieved through rigorous trials that Grow-H has never undergone.
Why do so many sources claim Grow-H builds muscle?
Because it is easy to borrow growth hormone’s anabolic reputation and attach it to a compound that raises growth hormone, while skipping the step of asking whether that elevation produces measurable strength. The chain “GH builds muscle → Grow-H raises GH → Grow-H builds muscle” sounds airtight but has a weak middle link (GH’s real strength effect is small to absent) and a missing final link (no trial of the blend).67
References
- Teichman SL, Neale A, Lawrence B, Gagnon C, Castaigne JP, Frohman LA. Prolonged stimulation of growth hormone (GH) and insulin-like growth factor I secretion by CJC-1295, a long-acting analog of GH-releasing hormone, in healthy adults. J Clin Endocrinol Metab. 2006;91(3):799-805. PMID: 16352683. https://pubmed.ncbi.nlm.nih.gov/16352683/
- Raun K, Hansen BS, Johansen NL, et al. Ipamorelin, the first selective growth hormone secretagogue. Eur J Endocrinol. 1998;139(5):552-561. PMID: 9849822. https://pubmed.ncbi.nlm.nih.gov/9849822/
- Kojima M, Hosoda H, Date Y, Nakazato M, Matsuo H, Kangawa K. Ghrelin is a growth-hormone-releasing acylated peptide from stomach. Nature. 1999;402(6762):656-660. PMID: 10604470. https://pubmed.ncbi.nlm.nih.gov/10604470/
- Sigalos JT, Pastuszak AW. The safety and efficacy of growth hormone secretagogues. Sex Med Rev. 2018;6(1):45-53. PMID: 28189979. PMCID: PMC5632578. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5632578/
- Liu H, Bravata DM, Olkin I, et al. Systematic review: the safety and efficacy of growth hormone in the healthy elderly. Ann Intern Med. 2007;146(2):104-115. PMID: 17227934. https://pubmed.ncbi.nlm.nih.gov/17227934/
- Meinhardt U, Nelson AE, Hansen JL, et al. The effects of growth hormone on body composition and physical performance in recreational athletes: a randomized trial. Ann Intern Med. 2010;152(9):568-577. PMID: 20439575. https://pubmed.ncbi.nlm.nih.gov/20439575/
- Doessing S, Heinemeier KM, Holm L, et al. Growth hormone stimulates the collagen synthesis in human tendon and skeletal muscle without affecting myofibrillar protein synthesis. J Physiol. 2010;588(Pt 2):341-351. PMID: 20123793. https://pubmed.ncbi.nlm.nih.gov/20123793/
- Falutz J, Allas S, Blot K, et al. Metabolic effects of a growth hormone-releasing factor in patients with HIV. N Engl J Med. 2007;357(23):2359-2370. PMID: 18057338. https://pubmed.ncbi.nlm.nih.gov/18057338/
- aidsmap (NAM). Lipodystrophy study halted after patient death (ConjuChem CJC-1295 Phase 2). 2006. https://www.aidsmap.com/news/jul-2006/lipodystrophy-study-halted-after-patient-death
- World Anti-Doping Agency. The Prohibited List: S2 Peptide Hormones, Growth Factors, Related Substances and Mimetics. https://www.wada-ama.org/en/prohibited-list
- U.S. Food and Drug Administration. Certain bulk drug substances for use in compounding that may present significant safety risks (Category 2 review; CJC-1295 and ipamorelin). https://www.fda.gov/drugs/human-drug-compounding/certain-bulk-drug-substances-use-compounding-may-present-significant-safety-risks
Educational and research-use disclaimer: This article is provided solely for scientific and educational purposes. Grow-H (a blend of CJC-1295 without DAC and ipamorelin) is not approved by the FDA, EMA, or any comparable regulator for the treatment, cure, or prevention of any disease, and no human clinical trial has demonstrated that it boosts strength or accelerates tissue repair. Nothing here is medical advice or a recommendation for human use. Growth-hormone secretagogues are prohibited in sport by WADA. Any legitimate investigation of these compounds should occur within properly authorized preclinical or clinical research under appropriate oversight. Readers should consult qualified professionals and applicable regulations before making any decisions.