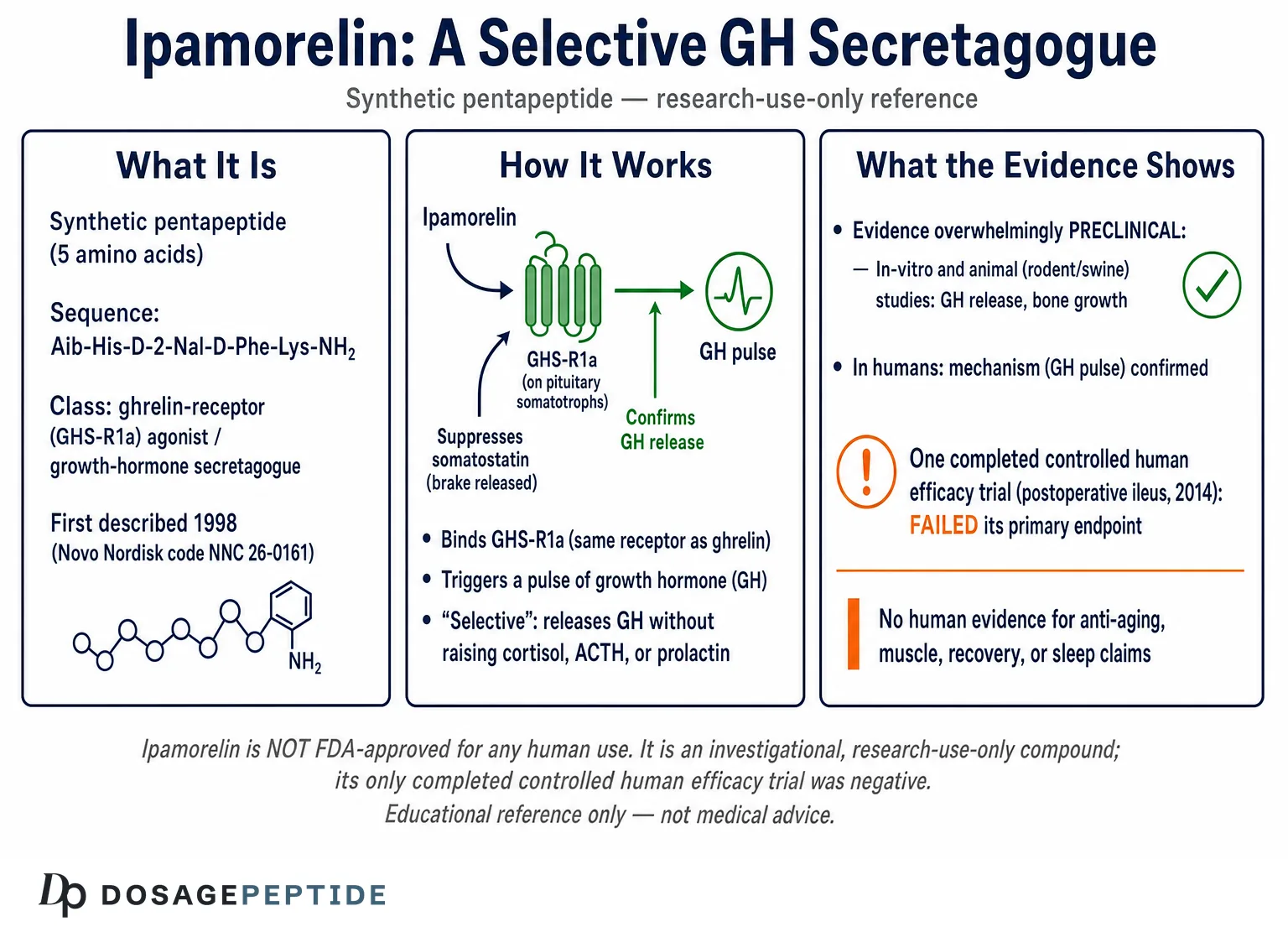
Ipamorelin is a synthetic pentapeptide growth-hormone secretagogue that selectively activates the ghrelin receptor (GHS-R1a) to trigger a pulse of growth hormone (GH) from the pituitary, and it has become one of the most studied research peptides in the growth hormone and anti-aging category. This reference examines what is actually known about Ipamorelin — its structure, its selective mechanism of action, and the honest state of the evidence, which is overwhelmingly preclinical with a single completed human trial that failed its primary endpoint. Throughout, the framing is research and educational: Ipamorelin is not approved by the FDA for any human therapeutic use and is handled only as an investigational, research-use-only compound.
What is Ipamorelin?
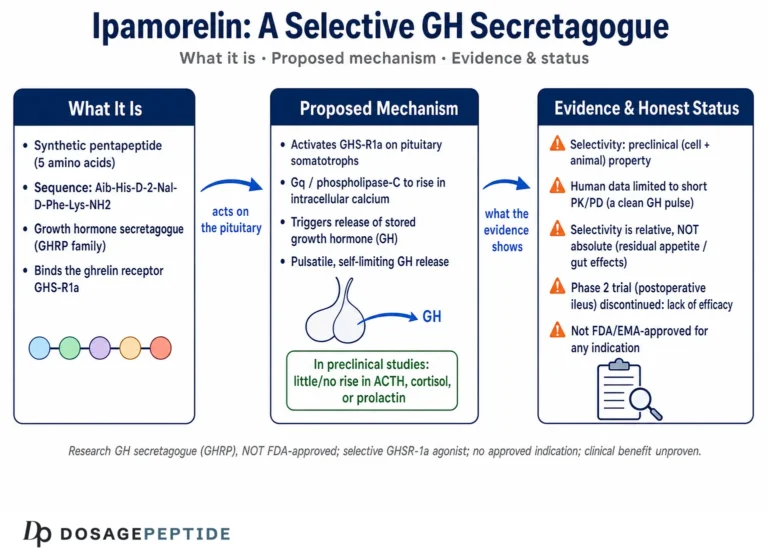
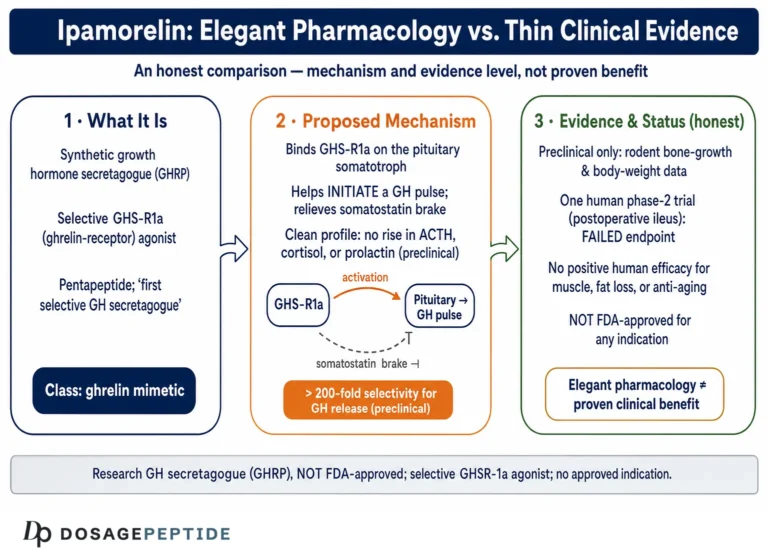
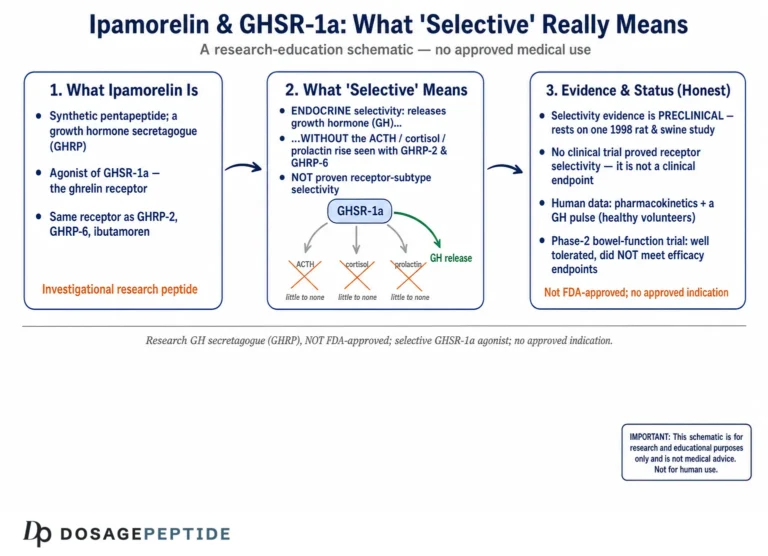
Ipamorelin is a short synthetic peptide belonging to the class of compounds called growth-hormone secretagogues (GHSs) — molecules that prompt the somatotroph cells of the anterior pituitary to release stored growth hormone. It was first described in 1998 by Raun and colleagues at Novo Nordisk, who titled their paper “Ipamorelin, the first selective growth hormone secretagogue.”[1] The word “selective” is the defining feature of the molecule and the reason it remains a reference compound decades later: unlike the earlier growth-hormone-releasing peptides (GHRPs), Ipamorelin releases GH without meaningfully disturbing the other pituitary hormones.
The compound carried the internal development code NNC 26-0161 during its pharmaceutical program at Novo Nordisk. It was later licensed and advanced into human clinical testing by Helsinn Therapeutics for a gastrointestinal indication, postoperative ileus, before development was discontinued. Today, having never reached market as a medicine, Ipamorelin is encountered almost exclusively as a research peptide.
Its enduring interest is easy to explain. The GH secretagogue field spent the 1980s and 1990s searching for a compound that could raise growth hormone the way GHRH does — cleanly, without the collateral endocrine effects of the first-generation GHRPs. Ipamorelin was the first molecule to achieve that goal, which is why its 1998 description carried the word “first” in the title. That historical primacy, combined with an unusually thorough characterization dataset, is why Ipamorelin remains the reference selective ghrelin mimetic against which newer compounds are compared, even though it never became a drug.
How Ipamorelin fits into the growth hormone peptide family
The peptides that raise GH split into two mechanistic families, and understanding the split is essential to reading any Ipamorelin literature accurately:
- GHRH analogs (sermorelin, CJC-1295, tesamorelin) mimic growth-hormone-releasing hormone and act at the GHRH receptor. They amplify the amplitude of natural GH pulses.
- Ghrelin mimetics / GHRPs (Ipamorelin, GHRP-2, GHRP-6, hexarelin) mimic the stomach hormone ghrelin and act at the ghrelin receptor GHS-R1a. They initiate a GH pulse and also suppress somatostatin, the brake on GH release.
Ipamorelin sits firmly in the second family. Its distinguishing trait within that family is a clean hormonal profile: it captures the GH-releasing potency of the GHRPs while shedding almost all of their off-target endocrine effects.
This distinction is not academic. GHRH analogs and ghrelin mimetics differ in half-life, in the shape of the GH response they produce, in their side-effect liabilities, and in their regulatory status. Confusing the two families — for example, treating Ipamorelin as if it were a GHRH analog like tesamorelin — leads directly to misreading the evidence, because a study on one class says little about the other. Keeping the two arms straight is the single most useful framework for evaluating any claim in this space.
What is the chemical structure of Ipamorelin?
Ipamorelin is a pentapeptide — a chain of five amino acid residues — with a C-terminal amide. Its sequence is Aib-His-D-2-Nal-D-Phe-Lys-NH2, where Aib is the non-natural amino acid alpha-aminoisobutyric acid, D-2-Nal is D-2-naphthylalanine, and the terminal residues are stabilized as an amide rather than a free carboxyl.[2] The presence of D-amino acids and the unnatural Aib and 2-naphthylalanine residues is deliberate: these substitutions resist enzymatic breakdown and lock the molecule into a conformation that fits the ghrelin receptor while avoiding the receptors responsible for the earlier GHRPs’ side effects.
Raun and colleagues arrived at this structure by working from GHRP-1 and systematically removing the central Ala-Trp dipeptide, a modification that preserved GH-releasing potency while dramatically improving selectivity.[1]
| Property | Value |
|---|---|
| Peptide class | Synthetic pentapeptide; ghrelin-receptor (GHS-R1a) agonist / GH secretagogue |
| Amino acid sequence | Aib-His-D-2-Nal-D-Phe-Lys-NH2 |
| Molecular formula | C38H49N9O5 |
| Molecular weight | ~711.9 g/mol |
| CAS number | 170851-70-4 |
| Development code | NNC 26-0161 (Novo Nordisk) |
| Reported plasma half-life | ~2 hours (research reports) |
| Routes studied | Intravenous and subcutaneous (research/experimental) |
The molecular weight (~712 g/mol) and formula (C38H49N9O5) are consistent across pharmacological reference databases.[2] The reported plasma half-life of roughly two hours is longer than that of the very short-acting GHRH fragment sermorelin but far shorter than the multi-day depot behavior of CJC-1295 with DAC.
How does Ipamorelin work? Mechanism of action
Ipamorelin is an agonist of the growth-hormone secretagogue receptor type 1a (GHS-R1a), the same receptor targeted by the endogenous hormone ghrelin. Understanding the mechanism requires briefly tracing the receptor’s discovery, because the pharmacology came before the biology.
The ghrelin receptor: from synthetic secretagogues to a natural hormone
The GHS-R was cloned in 1996 by Howard and colleagues, who identified an orphan G-protein-coupled receptor in the pituitary and hypothalamus through which synthetic GH secretagogues acted.[3] At the time the receptor had no known natural ligand. Three years later, in 1999, Kojima and colleagues purified that natural ligand from stomach tissue and named it ghrelin — a 28-amino-acid acylated peptide whose octanoyl modification at serine-3 is essential for activity.[4] This sequence — synthetic drug first, receptor second, natural hormone third — is a textbook example of reverse pharmacology, and it means Ipamorelin is best understood as a synthetic ghrelin mimetic.
Signaling: how GHS-R1a activation releases growth hormone
GHS-R1a is a Gq/11-coupled receptor. When Ipamorelin binds, it activates phospholipase C (PLC), which generates inositol trisphosphate (IP3) and diacylglycerol. IP3 mobilizes calcium from intracellular stores, and the resulting rise in intracellular calcium in the somatotroph triggers exocytosis of stored growth hormone.[5] A notable feature of GHS-R1a is its unusually high constitutive activity: the receptor signals at roughly 50% of its maximal capacity even in the absence of any ligand, a property that has physiological consequences for baseline GH tone.[5]
Beyond directly stimulating the somatotroph, ghrelin-receptor agonists act at the hypothalamus to inhibit somatostatin, the hormone that normally restrains GH secretion. By simultaneously pushing on the accelerator (direct pituitary stimulation) and easing off the brake (somatostatin suppression), Ipamorelin produces a discrete, pulsatile release of GH rather than a flat, sustained elevation. This preservation of pulsatility is one reason ghrelin mimetics are of research interest — natural GH secretion is pulsatile, and pulsatility appears important to downstream signaling.
Why is Ipamorelin called “selective”?
This is the central and best-documented property of Ipamorelin. In the original characterization, Raun and colleagues showed that in conscious swine, Ipamorelin released GH with potency comparable to GHRP-6, but — critically — without co-releasing adrenocorticotropic hormone (ACTH), cortisol, prolactin, follicle-stimulating hormone (FSH), luteinizing hormone (LH), or thyroid-stimulating hormone (TSH), even at doses far above the threshold needed for GH release.[1] This distinguishes it sharply from GHRP-6 and hexarelin, which reliably raise cortisol, prolactin, and appetite alongside GH.
The molecular basis for this selectivity is thought to lie in the specific residue substitutions that let Ipamorelin engage the GH-releasing pathway of GHS-R1a while avoiding the receptor interactions that drive ACTH and prolactin output. For researchers, this clean profile is the entire appeal of the molecule: it isolates the GH-releasing effect of ghrelin-receptor agonism from the confounding stress-hormone and appetite effects of older GHRPs.
What about ghrelin’s other effects — appetite and metabolism?
Ghrelin itself is far more than a GH secretagogue; it is the body’s principal orexigenic (appetite-stimulating) hormone, rising before meals and signaling hunger through GHS-R1a in the hypothalamic arcuate nucleus. The ghrelin receptor is also expressed in the pancreas, gastrointestinal tract, cardiovascular tissue, and brain reward circuits, which is why endogenous ghrelin influences energy balance, gastric motility, insulin secretion, and even mood.[4] A synthetic agonist at this receptor could, in principle, touch any of these systems. In the original characterization, however, Ipamorelin was noted for not driving the pronounced appetite response seen with GHRP-6, which suggests its engagement of the receptor is biased toward the GH-releasing signaling output.[1] The mechanistic implication — a ghrelin-receptor agonist that releases GH without strongly triggering hunger — is a large part of why Ipamorelin is treated as a distinct research tool rather than just another GHRP.
It was precisely ghrelin’s effect on gut motility that motivated the one human efficacy program: postoperative ileus is a condition of impaired gastrointestinal motility after surgery, and a ghrelin mimetic was a mechanistically reasonable candidate to accelerate recovery of gut function. That the trial failed on its motility-related endpoint is therefore doubly informative — it is a negative result on the one indication most directly aligned with the receptor’s known biology.
How does the growth hormone axis work, and where does Ipamorelin act?
To interpret any Ipamorelin claim, it helps to understand the system the peptide is nudging. Growth hormone secretion is not a simple on/off switch; it is a tightly regulated, pulsatile output governed by opposing hypothalamic signals and a downstream feedback loop through the liver.
The three-hormone control system
Somatotroph cells in the anterior pituitary release GH under the control of two hypothalamic hormones that pull in opposite directions. Growth-hormone-releasing hormone (GHRH) stimulates GH secretion, while somatostatin (SST) inhibits it.[12] Ghrelin — and the synthetic ghrelin mimetics like Ipamorelin — adds a third input, acting through GHS-R1a to both stimulate the somatotroph directly and blunt somatostatin’s inhibitory tone. This is why ghrelin-receptor agonists and GHRH act on genuinely separate arms of the same axis, and why they can be complementary.
The net output of this system is pulsatile. In healthy adults, roughly 6 to 12 discrete GH pulses occur over 24 hours, with the largest burst typically arriving 60 to 90 minutes after sleep onset.[12] Between pulses, GH falls to very low levels. This pulsatility is not incidental — downstream tissues read the pattern of GH exposure, not just the average level, which is one reason researchers find secretagogues that preserve pulsatile release (like Ipamorelin) mechanistically interesting compared with exogenous recombinant GH, which produces a flat, non-physiological elevation.
The GH–IGF-1 loop and negative feedback
Once released, GH travels to peripheral tissues and binds the GH receptor, activating the JAK2/STAT5 signaling pathway. The dominant downstream response is production of insulin-like growth factor 1 (IGF-1), roughly three-quarters of which is generated by the liver.[13] IGF-1 mediates many of the anabolic, growth-promoting effects classically attributed to GH. IGF-1 also closes a negative-feedback loop: rising IGF-1 stimulates somatostatin release and suppresses both GH and GHRH, keeping the system in check.[13]
This feedback architecture has an important implication for how ghrelin mimetics behave. Because Ipamorelin works upstream, on the pituitary and hypothalamus, its GH-releasing effect is still constrained by the body’s own somatostatin brake and IGF-1 feedback. In principle, this makes it self-limiting in a way that directly injected GH is not — a theoretical safety consideration frequently cited in the research rationale for secretagogues, though not one that has been settled by controlled long-term human data.
Somatopause: the age-related decline the axis undergoes
The GH/IGF-1 axis does not stay constant across the lifespan. GH secretion declines progressively with age — on the order of roughly 14% per decade after age 30 in commonly cited estimates — with a parallel fall in circulating IGF-1, a phenomenon termed somatopause.[13] The decline is driven largely by central neuroendocrine changes: the aging hypothalamus tends to produce less GHRH and more somatostatin, and pituitary responsiveness to secretagogues diminishes. This age-related decline is the biological backdrop against which GH secretagogues are studied in the anti-aging and longevity literature.
It is essential to be careful here. The existence of somatopause explains why researchers are interested in agents that can raise GH in older organisms; it does not establish that raising GH with Ipamorelin improves healthspan, body composition, or any hard outcome in humans. The GH/IGF-1 axis in aging is genuinely complex — higher IGF-1 signaling is associated with growth and repair but also, in some models, with reduced longevity — and this tension is an unresolved question, not a settled benefit.[13]
What does the evidence actually show? An honest review by study type
The single most important thing to understand about Ipamorelin is the shape of its evidence base. It is overwhelmingly preclinical. There is a rich body of in-vitro and animal data, one small early-human GH-stimulation program, and exactly one completed, published, controlled human efficacy trial — which was negative. Below, the evidence is separated by tier and labeled honestly.
In-vitro evidence
The foundational work established Ipamorelin’s pharmacology at the cellular level. In the original Raun study, Ipamorelin displaced radioligand binding at the pituitary GHS receptor and released GH from primary rat pituitary cells in culture, demonstrating that it acts directly at the pituitary somatotroph and not solely through central mechanisms.[1] This receptor-level and cell-level work defines how the peptide works but says nothing about clinical benefit in humans.
Animal evidence
The animal literature is the strongest part of Ipamorelin’s evidence base, and it is genuinely substantial — but it is animal data, and it must not be read as proof of human effect.
- GH release in swine. In conscious pigs, Ipamorelin released GH dose-dependently with an ED50 in the low-nanomole-per-kilogram range and a clean hormonal profile as described above.[1]
- Longitudinal bone growth in rats. Johansen and colleagues (1999) reported that Ipamorelin administered three times daily for 15 days produced dose-dependent increases in longitudinal bone growth rate in female rats — from about 42 µm/day in vehicle controls to as much as 52 µm/day at higher doses — along with dose-dependent body-weight gain.[6]
- Bone mineral content in rats. Svensson and colleagues (2000) found that Ipamorelin (0.5 mg/kg/day) and GHRP-6 both increased bone mineral content in young adult female rats over 12 weeks, measured serially in vivo by dual-energy X-ray absorptiometry.[7]
- Counteracting glucocorticoid bone loss in rats. Andersen and colleagues (2001) reported that in a rat model of glucocorticoid-induced catabolism, combining Ipamorelin with the glucocorticoid raised the periosteal bone-formation rate roughly four-fold compared with glucocorticoid alone.[8]
Taken together, these rodent studies show a coherent, GH-mediated anabolic signal on bone and body weight in animals. They are the reason Ipamorelin is often discussed in the context of bone and body composition — but every one of these findings is in rats or pigs, not humans.
The bone findings deserve a careful read because they are frequently overstated. In the longitudinal-growth study, the effect was real but modest — growth rate rose from about 42 to 52 µm/day at the top dose — and, notably, IGF-1 levels and standard bone-metabolism markers were not significantly altered, suggesting the effect was driven by intermittent GH pulses rather than a sustained rise in systemic IGF-1.[6] The glucocorticoid study is arguably the most clinically suggestive of the animal work: glucocorticoids are a well-known cause of bone loss in humans, and Ipamorelin’s roughly four-fold restoration of periosteal bone-formation rate in glucocorticoid-treated rats points to a plausible protective mechanism — but again, this is a rat model and has never been reproduced in a human trial.[8]
It is also worth appreciating the design quality of the selectivity work in swine, because it is what elevates Ipamorelin above other GHRPs in the literature. Rather than simply measuring GH, Raun and colleagues measured a full panel of pituitary hormones after escalating doses, and demonstrated that even at exposures far above the GH-releasing threshold, ACTH, cortisol, prolactin, and the gonadotropins stayed flat.[1] A selective effect that holds across a wide dose range is a much stronger claim than selectivity observed at a single dose, and it is the empirical backbone of Ipamorelin’s reputation.
Human evidence: limited and, on efficacy, negative
Human data on Ipamorelin are sparse. During its pharmaceutical development the compound was shown to raise plasma GH in humans, consistent with its mechanism, and early tolerability was acceptable enough to justify further trials.[2] The one completed, published, controlled efficacy trial was Helsinn’s Phase II study in postoperative ileus (POI), reported by Beck and colleagues in 2014.[9]
In that randomized, double-blind, placebo-controlled proof-of-concept trial (registered as NCT00672074), adults undergoing open or laparoscopic bowel resection received intravenous Ipamorelin 0.03 mg/kg or placebo twice daily for up to seven postoperative days.[10] The primary endpoint was time to tolerance of a solid meal. The result was negative: median time to first tolerated meal was 25.3 hours with Ipamorelin versus 32.6 hours with placebo, a difference that did not reach statistical significance (p=0.15), and there were no significant differences in the key or secondary efficacy analyses.[9] On the safety side, Ipamorelin was well tolerated, with treatment-emergent adverse events occurring at a similar or slightly lower rate than placebo. Development for this indication was subsequently discontinued for lack of efficacy.[2]
A few details of the POI trial are worth drawing out because they are instructive about how to weigh Ipamorelin evidence generally. First, the numerical trend actually favored Ipamorelin — 25.3 versus 32.6 hours to first tolerated meal — but the difference did not reach statistical significance, meaning it could not be distinguished from chance at the study’s sample size.[9] A non-significant trend is not evidence of efficacy; it is an inconclusive result that, in a proof-of-concept design, is treated as a failure to demonstrate benefit. Second, an exploratory subgroup analysis suggested any signal was limited to patients undergoing open (rather than laparoscopic) procedures — the kind of post-hoc observation that generates hypotheses but cannot confirm them. Third, the tolerability data are genuinely useful: a defined IV dose given twice daily for up to a week produced adverse events at a rate comparable to placebo, which is a real, if narrow, human safety data point.[10]
The honest summary of human evidence is therefore: Ipamorelin does what its mechanism predicts (it raises GH) and was reasonably well tolerated in a short IV course, but the only controlled clinical efficacy trial failed to demonstrate benefit for its studied indication. There are no completed controlled human trials supporting the anti-aging, body-composition, recovery, or longevity uses for which Ipamorelin is popularly discussed. Anyone citing Ipamorelin as “clinically proven” for any purpose is misreading the record.
What research models are used to study Ipamorelin?
The methods behind the studies above illustrate how GH secretagogues are characterized and are useful for interpreting any Ipamorelin claim.
- Receptor binding assays. Radioligand displacement at the cloned GHS-R1a establishes affinity and selectivity versus related receptors.
- Primary pituitary cell culture. Isolated rat somatotrophs are used to measure direct, in-vitro GH release and to separate pituitary effects from hypothalamic ones.
- Conscious large-animal models (swine). Pigs were the key model for Raun’s selectivity work because their neuroendocrine responses allow simultaneous measurement of GH, ACTH, cortisol, prolactin, and gonadotropins after a single agent.[1]
- Rodent models with DXA and bone histomorphometry. Osmotic minipumps or repeated subcutaneous injection deliver the peptide, and dual-energy X-ray absorptiometry plus histomorphometry quantify bone mineral content and formation rate.[7]
- Randomized controlled human trials. The POI program used the gold-standard design — randomized, double-blind, placebo-controlled — with an objective functional endpoint (time to tolerated meal).[9]
Each model answers a different question, and confusing them is the commonest error in peptide claims. A receptor binding assay tells you the compound engages GHS-R1a; it cannot tell you whether that produces a physiological benefit. A rodent bone study tells you GH-mediated anabolism occurs in a rat; it cannot tell you the same happens in a human. Only the randomized human trial can speak to clinical efficacy, and for Ipamorelin that single trial was negative. Reading the evidence in this layered way — in-vitro establishes mechanism, animal establishes biological plausibility, human establishes clinical effect — is the discipline that separates an honest assessment from marketing.
The reverse-pharmacology story and why it matters for interpretation
Ipamorelin’s development history is itself a lesson in cautious interpretation. The synthetic GH secretagogues came first, in the 1980s; the receptor they act on (GHS-R) was cloned in 1996; and the natural hormone that receptor evolved to sense (ghrelin) was identified only in 1999.[3][4] This means that for its first decade, Ipamorelin was a drug in search of a biology. When the biology arrived, it revealed that GHS-R1a is a receptor with wide-ranging roles — in appetite, metabolism, cardiovascular function, and reward — far beyond GH release. The lesson for anyone reading Ipamorelin claims is that a receptor selective agonist can still have unanticipated downstream effects, precisely because the receptor itself is embedded in multiple physiological systems. Selectivity for GH release among pituitary hormones is not the same as selectivity for a single physiological outcome.
How does Ipamorelin compare to other growth hormone peptides?
Ipamorelin is frequently compared to other GH-axis peptides, and the comparison is where its selective profile stands out. The table below summarizes the mechanistic differences. Note that regulatory status varies dramatically: only tesamorelin is FDA-approved, and only for a narrow indication.
| Peptide | Class / target | Approx. half-life | Selectivity notes | Regulatory status |
|---|---|---|---|---|
| Ipamorelin | Ghrelin mimetic (GHS-R1a agonist) | ~2 h | Highly selective; minimal cortisol/prolactin/ACTH effect | Not FDA-approved; research use only |
| GHRP-6 | Ghrelin mimetic (GHS-R1a agonist) | Short (minutes) | Raises cortisol, prolactin, and appetite alongside GH | Not FDA-approved; research use only |
| GHRP-2 | Ghrelin mimetic (GHS-R1a agonist) | Short (minutes) | Potent GH release; some cortisol/prolactin rise | Not FDA-approved; research use only |
| Sermorelin | GHRH analog (GHRH-R agonist) | ~2–3 min | GHRH(1-29) fragment; very short, pulsatile action | Historically approved; niche/research use |
| CJC-1295 (with DAC) | GHRH analog (GHRH-R agonist) | ~5–8 days | Albumin-binding depot; sustained GHRH signaling | Not FDA-approved; research use only |
| Tesamorelin | GHRH analog (GHRH-R agonist) | ~26 min | Stabilized GHRH(1-44); reduces visceral fat | FDA-approved (HIV-associated lipodystrophy) |
Ipamorelin vs. GHRP-6 and GHRP-2
All three are ghrelin mimetics acting at the same receptor, so they share the core GH-releasing mechanism. The difference is cleanliness. GHRP-6 is notorious for stimulating hunger and raising cortisol and prolactin; GHRP-2 is a more potent GH releaser but still shows some cortisol and prolactin activity. Ipamorelin was engineered specifically to keep the GH signal and drop the rest, and in head-to-head animal work it matched GHRP-6’s GH potency without the ACTH/cortisol/prolactin rise.[1]
Ipamorelin vs. sermorelin, CJC-1295, and tesamorelin
These three are a different mechanistic class — GHRH analogs acting at the GHRH receptor. They are not interchangeable with Ipamorelin. Sermorelin is a short GHRH fragment with a half-life of minutes; CJC-1295 with DAC is engineered to bind albumin and persist for days; and tesamorelin is a stabilized GHRH(1-44) analog and the only compound in this entire comparison that is FDA-approved, specifically for reducing excess visceral fat in HIV-associated lipodystrophy. For a deeper treatment of the approved GHRH analog, see our companion reference on what tesamorelin is, how it works, and its side effects.
The synergy rationale: why GHRH analogs and Ipamorelin are studied together
Because Ipamorelin (ghrelin arm) and GHRH analogs (GHRH arm) act on two separate receptors and two separate pathways, there is a well-grounded pharmacological rationale for combining them. GHRH primarily amplifies pulse amplitude via the cAMP/protein-kinase-A pathway, while ghrelin-receptor agonism drives calcium-dependent release through the Gq/PLC pathway and simultaneously suppresses somatostatin. Because these are non-redundant mechanisms converging on the same somatotroph, the combined GH output can exceed the simple sum of either agent alone — the definition of synergy rather than mere addition.
The molecular basis for this cooperativity has been studied directly. Work published in PNAS demonstrated that GHRH can act as an agonist at the ghrelin receptor GHS-R1a itself, that GHRH potentiates ghrelin’s inositol-phosphate signaling, and that the presence of GHRH increases ghrelin binding capacity in a dose-dependent, positively cooperative manner in pituitary cells.[11] Ghrelin-receptor activation also amplifies GHRH-induced cAMP accumulation through a PKC-dependent mechanism. In other words, the two receptors do not simply operate in parallel; they physically and functionally interact, which provides a genuine mechanistic foundation for co-administration.
This dual-pathway logic is the reason combinations such as CJC-1295 with Ipamorelin are so commonly studied together, and why a short-half-life ghrelin mimetic is often paired with a longer-acting GHRH analog to keep both arms engaged. It is important to be clear, however, that the synergy rationale is mechanistic and preclinical — it explains why a combination should produce more GH, but it is not the same as controlled clinical proof of superior human outcomes such as body-composition change, recovery, or longevity. No completed human trial has demonstrated that a CJC-1295/Ipamorelin combination improves any hard clinical endpoint.
What is the pharmacology and handling of Ipamorelin in research settings?
Ipamorelin is supplied for research as a lyophilized (freeze-dried) white powder, most commonly in 5 mg or 10 mg vials, and requires reconstitution before use in experimental models. Because the intact peptide is unstable in solution and sensitive to heat and light, handling protocols emphasize cold-chain storage of the powder and careful reconstitution technique.
General research-handling principles reported for peptides of this type include storing the sealed lyophilized vial refrigerated or frozen, reconstituting with bacteriostatic or sterile water introduced slowly down the vial wall (never injected forcefully onto the powder), gentle swirling rather than vigorous shaking to avoid shearing the peptide, and refrigerating the reconstituted solution with use within a limited window. For the mechanics of turning a milligram figure into a concentration and volume, our peptide reconstitution guide walks through the process step by step, and the dosage calculator handles the arithmetic of concentration per unit for a given vial size.
These handling notes are provided strictly in a research and educational context. They describe how the compound is managed in laboratory settings, not instructions for human administration.
Stability, half-life, and administration characteristics
Ipamorelin’s reported plasma half-life of roughly two hours reflects the metabolic stability engineered into its structure. Native ghrelin is degraded quickly, and unmodified peptides are vulnerable to serum peptidases. The unnatural residues in Ipamorelin — alpha-aminoisobutyric acid (Aib), the D-configuration amino acids, and the C-terminal amide — are the reason it survives longer in circulation than an ordinary linear peptide of similar length. Even so, a two-hour half-life is short relative to the depot GHRH analog CJC-1295 with DAC, and this difference in duration is a central variable that research designs must account for: a short half-life favors discrete, pulse-like GH release, whereas a long half-life produces more continuous receptor occupancy.
In the human POI trial, Ipamorelin was delivered by intravenous infusion, while the animal characterization work used both intravenous and subcutaneous routes.[2] Route matters because it changes the peak concentration and the shape of the exposure curve, which in turn shapes the GH-release response. As a peptide, Ipamorelin is not orally bioavailable in any meaningful way — the digestive tract degrades it — which is why parenteral routes dominate the research literature.
Reconstitution and concentration math in research
Reconstitution converts a labeled mass of lyophilized peptide into a solution of known concentration. The core relationship is simple: concentration equals the peptide mass divided by the volume of solvent added. A 5 mg vial reconstituted with 2 mL of solvent yields 2.5 mg/mL; the same 5 mg reconstituted with 1 mL yields 5 mg/mL. The vial size therefore does not, by itself, determine concentration — the solvent volume the researcher chooses does. This is precisely why the 5 mg and 10 mg presentations have separate protocol references, and why a dedicated calculator removes a common source of error. Our dosage calculator and reconstitution guide exist for exactly this arithmetic. Again, these are research-context tools; nothing here constitutes guidance for human dosing.
Vial-specific research protocols
Different vial strengths change the concentration math and the practical handling of the reconstituted solution. Detailed, size-specific research protocols are available for the two most common presentations: the Ipamorelin 10 mg vial dosage protocol and the Ipamorelin 5 mg vial dosage protocol. If any term in this article is unfamiliar — secretagogue, somatostatin, GHS-R1a, lyophilized — the peptide glossary defines it.
What are the limitations, open questions, and safety signals?
A genuinely useful reference is explicit about what is not established. For Ipamorelin, the gaps are large.
- No positive human efficacy data. The only completed controlled human trial was negative for its endpoint. Every popular claim about anti-aging, recovery, body composition, or sleep rests on mechanism and animal data, not human outcomes.[9]
- No long-term human safety data. The Beck trial dosed for up to seven days intravenously. There is no controlled evidence on the safety of chronic or long-term exposure in humans.[10]
- Theoretical class effects of raising GH. Any agent that increases GH raises theoretical concerns common to the GH axis — effects on insulin sensitivity and blood glucose, fluid retention, and joint symptoms — but these have not been systematically characterized for Ipamorelin specifically in controlled human studies.
- Product-quality uncertainty. Because Ipamorelin is sold as a research chemical rather than a regulated drug, identity, purity, and sterility are not guaranteed by any regulator, and independent testing has repeatedly found variability in research-peptide products across the market.
- Open mechanistic questions. The precise contribution of GHS-R1a constitutive activity, and the degree to which the ghrelin–GHRH synergy translates to durable physiological outcomes, remain active research questions.[5]
How reliable is the quality of research-grade Ipamorelin?
Because Ipamorelin is sold as a research chemical rather than a regulated pharmaceutical, the identity, purity, and sterility of a given vial are not guaranteed by any regulatory authority. This is not a hypothetical concern. A 2026 analysis titled “Evaluation of Research Grade Peptides Marketed Directly to Consumers Reveals Extensive Variability in Purity and Measured Abundance” examined thousands of samples across fourteen compounds — Ipamorelin explicitly among them — and found that, depending on the quality model applied, between roughly 42% and 71% of samples failed to meet basic quality criteria, with measurable endotoxin contamination present in about 15% of samples.[14]
The practical consequences for research integrity are significant. A certificate of analysis supplied by a vendor is not the same as independent verification, and purity overstatement is a recurring finding when the two are compared. For any experimental use, the identity of the material (is it actually Ipamorelin and not a different or degraded peptide?), its stated purity, and its endotoxin burden are variables that must be established independently rather than assumed. This is a core reason the compound is appropriate only for controlled research settings equipped to characterize what they are actually working with.
| Quality dimension | Why it matters in research | How it is assessed |
|---|---|---|
| Identity | Confirms the vial contains Ipamorelin, not a different or partial peptide | Mass spectrometry (molecular weight ~711.9) |
| Purity | Impurities as low as ~1% can confound biological assays | HPLC (high-performance liquid chromatography) |
| Endotoxin / sterility | Contamination invalidates results and poses biohazard | Endotoxin (LAL) and sterility testing |
| Content / abundance | Actual peptide mass may differ from the label | Quantitative assay vs. stated vial mass |
What is the current regulatory status of Ipamorelin?
As of July 2026, Ipamorelin is not approved by the U.S. FDA for any human therapeutic indication. It never reached market as a medicine; its clinical development for postoperative ileus was discontinued after the Phase II trial failed to show efficacy.[2] It is therefore classified and handled as a research-use-only compound, not a drug intended for human diagnosis, treatment, or prevention of disease.
The compounding landscape has been a subject of active regulatory attention. Ipamorelin was among the peptides placed under FDA scrutiny in the review of substances nominated for compounding under Section 503A, and it has been discussed alongside other GH-axis peptides in the ongoing reassessment of peptide compounding policy. Regulatory positions in this area have shifted and remain in flux, so anyone tracking status for compounding purposes should consult current FDA communications directly rather than rely on secondary summaries. What is not in flux is the core fact: Ipamorelin has no FDA marketing approval as a therapeutic product.
The regulatory bottom line for this reference is straightforward. Ipamorelin is an investigational research peptide. It is discussed here for scientific and educational purposes, and nothing in this article should be read as endorsing human use or as medical advice.
What are the open questions and future research directions?
Ipamorelin’s file is not closed — it is simply incomplete. Several questions remain genuinely unresolved and would need controlled study to answer.
- Does the selective GH release translate to any human benefit? The bone-anabolic and body-composition effects seen in rodents have never been tested in a controlled human trial with those outcomes as endpoints. Whether Ipamorelin’s pulsatile GH release produces meaningful change in human bone density, lean mass, or metabolic markers is unknown.
- What is the long-term safety of chronic GH elevation via a secretagogue? The only human safety data come from a seven-day IV course.[10] Sustained elevation of the GH/IGF-1 axis carries theoretical concerns — insulin resistance, fluid retention, and the complex and unsettled relationship between IGF-1 signaling and longevity[13] — none of which have been characterized for Ipamorelin over meaningful timeframes.
- Does combining Ipamorelin with a GHRH analog improve outcomes, or just GH numbers? The synergy at the level of GH secretion is mechanistically supported,[11] but whether a larger GH pulse yields a better clinical result — or simply a bigger number — is untested in controlled human trials.
- How much does product quality distort the existing informal evidence? Given documented purity and contamination problems in gray-market Ipamorelin,[14] anecdotal reports of effects (or side effects) may reflect impurities or misidentified peptides rather than Ipamorelin itself.
- Will the regulatory status change? Peptide compounding policy has been under active reassessment, and Ipamorelin’s standing could shift. This is a policy question to track through primary FDA sources, not a settled matter.
Until these questions are addressed by properly designed studies, the accurate description of Ipamorelin is a well-characterized, selective research peptide with strong preclinical mechanism, meaningful animal data on bone and growth, one negative human efficacy trial, acceptable short-term human tolerability, and no proven human therapeutic benefit. That description is neither hype nor dismissal — it is simply where the evidence stands.
What is Ipamorelin studied for, and what are the common misconceptions?
Ipamorelin is widely discussed online in the context of anti-aging, muscle gain, fat loss, injury recovery, and sleep quality. It is worth stating plainly which of these are grounded in evidence and which are extrapolations from mechanism.
What the evidence base actually supports
- GH release. Ipamorelin reliably and selectively releases growth hormone in animals and humans. This is well established.[1]
- Anabolic effects on bone and body weight in rodents. Multiple rat studies show increased longitudinal bone growth, bone mineral content, and body weight.[6][7] These are animal findings.
- Acceptable short-term tolerability in a human IV course. The POI trial found adverse events comparable to placebo over up to seven days.[9]
Common misconceptions to correct
- “Ipamorelin is proven for anti-aging.” There is no controlled human trial demonstrating anti-aging, longevity, or healthspan benefit. The anti-aging rationale rests on the somatopause concept and animal anabolic data, not human outcomes.
- “It builds muscle in humans.” No completed human trial has demonstrated muscle-mass or strength gains from Ipamorelin. Body-weight and bone data are from rodents.[7]
- “It failed the ileus trial, so it doesn’t raise GH.” Incorrect — the trial failed on a gut-motility endpoint, not on GH pharmacology. Ipamorelin does raise GH; what it did not do was translate that into a clinical benefit for postoperative ileus.[9]
- “Because it’s natural/ghrelin-like, it’s inherently safe.” Mechanistic plausibility is not safety data. Long-term human safety of chronic GH elevation via Ipamorelin has not been characterized in controlled studies.
- “Research-grade material is the same as pharmaceutical-grade.” Independent testing repeatedly finds purity and contamination problems in gray-market peptides, including Ipamorelin.[14]
The honest posture toward Ipamorelin is that of a mechanistically elegant, well-characterized research peptide whose human clinical value remains unproven. That is not a dismissal — it is an accurate reading of a compound with strong preclinical credentials and a thin, and so far negative, human efficacy record.
Frequently Asked Questions
Is Ipamorelin FDA-approved?
No. Ipamorelin is not approved by the FDA for any human therapeutic use. It was developed pharmaceutically as NNC 26-0161 and later tested in a Phase II human trial for postoperative ileus, but that trial failed its primary efficacy endpoint and development was discontinued. Today it is handled as a research-use-only compound, not an approved medicine.
What makes Ipamorelin different from GHRP-6 and GHRP-2?
All three activate the same ghrelin receptor (GHS-R1a) to release growth hormone, but Ipamorelin is far more selective. In the original characterization, Ipamorelin released GH with potency comparable to GHRP-6 but without meaningfully raising cortisol, ACTH, prolactin, or appetite — the off-target effects that make GHRP-6 and, to a lesser degree, GHRP-2 less clean pharmacological tools.
Does Ipamorelin actually raise growth hormone in humans?
Yes, at the level of mechanism it does. During pharmaceutical development Ipamorelin was shown to increase plasma growth hormone in humans, consistent with its ghrelin-receptor agonism. What is missing is proof that this GH rise translates into a clinical benefit: the one completed controlled human efficacy trial, in postoperative ileus, was negative.
Is there any human clinical evidence that Ipamorelin works?
Not for any of its popular uses. The only completed, published, controlled human efficacy trial studied postoperative ileus after bowel surgery and found no significant benefit over placebo. All claims about anti-aging, muscle, bone, recovery, or sleep are based on mechanism and animal studies, not on positive human outcome data.
What is the half-life of Ipamorelin?
Research reports describe a plasma half-life of roughly two hours. That is longer than the very short-acting GHRH fragment sermorelin (a few minutes) but far shorter than CJC-1295 with DAC, which binds albumin and persists for several days. Half-life is one of the properties that distinguishes the different growth-hormone peptides from one another.
How does Ipamorelin compare to tesamorelin?
They belong to different mechanistic classes. Ipamorelin is a ghrelin mimetic acting at GHS-R1a, whereas tesamorelin is a stabilized GHRH analog acting at the GHRH receptor. Crucially, tesamorelin is FDA-approved for reducing visceral fat in HIV-associated lipodystrophy, while Ipamorelin has no FDA approval for any indication.
Why are Ipamorelin and CJC-1295 studied together?
Because they act on two different receptors and two complementary pathways. GHRH analogs like CJC-1295 amplify GH pulse amplitude, while Ipamorelin initiates release through the ghrelin receptor and suppresses somatostatin. Mechanistic studies show the two pathways can interact synergistically, which is the pharmacological rationale for pairing them — though this rationale is preclinical, not proven in controlled human outcome trials.
How is Ipamorelin handled and stored in research settings?
It is typically supplied as a lyophilized powder in 5 mg or 10 mg vials and reconstituted with sterile or bacteriostatic water before experimental use. Because the peptide is unstable in solution, protocols emphasize refrigerated or frozen storage of the powder, gentle reconstitution, and limited use windows once dissolved. These are laboratory-handling notes for research contexts, not human-use instructions.
References
- Raun K, Hansen BS, Johansen NL, et al. Ipamorelin, the first selective growth hormone secretagogue. European Journal of Endocrinology. 1998;139(5):552–561. https://academic.oup.com/ejendo/article-abstract/139/5/552/6748390
- Ipamorelin. Wikipedia (pharmacological identity, development history, and clinical status). https://en.wikipedia.org/wiki/Ipamorelin
- Howard AD, Feighner SD, Cully DF, et al. A receptor in pituitary and hypothalamus that functions in growth hormone release. Science. 1996;273(5277):974–977. https://www.science.org/doi/10.1126/science.273.5277.974
- Kojima M, Hosoda H, Date Y, Nakazato M, Kangawa K. Ghrelin is a growth-hormone-releasing acylated peptide from stomach. Nature. 1999;402(6762):656–660. https://www.nature.com/articles/45230
- Mear Y, Enjalbert A, Thirion S. GHS-R1a constitutive activity and its physiological relevance. Frontiers in Neuroscience. 2013;7:87. https://pmc.ncbi.nlm.nih.gov/articles/PMC3665924/
- Johansen PB, Nowak J, Skjaerbaek C, et al. Ipamorelin, a new growth-hormone-releasing peptide, induces longitudinal bone growth in rats. Growth Hormone & IGF Research. 1999;9(2):106–113. PMID 10373343. https://pubmed.ncbi.nlm.nih.gov/10373343/
- Svensson J, Lall S, Dickson SL, et al. The GH secretagogues ipamorelin and GH-releasing peptide-6 increase bone mineral content in adult female rats. Journal of Endocrinology. 2000;165(3):569–577. https://joe.bioscientifica.com/view/journals/joe/165/3/569.xml
- Andersen NB, Malmlöf K, Johansen PB, et al. The growth hormone secretagogue ipamorelin counteracts glucocorticoid-induced decrease in bone formation of adult rats. Growth Hormone & IGF Research. 2001;11(5):266–272. PMID 11735244. https://www.sciencedirect.com/science/article/abs/pii/S1096637401902394
- Beck DE, Sweeney WB, McCarter MD; Ipamorelin 201 Study Group. Prospective, randomized, controlled, proof-of-concept study of the ghrelin mimetic ipamorelin for the management of postoperative ileus in bowel resection patients. International Journal of Colorectal Disease. 2014;29(12):1527–1534. PMID 25331030. https://link.springer.com/article/10.1007/s00384-014-2030-8
- Safety and Efficacy of Ipamorelin for Management of Post-Operative Ileus (NCT00672074). ClinicalTrials.gov. https://clinicaltrials.gov/study/NCT00672074
- Casanueva FF, Camiña JP, Carreira MC, et al. Growth hormone-releasing hormone as an agonist of the ghrelin receptor GHS-R1a. Proceedings of the National Academy of Sciences. 2008;105(51):20452–20457. PMID 19088192. https://pubmed.ncbi.nlm.nih.gov/19088192/
- Steyn FJ, Tolle V, Chen C, Epelbaum J. Neuroendocrine regulation of growth hormone secretion. Comprehensive Physiology. 2016;6(2):687–735. https://onlinelibrary.wiley.com/doi/10.1002/j.2040-4603.2016.tb00692.x
- Junnila RK, List EO, Berryman DE, Murrey JW, Kopchick JJ. The GH/IGF-1 axis in ageing and longevity. Nature Reviews Endocrinology (PMC review). 2013;9(6):366–376. https://pmc.ncbi.nlm.nih.gov/articles/PMC4074016/
- Evaluation of Research Grade Peptides Marketed Directly to Consumers Reveals Extensive Variability in Purity and Measured Abundance. 2026. https://www.researchgate.net/publication/404218857